")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
The Association Between Health-Related Behaviors and Traditional Chinese Medicine Syndromes in Type 2 Diabetes Mellitus Patients
Authors Wang L, Li J, Dang Y, Pan R, Niu Y
Received 28 March 2023
Accepted for publication 23 June 2023
Published 30 June 2023 Volume 2023:16 Pages 1977—1985
DOI https://doi.org/10.2147/DMSO.S409179
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Liqun Wang,1,2,* Jiangping Li,1,2,* Yuqi Dang,3 Ruiping Pan,4 Yang Niu5
1Department of Epidemiology and Statistics, School of Public Health at Ningxia Medical University, Yinchuan, Ningxia, People’s Republic of China; 2Key Laboratory of Environmental Factors and Chronic Disease Control, Ningxia Medical University, Yinchuan, Ningxia, People’s Republic of China; 3Department of Endocrinology, Yinchuan Hospital of Traditional Chinese Medicine, Yinchuan, Ningxia, People’s Republic of China; 4Department of Chinese Medicine, the Second People’s Hospital of Shizuishan, Shizuishan, Ningxia, People’s Republic of China; 5Key Laboratory of the Ningxia Ethnomedicine Modernization, Ministry of Education, Ningxia Medical University, Yinchuan, Ningxia, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yang Niu, Key Laboratory of the Ningxia Ethnomedicine Modernization, Ministry of Education, Ningxia Medical University, Yinchuan, 750004, People’s Republic of China, Tel +8613909574577, Email [email protected]
Background: Traditional Chinese medicine (TCM) has certain advantages in treating diabetes via TCM syndromes differentiation, and health-related behaviors can regulate TCM syndromes. This study aimed to identify the clusters of TCM syndromes in type 2 diabetes mellitus (T2DM) patients and to explore the association between health-related behaviors and those TCM syndromes clusters.
Methods: This was a cross-sectional study of 1761 T2DM patients from the Ningxia Province. The TCM syndromes (11 TCM syndromes in total) scale was used to collect the syndrome information. Health-related behaviors, including smoking, alcohol use, tea drinking, the intensity of physical activity, sleep quality, and sleep duration, were collected via a face-to-face interview questionnaire. Latent profile analysis was employed to identify clusters of 11 TCM syndromes. Multinomial logistic regression was employed to examine the relationships between health-related behaviors and clusters of TCM syndromes.
Results: TCM syndromes in T2DM patients were classified into three profiles using latent profile analysis: light, moderate, and heavy. Participants with poor health-related behaviors were more likely to have heavy 1.49 (95% CI: 1.12, 1.99) or moderate 1.75 (95% CI: 1.10, 2.79) profiles than those with good health-related habits. Smokers, tea drinkers, and those with poor sleep quality were more likely to have a moderate profile and heavy profile than a light profile. Compared with heavy physical activity, moderate activity 0.24 (95% CI: 0.07, 0.88) was negatively associated with a heavy profile.
Conclusion: Results showed that most participants had light or moderate levels of TCM syndromes, and those with poor health-related behaviors were more likely to have heavy or moderate profiles. In the context of precision medicine, these results have important implications for understanding the prevention and treatment of diabetes via changing lifestyles and behaviors to regulate TCM syndromes.
Keywords: health-related behaviors, traditional Chinese medicine syndromes, latent profile analysis, T2DM patients
Introduction
As a common chronic non-communicable disease, diabetes has become a major public health issue in the world.1 A recent study indicated that there were approximately 422 million diabetes patients worldwide, most of which were type 2 diabetes mellitus (T2DM) cases.2 In China, the prevalence of diabetes has increased steadily, and prolonged hyperglycemia leads to complications that seriously affect the patient’s life quality.3,4 Therefore, strategies to prevent and control diabetes have become an urgent public health need in China and the world.
Since a significant proportion of patients fail to get satisfactory treatment from conventional medicine, many seek help from complementary and alternative medicine, especially Traditional Chinese medicine (TCM).5 TCM has a long history and unique advantages in diagnosing and treating T2DM. It can classify the patients into TCM syndrome types through syndrome differentiation or “bian zheng lun zhi” in Chinese.6 That is, the patient’s causes, symptoms, pulse conditions, etc., are combined with traditional Chinese medicine theory to conduct a comprehensive analysis, judgment and treatment.6 Through the differentiation of TCM syndromes, holistic treatment can be carried out to regulate the balance of qi and blood, yin and yang of bodies. TCM syndrome types, such as Yin deficiency, Yang deficiency, Qi deficiency, blood deficiency, phlegm dampness, heat formation, and damp heat, play an indispensable role in treating T2DM. Different treatments can be conducted based on the TCM syndrome types of T2DM patients.7 Meanwhile, the newly published diagnosis and treatment guidelines for combining the disease and syndrome of T2DM suggested that during the diagnosis and treatment of T2DM, prescriptions can be optimized according to syndrome differentiation and treatment, and drugs can be used rationally to achieve both symptom and disease treatment.8 Moreover, syndrome differentiation has shown great efficacy in treating T2DM.9
However, T2DM patients usually have many combined syndromes rather than a single TCM syndrome, and the interaction between deficiency and excess syndrome complicates the condition. Given the complex characteristics of TCM syndromes, there is a growing research interest in TCM syndromes to provide opportunities for effective interventions for diabetes. Latent profile analysis, one of the more complex analytical methods, can help understand the complex relationships among TCM syndromes. Latent profile analysis has increasingly been applied in other studies;10–12 however, no study has estimated profiles of TCM syndromes until now.
Identifying modifiable health-related behavioral determinants of different clusters of TCM syndromes is paramount to providing an effective approach to diabetes patients. Modifiable health-related behaviors, including smoking, excessive alcohol use, tea drinking, poor diet, insufficient sleeping, poor sleep quality, and physical inactivity, are associated with individuals’ health, such as obesity, diabetes, coronary heart disease, and self-reported multiple chronic conditions.13–16 Previous studies have reported the association between health-related behaviors and TCM syndromes among patients with acute myocardial infarction or dyslipidemia and suggested a positive relationship between smoking, alcohol use, and Phlegm-dampness syndrome.17,18 A recent study found that sleep quality was associated with kidney deficiency, blood deficiency, and blood stasis syndrome in patients with cognitive impairment.19 No study has directly linked health-related behaviors with TCM syndromes among T2DM patients.
Hence, this study aimed to identify different clusters of TCM syndromes in T2DM patients and to examine the relationships between these clusters and indicators of health-related behaviors.
Materials and Methods
Data Source and Study Sample
We conducted a cross-sectional analysis based on data obtained from August 2019 to November 2020 in Ningxia Province, China. The detailed sampling process can be found elsewhere.20 Briefly, we selected all participants who completed the survey. At stage one, 48 government hospitals (as recorded in the Ningxia Statistics Bureau) were selected as the primary sampling units (PSU). At stage two, hospital types were classified as Chinese medicine hospitals and general hospitals. At stage three, 10 hospitals (five Chinese medicine and five general hospitals) were selected using a probability proportionate to size (PPS) sampling method based on the hospital size and number of beds. Then, T2DM patients in each hospital’s endocrinology department were selected.
Ultimately, we recruited 1761 participants (Figure 1) who had lived at their current address for at least six months and were more than 18 years old. We excluded patients with: a) severe mental disorders; b) a severe illness that prevents communication; c) deafness, aphasia or other language barriers; d) pregnancy or lactation; e) diabetic ketoacidosis in the past month; f) malignant tumor; and g) refusal to sign an informed consent. The Institutional Review Board of the Yinchuan Hospital of Traditional Chinese Medicine approved this study. The research procedures of this study involving human participants conformed with the 1964 Helsinki declaration and the later amendments or similar ethical standards.
 |
Figure 1 Selection of study participants. |
Dependent Variables
TCM Syndromes
TCM syndromes was defined as a pathological summary of the body at a certain stage in the process of disease development. According to the diagnostic criteria of the syndrome and the clinical performance at the investigation time, patients’ information was collected to measure the distribution and manifestation of TCM syndromes or “bian zheng lun zhi”, in Chinese, through syndrome differentiation. Syndrome differentiation is the process of summarizing all symptoms and signs gathered by the four examinations, namely looking, smelling, questioning, and palpating (or pulse-feeling). Each of the four-examination information is divided into none, light, moderate, and heavy, with a score of 0, 2, 4, 6, respectively. The syndrome decides the therapeutic methods.21 In this study, TCM syndromes mainly include Yin-deficiency syndrome, Yang-deficiency syndrome, Qi-deficiency syndrome, blood deficiency syndrome, Qi-stasis syndrome, blood stasis syndrome, hyperactivity of liver yang syndrome, Phlegm-dampness syndrome, Junction-heat syndrome, Depression-heat syndrome, and damp-heat syndrome. The TCM syndromes scale was used to collect the syndrome information, with higher scores indicating higher severity of TCM syndrome. The study’s reliability tests were: Cronbach a=0.842 (95% confidence interval [CI]: 0.725–0.926); split-half reliability coefficient: R=0.869.
Explanatory Factors
The study included six health-related behaviors, smoking, alcohol use, tea drinking, physical activity, sleep quality, and sleep duration. Smoking was defined as consuming one cigarette or more per day and lasting at least six months. Alcohol use was defined as drinking more than one glass of alcohol in the past month, equal to half a bottle of beer or 125 milliliters of grape or fruit wine or 40 milliliters of white wine. Tea drinking frequency was assessed by asking the question, “How often do you drink tea (days per week)?” with possible responses: once a day or more, 5–6 times/week, 3–4 times/week, 1–2 times/week, less than once a week and never. We defined tea drinking as dichotomous variables (yes vs no).
Physical activity was estimated using the question, “Do you perform at least 30 minutes of physical activity at work and/or leisure time more than 4 days a week (yes vs no)?”.
The intensity of physical activity was investigated by asking: “How about the intensity of physical activity (light, moderate, heavy)?”. Sleep quality was classified into three categories: poor, moderate, and good using the question, “What do you think of your sleep quality?” Sleep duration was collected as continuous data in this study, and participants who reported 7–9 hours of sleep were classified as the normal sleep group.22
Covariates
Demographic information included age, gender, ethnicity (Han vs minority), residence (rural vs urban), educational attainment, marital status (unmarried, married, and widowed or divorced), occupation (farmer vs others), and family income. Family income was defined as the family’s average individual monthly income and was divided into five groups: <1000 RMB, 1000–1999 RMB, 2000–2999 RMB, 3000–4999 RMB, and 5000 RMB or more.
Body mass index (BMI, computed by body weight in kilograms divided by square of height in meters), the combination of meat and vegetable in diet (meat-based, vegetarian-based, half-meat and half-vegetarian), other chronic diseases (yes vs no), family history of T2DM (yes vs no), taking hypoglycemic drugs (yes vs no), T2DM complications (yes vs no), and disease duration (continuous data) were abstracted from medical records.
Statistical Analysis
Latent profile analysis (LPA) was performed to classify continuous data into optimal clusters using Mplus version 8.0.23 We examined the latent profile models using data from 11 TCM syndromes. Different criteria were used to evaluate the LPA model fit and choose the best reading profile models. The Akaike’s Information Criterion (AIC), Bayesian Information Criterion (BIC), and aBIC (Bayesian Information criterion using sample size adjustment) were applied to compare models with different numbers of profiles. Lower values of these fit indices indicated better model fit. The Lo-Mendell-Rubin-Adjusted (LMRA) likelihood ratio test and the Bootstrapped likelihood ratio test (BLRT) were employed to compare models with adjacent numbers of profiles. A p-value of <0.05 indicates that a particular model fits better than another with one fewer profiles.24 Continuous variables were presented as mean (standard deviation), and categorical variables were expressed as frequencies and percentages (n%). Differences in continuous or categorical variables across TCM syndromes profiles were tested using ANOVA analysis or Chi-square test. The ordinal logistic regression model could not be used because the p-value of the parallelism test was < 0.05. Therefore, multinomial logistic regression was used to examine the relationships between health-related behaviors and clusters of TCM syndromes after controlling for age, gender, marital status, education, occupation, economic condition, residence, BMI, other chronic diseases, T2DM complications, disease duration, the combination of meat and vegetable in diet, family history of T2DM, and in-take of hypoglycemic drugs. Analyses were performed using the Statistical Package for the Social Sciences (SPSS) version 24.0 (SPSS Inc., Chicago, Illinois).
Results
Latent Profile Analysis
A total of 1761 participants were included in this study (Supplementary Table 1). There were 11 TCM syndromes, and models with one to four latent profiles were estimated using latent profile analysis. Model-fit indices are presented in Table 1. As the number of estimated profiles increased, the AIC, BIC, and aBIC generally decreased, while entropy remained above 0.80 in all models. However, the LMRA and BLRT p-values in the four-cluster model were not significant, indicating that the three-cluster model was the preferred model according to that criterion.
 |
Table 1 Model-Fit Indices for Latent Class Factor Analysis for TCM Syndromes (N=1761) |
Figure 2 exhibits the cluster-specific estimated probabilities of TCM syndromes for the three-cluster model from LPA according to TCM syndromes scores. Class 1 was characterized by light overall TCM syndromes and was named the Light syndrome profile, with 37.9% of the participants belonging to Class 1. Class 2 was characterized by moderate overall TCM syndromes and was labelled the Moderate syndrome profile, with 47.7% belonging to Class 2. Finally, Class 3 was characterized by heavy overall TCM syndromes and was named the Heavy syndrome profile. Only 14.4% belonged to Class 3. Yin-deficiency syndrome, Qi-deficiency syndrome, and Phlegm-dampness syndrome were most frequent in T2DM patients (Figure 2).
 |
Figure 2 Cluster-specific probabilities of TCM syndromes for the three-cluster model. |
Characteristics of Three Clusters
Table 2 shows the characteristics of three profiles. Females, living in rural areas, with lower economic levels, other chronic diseases, T2DM complications, and long disease duration were distributed more in the heavy profile. Meanwhile, smokers were more common among the moderate profile. Patients who drank tea more often and had poor sleep quality and shorter or longer sleep duration were more common among moderate or heavy profile.
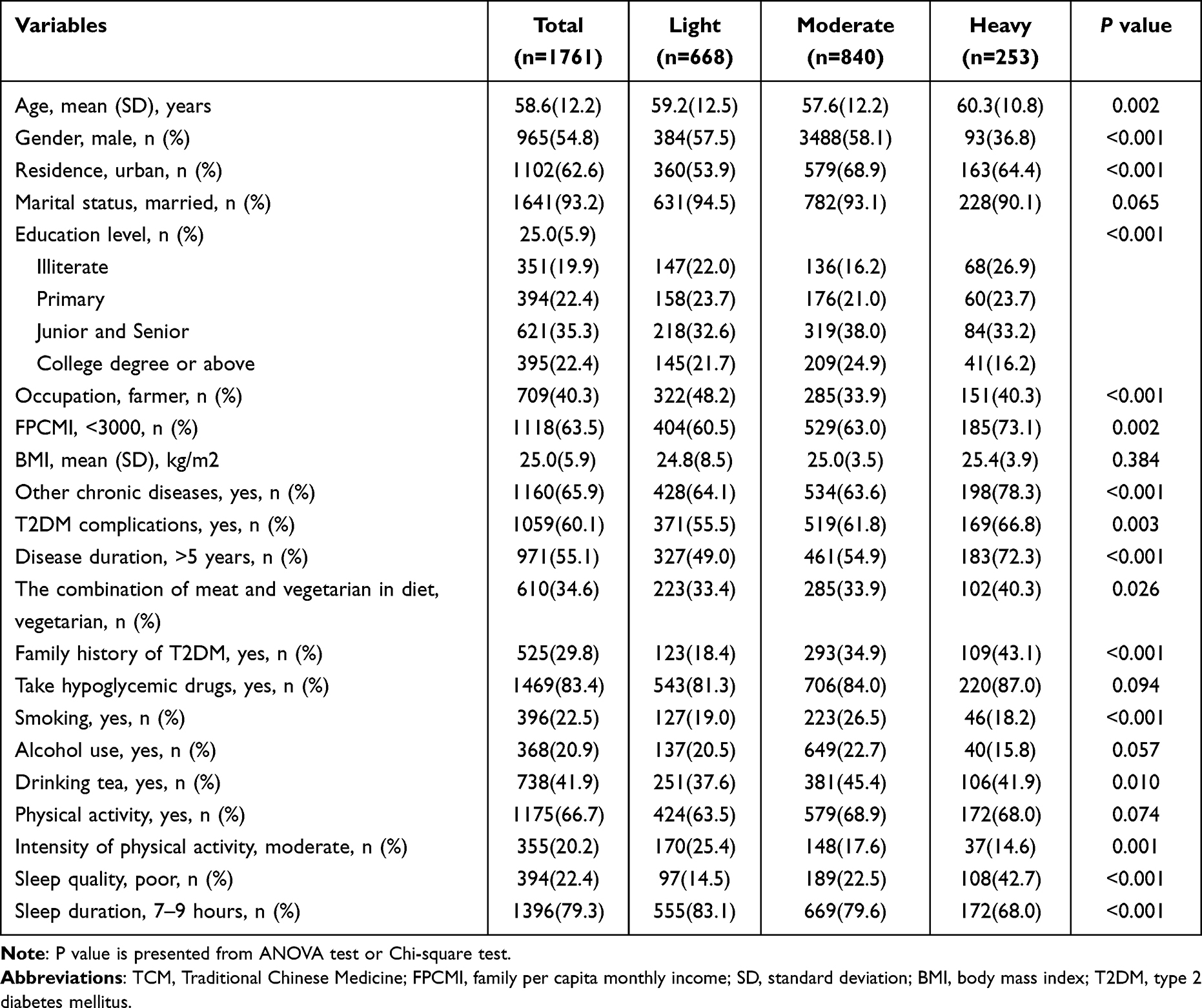 |
Table 2 Characteristics and TCM Syndrome Distribution of the Clusters |
Multinomial Logistic Regression Analysis
As shown in Table 3, after controlling the confounders, T2DM patients with poor health-related behaviors were more likely to have a heavy or moderate profile than those with good health-related habits. Among the six health-related indicators, smoking showed significance in the profile of TCM syndromes. The relative risk ratios for moderate and heavy profiles were 1.49 (95% CI: 1.12, 1.99) and 1.75 (95% CI: 1.10, 2.79), respectively. In addition, patients who drank tea and had poor sleep quality were more likely to have moderate and heavy profiles than a light profile. Furthermore, moderate intensity of physical activity was negatively associated with the heavy profile compared with heavy physical activity. Meanwhile, those whose sleep duration did not in the normal range (7–9 hours) were more likely to have a heavy profile. Finally, those with poor health-related behaviors were more likely to with heavy or moderate profile.
 |
Table 3 Relative Risk Ratios for the Relationships Between Health Behaviors and Clusters from Multinomial Logistic Regression Analyses (n=1761)a |
Discussion
The current study explored the clusters of eleven TCM syndromes in 1761 T2DM patients, namely: Yin-deficiency syndrome, Yang-deficiency syndrome, Qi-deficiency syndrome, blood deficiency syndrome, Qi-stasis syndrome, blood stasis syndrome, hyperactivity of liver yang syndrome, Phlegm-dampness syndrome, Junction-heat syndrome, Depression-heat syndrome, and damp-heat syndrome. Latent profile analysis identified three profiles (light, moderate and heavy) in this study, with 85.6% belonging to the light or moderate profile. In addition, this study reported associations between health-related behaviors and the profiles of TCM syndrome.
The LPA showed that 85.6% of TCM syndromes of T2DM patients belonged to the light or moderate level, implying a lower prevalence of heavy levels of TCM syndromes even if various kinds of TCM syndromes appeared. This finding may provide more opportunities for physical regulation and further control of diabetes. In addition, this study found that Yin-deficiency, Qi-deficiency, and Phlegm-dampness syndromes were more common in T2DM patients. A previous study reported that Qi and Yin deficiency syndromes were common TCM syndromes in male patients with T2DM.25 A study of 270 T2DM patients showed Yin deficiency, Qi deficiency, and Phlegm-dampness or damp-heat syndromes were more frequent than other syndromes.26,27
Another aim of this study was to explore the relationship between health-related behaviors and the profiles of TCM syndrome. The results showed that smoking was a possible risk factor for light or moderate profile. A previous study has suggested that long-term smoking and alcohol drinking can cause Yin deficiency of the lung, damp-heat and turbid phlegm, poor Qi and blood operation, and phlegm-dampness syndrome.28 In addition, participants with poor sleep quality were more likely to have moderate and heavy profiles. The possible reason may be that T2DM patients with Yang deficiency syndrome frequently urinate at night. In addition, participants with poor sleep quality were prone to headaches, dizziness, irritability, etc., which could lead to hyperactivity of liver yang syndrome.28 It was also reported that people with poor sleep quality had poorer mental health,29 which can further exacerbate the Qi-stasis syndrome. Furthermore, this study found that those with sleep duration outside the normal range (7–9 hours) were more likely to have a heavy profile. This result was consistent with a previous study in which longer or shorter nighttime sleep duration was positively correlated with the Yang-deficiency, Qi-stasis, Junction-heat, Depression-heat, and damp-heat syndromes.30 The positive association between drinking tea and moderate or heavy profile can be explained by the fact that in China, people usually like to add sugar when drinking tea, and the intake of excess sugar may aggravate the progress of diabetes,31,32 leading to the heavy level of TCM syndromes. In summary, T2DM patients with poor health-related behaviors were more likely to have heavy or moderate profiles, and this may reflect a potential method in T2DM treatment via lifestyle modification. The treatment of diabetes can be based on western medicine, such as oral hypoglycemic drugs or insulin injections, and then different treatments are chosen, particularly methods based on various TCM syndromes, to optimize the treatment. The possible mechanism may be that according to TCM syndromes to formulate TCM prescriptions, which specific to the treatment of T2DM, for example, resolving phlegm, and dehumidifying and activating the blood can help improve lipid metabolism could reduce fat accumulation, improve circulation, promote the use of nutrients in the body, increase the utilization of insulin in the muscles and other cells, and reduce insulin resistance.33
Strength and Limitations
The strengths of this study were as follows. First, this study employed LPA to identify clusters of TCM syndromes in T2DM patients. Second, this study is the first to examine the profiles of TCM syndromes and how these are associated with health-related behaviors. Third, given the increasing rate of diabetes in the Chinese population, the present findings have relevance for understanding the prevention and treatment of diabetes. However, this study had some limitations. This was a cross-sectional analysis that prevents making causal inferences. In addition, there results may be affected by selection bias as all participants were from the endocrinology department of hospitals. Besides, the use of questionnaire to collect some information may have memory bias although we carefully defined our survey questions, and the interviews were conducted by well-trained interviewers. Finally, although this study uses a structured and quantitative TCM syndrome scale, it is still difficult to avoid subjectivity in the process of TCM syndrome differentiation, which has a certain impact on the results.
Conclusions
This is the first study to investigate the relationship between different levels of TCM syndromes in a sample of T2DM patients. The results suggested that most participants had light or moderate levels of TCM syndromes. Additionally, those with poor health-related behaviors were more likely to have heavy or moderate profiles. These results have important implications for understanding the prevention and treatment of diabetes via changing lifestyles and behaviors to regulate TCM syndromes and provide a reference and suggestions for individualized and precision treatments.
Data Sharing Statement
The data used to support the findings of this study are included within the Supplementary Table 1.
Informed Consent
All the participants provided a written informed consent form at the beginning of the survey.
Acknowledgments
We thank all hospitals and participants for their cooperation, and thank professor Yi Nan for guidance of TCM syndrome scale, thank Dr. Ning Yan for language modification.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Natural Science Foundation of China (grant number 82204955).
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Maffi P, Secchi A. The burden of diabetes: emerging data. Dev Ophthalmol. 2017;60:1–5.
2. Cooke S, Pennington K, Jones A, et al. Effects of exercise, cognitive, and dual-task interventions on cognition in type 2 diabetes mellitus: a systematic review and meta-analysis. PLoS One. 2020;15(5):e0232958.
3. Ma RC. Epidemiology of diabetes and diabetic complications in China. Diabetologia. 2018;61(6):1249–1260. doi:10.1007/s00125-018-4557-7
4. Francesca V, Pamela P, Carlo G, et al. Metabolic syndrome, serum uric acid and renal risk in patients with T2DM. PLoS One. 2017;12(4):e176058. doi:10.1371/journal.pone.0176058
5. Zeng XX, Bian ZX, Wu TX, et al. Traditional Chinese Medicine Syndrome Distribution in Chronic Hepatitis B Populations: a Systematic Review. Am J Chine Med. 2011;39(6):1061–1074. doi:10.1142/S0192415X11009408
6. Xutian S, Zhang J, Louise W. New exploration and understanding of traditional Chinese medicine. Am J Chine Med. 2009;37(5):411–426. doi:10.1007/s10900-012-9543-2
7. Fu C, Zhang NL, Chen BX, et al. Identification and classification of traditional Chinese medicine syndrome types among senior patients with vascular mild cognitive impairment using latent tree analysis. J Integr Med. 2017;15(3):186–200. doi:10.1016/S2095-4964(17)60335-2
8. Professional Committee of Endocrine and Metabolic Diseases, Integrated Traditional Chinese and Western Medicine Branch, Chinese Medical Association. Diagnosis and treatment guide for combination of disease and syndrome of type 2 diabetes. J Traditional Chine Med. 2021;62(4):361–368.
9. Wang Q. The Present Situation of TCM Treatment for Diabetes and its Researches. J Traditional Chine Med. 2003;23(1):67–73.
10. Grant R, Becnel JN, Giano ZD, et al. A latent profile analysis of young adult lifestyle behaviors. Am J Health Behav. 2019;43(6):1148–1161. doi:10.5993/AJHB.43.6.12
11. Gagliardini G, Gullo S, Tinozzi V, et al. Mentalizing subtypes in eating disorders: a latent profile analysis. Front Psychol. 2020;11:56429. doi:10.3389/fpsyg.2020.564291
12. Ekblom-bak E, Stenling A, Eriksson JS, et al. Latent profile analysis patterns of exercise, sitting and fitness in adults-Associations with metabolic risk factors, perceived health, and perceived symptoms. PLoS One. 2020;15(4):e232210. doi:10.1371/journal.pone.0232210
13. Park S, Shin J, Baek S. Analysis of Health-Related Behaviors of Adult Korean Women at Normal BMI with Different Body Image Perceptions: results from the 2013-2017 Korea National Health and Nutrition Examination Survey (KNHNES). Int J Environ Res Public Health. 2020;17(15):5534. doi:10.3390/ijerph17155534
14. Manas K, Dariush M, Donna S, et al. Long-chain omega-3 fatty acids, fish intake, and the risk of type 2 diabetes mellitus. Am J Clin Nutrition. 2009;90(3):613–620. doi:10.3945/ajcn.2008.27424
15. Chow CK, Jolly S, Rao-Melacini P, et al. Association of Diet, Exercise, and Smoking Modification with Risk of Early Cardiovascular Events After Acute Coronary Syndromes. Circulation. 2010;121(6):750–758. doi:10.1161/CIRCULATIONAHA.109.891523
16. Cao Y, Jarnecke M, Krause JS. Health-related behaviors and multiple chronic health conditions among persons with traumatic spinal cord injury. Spinal Cord. 2019;57(5):367–371. doi:10.1038/s41393-018-0227-3
17. Li CC. Study on the characteristics of AMI patients’ unhealthy lifestyle, TCM syndromes and their correlation with TCM syndromes. Liaoning Univ Traditional Chine Med. 2019:56.
18. Ni JJ, Cui YM, Liu LJ, et al. Study on the correlation between TCM syndromes of dyslipidemia and patients’ lifestyle. Henan Traditional Chine Med. 2009;29:866–867.
19. Si YF. Study on the correlation between sleep characteristics and TCM syndromes in patients with cognitive impairment. Beijing Univ Traditional Chine Med. 2021;4:545.
20. Wang LQ, Li JP, Dang YQ, et al. Relationship Between Social Capital and Depressive Symptoms Among Type 2 Diabetes Mellitus Patients in Northwest China: a Mediating Role of Sleep Quality. Front Psychiatry. 2021;12:725197. doi:10.3389/fpsyt.2021
21. Philippe Sionneau BF. The Treatment of Modern Western Medical Diseases with Chinese Medicine. Boulder: Blue Poppy Press; 2001.
22. Hirshkowitz M, Whiton K, Albert SM. National Sleep Foundation’s sleep time duration recommendations: methodology and results summary. Sleep Health. 2015;1(1):40–43. doi:10.1016/j.sleh.2014.12.010
23. Muthén LK, Muthén B. Mplus: Statistical Analysis with Latent Variables, User’s Guide. Los Angeles; 2007.
24. Nylund KL, Asparouhov T, Muthén BO. Deciding on the Number of Classes in Latent Class Analysis and Growth Mixture Modeling: a Monte Carlo Simulation Study. Structural Equation Modeling. A Multidisciplinary J. 2007;14:535–569.
25. Yang X, Wang Y. Correlation analysis of serum progesterone with clinical indicators and common traditional Chinese medicine syndrome types in male type 2 diabetic patients. Nan Fang Yi Ke Da Xue Xue Bao. 2019;39(5):586–590. doi:10.12122/j.issn.1673-4254.2019.05
26. Xiang XY, Ran YZ. Investigation and research on physique types and clinical syndromes of TCM in 270 patients with type 2 diabetes. World Traditional Chine Med. 2014;9:1599–1602.
27. Xu WJ, Zhang LX, Huang YH, Yang QX, Xiao FB, Zhang DQ. Discrimination of type 2 diabetes mellitus corresponding to different traditional Chinese medicine syndromes based on plasma fatty acid profiles and chemometric methods-ScienceDirect. J Ethnopharmacol. 2012;143(2):463–468. doi:10.1016/j.jep.2012.06.045
28. Si XT. Discussion on TCM Dialectical Types of Type 2 Diabetes and Related Factors. Shandong Univ Traditional Chine Med. 2017;1:65.
29. Huang MC, Guo JW, Liu YZ. Research on the mental health status and its influencing factors of the middle-aged and elderly population in rural areas. Soft Sci Health. 2012;26:445–448.
30. Chen MX, Li DT, Zhang X, et al. The relationship between the length of sleep at night and the length of noon sleep and metabolic syndrome in adults in Chengdu. Modern Preventive Med. 2019;46:1439–1442.
31. Lean MEJ, Lisa TM. Sugar and Type 2 diabetes. Br Med Bull. 2016;120(1):43–53. doi:10.1093/bmb/ldw037
32. Johnson RJ, Nakagawa T, Sanchez-Lozada LG, et al. Sugar, uric acid, and the etiology of diabetes and obesity. Diabetes. 2013;62(10):3307–3315. doi:10.2337/db12-1814
33. Wang PP, Ke CM, Yao DY, et al. A Cohort Study on Associations between Fundus/intraocular Pressure Abnormality and Medical Check-up Items. Curr Eye Res. 2021;46:704–709. doi:10.1080/02713683.2020.1826978
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.