")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
The association between depression, anxiety and substance use among Canadian post-secondary students
Authors Esmaeelzadeh S, Moraros J, Thorpe L , Bird Y
Received 13 September 2018
Accepted for publication 6 November 2018
Published 23 November 2018 Volume 2018:14 Pages 3241—3251
DOI https://doi.org/10.2147/NDT.S187419
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Sarvenaz Esmaeelzadeh,1 John Moraros,1 Lilian Thorpe,2 Yelena Bird1
1School of Public Health, University of Saskatchewan, Saskatoon, SK, Canada; 2Community Health and Epidemiology, University of Saskatchewan, Saskatoon, SK, Canada
Purpose: This study aims to examine the association between depression, anxiety and substance use among Canadian post-secondary students.
Methods: This study used data from the spring 2016, American College Health Association – National College Health Assessment II (ACHA-NCHA II) survey. It includes 43,780 college students from 41 Canadian post-secondary institutions. The exposure variables of interest were alcohol, cannabis and tobacco use, and the outcome variables of interest were diagnosis or treatment for depression and/or anxiety. Descriptive statistics, univariate and multivariate logistic regression models were used to analyze our data.
Results: Our study found that 14.7% of post-secondary students were diagnosed or treated for depression and 18.4% for anxiety within the past 12 months. Among current (past 30 days) substance use, it was reported that alcohol (69.3%), cannabis (17.9%) and tobacco (11%) were the most common. There was a significant association between depression and current tobacco use (OR =1.36, 95% CI: 1.22–1.52, P<0.001) and current cannabis use (OR =1.17, 95% CI: 1.05–1.31, P<0.001). There was also a gender-specific association between anxiety and female alcohol users (OR =1.41, 95% CI: 1.24–1.62, P<0.001).
Conclusion: The results of this study found significant associations between depression, tobacco use and cannabis use, and anxiety and alcohol use among post-secondary students. These conditions should be screened concurrently for improved outcomes among this vulnerable population.
Keywords: depression, anxiety, alcohol, cannabis, tobacco, post-secondary students
Introduction
Depression, anxiety and substance use pose a major public health concern. These conditions contribute a significant portion of the world’s disease burden measured by disability-adjusted life years.1 The majority of depression, anxiety and substance use cases, often times, emerge during young adulthood, making post-secondary students a particularly vulnerable group.2 Early onset of co-occurrence may disrupt the course of cognitive and emotional development and may negatively impact a student’s life and well-being (ie, education, relationships, health and safety). Due to the lack of integrated health care services for co-occurring disorders, affected students are more likely to experience negative outcomes and become high-end users of health care resources.3
Young adulthood represents a critically important time as students transition from high school to post-secondary studies to pursue greater educational opportunities, develop personal relationships and achieve their career goals. Post-secondary education provides students with many opportunities and challenges for their personal development and growth. Among the challenges faced are increased independence and responsibility that may at times, lead to highly stressful situations.4 The competitive nature and pressurized academic environment of post-secondary education makes some students vulnerable to develop depression, anxiety and substance use problems either independently or concurrently.1 These conditions may affect their academic progress, personal development and professional life.5,6
Depression, anxiety and substance use are closely linked and represent a growing concern for many university campuses across Canada. A recent national survey of colleges and universities found that one in five Canadian post-secondary students are depressed and anxious (20%) and more students are reporting being in distress than 3 years ago.7,8 Similarly, the prevalence of current alcohol (83%), cannabis (30%) and tobacco (18%) use is highest among individuals aged 20–24 years, a large proportion of whom are post-secondary students.9 In addition, substance use is reported to lead to several adverse outcomes for students including poor academic performance,10 unintentional injuries11 and increased engagement in other risky behaviors.12,13
Post-secondary students suffering from concurrent disorders experience more serious medical, social and emotional problems.14 Affected individuals are often undiagnosed,2 refractory to treatments15 and require more extensive health care support.15,16 Depression, anxiety and substance use can co-occur due to a variety of reasons including: 1) common risk factors (such as biological factors or traumatic events);17,18 2) self-medication hypothesis (individuals already suffering from depression and anxiety may exhibit a maladaptive response and self-medicate by using substances to forget bad feelings, cope with problems and relieve the symptoms of their mental health disorder);19 3) substance use-induced mental health problems (individuals may develop depression and/or anxiety as a direct [ie, pharmacogenic] consequence of their substance use)17 and 4) substance use-related mental health problems (individuals may develop depression and/or anxiety as an indirect [ie, socioeconomic stressors, unemployment, dysfunctional relationships] consequences of their substance use).14,20 However, due to the multifactorial nature of this problem, it is not yet clear whether an independent association exists between depression, anxiety and substance use as the literature reports inconsistent findings.21–24
There has been considerable attention given to depression, anxiety and substance use among high school students;25–27 however, less is known about post-secondary students. Moreover, much of the published research examining the association between depression, anxiety and substance use has been conducted in countries other than Canada.28–31 Therefore, this study aims to examine the association between depression, anxiety and substance use among Canadian post-secondary students.
Materials and methods
Data and sample
This study used data from the American College Health Association – National College Health Assessment II (ACHA-NCHA II) – Canadian Reference Group survey, spring 2016. The population of interest in this national survey was post-secondary students. The 2016, ACHA-NCHA II survey consists of data from 43,780 students representing 41 Canadian post-secondary institutions. These institutions either surveyed all their students or used a representative random sampling method. The overall participation rate was 19.2%.7
Outcome variables
The outcome variables of interest in this study were history of depression and/or anxiety (yes/no). Respondents were specifically asked to indicate whether they had been diagnosed or treated by a medical professional for depression and/or anxiety within the past 12 months.
Exposure variables
Substance use was the primary exposure of interest and specifically, alcohol, cannabis and tobacco use. Responses were re-categorized as: never (never used the substance), former (used the substance but not within the past 30 days) and current users (used the substance within the past 30 days).
Sociodemographic and other variables
Sociodemographic and other variables were selected for inclusion in our study after review of the existing scientific literature.32–42 It is well-documented that mental health disorders are associated with the sociodemographic characteristics of an individual. Young adults between the ages of 18 and 24 years are reported to have the highest occurrence of mental health disorders than any other age group.32 Depression is more common among females, single or divorced individuals, ethnic minorities and those with alcohol or drug use disorders.33 Anxiety is more common among females, separated or divorced individuals, ethnic minorities and those with other mental health and substance use disorders.34 In addition, there are other factors that have been shown to be associated with the mental health status of post-secondary students. These factors include their study status (undergraduate or graduate), international student status (yes, no), enrollment status (part time or full-time), housing (living on or off-campus) and academic performance (grade point average [GPA]).35–42
In our study, the gender variable had three levels: male, female and non-binary (those who cannot describe themselves as solely male or female). Age groups were re-categorized as follows: 18–20, 21–23 and 24 years or older. Ethnicity was self-reported from the following question: Do you usually describe yourself as White, Black, Hispanic/Latino, Asian/Pacific Islander, American Indian/Alaskan Native/Native Hawaiian, Biracial/Multiracial or Other? Participants were also asked about their marital status: single, married, separated/divorced or other. In addition, there were questions that described the following: international student (yes/no), housing (live with their parents/on-campus/off-campus), enrollment status (full-time/part-time/other), study status (undergraduate/graduate/other) and GPA (A/B/C/D or F/not applicable).
Questions pertaining to other substance use included: cocaine, methamphetamine, sedatives, hallucinogens, opiates, inhalants, 3, 4-methylenedioxymethamphetamine (MDMA), and other club and illegal drugs. Participants were then re-categorized into three groups: never (never used any of the other substances), former (used but not within the past 30 days) and current users (used within the past 30 days). Questions pertaining to other mental health disorders (yes/no) were re-categorized based on participant’s response to the following questions: Have you been diagnosed or treated by a medical professional for any of the following mental health disorders: anorexia, attention-deficit hyperactivity disorder, bipolar disorder, bulimia, insomnia and schizophrenia within the past 12 months. If yes, the participant was coded as yes for the other mental health disorders variable.
Data analysis
Descriptive statistics for the exposure and outcome variables of interest and other co-variates were examined. Univariate analysis was conducted to assess the crude association of one explanatory variable at a time with the outcome variable of interest (depression or anxiety). During univariate analysis, variables with a significance level of <0.15 were screened and were included in the multivariate analysis. According to the literature, a significance level of <0.25 may be used as the cutoff point, when selecting variables for inclusion in multivariate analysis.43,44 In our study, the sample size was large and the probability of having statistically significant P-values high. Therefore, a more conservative significance level of <0.15 was used as our cutoff point to screen for variables.
Two separate multivariable logistic regression models were built using depression and anxiety as the outcomes of interest. Both models used substance use behavior (alcohol, cannabis and tobacco use) as the main exposures while controlling for demographic characteristics and other factors. Multicollinearity among independent variables was assessed using the variance inflation factor (<2.5 indicated no multicollinearity). Backward selection strategy was used to build the final models. The confounding effect of statistically insignificant variables was assessed before they were removed from the models. A change of 10% or more in the regression coefficient of the primary predictor suggested that the variable is a confounder. A cutoff point of 15%–20% is most commonly used in the literature.44 However, given our large sample size we used a more conservative cutoff point of 10% so that more potential confounders could be included. All potential two-way interactions were assessed using a level of significance of 0.05 (α=0.05). Akaike information criterion was used to estimate and compare the relative quality of our models. Model fitness was assessed using the Hosmer–Lemeshow goodness-of-fit test.43 Receiver operating characteristic (ROC)43 curve was used to check the ability of the two logistic regression models to predict the probability of depression and anxiety. All statistical analyses were computed using Statistical Analysis System (SAS) version 9.4.
Results
Descriptive statistics
Of the 43,780 post-secondary students, 14.7% were diagnosed or treated by a medical professional for depression and 18.4% for anxiety within the past 12 months. Among substance use, alcohol (69.3%), cannabis (17.9%) and tobacco use (11%) were most common in the past 30 days. The majority of participants were female (67.9%), White (70.7%), ages 18–20 years (40.3%), single (83%), undergraduate students (83.2%), domestic (90.6%), living off-campus (53.3%), studying full-time (93.3%) and with a GPA of B (45.1%). Among all participants, depression, anxiety and predictor variables had <2% missing data. Table 1 provides detailed descriptive statistics of the study population.
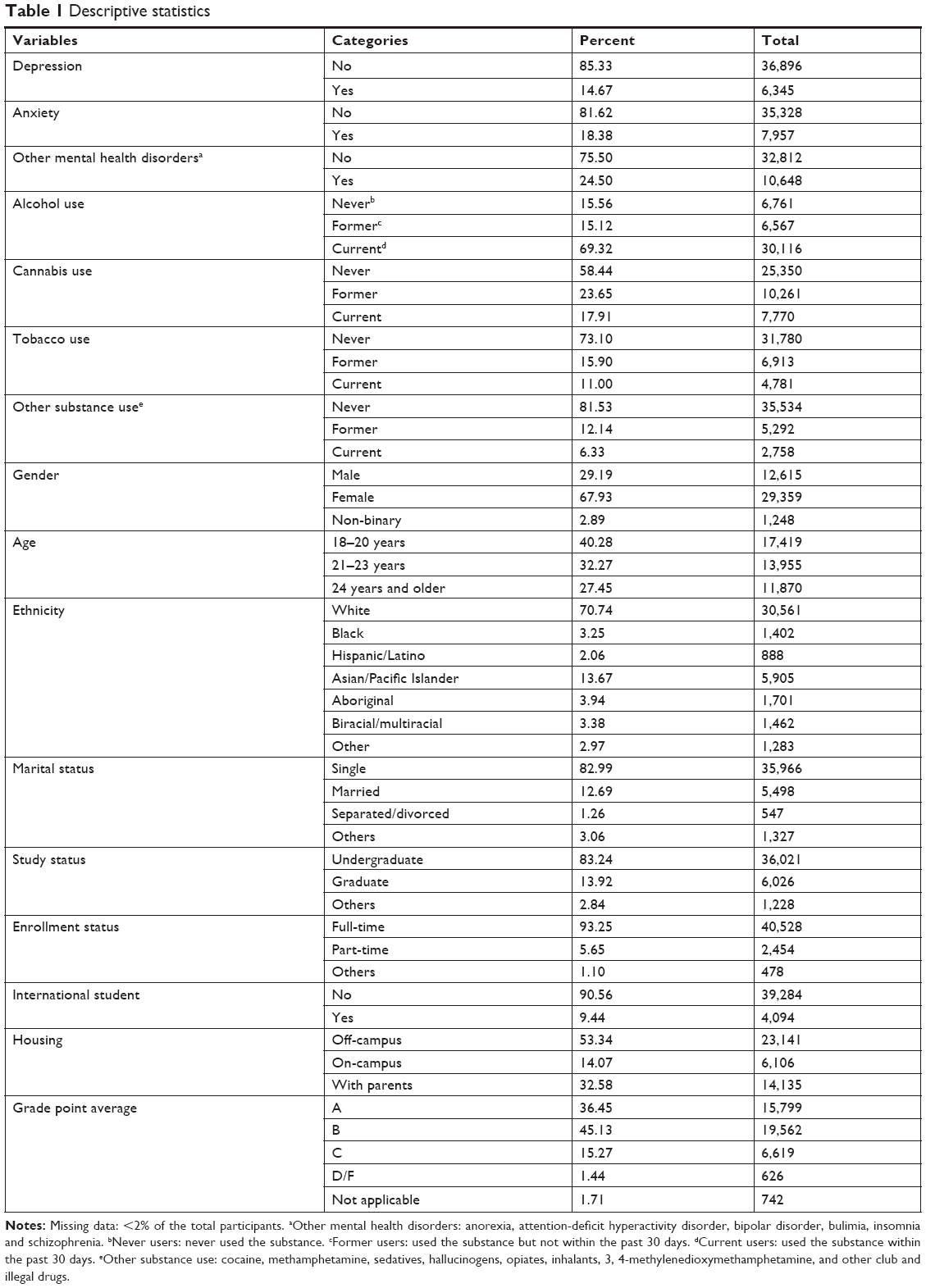 | Table 1 Descriptive statistics |
Univariate analysis
Participants reporting current (past 30 days) alcohol use were 1.74 (95% CI: 1.60–1.90) times more likely than those who never used alcohol to report depression. Participants reporting current cannabis use were 2.23 (95% CI: 2.08–2.38) times more likely than those who never used cannabis to report depression. Individuals reporting current tobacco use were 2.49 (95% CI: 2.31–2.68) times more likely than those who never used tobacco to report depression. When examining the unconditional association between substance use and anxiety, participants who were current alcohol users were 1.92 (95% CI: 1.77–2.08) times more likely to report anxiety compared with those who never used alcohol. Participants who were current cannabis users were 2.00 (95% CI: 1.88–2.13) times more likely to report anxiety compared with those who never used cannabis. Finally, participants who were current tobacco users were 2.04 (95% CI: 1.90–2.19) times more likely than those who never used tobacco to report anxiety. Table 2 summarizes the univariate analysis examining depression, anxiety, substance use and other risk factors.
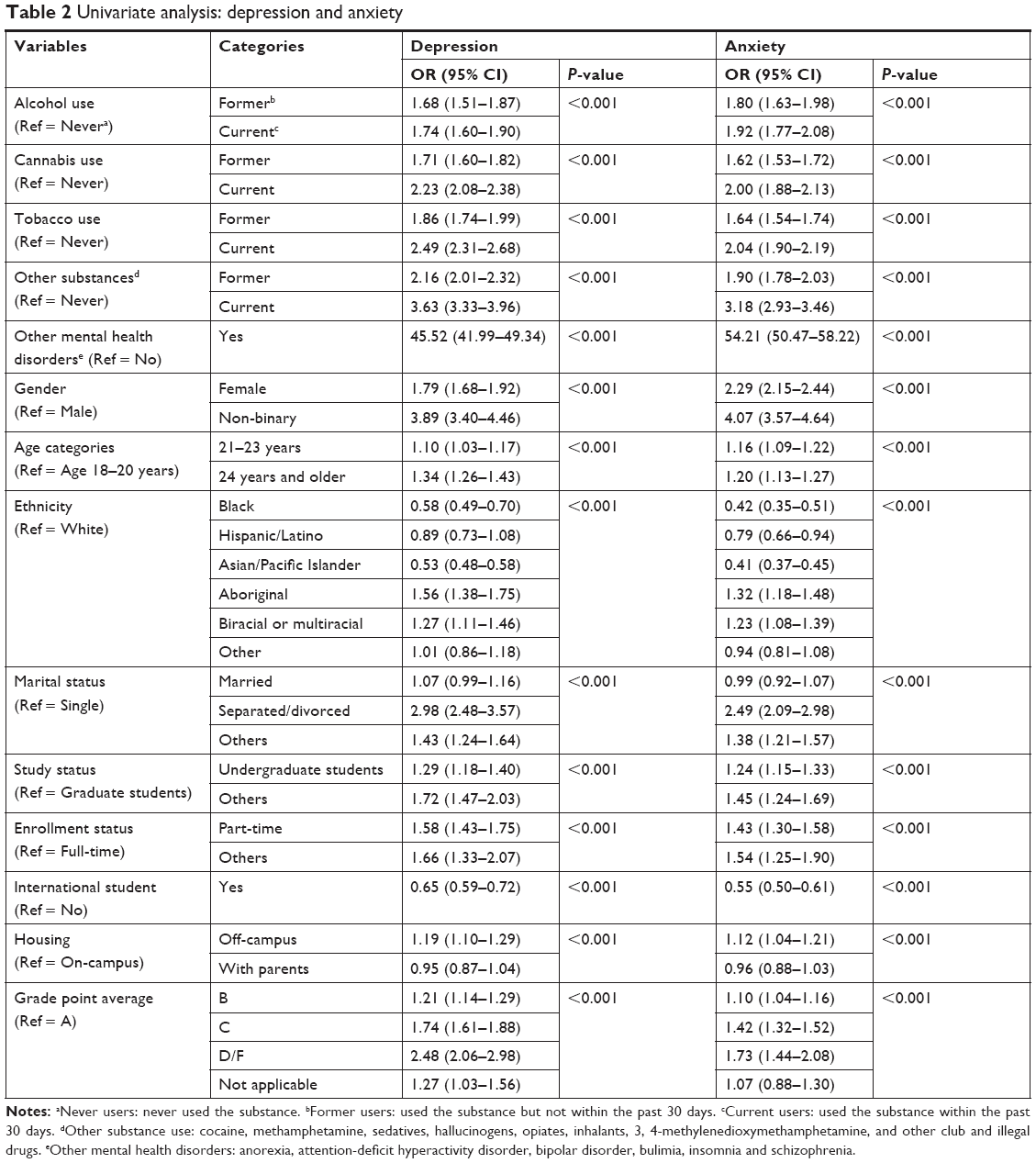 | Table 2 Univariate analysis: depression and anxiety |
Multivariate analysis
Model 1: Depression and substance use
An interaction effect was observed in our final model between cannabis use and other mental health disorders. Specifically, current cannabis users with (OR =1.17, 95% CI: 1.05–1.31) or without (OR =1.29, 95% CI: 1.05–1.57) other mental health disorders were more likely to have depression compared with never cannabis users (P-value 0.05). Former cannabis users without other mental health disorders were more likely to have depression (OR =1.38, 95% CI: 1.16–1.65) compared to never cannabis users (P-value 0.05). The odds of having depression were greater for current tobacco users (OR =1.36, 95% CI: 1.22–1.52) and to a lesser extent former tobacco users (OR =1.20, 95% CI: 1.09–1.33) compared to never tobacco users (P-value<0.001). In addition, the odds of having depression were significantly increased for the following groups: current and former users of other substances compared to never users of other substances; females and non-binary gendered individuals compared to males; participants ages 24 years and older compared to those ages 18–20 years; divorced compared to single students; part-time compared to full-time students; undergraduate compared to graduate students and individuals reporting a GPA of D or F compared to those with a GPA of A (P-value<0.001) (Table 3).
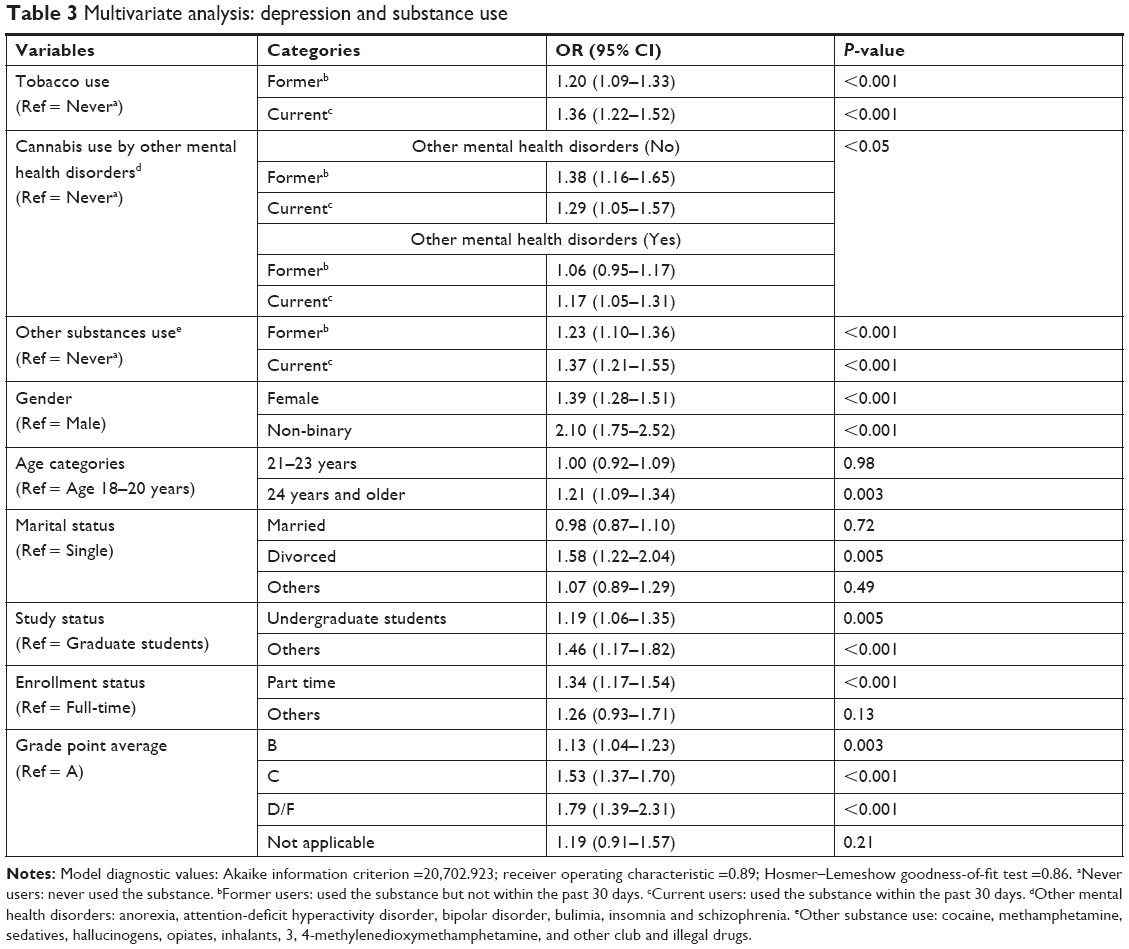 | Table 3 Multivariate analysis: depression and substance use |
Model 2: Anxiety and substance use
An interaction effect was observed in our final model between alcohol use and gender. Specifically, the odds of having anxiety were 41% greater for female current alcohol users (OR =1.41, 95% CI: 1.24–1.62) and 43% for former alcohol users (OR =1.43, 95% CI: 1.22–1.68) compared to female non-alcohol users (P-value<0.05). The odds of having been diagnosed with anxiety was increased for current users of other substances (OR =1.28, 95% CI: 1.14–1.45) compared to never users of other substances; students ages 21–23 years compared to those ages 18–20 years old (OR =1.18, 95% CI: 1.08–1.28); part time (OR =1.23, 95% CI: 1.07–1.42) compared to full-time students; students with GPA of A (OR =0.91, 95% CI: 0.84–0.99) compared to students with GPA of B and for those students with other mental health disorders (OR =50.77, 95% CI: 47.10–54.72) compared to those without other mental health disorders (P-value<0.001). In addition, the odds of having been diagnosed with anxiety were decreased among Black (OR =0.59, 95% CI: 0.46–0.75) and Asian or Pacific Islander (OR =0.59, 95% CI: 0.52–0.67) students compared to White students (P-value<0.001); married students (OR =0.86, 95% CI: 0.77–0.96) compared to single students; and domestic students (OR =1.32, 95% CI: 1.15–1.53) compared to international students (Table 4).
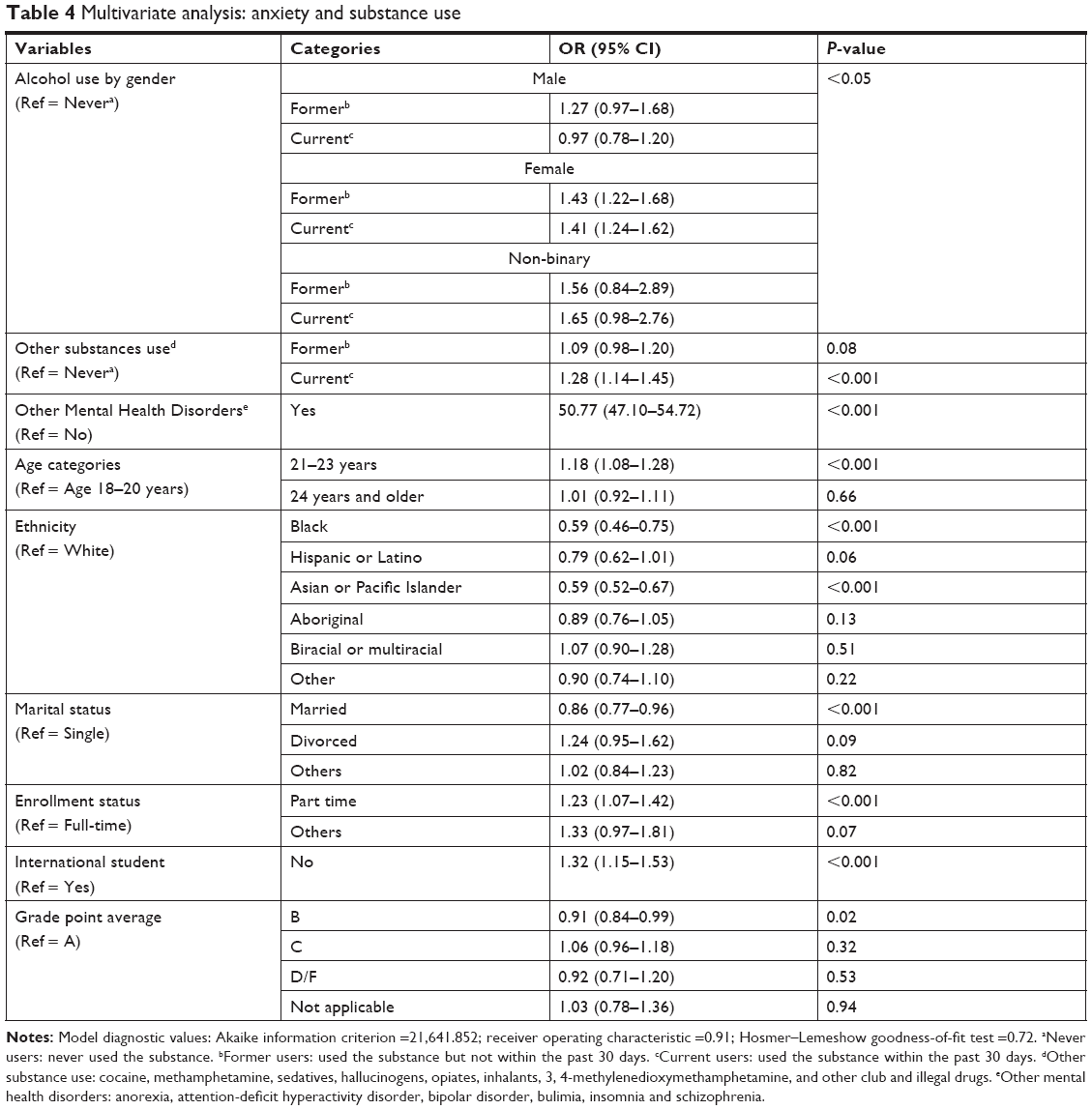 | Table 4 Multivariate analysis: anxiety and substance use |
Model fit and predicted probability
The final models for depression and anxiety with the interaction terms showed a good fit to the data, when examined by using the Hosmer–Lemeshow goodness-of-fit test (P-value=0.86 and P-value=0.72, respectively). The predicted probability of the final models by the area under the receiver operating characteristic curve was 0.89 (depression) and 0.91 (anxiety) and thus, the prediction ability of the models is said to be satisfactory.
Discussion
Our study is among the first to examine the association between depression, anxiety and substance use among post-secondary students in Canada. Specifically, we found a higher rate of depression and anxiety (14.7% and 18.4%) among post-secondary students in 2016 compared to 2013 (10.0% and 12.3%).8 In addition, we observed a small increase in alcohol (83.6% in 2013 to 84.4% in 2016) and cannabis use (39.9% in 2013 to 41.6% in 2016).8 Encouragingly, there was a decrease in tobacco use (29.2% in 2013 to 26.9% in 2016).8 Overall, substance use remains a serious public health concern and is highly prevalent among Canadian post-secondary students.
Depression and alcohol use were significantly associated in our univariate analysis. However, in our final logistic regression model, depression was not significantly associated with alcohol use. This provides evidence in support of previous studies, which did not find an association between depression and alcohol use among post-secondary students.24,45 However, other studies contradict our finding but were mainly focused in scope to the adolescent student population.46,47 Age may play a critical role in this association as the harmful effects of alcohol use and/or depression may differentially impact adolescents (high school students) compared to young adults (post-secondary students).48,49 Evidence suggests that underage alcohol use is associated with neurodegeneration,50 changes in functional brain activity51 and neurocognitive impairments,49 leading to the development of mental health disorders such as depression.48
Depression was significantly associated with an interaction between cannabis use and other mental health disorders. Our findings are, in part, supported by those reported in previous studies, which found a significant correlation between cannabis use and depression.45,52 However, these studies did not test for the same joint effect of cannabis and other mental health disorders on depression. Therefore, other mental health disorders could be important a priori predictors that need to be taken into consideration in our efforts to identify vulnerable and previously understudied subgroups, who may be more (or less) likely to develop depression.
In general, studies have shown that the association between depression and cannabis use could be attributed to direct and/or indirect factors. Direct factors linking depression and cannabis use include having a genetic predisposition to both conditions53 and biological mechanisms54 altering neurochemical activities in the brain.55 Indirect factors such as a student’s maladaptive cognitive skills and coping mechanisms (such as their own perceptions, social relationships and coping with undesirable life events) may also lead them to suffer from the co-occurrence of depression and cannabis use.56
Our results revealed a significant association between depression and tobacco use. This finding is consistent with previous studies that suggest an association exists between depression and current smoking among post-secondary students.45,52 In our study, both current and former smokers were more likely to be diagnosed with depression compared to never smokers. However, there was no statistically significant difference between current and former smokers. This is an important finding as it suggests that former smokers are also at risk to suffer from depression. There may be a biological explanation for this finding. Smoking initially increases the release of dopamine neurotransmitters, which eventually may cause the receptors to become insensitive and therefore, over time may require an increased stimulation to have the same affect.57 Upon smoking cessation, due to the deprivation of dopamine and the occurrence of withdrawal symptoms, the depressive symptoms may develop.57 Thus, health care providers at post-secondary institutions should be made aware of the risk of depression not only among current but also former smokers.
Anxiety was associated with a significant interaction between alcohol use and gender. Females who used alcohol (current and former users) were at an increased risk of self-reported anxiety compared to males. This is in accordance with a previous study that found a stronger association between anxiety and alcohol use among females compared to males.58 Anxiety among male and non-binary participants was not significantly associated with alcohol use. These findings help highlight that in order to improve mental health disorders and substance use outcomes among post-secondary students, interventions need to be population specific, sensitive, relatable and account for the different risk profiles among the genders.
Strengths and limitations
This study has several strengths. It used a recent dataset with a large, nationally representative sample size. The survey instrument is robust, reliable and valid. It investigated the characteristics and risk factors of two of the most common mental health disorders (depression and anxiety) and three most common substance use (alcohol, cannabis and tobacco). Finally, it is one of a few studies to examine these associations among post-secondary students in Canada. Our study also has a few limitations. The ACHA-NCHA II, spring 2016, survey is drawn from a convenience sample and its results may not be entirely generalizable. The survey questions regarding substance use focused on frequency but no information on initiation or duration were provided. The survey questions regarding depression, anxiety and substance use were self-reported and due to their private and sensitive nature and possible association with social stigma and discrimination, there may be some degree of underreporting by the participants. However, previous studies have shown that the use of self-reports for risky health behaviors are accurate and valid.59 Finally, our study is cross-sectional in design and therefore, it permits us to report on possible associations but it is unable to determine directionality or causal relationships between depression, anxiety and substance use. Further research with longitudinal studies is warranted.
Conclusion
This study examined the association between depression, anxiety and substance use among post-secondary students in Canada. A significant association was found between depression, tobacco use and cannabis use and a gender-specific association between anxiety and female alcohol users. These conditions should be screened concurrently for improved outcomes among this vulnerable population. Interventions that increase awareness and help fight the growing perception of substance use as a normalized and accepted behavior among post-secondary students may help address issues related to their depression and anxiety. The results of this study can be used to help inform university student health services, administrators and health care professionals in their efforts to design and implement comprehensive interventions, appropriate policies and effective health promotion strategies.
Ethics statement
The opinions, findings, and conclusions presented/reported in this article are those of the authors and are in no way meant to represent the corporate opinions, views, or policies of the American College Health Association (ACHA). ACHA does not warrant nor assume any liability or responsibility for the accuracy, completeness or usefulness of any information presented in this article. This study is exempt from ethics approval because it relies on the use of ACHA micro-files and secondary analysis of anonymous data (Tri-Council Policy Statement, articles 2.2 and 2.4, respectively). Participation in this survey was voluntary.
Acknowledgments
We gratefully acknowledge the support of Ms Rita Hanoski, Health Education and Promotion Coordinator and Ms Jocelyn Orb, Manager, Student Health Services, University of Saskatchewan. This research was supported, in part, by an internal grant from the School of Public of Public Health, University of Saskatchewan.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Pedrelli P, Nyer M, Yeung A, Zulauf C, Wilens T. College students: mental health problems and treatment considerations. Acad Psychiatry. 2015;39(5):503–511. | ||
Auerbach RP, Alonso J, Axinn WG, et al. Mental disorders among college students in the World Health Organization World Mental Health Surveys. Psychol Med. 2016;46(14):2955–2970. | ||
Breslau J, Lane M, Sampson N, Kessler RC. Mental disorders and subsequent educational attainment in a US national sample. J Psychiatr Res. 2008;42(9):708–716. | ||
Parker JDA, Summerfeldt LJ, Hogan MJ, Majeski SA. Emotional intelligence and academic success: examining the transition from high school to university. Pers Individ Dif. 2004;36(1):163–172. | ||
Eisenberg D, Golberstein E, Hunt JB. Mental health and academic success in college. B E J Econom Anal Policy. 2009;9(1):40. | ||
Dusselier L, Dunn B, Wang Y, Shelley MC 2nd, Whalen DF. Personal, health, academic, and environmental predictors of stress for residence hall students. J Am Coll Health. 2005;54(1):15–24. | ||
American College Health Association. American College Health Association-National College Health Assessment II: Canadian Reference Group Executive Summary Spring 2016; 2016. Available from: https://www.acha.org/documents/ncha/NCHA-II%20SPRING%202016%20CANADIAN%20REFERENCE%20GROUP%20EXECUTIVE%20SUMMARY.pdf. Accessed September 9, 2018. | ||
American College Health Association. American College Health Association-National College Health Assessment II: Canadian Consortium Reference Group Executive Summary Spring 2013; 2013. Available from: https://uwaterloo.ca/institutional-analysis-planning/sites/ca.institutional-analysis-planning/files/uploads/files/ncha-ii_spring_2013_canadian_reference_group_executive_summary.pdf. Accessed September 9, 2018. | ||
Health Canada [webpage on the Internet]. Canadian tobacco alcohol and drugs (CTADS): 2015 summary; 2017. Government of Canada. Available from: https://www.canada.ca/en/health-canada/services/canadian-tobacco-alcohol-drugs-survey/2015-summary.html. Accessed September 9, 2018. | ||
Brook JS, Adams RE, Balka EB, Johnson E. Early adolescent marijuana use: risks for the transition to young adulthood. Psychol Med. 2002;32(1):79–91. | ||
Hingson RW, Zha W. Age of drinking onset, alcohol use disorders, frequent heavy drinking, and unintentionally injuring oneself and others after drinking. Pediatrics. 2009;123(6):1477–1484. | ||
Li D, Yang X, Ge Z, et al. Cigarette smoking and risk of completed suicide: a meta-analysis of prospective cohort studies. J Psychiatr Res. 2012;46(10):1257–1266. | ||
Baskin-Sommers A, Sommers I. The co-occurrence of substance use and high-risk behaviors. J Adolesc Health. 2006;38(5):609–611. | ||
Canadian Centre on Substance abuse. Substance abuse in Canada: concurrent disorders; 2009. Available from: http://www.ccsa.ca/Resource%20Library/ccsa-011811-2010.pdf. Accessed September 9, 2018. | ||
Sheehan MF. Dual diagnosis. Psychiatr Q. 1993;64(2):107–134. | ||
Torrens M, Rossi PC, Martinez-Riera R, Martinez-Sanvisens D, Bulbena A. Psychiatric co-morbidity and substance use disorders: treatment in parallel systems or in one integrated system? Subst Use Misuse. 2012;47(8–9):1005–1014. | ||
Quello SB, Brady KT, Sonne SC. Mood disorders and substance use disorder: a complex comorbidity. Sci Pract Perspect. 2005;3(1):13–21. | ||
Kilpatrick DG, Ruggiero KJ, Acierno R, Saunders BE, Resnick HS, Best CL. Violence and risk of PTSD, major depression, substance abuse/dependence, and comorbidity: results from the National Survey of Adolescents. J Consult Clin Psychol. 2003;71(4):692–700. | ||
Khantzian EJ. The self-medication hypothesis of substance use disorders: a reconsideration and recent applications. Harv Rev Psychiatry. 1997;4(5):231–244. | ||
Kendler KS, Prescott CA, Myers J, Neale MC. The structure of genetic and environmental risk factors for common psychiatric and substance use disorders in men and women. Arch Gen Psychiatry. 2003;60(9):929–937. | ||
O’Loughlin J, O’Loughlin EK, Wellman RJ, et al. Predictors of cigarette smoking initiation in early, middle, and late adolescence. J Adolesc Health. 2017;61(3):363–370. | ||
Georgiades K, Boyle MH. Adolescent tobacco and cannabis use: young adult outcomes from the Ontario Child Health Study. J Child Psychol Psychiatry. 2007;48(7):724–731. | ||
Villarosa MC, Madson MB, Zeigler-Hill V, Noble JJ, Mohn RS. Social anxiety symptoms and drinking behaviors among college students: the mediating effects of drinking motives. Psychol Addict Behav. 2014;28(3):710–718. | ||
Weitzman ER. Poor mental health, depression, and associations with alcohol consumption, harm, and abuse in a national sample of young adults in college. J Nerv Ment Dis. 2004;192(4):269–277. | ||
Rasic D, Weerasinghe S, Asbridge M, Langille DB. Longitudinal associations of cannabis and illicit drug use with depression, suicidal ideation and suicidal attempts among Nova Scotia high school students. Drug Alcohol Depend. 2013;129(1–2):49–53. | ||
Simantov E, Schoen C, Klein JD. Health-compromising behaviors: why do adolescents smoke or drink? Identifying underlying risk and protective factors. Arch Pediatr Adolesc Med. 2000;154(10):1025–1033. | ||
Kubik MY, Lytle LA, Birnbaum AS, Murray DM, Perry CL. Prevalence and correlates of depressive symptoms in young adolescents. Am J Health Behav. 2003;27(5):546–553. | ||
Chung SS, Joung KH. Risk factors for current smoking among American and South Korean adolescents, 2005–2011. J Nurs Scholarsh. 2014;46(6):408–415. | ||
Pedersen W. Does cannabis use lead to depression and suicidal behaviours? A population-based longitudinal study. Acta Psychiatr Scand. 2008;118(5):395–403. | ||
Manrique-Garcia E, Zammit S, Dalman C, Hemmingsson T, Allebeck P. Cannabis use and depression: a longitudinal study of a national cohort of Swedish conscripts. BMC Psychiatry. 2012;12:112. | ||
Mangerud WL, Bjerkeset O, Holmen TL, Lydersen S, Indredavik MS. Smoking, alcohol consumption, and drug use among adolescents with psychiatric disorders compared with a population based sample. J Adolesc. 2014;37(7):1189–1199. | ||
Kessler RC, Amminger GP, Aguilar-Gaxiola S, Alonso J, Lee S, Ustün TB. Age of onset of mental disorders: a review of recent literature. Curr Opin Psychiatry. 2007;20(4):359–364. | ||
Sadock BJ, Sadock VA, Ruiz P. Kaplan and Sadock’s Concise Textbook of Clinical Psychiatry. 4th ed. Philadelphia: Wolters Kluwer; 2016. | ||
Martin P. The epidemiology of anxiety disorders: a review. Dialogues Clin Neurosci. 2003;5(3):281–298. | ||
Farrer LM, Gulliver A, Bennett K, Fassnacht DB, Griffiths KM. Demographic and psychosocial predictors of major depression and generalised anxiety disorder in Australian university students. BMC Psychiatry. 2016;16:241. | ||
Forbes-Mewett H, Sawyer A-M. Mental health issues amongst International students in Australia: perspectives from professionals at the coal-face in the Australian sociological association conference local lives/global networks. New South Wales: University of Newcastle; 2011. | ||
Oswalt SB, Riddock CC. What to do about being overwhelmed: graduate students, stress, and university services. Coll Stud Aff J. 2007;27(1):24–44. | ||
Kausar R. Perceived stress, academic workloads, and use of coping strategies by university students. J Behav Sci. 2010;20(1):31–34. | ||
Wyatt T, Oswalt SB. Comparing mental health issues among undergraduate and graduate students. Am J Health Educ. 2013;44(2):96–107. | ||
Beiter R, Nash R, McCrady M, et al. The prevalence and correlates of depression, anxiety, and stress in a sample of college students. J Affect Disord. 2015;173:90–96. | ||
Andrews B, Wilding JM. The relation of depression and anxiety to life-stress and achievement in students. Br J Psychol. 2004;95(Pt 4):509–521. | ||
Haines ME, Kashy DA, Norris MP. The effects of depressed mood on academic performance in college students. J Coll Stud Dev. 1996;37(5):219–226. | ||
Hosmer DW, Lemeshow S, Sturdivant RX. Applied Logistic Regression. 3rd ed. Hoboken, NJ: John Wiley and Sons, Inc; 2013. | ||
Bursac Z, Gauss CH, Williams DK, Hosmer DW. Purposeful selection of variables in logistic regression. Source Code Biol Med. 2008;3:17. | ||
Roberts SJ, Glod CA, Kim R, Hounchell J. Relationships between aggression, depression, and alcohol, tobacco: implications for healthcare providers in student health. J Am Acad Nurse Pract. 2010;22(7):369–375. | ||
Richter L, Pugh BS, Peters EA, Vaughan RD, Foster SE. Underage drinking: prevalence and correlates of risky drinking measures among youth aged 12–20. Am J Drug Alcohol Abuse. 2016;42(4):385–394. | ||
Naicker K, Galambos NL, Zeng Y, Senthilselvan A, Colman I. Social, demographic, and health outcomes in the 10 years following adolescent depression. J Adolesc Health. 2013;52(5):533–538. | ||
Zeigler DW, Wang CC, Yoast RA, et al. The neurocognitive effects of alcohol on adolescents and college students. Prev Med. 2005;40(1):23–32. | ||
Pedrelli P, Shapero B, Archibald A, Dale C. Alcohol use and depression during adolescence and young adulthood: a summary and interpretation of mixed findings. Curr Addict Rep. 2016;3(1):91–97. | ||
Crews FT, Braun CJ, Hoplight B, Switzer RC 3rd, Knapp DJ. Binge ethanol consumption causes differential brain damage in young adolescent rats compared with adult rats. Alcohol Clin Exp Res. 2000;24(11):1712–1723. | ||
Arango V, Underwood MD, Mann JJ. Fewer pigmented neurons in the locus coeruleus of uncomplicated alcoholics. Brain Res. 1994;650(1):1–8. | ||
Lee Ridner S, Staten RR, Danner FW. Smoking and depressive symptoms in a college population. J Sch Nurs. 2005;21(4):229–235. | ||
Otten R, Engels RC. Testing bidirectional effects between cannabis use and depressive symptoms: moderation by the serotonin transporter gene. Addict Biol. 2013;18(5):826–835. | ||
Ronan PJ, Wongngamnit N, Beresford TP. Molecular mechanisms of cannabis signaling in the brain. Prog Mol Biol Transl Sci. 2016;137:123–147. | ||
Degenhardt L, Hall W, Lynskey M. Exploring the association between cannabis use and depression. Addiction. 2003;98(11):1493–1504. | ||
McLaren J, Lemon J, Robins L, Mattick RP. Cannabis and mental health: Put into context. National drug strategy; 2008. Available from: http://www.nationaldrugstrategy.gov.au/internet/drugstrategy/Publishing.nsf/content/mono68-toc. Accessed September 9, 2018. | ||
Quattrocki E, Baird A, Yurgelun-Todd D. Biological aspects of the link between smoking and depression. Harv Rev Psychiatry. 2000;8(3):99–110. | ||
Wu P, Goodwin RD, Fuller C, et al. The relationship between anxiety disorders and substance use among adolescents in the community: specificity and gender differences. J Youth Adolesc. 2010;39(2):177–188. | ||
Jackson CT, Covell NH, Frisman LK, Essock SM. Validity of self-reported drug use among people with co-occurring mental health and substance use disorders. J Dual Diagn. 2005;1(1):49–63. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.