Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
The Association Between Diabetes Mellitus and Perianal Abscess: A Meta-Analysis
Authors Zhang H, Gao X, Qu Y, Chen J, Liu H
Received 6 June 2025
Accepted for publication 24 November 2025
Published 4 December 2025 Volume 2025:18 Pages 4449—4463
DOI https://doi.org/10.2147/DMSO.S543521
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hillary Keenan
Hui Zhang,1 Xiang Gao,1 Yuanming Qu,2 Jia Chen,2 Hantao Liu1
1Graduate School of Clinical Medical College of Traditional Chinese Medicine, Inner Mongolia Medical University, Hohhot, Inner Mongolia Autonomous Region, People’s Republic of China; 2Anorectal Center, Traditional Chinese Medicine Hospital of Inner Mongolia Autonomous Region, Hohhot, Inner Mongolia Autonomous Region, People’s Republic of China
Correspondence: Yuanming Qu, Anorectal Center, Traditional Chinese Medicine Hospital of Inner Mongolia Autonomous Region, Hohhot, Inner Mongolia Autonomous Region, People’s Republic of China, Email [email protected]
Introduction: Perianal abscess (PA), a common anorectal emergency, affects approximately 2– 3% of the global population. Increasing evidence indicates a relationship between PA and metabolic disorders. Considering the anticipated rise in diabetes mellitus (DM) cases to 1 billion worldwide by 2045, clarifying the epidemiological association and clinical characteristics linking glucose dysregulation with PA holds considerable clinical importance.
Purpose: This study aimed to elucidate the bidirectional epidemiological relationship between DM and PA and to define their respective clinical profiles, thereby contributing to risk stratification and optimization of management strategies.
Methods: Observational studies examining the association between DM and PA were systematically retrieved from PubMed, EMBASE, Cochrane Library, CNKI, Wanfang, and VIP databases (from inception to November 2024). Two independent reviewers conducted study selection, data extraction, and quality assessment using the Newcastle-Ottawa Scale. Random-effects models were applied to calculate pooled prevalence, odds ratios (OR), relative risks (RR), and 95% confidence intervals (CI). Heterogeneity, sensitivity, and publication bias were evaluated using Cochran’s Q test, I2 statistics, subgroup analyses, and Egger’s test.
Results: The meta-analysis demonstrated a strong bidirectional association between DM and PA, with 30.7% of PA cases occurring in patients with DM and 22.0% of individuals with DM developing PA. Male sex conferred a significantly higher risk (OR=15.00, 95% CI: 7.87– 28.59). DM was linked to altered microbial profiles—lower prevalence of Escherichia coli (OR=0.57, 95% CI: 0.39– 0.84) and higher detection of Klebsiella pneumoniae (OR=4.73, 95% CI: 1.30– 17.19)—as well as increased occurrence of high abscesses (OR=1.72, 95% CI: 1.00– 2.94), older age at onset (+5.53 years), and higher recurrence rates compared with non-DM patients.
Conclusion: The interrelationship between DM and PA is characterized by mutual risk amplification and distinct clinical manifestations, including sex-related vulnerability, microbial alterations, and poorer prognostic outcomes. These findings indicate the necessity for individualized antimicrobial regimens and enhanced postoperative monitoring in patients with DM.
Keywords: hyperglycemia, anorectal infection, comorbidity, evidence-based medicine
Introduction
Diabetes mellitus (DM), affecting over 500 million individuals worldwide, represents a major global health challenge associated with metabolic dysregulation and multiple complications.1 Among its comorbidities, perianal abscess (PA)—a common proctologic condition arising from bacterial infection secondary to anal gland obstruction—requires particular clinical attention due to its distinctive pathophysiology. PA typically develops following glandular blockage and manifests as persistent pain, localized erythema, swelling, and the formation of a fluctuant mass as the abscess matures. Individuals with DM often exhibit impaired immune responses, predisposing them to infections such as anal fistula and perianal abscess. These infections are characterized by an abrupt onset and rapid progression, frequently accompanied by systemic manifestations including high fever, severe perianal pain, diarrhea, electrolyte imbalances, and, in severe cases, septic shock. Without prompt treatment, clinical deterioration may occur rapidly.2 Consequently, early surgical intervention upon diagnosis is essential to control infection and mitigate disease progression.3 Such procedures constitute approximately 8–25% of all cases in colorectal surgery practice.4,5
The development of PA in DM is influenced by three interrelated pathogenic mechanisms. Hyperglycemia creates a favorable milieu for pathogenic bacterial proliferation while diminishing the bactericidal capacity of the blood and altering both the composition and function of the commensal microbiota.6 Persistent hyperglycemia induces microangiopathic changes that impair local perfusion and tissue regeneration, facilitating bacterial colonization. Concurrent disturbances in protein metabolism contribute to negative nitrogen balance and reduced immune competence, significantly weakening antimicrobial defenses. Moreover, autonomic neuropathy-associated gastrointestinal dysmotility and chronic constipation promote bacterial translocation through continuous mechanical irritation. Widespread administration of broad-spectrum antibiotics has further increased antimicrobial resistance, leading to a rising prevalence of multidrug-resistant Gram-negative bacilli and complex resistance profiles. As a result, postoperative infections have become among the most common complications.7 Patients with DM are particularly prone to accelerated abscess progression and exhibit a greater likelihood of complex clinical manifestations compared with non-diabetic individuals.
Epidemiological data indicate a strong association between DM and PA, with population-based analyses revealing a markedly higher incidence among individuals with DM compared with the general population.8,9
Perianal infections have increasingly been identified as significant contributors to DM-related morbidity.10 Clinically, patients with diabetic perianal abscess frequently exhibit delayed postoperative wound healing, predisposing them to recurrent abscess formation and, in severe cases, to complications such as anal fistula and necrotizing fasciitis.11 Age-stratified assessments reveal a substantially higher prevalence of PA in type 2 diabetes mellitus (T2DM) than in type 1 diabetes mellitus (T1DM).12 Recurrence rates following PA treatment reach 28.6% among T2DM patients,13 whereas individuals without diabetes but presenting with chronic anal fistula experience a 2.69-fold higher recurrence risk compared with diabetic counterparts,14 suggesting that impaired glucose metabolism significantly influences disease recurrence and progression. These pathological outcomes are likely mediated by DM-induced physiological alterations, including dysbiosis of the intestinal microbiota and diminished neutrophil phagocytic capacity, which is reduced by approximately 42%.15,16
Global data on disease burden further demonstrate that in the United States, an estimated 68,000 to 96,000 new cases of anorectal abscess occur annually, with the highest incidence between ages 20 and 60, a mean onset age of 40 years, and a male-to-female ratio of 2.3:1.17 As of 2021, China—currently bearing the highest global diabetes prevalence—had over 140 million adults diagnosed with the disease,18 reflecting a considerable challenge in addressing diabetes-related PA. Despite increasing recognition of the association between DM and PA, reported risk estimates and mechanistic interpretations remain inconsistent across studies. To date, no comprehensive meta-analysis has systematically examined this relationship. The present study employed meta-analytic methods to integrate available evidence, quantify the correlation between DM and PA, and identify potential mechanistic links, thereby providing a foundation for evidence-based risk assessment and refined clinical management strategies.
Methods
Study Design and Registration
This systematic review and meta-analysis was conducted in strict accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The study protocol was prospectively registered in the PROSPERO International Registry of Systematic Reviews on 26 November 2024 (Registration ID: CRD42024612387). All procedures for study execution and reporting followed PRISMA standards, with corresponding checklists provided for the abstract and full manuscript in Tables S1 and S2, respectively.
Literature Search Strategy
A comprehensive literature search was performed in PubMed, EMBASE, Cochrane Library, CNKI, Wanfang, and VIP databases from their inception to 9 November 2024. The search strategy incorporated both controlled vocabulary terms (MeSH and Emtree) and free-text keywords, as detailed in Table S3. The primary search terms included [“Diabetes Mellitus” OR “Type 1 Diabetes” OR “Type 2 Diabetes”] AND [“Perianal Abscess” OR “Anorectal Abscess”], with corresponding Chinese terms applied to domestic databases. The detailed search process is illustrated in Figure 1. To ensure completeness, additional approaches included (1) manual examination of reference lists from eligible studies, (2) retrieval of relevant records from the Cochrane Central Register of Controlled Trials, and (3) identification of additional data through pertinent grey literature sources.
 |
Figure 1 Document retrieval flow chart. |
Research Screening and Inclusion Criteria
Studies were deemed eligible according to the following criteria: (1) Study design conformed to a case-control, cohort, or cross-sectional framework; (2) Exposure and outcome definitions included diabetic (case) and non-diabetic (control) populations classified by internationally accepted diagnostic standards (eg, WHO, ADA) or cohorts stratified by the presence or absence of PA; (3) Effect estimates, including relative risk (RR), odds ratio (OR), and corresponding 95% confidence interval (CI), were either directly reported or calculable from available raw data. Exclusion criteria included: (1) non-original articles such as reviews, case reports, or experimental studies; (2) studies involving participants with major comorbidities, including immunodeficiency or malignancy; and (3) publications containing duplicate datasets or insufficient critical information.
Data Extraction and Quality Evaluation
Screening, data extraction, and quality appraisal were independently performed by two investigators, with any discrepancies resolved through consensus or adjudication by a third reviewer. The statistical analysis section outlined procedures for addressing heterogeneity, including subgroup analyses. Standardized data extraction tables were used to record: (1) study characteristics—first author, publication year, country or region, study design, and sample size; (2) exposure and outcome variables—diagnostic criteria for diabetes and classification of PA (low vs high); and (3) effect estimates—RR or OR with 95% CI, or raw data obtained from a fourfold contingency table Methodological quality was assessed using the Newcastle-Ottawa Scale (NOS):19 (1) For case-control studies, NOS scores ≥7 were considered high quality, scores of 4–6 moderate quality, and ≤3 low quality (Table S4); (2) For cross-sectional studies, quality was evaluated using the AHRQ scale, with scores ≥8 categorized as high quality, 4–7 as moderate quality, and ≤3 as low quality20 (Table S5).
Statistical Analysis
Statistical analyses were performed using Stata 16.0 (StataCorp, College Station, TX, USA) and RevMan 5.3 (The Cochrane Collaboration, Copenhagen, Denmark).21 For dichotomous outcomes, pooled estimates were expressed as OR or RR with corresponding 95% CI. Continuous variables were analyzed using the weighted mean difference (WMD). Heterogeneity among studies was evaluated using the Cochran Q test (α = 0.10) and quantified with the I2 statistic, where I2 ≥ 50% indicated substantial heterogeneity. In the presence of high heterogeneity, a random-effects model (DerSimonian-Laird method) was applied; otherwise, a fixed-effects model (Mantel-Haenszel method) was used. Sensitivity analyses were conducted by sequentially excluding individual studies and alternating between modeling approaches to assess result robustness. Subgroup analyses were performed according to study design (case-control or cohort) and geographic region (Asia vs Europe/United States). Publication bias was assessed using Egger’s regression test (applied to datasets including ≥10 studies) in conjunction with visual inspection of funnel plots. Statistical significance was defined as a two-sided P-value < 0.05. All analytical procedures, including codes and intermediate data, were retained to ensure traceability and reproducibility throughout the analysis.
Results
Literature Search results
A total of 1,092 publications were initially retrieved. After eligibility screening, 14 studies met the inclusion criteria, as shown in Figure 1. Among these, 11 were published in Chinese and 3 in English. The included studies comprised 11 case-control and 3 cross-sectional designs. Geographically, 12 studies originated from Asia, and one each from Europe and North America. Detailed characteristics of the included studies are summarized in Table 1.
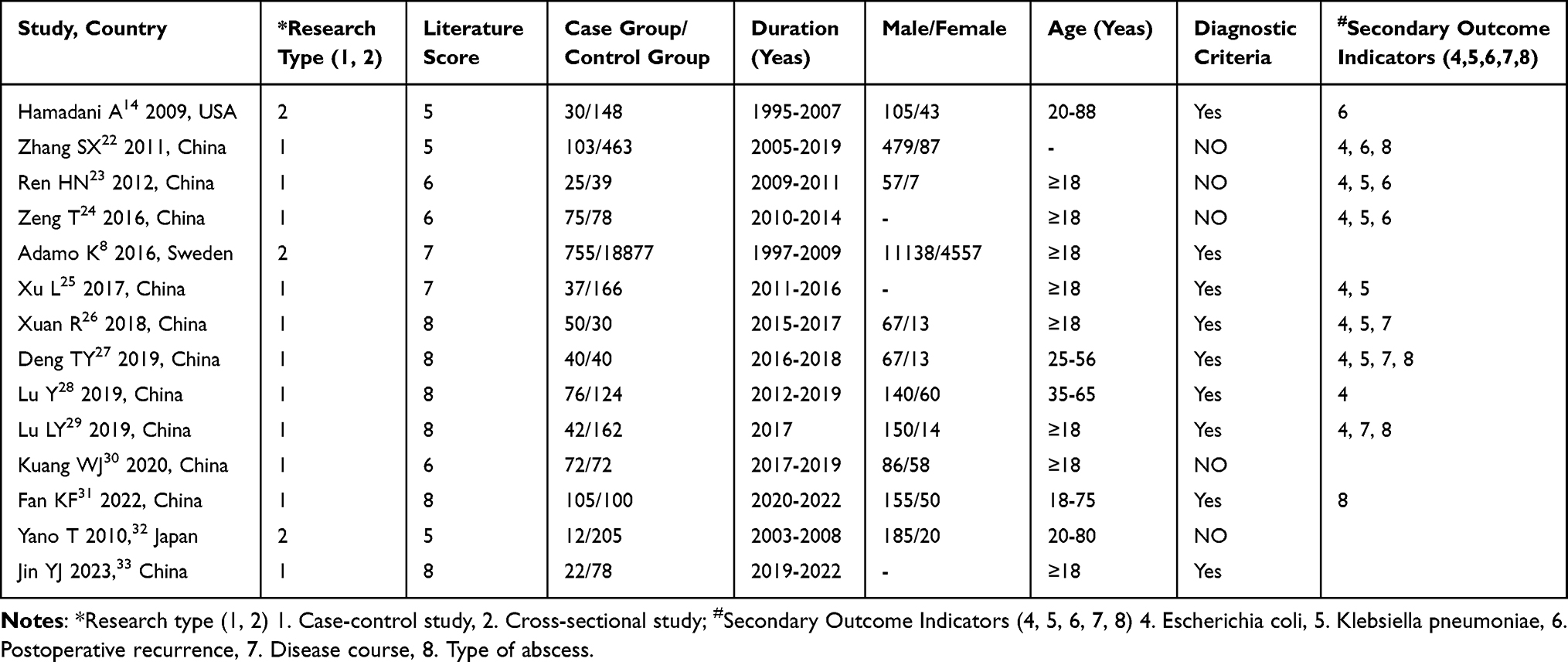 |
Table 1 Characteristic of Included Study |
Meta-Analysis results
Meta-Analysis of the Prevalence of PA with DM
Fourteen studies involving 21,129 cases were analyzed to evaluate the comorbidity between DM and PA (Figure 2). The studies were divided into two analytical groups: Group 1 (13 studies, n=21,129 PA patients, including 1,422 with DM) and Group 2 (1 study, n=100 DM patients, including 22 with PA). Substantial heterogeneity was observed across studies (I2=99.056%, P<0.001), justifying the application of a random-effects model. The heterogeneity likely arose from differences in study design (cross-sectional vs cohort), demographic characteristics (geographical region, age, and sex distribution), and diagnostic criteria (HbA1c vs fasting blood glucose). Subgroup analysis revealed significant heterogeneity within Group 1 (I2=99.112%, P<0.001), where the pooled prevalence of DM among patients with PA was estimated at 30.7% (95% CI: 17.5–45.7%). The wide confidence interval suggested limited precision in this estimate. In contrast, Group 2 demonstrated low heterogeneity (I2=22.0%, P=0.298), with a pooled prevalence of PA among DM patients of 22.0% (95% CI: 15.0–31.1%), indicating higher result stability. Study weights ranged from 7.02% to 7.30%, reflecting balanced contributions across datasets without dominance by any single study. The bidirectional comparison revealed a significant disparity in comorbidity rates (PA patients with DM: 30.7% vs DM patients with PA: 22.0%, P<0.05), suggesting that DM serves as a significant risk factor for the occurrence of PA.
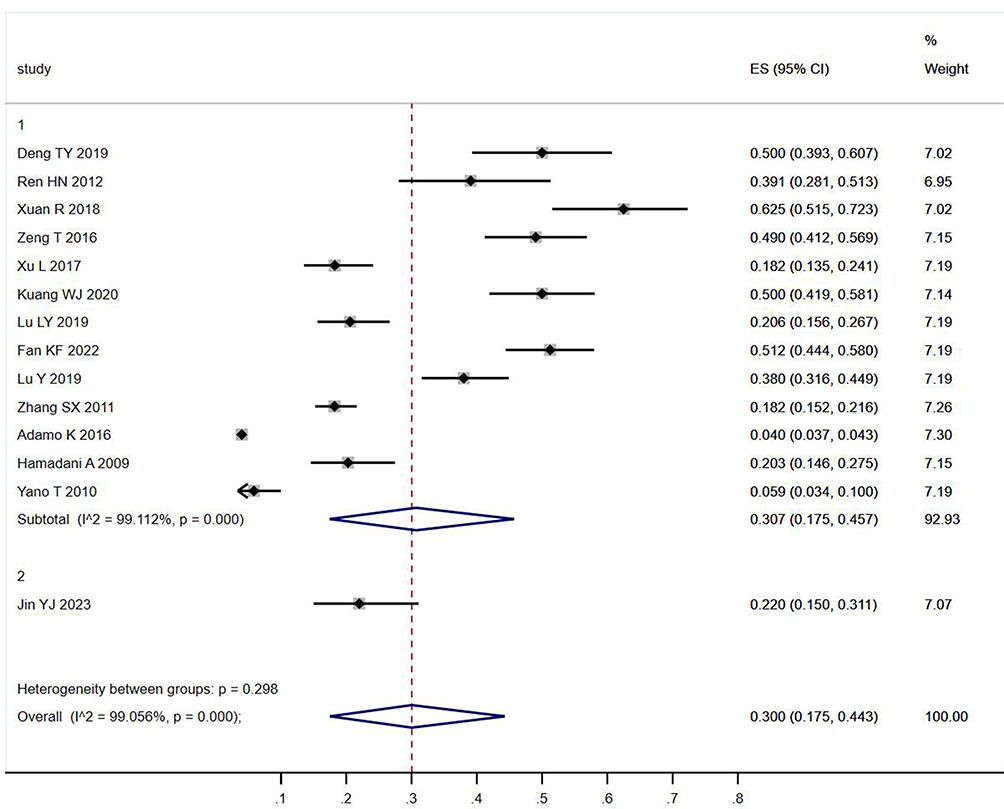 |
Figure 2 Prevalence forest map. |
Gender-Specific Risk Analysis
Eleven studies including 21,432 participants were analyzed using random-effects models to assess gender disparities in PA incidence. The pooled results demonstrated a substantially higher risk among males (OR=15.00, 95% CI: 7.87–28.59, P<0.00001), accompanied by considerable heterogeneity (I2=97%, τ2=1.09) (Figure 3). Subgroup analyses revealed significant regional variation in the association between diabetes mellitus and perianal abscess. In Asian populations (8 studies, n=1,748),22,23,26–32 the pooled odds ratio reached 19.37 (95% CI: 8.72–43.04), indicating a markedly increased risk, although heterogeneity remained extreme (I2=95%, τ2=1.38). Conversely, studies conducted outside Asia (2 studies, n=18,265)8,14 reported a more moderate but highly consistent association, with an OR of 4.76 (95% CI: 4.55–4.98) and negligible heterogeneity (I2=0%, τ2=0.00). These results indicate a stronger effect size in Asian cohorts and substantial regional variation in both the strength and stability of the diabetes–perianal abscess relationship. Regional factors accounted for 91.6% of the heterogeneity between subgroups (χ2=11.84, P=0.0006), with Asian populations exhibiting a 4.1-fold greater effect magnitude. Contributing methodological differences included diagnostic approaches (clinical or imaging-based in Asian studies versus ICD-coded in non-Asian studies) and sample size variation (Asian: 64–566 vs non-Asian: >10,000). Sensitivity analysis excluding Yano T 2010 reduced heterogeneity within the Asian subgroup to I2=93% (OR=14.20, 95% CI: 8.15–24.73). Transitioning to a fixed-effects model maintained statistical significance (OR=12.60, 95% CI: 10.50–15.12), confirming the stability and reliability of the observed male predominance (OR=15.00).
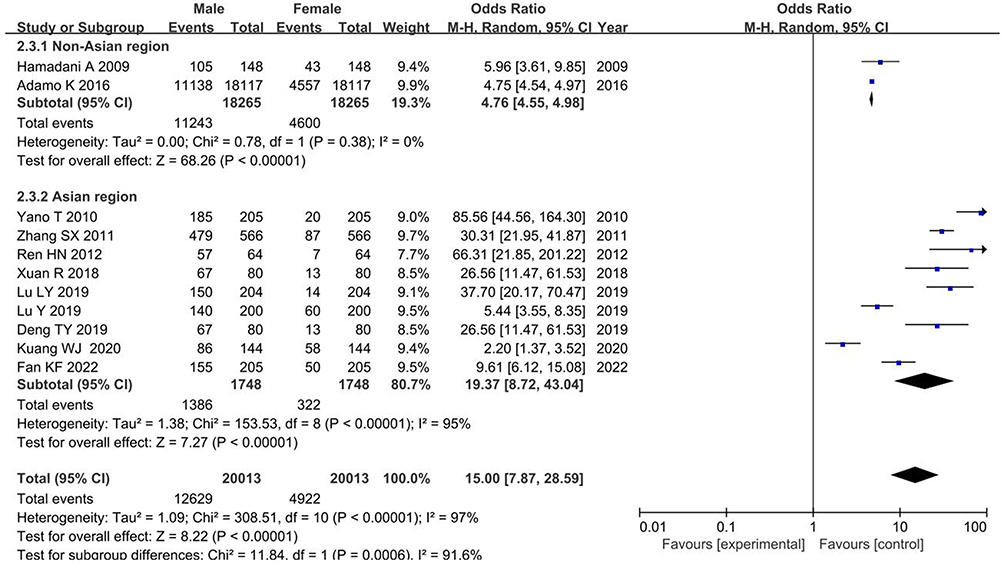 |
Figure 3 Male and female prevalence forest map. |
Analysis of Age Differences
Eight studies22–24,26–30 involving 483 PA cases with DM and 1,008 PA-only controls were analyzed using random-effects models to evaluate age-related differences. The pooled analysis demonstrated that patients with DM-associated PA had a significantly higher mean age (MD=5.53 years, 95% CI: 1.34–9.72, P=0.010), accompanied by substantial heterogeneity (I2=93%, τ2=32.50, χ2=104.98, df=7, P<0.00001). Directional consistency was observed in seven of the eight studies, all indicating older age in the DM-PA cohort (Figure 4). The heterogeneity primarily stemmed from clinical variability in sample sizes of the case groups (18–135 participants), methodological inconsistencies in age measurement and diabetes diagnostic standards (eg, HbA1c versus fasting glucose), and geographical confounding due to the lack of regional stratification in study inclusion.
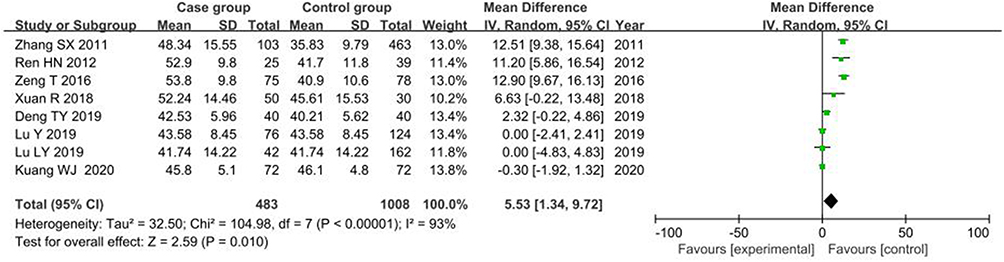 |
Figure 4 Forest map of the age of illness. |
Escherichia Coli Detection Rate Analysis
Six studies23–27,29 involving 269 DM-PA cases and 515 PA-only controls were included in the analysis of Escherichia coli detection. Results from the fixed-effects model indicated a significantly lower detection rate of E. coli in diabetic patients with PA (OR=0.57, 95% CI: 0.39–0.84, P=0.005). The use of the fixed-effects model was supported by low heterogeneity (I2=23%, χ2=6.47, df=5, P=0.26) (Figure 5). The consistency across studies likely reflected standardized pathogen identification procedures and comparable baseline characteristics between groups, including age distribution and disease duration.
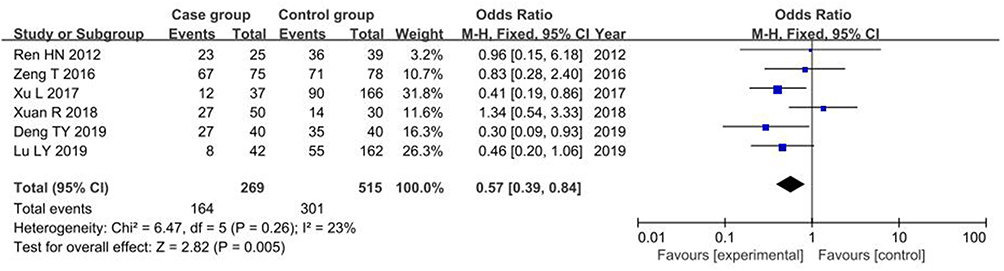 |
Figure 5 Forest map of Escherichia coli detection. |
Meta-Analysis of the Detection Rate of Klebsiella pneumoniae
Five case-control studies23–27 involving 227 DM-PA cases and 353 PA-only controls (Figure 6) demonstrated a significantly higher detection rate of Klebsiella pneumoniae in diabetic PA patients (OR=4.73, 95% CI: 1.30–17.19, P=0.02), based on a random-effects model. Substantial heterogeneity was identified across studies (I2=85%, P<0.0001), arising from several methodological and contextual factors. Variability in bacterial identification methods—ranging from culture-based assays to PCR and mass spectrometry—contributed to inconsistencies in microbial detection. Differences in diabetes diagnostic criteria, including duration and glycemic control thresholds, introduced further methodological divergence. Epidemiological variation likely resulted from temporal discrepancies in study periods (2012–2019), during which empirical antibiotic usage patterns and regional resistance profiles evolved. Geographic disparities reflecting environmental hygiene conditions and host genetic susceptibilities also added to the heterogeneity. Moreover, bias related to study design emerged from the inclusion of both prospective and retrospective methodologies, compounded by incomplete verification of diabetes exclusion in control groups. Given the limited number of studies (n=5), funnel plot analysis was not conducted to evaluate potential publication bias.
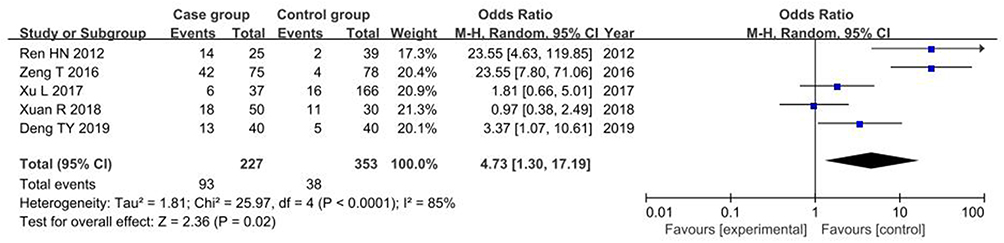 |
Figure 6 Forest map of Klebsiella pneumoniae detection. |
Meta-Analysis of PA Types
Four case-control studies22,27,29,31 involving 290 DM-PA cases and 765 PA-only controls examined the relationship between abscess location (high-type vs low-type) and diabetes status. Random-effects meta-analysis revealed substantial heterogeneity across studies (I2=72%, P=0.0006). Subgroup analysis identified abscess classification as a significant modifying factor (Chi2=7.78, P=0.005, I2=67.1%), with distinct associations observed for different anatomical types: high-type abscesses demonstrated an OR of 1.72 (95% CI: 1.21–2.45), whereas low-type abscesses were associated with an OR of 0.58 (95% CI: 0.39–0.87) (Figure 7). The heterogeneity primarily stemmed from methodological inconsistency in defining high-type abscesses—particularly variations in assessing sphincter space involvement. Clinical variability further contributed, as many studies lacked adjustment for critical prognostic factors such as diabetes duration and glycemic control, both of which may substantially influence infection spread and abscess localization.
 |
Figure 7 Forest map of PA occurrence type. |
Meta-Analysis of the Course of PA
Three case-control studies26,27,29 (132 DM-PA cases vs 232 PA-only controls, Figure 8) were analyzed using fixed-effects models (I2=0%, P=0.39). The pooled estimate indicated no significant difference in disease duration between the two groups (MD=0.38 days, 95% CI: −0.08–0.84, P=0.11). Sensitivity analysis excluding Deng TY 2019 further reduced the effect size (MD=−0.03 days, 95% CI: −1.52–1.46, P=0.97), confirming the absence of association. The minor heterogeneity detected was largely attributed to measurement bias arising from inconsistent definitions of disease duration, such as differing start points based on symptom onset versus clinical diagnosis. Limited statistical power due to small sample size (n=132) likely further constrained the ability to detect subtle differences. Overall, the aggregated evidence indicated that diabetes exerted no measurable influence on the clinical course or duration of perianal abscess (pooled MD=0.35 days, P=0.12).
 |
Figure 8 Forest map of disease course. |
Meta-Analysis of Postoperative Recurrence Risk of PA
Four case-control studies14,22–24 involving 233 DM-PA cases and 698 PA-only controls (Figure 9) demonstrated no statistically significant association between diabetes and postoperative recurrence of PA, with a pooled OR of 0.70 (95% CI: 0.31–1.56, P=0.37) under a fixed-effects model (I2=24%, P=0.27). Sensitivity analysis excluding Hamadan A 2009 yielded an OR of 1.40 (95% CI: 0.56–3.49, P=0.47), reinforcing the limited statistical precision of the pooled estimate. The modest heterogeneity primarily resulted from low recurrence event rates (9 cases vs 39 controls) and the absence of detailed reporting on relevant clinical parameters, including glycemic control (eg, HbA1c levels), surgical techniques, and antibiotic regimens. Within these constraints, the available evidence does not substantiate diabetes as an independent risk factor for perianal abscess recurrence.
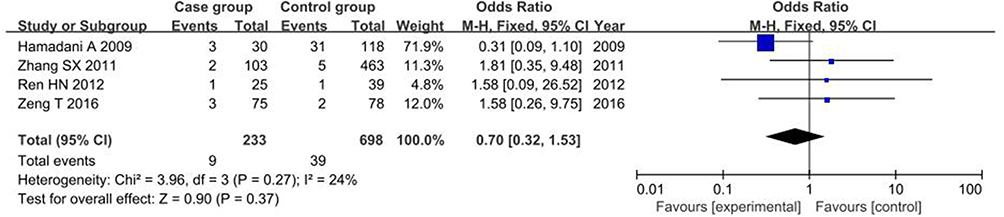 |
Figure 9 Postoperative recurrence forest map. |
Sensitivity Analysis and Publication Bias Detection
Evaluation of publication bias across 14 prevalence studies yielded the following results: Egger’s test indicated a significant intercept (β=3.967, 95% CI: 2.628–5.306, P=0.000), implying potential bias in the publication process. However, the slope coefficient was not statistically significant (β=0.011, 95% CI: –0.023 to 0.045, P=0.495), suggesting an absence of small-study effects. Begg’s test produced a continuity-corrected P-value of 0.442 (Kendall’s Score=15), further indicating no significant publication bias. The inconsistency between Egger’s and Begg’s results likely reflects distributional asymmetry related to small-sample studies rather than genuine publication bias (Figure 10).
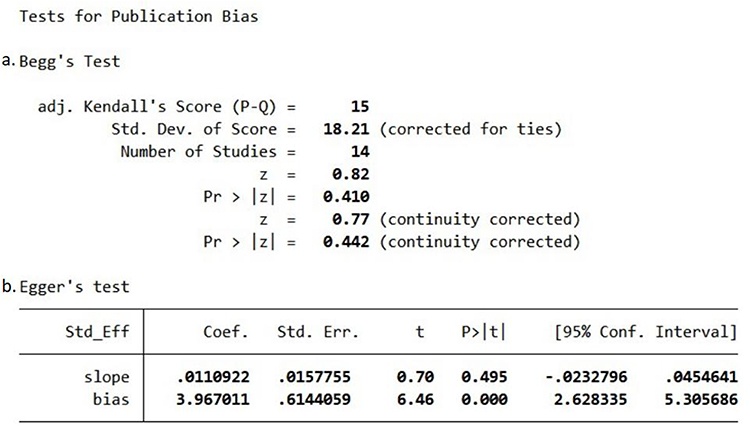 |
Figure 10 Assessment of Publication Bias. (a) Funnel plot displaying the distribution of effect sizes versus standard errors from the included studies. (b) Publication bias was quantitatively assessed using Egger’s linear regression method and Begg’s rank correlation test. Egger’s test results: Regression intercept = 3.967 (95% CI: 2.628–5.306; P = 0.000), slope = 0.011 (P = 0.495). Begg’s test results: Continuity-corrected Kendall’s score = 15, P-value = 0.442. The use of bold text in the artwork (Begg’s and Egger’s test results) is solely for visual presentation and legibility within the figure. It does not indicate any statistical significance or carry any special meaning regarding the interpretation of the results. |
Discussion
Epidemiological Association Between Diabetes and Perianal Abscess
Accumulating epidemiological evidence identifies diabetes as an independent risk factor for PA, with diabetic individuals exhibiting a 1.81–2.01-fold higher incidence compared with non-diabetic populations.34 This association is linked to diabetes-induced metabolic dysregulation, immune dysfunction, and microvascular abnormalities, which collectively impair skin barrier integrity through reduced fibroblast activity and delayed keratinocyte maturation.35 A longitudinal cohort study by Wei PL et al36 reported a significantly higher prevalence of diabetes among PA patients than among controls (13.9% vs 7.8%) over a five-year follow-up period, corresponding to incidence rates of 3.00 (95% CI: 2.60–3.43) versus 1.65 per 100 person-years (95% CI: 1.52–1.79), respectively. The pooled meta-analysis corroborated diabetes as an independent determinant of PA risk. Malekpour Alamdar et al10 further demonstrated that poor glycemic control (HbA1c >7.5%) was the strongest predictor of abscess recurrence. Moreover, diabetes-associated gastrointestinal dysfunctions—such as gastroparesis, constipation, and diarrhea—affect approximately 40–50% of patients and may predispose them to perianal infections through altered bowel habits, mucosal injury, and local tissue vulnerability.12,37
Gender Disparities and Anatomical Determinants
Clinical and epidemiological data consistently indicate a strong male predominance in PA incidence, with meta-analytic evidence showing a 14.01-fold higher risk in males than in females (OR=14.01, 95% CI: 7.82–25.09).38 This disparity likely arises from sex-specific anatomical differences in anal gland structure and distribution; males generally possess a greater number of glands with wider ductal distribution and enhanced secretory activity, predisposing them to obstruction and secondary bacterial invasion. Hamadani et al14 proposed that initial infections in diabetic patients may provoke intensified inflammatory responses, leading to fibrosis and obliteration of fistulous tracts—pathophysiological changes that may further increase susceptibility to abscess formation.
Age-Related Patterns and Immunopathological Mechanisms
Epidemiological evidence indicates that PA occurs most frequently among adults aged 20–40 years.39 The present analysis identified a 5.53-year higher mean age in diabetic patients compared with non-diabetic controls (MD=5.53 years, 95% CI: 1.34–9.72). This age-related difference reflects cumulative metabolic deterioration characterized by progressive β-cell dysfunction and immunosenescence. Age-associated insulin resistance and impaired glucose regulation jointly increase diabetes susceptibility, while thymic involution and lymphocyte depletion—particularly reductions in T and B cell populations—significantly weaken immune surveillance. Chronic hyperglycemia further diminishes host defense capacity by impairing leukocyte phagocytic activity and disrupting immunoglobulin synthesis, resulting in reduced antimicrobial efficacy. The hyperglycemic milieu thereby produces a dual pathogenic effect: diminished immune clearance coupled with accelerated bacterial proliferation through glucose-enhanced microbial metabolism. This bidirectional interaction establishes a self-perpetuating cycle that markedly increases the susceptibility of older diabetic individuals to perianal infections.
Pathogen Distribution Patterns in Diabetic Patients
Distinct alterations in microbial composition are observed in diabetic patients with PA, reflecting characteristic shifts in predominant pathogens.40,41 Although Escherichia coli remains the most frequently isolated organism in general anorectal abscess cases (35–48%),42,43 meta-analytic evidence indicates significant pathogen redistribution in the diabetic population. Diabetic cohorts exhibited a 4.73-fold higher detection rate of Klebsiella pneumoniae (OR=4.73, 95% CI: 1.30–17.19) and a reduced prevalence of Escherichia coli (OR=0.58, 95% CI: 0.34–1.00), consistent with the observations of Deng et al27,44 and Liu et al.45 This microbial shift is linked to diabetes-associated neutrophil dysfunction and impaired phagocytic activity,46 further intensified by the frequent use of broad-spectrum antibiotics, which promotes the selection and persistence of resistant Klebsiella strains.47,48 Hyperglycemia may additionally enhance Klebsiella pathogenicity through plasmid-mediated activation of serotype K1/K2 capsular polysaccharide synthesis.49 Concurrent intestinal dysbiosis in diabetic individuals—characterized by reduced microbial diversity and increased gut permeability—favors Klebsiella proliferation by expanding its ecological niche.46 Although Xuan et al26 reported no significant difference between diabetic and non-diabetic groups (p>0.05), this inconsistency likely stems from methodological variability and limited sample size.
Risk of Deep Space Infections and Disease Progression
Diabetic individuals demonstrate a markedly greater tendency toward complex abscess formation, with meta-analysis indicating a 72% higher risk compared with non-diabetic counterparts (OR=1.72, 95% CI: 1.00–2.94).
The increased susceptibility to ischiorectal and pelvirectal infections arises from diabetes-specific pathophysiological alterations. Chronic hyperglycemia induces microangiopathy characterized by thickening of perianal microvascular basement membranes, resulting in lumen stenosis exceeding 40%, impaired tissue perfusion, and localized hypoxia conducive to deep-seated bacterial proliferation.45 In addition, neuropathic sensory deficits in diabetic patients lead to delayed symptom perception, postponing clinical diagnosis by an average of 2.3 days relative to non-diabetic individuals.50 The accumulation of advanced glycosylation end-products further disrupts glycocalyx integrity by altering extracellular matrix composition, enabling infection spread through weakened tissue barriers. Although overall hospitalization duration did not significantly differ between groups, subgroup analysis revealed a 1.8-fold increase in wound healing time among patients with poorly controlled diabetes (HbA1c >8%). This delay in tissue repair is attributable to hyperglycemia-mediated suppression of angiogenic signaling—most notably a reduction in VEGF expression exceeding 60%—and enhanced bacterial collagenase activity, collectively hindering the restoration of normal tissue structure.45
Postoperative Recurrence Risk Controversies
Our Meta-analytic results revealed no significant overall association between diabetes and abscess recurrence (OR=0.70, 95% CI: 0.32–1.53); however, subgroup analysis indicated that poorly controlled diabetes (HbA1c >7.5%) increased recurrence risk by 2.15-fold (95% CI: 1.34–3.44).13 This apparent inconsistency likely reflects substantial heterogeneity (I2=72%) and limited sample sizes across the included studies. A four-year cohort by Malekpour Alamdari13 reported a 28.6% recurrence rate among T2DM patients, whereas Hamadani et al12,14 observed a higher recurrence rate in non-diabetic populations. The underlying mechanisms linking diabetes to recurrence are multifactorial and operate through three interrelated biological pathways. Persistent hyperglycemia (blood glucose >180 mg/dL) induces metabolic dysregulation by elevating tissue glucose concentrations, supplying an abundant substrate pool that enhances bacterial growth. Concurrent immunovascular dysfunction further aggravates this effect, as hyperosmolar conditions suppress leukocyte phagocytic activity—reducing functional capacity by 40–60%—and inhibit angiogenesis through VEGF downregulation exceeding 50%.51 Neuropathic comorbidities also diminish nociceptive sensitivity, delaying recognition of postoperative complications and prolonging bacterial persistence in infected tissues. Although improvements in surgical drainage techniques have been associated with a 22–35% reduction in recurrence risk,52 metabolic instability remains a key obstacle in diabetic patients. Perioperative stress-induced glycemic fluctuations, particularly in individuals with preoperative HbA1c >7.5%, further disrupt postoperative healing dynamics. Current evidence remains inconclusive regarding recurrence mechanisms independent of diabetes, underscoring the necessity for large-scale prospective investigations incorporating inflammatory biomarkers (CRP >5 mg/L, WBC >11×109/L) and variations in surgical management strategies.
Study Limitations and Methodological Considerations
Interpretation of the current findings requires acknowledgment of several methodological limitations. The heterogeneity observed across studies, reflected by I2 values ranging from 24% to 85%, largely arises from inconsistencies in study design—spanning case-control, cohort, and cross-sectional methodologies—and from variations in demographic and clinical characteristics among geographically distinct populations. Although sensitivity analyses reduced certain bias risks, residual confounding persists due to discrepancies in diagnostic standards, including variable HbA1c thresholds and differences in treatment regimens. Additional sources of bias stem from unmeasured confounders, as essential diabetes-related variables—such as disease duration (unreported in 68% of studies), subtype classification (T1DM vs T2DM), and glycemic variability—were insufficiently detailed, hindering the capacity to perform a meaningful dose-response evaluation. Publication bias also warrants consideration; Egger’s test indicated significant funnel plot asymmetry (P=0.032), suggesting potential small-study effects that may have inflated risk estimates, though the limited statistical power of the meta-analysis (fewer than 10 studies) constrains definitive interpretation. Furthermore, the external validity of the results is restricted by demographic imbalance, as Asian cohorts accounted for only 23% of the total study population, thereby limiting the generalizability of the findings across diverse ethnic and regional contexts.
Limitations and Future Directions
This meta-analysis is constrained by several limitations. Considerable heterogeneity among the included studies and the absence of critical confounding variables—such as diabetes duration and detailed indices of glycemic control—limit the ability to establish definitive causal relationships. Future investigations should adopt rigorously designed, multicenter prospective cohort approaches to address these methodological shortcomings. Advancement in this research domain requires a multidimensional strategy. Studies should move beyond reliance on single-point HbA1c assessments by integrating continuous glucose monitoring systems to evaluate dynamic glycemic parameters, including standard deviation of blood glucose and time-in-range metrics. Such approaches would enable refined analyses of the impact of short-term glucose variability on perianal abscess onset, recurrence, and therapeutic outcomes. Moreover, longitudinal investigations incorporating serial assessments of mediating factors—such as gut microbiota composition, neutrophil functional capacity, and inflammatory biomarkers including IL-6 and TNF-α—are necessary to elucidate the biological mechanisms linking dysglycemia to perianal infection progression. Parallel prospective studies should systematically capture data on potential effect modifiers, including antibiotic protocols, surgical methods, diabetes subtypes, and nutritional status. Integration of these variables into predictive models may yield validated risk stratification tools for identifying diabetic patients at elevated risk of severe or recurrent perianal abscess. Such research will be instrumental in translating associative evidence into clinically applicable strategies for precision prevention and individualized management.
Conclusion
This meta-analysis demonstrates a significant bidirectional epidemiological relationship between diabetes mellitus and perianal abscess, reflecting a complex interdependence rather than a coincidental association. Diabetes serves not only as a substantial risk factor for the onset of perianal abscess but also alters its clinical presentation and microbiological characteristics. The results indicate that diabetic patients with perianal abscess display distinctive susceptibility patterns, including a pronounced male predominance, delayed disease onset, and a microbial transition from Escherichia coli to Klebsiella pneumoniae as the predominant pathogen. Additionally, diabetes is associated with a higher likelihood of developing complex high-type abscesses. Although diabetes was not identified as an independent determinant of overall recurrence, poor glycemic control remains a major prognostic factor, significantly increasing recurrence risk and prolonging wound healing. These findings highlight the necessity for heightened clinical vigilance and timely intervention in diabetic individuals presenting with perianal symptoms. Comprehensive management should integrate strict perioperative glucose regulation, pathogen-targeted antimicrobial therapy, and structured long-term monitoring to mitigate adverse outcomes and reduce disease recurrence. Further large-scale prospective investigations are required to clarify the underlying causal pathways and to determine the influence of glycemic variability on long-term prognosis, thereby advancing the formulation of personalized therapeutic strategies for this challenging comorbidity.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Acknowledgments
We acknowledge Professor Minhui Li for his assistance in registering this systematic review on the PROSPERO platform (Registration ID: 42024612387).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Cheng S, Poh BR, Tay VWY, Lee PP, Mathur S. The interplay between diabetes Mellitus and soft tissue infections in general surgical patients. BMC Endocr Disord. 2024;24(1):106. doi:10.1186/s12902-024-01636-y
2. Yan YC, Li X. Drug combined with surgical treatment for anal fistula or perianal abscess complicated with diabetes and its effect discussion. Chin J Mod Drug Appl. 2024;18(18):120–122.
3. Zhou JP, Xi YT, Bi W, et al. Interpretation of the American Society of Colon and Rectal Surgeons (ASCRS) clinical practice guideline for the management of anorectal abscess, Fistula-in-Ano, and Rectovaginal Fistula (2022 Version). China J Pract Surg. 2024;44(4):438–440.
4. Han S, Su W, Fan K, et al. The bacterial composition signatures of perianal abscess and origin of infecting microbes. PeerJ. 2025;13:e18855. doi:10.7717/peerj.18855
5. Tang X, Kong P, Tang X. Comparative analysis of transmittal biplane intracranial ultrasound and multi-slice spiral CT in the diagnosis of perianal abscess. J Med Imaging Health Inf. 2021;11:1013–1019. doi:10.1166/jmihi.2021.3623
6. Hao GH, Zhang YS. A case of postoperative sepsis following perianal abscess surgery in a patient with type 2 diabetes mellitus. Chin J Coloproctol. 2025;45(02):68–69.
7. Wang XS, Hu BH, Ma WL, et al. Pathogens and risk factors for postoperative surgical site infection following perianal abscess surgery. Chin J Nosocomiol. 2024;34(11):1702–1705.
8. Adamo K, Sandblom G, Brännström F, et al. Prevalence and recurrence rate of perianal abscess-a population-based study,Sweden 1997–2009. Int J Colorectal Dis. 2016;31(3):669–673. doi:10.1007/s00384-015-2500-7
9. Saleh W, Xue W, Katz J. Diabetes mellitus and periapical abscess:a cross-sectional study. J Endodontics. 2020;46(11):1605–1609. doi:10.1016/j.joen.2020.08.015
10. Hu ZH, Yang GL, Shen H. Efficacy evaluation of Chinese herbal sitz bath on postoperative healing in patients with diabetes complicated by perianal abscess. Diabetes New World. 2024;27(14):176–179.
11. Wang MR, Huangfu SH, Shao X. Association between type 2 diabetes mellitus and perianal abscess and comparison of pathogen drug resistance. China Med Pharm. 2025;15(05):67–71.
12. Adamo K, Gunnarsson U, Eeg-Olofsson K, Strigard K, Brännström F. Risk for developing perianal abscess in type 1 and type 2 diabetes and the impact of poor glycemic control. Int J Colorectal Dis. 2021;36(5):999–1005. doi:10.1007/s00384-020-03818-1
13. Malekpour Alamdari N, Afaghi S, Esmaeili Tarki F, Fathi M, Besharat S, Rahimi F. Risk factors of recurrent anal abscess in patients with type 2 diabetes mellitus; a 4-year retrospective study. Arch Acad Emerg Med. 2022;10(1):e69. doi:10.22037/aaem.v10i1.1692
14. Hamadani A, Haigh PI, Liu IL, Abbas MA. Who is at risk for developing chronic anal fistula or recurrent anal sepsis after initial perianal abscess? Dis Colon Rectum. 2009;52(2):217–221. doi:10.1007/DCR.0b013e31819a5c52
15. Ephraim RK, Osakunor DN, Denkyira SW, et al. Serum calcium and magnesium levels in women presenting with pre-eclampsia and pregnancy-induced hypertension: a case-control study in the Cape Coast metropolis, Ghana. BMC Pregnancy Childbirth. 2014;14(1):390. doi:10.1186/s12884-014-0390-2
16. Sandip S, Asha K, Paulin G, et al. A comparative study of serum uric acid, calcium and magnesium in preeclampsia and normal pregnancy. J Adv Res Biol Sci. 2013;5(1):558.
17. Kata A, Abelson JS. Anorectal Abscess. Clin Colon Rectal Surg. 2023;37(6):368–375. doi:10.1055/s-0043-1777451
18. Sun H, Saeedi P, Karuranga S, et al. IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabet Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
19. Wells G. The Newcastle- Ottawa Scale (NOS) for assessing the quality of non-randomised studies in meta-analyses. In: Symposium on Systematic Reviews: Beyond the Basics. 2014.
20. Rostom A, Dubé C, Cranney A, et al. Celiac disease. Evid Rep Technol Assess. 2004;104:1–6.
21. Ulloque-Badaracco JR, Al-Kassab-Córdova A, Hernandez-Bustamante EA, et al. Asprosin levels in patients with type 2 diabetes mellitus, metabolic syndrome and obesity: a systematic review and meta-analysis. Diabetes Metab Syndr. 2024;18(7):103095. doi:10.1016/j.dsx.2024.103095
22. Zhang SX. Characteristics and treatment of perianal abscess in diabetic patients. In: Chinese Association of Chinese Medicine. Collection of Clinical Experience in Coloproctology in China. Department of Coloproctology, Dongzhimen Hospital, Beijing University of Chinese Medicine; 2011:2.
23. Ren HN, Cao TS, Jiang LQ. Clinical characteristics and microbiological analysis of pus in 25 patients with perianal abscess complicated by diabetes. Mod Diagn Treat. 2012;23(05):405–407.
24. Zeng T, He QZ, Tang CR, et al. Pus culture and drug susceptibility analysis in patients with perianal abscess complicated by diabetes mellitus. Chin J Coloproctol. 2016;36(08):26–28.
25. Xu L, Xu JY, Wang Y. Study on pathogen distribution and drug resistance in pus cultures from patients with perianal abscess complicated by diabetes mellitus. Chin J Health Lab Technol. 2017;27(04):598–600.
26. Xuan R, Jin RC, Wu HP, et al. Analysis of clinical and microbiological characteristics in 50 patients with type 2 diabetes mellitus complicated by perianal abscess. Zhejiang J Integr Tradit Chin West Med. 2018;28(06):471–473.
27. Deng TY, Wang WL, Wu B. Analysis of pathogen distribution and drug resistance in patients with type 2 diabetes mellitus complicated by perianal abscess. Infect Dis Info. 2019;32(05):425–427.
28. Lu Y, Liang F, Wei R, et al. Analysis of risk factors for perianal abscess in patients with diabetes mellitus. J Prev Med Chin People’s Liberation Army. 2019;37(02):69–70+73.
29. Lu LY. Study on the influence of Diabetes Mellitus on the Occurrence and Development of Perianal Abscess. Shanghai University of Traditional Chinese Medicine; 2019.
30. Kuang WJ, Huang SZ, Mai LF. Impact of diabetes mellitus on treatment outcomes of anal fistula and perianal abscess. J Math Med. 2020;33(06):817–818.
31. Fan KF, Guo N, Yu TD, et al. Changes and significance of serum TGF-β, MMP-2, IL-17A, ACTA, and CRP levels in patients with diabetic perianal abscess before and after VSD treatment. J Clin Exp Med. 2022;21(21):2330–2334.
32. Yano T, Asano M, Matsuda Y, Kawakami K, Nakai K, Nonaka M. Prognostic factors for recurrence following the initial drainage of an anorectal abscess. Int J Colorectal Dis. 2010;25(12):1495–1498. doi:10.1007/s00384-010-1011-9
33. Jin YJ, Wang Y, Li AR, et al. Clinical characteristics of diabetic patients complicated with perianal abscess and their correlation with HbA1C, WBC, ACTA, and MMP-2. J Mol Diagn Ther. 2023;15(05):776–779.
34. Tang X, Li XY, He TH, et al. Advances in diagnosis and treatment of perianal abscess and anal fistula complicated with diabetes mellitus. J Pract Med. 2022;38(16):2100–2105.
35. Cruz TB, Carvalho FA, Matafome PN, et al. Mice with type 2 diabetes present significant alterations in their tissue biomechanical properties and histological features. Biomedi-Cines. 2021;10(1):57. doi:10.3390/biomedicines10010057
36. Wei PL, Keller JJ, Kuo LJ. Increased risk of diabetes following perianal abscess: a population-based follow-up study. Int J Colorectal Dis. 2013;28(2):235–240. doi:10.1007/s00384-012-1519-2
37. Sang MM, Wu TZ, Sun ZL. Pathogenesis and advances in clinical diagnosis and treatment of diabetes-related gastrointestinal symptoms. Chin J Diabetes. 2021;13(5):513–516.
38. Sigmon DF, Emmanuel B, Tuma F. Perianal Abscess. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
39. Huang XF. Correlation between serum magnesium concentration and insulin resistance in patients with PCOS. Int J Reprod Health / Plan. 2011;(5):416.
40. Amoroso C, Perillo F, Strati F, et al. The role of gut microbiota biomodulators on mucosal immunity and intestinal inflammation. Cells. 2020;9(5):1234. doi:10.3390/cells9051234
41. Ansaldo E, Farley TK, Belkaid Y. Control of Immunity by the Microbiota. Annu Rev Immunol. 2021;39:449–479. doi:10.1146/annurev-immunol-093019-112348
42. Alabbad J, Abdul Raheem F, Alkhalifa F, Hassan Y, Al-Banoun A. Alfouzan W. Retrospective clinical and microbiologic analysis of patients with anorectal abscess. Surg Infect. 2019;20(1):31–34. doi:10.1089/sur.2018.144
43. Sang YF, He HT. Analysis of pus pathogen examination and drug resistance in patients with T2DM complicated with perianal abscess. Shenzhen J Integr Tradit Chin West Med. 2023;33(04):104–106.
44. Li TH, Li X, Wang Y. Analysis of bacterial distribution and drug susceptibility results in pus from patients with perianal abscess and diabetes mellitus. J Pract Diabetol. 2021;17(1):12–13.
45. Liu CK, Liu CP, Leung CH, Sun FJ. Clinical and microbiological analysis of adult perianal abscess. J Microbiol Immunol Infect. 2011;44:204–208. doi:10.1016/j.jmii.2011.01.024
46. Liu S, Ge X, Xu X, Zhang K, Lu X. Alterations of gut microbiota in pyogenic liver abscess patients with and without type 2 diabetes mellitus. Infect Drug Resist. 2024;17:2149–2158. doi:10.2147/IDR.S456423
47. Yang XZ, Wang LH, Peng LP, et al. Research progress on elderly type 2 diabetes mellitus complicated with invasive pulmonary fungal disease. Chin J Geriatr. 2023;43(16):4087–4092.
48. Li XE, Hua CS, Tang QZ, et al. Distribution and influencing factors of vitamin D and vitamin K2 in hospitalized patients with type 2 diabetes mellitus. Chin J Clin Pathol. 2024;16(04):337–341.
49. Liu F. Analysis of risk factors for bloodstream infections and mortality caused by multidrug-resistant Klebsiella pneumoniae [dissertation]. Hubei University of Medicine; 2023.
50. Turner SV, Singh J. Perirectal Abscess. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
51. Liu Z, Huang G, Hou J, et al. Study on influencing factors of anal fistula formation after incision and drainage of perianal abscess. Mod Med Health Res. 2018;2(20):127–128.
52. Narayanan S, Althans AR, Reitz KM, et al. Drainage of anorectal abscesses in the operating room is associated with a decreased risk of abscess recurrence and fistula formation. Am J Surg. 2023;225(2):347–351. doi:10.1016/j.amjsurg.2022.09.005
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.