Back to Journals » Lung Cancer: Targets and Therapy » Volume 14
The Additional Exclusions of ROS1 Fusions (In Addition to EGFR Mutation and ALK Fusions) in the Cemiplimab NSCLC FDA Indication (EMPOWER-Lung 1 and -Lung 3). Catching Up with Current Scientific View of Immunotherapy in Never-Smoker Predominant Actionable Driver Mutation Positive NSCLC?
Received 30 April 2023
Accepted for publication 20 June 2023
Published 23 June 2023 Volume 2023:14 Pages 63—69
DOI https://doi.org/10.2147/LCTT.S413611
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Fengying Wu
Danielle Brazel,1 Saihong Ignatius Ou1,2
1University of California Irvine School of Medicine, Department of Medicine, Orange, CA, 92868, USA; 2Chao Family Comprehensive Cancer Center, Orange, CA, 92868, USA
Correspondence: Saihong Ignatius Ou, University of California Irvine School of Medicine, Department of Medicine, Division of Hematology-Oncology, Chao Family Comprehensive Cancer Center, 200 South Manchester, Suite 400, Orange, CA, 92868, USA, Tel +1 714-456-5153, Fax +1 714-345-2242, Email [email protected]
Abstract: Cemiplimab is one of seven immune checkpoint inhibitors (ICIs) approved for the first-line (1L) treatment of advanced NSCLC in the US based on EMPOWER-Lung 1 and -Lung 3 trials. In addition to exclusion of NSCLC patients harboring EGFR mutations and ALK fusion from 1L treatment with ICIs, exclusion of ROS1 fusion is an additional unique exclusion the use of criterion for cemiplimab in the US FDA indication based on the design of the EMPOWER lung trials. We review the effectiveness of ICIs in never-smoker predominant NSCLC with driver mutations (EGFR, ALK, ROS1, RET, HER2) and question whether exclusion of ROS1 fusion would put cemiplimab at a competitive disadvantage given the requirement for insurance to prove ROS1 fusion negativity. We further discuss whether the US FDA as a regulatory authority has the right and responsibility to harmonize the use of ICIs in these actionable driver mutations to standardize community practice for the benefit of patients and to advance the development of next-generation treatment for these driver mutations.
Keywords: cemiplimab, immunotherapy, actionable driver mutation, ROS1 fusion
Introduction
As of March 2023, there are seven immune checkpoint inhibitors (ICIs) approved in the United States (US) for the first-line (1L) treatment of advanced or metastatic non-small cell lung cancer (NSCLC). These ICIs include pembrolizumab (Keynote [KN]-024, KN-042, KN-189, and KN-407),1–4 atezolizumab (IMpower-110, −130, −150),5–7 cemiplimab (EMPOWER-Lung-01, −03),8,9 nivolumab + ipilimumab (without or witho chemotherapy (Checkmate [CM CM-227, CM-9LA] respectively),10,11 and durvalumab + tremelimumab with chemotherapy (POSEIDON)12 based on 12 positive pivotal randomized Phase 3 clinical trials (Table 1).
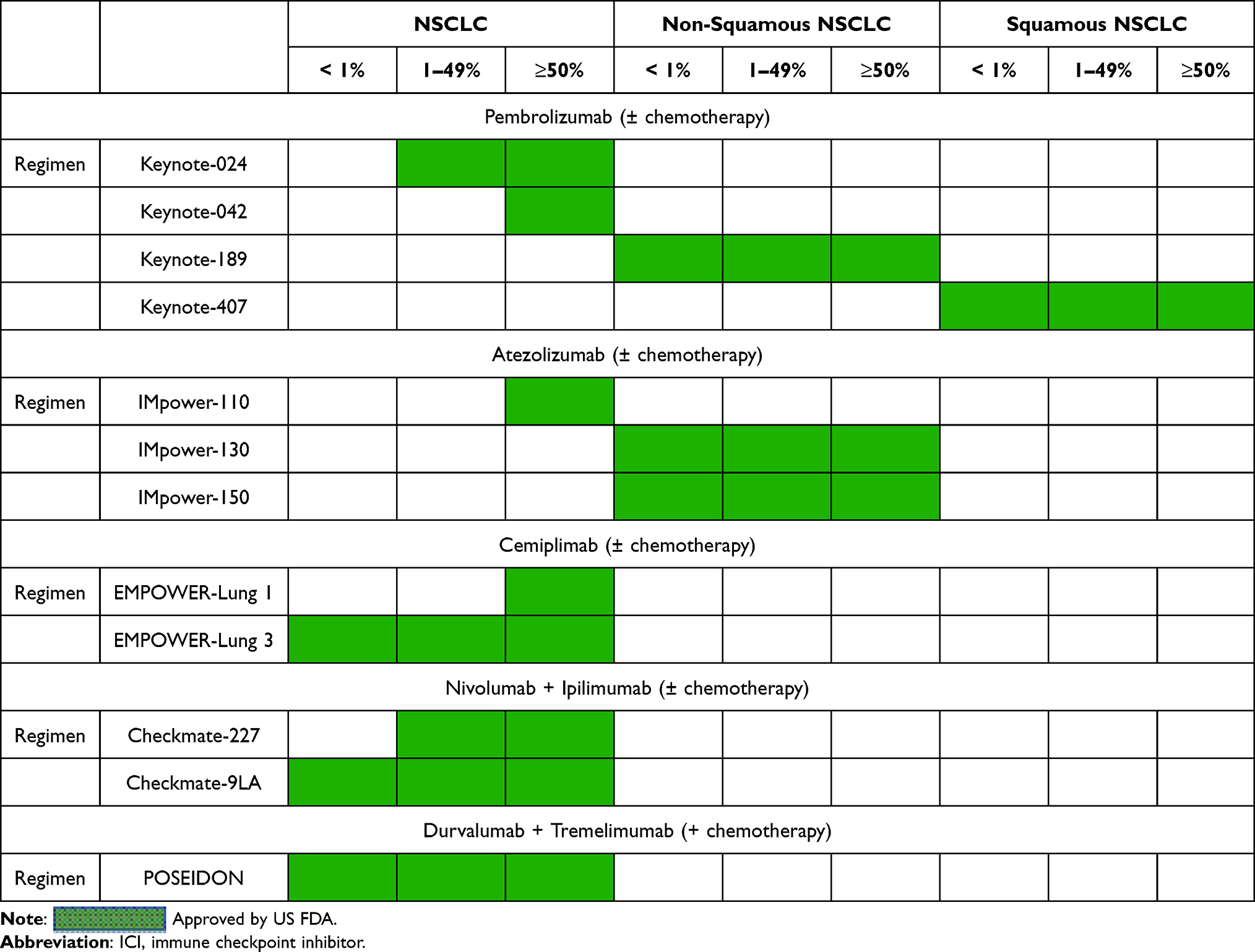 |
Table 1 Approved ICI Regimens in the US for 1st-Line Treatment of Advanced NSCLC by Histology and PD-L1 Expression |
Some of the ICIs approvals rely on the level of PD-L1 expression while some are histology-specific. Some of the regimens are ICI monotherapy, combination ICIs, ICI in addition to chemotherapy or all (Table 1). As presented in Table 1, there is substantial overlap in the indications especially among NSCLC regardless of histology thus medical oncologists have many treatment options. Uniform among indications for all regimens is that NSCLC patients with activating epidermal growth factor receptor (EGFR) mutations (EGFR+) and anaplastic lymphoma kinase (ALK) fusions (ALK+) were excluded (not indicated by US package insert). Additionally, unique to cemiplimab usage included an addition exclusion of ROS proto-oncogene 1 (ROS1) fusions (ROS1+) based on the designs of EMPOWER-Lung trials. This editorial focuses on the implication of this unique ROS1+ exclusion for cemiplimab and the deeper role of efficacy and use of immunotherapy in never-smoker predominant driver mutation positive NSCLC.
Primary Data of EMPOWER-Lung 1 and -Lung 3
The exclusion of ROS1 fusions in the indication of cemiplimab is due to the design of EMPOWER-Lung-01 and −03 trial both excluding ROS1+ NSCLC patients in addition to standard exclusions of EGFR+ and ALK+ NSCLC patients common to all other 10 chemotherapy regimens.13 The Food and Drug Administration (FDA) approved cemiplimab monotherapy in PD-L1 ≥ 50% on February 22, 2021 based on the EMPOWER-Lung 1 trial (NCT03088540).8 NSCLC patients with PD-L1 expression ≥ 50% (N = 710) were randomized 1:1 to either cemiplimab 350 milligrams (mg) intravenously every 3 weeks versus platinum-based chemotherapy. Primary outcomes were progression-free survival (PFS) and overall survival (OS) assessed by blinded independent central review (BICR). Overall, cemiplimab demonstrated statistically significant improvement in median OS at 22.1 months (95% confidence interval (CI): 17.7 to not reached) for patients receiving cemiplimab compared with 14.3 months (95% CI: 11.7–19.2) in the platinum chemotherapy arm (HR = 0.68; 95% CI: 0.53–0.87, p=0.0022). Median PFS per BICR assessment was also statistically significantly improved at 6.2 months (95% CI: 4.5–8.3) verses 5.6 months (95% CI: 4.5–6.1) in the cemiplimab and chemotherapy arms, respectively (HR = 0.59; 95% CI: 0.49, 0.72, p<0.0001). The authors found overall response rate (ORR) of 37% (95% CI: 32–42) treated with cemiplimab and 21% (95% CI: 17, 25) treated with chemotherapy.
Subsequently, FDA granted approval for chemotherapy + cemiplimab on November 22, 2022 based on EMPOWER-Lung 3 trial.9 Four hundred sixty-six NSCLC patients were randomized in a 2:1 assignment to either cemiplimab plus platinum-based chemotherapy every 3 weeks for a total of 4 cycles followed by cemiplimab plus maintenance chemotherapy or placebo plus platinum-based chemotherapy every 3 weeks for a total of 4 cycles followed by placebo and maintenance chemotherapy. The primary outcome was OS with secondary outcomes of PFS and ORR as assessed by BICR. In the most recent update of June 14, 2022, data cut-off, the median duration of follow-up for the study was 28.4 months (interquartile range [IQR]: 26.0–31.0): 28.3 months (IQR: 25.9–31.1) in the cemiplimab plus chemotherapy arm and 28.7 months (IQR: 26.2–31.0) in the placebo plus chemotherapy arm. Median OS with the cemiplimab combination was 21.1 months (95% CI: 15.9–23.5) versus 12.9 months (95% CI: 10.6–15.7) with chemotherapy alone (HR = 0.65; 95% CI: 0.51–0.82; P=0.0003). Patients with squamous (SqCC) NSCLC (n=200) demonstrated a 2-year median OS of 22.3 months (95% CI: 15.7–27.2) with the cemiplimab plus chemotherapy versus 13.8 months (95% CI: 9.3–18.0) with chemotherapy alone (HR=0.61; 95% CI: 0.42–0.87). Importantly with longer follow-up time, the OS was significantly improved further than the outcomes observed at the initial time of data presentation. The median OS for non-SqCC histology was 19.4 months (95% CI: 14.0–23.5) with cemiplimab plus chemotherapy versus 12.4 months (95% CI: 10.1–16.1) with chemotherapy alone (HR = 0.64; 95% CI: 0.47–0.88).14 In the cemiplimab plus chemotherapy group, median PFS was 8.2 months (95% CI: 6.4–9.0) versus 5.5 months (95% CI: 4.3–6.2) with chemotherapy alone (HR = 0.55; 95% CI: 0.44–0.68; P<0.0001). When analyzed by independent central review, the ORR was 43.6% (95% CI: 38.0–49.3) in the cemiplimab plus chemotherapy group versus 22.1% (95% CI: 15.8–29.5) in the chemotherapy alone group (P<0.0001). The most common associated with cemiplimab (≥15% of participants) adverse events include alopecia, musculoskeletal pain, nausea, fatigue, peripheral neuropathy, and decreased appetite.
Actionable Driver Mutation in NSCLC Associated with Never-Smokers
Many actionable driver mutations are associated with never-smoking status such as EGFR mutations (del19, L858R, exon 20 insertions, L861, S761, G719X), human epidermal growth factor receptor 2 (HER2) exon 20 insertions, and the three major receptor tyrosine kinase fusions (ALK, ROS1, RET [rearranged during transfection]).15 A large-scale global retrospective analysis of ICIs in never-smoker associated actionable driver mutations indicated that ICIs have minimal activity in this setting.16
Discussion Point 1. Reviewing the Evidence of ICI in EGFR+ NSCLC, the Most Common Canonical Actionable Driver Mutation Associated with Never-Smokers
The most common never-smoker associated actionable driver mutation in NSCLC are the canonical EGFR mutations (deletion 19 and L858R). There is now ample evidence from small scale to randomized phase 3 trial that indicated ICI alone or with chemotherapy has minimal activity in EGFR+ NSCLC with no statistical improvement in PFS or OS.17–20 While much less has been reported on the efficacy of ICI in EGFR exon 20 insertion (EGFRex20ins) mutations, patient characteristics are similar to patients with canonical EGFR mutation.21,22 Thus, it is generally accepted that EGFRex20ins will respond minimally to ICI similar to the canonical EGFR mutations.23 A series of 36 EGFRex20ins patients showed ORR 25% treated with ICI compared to 0% with classic mutations.23 Similarly, PFS with ICI was 2.9 months in EGFRex20ins verses 1.9 months with classic EGFR mutations. Indeed the pivotal registration trials in the first-line setting, of the two drugs approved for treatment of EGFRex20ins, platinum-based chemotherapy is the standard comparison arm not combination of chemotherapy and ICI. For mobocertinib (TAK-788), the pivotal trial (EXCLAIM-2, NCT04129502) is comparing mobocertinib to platinum-based chemotherapy. For amivantamab, the pivotal trial is comparing platinum-based chemotherapy with or without amivantamab (PAPILLON, NCT04538664).
Discussion Point 2. Does Pembrolizumab, Atezolizumab, Nivolumab + Ipilimumab, and Durvalumab + Tremelimumab Work in ROS1+ NSCLC That By FDA Indication Cemiplimab Does Not?
While this seems like a rhetorical question, it is generally believed there is really no discernable difference in efficacy among the current PD-1 and PD-L1 inhibitors in NSCLC. Thus, we would anticipate the six other ICIs would have minimal efficacy in ROS1+ NSCLC. There is much less literature on the role of ICIs in ROS1+ NSCLC. From the 7 ROS1+ NSCLC patients in the immunotarget database,16 only 1 (16.7%) out of 7 patients had responded to ICI therapy. It is generally assumed that oncologist would not prescribe ICIs for ROS1+ NSCLC patients. Nonetheless, the lack of specific FDA exclusion of other ICIs in ROS1+ NSCLC and the absence of negative efficacy data, the exclusion of cemiplimimab may paradoxically encourage a minority of oncologists to try ICIs other than cemiplimab in ROS1+ NSCLC.
Discussion Point 3. What is the Implication of Additional Exclusion of ROS1 Fusion in Order to Use Cemiplimab? Good Science but Bad Business?
Insurance companies in the US are increasingly requesting negative EGFR mutation and ALK fusion results before authorizing the use of ICIs as 1L treatment for NSCLC especially if it is combined with chemotherapy or double ICIs + chemotherapy. Although next-generation sequencing or at least multiplex sequencing platforms commonly used to molecularly profile NSCLC will include ROS1 fusion detection, the requirement to submit a ROS1 fusion negative report can be a detriment for the use of cemiplimab in many regions of the world where only EGFR mutation by polymerase chain reaction (PCR), ALK fusion by Immunohistochemistry (IHC), and PD-L1 expression by IHC were performed. While we agree ICI regimens should not be used as 1L treatment of ROS1+ NSCLC, we think the additional requirement of a negative ROS1 fusion test will dissuade oncologists to order cemiplimab in a treatment landscape where there are well-established and entrenched leaders, such as pembrolizumab. Paradoxically, this may dissuade pharmaceutical sponsors in the future to exclude additional molecular subtypes of NSCLC beyond EGFR+ and ALK+ NSCLC that clearly will not benefit from ICI and set the treatment of NSCLC backwards if FDA follow its traditional approval pathway of how the sponsor designed the trial.
Discussion Point 4. What is the Role of Immunotherapy in RET Fusion-Positive (RET+) NSCLC?+
NSCLC with RET fusion is one of the three most common receptor tyrosine kinases (RTKs). Like ALK and ROS1 fusions, the majority of RET+ NSCLC patients are never-smokers.24 The limited evidence of ICIs in RET+ NSCLC was also from the immunotarget database where the 1 out of 16 (6.3%) RET+ NSCLC patients responded to ICI therapy.16 Currently, there are two pivotal randomized trials comparing the approved RET TKIs, selpercatinib (LIBRETTO-431, NCT04194944) and pralsetinib (AcceleRET-Lung, NCT04222972) to platinum-based chemotherapy with or without pembrolizumab per investigator choice. Thus, the optional inclusion of pembrolizumab into platinum-based chemotherapy indicates the existence of equipoise of the efficacy of adding ICI to chemotherapy in RET+ NSCLC. The results of these two trials will go a long way to address the role of ICI in RET+ NSCLC.
Discussion Point 5. What is the Role of ICIs in HER2 Exon 20 Insertion Positive (HER2+) NSCLC?
Similarly, HER2 exon 20 insertion (HER2ex20ins) is another rare but actionable driver of mutation that has now FDA approved therapy with trastuzumab deruxtecan.25 Efficacy of ICI in HER2ex20ins is limited.26,27 Of the 91 patients with various HER2 mutations, 52 (57%) were never-smokers. Response of HER2ex20ins were examined in the pivotal randomized trial comparing trastuzumab deruxtecan to chemotherapy + ICI based on Keynote-189, which included pembrolizumab (DESTINY-Lung-04, NCT05048797). The chemotherapy regimen did not allow opting out of pembrolizumab. Hence the results of DESTINY-Lung-04 will help us understand any additional efficacy conferred by ICI with comparison to historic results of chemotherapy in likely actionable driver mutation positive NSCLC, but definitive will add toxicities. In this case, the sponsor took the conservative approach and the widely used the standard of care chemotherapy plus ICI regimen (Keynote-189 which only excluded EGFR+ and ALK+ NSCLC) for the comparison arm.
Discussion Point 6. What is the Role of ICI in METex14 Splice Site Mutation Positive NSCLC, BRAF V600E Positive NSCLC, and KRAS G12C+ NSCLC?
Not all actionable driver mutation positive NSCLC are found predominantly in never-smokers. In the FDA approval summary of capmatinib and tepotinib, two specific MET TKI approved for treatment of METex14+ NSCLC, 40% (39/97) of the capmatinib patients reported smoking history and 50% (76/152) of the tepotinib patients were ever-smokers.28 In the FDA approval summary of dabrafenib with or without trametinib for the treatment of BRAF V600E mutated NSCLC, 72.2% (143/198) of the BRAF V600E+ NSCLC patients were ever-smokers. In the FDA approval of sotorasib for KRAS G12C+ NSCLC, only 4.8% (6/126) of the sotorasib-treated KRAS G12C+ NSCLC were never-smokers. Similarly, only 4.3% (5/116) of the adagrasib-treated KRAS G12C+ NSCLC were never-smokers. Thus, a large percentage of these driver mutation positive NSCLC would likely respond to ICI monotherapy or in combination with chemotherapy.
Discussion Point 7. The Use of ICI is Not Prohibited in Resected Early or Locally Advanced NSCLC
The current US FDA indication for the use of ICI as monotherapy as adjuvant treatment for early-stage NSCLC after surgical resection based on IMpower-01029 and Keynote-09130 or as consolidation therapy after definitive chemoradiation based on results of the PACIFIC trial31 did not exclude EGFR+ or ALK+ NSCLC. Subgroup analysis of all three trials did not show any disease-free survival (DFS) benefit29–31 or OS)32 for ALK+ NSCLC. Subgroup analysis also did not show any DFS benefit for EGFR+ NSCLC for two of the three trials29,31 and no OS benefit for EGFR+ NSCLC.32 Indeed, further subgroup analysis of PACIFIC and other regional practice further confirmed consolidation ICI (durvalumab) did not improve OS.33,34 Thus, because FDA approval of any indication is only based on totality of that specific trial overall primary endpoint (not exclusion negative subgroup in positive or approving positive subgroup in a negative trial) result without consideration of existing scientific observations, the “non-exclusion” of ICI in the adjuvant treatment in early and maintenance treatment of locally advanced stage two most common driver mutation positive NSCLC is confusing and contradictory.
Discussion Point 8. Should the FDA Harmonize the Exclusion of ICI to a Set of Driver-Mutation Positive NSCLC Found Primarily in Never-Smokers Regardless of Stage Rather Than Let Sponsor Defined What Driver Mutation to Be Excluded and at What Stage?
At the time the EMPOWER-Lung trials initiated, the majority of data suggested ICIs are ineffective against never-smoker predominant driver mutation positive NSCLC. However, the cemiplimab ROS1+ NSCLC exclusion has inadvertently created a two-tier system for clinical use.
The remaining six ICI agents did not have ROS1+ NSCLC as an exclusion criterion for use. However, we doubt seasoned medical and thoracic oncologists will use ICI alone, ICIs in combination, chemo + IO, or chemo + ICI+ ICI in ROS1+ NSCLC. There exists clear evidence from published literature that ICI does not work on many of the established driver-mutation positive NSCLC (EGFR, ALK, ROS1). Nevertheless, without explicit FDA prohibition against the other six ICIs in ROS1+ NSCLC, less experienced medical professionals may consider their use in ROS1+ NSCLC without evidence of benefit. Furthermore, this prohibition is not extended to earlier stage NSCLC. It is hard to imagine that if ICI is generally not considered effective in stage 4, that the use of ICI is not excluded for use in earlier stage NSCLC especially the overwhelming evidence argues against any significant efficacy by subgroup analysis.
Concluding Remarks
We wrote this editorial fully understanding that FDA approval of each indication depends on the overall design of the trial based on intention to treat patient population. Given both positive EMPOWER lung trials excluded ROS1+ NSCLC in addition to EGFR+/ALK+ NSCLC, cemiplimab indication in the US carries the exclusion of ROS1+ NSCLC in addition to EGFR+/ALK+ NSCLC. However, we also question if specific exclusion of ROS1 fusion from cemiplimab indication may paradoxically encourage some oncologists to use the other six ICIs in ROS1+ NSCLC because no such prohibition existed for ROS1+ NSCLC for these six other ICIs (pembrolizumab, nivolumab, atezolizumab, durvalumab, ipilimumab, and tremelimumab) although there is no reason to believe any of the six ICIs would have appreciable efficacy in ROS1+ NSCLC. From a marketing standpoint, having to provide an additional negative molecular profiling test may be a “bridge too far” for cemiplimab especially if molecular profiling is done sequentially first with EGFR mutation followed by ALK or a small multiplex approach with IHC for PD-L1 and ALK and RT-PCR for EGFR mutations. Although this exclusion may seem like a minor difference in the overall drug indication between cemiplimab and the other six ICIs, it may muddle the tremendous advances in NSCLC by creating two “classes” of ICIs in the treatment of ROS1+ NSCLC. Worse, it may give the impression to some oncologists that is OK to use other ICIs in ROS1+ NSCLC but is likely ineffective. Thus, FDA should consider standardization the indication of ICIs in never-smoker predominant driver-mutation-positive NSCLC, such as ROS1+ NSCLC where currently registration trials for next-generation ALK TKIs.
Disclosure
Dr Saihong Ignatius Ou reports personal fees from Pfizer, JNJ/Janssen, Lilly, AnHeart Therapeutics, personal fees, stock ownership from Elevation Oncology, stock ownership from Turning Point Therapeutics, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. 2016;375(19):1823–1833. doi:10.1056/NEJMoa1606774
2. Mok TSK, Wu YL, Kudaba I, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet. 2019;393(10183):1819–1830. doi:10.1016/S0140-6736(18)32409-7
3. Gandhi L, Rodriguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378(22):2078–2092. doi:10.1056/NEJMoa1801005
4. Paz-Ares L, Luft A, Vicente D, et al. Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N Engl J Med. 2018;379(21):2040–2051. doi:10.1056/NEJMoa1810865
5. Herbst RS, Giaccone G, de Marinis F, et al. Atezolizumab for first-line treatment of PD-L1-selected patients with NSCLC. N Engl J Med. 2020;383(14):1328–1339. doi:10.1056/NEJMoa1917346
6. West H, McCleod M, Hussein M, et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019;20(7):924–937. doi:10.1016/S1470-2045(19)30167-6
7. Socinski MA, Jotte RM, Cappuzzo F, et al. Atezolizumab for first-line treatment of metastatic nonsquamous NSCLC. N Engl J Med. 2018;378(24):2288–2301. doi:10.1056/NEJMoa1716948
8. Sezer A, Kilickap S, Gümüş M, et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: a multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet. 2021;397(10274):592–604. doi:10.1016/S0140-6736(21)00228-2
9. Gogishvili M, Melkadze T, Makharadze T, et al. Cemiplimab plus chemotherapy versus chemotherapy alone in non-small cell lung cancer: a randomized, controlled, double-blind phase 3 trial. Nat Med. 2022;28(11):2374–2380. doi:10.1038/s41591-022-01977-y
10. Hellmann MD, Paz-Ares L, Bernabe Caro R, et al. Nivolumab plus ipilimumab in advanced non-small-cell lung cancer. N Engl J Med. 2019;381(21):2020–2031. doi:10.1056/NEJMoa1910231
11. Paz-Ares L, Ciuleanu TE, Cobo M, et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): an international, randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(2):198–211. doi:10.1016/S1470-2045(20)30641-0
12. Johnson ML, Cho BC, Luft A, et al. Durvalumab with or without tremelimumab in combination with chemotherapy as first-line therapy for metastatic non-small-cell lung cancer: the phase III POSEIDON study. J Clin Oncol. 2023;41(6):1213–1227. doi:10.1200/JCO.22.00975
13. Akinboro O, Larkins E, Pai-Scherf LH, et al. FDA approval summary: pembrolizumab, atezolizumab, and cemiplimab-rwlc as single agents for first-line treatment of advanced/metastatic PD-L1-high NSCLC. Clin Cancer Res. 2022;28(11):2221–2228. doi:10.1158/1078-0432.CCR-21-3844
14. Melkadze T, Gogishvili M, Makharadze T, et al. Cemiplimab plus chemotherapy versus chemotherapy alone in advanced non-small cell lung cancer: 2-year follow-up from the phase 3 EMPOWER-lung 3 part 2 trial. J Thorac. 2023;18(6):755–678.
15. Zhou F, Zhou C. Lung cancer in never smokers-the East Asian experience. Transl Lung Cancer Res. 2018;7(4):450–463. doi:10.21037/tlcr.2018.05.14
16. Mazieres J, Drilon A, Lusque A, et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: results from the IMMUNOTARGET registry. Ann Oncol. 2019;30(8):1321–1328. doi:10.1093/annonc/mdz167
17. Lisberg A, Cummings A, Goldman JW, et al. A phase II study of pembrolizumab in EGFR-mutant, PD-L1+, tyrosine kinase inhibitor naïve patients with advanced NSCLC. J Thorac Oncol. 2018;13(8):1138–1145. doi:10.1016/j.jtho.2018.03.035
18. Nogami N, Barlesi F, Socinski MA, et al. IMpower150 final exploratory analyses for atezolizumab plus bevacizumab and chemotherapy in key NSCLC patient subgroups with EGFR mutations or metastases in the liver or brain. J Thorac Oncol. 2022;17(2):309–323. doi:10.1016/j.jtho.2021.09.014
19. Mok TSK, Nakagawa K, Park K, et al. Nivolumab (NIVO) + chemotherapy vs chemotherapy in patients (pts) with EGFR-mutated metastatic non-small cell lung cancer (mNSCLC) with disease progression after EGFR tyrosine kinase inhibitors (TKIs) in CheckMate 722. Ann Oncol. 2022;33:S1561–S1562. doi:10.1016/j.annonc.2022.10.350
20. Yang JCH, Lee DH, Lee JS. Pemetrexed and platinum with or without pembrolizumab for tyrosine kinase inhibitor (TKI)-resistant, EGFR-mutant, metastatic nonsquamous NSCLC: Phase 3 KEYNOTE-789 study. J Clinic Oncol.2023; 41(17):suppl LBA9000–LBA9000. doi:10.1200/JCO.2023.41.17_suppl.LBA9000
21. Kosaka T, Yatabe Y, Endoh H, et al. Mutations of the epidermal growth factor receptor gene in lung cancer: biological and clinical implications. Cancer Res. 2004;64(24):8919–8923. doi:10.1158/0008-5472.CAN-04-2818
22. Huang SF, Liu HP, Li LH, et al. High frequency of epidermal growth factor receptor mutations with complex patterns in non-small cell lung cancers related to gefitinib responsiveness in Taiwan. Clin Cancer Res. 2004;10(24):8195–8203. doi:10.1158/1078-0432.CCR-04-1245
23. Negrao MV, Reuben A, Robichaux JP, et al. Association of EGFR and HER-2 exon 20 mutations with distinct patterns of response to immune checkpoint blockade in non-small cell lung cancer [abstract]. J Clin Oncol. 2018;36(Suppl. 15):9052. doi:10.1200/JCO.2018.36.15_suppl.9052
24. Lau SCM, Ou SI. And Still They Come Over Troubled Waters: Can Asia’s Third-Generation EGFR Tyrosine Kinase Inhibitors (Furmonertinib, Aumolertinib, Rezivertinib, Limertinib, Befotertinib, SH-1028, and Lazertinib) Affect Global Treatment of EGFR+ NSCLC. J Thorac Oncol. 2022;17(10):1144–1154. doi:10.1016/j.jtho.2022.08.016
25. Guisier F, Dubos-Arvis C, Viñas F, et al. Efficacy and safety of anti-PD-1 immunotherapy in patients with advanced non-small cell lung cancer with BRAF, HER2, or MET mutation or RET-translocation. GFPC 01-2018. J Thorac Oncol. 2020;15:628–636. doi:10.1016/j.jtho.2019.12.129
26. Li BT, Smit EF, Goto Y, et al. Trastuzumab deruxtecan in HER2-mutant non-small-cell lung cancer. N Engl J Med. 2022;386(3):241–251. doi:10.1056/NEJMoa2112431
27. Lau SCM, Fares AF, Le LW, et al. Subtypes of EGFR- and HER2- mutant metastatic NSCLC influence response to immune checkpoint inhibitors. Clin Lung Cancer. 2021;22:253–259. doi:10.1016/j.cllc.2020.12.015
28. Mathieu LN, Larkins E, Akinboro O, et al. FDA approval summary: capmatinib and tepotinib for the treatment of metastatic NSCLC harboring MET exon 14 skipping mutations or alterations. Clin Cancer Res. 2022;28(2):249–254. doi:10.1158/1078-0432.CCR-21-1566
29. Felip E, Altorki N, Zhou C, et al. Adjuvant atezolizumab after adjuvant chemotherapy in resected stage IB-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase 3 trial. Lancet. 2021;398(10308):1344–1357. doi:10.1016/S0140-6736(21)02098-5
30. O’Brien M, Paz-Ares L, Marreaud S, et al. Pembrolizumab versus placebo as adjuvant therapy for completely resected stage IB-IIIA non-small-cell lung cancer (PEARLS/KEYNOTE-091): an interim analysis of a randomised, triple-blind, phase 3 trial. Lancet Oncol. 2022;23(10):1274–1286. doi:10.1016/S1470-2045(22)00518-6
31. Antonia SJ, Villegas A, Daniel D, et al. Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N Engl J Med. 2017;377(20):1919–1929. doi:10.1056/NEJMoa1709937
32. Antonia SJ, Villegas A, Daniel D, et al. Overall survival with durvalumab after chemoradiotherapy in stage III NSCLC. N Engl J Med. 2018;379(24):2342–2350. doi:10.1056/NEJMoa1809697
33. Naidoo J, Antonia S, Wu YL, et al. Brief report: durvalumab after chemoradiotherapy in unresectable stage III EGFR-mutant NSCLC: a post-hoc subgroup analysis from PACIFIC. J Thorac Oncol. 2023. doi:10.1016/j.jtho.2023.02.009
34. Nindra U, Shahnam A, Stevens S, et al. Influence of EGFR mutation status and PD-L1 expression in stage III unresectable non-small cell lung cancer treated with chemoradiation and consolidation durvalumab. Asia Pac J Clin Oncol. 2023. doi:10.1111/ajco.13940
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Cemiplimab for the Treatment of Advanced Cutaneous Squamous Cell Carcinoma: Appropriate Patient Selection and Perspectives
Mager L, Gardeen S, Carr DR, Shahwan KT
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2135-2142
Published Date: 9 August 2023