")
Back to Journals » Infection and Drug Resistance » Volume 16
The Activities of Antimicrobials Against Stenotrophomonas maltophilia Isolates and Evaluation of Clinical Outcomes Among Treatment Regimens in Patients with Stenotrophomonas maltophilia Infections: A Retrospective Multicenter Cohort Study
Authors Boonmee P, Nasomsong W , Lorchirachoonkul N, Pungcharoenkijkul S, Juntanawiwat P, Chaemchaeng S, Santimaleeworagun W
Received 11 April 2023
Accepted for publication 12 July 2023
Published 9 August 2023 Volume 2023:16 Pages 5173—5184
DOI https://doi.org/10.2147/IDR.S416678
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Patchrapa Boonmee,1,2 Worapong Nasomsong,3 Narisorn Lorchirachoonkul,4 Supanun Pungcharoenkijkul,5 Piraporn Juntanawiwat,6 Suphatthra Chaemchaeng,7 Wichai Santimaleeworagun8,9
1College of Pharmacotherapy Thailand, Nonthaburi, Thailand; 2Department of Pharmacy, Ratchaburi Hospital, Ratchaburi, Thailand; 3Division of Infectious Diseases, Department of Internal Medicine, Phramongkutklao Hospital and College of Medicine, Bangkok, Thailand; 4Department of Medicine, Ratchaburi Hospital, Ratchaburi, Thailand; 5Pharmacy Unit, Nopparat Rajathanee Hospital, Bangkok, Thailand; 6Division of Microbiology, Phramongkutklao Hospital, Bangkok, Thailand; 7Division of Microbiology, Ratchaburi Hospital, Ratchaburi, Thailand; 8Department of Pharmaceutical Care, Faculty of Pharmacy, Silpakorn University, Nakorn Pathom, Thailand; 9Pharmaceutical Initiative for Resistant Bacteria and Infectious Disease Working Group (PIRBIG), Nakorn Pathom, Thailand
Correspondence: Wichai Santimaleeworagun, Department of Pharmaceutical Care, Faculty of Pharmacy, Silpakorn University, Nakorn Pathom, 73000, Thailand, Tel +66 3 425 5800, Fax +66 3 425 5801, Email [email protected]
Purpose: Stenotrophomonas maltophilia, a multidrug-resistant pathogen can cause hospital-acquired infections such as pneumonia, or bloodstream infection. S. maltophilia infection is associated with high mortality rates. This retrospective study examined the antimicrobial susceptibility profile of clinical S. maltophilia isolates and evaluated clinical outcomes, treatment regimens, and risk factors associated with 30-day mortality or treatment failure of S. maltophilia infections at three tertiary care hospitals in Central Thailand.
Patients and Methods: The characteristics, microbiological data, and clinical treatment outcomes were derived from medical records obtained from three tertiary care hospitals in Central Thailand from January 2017 to October 2022. The primary outcomes were treatment failure and 30-day mortality. The antimicrobial susceptibility rates of trimethoprim-sulfamethoxazole (TMP-SMX), levofloxacin, and ceftazidime were determined by minimum inhibitory concentration (MIC), which were based on broth microdilution and clear zone diameters using the disk diffusion method. However, we also report the susceptibility of minocycline and tigecycline in some clinical S. maltophilia strains (n = 149) and determined by MIC with E-test method.
Results: The antimicrobial susceptibility rates to TMP-SMX, levofloxacin, and ceftazidime were 97.1%, 93%, and 55.3%, respectively. The treatment failure rate and 30-day mortality were 66.3% and 49%, respectively. Significant factors associated with treatment failure included APACHE II score ≥ 15 (OR 3.37, 95% confidence interval (CI) 1.46– 7.76), polymicrobial infections (OR 3.20, 95% CI 1.35– 7.55). The significant factors associated with reduced treatment failure was treatment with TMP-SMX-based regimen (OR 0.29, 95% CI 0.11– 0.76). The 30-day mortality rate was associated with APACHE II score ≥ 15 (OR 3.27, 95% CI 1.45– 7.39) and septic shock (OR 2.53, 95% CI 1.36– 4.69).
Conclusion: The results indicate a high mortality rate for S. maltophilia infection. The predictive factors for an unfavourable outcome were severity of illness, septic shock, and non-use of TMP-SMX. Therefore, a TMP-SMX-based regimen is recommended for the treatment of S. maltophilia infections.
Keywords: co-trimoxazole, levofloxacin, mortality, Xanthomonas
Introduction
Stenotrophomonas maltophilia (formerly Xanthomonas maltophilia) is a lactose non-fermenting, aerobic gram-negative bacilli that lives in an aqueous-environment. It frequently colonizes on surfaces in a hospital environment, medical equipment, dialysis solutions, and overgrows in settings of broad-spectrum antibiotic use.1–3 S. maltophilia is a multidrug-resistant pathogen and remains problematic worldwide. It is associated with hospital-acquired infections, particularly pneumonia, followed by bloodstream infections. It is rarely associated with intraabdominal, urinary tract, or skin/soft tissue infections.4 Based on a previous systematic review in 2008, the overall mortality rate of S. maltophilia infections ranges from 21 to 69%.5
Risk factors for S. maltophilia infection include broad-spectrum antibiotics, admission to the intensive care unit (ICU), mechanical ventilator use, chronic respiratory diseases, haemodialysis, indwelling prosthetic devices, such as a central venous catheter, and immunocompromised status.6–10 S. maltophilia is difficult to treat due to it can form a biofilm which is a crucial factor in the adherence of bacteria and protection from antimicrobial agents.11 It also exhibits intrinsic resistance to various classes of antimicrobial agents, particularly β-lactams and aminoglycosides.12–14
The mainstay treatment of S. maltophilia infection is trimethoprim-sulfamethoxazole (TMP-SMX), which exhibits activity in respiratory tract samples and blood cultures (>90%), based on retrospectively reviewed 10-year data.15–17 According to the Infectious Disease Society of America Guidance on the Treatment of S. maltophilia Infections,18 the general approach for treating S. maltophilia infection may be divided into two approaches. First, monotherapy with TMP-SMX, minocycline, tigecycline, levofloxacin, or cefiderocol is preferred for mild infection. Second, for moderate-to-severe infection, combination therapy with at least two of the above drugs is recommended until clinical improvement or treatment with TMP-SMX and adding a second agent if no response is observed. The use of ceftazidime is not recommended for the treatment of S. maltophilia regardless of severity, because S. maltophilia exhibits intrinsic β-lactamase production, which inactivates ceftazidime.18
There is a limitation to using TMP-SMX if a patient has a history of severe drug hypersensitivity, including Steven’s Johnson syndrome, toxic epidermal necrolysis rendering the patient intolerable, or increased drug resistance.19–22 In 2020, the National Antimicrobial Resistant Surveillance Centre of Thailand (NARST) reported the resistance of S. maltophilia to TMP-SMX of 6.6%–7.7%.23 Therefore, levofloxacin was considered as the alternative treatment. The NARST also reported increasing fluoroquinolone-resistance of 10–12%,23 although several studies have shown that treatment efficacy with fluoroquinolones was similar to that of TMP-SMX.24–26
High mortality rates, clinical characteristics, and treatment outcomes of S. maltophilia infections have been rarely reported, including in Thailand. Moreover, the optimal treatment regimens for S. maltophilia infection have not been clearly elucidated. In this study, we assessed the antimicrobial susceptibility profile of clinical S. maltophilia isolates and evaluated clinical outcomes, treatment regimens, and risk factors associated with 30-day mortality and treatment failure.
Materials and Methods
Study Design and Participants
This was a multicenter retrospective study. The characteristics, microbiological data, and clinical treatment outcomes were derived from medical records available from three tertiary care hospitals in Central Thailand from January 2017 to October 2022. S. maltophilia isolates were collected from sterile and non-sterile sites. All patients ≥20 years old were diagnosed with infection according to the definition of the Centers for Disease Control and Prevention/National Healthcare Safety Network (CDC/NHSN) surveillance definitions for specific types of infections.27 They also experienced a first episode of S. maltophilia infection with a positive culture and complete medical records were eligible.
Ethics Approval
This study was approved by all study centres including the Institutional Review Board Royal Thai Army Medical Department at Phramongkutklao College of Medicine and Phramongkutklao Hospital (Approval number Q029h/64), Declaration of Helsinki, The Belmont Report, CIOMS Guideline International Conference on Harmonization in Good Clinical Practice at the Ratchaburi Hospital (Approval number COA-RBHEC 030/2021), and the Research and Ethics committee of the Nopparat Rajathanee Hospital (Approval number 3/2565, 5/2566). The informed consent was waived by the Institutional Review Board, due to retrospective design and deidentification of patient data.
Data Collection and Treatment Outcomes
The demographic and clinical variable data including age, gender, body weight, serum creatinine, serum albumin, hospitalization unit, co-morbidities, critically ill status, immunocompromised status, source of infection, antimicrobial therapy (drug, dosing regimen), invasive medical devices, treatment outcomes, and in-hospital mortality were obtained from medical records. The primary outcome was treatment failure and 30-day mortality.
Bacterial Identification and Antimicrobial Susceptibility
All of the clinical isolates were identified as S. maltophilia by Microflex LT MALDITOF-MS. Antimicrobial susceptibility testing was performed using the SensititreTM Aris HiQ System (broth microdilution method) or the Kirby-Bauer disk diffusion method. The results of minimum inhibitory concentration (MIC) were based on broth microdilution, and clear zone diameters were determined by the disk diffusion method. However, we also report the susceptibility testing of minocycline and tigecycline in some clinical S. maltophilia strains (n = 149) by using Epsilometer method (E-test).
The antimicrobial susceptibility was interpreted by the Clinical and Laboratory Standards Institute version 2022 (CLSI).28 Isolates were interpreted as “susceptible”, “intermediate”, or “resistant” to TMP-SMX, levofloxacin, ceftazidime and minocycline, while tigecycline was reported as MIC50 and MIC90 values, respectively, due to no susceptible breakpoints in the CLSI.
Definitions
Empirical antibiotic therapy was defined as the first agents prescribed for the initial treatment which is effective or not on S. maltophilia. Documented antibiotic therapy was defined as the administration of the drug corresponding to the susceptibility of S. maltophilia stains. Monotherapy was defined as the administration of a documented regimen of either TMP-SMX, levofloxacin, ceftazidime, or tigecycline which is susceptible for S. maltophilia isolates for at least 48 hours following diagnosis of an S. maltophilia infection. Combination therapy was defined as a patient receiving a documented regimen of either TMP-SMX or levofloxacin in combination with another active agent or susceptible, such as minocycline, ceftazidime, tigecycline or a combination of TMP-SMX with levofloxacin. Creatinine clearance was calculated by the Cockcroft–Gault equation. Acute Physiology and Chronic Health Evaluation II (APACHE II) and Sequential Organ Failure Assessment (SOFA) scores29 were assessed from the data from all patients regardless of ICU status. The Charlson comorbidity score (CCI)30 was calculated from comorbidity data extracted from medical records. Chronic respiratory diseases included chronic obstructive pulmonary disease (COPD), asthma, pulmonary fibrosis, cystic fibrosis, interstitial lung disease or lung cancer.31 Septic shock was defined as life-threatening organ dysfunction, serum lactate levels >2 mmol/L, persisting hypotension despite adequate volume resuscitation, which required a vasopressor to maintain mean arterial pressure >65 mmHg.32 Immunocompromised status was defined as a weakened immune system including immunosuppressant use, chemotherapy treatment, active treatment with high-dose systemic corticosteroids (eg, prednisolone 20 mg per day more than or equal 2 weeks), or HIV infection.33,34
Appropriate antibiotic agent was defined as the treatment of S. maltophilia with at least 1 active agent corresponding to the result of antimicrobial susceptibility of S. maltophilia isolate. Contrarily, inappropriate antibiotic agent was defined as a patient who received inactive agents against S. maltophilia based on antimicrobial susceptibility report. Treatment failure was defined as all causes of in-hospital mortality required to change or add alternative antimicrobial agents with in vitro susceptibility to S. maltophilia during therapy or positive repeat cultures after appropriate treatment within 72 h.35,36
Statistical Analysis
Demographics and clinical treatment outcomes were analysed using the statistical software SPSS for Windows version 27 (IBM Corp., Armonk, NY, USA). Patient data and clinical characteristics were analysed with descriptive statistics. Continuous variables were tested using a Student’s t-test or Mann–Whitney U-test. Categorical variables were tested using Chi-square or Fisher’s exact test. Logistic regression analysis was used to determine factors associated with treatment failure and 30-day mortality. The Log rank test was used to analyse survival data. Variables with a P value <0.1 by univariate analysis were subsequently entered into logistic regression models. P values <0.05 were considered statistically significant.
Results
Baseline Characteristics of Patients and Infections
Baseline characteristics of the patients and outcomes are listed in Table 1. Patients (n = 208) with a positive culture from January 2017 to October 2022 who met the definition for a specific type of infection were eligible for this study.27 The median age was 69 years, 60% were male, 51.9% had septic shock, 71.6% were on a mechanical ventilator, and 18.8% were immunocompromised. The median CCI score was 5. The median severity scores assessed by the APACHE II and SOFA score were 19 and 6, respectively. One-hundred and sixty-nine patients (81.3%) received documented therapy for S. maltophilia infection, whereas 39 patients (18.8%) received inactive treatment regimens. The most common infections were pneumonia 61.1% followed by bloodstream infection 33.2%. Among 208 cases of S. maltophilia infection, 46.2% were mono-microbial infections.
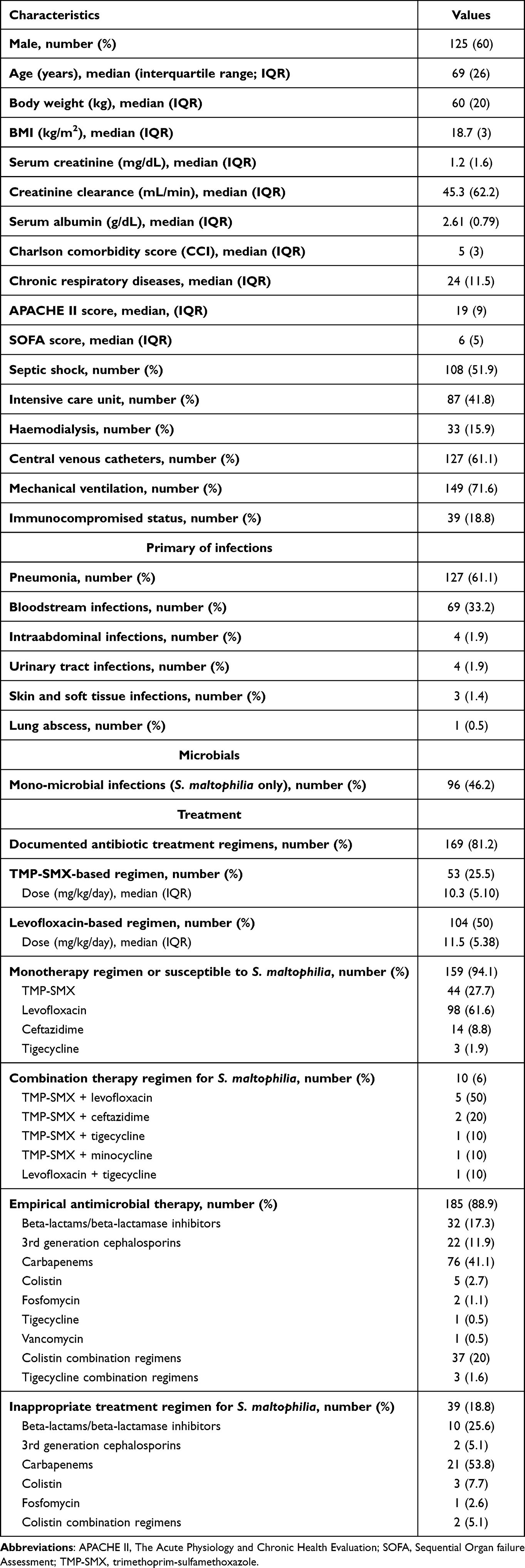 |
Table 1 Characteristics of Patients with S. maltophilia Infection (n = 208) |
Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing of 208 S. maltophilia clinical isolates revealed 97.1% susceptibility to TMP-SMX, 93% susceptibility to levofloxacin, and 55.3% susceptibility to ceftazidime. About 149 clinical isolates revealed 100% susceptibility to minocycline with and MIC50 and MIC90 of tigecycline were 0.25 and 0.75 µg/mL, respectively.
Risk Factors Associated with S. maltophilia Infections and Treatment Outcomes
The treatment outcomes are shown in Table 2. The treatment failure and 30-day mortality rates were 66.3% and 49%, respectively. The microbiological cure rate was 100% among patients with bloodstream infections who repeat hemoculture (n = 63 cases). Comparing survival among the patient characteristics, the significant factors associated with 30-day mortality were age ≥69 years, hypoalbuminemia (<2.5 g/dL), CCI score >5, APACHE II ≥15, mechanical ventilation, and septic shock (Table 3).
 |
Table 2 The Treatment Outcomes of S. maltophilia Infections (n = 208) |
 |
Table 3 Factor Associated with Treatment Failure and 30-Day in Hospital Mortality of S. maltophilia Infections |
Among antimicrobial treatment regimens, for the TMP-SMX-based versus levofloxacin-based regimen, the former was associated with significant factors for reducing treatment failure (Table 3). For dose regimens of both TMP-SMX or levofloxacin, mono or combination therapy, appropriate antibiotic agent or inappropriate antibiotic agent were not significant factors associated with 30-day mortality. However, the use of appropriate antibiotic agents against S. maltophilia tended to reduce the treatment failure rate compared with the use of inappropriate antibiotic agents (p = 0.099).
Factors Associated with 30-Day Mortality and Survival Time
Based on a logistic regression analysis, the significant factors associated with treatment failure were APACHE II score ≥15 (OR 3.37, 95% CI 1.46–7.76), polymicrobial infections (OR 3.20 95% CI 1.35–7.55), whereas use of a TMP-SMX-based regimen was significant to reduce treatment failure (OR 0.29, 95% CI 0.11–0.76). The 30-day mortality rate was associated with an APACHE II score ≥15 (OR 3.27, 95% CI 1.45–7.39) and septic shock (OR 2.53, 95% CI 1.36–4.69) (Table 3).
In a comparison of the Kaplan–Meier survival curves for treatment failure among the treatment regimens, we found that a TMP-SMX-based regimen was superior to a levofloxacin-based regimen (p <0.001) (Figure 1).
 |
Figure 1 Kaplan–Meier survival curve for treatment failure following the TMP-SMX and levofloxacin-based regimens. |
Discussion
The characteristics, treatment outcomes, and factors associated with 30-day mortality were few reported in Thailand. Our study included 208 isolates of S. maltophilia, which were collected at three tertiary care hospitals in the centre of Thailand from January 2017 to October 2022. Isolates were collected from sterile and non-sterile sites with a diagnosis of S. maltophilia infection.
S. maltophilia is challenging to eradicate because there are only a few antimicrobial treatment options. Previous studies indicated that S. maltophilia infection is associated with high mortality rates ranging from 21% to 69%. In this study, the 30-day mortality rate was 49%, which is consistent with the previous study.35,37–41
Consistent with the increasing emergence of resistance described in previous reports,15–17 the susceptibility rates to TMP-SMX and levofloxacin were 97.1% and 93%, respectively, in the present study. These susceptibility rates were similar to that reported by NARST in 2020, whereas the susceptibility rate of ceftazidime was low (55.3%). Thus, for the treatment of S. maltophilia infections in Thailand, TMP-SMX and levofloxacin are the recommended treatment options.
Among the hospitalized patients in this study, the most frequent S. maltophilia infections were pneumonia (61.1%) followed by bloodstream infections (33.2%). The baseline characteristics of patients in this study included chronic respiratory diseases (11.5%), immunocompromised status (18.8%) intensive care unit admission (41.8%), haemodialysis (15.9%), central venous catheters (61.1%), septic shock (51.9%), and mechanical ventilation (71.6%). The patients with severe illness had median APACHE II and SOFA scores of 19 and 6, respectively, which was similar to that of previous studies in which APACHE II and SOFA scores were 19 and 9, respectively.35,37–41
Several risk factors including ICU admission, broad-spectrum antibiotics, chronic respiratory disease, haemodialysis, central venous catheter and immunocompromised status were risk factors associated with mortality rates of S. maltophilia infections in previous studies.6–10 However, our analysis found that these risk factors had no statistically significant association with mortality rates.
Risk factors have been associated with mortality to S. maltophilia infection in prior studies, including mechanical ventilator use, admission to the ICU, septic shock, high APACHE II score ≥15, prolonged hospitalization, administration of broad-spectrum antimicrobials, and immunosuppressive status. However, there were also variables that we did not observe, such as admission to the ICU, prolonged hospitalization, immunocompromised status, and administration of broad-spectrum antibiotics.5,42
Risk factors significantly associated with 30-day mortality were APACHEII score ≥15 and septic shock. Furthermore, we found that a TMP-SMX-based regimen group was a protective factor for reduced 30-day mortality and treatment failure based on a logistic regression analysis. Kaplan–Meier survival curves showed a significant difference for the TMP-SMX-based regimen compared with levofloxacin-based regimen. From the meta-analysis and a systematic review,43 there was no statistically significant difference between TMP-SMX and levofloxacin. In the present study, we defined a broader scope of treatment outcomes in terms of treatment failure, which contributed to a greater difference between regimens. However, further well-designed studies are needed to corroborate this data.
Comparison of the dosing regimens, ≥10 or <10 mg/kg/day of trimethoprim was not significantly associated with mortality. We found significant treatment failure in the levofloxacin-based treatment group, which has been associated with higher mortality because of a higher severity of illness compared with a TMP-SMX-based regimen group.
Of the regimens, combination therapy has been used to improve clinical outcomes against isolates with limited therapeutic options or drug-resistant strains. In this study, only ten patients (6%) received combination therapy. Combination therapy was dependent on the severity of the illness, drug susceptibility in vitro, and designed to exhibit synergistic activity; therefore, the clinical outcome data for combination therapy were limited. However, from the results of this study, we recommend a TMP-SMX-based regimen with or without other additional agents to improve treatment outcomes for S. maltophilia infections. However, our study would like to support a robust data according to the Infectious Disease Society of America Guidance on the Treatment of S. maltophilia Infections about prefer using co-trimoxazole in mainstay of therapy either as monotherapy or preferably in combination with another active agent more than levofloxacin. Although our results for combination and monotherapy were not significantly different, there is a role for combination therapy in more favourable outcomes according to the current guidelines.18
This study had a limitation. The number of patients who received combination therapy was small, so we could not clearly assess the difference in mortality rate or treatment failure between monotherapy and combination therapy.
Conclusion
The results indicate a high mortality rate for S. maltophilia infection The predictive factors for an unfavourable outcome were severity of illness, septic shock, and non-use of TMP-SMX. Therefore, a TMP-SMX-based regimen is recommended for the treatment of S. maltophilia infections.; however, further studies are needed to confirm these data.
Acknowledgments
We thank the Phramongkutklao Hospital, Ratchaburi Hospital, and Nopparat Rajathanee Hospital for access to electronic medical records.
Funding
This research project is supported by Kasem Pungsriwong Foundation.
Disclosure
The authors report no conflicts of interest.
References
1. Loscalzo J, Kasper D, Hauser S, Longo D, Jameson J. Harrison’s Principles of Internal Medicine. McGraw Hill; 2022.
2. Adegoke AA, Stenstrom TA, Okoh AI. Stenotrophomonas maltophilia as an emerging ubiquitous pathogen: looking beyond contemporary antibiotic therapy. Front Microbiol. 2017;8:2276. doi:10.3389/fmicb.2017.02276
3. Brooke JS. Stenotrophomonas maltophilia: an emerging global opportunistic pathogen. Clin Microbiol Rev. 2012;25(1):2–41. doi:10.1128/CMR.00019-11
4. Hafiz TA, Aldawood E, Albloshi A, et al. Stenotrophomonas maltophilia epidemiology, resistance characteristics, and clinical outcomes: understanding of the recent three years’ trends. Microorganisms. 2022;10(12):2506. doi:10.3390/microorganisms10122506
5. Paez JI, Costa SF. Risk factors associated with mortality of infections caused by Stenotrophomonas maltophilia: a systematic review. J Hosp Infect. 2008;70(2):101–108. doi:10.1016/j.jhin.2008.05.020
6. Nseir S, Di Pompeo C, Brisson H, et al. Intensive care unit-acquired Stenotrophomonas maltophilia: incidence, risk factors, and outcome. Crit Care. 2006;10(5):R143. doi:10.1186/cc5063
7. Jeon YD, Jeong WY, Kim MH, et al. Risk factors for mortality in patients with Stenotrophomonas maltophilia bacteremia. Medicine. 2016;95(31):e4375.
8. Wang N, Tang C, Wang L. Risk factors for acquired Stenotrophomonas maltophilia pneumonia in intensive care unit: a systematic review and meta-analysis. Front Med. 2021;8:808391. doi:10.3389/fmed.2021.808391
9. Jian J, Xie Z, Chen L. Risk factors for mortality in hospitalized patients with Stenotrophomonas maltophilia bacteremia. Infect Drug Resist. 2022;15:3881–3886.
10. Chen Y, Suo J, Du M, et al. Clinical features, outcomes, and risk factors of bloodstream infections due to stenotrophomonas maltophilia in a tertiary-care hospital of china: a retrospective analysis. Biomed Res Int. 2019;2019:4931501. doi:10.1155/2019/4931501
11. Flores-Trevino S, Bocanegra-Ibarias P, Camacho-Ortiz A, et al. Stenotrophomonas maltophilia biofilm: its role in infectious diseases. Expert Rev Anti Infect Ther. 2019;17(11):877–893. doi:10.1080/14787210.2019.1685875
12. Tan CK, Liaw S-J, Yu C-J, et al. Extensively drug-resistant Stenotrophomonas maltophilia in a tertiary care hospital in Taiwan: microbiologic characteristics, clinical features, and outcomes. Diagn Microbiol Infect Dis. 2008;60(2):205–210. doi:10.1016/j.diagmicrobio.2007.09.007
13. Gil-Gil T, Martínez JL, Blanco P. Mechanisms of antimicrobial resistance in Stenotrophomonas maltophilia: a review of current knowledge. Expert Rev Anti Infect Ther. 2020;18(4):335–347. doi:10.1080/14787210.2020.1730178
14. Sánchez MB. Antibiotic resistance in the opportunistic pathogen Stenotrophomonas maltophilia. Front Microbiol. 2015;6:658. doi:10.3389/fmicb.2015.00658
15. Gajdacs M, Urban E. Prevalence and antibiotic resistance of Stenotrophomonas maltophilia in respiratory tract samples: a 10-year epidemiological snapshot. Health Serv Res Manag Epidemiol. 2019;6:2333392819870774. doi:10.1177/2333392819870774
16. Gajdacs M, Urban E. Epidemiological trends and resistance associated with Stenotrophomonas maltophilia bacteremia: a 10-year retrospective cohort study in a tertiary-care hospital in Hungary. Diseases. 2019;7(2):41. doi:10.3390/diseases7020041
17. Hamdi AM, Fida M, Abu Saleh OM, et al. Stenotrophomonas bacteremia antibiotic susceptibility and prognostic determinants: mayo clinic 10-year experience. Open Forum Infect Dis. 2020;7(1):ofaa008. doi:10.1093/ofid/ofaa008
18. Tamma PD, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious Diseases Society of America guidance on the treatment of ampc β-lactamase-producing Enterobacterales, carbapenem-resistant Acinetobacter baumannii, and Stenotrophomonas maltophilia infections. Clin Infect Dis. 2022;2022:1.
19. Hu L-F, Chang X, Ye Y, et al. Stenotrophomonas maltophilia resistance to trimethoprim/sulfamethoxazole mediated by acquisition of sul and dfrA genes in a plasmid-mediated class 1 integron. Int J Antimicrob Agents. 2011;37(3):230–234. doi:10.1016/j.ijantimicag.2010.10.025
20. Al-Jasser AM. Stenotrophomonas maltophilia resistant to trimethoprim-sulfamethoxazole: an increasing problem. Ann Clin Microbiol Antimicrob. 2006;5:23. doi:10.1186/1476-0711-5-23
21. Baseri Z, Dehghan A, Yaghoubi S, et al. Prevalence of resistance genes and antibiotic resistance profile among Stenotrophomonas maltophilia isolates from hospitalized patients in Iran. New Microbes New Infect. 2021;44:100943. doi:10.1016/j.nmni.2021.100943
22. Thong BY-H, Lucas M, Kang H-R, et al. Drug hypersensitivity reactions in Asia: regional issues and challenges. Asia Pac Allergy. 2020;10(1):e8. doi:10.5415/apallergy.2020.10.e8
23. Ministry of public health. National antimicrobial resistant surveillance center Thailand; 2023. Available from: http://narst.dmsc.moph.go.th/.
24. Cho SY, Kang C-I, Kim J, et al. Can levofloxacin be a useful alternative to trimethoprim-sulfamethoxazole for treating Stenotrophomonas maltophilia bacteremia? Antimicrob Agents Chemother. 2014;58(1):581–583. doi:10.1128/AAC.01682-13
25. Sarzynski SH, Warner S, Sun J, et al. Trimethoprim-Sulfamethoxazole versus levofloxacin for stenotrophomonas maltophilia infections: a retrospective comparative effectiveness study of electronic health records from 154 US hospitals. Open Forum Infect Dis. 2022;9(2):ofab644. doi:10.1093/ofid/ofab644
26. Watson L, Esterly J, Jensen AO, et al. Sulfamethoxazole/trimethoprim versus fluoroquinolones for the treatment of Stenotrophomonas maltophilia bloodstream infections. J Glob Antimicrob Resist. 2018;12:104–106. doi:10.1016/j.jgar.2017.09.015
27. National Healthcare Safety Network (NHSN). CDC/NHSN surveillance definitions for specific types of infections; 2023. Available from: https://www.cdc.gov/nhsn/pdfs/pscmanual/17pscnosinfdef_current.pdf.
28. CLSI. Performance Standards for Antimicrobial Susceptibility Testing M100.
29. Naqvi IH, Mahmood K, Ziaullaha S, et al. Better prognostic marker in ICU - APACHE II, SOFA or SAP II! Pak J Med Sci. 2016;32(5):1146–1151. doi:10.12669/pjms.325.10080
30. Charlson ME, Carrozzino D, Guidi J, et al. Charlson comorbidity index: a critical review of clinimetric properties. Psychother Psychosom. 2022;91(1):8–35. doi:10.1159/000521288
31. Shukla SD, Vanka KS, Chavelier A, et al. Chronic respiratory diseases: an introduction and need for novel drug delivery approaches. In: Targeting Chronic Inflammatory Lung Diseases Using Advanced Drug Delivery Systems. Academic Press; 2020:1–31.
32. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–1247. doi:10.1007/s00134-021-06506-y
33. Center for Disease Control and Prevention (CDC). People who are immunocompromised; 2023. Available from: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-who-are-immunocompromised.html.
34. Mahon JL, Stiller CR. The immunocompromised patient. Can Fam Physician. 1987;33:349–359.
35. Guerci P, Bellut H, Mokhtari M, et al. Outcomes of Stenotrophomonas maltophilia hospital-acquired pneumonia in intensive care unit: a nationwide retrospective study. Crit Care. 2019;23(1):371. doi:10.1186/s13054-019-2649-5
36. Keck JM, Perkins N, Adams D, et al. 1304. antimicrobial management of Stenotrophomonas maltophilia pneumonia: does TMP-SMX dose affect treatment failure? Open Forum Infect Dis. 2021;8(Suppl 1):740. doi:10.1093/ofid/ofab466.1496
37. Junco SJ, Bowman MC, Turner RB. Clinical outcomes of Stenotrophomonas maltophilia infection treated with trimethoprim/sulfamethoxazole, minocycline, or fluoroquinolone monotherapy. Int J Antimicrob Agents. 2021;58(2):106367. doi:10.1016/j.ijantimicag.2021.106367
38. Insuwanno W, Kiratisin P, Jitmuang A. Stenotrophomonas maltophilia infections: clinical characteristics and factors associated with mortality of hospitalized patients. Infect Drug Resist. 2020;13:1559–1566. doi:10.2147/IDR.S253949
39. Tuncel T, Akalın H, Payaslıoğlu M, et al. Healthcare-associated stenotrophomonas maltophilia bacteraemia: retrospective evaluation of treatment and outcome. Cureus. 2021;13(10):e18916. doi:10.7759/cureus.18916
40. Kanchanasuwan S, Rongmuang J, Siripaitoon P, et al. Clinical characteristics, outcomes, and risk factors for mortality in patients with Stenotrophomonas maltophilia bacteremia. J Clin Med. 2022;11(11):3085. doi:10.3390/jcm11113085
41. Shah MD, Coe KE, El Boghdadly Z, et al. Efficacy of combination therapy versus monotherapy in the treatment of Stenotrophomonas maltophilia pneumonia. J Antimicrob Chemother. 2019;74(7):2055–2059. doi:10.1093/jac/dkz116
42. Xun M, Zhang Y, Li B-L, Wu M, Zong Y, Yin Y-M. Clinical characteristics and risk factors of infections caused by Stenotrophomonas maltophilia in a hospital in northwest China. J Infect Dev Ctries. 2014;8:1000–1005. doi:10.3855/jidc.4236
43. Ko JH, Kang CI, Cornejo-Juárez P, et al. Fluoroquinolones versus trimethoprim-sulfamethoxazole for the treatment of Stenotrophomonas maltophilia infections: a systematic review and meta-analysis. Clin Microbiol Infect. 2019;25(5):546–554. doi:10.1016/j.cmi.2018.11.008
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.