")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Ability of Emergency Medical Service Staff to Predict Emergency Department Disposition: A Prospective Study
Authors Alghamdi A , Alshibani A , Binhotan M, Alsabani M, Alotaibi T, Alharbi R, Alabdali A
Received 15 June 2023
Accepted for publication 17 July 2023
Published 26 July 2023 Volume 2023:16 Pages 2101—2107
DOI https://doi.org/10.2147/JMDH.S423654
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Abdulrhman Alghamdi,1,2 Abdullah Alshibani,1,2 Meshary Binhotan,1,2 Mohmad Alsabani,2,3 Tareq Alotaibi,2,4 Rayan Alharbi,5 Abdullah Alabdali1,2
1Emergency Medical Services Department, College of Applied Medical Sciences, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 2King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 3Anesthesia Technology Department, College of Applied Medical Sciences, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 4Respiratory Therapy Department, College of Applied Medical Sciences, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 5Department of Emergency Medical Service, College of Applied Medical Sciences, Jazan University, Jazan, Saudi Arabia
Correspondence: Abdulrhman Alghamdi, Emergency Medical Services Department, College of Applied Medical Sciences, King Saud Bin Abdulaziz University for Health Sciences, P.O. Box.3660, Riyadh, 11481, Saudi Arabia, ; +96611 429 51986, Email [email protected]
Purpose: Paramedics’ decision to notify receiving hospitals and transport patients to an appropriate healthcare facility is based on the Prediction of Intensive Care Unit (ICU) and Hospital Admissions guide. This study aimed to assess the paramedics’ gestalt on both ward and ICU admission.
Patients and Methods: A prospective study was conducted at King Abdulaziz Medical City between September 2021 and March 2022. Paramedics were asked several questions related to the prediction of the patient’s hospital outcome, including emergency department (ED) discharge or hospital admission (ICU or ward). Additional data, such as the time of the ambulance’s arrival and the staff years of experience, were collected. The categorical characteristics are presented by frequency and percentage for each category.
Results: This study included 251 paramedics and 251 patients. The average age of the patients was 62 years. Of the patients, 32 (12.7%) were trauma, and 219 (87.3%) were non-trauma patients. Two-thirds of the patients (n=171, 68.1%) were predicted to be admitted to the hospital, and 80 (31.8%) of the EMS staff indicated that the patient do not need a hospital or an ambulance. The sensitivity, specificity, PPV, and NPV of the emergency medical service (EMS) staffs’ gestalt for patient admission to the hospital were, respectively (77%), (33%), (16%), and (90%). Further analysis was reported to defend the EMS staffs’ gestalt based on the level of EMS staff and the nature of the emergency (medical vs trauma), are reported.
Conclusion: Our study reports a low level of accurately predicting patient admission to the hospital, including the ICU. The results of this study have important implications for enhancing the accuracy of EMS staff predictive ability and ensuring that patients receive appropriate care promptly.
Keywords: emergency medical service, predictably, hospital admission, ambulance, patient discharge, sensitivity, specificity, positive predictive value, negative predictive value
Introduction
In recent years, healthcare systems globally experienced increasing pressure due to the growing and aging patient population, and the need for optimal resource allocation. Efficient patient management and accurate resource prediction are essential for ensuring that healthcare providers can deliver the best possible care. One critical aspect of this process is the early identification of patients who may require intensive care unit (ICU) or ward admissions, enabling healthcare facilities to prepare and allocate resources accordingly.
Emergency Medical Service (EMS) providers are the first responders to health emergencies and are responsible for providing an initial assessment, treatment, and the transport of patients to an appropriate healthcare facility.1 The paramedics are increasingly being used to predict hospital admissions.2–4 By using predictive analytics, the paramedics can identify patients who are at risk of requiring hospital care and intervene before they reach the emergency room.5 This supports a reduction of overcrowding in hospitals and improve patient outcomes.
To be able to accurately predict ICU admissions and hospitalization is essential for ensuring the appropriate allocation of resources and timely intervention. EMS staff need to be able to identify the patients who are at high risk of deteriorating and requiring critical care, so that they can be transported to an appropriate facility and receive the necessary treatment.
The paramedic’s gestalt is an important part of the hospital admission process. It is a holistic approach to patient care that considers the patient’s physical, mental, and emotional state. The paramedic’s gestalt includes assessing the patient’s vital signs, such as heart rate, blood pressure, respiratory rate, oxygen saturation level, and temperature. The paramedic will also assess the patient’s mental status by asking questions about their current condition and any past medical history. The paramedic will evaluate the patient’s emotional state by looking for signs of distress or agitation.
After the patient assessment, the paramedic will communicate with the receiving hospital staff. This communication includes information about the patient’s condition as well as any treatment that have been administered en route to the hospital. This information assists the hospital staff to prepare for the admission and provide appropriate care on arrival.
To predict ICU admissions, EMS staff typically assess a patient’s vital signs, medical history, and other relevant clinical information. They may also use various scoring systems, such as the Modified Early Warning Score (MEWS) or the National Early Warning Score (NEWS), which assign points based on a patient’s vital signs and clinical presentation to predict the likelihood of clinical deterioration and the need for ICU admission. Effective prediction of ICU admissions can also help streamline hospital resources and reduce overcrowding in emergency departments. Through identifying patients likely to require ICU admission, EMS staff can notify hospitals in advance to ensure that appropriate resources are available.
The study focused on whether emergency medical service personnel can accurately predict or anticipate what will happen to the patient they are transporting. In other words, can EMS staff predict whether a patient will be treated and released, admitted to the hospital, or sent to ICU? The question is whether EMS personnel have the ability to predict patient outcomes and the next steps with a reasonable degree of accuracy, or whether there is too much uncertainty to make accurate predictions about the patient’s disposition. The aim of this study was to assess paramedics’ gestalt on both ward or ICU admission.
Materials and Methods
Study Settings and Population
We conducted a prospective study at an adult ED of King Fahad Hospital at King Abdulaziz Medical City. King Fahad Hospital (KFH) is a tertiary teaching hospital with more than 1000 beds. The ED receive approximately 700 patients per ambulance monthly. All EMS staff transporting patients to KFH between September 2021 and March 2022 were eligible to participate in the study. Patients were eligible for the study if they were 18 years of age or older and were brought to the ED by ambulance.
Data Collection
The questionnaire explored if the EMS staff could predict whether the patient would be discharged from the ED or admitted to the hospital. If admitted, the question was whether the EMS staff could predict whether the patient would be admitted to ICU or a ward bed. In addition, basic information was also collected, including the date and time of arrival at the ED, the level of the ambulance service staff member (eg, paramedic, emergency medical technician), gender, age, and years of experience in the ambulance service.
The time of the data collection was based on the availability of data collectors and usually between 8:00 and 16:00, on weekdays. The data collectors approached all EMS staff and invited to complete the questionnaire. The hospital computer system (BESTcare) was used to record the actual ED diagnosis (trauma or non-trauma) and the patient’s disposal from the ED, length of stay, final diagnosis, and discharge date.
Analysis
At the end of the study, all the patients were followed up to assess their final disposition after the initial ED visit. The data were linked and analyzed. For the data analysis, we used the IBM SPSS version 25 (IBM Corp.; Armonk, NY, USA). We used mean and standard deviation to summarize the continuous variables, such as age, and frequency and percentage for the categorical variables. R studio (epi.stats package in R Version 3.5.0.) was used to assess the diagnostic accuracy.
Objective and Outcomes
The study questions was “What is the accuracy of emergency medical service staffs” predictions of emergency department disposition?”
The primary objective of the study was to determine the accuracy of emergency medical service staffs’ predictions of emergency department disposition.
The primary outcome was to assess the ability of the emergency medical service staff to predict hospital and ICU admission. The second outcome was to calculate the proportion of the patients admitted to the hospital of all the patients transported with an emergency ambulance.
Ethics
The study was approved by the King Abdullah International Medical Research Center (KAIMRC; Riyadh, Saudi Arabia) Institutional Review Board (IRBC/1713/21). All study participants were given information about the study and agreed to participate before they started.
Results
In this study, we approached 300 patients between September 2021 and March 2022, 49 patients had an incomplete questionnaire or missing outcomes. The average age of the patients was 62 years (SD 22.6, range 18–91) of which 125 were male (49.8%). Of the 251 patients, 32 (12.7%) were trauma patients and 219 (87.3%) non-trauma patients. Finally, only 35 (13.9%) of the patients were admitted to the hospital of which 8 (3.2%) were admitted to ICU.
The paramedics (n=251) were from different organizations. The EMS staff baseline data and demographic are presented in Table 1. In relation to the need of the patient to attend the ED, almost two-thirds of the EMS staff expected that the patient they transported will require hospital admission (n=171, 68.1%). The EMS staff indicated that 109 (43.4%) would be admitted to a ward and the remaining (n=62, 24.7%) patients would be admitted to ICU. For the remaining 80 (31.8%), the EMS staff indicated that the patient did not need a hospital or an ambulance.
 |
Table 1 Baseline Data for EMS Staff |
In Table 2, we demonstrate the sensitivity, specificity, PPV, and NPV of the paramedics’ gestalt decisions for the patient’s admission to the hospital (all admissions), ICU, and ward compared with actual outcomes. In Table 3, we displays the sensitivity, specificity, PPV, and NPV of the paramedics’ gestalt for the patient admission to the hospital based on the nature of the emergency (medical vs trauma). Finally, Table 4, the sensitivity, specificity, PPV, and NPV of the paramedics’ gestalt for patient admission to the hospital based on the level of EMS staff (paramedics versus technicians).
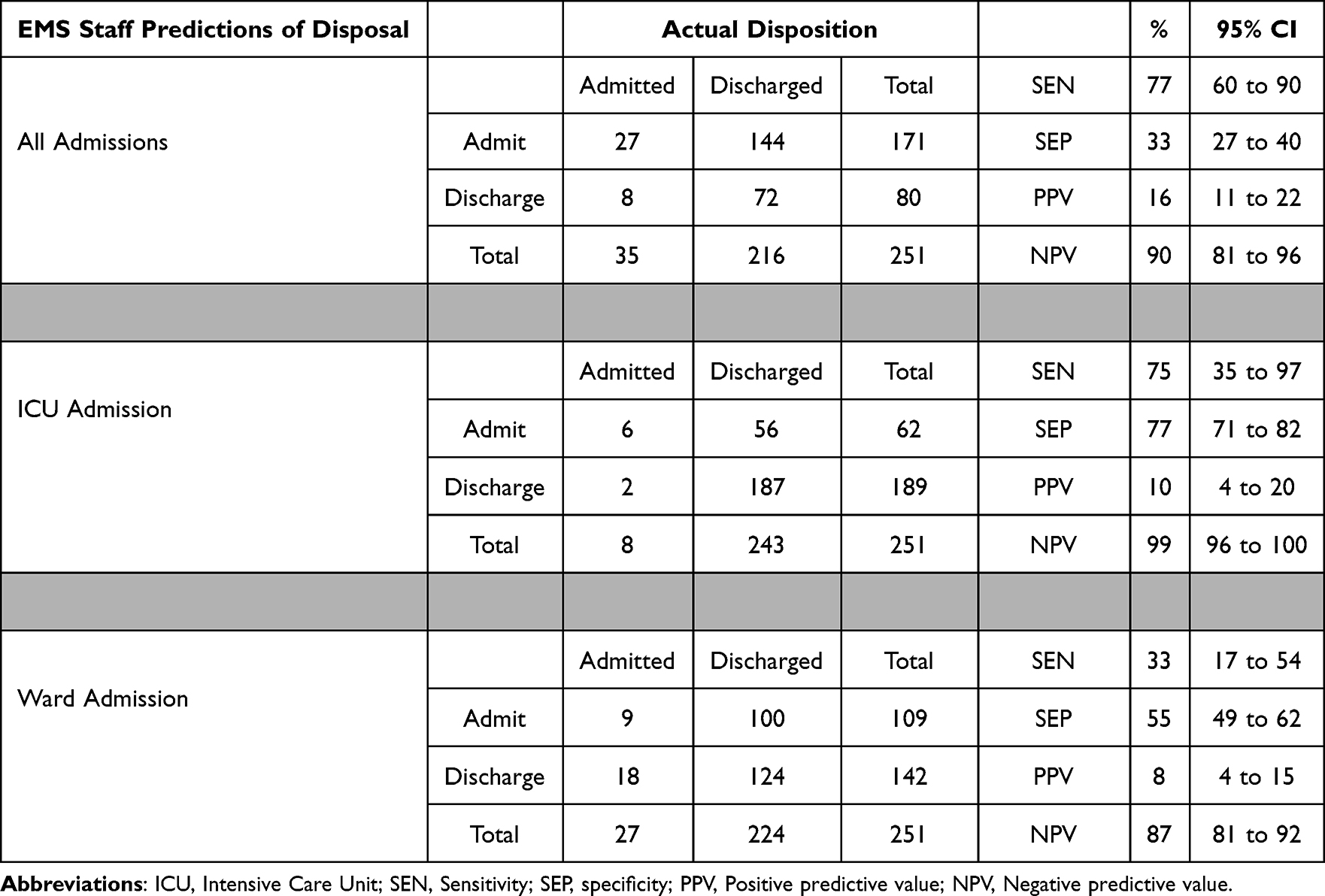 |
Table 2 EMS Staff Predictions of Disposal versus Actual Disposal |
 |
Table 3 EMS Staff Predictions of Disposal versus Actual Stratified by Nature of the Admission (Trauma or Non-Trauma) |
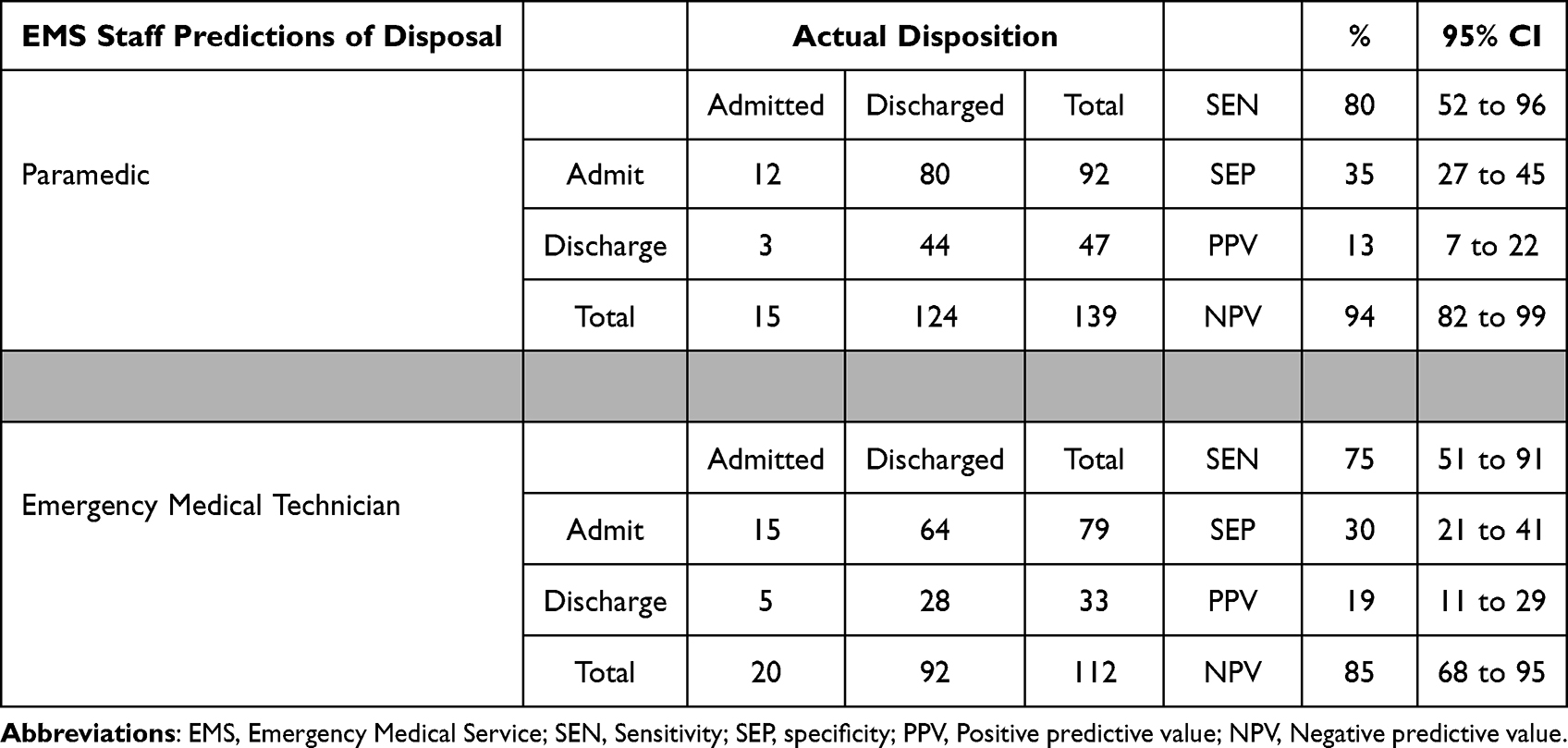 |
Table 4 EMS Staff Predictions of Disposal versus Actual Disposal and Categorized by Job Description |
Discussion
The study indicated a low level of accuracy when the EMS staff predicted the patient’s admission to an ICU or ward. The EMS staff’s performance improved when predicting discharge for all the hospital admissions. In addition, the EMS were more accurate when predicting non-trauma admission compared to traumatic admission.
The results of this study have important implications for improving the accuracy of EMS staff predictions and ensuring that the patients receive appropriate care in a timely manner. By identifying areas in which EMS staff may require additional training or support, healthcare providers can work to improve the accuracy of EMS staff predictions and reduce the risk of unnecessary hospital admissions.
Accurately predicting ICU admissions and hospitalization is essential for ensuring appropriate allocation of resources and timely intervention. EMS staff need to be able to identify patients who are at high risk of deteriorating and requiring critical care, so that they can be transported to an appropriate facility and receive the necessary treatment. In this study, we observed the precision of EMS staff in forecasting such dispositions. The outcomes demonstrated that these providers are accurate in predicting patients who do not need an ICU (99% NPV) or ward (83% NPV). They also had acceptable accuracy in predicting patients who will be sent home after treatment (77% sensitivity). The study’s findings are consistent with previous research investigating ability of the EMS staff to predict the demand for admission. For instance, a study found that EMS providers had a NPV of 96.2% for predicting ICU admission and a sensitivity of 73.3% for predicting patient discharge. The current study’s findings add to the growing body of evidence that highlights the accuracy of EMS providers in predicting patient dispositions.4
Both paramedics and EMTs provided almost similar predictions to the patients included. Although the paramedics had a higher sensitivity and specificity, 80% and 35%, respectively, compared to the EMTs, 75% and 30%, respectively. Clesham and Mason2 conducted a study in the UK to compare paramedics and EMTs in predicting ED admission and presented different findings. The paramedics had a higher sensitivity compared to EMTs with 76.8% (64% to 86) and 69.5% (61% to 77%), respectively. However, the EMTs had a higher specificity compared to the paramedics with 83.8% (77% to 89%) and 64.4% (53% to 74%), respectively. Similarly, Price and Hooker4 revealed that the paramedics had higher sensitivity when compared to EMTs with 80.3% (72.3–86.5%) and 57.7% (37.2–76.0%), respectively, in predicting the patient’s deposition. However, the paramedics had a lower specificity with 76.1% (68.6–82.2%) compared to the EMTs with 94.4% (87.0–97.9%). The differences between the findings, particularly for the EMTs, could be attributed the level of experience the participants or the quality of education the participants received.
With regards to the trauma and medical cases, there is supporting evidence showing that the paramedic’s subjective judgment could play a significant role in predicting the severity of the illness or injury and risk of adverse outcomes, although it could lead to non-adherence to guidelines and triage tools. A previous study reported that the paramedic’s subjective judgment improved the identification of patients with severe trauma (78%), compared to the triage tools (38%).6 Such judgments in trauma patients are usually made by experienced paramedics. Inexperienced paramedics and senior experienced paramedics who supervised other paramedics in training were more adherent to protocols and guidelines and did not usually make subjective judgments, possibly due to their lack of experience or familiarity with the protocols.7 The paramedics’ judgments in terms of illness severity and risk of adverse clinical outcomes could be improved through using prognostic tools, based primarily on the collected physiological measurements in prehospital care. Examples of the most common prognostic tools for prehospital use include The Critical Illness Prediction (CIP), Modified Early Warning Score (MEWS), and National Early Warning Score (NEWS).8 The use of these tools by paramedics in prehospital care have good to moderate discrimination in terms of mortality and ED disposition.8 However, none of these tools or other similar tools are currently applied in routine paramedic practice in Saudi Arabia. The paramedic’s judgment is mostly subjective without the aid or use of any prognostic tools to assess the illness severity or the risk of adverse clinical outcomes or specific trauma triage tools to aid transportation decisions. This could explain the decreased sensitivity of non-trauma admissions and decreased specificity for both trauma and non-trauma admissions in our study.
By accurately predicting ICU admission and hospitalization, EMS staff can assist in ensuring that the patients receive the appropriate level of care in a timely manner. This can improve the patient outcomes, reduce the burden on healthcare resources, and ultimately save lives. Finally, similarly to previous studies, there was insufficient evidence to support the ability of the EMS staff to predict the disposition of patient.5 To improve the accuracy of ICU admission and hospitalization prediction, the EMS staff can use a range of tools and techniques, such as the clinical decision support systems (eg, National Early Warning Score (NEWS) 2, quick Sequential Organ Failure Assessment (qSOFA), History and Electrocardiogram-only Manchester Acute Coronary Syndromes (HE-MACS)), risk stratification algorithms, and predictive modelling. These tools support EMS staff to identify the patients who are at high risk of adverse outcomes, such as acute myocardial Infarction, cardiac arrest, or sepsis.9–14
Though the ability of the EMS staff to predict ICU and ward admissions shows promise, challenges remain in terms of the implementation, data access and sharing, and ensuring that predictions are accurate and reliable. Future research should focus on refining predictive models, validating their performance in diverse patient populations, and exploring how these tools can be effectively integrated into EMS workflows.
Limitations
This study has several limitations. First, the data was collected from a single center in Saudi Arabia, so the findings may not be generalizable to other emergency medical services (EMS) systems. Second, the sample size may not be representative of the entire EMS workforce in Saudi Arabia. Third, the paramedics’ opinions may have been affected by the opinions of other healthcare providers working in the triage area of the emergency department, which could have introduced bias into the study.
Conclusion
In conclusion, currently EMS staff have a low level of predictive ability for predicting patient admission to hospital, including ICUs. However, the EMS staff could potentially improve patient care and resource allocation in healthcare systems. By leveraging clinical decision rules, advanced technologies, and innovative techniques, EMS providers can play a vital role in optimizing patient outcomes and enhancing the overall efficiency of healthcare delivery.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Villarreal M, Leach J, Ngianga-Bakwin K, Dale J. Can a partnership between general practitioners and ambulance services reduce conveyance to emergency care? Emerg Med J. 2017;34(7):459. doi:10.1136/emermed-2015-204924
2. Clesham K, Mason S, Gray J, Walters S, Cooke V. Can emergency medical service staff predict the disposition of patients they are transporting? Emerg Med J. 2008;25(10):691. doi:10.1136/emj.2007.054924
3. Levine SD, Colwell CB, Pons PT, Gravitz C, Haukoos JS, McVaney KE. How well do paramedics predict admission to the hospital? A prospective study. J Emerg Med. 2006;31(1):1–5. doi:10.1016/j.jemermed.2005.08.007
4. Price TG, Hooker EA, Neubauer J. Prehospital provider prediction of emergency department disposition. Prehospital Emerg Care. 2005;9(3):322–325. doi:10.1080/10903120590962012
5. Brown LH, Hubble MW, Cone DC, et al. Paramedic determinations of medical necessity: a meta-analysis. Prehospital Emerg Care. 2009;13(4):516–527. doi:10.1080/10903120903144809
6. Voskens FJ, van Rein EA, van der Sluijs R, et al. Accuracy of prehospital triage in selecting severely injured trauma patients. JAMA Surg. 2018;153(4):322–327. doi:10.1001/jamasurg.2017.4472
7. van Rein EA, van der Sluijs R, Raaijmaakers AM, Leenen LP, van Heijl M. Compliance to prehospital trauma triage protocols worldwide: a systematic review. Injury. 2018;49(8):1373–1380. doi:10.1016/j.injury.2018.07.001
8. Lane DJ, Wunsch H, Saskin R, et al. Assessing severity of illness in patients transported to hospital by paramedics: external validation of 3 prognostic scores. Prehospital Emerg Care. 2020;24(2):273–281. doi:10.1080/10903127.2019.1632998
9. Barak-Corren Y, Agarwal I, Michelson KA, et al. Prediction of patient disposition: comparison of computer and human approaches and a proposed synthesis. J Am Med Inform Assoc. 2021;28(8):1736–1745. doi:10.1093/jamia/ocab076
10. Seymour CW, Kahn JM, Cooke CR, Watkins TR, Heckbert SR, Rea TD. Prediction of critical illness during out-of-hospital emergency care. JAMA. 2010;304(7):747–754. doi:10.1001/jama.2010.1140
11. Alghamdi A, Howard L, Reynard C, et al. Enhanced triage for patients with suspected cardiac chest pain: the history and electrocardiogram-only Manchester acute coronary syndromes decision aid. Eur J Emerg Med. 2019;26(5):356–361. doi:10.1097/MEJ.0000000000000575
12. Monahan AC, Feldman SS. Models predicting hospital admission of adult patients utilizing prehospital data: systematic review using PROBAST and CHARMS. JMIR Med Inform. 2021;9(9):e30022. doi:10.2196/30022
13. Shirakawa T, Sonoo T, Ogura K, et al. Institution-specific machine learning models for prehospital assessment to predict hospital admission: prediction model development study. JMIR Med Inform. 2020;8(10):e20324. doi:10.2196/20324
14. Martín-Rodríguez F, López-Izquierdo R, Castro-Villamor MA, et al. A predictive model for serious adverse events in adults with acute poisoning in prehospital and hospital care. Austral Critical Care. 2021;34(3):209–216. doi:10.1016/j.aucc.2020.07.004
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.