Back to Journals » Journal of Inflammation Research » Volume 14
The Association Among Serum Growth Differentiation Factor 15 Level and Suicidal Ideation is Dependent on Testosterone Deficiency in Depressive Patients
Authors Peng R, Li D, Mei SQ, Li Y
Received 28 March 2021
Accepted for publication 2 June 2021
Published 24 June 2021 Volume 2021:14 Pages 2723—2730
DOI https://doi.org/10.2147/JIR.S313200
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Rui Peng, Di Li, Si-Qing Mei, Yan Li
Department of Clinical Laboratory, Renmin Hospital of Wuhan University, Wuhan, Hubei Province, 430060, People’s Republic of China
Correspondence: Yan Li
Department of Clinical Laboratory, Renmin Hospital of Wuhan University, 238 Jiefang Road, Wuhan, People’s Republic of China
Tel +86 27 88071553
Email [email protected]
Background: Elevated levels of growth differentiation factor (GDF)-15 and reduced levels of testosterone have been linked to depressive disorder, but whether they are also linked to suicidal ideation in patients with depression is unclear.
Methods: This retrospective study involved 301 patients ≥ 22 years old hospitalized for depression between July 2018 and November 2020 at Renmin Hospital of Wuhan University, of whom 120 had suicidal ideation. Serum levels of GDF-15 and testosterone were compared between patients with or without suicidal ideation.
Results: GDF-15 levels were significantly higher among patients with suicidal ideation than among those without, regardless of whether testosterone levels were above or below the median of 314 ng/dL. In multivariate logistic regression involving all patients, serum GDF-15 level was associated with low testosterone level (P=0.001). Among patients with testosterone < 314 ng/dL, an increase of 1 standard deviation in serum GDF-15 level translated to a 1.3-fold increase in the risk of suicidal ideation (P=0.007). This relationship was not observed in all population or patients with testosterone levels ≥ 314 ng/dL.
Conclusion: High serum GDF-15 level may be associated with an increased risk of suicidal ideation in patients with depression, and this association appears to be partly mediated by low testosterone levels.
Keywords: growth differentiation factor-15, testosterone, suicidal ideation, major depressive disorder
Introduction
Major depressive disorder (MDD) is a common mental illness that negatively affects daily living of people globally, and it is a leading cause of disability worldwide.1 MDD is associated with high healthcare costs, resulting in economic burden on patients and their families.2 Considering the economic burden and disability caused by depression, identification of MDD-related biomarkers might guide early diagnosis or targets for the treatment of MDD. Suicide-related event in patients with MDD is a leading cause of death in adolescents worldwide. Epidemiologic observations indicate that nearly 20% of adolescents with MDD consider suicide, more than 15% have formulated plans for suicide, and nearly 10% attempt suicide annually.3 Furthermore, it is well known that psychological, somatic, and psychosocial sequelae are the risk factors for suicidal ideation.4
While the etiology and mechanism of MDD are unclear, it may involve dysregulation of neurotransmitters, dysfunction of the hypothalamic-pituitary-thyroid axis, and inflammatory responses.5 Patients with long-term MDD have high levels of the peripheral inflammatory markers interleukin-6, tumor necrosis factor-alpha and C-reactive protein (CRP).6,7 A useful inflammatory biomarker for MDD might be growth differentiation factor-15 (GDF-15), a well-known inflammatory cytokine that has been associated with several diseases, including major bleeding, mortality, stroke, and diabetes.8–10 GDF-15 is associated with neuroinflammation in a mouse model of Parkinson’s disease, and its deficiency compromises dopaminergic neuron survival and microglial response.11 Serum GDF-15 levels are significantly increased in patients with depression who have suffered acute ischemic stroke.12 In view of this association, we speculated that GDF-15 may be a useful inflammatory biomarker for MDD.
In addition, MDD affects male and female differently. In fact, low testosterone is associated with higher risk of MDD.13,14 Interestingly, levels of GDF-15 may correlate with levels of testosterone: in cancer cells, testosterone directly regulates the expression of GDF-15.15,16 If this link also exists in depression, it may affect clinical manifestations of the disorder, since low testosterone levels are associated with greater risk of suicidal behavior among men with MDD.17 Thus, the present study explored whether levels of GDF-15 and testosterone are associated with suicidal ideation among men with depression.
Methods
Patients
This was a retrospective clinical study involving 301 men with MDD at least 22 years old who were hospitalized in the Department of Psychiatry at Renmin Hospital of Wuhan University between July 2018 and November 2020. All patients underwent Structured Clinical Interview for DSM-IV (SCID), Hamilton Depression Rating Scale (HDRS) and the Beck’s Suicidal Ideation Scale (SSI). Suicidal ideation was defined as a conscious intent of the depressive subjects to end their life; however, ambivalent, through means that the patient thought could lead to death. To be included, patients had to be diagnosed with MDD with symptoms of depression for at least 4 weeks prior to the study. Patients were excluded if they reported using illegal drugs, or substance abuse during the preceding 3 months. Patients were also excluded if they had a history of heart disease, kidney or inflammatory disease; any infection; current cancer; or major somatic disorders. Ethics approval was obtained from the Medical Ethics Review Committee of Renmin Hospital of Wuhan University. The clinical trial registration number is 20200988. Patients, at the time of admission, provided written consent for their anonymized medical data to be analyzed and published for research purposes. This study was also conducted in accordance with the Declaration of Helsinki.
Data Collection
Data were collected at the time of hospitalization on sociodemographic information (age, sex), lifestyle and health factors [current smoking and packs of cigarettes smoked per week, current alcohol consumption and quantity of alcohol consumed, and body mass index (BMI)], and clinical characteristics (duration of depression and antidepressant use). Smoking and alcohol use were evaluated by asking the subjects whether they smoked or drank, and if they did, they were asked to show the numbers of cigarettes smoked or drinking in present. BMI was evaluated by measuring the weight and height of both individuals on the same scale and calculated by dividing weight (in kilograms) by the square of height (in meters).
Blood Sampling and Assays
Patients were sampled after admission. They had to have been free of antidepressants or antipsychotic agents for at least one week prior to blood sampling, since these drugs can alter cytokine levels in serum.
Blood samples were drawn at 8 a.m. after overnight fasting. Samples were centrifuged, and the serum was stored at −70°C until assay. GDF-15 levels were measured using a commercial enzyme-linked immunosorbent assay kit (CusaBio, Wuhan, China). The manufacturer-specified detection range was 9.6–500 ng/mL GDF-15. All serum samples were diluted 10-fold before assay. Coefficients of variation for intra- and inter-assay reproducibility were, respectively, <8.0% and <10.0%.
Blood samples were also assayed for the following routine parameters using an Advia Centaur CP system (Siemens): total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-c), low-density lipoprotein cholesterol (LDL-c), Lipoprotein-a (Lp(a)), high-sensitivity C-reactive protein (hs-CRP), free thyroxine (FT4), free triiodothyronine (FT3), thyroid-stimulating hormone (TSH), and testosterone.
Statistical Analyses
Statistical analyses were performed using SPSS 20.0 (IBM, Chicago, IL, USA). Statistical tests were two-tailed, and P < 0.05 was defined as significant. Categorical data were shown as numbers (percentages), and continuous variables were shown as medians [inter-quartile range (IQR)]. Patients with or without suicidal ideation were categorized into groups of low testosterone or high testosterone, based on whether they had <314 or ≥314 ng/dL, which was the median testosterone levels observed in this study. Differences among the four groups were analyzed using the χ2 test or Mann–Whitney U-test. Spearman correlation was performed to analyze associations of GDF-15 levels with other biochemical factors, and multiple stepwise regression was carried out to identify factors associated with serum GDF-15 levels. Logistic regression was used to identify predictors of decreased testosterone levels. Associations between a change in serum level of GDF-15 [per 1 standard deviation (SD)] and suicidal ideation were explored using logistic regression.
Results
Patient Characteristics
A total of 301 male patients with depression with a median age of 43 years (IQR 22 to 65 years) were included. MDD patients with suicidal ideation (39.87%) were compared with patients without suicidal ideations. Irrespective of testosterone levels, patients with suicidal ideation had significantly higher levels of TG, hsCRP and FT4, longer depressive duration, and a higher usage of antidepressants compared to those without suicidal ideation (Table 1). The median GDF-15 level in serum was 112.01 (11.63–376.46) ng/mL across all patients, and it was significantly lower among those without suicidal ideation (90.16 ng/mL, IQR 11.63–253.04 ng/mL) than among those with suicidal ideation (132.49 ng/mL, IQR 32.07–376.46 ng/mL; Figure 1).
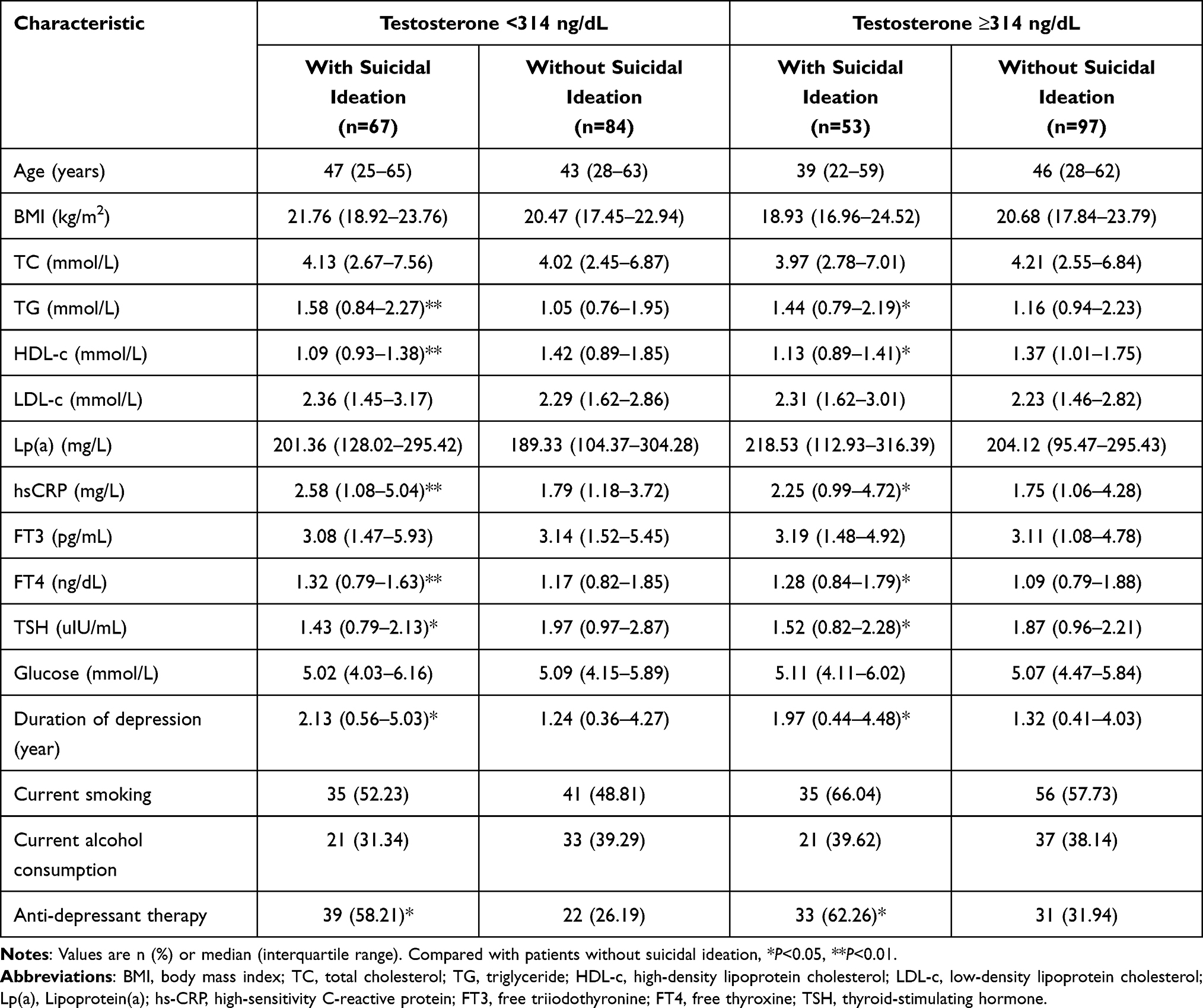 |
Table 1 Patient Characteristics |
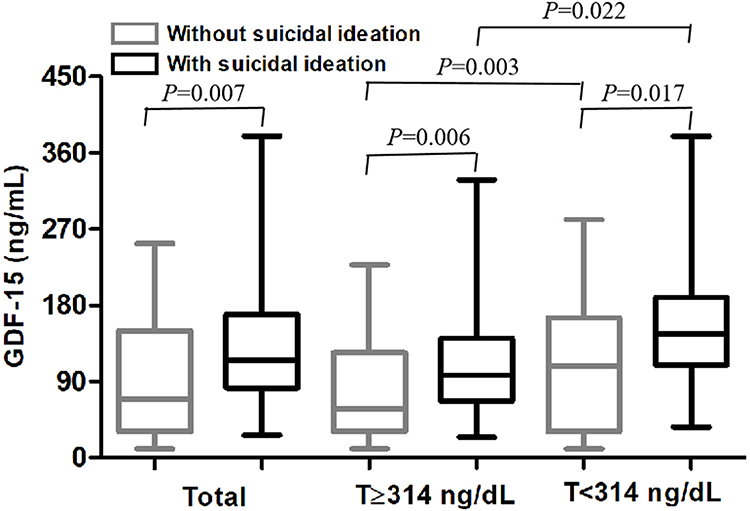 |
Figure 1 Tukey plot comparing serum GDF-15 levels between patients with or without suicidal ideation. Abbreviations: GDF-15, growth differentiation factor (GDF)-15; T, testosterone. |
Comparison of Serum GDF-15 Levels Between Those with Low or High Testosterone
The subgroup of patients with high testosterone, defined as levels ≥314 ng/dL, had a median testosterone GDF-14 level of 129.41 ng/mL (IQR 27.59–376.46 ng/mL), significantly higher than the median of 95.22 ng/mL (IQR 11.63–316.92 ng/mL) among patients with low testosterone. In both the low- and high-testosterone subgroups, GDF-15 levels were significantly lower among subjects without suicidal ideation than among those with ideation.
Univariate logistic regression showed that serum TG, HDL-c, hsCRP, FT3, TSH, and GDF-15 levels were related to low testosterone levels in patients with depression (Table 2). Multivariate logistic regression identified serum HDL-c, TSH, and GDF-15 levels as independent predictors of low testosterone levels (Table 2).
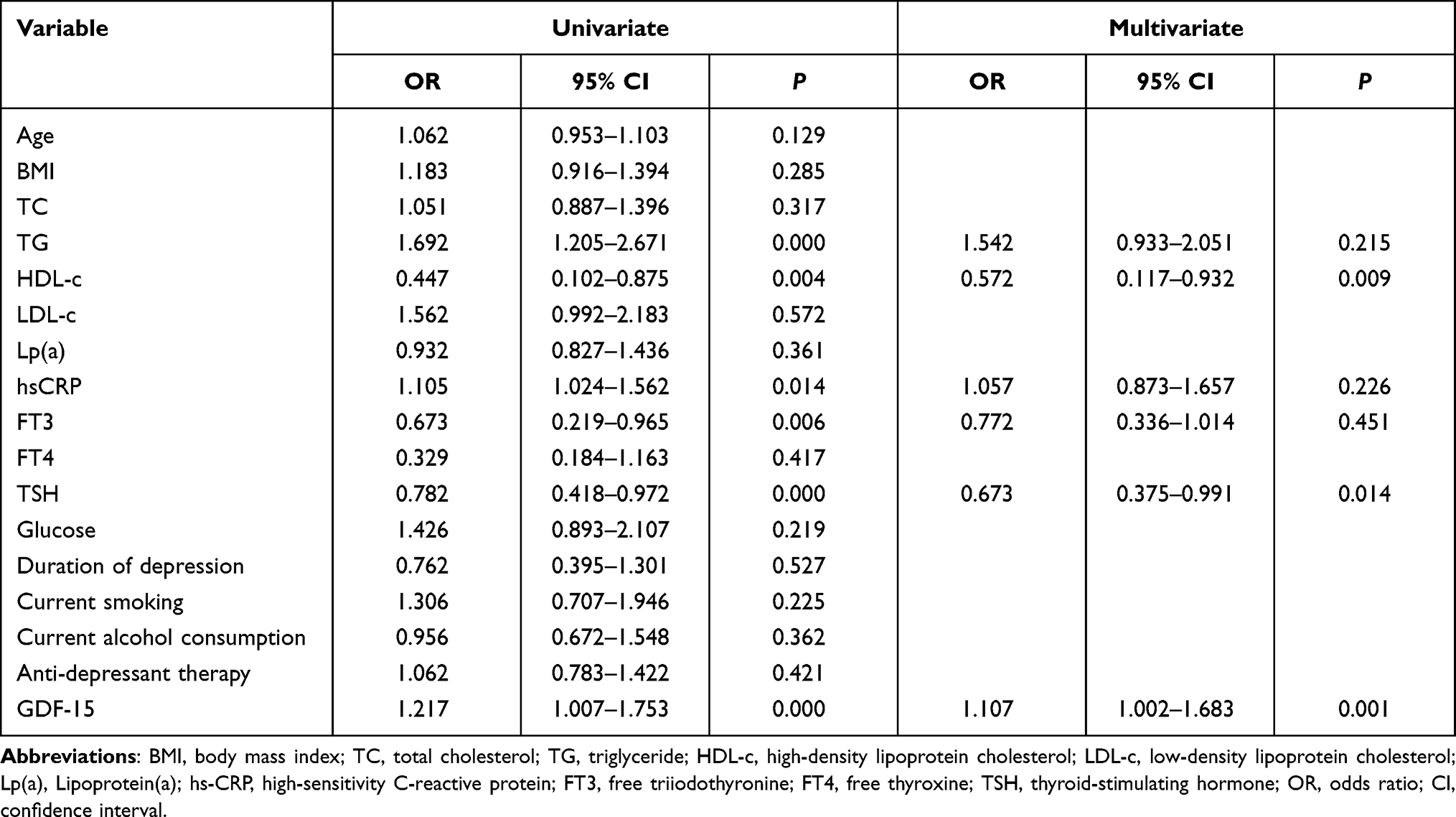 |
Table 2 Univariate and Multivariate Logistic Regression to Identify Factors Associated with Low Testosterone |
Associations Between Serum GDF-15 Level and Testosterone Level in Patients with Depression
Serum GDF-15 level was negatively associated with testosterone level (r=−0.218, P=0.003), HDL-c (r=−0.183, P<0.001) and TSH (r=−0.196, P=0.002), but positively associated with TC (r=0.153, P<0.001), TG (r=0.251, P=0.013), hsCRP (r=0.218, P=0.009) and FT4 (r=0.187, P<0.001). In multivariate stepwise regression, serum GDF15 level was defined as the dependent variable, while the independent variables were age, BMI, TC, TG, HDL-c, LDL-c, Lp(a), hs-CRP, FT3, FT4, TSH, Glu, testosterone, current smoking status, and current alcohol consumption status. This regression showed three variables to independently predict serum GDF-15 levels through a negative relationship: HDL-c, TSH, and testosterone (Table 3).
 |
Table 3 Multivariate Regression to Identify Factors Associated with Serum GDF-15 Levels in Patients with Depression |
Association Between Serum GDF-15 Level and Suicidal Ideation in Patients with Depression
A 1-SD increase in serum GDF-15 level was not associated with an increased risk of suicidal ideation in the entire sample of patients with depression, or in the subgroup of patients with high testosterone. Such an association was, however, observed in the subgroup of patients with low testosterone [odds ratio (OR) 1.452, 95% confidence interval (CI) 1.078–2.062, P=0.003; Table 4]. Similar results were obtained after correcting for several potential confounders in the multivariate model. Logistic regression showed that the use of antidepressants was negatively associated with suicidal ideation across all patients as well as separately in the low- and high-testosterone subgroups (all P<0.05).
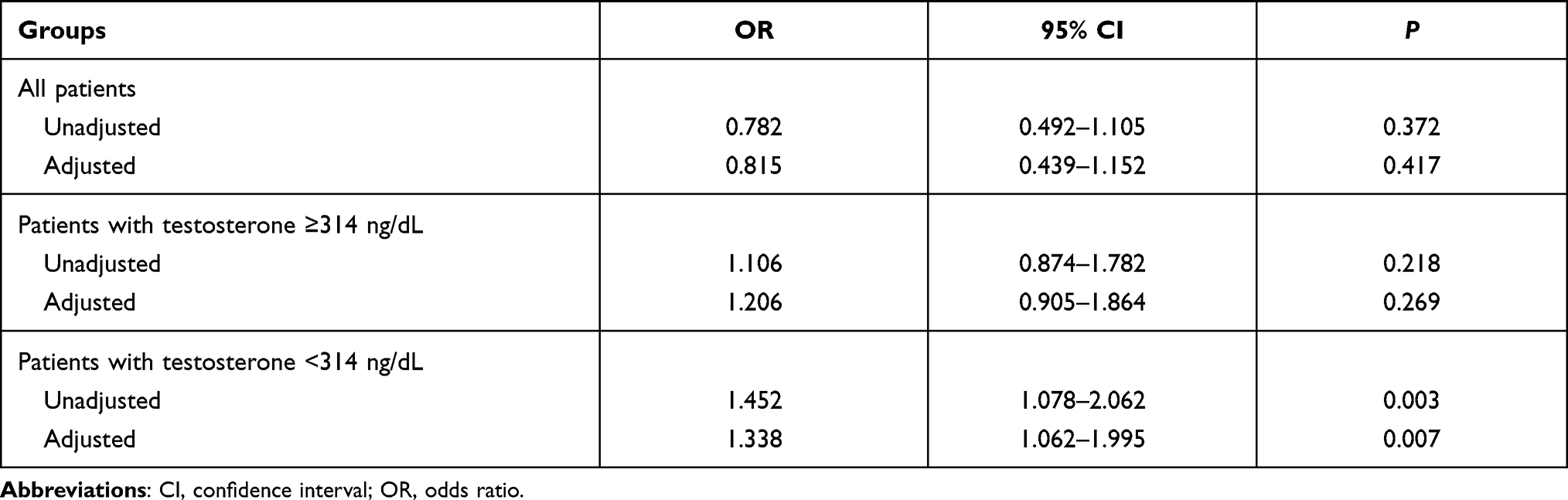 |
Table 4 Associations Between Serum GDF-15 and Suicidal Ideation in Patients with Depression |
Discussion
Although the mechanism of MDD is unclear, it has been associated with microglial activation, neuroinflammation and low testosterone in men. Given the medical burden and healthcare costs of depression, early detection and exploration of biomarkers in patients with depression are needed. Therefore, this study explores whether the inflammatory factor, GDF-15, is linked to the suicidal ideation in male depressive patients. The present study appears to be the first to investigate the relationship between serum GDF-15 level and suicidal ideation in male patients with depression. We found that serum GDF-15 levels were higher in patients with suicidal ideations than in those without suicidal ideation, regardless of their testosterone levels. More detailed analyses revealed that serum GDF-15 level was associated with suicidal ideation only in patients with testosterone levels below the median (314 ng/dL), but not in those with levels at or above the median. After adjusting for confounding factors, each 1-SD increase in serum GDF-15 level in low-testosterone patients was associated with a 1.3-fold increase in risk of suicidal ideation.
Many patients with long-standing MDD show an increased concentration of peripheral inflammatory cytokines, which has been linked to endocrine disturbances and deficiency of sex hormones.18 In fact, low testosterone has been associated with depression,13,14 and testosterone may protect against the disorder.19,20 We found here that GDF-15 levels correlated negatively with testosterone levels in patients with depression, similar to what has been reported for patients with coronary artery disease.21 GDF-15 has been demonstrated to be associated with the activation of microglia, which showed that GDF-15 deficiency compromises microglial response in the 6-hydroxydopamine mouse model of Parkinson’s disease.22 These findings showed that GDF-15 might contribute to the development of MDD and lead to the disease exacerbation. Previous study have also reported that severity of MDD is significant with a clear association of increased suicidality.23 Moreover, we also found that higher GDF-15 levels were associated with suicidal ideation. Similarly, serum GDF-15 levels have been shown to predict mood disorders in patients.24 High circulating GDF-15 levels have been associated with the development and progression of multiple disorders, such as cardiovascular and neurological disorders as well as cancer.25–27
Serum GDF-15 levels were significantly and negatively associated with testosterone in patients with coronary artery disease or HBV-associated hepatocellular carcinoma.28–30 Thus, the present research was to investigate the association among serum GDF-15 level and testosterone levels in depressive patients with or without suicidal ideation. Our data confirmed depressed subjects with suicidal ideation showed much higher serum GDF-15 levels than those without suicidal ideation, regardless of whether they had a testosterone <314 ng/dL or ≥314 ng/dL. The testosterone was authenticated as an independent factor negatively correlated with serum GDF-15 level. The increased GDF-15 level was closely associated with an increasing risk of suicidal ideation, and this correlation was dependent on testosterone deficiency. This phenomenon may be explained that the decreased of testosterone levels have direct effects on central nervous system functions and neuroinflammation, which regulate the suicidal ideation.
Our findings suggest a close relationship among serum GDF-15 level, testosterone level and suicidal ideation in male patients with depression. The mechanisms underlying this relationship remain to be explored, preferably in larger, prospective studies. GDF-15 may exert its damaging effects, in part, by activating microglia.11 Autopsy studies of patients with depression who commit suicide have detected activation of microglia in many.31 High levels of GDF-15 and other inflammatory cytokines in the circulation of patients with depression may injure the nervous system.32 Conversely, testosterone may protect against depression by decreasing neuroinflammation.33 Our study leads us to suggest that GDF-15 functions as a pro-inflammatory factor in the development and progression of depressive disorder, and that its activity may depend on testosterone levels, perhaps because testosterone regulates GDF-15 expression in the brain. Given that sex hormone deficiency contributes substantially to depressive and other health risks,34 and is also an important regulatory factor associated with serum GDF-15 levels.
In summary, serum GDF-15 level was significantly increased in depressive patients with testosterone deficiency. The elevated GDF-15 level was also significantly associated with an increasing risk of suicidal ideation in depressed patients, and this correlation was dependent on testosterone deficiency. Our results indicate that GDF-15 may be a potential biomarker to identify patients with depression who are at higher risk of suicidal behavior.
Data Sharing Statement
Data are available with the consent of the corresponding author.
Acknowledgments
This study was supported by the Fundamental Research Funds for the Central Universities (2042020kf0064). We thank Renmin Hospital of Wuhan University for providing technical consultation.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Vöhringer PA, Perlis RH. Discriminating between bipolar disorder and major depressive disorder. Psychiatr Clin North Am. 2016;39(1):1–10. doi:10.1016/j.psc.2015.10.001
2. Cuijpers P, Beekman AT, Reynolds CF
3. Croarkin PE, Nakonezny PA, Deng ZD, et al. High-frequency repetitive TMS for suicidal ideation in adolescents with depression. J Affect Disord. 2018;239:282–290.
4. Rukundo GZ, Kemigisha E, Ocan M, Adriko W, Akena DH. A systematic review of the risk factors for suicidal ideation, suicidal attempt and completed suicide among children and adolescents in sub-Saharan Africa between 1986 and 2018: protocol for a systematic review of observational studies. Syst Rev. 2018;7(1):230–238.
5. Blier P. Neurotransmitter targeting in the treatment of depression. J Clin Psychiatry. 2013;74:19–24.
6. Malekzadeh A, de Groot V, Beckerman H, van Oosten BW, Blankenstein MA, Teunissen CE. Challenges in multi-plex and mono-plex platforms for the discovery of inflammatory profiles in neurodegenerative diseases. Methods. 2012;56(4):508–513.
7. Dowlati Y, Herrmann N, Swardfager W, et al. A meta-analysis of cytokines in major depression. Biol Psychiatry. 2010;67:446–457.
8. Skowrońska M, Skrzyńska M, Machowski M, et al. Plasma growth differentiation factor 15 levels for predicting serious adverse events and bleeding in acute pulmonary embolism: a prospective observational study. Pol Arch Intern Med. 2020;130(9):757–765.
9. Altendahl M, Maillard P, Harvey D, et al. An IL-18-centered inflammatory network as a biomarker for cerebral white matter injury. PLoS One. 2020;15(1):e0227835.
10. Yin J, Zhu Z, Guo D, et al. Increased growth differentiation factor 15 is associated with unfavorable clinical outcomes of acute ischemic stroke. Clin Chem. 2019;65(4):569–578.
11. Kim DH, Lee D, Lim H, et al. Effect of growth differentiation factor-15 secreted by human umbilical cord blood-derived mesenchymal stem cells on amyloid beta levels in in vitro and in vivo models of Alzheimer’s disease. Biochem Biophys Res Commun. 2018;504(4):933–940.
12. Lu X, Duan J, Cheng Q, Lu J. The association between serum growth differentiation factor-15 and 3-month depression after acute ischemic stroke. J Affect Disord. 2020;260:695–702.
13. Barch DM, Shirtcliff EA, Elsayed NM, et al. Testosterone and hippocampal trajectories mediate relationship of poverty to emotion dysregulation and depression. Proc Natl Acad Sci U S A. 2020;117(36):22015–22023.
14. Giltay EJ, van der Mast RC, Lauwen E, Heijboer AC, Mwm DW, Comijs HC. Plasma testosterone and the course of major depressive disorder in older men and women. Am J Geriatr Psychiatry. 2017;25(4):425–437.
15. Kakehi Y, Segawa T, Wu XX, Kulkarni P, Dhir R, Getzenberg RH. Downregulation of macrophage inhibitory cytokine-1/prostate derived factor in benign prostatic hyperplasia. Prostate. 2004;59:351–356.
16. Liu T, Bauskin AR, Zaunders J, Brown DA, Pankhurst S, Russell PJ. Macrophage inhibitory cytokine 1 reduces cell adhesion and induces apoptosis in prostate cancer cells. Cancer Res. 2003;63:5034–5040.
17. Zitzmann M. Testosterone, mood, behaviour and quality of life. Andrology. 2020;8(6):1598–1605.
18. Tichomirowa MA, Keck ME, Schneider HJ, et al. Endocrine disturbances in depression. J Endocrinol Invest. 2005;28(1):89–99.
19. McHenry J, Carrier N, Hull E, Kabbaj M. Sex differences in anxiety and depression: role of testosterone. Front Neuroendocrinol. 2014;35(1):42–57.
20. Walther A, Breidenstein J, Miller R. Association of testosterone treatment with alleviation of depressive symptoms in men: a systematic review and meta-analysis. JAMA Psychiatry. 2019;76(1):31–40.
21. Jayaraman A, Lent-Schochet D, Pike CJ. Diet-induced obesity and low testosterone increase neuroinflammation and impair neural function. J Neuroinflammation. 2014;11:162–169.
22. Machado V, Haas SJ. von Bohlen Und Halbach O, Wree A, Krieglstein K, Unsicker K, Spittau B. Growth/Differentiation Factor-15 deficiency compromises dopaminergic neuron survival and microglial response in the 6-hydroxydopamine mouse model of Parkinson’s Disease. Neurobiol Dis. 2016;88:1–15.
23. Nicholas MN, Gooderham M. Psoriasis, depression, and suicidality. Skin Therapy Lett. 2017;22(3):1–4.
24. Frye MA, Nassan M, Jenkins GD, et al. Feasibility of investigating differential proteomic expression in depression: implications for biomarker development in mood disorders. Transl Psychiatry. 2015;5(12):e689.
25. Wollert KC, Kempf T, Wallentin L. Growth Differentiation Factor 15 as a biomarker in cardiovascular disease. Clin Chem. 2017;63(1):140–151.
26. Worthmann H, Kempf T, Widera C, et al. Growth differentiation factor 15 plasma levels and outcome after ischemic stroke. Cerebrovasc Dis. 2011;32(1):72–78.
27. Liu JY, Dong XX, Lu JN, et al. . Utility of GDF-15 as a diagnostic biomarker in gastric cancer: an investigation combining GEO, TCGA and meta-analysis. FEBS Open Bio. 2018;9(1):35–42.
28. Liu H, Dai W, Cui Y, Lyu Y, Li Y. Potential associations of circulating growth differentiation factor-15 with sex hormones in male patients with coronary artery disease. Biomed Pharmacother. 2019;114:108–122.
29. Liu H, Lyu Y, Li D, et al. Potential relation between soluble growth differentiation factor-15 and testosterone deficiency in male patients with coronary artery disease. Cardiovasc Diabetol. 2019;18(1):21–36.
30. Chen J, Dai W, Zhu C, Liu H, Li Y, Zhang P. Circulating levels of growth differentiation factor 15 and sex hormones in male patients with HBV-associated hepatocellular carcinoma. Biomed Pharmacother. 2020;121:109–117.
31. Brites D, Fernandes A. Neuroinflammation and depression: microglia activation, extracellular microvesicles and microRNA dysregulation. Front Cell Neurosci. 2015;9:476–483.
32. Voet S, Prinz M, van Loo G. Microglia in central nervous system inflammation and multiple sclerosis pathology. Trends Mol Med. 2019;25(2):112–123.
33. Collongues N, Patte-Mensah C, De Seze J, Mensah-Nyagan AG, Derfuss T. Testosterone and estrogen in multiple sclerosis: from pathophysiology to therapeutics. Expert Rev Neurother. 2018;18(6):515–522.
34. Slavich GM, Sacher J. Stress, sex hormones, inflammation, and major depressive disorder: extending social signal transduction theory of depression to account for sex differences in mood disorders. Psychopharmacology (Berl). 2019;236(10):3063–3079.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.