Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Association Between Domestic Violence and Adverse Pregnancy Outcomes in Pregnant Women Seeking Antenatal Care at Public Hospitals in Gedeo Zone: A Prospective Cohort Study
Authors Melaku G ![]() , Belay Getahun S
, Belay Getahun S ![]() , Abebe M
, Abebe M ![]() , Shumye S
, Shumye S ![]() , Semagn S
, Semagn S
Received 18 May 2023
Accepted for publication 23 June 2023
Published 29 June 2023 Volume 2023:16 Pages 1833—1843
DOI https://doi.org/10.2147/JMDH.S419473
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Getnet Melaku,1,* Senait Belay Getahun,1,* Mesfin Abebe,1,* Seid Shumye,2,* Selamawit Semagn3,*
1Department of Midwifery, College of Medicine and Health Sciences, Dilla University, Dilla, Ethiopia; 2Department of Psychiatry, College of Medicine and Health Sciences, Dilla University, Dilla, Ethiopia; 3Department of Public Health, College of Medicine and Health Sciences, Dilla University, Dilla, Ethiopia
*These authors contributed equally to this work
Correspondence: Getnet Melaku Ayele, Department of Midwifery, College of Medicine and Health Sciences, Dilla University, Po. Box: 419, Dilla, Ethiopia, Tel +251912711797, Email [email protected]
Background: Domestic violence is any harmful behavior by an intimate partner, such as physical, sexual, or psychological abuse. In Ethiopia, domestic violence is a serious and widespread problem. It affects two-thirds (64.6%) of pregnant women and increases the risk of maternal and perinatal morbidity and mortality. Domestic violence during pregnancy is a growing public health problem that may contribute to maternal and perinatal mortality, especially in low- and middle-income countries. This study aims to assess the association between domestic violence during pregnancy and the risk of adverse pregnancy outcomes in Gedeo Zone Public Hospitals, Southern Ethiopia.
Material and Methods: We conducted a prospective cohort study on 142 pregnant women in their third trimester who attended public health institutions in Gedeo Zone for antenatal care. We compared 47 women who were exposed to domestic violence with 95 who were not and followed them until 24 hours after delivery or drop-out. We used SPSS version-24 to analyze data and logistic regression to examine the association between domestic violence and pregnancy outcomes. We reported the results using an adjusted odds ratio with 95% confidence interval and P-value.
Results: Out of 142 women, who completed the follow-up, 47 were exposed to domestic violence and 95 were not. We found a strong link between domestic violence and preterm birth. Women exposed to domestic violence had a four-fold higher risk of preterm birth (AOR= 4.392, 95% CI: 1.117, 6.588) than those who were not. They also had a 2.5-fold higher risk of perinatal death (AOR= 2.562, 95% CI: 1.041, 6.308).
Conclusion: Domestic violence during pregnancy affects many pregnant women in southern Ethiopia and harms their babies. It leads to preterm birth and perinatal death, which can be prevented. The Ethiopian government and other stakeholders need to protect pregnant women from intimate partner violence urgently.
Keywords: domestic violence, pregnant women, preterm birth, perinatal death, prospective cohort
Introduction
Domestic violence (DV) is a grave violation of human rights and a major public health issue that affects millions of women around the world which occurs when an intimate partner inflicts physical, sexual, or psychological harm on their partner, through acts such as hitting, forcing sex, insulting, or controlling.1–4 It can have devastating consequences for women’s health and well-being, especially during pregnancy in which pregnant women who experience DV face a higher risk of adverse pregnancy outcomes, such as preterm birth, low birth weight, pregnancy loss, bleeding, infection, abdominal injury, fetal injury, and death.5–7 DV can also affect the mental health of pregnant women, leading to depression, anxiety, post-traumatic stress disorder (PTSD), suicidal thoughts, and other psychological problems.8–10
The prevalence of DV during pregnancy varies widely across countries and regions. According to the World Health Organization (WHO) and other studies, about 30% of women globally have experienced physical and/or sexual intimate partner violence (IPV) in their lifetime, and 29% have experienced IPV during their lifetime. However, in some settings, the prevalence of DV during pregnancy can be much higher.11–13 Moreover, DV during pregnancy can be more prevalent in some settings, posing a serious threat to the health and well-being of both the mother and the baby in low- and middle-income countries.14–16
According to a report by the National Partnership for Women & Families, domestic violence during pregnancy can lead to low birth weight, perinatal death, maternal injury, and other complications, such as high-blood pressure, bleeding, and preterm birth.17–19 In Ethiopia, two-thirds (64.6%) of pregnant women reported experiencing DV during their current pregnancy, with physical violence being the most common form (44.1%), followed by psychological (39.1%) and sexual (23.7%) violence.20–22
Ethiopia is also a low-income country with high maternal and perinatal mortality rates. According to the Ethiopian Demographic and Health Survey (EDHS) report from 2016, the maternal mortality ratio was 412 deaths per 100,000 live births, and the perinatal mortality rate was 46 deaths per 1000 pregnancies level.23,24 These rates indicate a great need for further efforts to reduce maternal and perinatal deaths and improve maternal and child health in which one of the potential factors that could contribute to these high mortality rates is DV during pregnancy.23,24 Thus, it is crucial that healthcare professionals provide support and care to women who experience domestic violence during pregnancy.3,25
Nevertheless, there is limited evidence on the causal relationship between DV during pregnancy and adverse pregnancy outcomes in Ethiopia and there are no cohort studies conducted in the study area where a high prevalence of DV during pregnancy is suspected.24,26,27 Due to recent attempts to reduce adverse pregnancy outcomes in Ethiopia, we believe that there is some available information about domestic violence as the root cause.24 Additionally, the low level of attention given by medical professionals for pregnant mothers who complain of their pregnancy and subsequent social implications of domestic violence has drawn attention to the issue.24,28,29
The study’s output will help the government know domestic violence and its association with adverse pregnancy outcomes to enhance their attempt to address Sustainable Development Goals (SDG-16) aiming to significantly reduce all forms of violence and related death rates everywhere by 2030. It will also help health professionals focus on the root causes of adverse pregnancy outcomes and intervene accordingly.28–30 Community health workers can create awareness on the impact of domestic violence on pregnancy outcomes and, researchers can use this study as a baseline.
Therefore, despite other causes contributing to maternal and perinatal mortality, domestic violence against pregnant women is an increasing public health concern particularly in low- and middle-income countries. The purpose of this study is to measure the association between domestic violence during pregnancy and the risk of adverse pregnancy outcomes in Gedeo Zone Public Hospitals, Southern Ethiopia.
Materials and Methods
The Aim, Design and Setting of the Study
A facility-based prospective cohort study was conducted in Gedeo Zone public hospitals of SNNPR, Ethiopia from May 2022 to July 2022 to investigate the relationship between domestic violence and adverse pregnancy outcomes.
Population
The source population for the study was all pregnant women inhabitants living in Gedeo Zone. The study included pregnant women who were in their third trimester and attending selected public health institutions for antenatal care follow-up. The study included pregnant women with a gestational age below 28 weeks. Women with multiple pregnancies, those who planned to deliver outside the selected public health institutions in the Gedeo Zone, and women with known medical diseases were excluded from the study.
Starting and End Points of Follow Up
The study recruited both pregnant women exposed to domestic violence and unexposed who were before 28 weeks of gestation during their ANC visit. Follow-up started at 28 weeks (3rd trimester) of pregnancy and continued until 24 hours after delivery or drop-out. The duration of the follow-up period for a subject was a maximum of 14 weeks (from 28 weeks onward).
Sample Size, Methods, and Procedure
The sample size was calculated using two sample proportion formulas in Epi-Info version-7 for windows. Calculation assumed that type I error of 5%, power of 80% and two exposed to one non-exposed in which the sample size proportion of adverse pregnancy outcome in the non-exposed cohort (10.2%) and in the exposed cohort (29.7%) had taken from retrospective cohort study done in Ghana.31,32 The minimum sample size was 138 (46 exposed and 92 non-exposed) and adding 10% drop-out rate, the final sample size was 152 (51 exposed and 101 non-exposed). (Let P= p1+ rp2/1+r and r=n2/n1; Where; P1=proportion of adverse pregnancy outcome among exposed P2=proportion of adverse pregnancy outcome among non-exposed, α=level of significance, Zα/2=1.96 at 95% CL, Power=80%=1-β, Zβ=1.28, n=the minimum required sample size in each group).
The study used a systematic random sampling technique to select samples for the study. Study subjects were identified based on the annual eligibility plan of deliveries in each hospital of Gedeo Zone health office. The total sample size was met by proportionally allocated samples from each hospital. Systematic random sampling technique was employed to get all cohorts.
The data was collected from study subjects using a pre-tested, interview-guided structured questionnaire which was adopted from the Swahili version of the “WHO Multi-Country Study on Women Health and Domestic Violence against Women” tool that had been validated in the Amhara region of Ethiopia.28,33 The questionnaire was developed in English and translated into Gedeofa and/or Amharic, then back to English to check for its consistency.
Socio-demographic data, causes of violence against pregnant women, and health facility factors leading to adverse pregnancy outcomes were collected at the time of recruitment. During a follow-up interview at 34 weeks’ gestation, the women’s exposure to emotional, sexual, and physical violence was determined. Within 24 hours after delivery, documentation of gestational age and measurement of birth weight was done. The duration of the first and second interviews was 30 to 45 minutes; the post-delivery interview lasted for 10 to 15 minutes. Women who delivered before 34 weeks of gestation were considered dropouts.
The study recruited 152 pregnant women (51 exposed and 101 non-exposed) who attended antenatal care, met the inclusion criteria, and agreed to participate. They were interviewed near the Antenatal Clinic at the time of recruitment and at the end of the day. Out of these, 142 pregnant women (47 exposed and 95 non-exposed) completed their follow-up and were interviewed again. A gestational age assessment was done using the last normal menstrual period (LMP) and/or date of fetal quickening for gestational age below 14 weeks and head circumference (HC) for gestational age 14–28 weeks for women having unknown LMP or ambiguous date of fetal quickening. Each participant was allocated a unique identification number. Information on socio-demographics, causes of violence against pregnant women, and health facility factors leading to adverse pregnancy outcomes were obtained through a face-to-face interview questionnaire.
Data Collection Method
The study data was collected using a pre-tested interview guided structured questionnaire that had five main parts: socio-demographic, psychological (emotional), physical and sexual violence, Household Conditions, others, and adverse pregnancy outcomes.
Data Quality Assurance
To ensure data quality, a professionally designed data collection tool was prepared, and data collectors were trained. Supervisors examined some of the collected data each day and provided immediate solutions for any problems. Before actual data collection, the questionnaire was tested on 5% of the total sample size (8 pregnant women) at Hawassa Adare Hospital to check the context of data. A minimum of 1 week recruitment and 4 weeks follow-up period were needed to perform the pre-test. After the pre-test was done, the questionnaire was revised accordingly.
Data Processing and Analysis
The collected data were checked for completeness, cleaned, processed, and entered EPI-info version-7 and then transported to SPSS version-24 computer software for analysis. Frequency distribution tables and statistical graphs were used to describe variables. Cross-tabulation and logistic regression were done to examine the association between dependent and independent variables. Variables with a p-value of less than 0.2 were entered into multivariable analysis and adjusted odds ratio (AOR) was seen to control confounding variables. A 95% confidence level and p-value of less than 0.05 were considered statistically significant.
Result
Socio-Demographic, Social Habits, and Reproductive Health Characteristics
In this study, 152 pregnant women at 28 weeks of gestational age were recruited and followed for approximately 14 weeks. Of these women, 51 were exposed and 101 were not exposed to the exposure variable (domestic violence). However, only 142 women (47 exposed and 95 non-exposed) completed the follow-up, resulting in a response rate of 93.4%. The mean age of pregnant mothers included in the study during their last birth was 25.04 (±SD=5.113) years. Most cohorts experienced less than three pregnancies, with 83 (58.5%) of non-exposed and 37 (26.1%) of exposed women falling into this category. In terms of educational status, 77 (54.2%) and 81 (57.0%) of non-exposed women and 42 (29.6%) and 42 (29.6%) of exposed women were literate, respectively.
The study assessed the employment and income status of the woman and her partner, as well as the drinking and chewing habits and frequency of her partner, and the history of extramarital relationships of both parties. Seventy-one (50.0%) of women who were not exposed to domestic violence and 39 (27.5%) of those who were exposed were unemployed. Additionally, more than 32 (22.5%) women who were not exposed and 12 (8.5%) who were exposed had no income per month (Table 1).
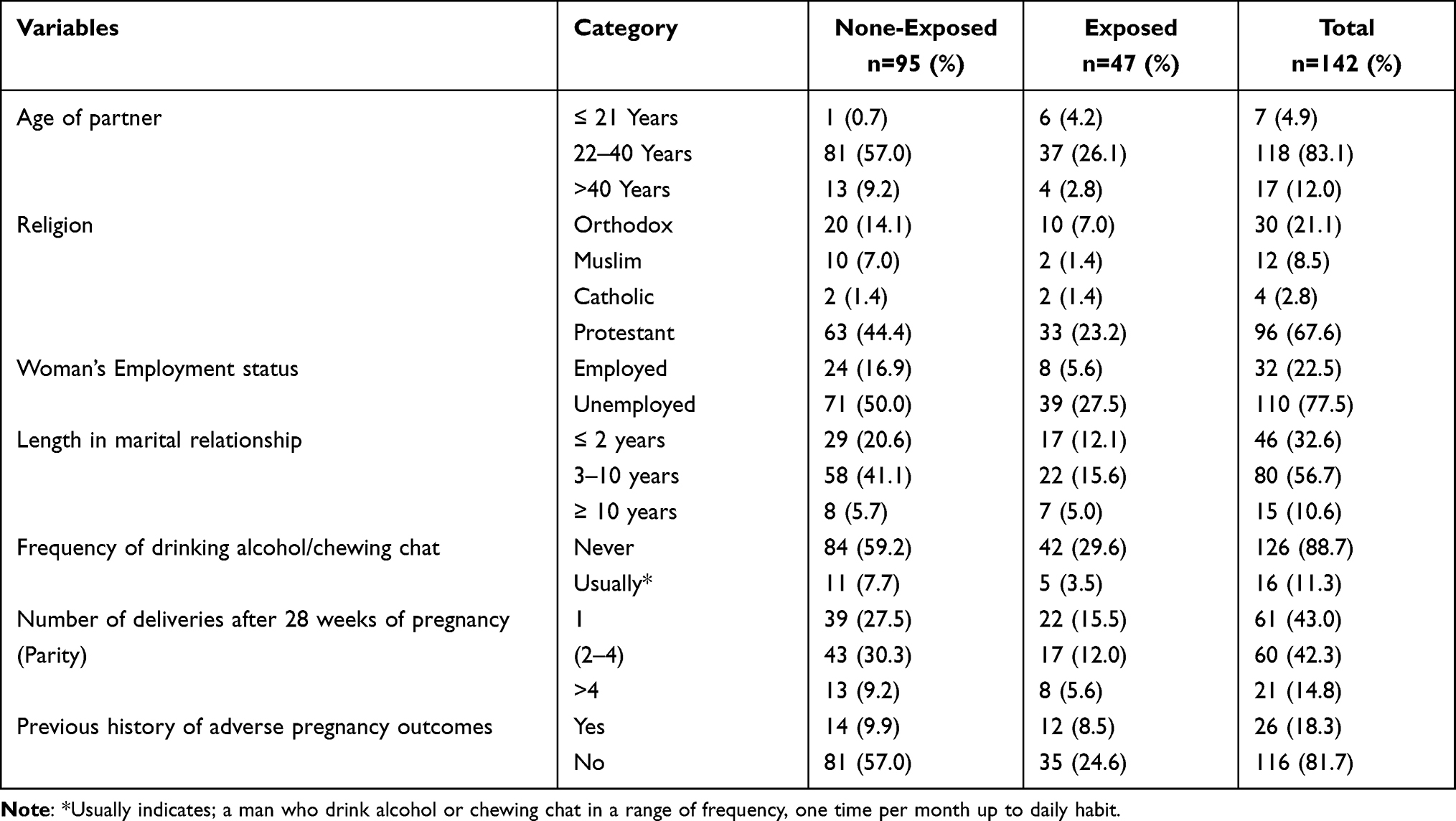 |
Table 1 Socio-Demographic, Social Habits and Reproductive Health Characteristics of Pregnant Women Attending at Gedeo Zone Public Hospitals, Southern, Ethiopia 2022 (n=142) |
The study also examined the adverse pregnancy outcomes that the pregnant women had experienced before. Out of the 26 women who had a history of such outcomes, bleeding during pregnancy was the most common among the non-exposed group (19.20%), while perinatal death was the most common among the exposed group (19.20%) (Figure 1).
 |
Figure 1 Types of adverse pregnancy outcomes that previously faced among women attending at Gedeo Zone Public Hospitals, Southern, Ethiopia 2022 (n=142); **Adverse pregnancy outcomes like breathing difficulty (asphyxia), fetal and maternal infection, and preterm birth. |
Magnitude of Domestic Violence
The study scrutinized different variables to identify types of domestic violence. Among the 47 pregnant mothers who completed their follow-up as an exposed group (exposed to domestic violence), about 23.2% experienced psychological violence, which was the most common type (Figure 2).
 |
Figure 2 Types of domestic violence that pregnant women experienced among women attending at Gedeo Zone Public Hospitals, Southern, Ethiopia 2022 (n=142). |
Household Condition and Perception Related Factors
At the time of recruitment, household ownership was assessed as a baseline data in which 27.4% of non-exposed and 40.4% of exposed groups had rented houses. On the other hand, about 56.8% of non-exposed and 66.0% of exposed groups were living with more than three individuals in their household. Regarding desire of the current pregnancy, 86.2% of non-exposed and 61.7% of exposed group were having their current pregnancy based on their desire (Table 2).
 |
Table 2 Household Condition and Perception Related Factors of Domestic Violence Among Pregnant Women Attending at Gedeo Zone Public Hospitals, Southern, Ethiopia 2022 (n=142) |
Adverse Pregnancy Outcome Related Variables
The gestational age during delivery of the current pregnancy was analyzed. Ninety-three (97.9%) of the non-exposed group and thirty-seven (28.5%) of the exposed group were delivered at term (after 37 weeks) of gestational age. Even though 78 (82.1%) mothers from the non-exposed group and 25 (53.2%) from the exposed group delivered normal-weight babies, 17 (17.9%) from the non-exposed group and 22 (46.8%) from the exposed group delivered low birth weight babies with a birth weight ≤2500 grams.
Out of all the women in the study, 8.4% of the non-exposed group and 21.3% of the exposed group experienced bleeding during late pregnancy. Regarding complications faced during and/or after pregnancy, 18.9% of the non-exposed women and 46.8% of the exposed group experienced perinatal death (Table 3).
 |
Table 3 Adverse Pregnancy Outcomes Due to Domestic Violence Among Pregnant Women Attending at Gedeo Zone Public Hospitals, Southern, Ethiopia 2022 (n=142) |
Associated Factors Between Any Domestic Violence and Preterm Birth, Low Birth Weight, Late Trimester Bleeding and Perinatal Death
The study examined the association between birth status in terms of gestational age, birth weight of the newborn, Late Trimester Bleeding, and perinatal death with domestic violence. The results showed that preterm birth and perinatal death had a statistically significant association with domestic violence. However, according to the study, neither low birth weight nor late trimester bleeding had any significant association with domestic violence. We found a statistically significant association between domestic violence and birth status in terms of gestational age. Thus, preterm birth is more than four times (AOR= 4.392, 95% CI: 1.117, 6.588) more likely to occur among pregnant women exposed to domestic violence. However, after adjustment of the stratified analysis (AOR), low birth weight and late trimester bleeding had no statistically significant association with domestic violence during pregnancy. In this study, the occurrence of perinatal death was found to have a significant association among women exposed to domestic violence. Women exposed to domestic violence were 2.5 times (AOR= 2.562, 95% CI: 1.041, 6.308) more likely to face perinatal death when compared with those who were unexposed to DV (Table 4).
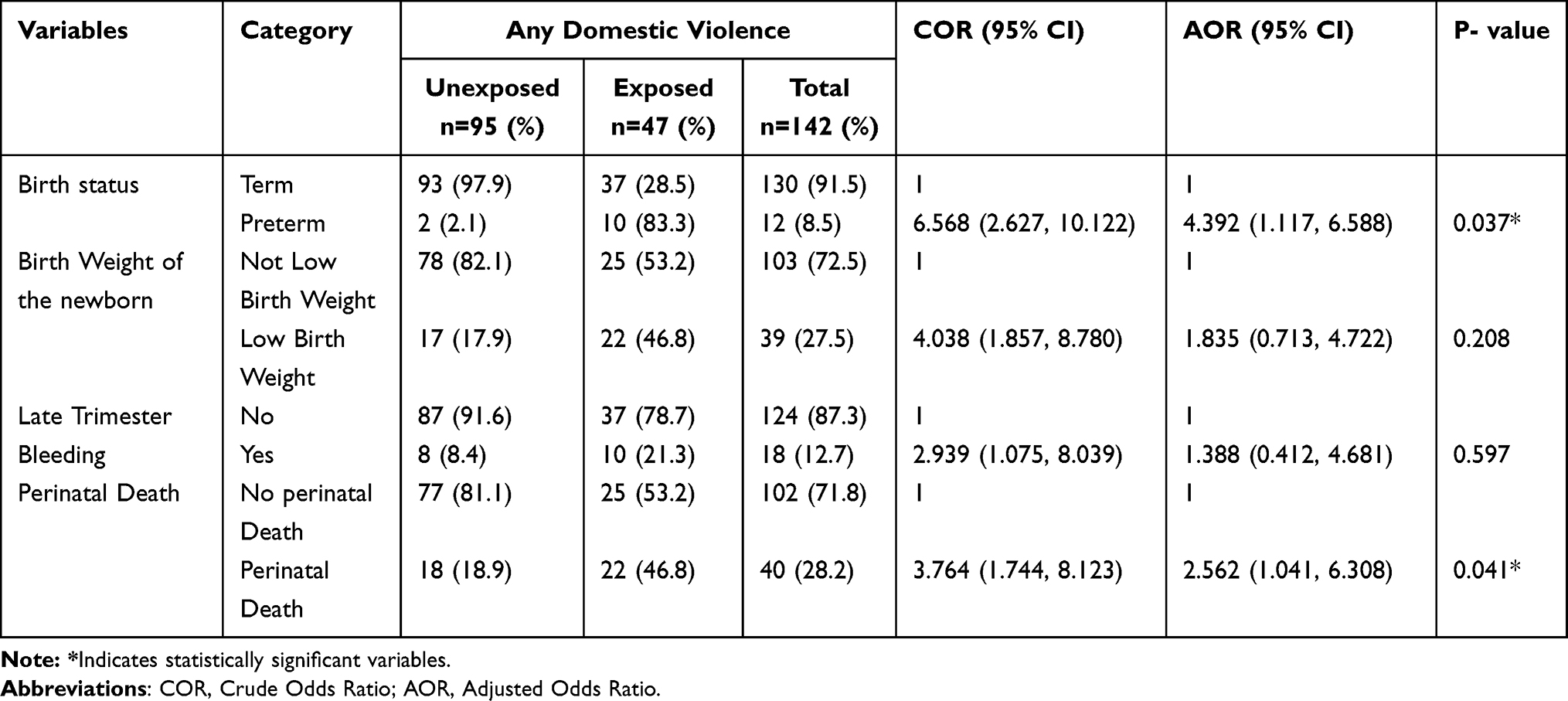 |
Table 4 Bivariate and Multivariable Analysis to Show the Associated Factors Between Any Domestic Violence and Adverse Pregnancy Outcomes Among Pregnant Women Attending at Gedeo Zone Public Hospitals, Southern, Ethiopia 2022 (n=142) |
Discussion
This study examined how domestic violence affects pregnancy outcomes among women who visited public health institutions. Pregnant women who were exposed or unexposed to domestic violence before 28 weeks of gestation were enrolled and followed up from their third trimester (28 weeks) until 24 hours after delivery or drop out. Our study found that psychological violence was the most prevalent form of domestic violence among pregnant women, affecting 23.2% of those who were exposed. This finding is consistent with studies from Brazil and Southeast Ethiopia.26,34 This finding is higher than those of other studies from India and Ethiopia.5,26,35–37 This might be because we only included pregnant women who visited healthcare institutions for any reason and followed them up during the data collection period, which could have increased the result.
Thus, this study found that the overall prevalence of domestic violence was 33.1%. This study is in line with studies done in Turkey, Brazil, and a meta-analysis review. Nevertheless, it is lower than studies conducted in Iran, Portugal and Southeast Oromia, Ethiopia. This may be due to the fact that the studies were conducted in large community-based surveys which could reveal the large prevalence of domestic violence.38,39 Domestic violence shortens the duration of pregnancy and increases the risk of preterm birth. Women who suffer from domestic violence have a fourfold higher chance (AOR= 4.392, 95% CI: 1.117, 6.588) of delivering too early. This result is consistent with several studies from both developed and developing countries.10,17
Our study did not find a significant link between domestic violence during pregnancy and low birth weight which agrees with a study from Nepal.40 Contrary to this result, a study from the Center on Trauma and Adversity at Case Western Reserve University, a systematic review and meta-analysis, a study done on Asian Immigrants, and studies from Northwest Ethiopia all reported different findings.19,41–44 A probable reason for this difference is that our sample size was too small, and we had a selection bias during the recruitment phase of our study. We also did not find a significant link between domestic violence and bleeding in the late trimester, unlike some studies from Canada and Bangladesh.45,46 This may be because we only included pregnant women and not their husbands and had different population characteristics.
This study revealed a significant link between domestic violence exposure and perinatal death. Women who were exposed to DV had a 2.5 times higher risk (AOR= 2.562, 95% CI: 1.041, 6.308) of losing their babies than women who were not exposed to DV. This finding is consistent with studies from Nepal and Bangladesh.18,40 An explanation for this is that domestic violence can cause physical and psychological stress, infections, injuries, and complications that can affect the health of the mother and the baby.
Conclusion
This prospective cohort study reveals the alarming prevalence and consequences of domestic violence against pregnant women in southern Ethiopia. Domestic violence during pregnancy not only harms the mothers, but also puts their babies at risk of preterm birth and perinatal death. These outcomes are unacceptable and preventable. The Ethiopian government and other stakeholders must act urgently to protect pregnant women from intimate partner violence. Moreover, to enhance the health care systems’ response to domestic violence in developing countries, we need more evidence-based knowledge on its effects on pregnant women, more training and support for ANC staff to deal with domestic violence, and more effective interventions to address this issue.
Abbreviations
ANC, Antenatal Care; AOR, Adjusted Odds Ratio; CL, Confidence Level; DV, Domestic Violence; EDHS, Ethiopian Demographic and Health Survey; HC, Head Circumference; IPV, Intimate Partner Violence; IRB, Institutional Review Board; LMP, Last normal menstrual period; SDG, Sustainable Development Goals; SGA, Small for Gestational Age; SNNPR, South Nation Nationalities Peoples Region; WHO, World Health Organization.
Data Sharing Statement
The corresponding author will provide the data that supports this study upon reasonable request. The data are not publicly accessible for ethical and privacy reasons. The data consists of anonymized demographic and clinical data of the participants and questionnaires. The data will remain available for 10 years after this paper is published. Please contact Getnet Melaku Ayele at [email protected] or [email protected] to request data access.
Ethics Approval and Consent to Participate
As recommended by the Declaration of Helsinki, the likelihood of benefits from the current research was considered. Research on domestic violence during pregnancy and adverse pregnancy outcomes raises important ethical and methodological challenges in addition to those raised by any other type of research on human subjects. Therefore, this study was conducted in accordance with the WHO’s ethical and safety recommendations for research on domestic violence and pregnancy outcomes. Ethical approval was provided by the Institutional Review Board (IRB) of Dilla University, College of Medicine, and Health Sciences (protocol unique number 015/18-06) and an official support letter was written to Gedeo Zone Health Office. Then, an official letter was obtained from Gedeo Zone Health Office to each hospital. In addition, informed written consent was obtained from pregnant mothers who were selected for the study. The study participants’ right to withdraw from the study at any time during data collection was assured.
Acknowledgments
We thank the Gedeo Zone health department for their cooperation and permission to conduct this study in the area. We also thank the personnel of Gedeo Zone hospitals and the pregnant women who participated in this study for their valuable contributions. Furthermore, we are grateful to Dilla University for giving us this opportunity and providing us with financial support, data collectors and supervisors for their role in recruitment, follow-up and data collection and the anonymous reviewers for their constructive comments and suggestions that improved the quality of the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received funding from Dilla University Research and Dissemination Office. The sponsor participated in the study conception, design, data collection and interpretation, and gave permission for publication. Even though, the funding source had a role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript, the authors have full control of all primary data and agree to allow the journal to review their data if requested.
Disclosure
The authors declare they have no conflicts of interest in this work.
References
1. Nicolaidis C, Paranjape A. Defining intimate partner violence: controversies and implications. Intimate Partner Violence. Oxford University Press; 2009:19–29.
2. Flury M, Nyberg E, Riecher-Rössler A. Domestic violence against women: definitions, epidemiology, risk factors and consequences. Review article. Swiss Med Wkly. 2010;140(3536):w13099. doi:10.4414/smw.2010.13099
3. Levy BS, Patz JA. Climate change, human rights, and social justice. Review article. Ann Global Health. 2015;81(3):310–322. doi:10.1016/j.aogh.2015.08.008
4. García-Moreno C, Stöckl H. Protection of sexual and reproductive health rights: addressing violence against women. Int J Gynecol Obstetr. 2009;106(2):144–147. doi:10.1016/j.ijgo.2009.03.053
5. James L, Brody D, Hamilton Z. Risk factors for domestic violence during pregnancy: a meta-analytic review. Violence Vict. 2013;28(3):359–380. doi:10.1891/0886-6708.VV-D-12-00034
6. Jahanfar S, Howard LM, Medley N. Interventions for preventing or reducing domestic violence against pregnant women. Cochrane Database Syst Rev. 2014;(11). doi:10.1002/14651858.CD009414.pub3
7. Lannert BK, Garcia AM, Smagur KE, et al. Relational trauma in the context of intimate partner violence. Child Abuse Negl. 2014;38(12):1966–1975. doi:10.1016/j.chiabu.2014.10.002
8. Campo M. Domestic and Family Violence in Pregnancy and Early Parenthood. Australian Institute of Family Studies; 2015.
9. Rayment-Jones H, Harris J, Harden A, et al. Project20: interpreter services for pregnant women with social risk factors in England: what works, for whom, in what circumstances, and how? Int J Equity Health. 2021;20(1):1. doi:10.1186/s12939-021-01570-8
10. Rao D, Kumar S, Mohanraj R, et al. The impact of domestic violence and depressive symptoms on preterm birth in South India. Soc Psychiatry Psychiatr Epidemiol. 2016;51(2):225–232. doi:10.1007/s00127-015-1167-2
11. Krahé B. Violence against women. Curr Opinion Psychol. 2018;19:6–10. doi:10.1016/j.copsyc.2017.03.017
12. Sardinha L, Maheu-Giroux M, Stöckl H, Meyer SR, García-Moreno C. Global, regional, and national prevalence estimates of physical or sexual, or both, intimate partner violence against women in 2018. Lancet. 2022;399(10327):803–813. doi:10.1016/S0140-6736(21)02664-7
13. Kapiga S, Harvey S, Muhammad AK, et al. Prevalence of intimate partner violence and abuse and associated factors among women enrolled into a cluster randomized trial in northwestern Tanzania. BMC Public Health. 2017;17(1):1–11. doi:10.1186/s12889-017-4119-9
14. Alhusen JL, Ray E, Sharps P, Bullock L. Intimate partner violence during pregnancy: maternal and neonatal outcomes. J Women’s Health. 2015;24(1):100–106. doi:10.1089/jwh.2014.4872
15. Ncube CN, Enquobahrie DA, Albert SM, Herrick AL, Burke JG. Association of neighborhood context with offspring risk of preterm birth and low birthweight: a systematic review and meta-analysis of population-based studies. Soc Sci Med. 2016;153:156–164. doi:10.1016/j.socscimed.2016.02.014
16. Grote NK, Bridge JA, Gavin AR, et al. A meta-analysis of depression during pregnancy and the risk of preterm birth, low birth weight, and intrauterine growth restriction. Arch Gen Psychiatry. 2010;67(10):1012–1024. doi:10.1001/archgenpsychiatry.2010.111
17. Shah PS, Shah J. Maternal exposure to domestic violence and pregnancy and birth outcomes: a systematic review and meta-analyses. J Women’s Health. 2010;19(11):2017–2031. doi:10.1089/jwh.2010.2051
18. Ferdos J, Rahman MM, Jesmin SS, Rahman MA, Sasagawa T. Association between intimate partner violence during pregnancy and maternal pregnancy complications among recently delivered women in Bangladesh. Aggress Behav. 2018;44(3):294–305. doi:10.1002/ab.21752
19. Holmes MR, Bender AE, Crampton DS, Voith LA, Prince DM. Research foundations of GreenBook interventions to address the co‐occurrence of child maltreatment and adult domestic violence. Juv Fam Court J. 2019;70(4):11–36. doi:10.1111/jfcj.12150
20. Howard LM, Oram S, Galley H, Trevillion K, Feder G, Tsai AC. Domestic violence and perinatal mental disorders: a systematic review and meta-analysis. PLoS Med. 2013;10(5):e1001452. doi:10.1371/journal.pmed.1001452
21. Mahapatro M, Gupta RN, Gupta V, Kundu AS. Domestic violence during pregnancy in India. J Interpers Violence. 2011;26(15):2973–2990. doi:10.1177/0886260510390948
22. Alebel A, Kibret GD, Wagnew F, et al. Intimate partner violence and associated factors among pregnant women in Ethiopia: a systematic review and meta-analysis. Reprod Health. 2018;15(1):1–2. doi:10.1186/s12978-018-0637-x
23. Getaneh T, Asres A, Hiyaru T, Lake S. Adverse perinatal outcomes and its associated factors among adult and advanced maternal age pregnancy in Northwest Ethiopia. Sci Rep. 2021;11(1):14072. doi:10.1038/s41598-021-93613-x
24. Demographic IE. Health survey 2016: key indicators report. Addis Ababa, Ethiopia, and Rockville, Maryland, USA. Ethiopia: Ethiopia Demographic and Health Survey; 2016.
25. Basu S, Ratcliffe G. Developing a multidisciplinary approach within the ED towards domestic violence presentations. Emerg Med J. 2014;31(3):192–195. doi:10.1136/emermed-2012-201947
26. Yohannes K, Abebe L, Kisi T, et al. The prevalence and predictors of domestic violence among pregnant women in Southeast Oromia, Ethiopia. Reprod Health. 2019;16(1):1. doi:10.1186/s12978-019-0694-9
27. Asratie MH. Domestic violence during COVID-19 pandemic among pregnant women registered for antenatal care and selected adverse pregnancy outcomes in Amhara region Ethiopia: prospective cohort study design. Clin Epidemiol Global Health. 2022;17:101146. doi:10.1016/j.cegh.2022.101146
28. Berhanie E, Gebregziabher D, Berihu H, Gerezgiher A, Kidane G. Intimate partner violence during pregnancy and adverse birth outcomes: a case-control study. Reprod Health. 2019;16(1):1–9. doi:10.1186/s12978-019-0670-4
29. Belay HG, Debebe GA, Ayele AD, et al. Intimate partner violence during pregnancy and adverse birth outcomes in Ethiopia: a systematic review and meta-analysis. PLoS One. 2022;17(12):e0275836. doi:10.1371/journal.pone.0275836
30. McDermott CL, Acheampong E, Arora-Jonsson S, et al. SDG 16: peace, justice and strong institutions–a political ecology perspective. In: Katila P, Pierce Colfer CJ, de Jong W, Galloway G, Pacheco P, Winkel G, editors. Sustainable Development Goals: Their Impacts on Forests and People. Cambridge, UK: Cambridge University Press; 2019:510–540.
31. Ngamjarus C. n4Studies: sample size calculation for an epidemiological study on a smart device. Siriraj Med J. 2016;68(3):160–170.
32. Pool MS, Otupiri E, Owusu-Dabo E, De Jonge A, Agyemang C. Physical violence during pregnancy and pregnancy outcomes in Ghana. BMC Pregnancy Childbirth. 2014;14(1):1–8. doi:10.1186/1471-2393-14-71
33. Pallitto CC, García-Moreno C, Jansen HA, et al. Intimate partner violence, abortion, and unintended pregnancy: results from the WHO multi-country study on women’s health and domestic violence. Int J Gynecol Obstetr. 2013;120(1):3–9. doi:10.1016/j.ijgo.2012.07.003
34. Ludermir AB, Araújo TV, Valongueiro SA, Muniz ML, Silva EP. Previous experience of family violence and intimate partner violence in pregnancy. Rev Saude Publica. 2017;51:85. doi:10.11606/S1518-8787.2017051006700
35. Adhena G, Oljira L, Dessie Y, Hidru HD. Magnitude of intimate partner violence and associated factors among pregnant women in Ethiopia. Adv Public Health. 2020;2020:1–9. doi:10.1155/2020/1682847
36. Begum S, Donta B, Nair S, et al. Socio-demographic factors associated with domestic violence in urban slums, Mumbai, Maharashtra, India. Indian J Med Res. 2015;141(6):783. doi:10.4103/0971-5916.160701
37. Noori A, Sanago A, Jouybari L, Azimi M. Survey of types of domestic violence and its related factors in pregnant mothers in Kalaleh at 2014. Iran J Obstet Gynecol Infertil. 2017;19(39):54–62. doi:10.22038/ijogi.2017.8422
38. Okada MM, Hoga LA, Borges AL, Albuquerque RS, Belli MA. Domestic violence against pregnant women. Acta Paulista de Enfermagem. 2015;28(3):270–274. doi:10.1590/1982-0194201500045
39. Almeida FS, Coutinho EC, Duarte JC, et al. Domestic violence in pregnancy: prevalence and characteristics of the pregnant woman. J Clin Nurs. 2017;26(15–16):2417–2425. doi:10.1111/jocn.13756
40. Pun KD, Rishal P, Darj E, et al. Domestic violence and perinatal outcomes–a prospective cohort study from Nepal. BMC Public Health. 2019;19(1):1–9. doi:10.1186/s12889-019-6967-y
41. Donovan BM, Spracklen CN, Schweizer ML, et al. Intimate partner violence during pregnancy and the risk for adverse infant outcomes: a systematic review and meta‐analysis. BJOG. 2016;123(8):1289–1299. doi:10.1111/1471-0528.13926
42. Desta M, Getaneh T, Memiah P, et al. Is preterm birth associated with intimate partner violence and maternal malnutrition during pregnancy in Ethiopia? A systematic review and meta analysis. Heliyon. 2021;7(10):e08103. doi:10.1016/j.heliyon.2021.e08103
43. Lee YS, Hadeed L. Intimate partner violence among Asian immigrant communities: health/mental health consequences, help-seeking behaviors, and service utilization. Trauma Violence Abuse. 2009;10(2):143–170. doi:10.1177/1524838009334130
44. Yimer T, Gobena T, Egata G, Mellie H. Magnitude of domestic violence and associated factors among pregnant women in Hulet Ejju Enessie District, Northwest Ethiopia. Adv Public Health. 2014;2014:1–8. doi:10.1155/2014/484897
45. Auger N, Low N, Lee GE, Ayoub A, Luu TM. Pregnancy outcomes of women hospitalized for physical assault, sexual assault, and intimate partner violence. J Interpers Violence. 2022;37(13–14):NP11135. doi:10.1177/0886260520985496
46. Das TK, Bhattacharyya R, Alam MF, Pervin A. Domestic violence in Sylhet, Bangladesh: analysing the experiences of abused women. Soc Change. 2016;46(1):106–123. doi:10.1177/0049085715618561
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.