")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
The Association Between Financial Incentives and Job Performance Among Primary Care Providers in Six Provinces of China
Authors Wang H , Zhao S , Liu Q, Wang J, Yuan B
Received 28 July 2022
Accepted for publication 2 December 2022
Published 9 December 2022 Volume 2022:15 Pages 2323—2334
DOI https://doi.org/10.2147/RMHP.S384114
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Haiyan Qu
Haipeng Wang,1,2,* Shichao Zhao,3,* Qian Liu,4 Jinyu Wang,3 Beibei Yuan5
1Centre for Health Management and Policy Research, School of Public Health, Cheeloo College of Medicine, Shandong University, Jinan, People’s Republic of China; 2NHC Key Laboratory of Health Economics and Policy Research, Shandong University, Jinan, People’s Republic of China; 3School of Public Administration, Shandong Normal University, Jinan, People’s Republic of China; 4School of Social Development and Public Policy, Beijing Normal University, Beijing, People’s Republic of China; 5China Center for Health Development Studies, Peking University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Beibei Yuan, China Center for Health Development Studies, Peking University, Box 505, 38 Xue Yuan Road, Haidian District, Beijing, 100191, People’s Republic of China, Email [email protected]
Objective: This study aims to explore the association between financial incentives and job performance of primary care providers (PCPs) from a nationally representative survey in China.
Methods: This is a cross-sectional study conducted in six provinces of China in 2019. A sample of 1388 PCPs participated in the survey was selected using a stratified cluster sampling method. A self-administered questionnaire composed of socio-demographic, work-related characteristics, financial incentives received by PCPs and their job performance was used. The association between financial incentives and job performance are analyzed using logistic regression model. The significance level for statistics is set at P < 0.05.
Results: The PCPs with higher real income level have lower contextual performance (OR = 0.67, p < 0.01) and learning performance (OR = 0.63, p < 0.01) than those with lower real income level. The PCPs with the expectation of income rising above 50% have lower contextual performance (OR = 0.66, p < 0.05) than those with the expectation of income rising above 20%. The PCPs with preference for monetary income have lower task performance (OR = 0.62, p < 0.01), contextual performance (OR = 0.55, p < 0.01) and learning performance (OR = 0.57, p < 0.01) than those without lower preference for monetary income. The percent of performance-based income has no significant effect on all the three dimensions of job performance.
Conclusion: Financial incentive was regarded as the most important motivating factor of PCPs in China, but existing financial incentives received by PCPs could not improve their job performance. The findings can be attributed to the unsatisfying total income level, “intrinsic motivation crowding out” effect, and the poorly designed performance-based salary system for PCPs. Policy attention is called for to continuing efforts and system reform to increase the total income level for PCPs in China, and improve the performance-based salary system to better motivate PCPs and improve their job performance.
Keywords: financial incentive, job performance, primary care providers, China
Introduction
The primary health-care institutions (PHCIs) provide basic public health service and basic medical health service for the residents, and constitute the essential part of China’s “Three-tiered” health-care delivery network in China.1 As direct providers of health services, the availability of productive and responsive health workforce is critical for the health system. Primary care providers (PCPs) constitute an essential part of health human resources in Chinese health-care system and should play the role of “health gatekeeper” of residents. The evidences in China confirm that the availability of enough skilled and motivated PCPs, and their better job performance, is correlated to high-quality health services and better health outcomes of residents.2
Job performance of health providers can be expressed in three aspects: task performance, contextual performance and learning performance:3 1) Task performance is defined as the effectiveness with which workers perform activities that contribute to the organization’s technical core.4 2) Contextual performance is maintaining the broader organizational, social, and psychological environment in which the technical core must function.5 3) Learning performance reflects the process of forming a plan, learning and applying new knowledge and skills in a changing organizational environment.6 Job performance is determined by the resource availability, work competence and work motivation.7 Work motivation is the degree of willingness to exert and maintain an effort towards organizational goals, which plays a crucial role in the choice and persistence of work behaviours.7,8 Without being motivated, health workers’ knowledge probably cannot result in the high-quality performance, which is so-called “know-do gap”.9,10 In fact, poor job performance due to the lack of motivation is a common challenge in low- and middle-income countries,11 which manifests as inappropriate care delivered and the poor health outcome of patients.12,13 It is found that low income, heavy workload, and limited opportunities for professional development are main demotivating factors among PCPs all over the world.14–16
Therefore, some incentive measures have been advocated and taken to improve the motivation and performance of PCPs, which can be divided into financial incentives and non-financial incentives. The classical content motivation theories, including Maslow’s hierarchy of needs theory, Alderford’s need theory and Herzberg’s two-factor theory all emphasize the importance of financial incentives to meet the basic need.17 Empirical studies proved that financial incentives as a core motivating factor could lead to improvement in job performance and health-care quality.18–20 In China, many studies have shown that the PCPs are often substantially underpaid which decreased their work passion and increased turnover intention and job burnout.1,21,22
A number of literature have found financial incentives, such as income level and non-monetary welfare, are predictors of motivation measured by job satisfaction of health workers in China.20,23 However, existing studies rarely explore the quantitative association between financial incentives and job performance. Moreover, PHCIs have experienced substantial changes in PCPs’ income system since comprehensive health system reform being launched in 2009, ie, changing to performance-based income, which implies changes in financial incentives received by PCPs and must have impact on behavior and performance of PCPs. Therefore, this study aims to examine the association between financial incentives and job performance among PCPs in China, in order to provide empirical evidence to better motivate PCPs through proper financial incentives and improve their job performance.
Methods
Study Design and Sample
This is a cross-sectional study conducted in mainland China in 2019. A stratified sampling method was applied to select PHCIs and PCPs. Firstly 6 prefectures from 6 provinces throughout the eastern, middle and western regions representing the high-, middle- and low-level economic status and different development stage of primary health system were selected. Second, we randomly selected 2 districts or counties in each sampled prefectures. Third, we randomly selected 6 community health-care centers in each sampled district and 6 township health-care centers in each sampled county. If there were no counties in certain prefecture, 12 community health-care centers were randomly selected instead. Finally, 72 PHCIs were selected, including 47 community health-care centers in the urban areas and 25 township health-care centers in the rural areas. All the PCPs in the selected PHCIs were recruited in the survey (Figure 1).
 |
Figure 1 The sample methods and compositions of the participants. |
Data Collection
The research team visited the selected primary care institutions to collect data. All PCPs on duty on the investigation day were invited to participate in the survey. Each participant completed a self-administered questionnaire independently, with research team being on site to address their questions. In total, 1430 PCPs were invited to participate in the survey. After excluding the questionnaires with missing key variables, the final sample included in the analysis was 1388 PCPs, including 397 physicians, 366 nurses, 313 public health workers (PHWs) and 312 technicians. The response rate in the survey was 97%. All participants were voluntary and their responses were anonymous. Informed consents from the PCPs were obtained in the survey. This study was approved by the Ethics Committee of Peking University Health Science Center (code of ethics: PKU201412128). This study complied with the guidelines outlined in the Declaration of Helsinki.
Theoretical Basis
The measurement of financial incentives perceived by PCPs was based on expectancy theory and equity theory. Expectancy theory hypothesizes that for the workers with preference on monetary benefits, he/she perceiving the link between financial rewards he/she will get with his/her work outputs forms his feeling of fairness and guiding his/her work behaviors. Equity theory explains that when an employee recognizes that he/she is overpaid compared to other individuals at referent firms, he/she would be motivated to increase their work effort in order to justify the over-payment.24 Therefore, in this study, we used the real income level to measure the level of financial rewards PCPs got, used the expected income level to measure the perceived over- or less-paid level of PCPs, and used the percentage of performed-based income to measure the extent of linkage between financial rewards and work outputs. As the basis of two theories is the preference of workers on monetary income, we also measured the preference for monetary income through participants ranking the all financial and non-financial motivating factors in questionnaire.
Measures and Variables
The real income level was measured in the perspective of relative level, ie, whether or not the month income of participants was higher than the average income of all investigated PCPs in their institution, and was divided into two groups (lower, higher). The expected income was measured using percentage of income rising desired by the investigated PCPs based on his/her subjective evaluation on his/her performance, and was classified into three groups (desired increase amount being ≤20% of existing level of income, 21–50%, >50%). The performance-based income was measured by the percentage of floating income amount linked to individual’s performance to his or her total income, and was categorized into three groups (≤20%, 21–50%, >50%). Preference for monetary income was assessed by whether or not the participants regarded income increasing as the most important incentive for better job performance, and was divided into two groups (no, yes).
Job performance was defined as the effectiveness of an individual in carrying out his or her roles and responsibilities related to his/her job.25,26 We assessed job performance with a multifaceted instrument developed based on the existing literature.27,28 Final measures consisted of three dimensions including 4 items measuring task performance with, 5 items measuring contextual performance with and 3 items measuring learning performance. The responses of participants were measured using a 6-point Likert scale from 1 (highly disagree) to 6 (highly agree).29,30 The Cronbach’s alphas for the three dimensions were 0.888, 0.835, and 0.893, respectively, being acceptable in reliability test. For the three dimensions, the total scores were divided into three levels of job performance, including task performance (≤16, 17–20, 21–24), contextual performance (≤20, 21–25, 26–30) and learning performance (≤12, 13–15, 16–18).
We also collected a number of covariates regarding the social-demographic and work-related characteristics of the PCPs. Social-demographic variables included gender (female, male), age in years (<30, 30–39, 40–49, ≥50), marriage status (un-married, married), education (postgraduate, bachelor, junior college, high school or below). Work-related variables included work position (physicians, nurses, PHWs, other technicians), technical title (senior/vice-senior, intermediate, primary, no title), employment mode (formal, casual), administrative post (yes, no), years of working (<5, 5–9, ≥10).
Statistical Analyses
We conducted descriptive analysis to examine individual characteristics, financial incentives, and job performance of the participants, and frequency (N) and percentage (%) statistics were calculated and presented. Chi square (χ2) tests were used to examine the association between financial incentives (real income level, percent of performance-based income, percent of income rising expectation to existing income level, and preference for monetary income) and job performance (task performance, contextual performance, learning performance). We applied multivariate logistic regression to explore the determinants of job performance, where financial incentives variables were taken as principal independent variables and individual characteristics were used as controlled variables, and job performance (task performance, contextual performance, learning performance) were dependent variables. Odds ratios (ORs) with corresponding 95% confidence intervals (CI) were presented. All the statistical analyses were conducted using STATA 15. The significance level for statistics was set at P < 0.05.
Results
Characteristics of the Participants
The characteristics of 1388 participants are presented in Table 1. Most of the participants were female (75.52%), and married (77.57%). Physicians accounted for 28.60% of the PCPs surveyed, followed by nurses (26.37%) and PHWs (22.55%). The majority were between 30 and 39 years old (45.02%) and 30.2% were under 30 years old (29.65%). Approximately 65% of them had a bachelor’s or higher degree and 58.8% held a junior technical title. Only 7.57% of the participants had senior or vice-senior technical titles, and only 18.72% had no technical titles. Nearly 40% of the investigated participants were under casual employment contract. About 11% of the surveyed PCPs had an administrative post. About 40% of the PCPs had worked for less than 5 years, while nearly 33% had worked for 5–9 years (Table 1).
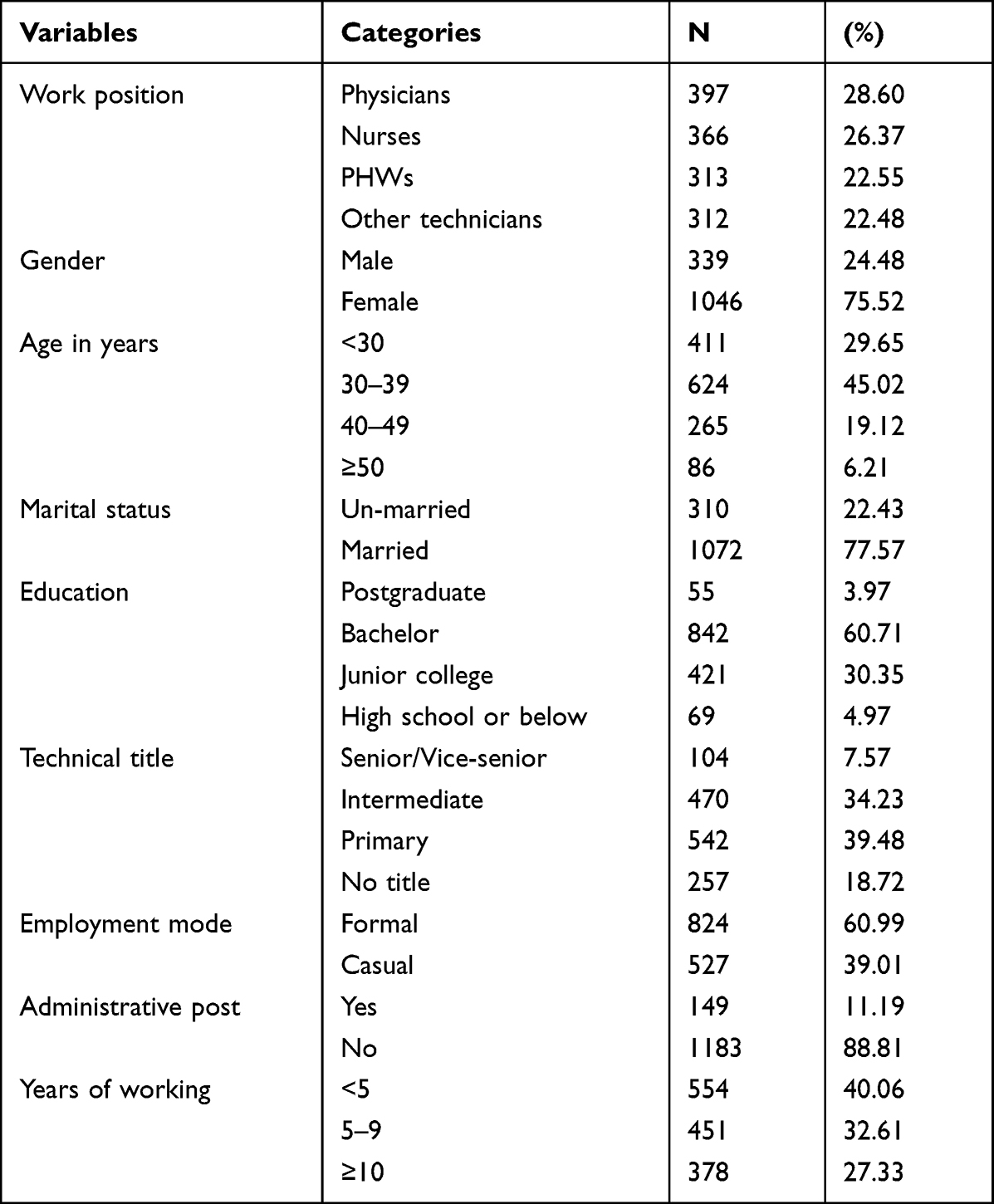 |
Table 1 Characteristics of the PCPs Participating in This Study |
Descriptive Analysis of Financial Incentives and Job Performance
In terms of real income level, compared with the average income level of one institution, 60% of the PCPs had lower income level than the average income of their institution. In terms of expectation on income rising, 46.82% of the PCPs expected that their income should rise by 20% or less considering their current job performance, and 41.98% of the PCPs thought their income should increase by 21% to 50%. In terms of percentage of performance-based income, 66.81% of the PCPs perceived the performance-based income accounting for 21% to 50% of their total income. Nearly 70% of the PCPs have rated monetary income as the most important motivating factor. As for job performance, 41.74% of the PCPs reported high task performance, while 13.04% of the PCPs had low task performance. About 38.21% of the PCPs reported high contextual performance, while 14.76% of the PCPs had low contextual performance. Approximately 34.63% of the PCPs reported high learning performance, while 24.10% of the PCPs had low learning performance (Table 2).
 |
Table 2 The Financial Incentives and Job Performance of the PCPs in China |
Association Between Financial Incentives and Job Performance
There were significant differences in task performance between the PCPs with lower and higher real income level (P = 0.007), as well as among the PCPs with different percent of performance-based income (P = 0.029). However, both the real income level and the performance-based income had no significant impact on contextual performance and learning performance (P > 0.05). There were significant differences in contextual performance (P = 0.012) and learning performance (P = 0.007) among the PCPs with different levels of income rising expectation. Nevertheless, the expectation on income rising had no significant impact on task performance (P > 0.05). There were significant differences in contextual performance (P = 0.001) and learning performance (P = 0.001) among the PCPs with or without preference for monetary income. However, whether having preference for monetary income was not associated with different levels of task performance (P > 0.05) (Table 3).
 |
Table 3 The Association Between Financial Incentives and Job Performance by Chi square Tests |
Logistic Regression Analysis on Determinants of Job Performance
Compared with the PCPs with lower real income level, the PCPs with higher real income level have lower contextual performance (OR = 0.67, p = 0.004) and learning performance (OR = 0.63, p = 0.001). The PCPs with the expectation on income rising by >50% had lower contextual performance (OR = 0.66, p = 0.036) than these with perception on income rising by ≤20%. The PCPs who had strong preference for monetary income had lower task performance (OR = 0.62 p = 0.001), lower contextual performance (OR = 0.55 p = 0.001) and lower learning performance (OR = 0.57, p = 0.001) than those without. However, percentage of performance-based income was not significantly associated with all three dimensions of job performance (p > 0.05) (Table 4).
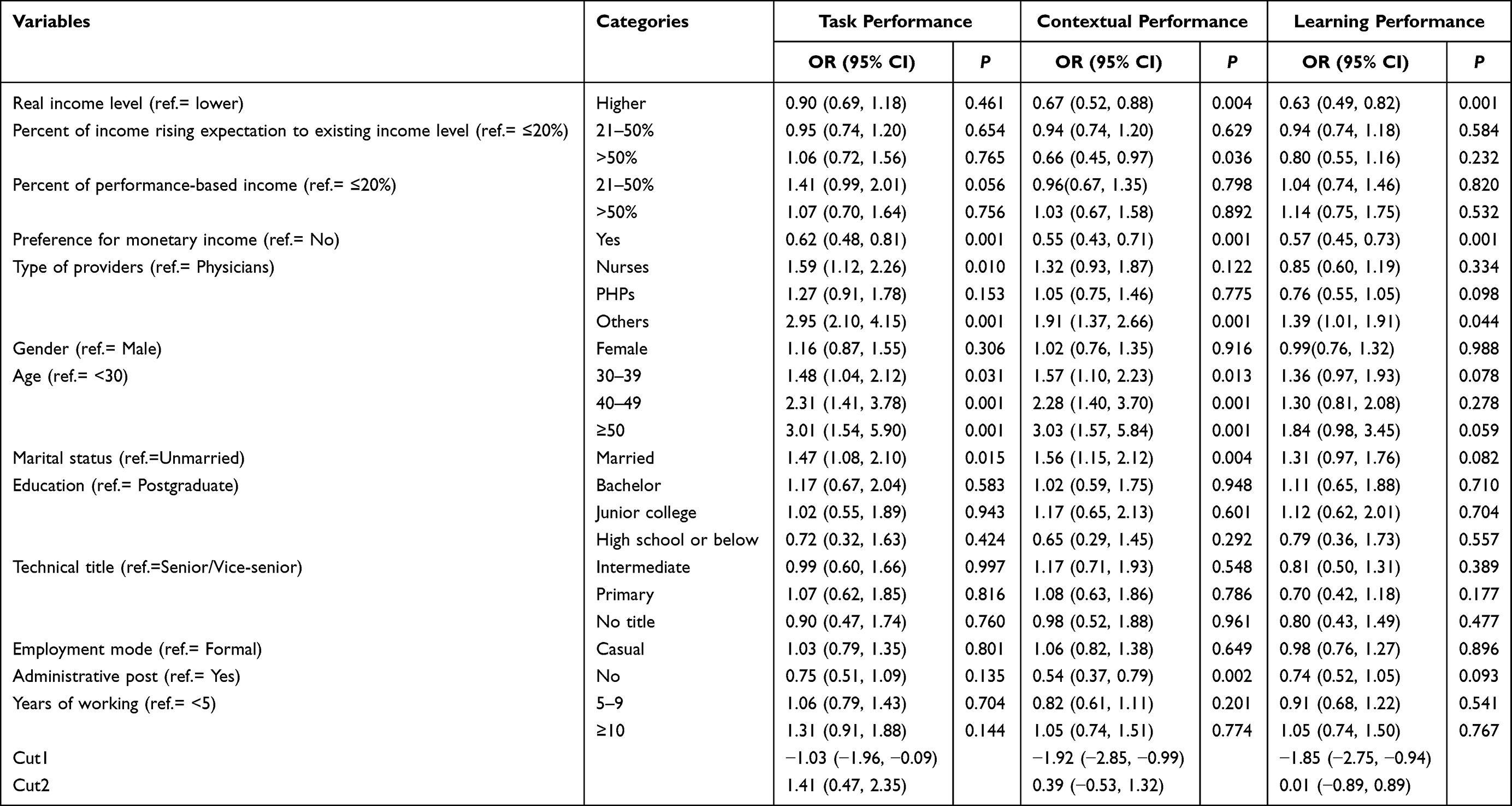 |
Table 4 The Results of Multivariate Logistic Regression Analysis on Determinants of Job Performance |
Discussion
The results of this cross-sectional study provided empirical evidences on the status of financial incentives received by PCPs in China and the associations between financial incentives and the job performance of PCPs. We measured financial incentives in multi-dimensions, including real income level, expected income level, percentage of performance-based income, and preference for monetary income. The results show that 1) The PCPs with higher real income level had lower contextual performance and learning performance. 2) The PCPs with expectation on more income rising had lower level of contextual performance. 3) The percentage of performance-based income to total income had no significant impact on the three dimensions of job performance. 4) Most of PCPs regarded monetary income as the most important motivating factor, and the strong preference for monetary income is associated to lower level of all three dimensions of job performance. 5) Real income level, expectation on income rising and performance-based income had no significant impact on task performance.
Our findings demonstrated that the PCPs with higher real income level had lower contextual performance and learning performance than those with lower income level. One possible reason is that the PCPs with higher income level are more satisfied with the current situation and lack motivation for further self-development, ie, lower learning performance. Another possible reason is the PCPs with higher income level lack intrinsic motivation according to the self-determinant theory, which explains that too much financial incentives could destroy intrinsic motivation and reduce the enjoyment of tasks in the long term.31,32 Specifically, when a task is linked with receiving monetary rewards, people infer that the task is difficult or unpleasant so that their intrinsic motivation for the rewarded activity will be crowded out by extrinsic incentive,33,34 which is referred to as “intrinsic motivation crowding out”.35
The findings suggested that the PCPs with expectation on more income rising had lower score level of contextual performance. The contextual performance means the performance related to the self-disciplined behaviors of employees to the realization of organizational goals.27 The PCPs having expectation on more income rising means that they did not perceive to be compensated equally for the work they were doing,36–38 so they may not perform certain behaviors being consistent to what their organization desired. When there is a gap between real and expected income, the PCPs may supplement their income by doing something contrary to organization goal, ie, poor contextual performance, such as engaging in other income-earning activities, informal fees from their patients, or providing unnecessary medical treatment to meet their financial expectation.39,40
It was found that the percentage of performance-based income to total income level had no significant association with the three dimensions of job performance among the PCPs, which is similar with previous study.20,41 One reason might be that the culture of the workplace PHCIs are strongly influenced by traditional Chinese culture, which is that the doctrine of the equal income distribution and preference for stability.42 Therefore, most PCPs may prefer stable income rather than higher percentage of income being floated based on their job performance. Another reason is that the performance-based salary system has not designed and developed very well. The first restriction on performance-based salary system is the low level of total income for PCPs, using some part of the limited amount of total income is difficult to motivate the PCPs by “price effect”.43 The second shortcoming is performance indicators used by current system, which is dominated by the quantity of services delivered and requirement on the process of service delivery. It was found that the performance evaluation is more used to find the faults but not support the improvement, which resulted in that current performance-based salary system could not play the incentive role in practice.22,47
It was found that nearly 70% of the PCPs regarded income as the most important motivating factor, which was consistent with previous study.44,45 The absolute income level of the PCPs is generally low especially compared with the income level of other health sectors and professionals,46,47 so earning more monetary income still being their dominant need. In addition, it is also found that the PCPs who regarded income as the most important motivating factor had lower scores on all three dimensions of job performance, which implies that income not satisfying the need of PCPs had direct destructive effect on their work performance.48,49 The studies in other developing countries also have shown that job dissatisfaction in health workers is primarily attributed to low income,50,51 which was regarded as an important predictor of job performance.
This study showed that real income level, expectation on income rising and the percentage of performance-based income had no significant impact on task performance, which can be explained by the nature of task performance and job characteristic of the PCPs. Task performance refers to basic requirement of performance in work, which fulfill the productive activities directly related to work tasks.5 Whether there are financial incentives or not, the PCPs usually have to undertake the task activities required by job demand due to pressure instead of interest.45 In addition, the job of PCPs is critical to patients’ health and life, and the feature of medical services means that the task performance of health workers is more stimulated by sense of responsibility and professional ethics rather than income.
This study provides further evidence of the need for relevant policies and targeted interventions to improve job performance of the PCPs. Firstly, the total income of PCPs should be increased to a rational level to satisfy the essential need of the PCPs, as this study shows the importance of real income level and its negative effect on job performance. Only when the level of income was satisfying, the performance-based income measures could work well.45 Comprehensive health system to strengthen PHCIs for attracting patients to primary health providers rather than hospitals is the long-term and fundamental channel to improve income level of PCPs. Secondly, performance-based salary system should be designed appropriately to promote work motivation of the PCPs. The linkage between income level and job performance should be clearly established through being transparence in performance indicators and performance target, and increase the proportion of floating income linked to performance in total income to reflect “work more, reward more”. Performance indicator and assessment process must cover both process and outcome indictors, and applied supportive evaluation but not fault-finding evaluation method. Thirdly, PHCIs managers and policy-makers should pay attention to the learning performance of the PCPs. Learning performance is the lowest among three dimensions of job performance, and it means the health workers mobilizing self-resources to learn new knowledge and skills for changing the organizational environments and achieving performance goal. Learning performance implies high level of motivation, and is hard to achieve without enough financial incentives, but the improvement in learning performance still need the supports of non-financial incentives, such as enough learning opportunity and time as well as the career promotion arrangements.
There are several limitations in this study. First, this study used cross-sectional data, which could only find the association between financial incentives and job performance among the PCPs, but cannot draw any causal inference. Second, this study is a sample survey of some provinces in China, and the six provinces covered different economic development levels and the PHCIs were in the different development stages. However, considering the rapid development of primary health systems and the diversity of primary health system reforms in different areas, the generalization and application of these conclusions should be explained combined with contexts and environments analysis. Third, the data of financial incentives and job performance are self-reported, which may have the problem of over estimation of job performance.
Conclusion
This study presents the association between financial incentives and job performance among the PCPs in China. The results imply that financial income is regarded as the most important motivation factor, but could not effectively improve the job performance of the PCPs. Those who have higher real income level show worse job performance, which may be caused by the unsatisfactory real income level and so-called “intrinsic motivation crowding out” effect. In addition, performance-based income has no significant effect on job performance because the performance-based salary system does not actually reward PCPs according to their workload and contribution in practice. Policy attention is called for to increase the level of real income and improve the performance-based salary system to motivate PCPs and promote their job performance, especially learning performance.
Abbreviations
PCPs, primary care providers; PHCIs, primary health care institutions; PHWs, public health workers; ORs, odds ratios; CI, confidence intervals.
Data Sharing Statement
The data of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Review Board of the School of Public Health, Peking University (code of ethics: PKU201412128). Informed consent was obtained from all participants in the survey.
Acknowledgments
The authors are grateful to all the individuals and organizations that participated and supported this study, and conducted the data collection.
Author Contributions
BBY designed the study and collected the data. HPW conducted data analyses and interpretation. HPW, SCZ, QL and JYW took part in the data analysis and interpretation, drafting, revising and critically reviewing the manuscript. BBY and HPW revised and edited the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by Beijing Natural Science Foundation (No. 71403008) and National Natural Science Foundation (No. 72204150).
Disclosure
The authors declare no potential conflicts of interest in this work.
References
1. Li X, Lu J, Hu S, et al. The primary health-care system in China. Lancet. 2017;390(10112):2584–2594. doi:10.1016/S0140-6736(17)33109-4
2. Wang H, Jin Y, Wang D, Zhao S, Sang X, Yuan B. Job satisfaction, burnout, and turnover intention among primary care providers in rural China: results from structural equation modeling. BMC Fam Pract. 2020;21(1):12. doi:10.1186/s12875-020-1083-8
3. Zhao S. Study on the current situation and relationship of work attitude and performance of health technical personnel in township health centers of three provinces in China PhD Thesis. Jinan: Shandong University; 2015. (in Chinese).
4. Borman WC, Motowidlo S. Expanding the criterion domain to include elements of contextual performance. In: Schmitt N, Borman WC, editors. Personnel Selection in Organizations. New York: JossyBass; 1993:71-98.
5. Borman WC, Motowidlo SJ. Task performance and contextual performance: the meaning for personnel selection research. Hum Perform. 1997;10(2):99–109. doi:10.1207/s15327043hup1002_3
6. London M, Mone EM, Scott JC. Performance management and assessment: methods for improved rater accuracy and employee goal setting. Hum Resour Manage. 2004;43(4):319–336. doi:10.1002/hrm.20027
7. Franco LM, Bennett S, Kanfer R. Health sector reform and public sector health worker motivation: a conceptual framework. Soc Sci Med. 2002;54(8):1255–1266. doi:10.1016/S0277-9536(01)00094-6
8. Alhassan RK, Spieker N, van Ostenberg P, Ogink A, Nketiah-Amponsah E, de Wit TFR. Association between health worker motivation and healthcare quality efforts in Ghana. Hum Resour Health. 2013;11(1):37. doi:10.1186/1478-4491-11-37
9. Rowe AK, de Savigny D, Lanata CF, Victora CG. How can we achieve and maintain high-quality performance of health workers in low-resource settings? Lancet. 2005;366(9490):1026–1035. doi:10.1016/S0140-6736(05)67028-6
10. Bhatnagar A, George AS. Motivating health workers up to a limit: partial effects of performance-based financing on working environments in Nigeria. Health Policy Plan. 2016;31(7):868–877. doi:10.1093/heapol/czw002
11. World Health Organization. The World Health Report 2006: Working Together for Health. World Health Organization; 2006.
12. Dieleman M, Gerretsen B, van der Wilt GJ. Human resource management interventions to improve health workers’ performance in low and middle income countries: a realist review. Health Res Policy Syst. 2009;7(1):7. doi:10.1186/1478-4505-7-7
13. Gupta J, Patwa MC, Khuu A, Creanga AA. Approaches to motivate physicians and nurses in low- and middle-income countries: a systematic literature review. Hum Resour Health. 2021;19(1):4. doi:10.1186/s12960-020-00522-7
14. Tripathy JP, Goel S, Kumar AMV. Measuring and understanding motivation among community health workers in rural health facilities in India-a mixed method study. BMC Health Serv Res. 2016;16(1):366. doi:10.1186/s12913-016-1614-0
15. Belaid L, Dagenais C, Moha M, Ridde V. Understanding the factors affecting the attraction and retention of health professionals in rural and remote areas: a mixed-method study in Niger. Hum Resour Health. 2017;15(1):60. doi:10.1186/s12960-017-0227-y
16. Ayalew F, Kibwana S, Shawula S, et al. Understanding job satisfaction and motivation among nurses in public health facilities of Ethiopia: a cross-sectional study. BMC Nurs. 2019;18(1):46. doi:10.1186/s12912-019-0373-8
17. Kanfer R, Frese M, Johnson RE. Motivation related to work: a century of progress. J Appl Psychol. 2017;102(3):338. doi:10.1037/apl0000133
18. Willis-Shattuck M, Bidwell P, Thomas S, Wyness L, Blaauw D, Ditlopo P. Motivation and retention of health workers in developing countries: a systematic review. BMC Health Serv Res. 2008;8(1):247. doi:10.1186/1472-6963-8-247
19. Lester H, Schmittdiel J, Selby J, et al. The impact of removing financial incentives from clinical quality indicators: longitudinal analysis of four Kaiser Permanente indicators. BMJ. 2010;340:c1898. doi:10.1136/bmj.c1898
20. Li H, Yuan B, Wang D, Meng Q. Motivating factors on performance of primary care workers in China: a systematic review and meta-analysis. BMJ Open. 2019;9(11):e028619. doi:10.1136/bmjopen-2018-028619
21. Wen T, Zhang Y, Wang X, Tang G. Factors influencing turnover intention among primary care doctors: a cross-sectional study in Chongqing, China. Hum Resour Health. 2018;16(1):1–11. doi:10.1186/s12960-018-0274-z
22. Zhou XD, Li L, Hesketh T. Health system reform in rural China: voices of health workers and service-users. Soc Sci Med. 2014;117:134–141. doi:10.1016/j.socscimed.2014.07.040
23. Zhang M, Yang R, Wang W, Gillespie J, Clarke S, Yan F. Job satisfaction of urban community health workers after the 2009 healthcare reform in China: a systematic review. Int J Qual Health Care. 2016;28(1):14–21. doi:10.1093/intqhc/mzv111
24. Balkin DB, Werner S. Theorizing the relationship between discretionary employee benefits and individual performance. Hum Resour Manag Rev. 2022;100901. doi:10.1016/j.hrmr.2022.100901
25. AbuAlRub RF. Job stress, job performance, and social support among hospital nurses. J Nurs Scholarsh. 2004;36(1):73–78. doi:10.1111/j.1547-5069.2004.04016.x
26. Motowidlo SJ. Job performance. Handb Psychol Ind Organ Psychol. 2003;12(4):39–53.
27. Campbell JP, McHENRY JJ, Wise LL. Modeling job performance in a population of jobs. Pers Psychol. 1990;43(2):313–575. doi:10.1111/j.1744-6570.1990.tb01561.x
28. Pulakos ED, Arad S, Donovan MA, Plamondon KE. Adaptability in the workplace: development of a taxonomy of adaptive performance. J Appl Psychol. 2000;85(4):612–624. doi:10.1037/0021-9010.85.4.612
29. Borman WC, Buck DE, Hanson MA, Motowidlo SJ, Stark S, Drasgow F. An examination of the comparative reliability, validity, and accuracy of performance ratings made using computerized adaptive rating scales. J Appl Psychol. 2001;86:965–973. doi:10.1037/0021-9010.86.5.965
30. Campbell CH, Ford P, Rumsey MG, et al. Development of multiple job performance measures in a representative sample of jobs. Pers Psychol. 1990;43(2):277–300. doi:10.1111/j.1744-6570.1990.tb01559.x
31. Gillam SJ, Siriwardena AN, Steel N. Pay-for-performance in the United Kingdom: impact of the quality and outcomes framework—a systematic review. Ann Fam Med. 2012;10(5):461–468. doi:10.1370/afm.1377
32. Deci EL, Olafsen AH, Ryan RM. Self-determination theory in Work Organizations: the State of a science. Annu Rev Organ Psychol Organ Behav. 2017;4(1):19–43. doi:10.1146/annurev-orgpsych-032516-113108
33. Mehrotra A, Sorbero MES, Damberg CL. Using the lessons of behavioral economics to design more effective pay-for-performance programs. Am J Manag Care. 2010;16(7):497–503.
34. Flannery M. Self-determination theory: intrinsic motivation and behavioral change. Oncol Nurs Fórum. 2017;44. doi:10.1188/17.ONF.155-156
35. Frey BS, Jegen R. Motivation crowding theory. J Econ Surv. 2001;15(5):589–611. doi:10.1111/1467-6419.00150
36. Kalk A, Paul FA, Grabosch E. ‘Paying for performance’ in Rwanda: does it pay off? Trop Med Int Health. 2010;15(2):182–190. doi:10.1111/j.1365-3156.2009.02430.x
37. Chimhutu V, Songstad NG, Tjomsland M, Mrisho M, Moland KM. The inescapable question of fairness in Pay-for-performance bonus distribution: a qualitative study of health workers’ experiences in Tanzania. Glob Health. 2016;12(1):77. doi:10.1186/s12992-016-0213-5
38. Zitti T, Gautier L, Coulibaly A, Ridde V. Stakeholder perceptions and context of the implementation of performance-based financing in District Hospitals in Mali. Int J Health Policy Manag. 2019;8(10):583–592. doi:10.15171/ijhpm.2019.45
39. Roenen C, Ferrinho P, Van Dormael M, Conceição MC, Van Lerberghe W. How African doctors make ends meet: an exploration. Trop Med Int Health. 1997;2(2):127–135. doi:10.1046/j.1365-3156.1997.d01-240.x
40. McCoy D, Bennett S, Witter S, et al. Salaries and incomes of health workers in sub-Saharan Africa. Lancet. 2008;371(9613):675–681. doi:10.1016/S0140-6736(08)60306-2
41. Li J, Hurley J, DeCicca P, Buckley G. Physician response to pay-for-performance: evidence from a natural experiment. Health Econ. 2014;23(8):962–978. doi:10.1002/hec.2971
42. Yuan B, Yu Y, Zhang H, Li H, Kong C, Zhang W. Satisfaction of township hospitals health workers on how they are paid in China. Int J Environ Res Public Health. 2021;18(22):11978. doi:10.3390/ijerph182211978
43. Ma X, Wang H, Yang L, Shi L, Liu X. Realigning the incentive system for China’s primary healthcare providers. BMJ. 2019;365:l2406. doi:10.1136/bmj.l2406
44. Yu C, Li X, Liang H, Zhang Z, Fang D. The effects of monetary incentives on physicians’ effort and patient satisfaction: understanding the links between monetary incentives and physicians’ effort. Int J Environ Res Public Health. 2022;19(20):13075. doi:10.3390/ijerph192013075
45. Chandler CIR, Chonya S, Mtei F, Reyburn H, Whitty CJM. Motivation, money and respect: a mixed-method study of Tanzanian non-physician clinicians. Soc Sci Med. 2009;68(11):2078–2088. doi:10.1016/j.socscimed.2009.03.007
46. Soler JK, Yaman H, Esteva M, et al. Burnout in European family doctors: the EGPRN study. Fam Pract. 2008;25(4):245–265. doi:10.1093/fampra/cmn038
47. Ran LM, Luo KJ, Wu YC, Yao L, Feng YM. An analysis of China’s physician salary payment system. J Huazhong Univ Sci Technolog Med Sci. 2013;33(2):309–314. doi:10.1007/s11596-013-1116-9
48. Li H, Kong P, Yu H, Zhao S, Yuan J, Meng Q.Incentive factors influencing work behavior of primary care providers in China. Chin J Health Policy. 2012;5(3):6–11.
49. Xu W, Pan Z, Li Z, Lu S, Zhang L. Job burnout among primary healthcare workers in rural china: a multilevel analysis. Int J Environ Res Public Health. 2020;17(3):727. doi:10.3390/ijerph17030727
50. Dieleman M, Cuong PV, Anh LV, Martineau T. Identifying factors for job motivation of rural health workers in North Viet Nam. Hum Resour Health. 2003;1(1):10. doi:10.1186/1478-4491-1-10
51. Stilwell B, Diallo K, Zurn P, Vujicic M, Adams O, Poz MD. Migration of health-care workers from developing countries: strategic approaches to its management. Bull World Health Organ. 2004;6:595–600.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.