")
Back to Journals » International Journal of General Medicine » Volume 17
The Administration of Lemborexant at Admission is Not Associated with Inpatient Falls: A Multicenter Retrospective Observational Study
Authors Hirata R , Katsuki NE, Shimada H, Nakatani E , Shikino K , Saito C , Amari K, Oda Y, Tokushima M, Tago M
Received 28 November 2023
Accepted for publication 11 March 2024
Published 25 March 2024 Volume 2024:17 Pages 1139—1144
DOI https://doi.org/10.2147/IJGM.S452278
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Risa Hirata,1 Naoko E Katsuki,1 Hitomi Shimada,2 Eiji Nakatani,3 Kiyoshi Shikino,4,5 Chihiro Saito,6 Kaori Amari,7 Yoshimasa Oda,8 Midori Tokushima,1 Masaki Tago1
1Department of General Medicine, Saga University Hospital, Saga, Japan; 2Shimada Hospital of Medical Corporation Chouseikai, Saga, Japan; 3Graduate School of Public Health, Shizuoka Graduate University of Public Health, Shizuoka, Japan; 4Department of General Medicine, Chiba University Hospital, Chiba, Japan; 5Department of Community-Oriented Medical Education, Chiba University Graduate School of Medicine, Chiba, Japan; 6Shizuoka General Hospital, Shizuoka, Japan; 7Department of Emergency Medicine, Saga-Ken Medical Centre Koseikan, Saga, Japan; 8Department of General Medicine, Yuai-Kai Foundation and Oda Hospital, Saga, Japan
Correspondence: Masaki Tago, Department of General Medicine, Saga University Hospital, 5-1-1 Nabeshima, Saga, 849-8501, Japan, Tel +81 952 34 3238, Fax +81 952 34 2029, Email [email protected]
Purpose: There has been no large-scale investigation into the association between the use of lemborexant, suvorexant, and ramelteon and falls in a large population. This study, serving as a pilot investigation, was aimed at examining the relationship between inpatient falls and various prescribed hypnotic medications at admission.
Patients and Methods: This study was a sub-analysis of a multicenter retrospective observational study conducted over a period of 3 years. The target population comprised patients aged 20 years or above admitted to eight hospitals, including chronic care, acute care, and tertiary hospitals. We extracted data on the types of hypnotic medications prescribed at admission, including lemborexant, suvorexant, ramelteon, benzodiazepines, Z-drugs, and other hypnotics; the occurrence of inpatient falls during the hospital stay; and patients’ background information. To determine the outcome of inpatient falls, items with low collinearity were selected and included as covariates in a forced-entry binary logistic regression analysis.
Results: Overall, 150,278 patients were included in the analysis, among whom 3,458 experienced falls. The median age of the entire cohort was 70 years, with men constituting 53.1%. Binary logistic regression analysis revealed that the prescription of lemborexant, suvorexant, and ramelteon at admission was not significantly associated with inpatient falls.
Conclusion: The administration of lemborexant, suvorexant, and ramelteon at admission may not be associated with inpatient falls.
Keywords: lemborexant, hypnotics, in-hospital falls, risk factor
Introduction
In-hospital falls present significant challenges, contributing to societal burdens such as increased healthcare costs and physical and psychological burdens on patients,1 including physical sequelae and fear of falls.2,3 Hypnotic medications are recognized risk factors for falls,4 and their use often increases during hospitalization because of changes in both the environment and the patient’s condition, leading to insomnia.5 While benzodiazepine hypnotics (BZs) have been previously reported to be associated with falls,6 in recent years, new hypnotic medications, such as lemborexant, suvorexant, and ramelteon, have become available. However, there is a dearth of multicenter studies examining the association between these novel hypnotic medications and falls. Definitive evidence of the association between suvorexant and falls has not been shown, even in studies with small populations.7,8 Remarkably, the relationship between lemborexant and falls has been scarcely investigated, with only few single-center studies addressing this issue.9 This study, serving as a pilot investigation, was aimed at examining the association between inpatient falls and various hypnotic medications by using multicenter data.
Materials and Methods
This study was a sub-analysis of an unpublished multicenter retrospective study conducted from April 1, 2018, to March 31, 2021, targeting patients aged 20 years or above admitted to eight hospitals, including chronic care, acute care, and tertiary hospitals. Patient data, including background information such as age,10,11 sex, underlying conditions, and the occurrence of inpatient falls, were extracted from their medical records. We collected prescription data from drug pharmacy records for medications with the first three digits of the Ministry of Health, Labour and Welfare Drug Code (YJ Code) 112, suvorexant, lemborexant, and ramelteon, up to the day following admission. Subsequently, we categorized these medications into the following groups: BZs, Z-drugs, suvorexant, lemborexant, ramelteon, and other hypnotics. The collected data on underlying conditions included those pertaining to emergency admission,10 Bedriddenness Rank,10,12 Cognitive Function Score,10,13 activities of daily living (ability to eat, transferring, groom, use the toilet, bathe, walk independently on ground level, climb stairs, change clothes, maintain bowel and bladder self-control),10 emergency transportation,14 referral letter,14 care level,15 consciousness disturbance, admitting department,10 dysphagia, urinary frequency,16 diabetes mellitus (ICD-10: E10-14),17 history of stroke (I60.0-I64, I69),18,19 lower limb paralysis (G81.0, G81.1, G81.9, G83.1, G82.1), Parkinson’s syndrome (G20, G21),11 ophthalmic diseases (H25, H26, H28.1, H40 (other than 40.7), H42, Q15.0), visual impairment (assessment through self-report),20 alcoholism (F10.0–10.9), surgical operations during hospital stay,15 rehabilitation,15 antipsychotic medication use,13 independence in taking prescription drugs, use of mobility aids,21 and history of falls before admission.11,12 The Bedriddenness Rank and the Cognitive Function Score are public activities of daily living scales developed by Japan’s Ministry of Health, Labour and Welfare. The Bedriddenness Rank has five major classes (normal, J, A, B, and C), and the Cognitive Function Score has six (normal, I, II, III, IV, and M).20 In analyzing inpatient falls as the outcome, all categories of hypnotic medications and factors collected, ensuring a Spearman correlation coefficient of <0.5 for low collinearity among all variables, were included. For highly collinear pairs, one of the variables was selected as a covariate, and all variables were forced into a binary logistic regression analysis. The significance level was set at <0.05. This study adheres to the principles outlined in the Declaration of Helsinki, as well as the Ethical Guidelines for Medical and Health Research Involving Human Subjects issued by the Japanese Ministry of Health, Labour and Welfare and the Ministry of Education, Culture, Sports, Science, and Technology. The study was approved by the Ethics Committee of Saga University Hospital (approval ID: 2023–08-SC-07).
Results
Overall, 150,278 patients aged 20 years or older admitted during the study period, with 3,458 cases of falls, were included. The median age was 70 years, and 53.1% were men (Table 1). Among these inpatients, 390 (0.3%), 2,777 (1.8%), 2,130 (1.4%), 13,271 (8.8%), and 5,634 (3.7%) were prescribed lemborexant, suvorexant, ramelteon, BZs, and Z-drugs, respectively. Hospital, age, sex, emergency admission, Bedriddenness Rank (normal, J, A, B, or C), Cognitive Function Score (normal, I, II, III, IV, or M), emergency transportation, referral letter, care level, consciousness disturbance, use of walking aids, admitting department, independence of ground-level walking (independent or assisted), dysphagia, urinary frequency, diabetes mellitus, history of stroke, lower limb paralysis, Parkinson’s syndrome, ophthalmic diseases, visual impairment, alcoholism, surgical operation during hospital stay, rehabilitation, antipsychotic medication, and history of falls had Spearman correlation coefficients of <0.5 each. Logistic regression analysis was performed for these factors and the six hypnotic medications (lemborexant, suvorexant, ramelteon, BZs, Z-drugs, and others) totaling 32 items. We found that the prescription of lemborexant (p = 0.431), suvorexant (p = 0.167), and ramelteon (p = 0.412) at admission was not significantly associated with in-hospital falls. In contrast, the prescription of BZs and Z-drugs at admission had odds ratios of 1.26 (p < 0.001) and 1.29 (p = 0.001), respectively, indicating a significant association with falls (Table 2).
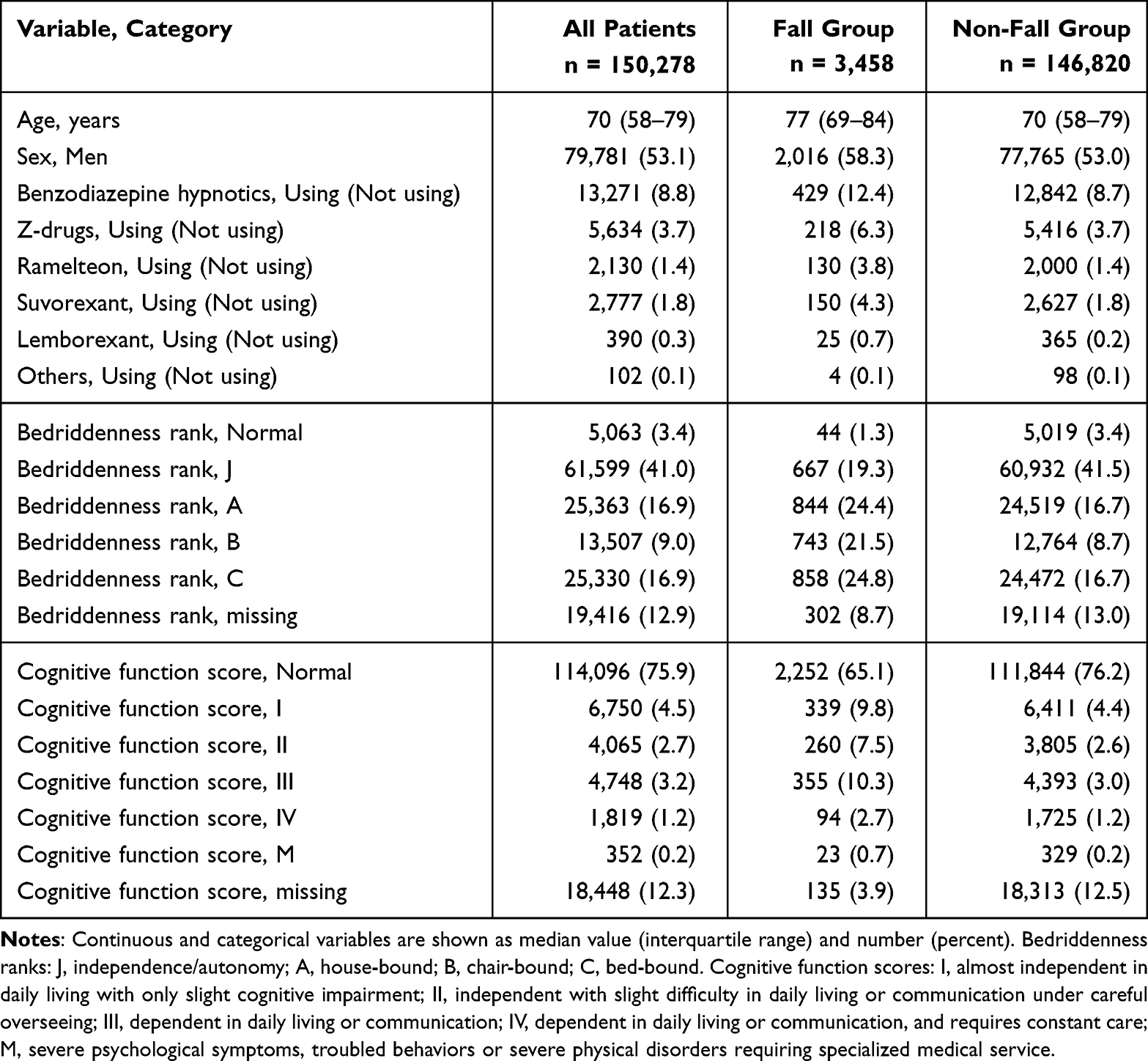 |
Table 1 Characteristics of Patients |
 |
Table 2 Results of Multivariable Logistic Regression Analysis (Extracted) |
Discussion
In this study, BZs and Z-drugs were found to be significantly associated with in-hospital falls. However, new hypnotic medications prescribed at admission, namely lemborexant, suvorexant, and ramelteon, were not significantly associated with falls in this multicenter study.
The association between novel hypnotic medications and falls has thus far been reported only in small-scale studies.8,22,23 In a study by Sogawa et al investigating the relationship between lemborexant and falls in a single-center study, lemborexant reduced the risk of falls.9 Furthermore, the association of suvorexant with falls yielded different results from previous studies.7,8 This discrepancy may be attributed to variations in analytical methods and the studies being focused on single-center or small-scale facilities. However, the present study, conducted across multiple facilities, did not reveal a significant association between lemborexant, ramelteon, and suvorexant and falls. BZs and Z-drugs exhibit pharmacological actions related to the gamma-aminobutyric acid (GABA) receptors, contributing to reported effects such as sedation and muscle relaxation.24 These medications are also known to be associated with various side effects, including delirium, orthostatic hypotension, dizziness, motor impairment such as muscle weakness and extrapyramidal symptoms, and visual impairment,25 and were significantly associated with falls in this study; this finding was similar to those of previous studies.6,10 However, unlike BZs and Z-drugs, the new hypnotic medications, lemborexant, suvorexant, and ramelteon, do not interact with GABA receptors.24 Ramelteon utilizes melatonin, which controls circadian rhythms through G protein–coupled receptors (MT1/MT2) and lemborexant and suvorexant utilize orexin antagonists through orexin receptors to regulate sleep cycles.24 These novel hypnotic medications, unlike BZs and Z-drugs, are less likely to induce sedation or muscle relaxation, pharmacologically minimizing the risk of falls and suggesting a potential lack of association with falls.24 Additionally, lemborexant, suvorexant, and ramelteon have been reported to have preventive effects against the onset of delirium.26,27 Because Japan is a leading aged society globally and the median age of our study population was 70 years, falls in older individuals can be influenced by factors such as delirium,28 making it plausible that the new hypnotic medications were not significantly associated with falls owing to their potential inhibitory effects against delirium onset.
Limitations
The present study was a pilot and retrospective observational study. Data collection regarding hypnotic medications was based on their prescription status only at admission; thus, the study lacked adjustments for medications either added or discontinued during hospitalization. This study was conducted in hospitals across various prefectures, with six out of eight facilities located in rural prefectures in Japan. The majority of the population consisted of inpatients from acute care or tertiary hospitals, potentially introducing selection bias. Additionally, due to the unavailability of data on fall prevention measures, the effect of interventions for fall prevention could not be assessed.
Conclusion
The administration of lemborexant, suvorexant, and ramelteon at admission may not be associated with in-hospital falls. Because their pharmacological actions are distinct from those of the well-established fall-related agents such as BZs and Z-drugs, these medications may not induce sedation and muscle relaxation, which contribute to the risk of falls. Furthermore, the potential of these drugs to prevent delirium might be related to lower fall risks. Further research is necessary to elucidate the association between hypnotic medications and in-hospital falls, considering factors such as the prescription history of hypnotic medications after admission, the time of the most recent ingestion of hypnotic medications before a fall, and the timing of the fall itself.
Abbreviations
BZs, benzodiazepines GABA, gamma-aminobutyric acid.
Data Sharing Statement
The datasets generated and analyzed during the current study are available in the UMIN-ICDR repository (https://center6.umin.ac.jp/cgi-bin/icdr_e/ctr_view.cgi?recptno=R000050831).
Ethics Approval and Informed Consent
This study conforms to Ethical Guidelines for Medical and Health Research Involving Human Subjects issued by the Japanese Ministry of Health, Labour and Welfare and the Ministry of Education, Culture, Sports, Science, and Technology. The study was approved by the Ethics Committee of Saga University Hospital (approval ID: 2023-08-SC-07). We obtained consent from all patients by using the hospital’s comprehensive agreement method, and patients’ anonymity was protected. We disclosed study information on the hospital’s website and allowed patients to opt out of participation.
Acknowledgments
We thank Miho Hayashida, Naoko Otsubo, Dr. Tomoyo Nishi, Dr. Shizuka Yaita, Dr. Yuka Hirakawa, Dr. Masahiko Nakamura, Dr. Shun Yamashita, Dr. Yoshinori Tokushima, Dr. Hidetoshi Aihara, Dr. Motoshi Fujiwara, and Prof. Mariko Yoshimura from Saga University Hospital; Kenta Yamaguchi, Yuka Hisamoto, Yasuhiro Chibu, and Toshinobu Eguchi from Yuai-Kai Foundation and Oda Hospital; Tomokazu Ichibakase and Dr. Kazuya Kurogi from National Hospital Organization Ureshino Medical Center; Yoshihiko Nakashima, Kaori Hamai, and Dr. Maiko Ono from Karatsu Municipal Hospital; and Yuriko Takao, Mika Tokushima, Yoshiro Nakayama, and Dr. Kozo Naito from Saga-Ken Medical Centre Koseikan for assistance with data acquisition.
Author Contributions
All authors made a significant contribution to the work reported with respect to the conception, study design, execution, acquisition of data, analysis, and interpretation. All authors participated in drafting, revising, or critically reviewing the article and approved the final version submitted for publication. All the authors have agreed to the journal submission and agree to be accountable for all aspects of the work.
Funding
This work was supported by JSPS KAKENHI (Grant Number JP21H03166).
Disclosure
Masaki Tago is supported by grants from the Japan Society for the Promotion of Science, JSPS KAKENHI (Grant Number JP18K17322 and JP21H03166). Naoko E. Katsuki is supported by grants from the Japan Society for the Promotion of Science, JSPS KAKENHI (Grant Number JP23K16257). The sponsor of the study had no role in the preparation of the manuscript. The authors report no other conflicts of interest in this work.
References
1. Dykes PC, Curtin-Bowen M, Lipsitz S, et al. Cost of inpatient falls and cost-benefit analysis of implementation of an evidence-based fall prevention program. JAMA Health Forum. 2023;4(1):e225125. doi:10.1001/jamahealthforum.2022.5125
2. Alamri SH, Ghamri RA, Alshehri WH, et al. Falls and correlations among community-dwelling older adults: a cross-sectional study in Jeddah, Saudi Arabia. Pak J Med Sci. 2023;39(1):109–116. doi:10.12669/pjms.39.1.6993
3. Chung MC, McKee KJ, Austin C, et al. Posttraumatic stress disorder in older people after a fall. Int J Geriatr Psychiatry. 2009;24(9):955–964. doi:10.1002/gps.2201
4. Obayashi K, Araki T, Nakamura K, et al. Risk of falling and hypnotic drugs: retrospective study of inpatients. Drugs R D. 2013;13(2):159–164. doi:10.1007/s40268-013-0019-3
5. Badr AF, Kurdi S, Alshehri S, McManus C, Lee J. Pharmacists’ interventions to reduce sedative/hypnotic use for insomnia in hospitalized patients. Saudi Pharm J. 2018;26(8):1204–1207. doi:10.1016/j.jsps.2018.07.010
6. Herzig SJ, Rothberg MB, Moss CR, et al. Risk of in-hospital falls among medications commonly used for insomnia in hospitalized patients. Sleep. 2021;44(9):zsab064. doi:10.1093/sleep/zsab064
7. Torii H, Ando M, Tomita H, et al. Association of hypnotic drug use with fall incidents in hospitalized elderly patients: a case-crossover study. Biol Pharm Bull. 2020;43(6):925–931. doi:10.1248/bpb.b19-00684
8. Ishibashi Y, Nishitani R, Shimura A, et al. Non-GABA sleep medications, suvorexant as risk factors for falls: case-control and case-crossover study. PLoS One. 2020;15(9):e0238723. doi:10.1371/journal.pone.0238723
9. Sogawa R, Emoto A, Monji A, et al. Association of orexin receptor antagonists with falls during hospitalization. J Clin Pharm Ther. 2022;47(6):809–813. doi:10.1111/jcpt.13619
10. Tago M, Katsuki NE, Oda Y, Nakatani E, Sugioka T, Yamashita SI. New predictive models for falls among inpatients using public ADL scale in Japan: a retrospective observational study of 7,858 patients in acute care setting. PLoS One. 2020;15(7):e0236130. doi:10.1371/journal.pone.0236130
11. Chu LW, Chi I, Chiu AY. Incidence and predictors of falls in the Chinese elderly. Ann Acad Med Singap. 2005;34(1):60–72. doi:10.47102/annals-acadmedsg.V34N1p60
12. Hirata R, Tago M, Katsuki NE, et al. History of falls and bedriddenness ranks are useful predictive factors for in-hospital falls: a single-center retrospective observational study using the saga fall risk model. Int J Gen Med. 2022;15:8121–8131. doi:10.2147/IJGM.S385168
13. Sousa LM, Marques-Vieira CM, Caldevilla MN, Henriques CM, Severino SS, Caldeira SM. Risk for falls among community-dwelling older people: systematic literature review. Rev Gaucha Enferm. 2017;37(4):e55030. doi:10.1590/1983-1447.2016.04.55030
14. Yaita S, Tago M, Katsuki NE, et al. A simple and accurate model for predicting fall injuries in hospitalized patients: insights from a retrospective observational study in Japan. Med Sci Monit. 2023;29:e941252. doi:10.12659/MSM.941252
15. Hayakawa T, Hashimoto S, Kanda H, et al. Risk factors of falls in inpatients and their practical use in identifying high-risk persons at admission: Fukushima Medical University Hospital cohort study. BMJ Open. 2014;4(8):e005385. doi:10.1136/bmjopen-2014-005385
16. Nakagawa H, Niu K, Hozawa A, et al. Impact of nocturia on bone fracture and mortality in older individuals: a Japanese longitudinal cohort study. J Urol. 2010;184(4):1413–1418. doi:10.1016/j.juro.2010.05.093
17. Noh HM, Song HJ, Park YS, Han J, Roh YK. Fall predictors beyond fall risk assessment tool items for acute hospitalized older adults: a matched case-control study. Sci Rep. 2021;11(1):1503. doi:10.1038/s41598-021-81034-9
18. Ganz DA, Bao Y, Shekelle PG, Rubenstein LZ. Will My Patient Fall? JAMA. 2007;297(1):77–86. doi:10.1001/jama.297.1.77
19. Lukaszyk C, Harvey L, Sherrington C, et al. Risk factors, incidence, consequences and prevention strategies for falls and fall-injury within older indigenous populations: a systematic review. Aust N Z J Public Health. 2016;40(6):564–568. doi:10.1111/1753-6405.12585
20. Aihara H, Tago M, Oishi T, Katsuki NE, Yamashita SI. Visual impairment, partially dependent ADL and extremely old age could be predictors for severe fall injuries in acute care settings. Int J Gerontol. 2018;12(3):175–179. doi:10.1016/j.ijge.2018.02.014
21. Deandrea S, Bravi F, Turati F, Lucenteforte E, La Vecchia C, Negri E. Risk factors for falls in older people in nursing homes and hospitals. A systematic review and meta-analysis. Arch Gerontol Geriatr. 2013;56(3):407–415. doi:10.1016/j.archger.2012.12.006
22. Oda S, Takechi K, Hirai S, Takatori S, Otsuka T. Association between nocturnal falls and hypnotic drug use in older patients at acute care hospitals. Eur J Clin Pharmacol. 2023;79(6):753–758. doi:10.1007/s00228-023-03485-5
23. Ishigo T, Takada R, Kondo F, et al. ラメルテオン・スボレキサントを含めた睡眠薬の服用と転倒への影響:症例対照研究 [Association suvorexant and ramelteon use with the risk of falling: a retrospective case-control study]. Yakugaku Zasshi. 2020;140(8):1041–1049. doi:10.1248/yakushi.20-00018 Japanese.
24. Schroeck JL, Ford J, Conway EL, et al. Review of safety and efficacy of sleep medicines in older adults. Clin Ther. 2016;38(11):2340–2372. doi:10.1016/j.clinthera.2016.09.010
25. Capiau A, Huys L, van Poelgeest E, et al. Therapeutic dilemmas with benzodiazepines and Z-drugs: insomnia and anxiety disorders versus increased fall risk: a clinical review. Eur Geriatr Med. 2023;14(4):697–708. doi:10.1007/s41999-022-00731-4
26. Matsuoka A, Tobita S, Sogawa R, et al. Evaluation of suvorexant and lemborexant for the prevention of delirium in adult critically ill patients at an advanced critical care center: a single-center, retrospective, observational study. J Clin Psychiatry. 2022;84(1):22m14471. doi:10.4088/JCP.22m14471
27. Hatta K, Kishi Y, Wada K, et al. Real-world effectiveness of ramelteon and suvorexant for delirium prevention in 948 patients with delirium risk factors. J Clin Psychiatry. 2019;81(1):19m12865. doi:10.4088/JCP.19m12865
28. Mazur K, Wilczyński K, Szewieczek J. Geriatric falls in the context of a hospital fall prevention program: delirium, low body mass index, and other risk factors. Clin Interv Aging. 2016;11:1253–1261. doi:10.2147/CIA.S115755
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.