")
Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 14
The Ability of Dental Interns and Freshly Graduated Dentists to Assess Tooth Restorability. A Multicenter, Cross-Sectional Study
Authors Aldowah O
Received 18 August 2022
Accepted for publication 16 November 2022
Published 22 November 2022 Volume 2022:14 Pages 337—352
DOI https://doi.org/10.2147/CCIDE.S386676
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Christopher E. Okunseri
Omir Aldowah
Prosthetic Dental Science Department, Faculty of Dentistry, Najran University, Najran, Kingdom of Saudi Arabia
Correspondence: Omir Aldowah, Email [email protected]
Purpose: Treatment planning should be integrated to gain and apply essential data to decide. It is necessary to evaluate the endodontic and periodontal condition of the tooth, in addition to its restorability. Treatment planning is emphasized as a crucial clinical skill for a certified dental practitioner in the General Dental Council learning outcomes. The role of dental schools is to guarantee that dental graduates have the knowledge, skills, and competence to choose appropriate treatment options for teeth. The primary objective of our study was to assess the ability of dental interns and recently graduated dentists from different dental schools for tooth restorability.
Participants and Method: This was a multicentral, cross-sectional study. Participant recruitment was achieved by sending an online questionnaire to the interns and graduate units at the assigned universities. The questionnaire consisted two parts. The first part record general information about participants and opinions regarding their training of restorability assessment. The second part include five hypothetical clinical case scenarios, where the participants were asked to choose the restorability decisions, rationales for the options, and prognosis of the tooth/teeth. The data was analyzed by using SPSS software version 26.
Results: 104 respondents participated in this survey. The decision and prognosis of all clinical scenarios were not significantly associated with gender, experience, place of work and place of study. Only the decision and prognosis of scenario 1 showed significant relationship with place of graduation. Developing universities graduates showed significantly higher percentage for restorability as against developed universities graduates (p=0.001) and developing universities and recently established institutions graduates showed significantly higher percentage for the questionable prognosis as against developed universities graduates (p=0.018).
Conclusion: The inability of dental interns and freshly graduate dental practitioners to make decisions highlighted questions regarding the condition of learning outcomes and graduate attributes.
Keywords: dental, interns, recent graduates, teeth restorability, assessment
Introduction
The planning of dental treatment can be difficult, and it involves the clinician to take into consideration a large number of aspects that are interconnected in order to formulate an acceptable treatment strategy. It is necessary to evaluate the endodontic and periodontal condition of the tooth, in addition to its restorability.1 Advanced materials, techniques, and an extensive range of treatment modalities allow the dental team to provide effective, predictable, and long-lasting restorative treatments even with compromised teeth. Replacement of unsalvageable teeth with a denture, bridge, or dental implant may well be indicated and worthwhile. A careful restorability assessment should be carried out before choosing which treatment options fit the tooth.2 The determination of whether or not to keep a tooth that can be restored may be a straightforward one in some cases. Take, for instance, a molar tooth in an intact arch that has been diagnosed with an endodontic problem and that has adequate sound coronal tooth structure and periodontal support. However, a tooth that has a comparable endodontic condition may not be able to be restored if it does not have sufficient healthy coronal tooth structure to provide a suitable ferrule for a crown. In this case, the tooth would be considered non-restorable.3 A holistic approach should be taken to decide whether to restore a compromised tooth or to advise the patient that restoring the tooth is not feasible and recommend the patient leave it alone or extract it. Endodontic status, periodontal status, and structural integrity need to be assessed.4,5 Additionally, patients’ medical and dental conditions, age, and expectations should all be carefully considered in the decision-making process.6 Further, the skills and experience of the clinician might have an effect on the treatment decisions and the treatment plan. Appropriate case selection is more likely to result in a successful outcome.7
Treatment planning is emphasized as a crucial clinical skill for certified dental practitioners in the General Dental Council learning outcomes.8 However, there is minimal published research on the subject of teaching treatment planning, and dentistry curricula lack a standardized teaching methodology.9 The role of dental schools is to guarantee that dental graduates have the knowledge, skills, and competence to choose the appropriate treatment options for teeth.10
However, several studies, particularly in Europe, have demonstrated that the standard of endodontic treatment provided by general dentists and the frequency of inadequately filled root canals in relation to healthy periapical areas is not high.11 Epidemiological studies results showed different clinical outcomes in various regions of the world, with prevalence rate of inadequate root canal fillings reaching up to 72.4%, and with 87.0% of these teeth showing apical periodontitis.12,13 Without a doubt, a favorable endodontic treatment outcome is not solely dependent on the effectiveness of the root canal procedure (and, consequently, a tight coronal and apical closure of the shaped and cleaned root canal). To prevent reinfection and promote the healing of apical periodontitis, good quality of the corresponding post endodontic restorations would seem to be a necessary prerequisite in addition to properly executed root canal fillings.13–15 Dental practitioners should be encouraged to consider all options for the management of compromised teeth and justify the case for tooth preservation by vital pulp therapy, root canal treatment, or nonsurgical/surgical retreatment, followed by adequate coronal restoration, and should balance this against tooth loss and a prosthetic/implant-supported replacement, which depends initially on achieving an accurate diagnosis.16
Worldwide, the graduates have to pass a test from an authority to practice dentistry, such as the American Dental Association in the USA or the General Dental Council in the UK.8 Those authorities mostly elaborate the learning outcomes that dental graduates should achieve in the undergraduate studies, For instance, the General Dental Council learning outcomes emphasize treatment planning as an essential clinical competence for registered general dentists.8
However, there is little published literature on the teaching of treatment planning, and dentistry curricula needs to improve the format of teaching the treatment planning.9 Eliyas et al 2019 claimed that many undergraduates reportedly lacked formal instruction in evaluating the restorability of teeth.17 It has been demonstrated that treatment planning is one of the most essential abilities for dental graduates to master in preparation for clinical practice.18 It has been reported that undergraduate dental students felt less confident in establishing a comprehensive treatment plan compared to other clinical skills.19 A study of 186 newly certified dentists and their educational supervisors revealed that 56% of educational supervisors reported that trainees were “poorly” or “very poorly” prepared for diagnostic and treatment planning in general practice.20 Dental graduates from dental colleges in Saudi Arabia must pass a test from the Saudi Commission for Health Specialties to practice dentistry in Saudi Arabia. Dental colleges in Saudi Arabia have different curriculums with different programme learning outcomes. The absence of learning outcomes from higher authorities such as the Saudi Commission for Health Specialties may cause variations in the skills of graduates to assess tooth restorability. The effect of the design of programme learning outcomes and graduate attributes in the Saudi dental colleges without guidance from the higher authorities might influence the adequacy of learning outcomes. The ability of dental practitioners to correctly diagnose the condition depends on a variety of criteria, including their level of expertise, level of experience, and level of critical thinking.21,22 It is essential for dental practitioners to be able to determine the source of an infection and assess the severity of a disease before making a decision regarding whether or not to treat the condition, extract the affected tooth, or send the patient to the appropriate specialist.22 Accordingly, graduates’ skills and competences need to be investigated among graduates from different colleges in Saudi Arabia. The findings of this observational study will provide dental educators with useful insights that may be used to reduce the number of errors made by dental graduates when interpreting clinical and radiographic data and to construct continuing education for dental professionals. The primary objective of this cross-sectional study was to assess the ability of dental interns and recently graduated dentists from different dental schools for tooth restorability. The null hypothesis proposes that the dental interns and recently graduated dentists from different dental schools of Saudi Arabia are capable of making decisions for tooth restorability.
Methodology
This study was approved by the research ethics committee at Najran University, Reference No.: 443/40-50397-DS, Appendix 1. The targeted population in this survey study includes recently graduated dentists and interns in multiple dental schools in Saudi Arabia. Participant recruitment was achieved by sending an online questionnaire to the interns and graduate units at the assigned universities. Participants were offered an incentive in the form of a draw. This offer was 1000 Riyals for 2 participants.
The main questionnaire consisted of two parts, Appendix 2. The first part includes eight questions recorded general information about participants and their opinions regarding the training of restorability assessment in the undergraduate study. The Likert scale was used with questions that assessed participants’ thoughts regarding the training of restorability assessment in the undergraduate study. The second part included hypothetical clinical case scenarios, where the participants were asked to choose the restorability decisions, rationales for the options, and prognosis of the tooth/teeth. The clinical case scenarios were built based on the Dawood and Patel2 Index. All the questions were multiple-choice questions. However, for some questions, the participants were provided space to add rationales that were not listed among the options. The guideline of the American Association of Endodontists for a compromised tooth was used as a guide for prognosis options.23
All participants were provided with information about the research study in the invitation email. Consent was obtained from all participants in the first part of the online survey. Since the restorability assessment is mainly subjective, a team of three consultants in prosthodontics, endodontics, and periodontics were recruited to be a control group. They teach in the included centers. They decided the restorability individually. Then, they held a meeting to discuss the decision and prognosis of the cases in which the decision and prognosis of the individual consultant differed. They have at least 10 years of experience. Their restorability decision and prognosis were used as the control data for this study. The control group of this study benefits in studying the significance of the variables on the participants’ decision and prognosis.
The first clinical scenario was a hypothetical case with a need for a comprehensive treatment plan. The presented tooth, mandibular left first molar, was endodontically diagnosed as chronic abscess,24 and non-periodontally involved. It was scored as Level 1 based on the Patel et al restorability index, Figure 1A. The second clinical scenario provided a hypothetical case of a discolored tooth related to the anterior central crowns. The presented teeth were endodontically diagnosed as asymptomatic apical periodontitis,24 and non-periodontally involved. It was scored as Level 6 based on the Patel et al restorability index, Figure 1B. The third hypothetical clinical scenario presented a patient who complained of a broken restoration with a badly broken tooth, maxillary right first premolar, with type II diabetes mellitus. The presented tooth was endodontically diagnosed as asymptomatic apical periodontitis,24 and periodontally involved. It was scored as Level 2 based on the Patel et al restorability index, Figure 1C. The fourth hypothetical clinical scenario presented a patient with pus discharge from the mandibular right first premolar. The presented tooth was endodontically diagnosed as chronic abscesses,24 and periodontally involved. It was scored as Level 2 based on the Patel et al restorability index, Figure 1D. The fifth hypothetical clinical scenario presented a patient with gingival recession in the upper posterior teeth, maxillary right first premolar. The presented tooth was endodontically normal pulp,24 and periodontally involved. It was scored as Level 2 based on the Patel et al restorability index, Figure 1E.
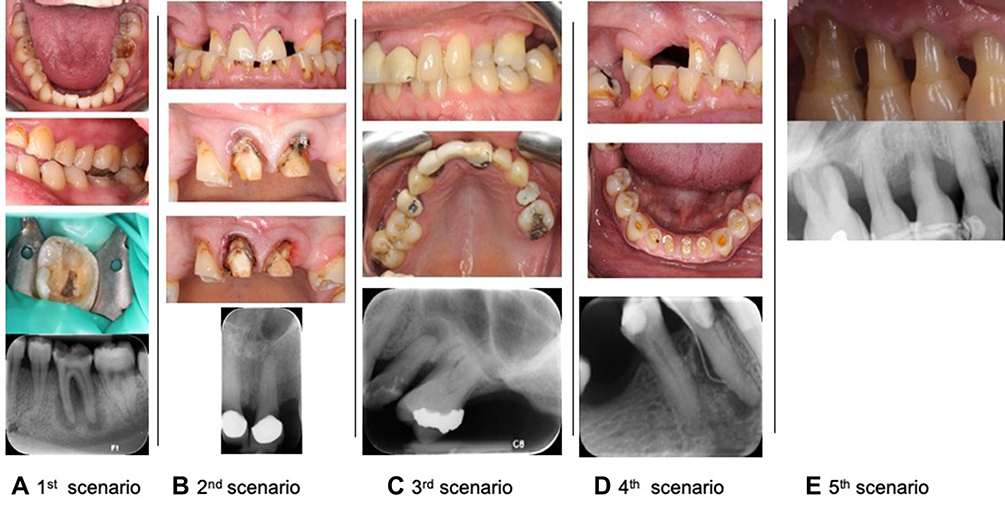 |
Figure 1 Photos of clinical scenarios. |
The participants’ graduation institutions were divided into three categories: developed universities (eg, King Saud University), developing universities (eg, King Khalid University), and newly established universities (eg, Najran University). Number of cases in many cells of cross-sectional tables was very low, “strongly agree” was merged with “agree”, and “strongly disagree” was merged with “disagree”.
Statistical Analysis
The collected data was stored and analyzed by using SPSS software version 26. Data was grouped based on dental schools, years of experience, and sectors where participants practice dentistry. The collected data was analyzed descriptively for each group; the percentages were used to describe the frequencies for each question. Chi-square test was done to determine the association among the different groups. The p-value was set at <0.05.
Results
One hundred and four respondents participated in this survey. Response rate was 49%. Seventy-one (68.3%) participants were males, and 49 (47.1%) respondents were busy in the internship, while 38 (36.5%) dentists were working with one years of experience and remaining were looking for the job. Twenty-six working dentists (68.4%) were attached to the private sector’s clinics. Fifty-nine (57.8%) of the respondents were connected with government institutions, most of them (85.1%) were their internship in government hospital/clinics, Figure 2. Also, Figure 3 shows the thoughts of participants regarding their training of the restorability assessment and their readiness to assess the restorability by responding to the following statements: 1) Undergraduate courses prepare the dentists to assess tooth restorability’, 2) Restorability assessment of teeth is more difficult when the dentists work independently’, and 3) Recommended that the dental schools need to pay more attention to the restorability assessment in their curriculums’.
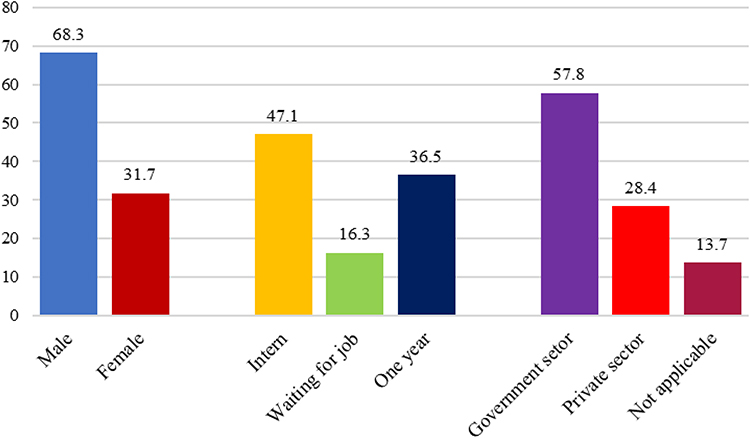 |
Figure 2 Descriptive statistics of gender, experience and place of practice. |
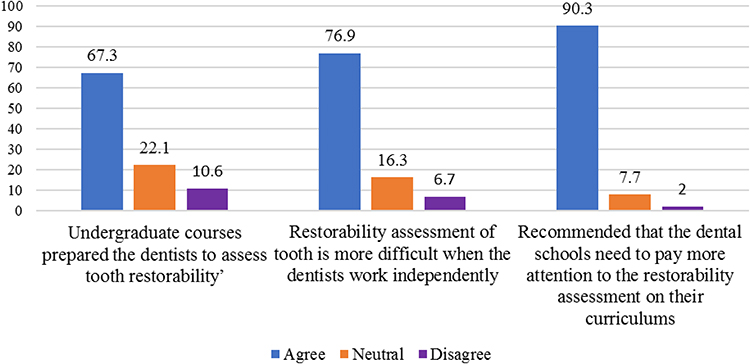 |
Figure 3 Descriptive statistics for participants thought about restorability assessment. |
Decision of restorability assessment of clinical scenarios are presented in Figure 4. The prognosis of restorability assessment of clinical scenarios is presented in Figure 5.
 |
Figure 4 Decisions of restorability assessment. |
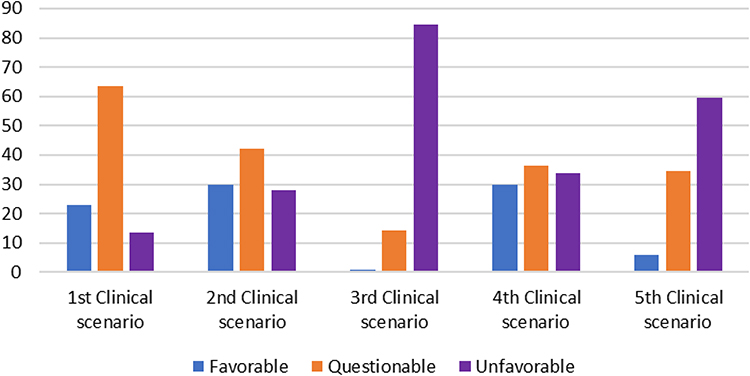 |
Figure 5 Prognosis of clinical scenarios. |
In all the attached tables, the p-conc with (*) indicates that the chi-square result may not be valid due to low sample size. However, none of the p-values showed any significant association, except in one case of Table 1.
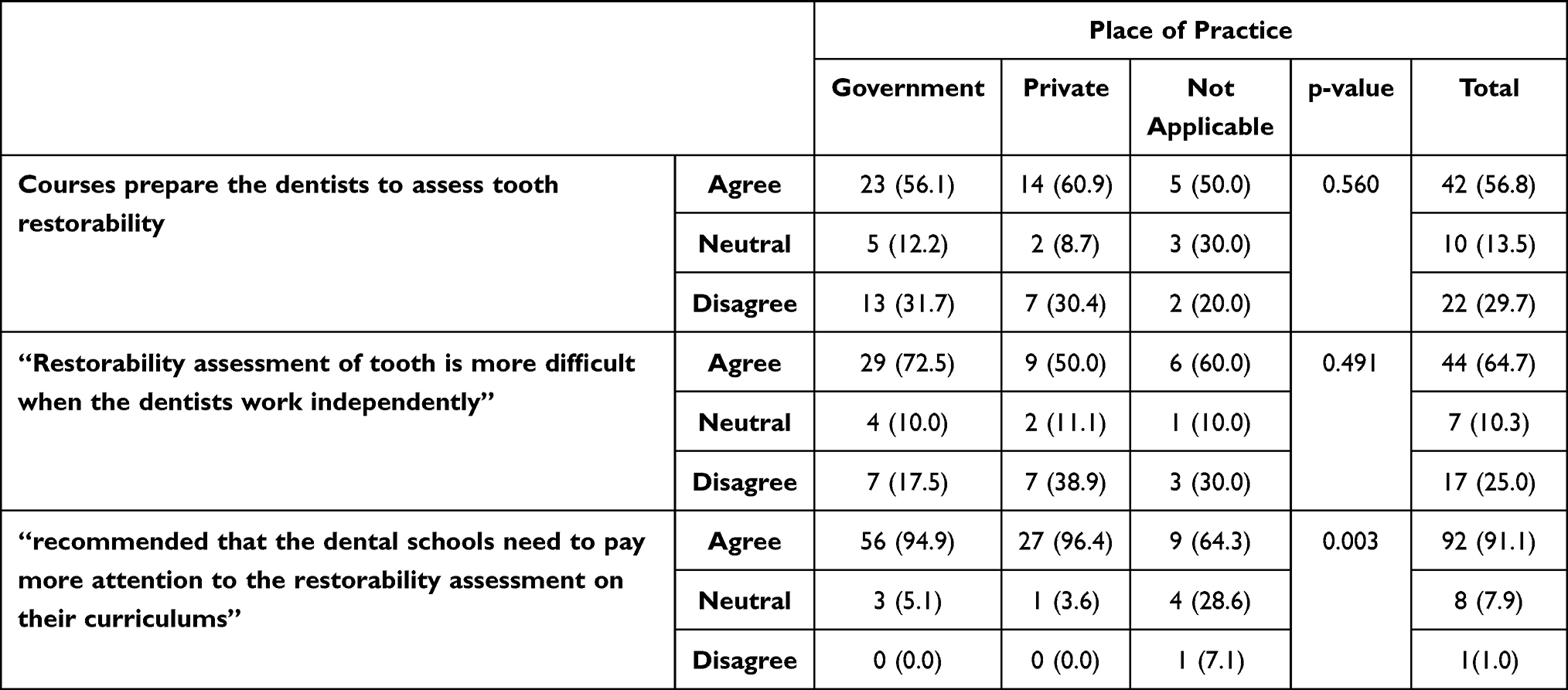 |
Table 1 Association Between Courses of Restorability in Undergraduate, Assessing Restorability Independently and Recommended Curriculum Place of Practice (Private or Governmental Sector) |
Table 2 shows the association of depended variables: 1) Undergraduate courses prepare the dentists to assess tooth restorability’, 2) Restorability assessment of tooth is more difficult when the dentists work independently’, and 3) Recommended that the dental schools need to pay more attention to the restorability assessment on their curriculums’ with independent variables 1. Gender (male/female) and 2. Experience (Waiting for a job/one year/Internship). Even though there was no significant association of gender versus any dependent variables (p > 0.05). However, male respondents agreed in higher parentage for adequacy undergraduate course to assess the restorability. Higher percentage of female respondents recommended that the dental schools need to pay more attention to the restorability assessment on their curriculums.
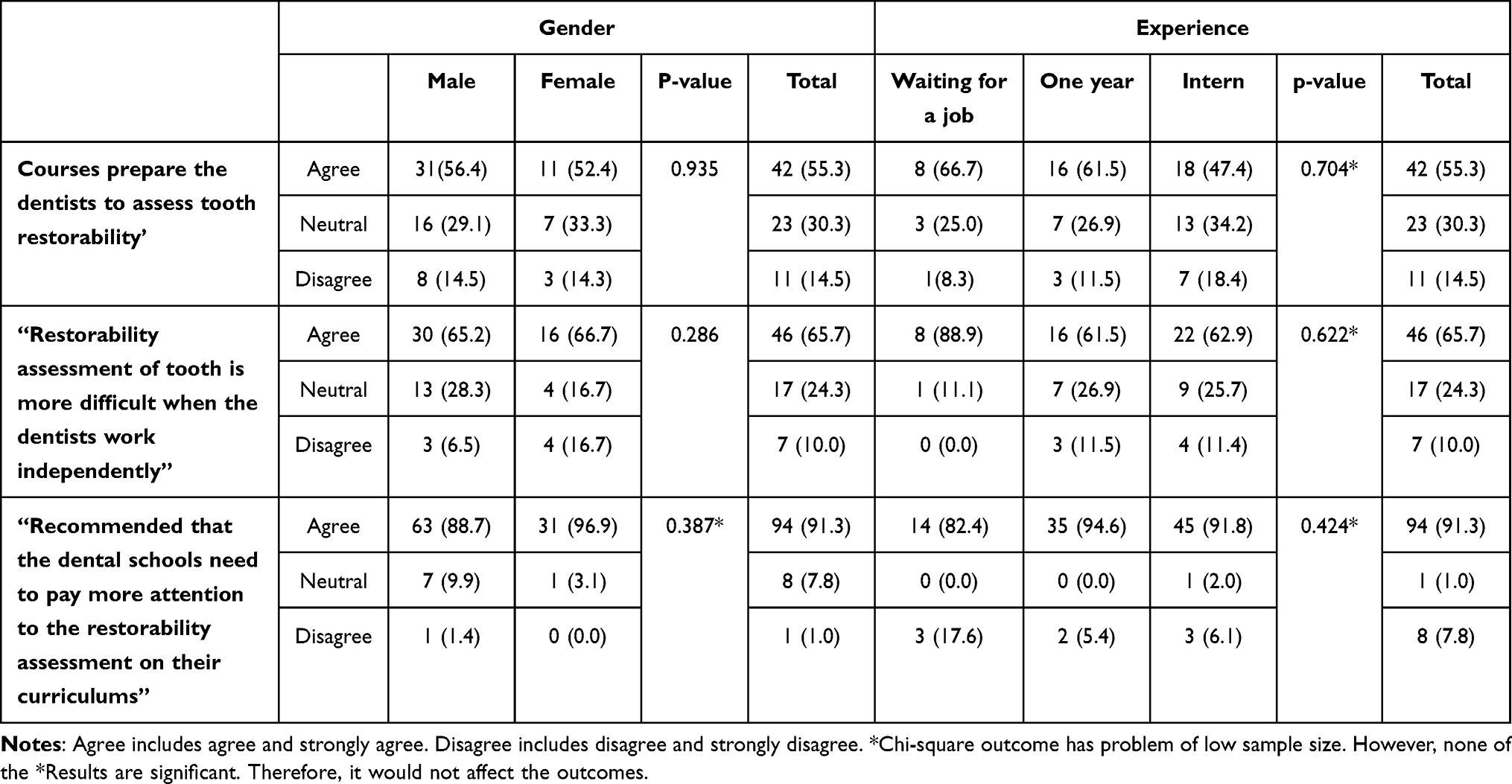 |
Table 2 Association Between Courses of Restorability in Undergraduate, Assessing Restorability Independently and Recommended Curriculum with Gender and Experience |
Table 3 describes the association of independent variables: 1. Gender (male/female) and 2. Experience (waiting for a job/one year/intern) with dependent variables of i) decision of restorability (yes/no), and ii) prognosis (favorable/questionable/unfavorable) of five different scenarios defined in the methodology. There is no significant association between different scenarios and gender, either in decision of restorability or prognosis (p > 0.05). However, male dentists showed a noticeably higher percentage of decisions of non-restorability in scenario 1 and scenario 4. There was also no statistical association between the experiences of the dentists versus decision of restorability and prognosis (p>0.05). However, dentists who are “waiting for a job” showed higher percentage with non-favorable option in scenario 2. Prognosis with higher percentage of unfavorable scenario was indicated by “one-year” experience dentists in scenario 3 and scenario 4.
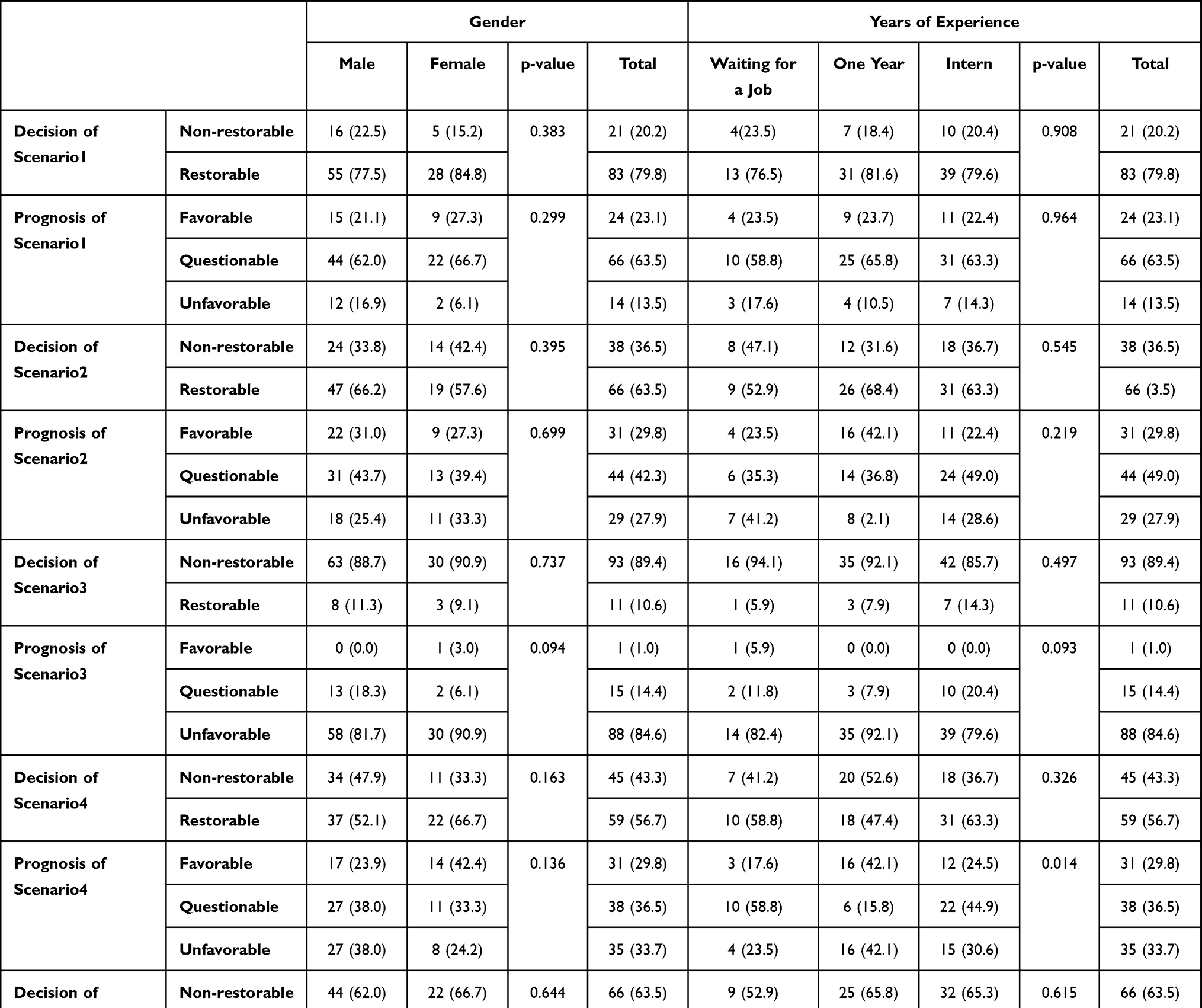 |
Table 3 Association Between Restorability Decision and Favorability of Different Scenarios with Gender and Experience |
The association of place of practice (Government/Private/Non-applicable) with dependent variables: 1) Courses prepare the dentists to assess tooth restorability’, 2) Restorability assessment of tooth is more difficult when the dentists work independently’, and 3) Recommended that the dental schools need to pay more attention to the restorability assessment on their curriculums’ is shown in Table 1. Only dependent number 3) Recommended curriculum’ showed a statistically significant association with place of practice. However, since number of cases were quite few in some cells. Therefore, this association is also not very much valid.
Table 4 discusses the association of place of practice with decision of restorability and prognosis of 5 different scenarios indicated in methodology. None of the “decision of restorability” and prognosis showed any statistical significance with place of practice. However, the dentists with private practice showed markedly higher percentage for “unfavorable case” of prognosis in scenario 3.
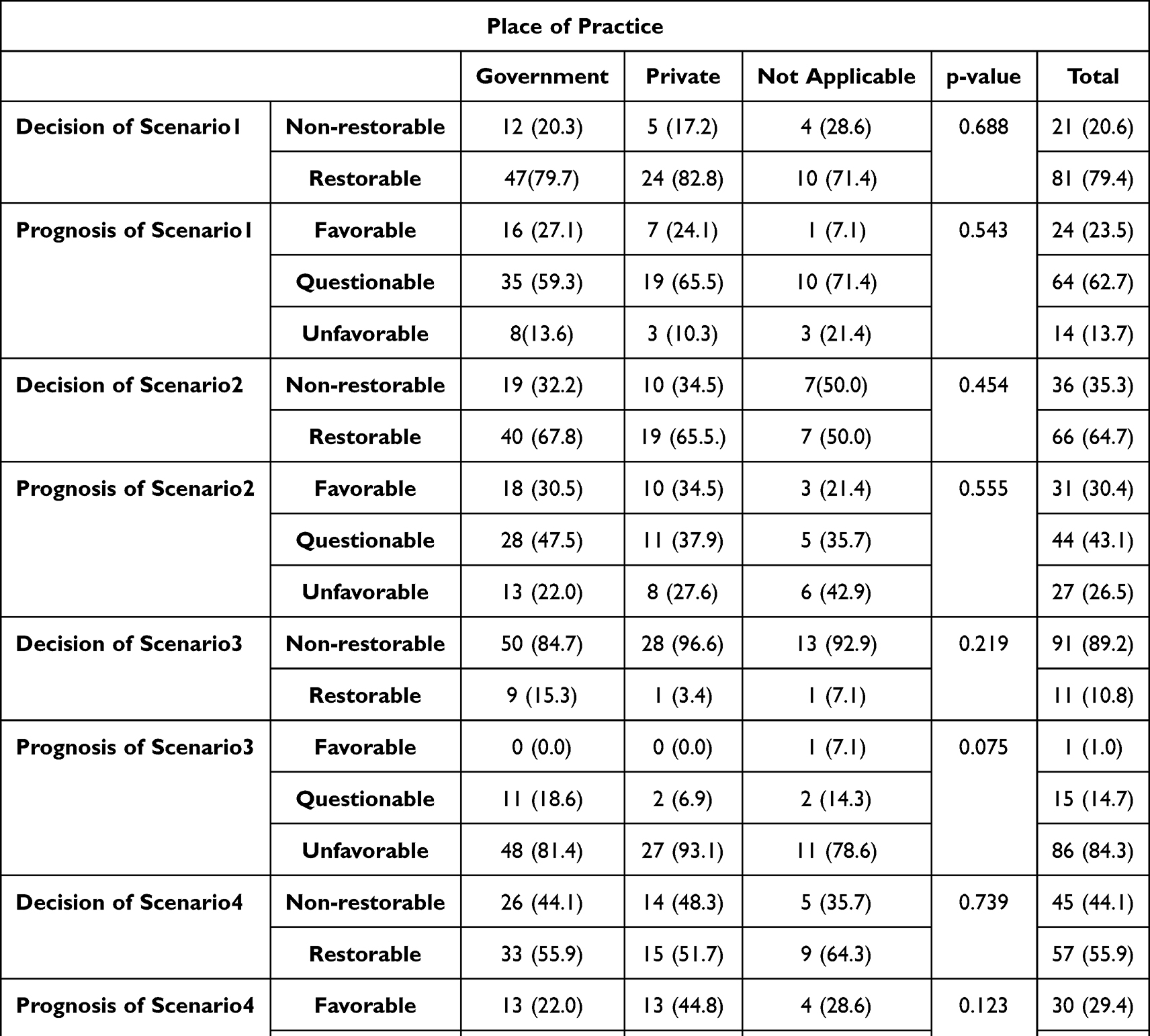 |
Table 4 Association Between Restorability Decisions and Favorability of Different Scenarios with Place of Practice (Private or Governmental Sector) |
Table 5 shows the association of graduation institutes with adequacy of restorability courses, difficulty of independent assessment and recommendation of paying attention of restorability courses. Adequacy of restorability courses was significantly associated with place of graduation (p<0.05). Seventy-five percent of developed universities graduates agreed for adequacy of restorability courses against 38.7% of the graduates from developing universities. Other factors (difficulty of independent assessment and recommendation of paying attention of restorability courses did not show any statistical significance with place of graduation).
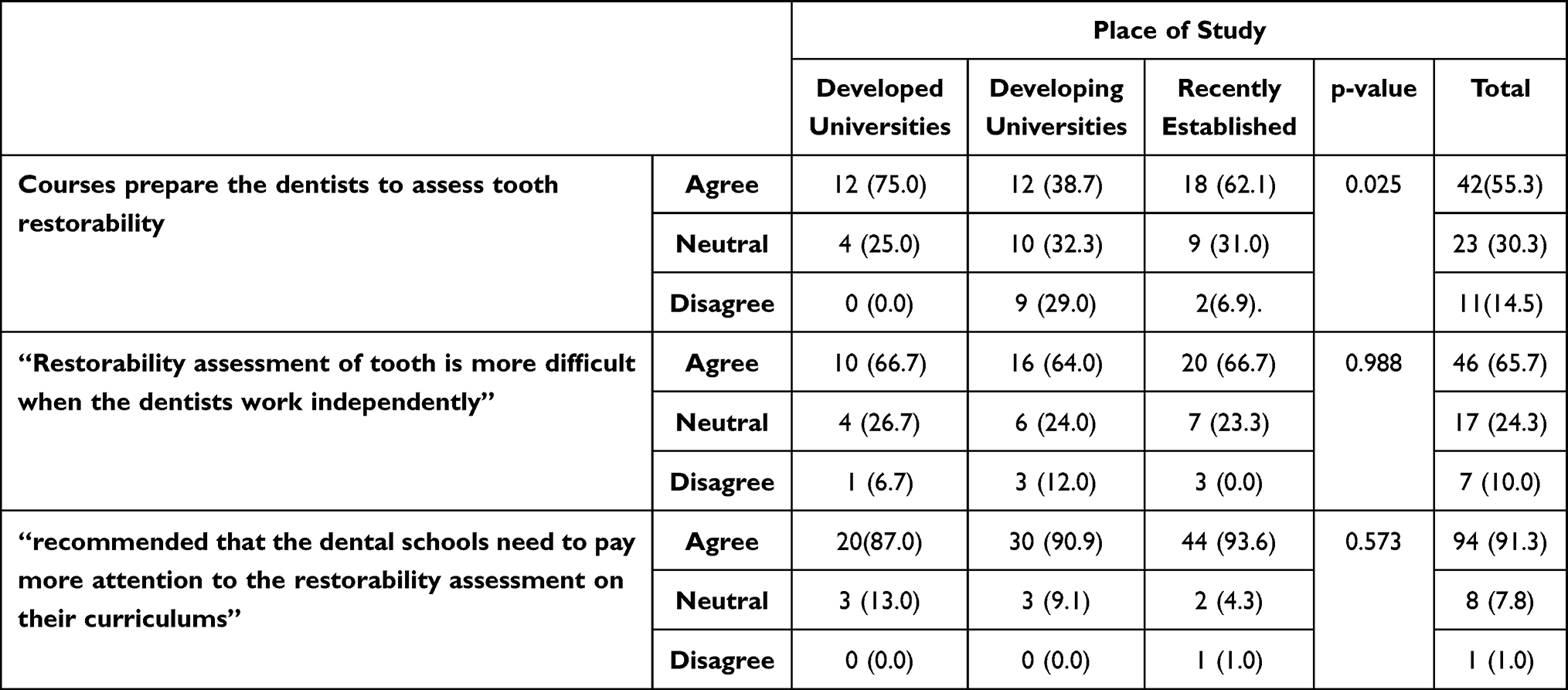 |
Table 5 Association Between Courses of Restorability in Undergraduate, Assessing Restorability Independently and Recommended Curriculum with Place of Study (Dental Colleges) |
Table 6 discusses the association of institute of graduation with different scenarios indicated earlier. Only the decision and prognosis of scenario 1 showed significant relationship with place of graduation. Developing universities graduates showed significantly higher percentage for restorability as against developed universities graduates (p<0.05) and developing universities and recently established institutions graduates showed significantly higher percentage for the questionable prognosis as against developed universities graduates (p<0.05). The decision and prognosis of recently established scenarios did not show any significant association with place of graduation.
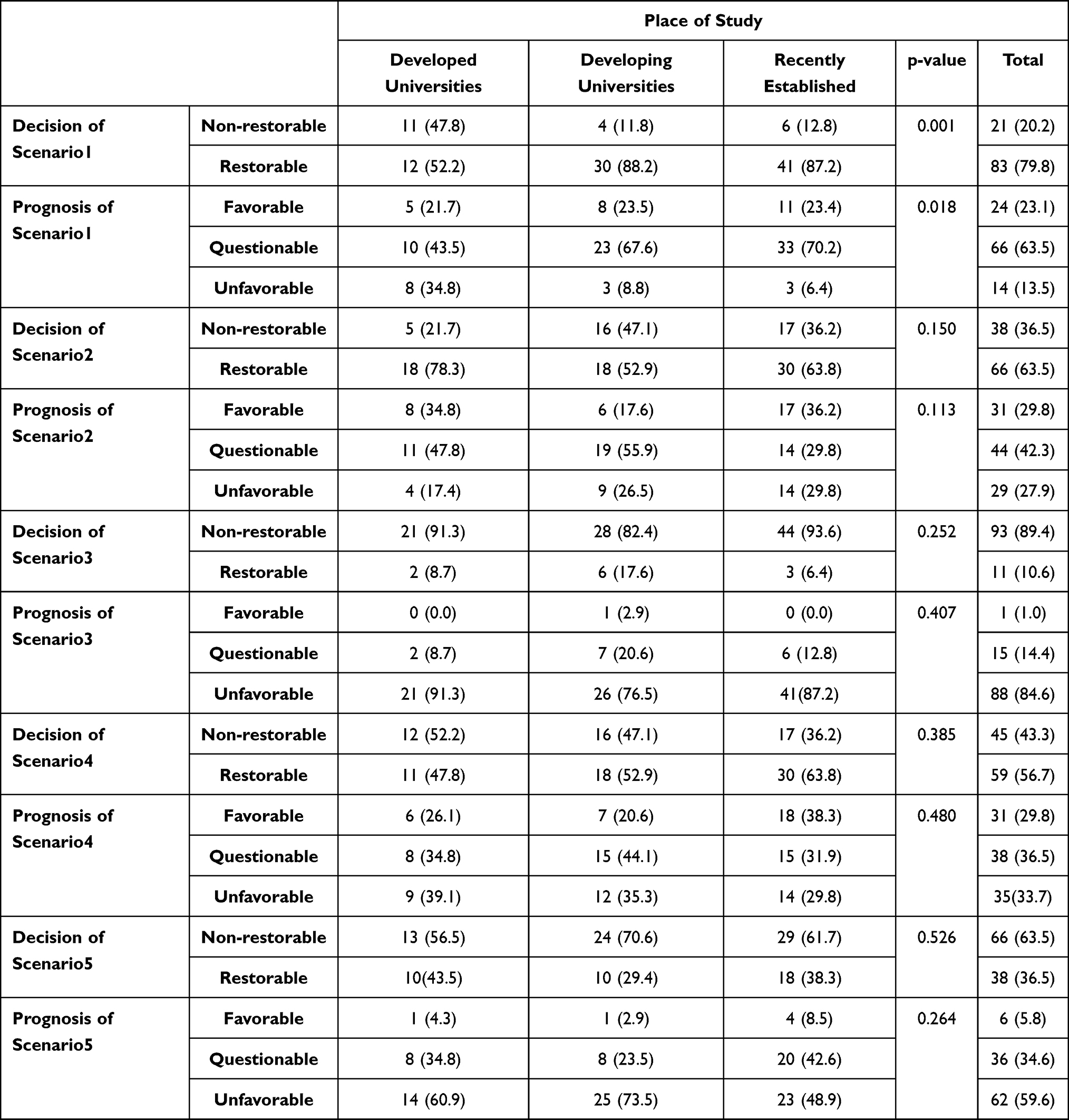 |
Table 6 Association Between Restorability Decision and Favorability of Different Scenarios with Place of Study (Dental Colleges) |
Table 7 shows reasons indicated by the respondents in each scenario. Simple root canal system, probing depth < 5.5, Furcation involvement and untreatable periodontal disease were the main four reasons mentioned by the dentists for scenario 1. Thirty-eight percent of the respondents picked up “A simple root canal system” in this scenario. A simple root canal system, sub-gingival margin, inadequate structure, and minimal tooth structure were the main four factors indicated by the dentists for scenario 2. A simple root canal system was picked up by the majority of the respondents with 34.6%. Untreatable periodontal disease, probing depth > 5.5, minimal tooth structure and inadequate structure for ferrule were the major the four reasons shown by the dentists in scenario 3. Untreatable periodontal disease showed the highest percentage of 65.4% among them. A simple root canal system, probing depth > 5.5, a complete root canal system and inadequate structure for ferrule were the top four opinions for scenario 4. The highest reason with 25% was a simple root canal system as indicated by the respondents. Untreatable periodontal disease, probing depth > 5.5, furcation involvement and inadequate structure for ferrule were the four main reasons for scenario 5 as indicated by the dentists. Untreatable periodontal disease was the highest reasons with 50.0% for this scenario.
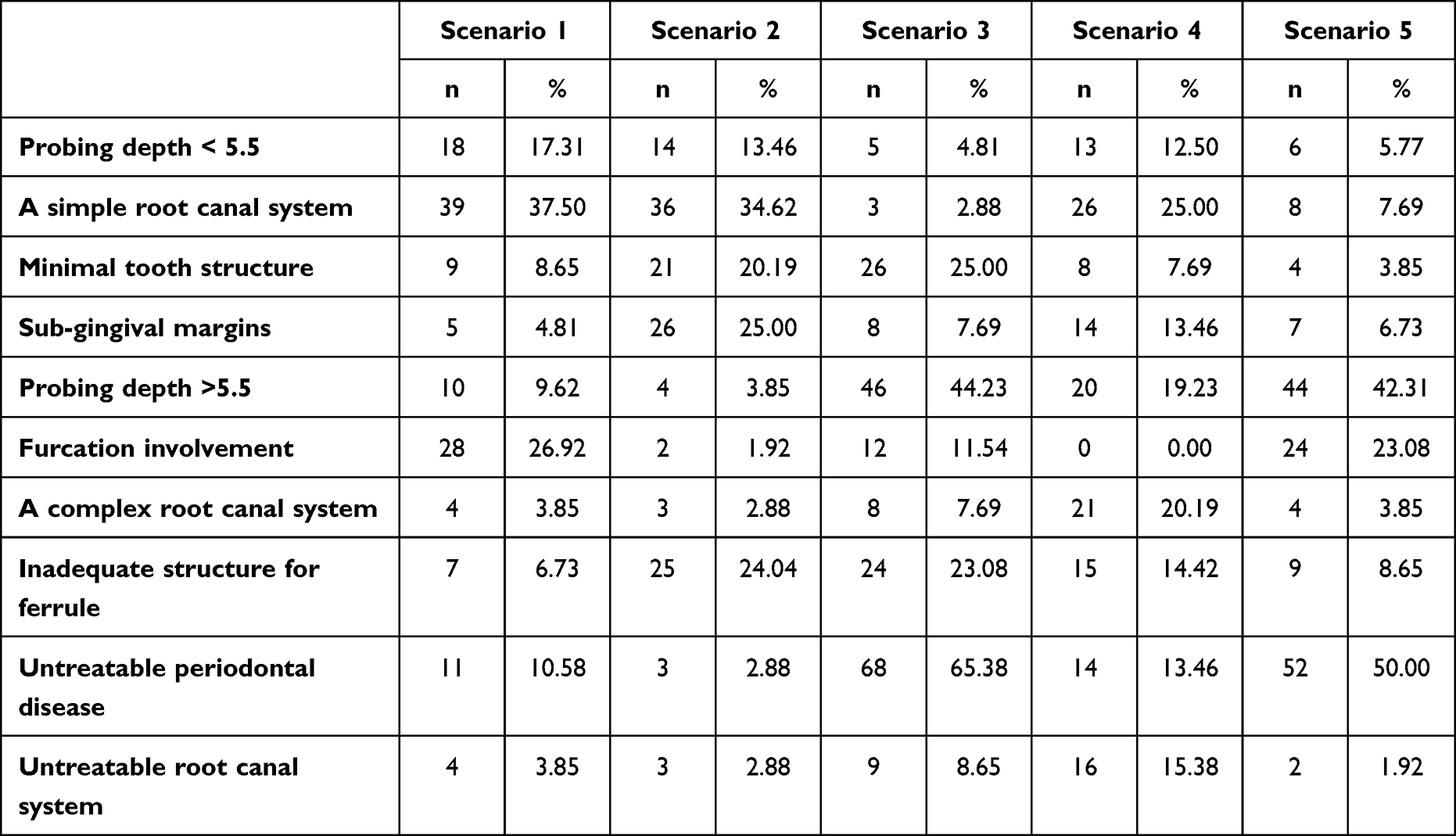 |
Table 7 Reasons of Decision in Each Scenarios Indicated by the Respondents |
Table 8 shows the decision and prognosis of the control group. These data were used to compare the selected decisions and the prognosis by the participants, with different varaibles.
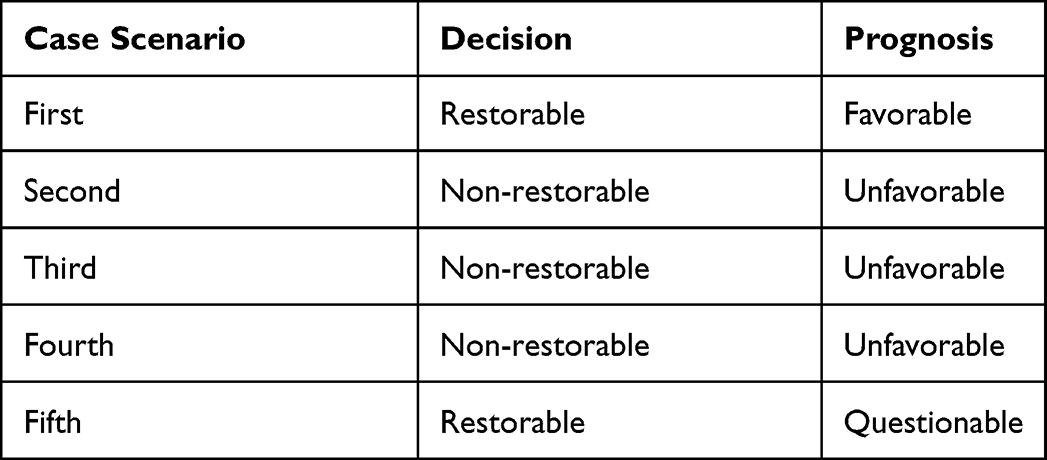 |
Table 8 Control Group’s Decision and Prognosis |
Discussion
The current study aims to assess the ability of dental interns and freshly graduated dentists graduated from different dental colleges to assess tooth restorability. The online survey was used since it is an economic, easy to access, rapid, and efficient method of collecting data.25 Participants’ demographic information, such as gender, years of experience, and place of practice, were gathered. Since studying the influence of experience on the learning curve was out of the scope of this study, the study focused on the interns and recent graduates. Accordingly, the question of experience has been added to include only targeted participants and to help in the interpretation of other questions of background. By conducting the study at multi-centers, the methodology reduced sampling bias and increased external validity.
The study results reported 55.3% of study participants agreed that undergraduate courses prepared dentists to assess the restorability. These abilities received better scores in the majority of the other studies as well.26,27 This was also consistent with the findings of Karaharju-Suvanto et al,28 in which a vast majority of dentist discovered that their undergraduate dentistry course provided them with an appropriate and even extensive instruction in cariology and periodontology. It is apparent that the best competency is obtained in dealing with difficulties that dentists experience regularly in practice, as well as those that students encounter frequently during their dental education. Conversely, the lowest level of competence was observed in sectors with the fewest procedures in general practice. However, 65.7% participants found restorability assessment of tooth is more difficult when they work independently. This finding is consistent with a study done by Gilmore et al29 who found that some students depended on supervisors and got worried when they were not “helping enough”. It could be inferred that undergraduate courses might need to be modified to prepare dentists to take decisions independently since most of the restorability decisions in clinical exposure are made by instructors.
The majority 91.3% of participants were satisfied with their undergraduate courses. This finding agrees with the results of a study conducted by Alqarni et al, 202130 in which more than 88% of respondents were satisfied with their undergraduate courses and thought that the course was pertinent. In addition, the participants felt that dental schools should focus more on restorability assessment in their curriculums. Their suggestion could be due to less exposure to such clinical cases as they face in real practice, where trainees find it difficult to decide the restorability. Generally, decisions of restorability cohere with prognosis, which may indicate that the participants studied the clinical scenarios carefully and answered questions responsibly, Figures 4 and 5.
This study results show no statistically significant association between undergraduate courses of restorability, assess the restorability independent and recommended curriculum with gender and experience (p-value >0.05). This finding is consistent with the findings of Alqarni et al, which found no statistically significant association between the genders and their responses.30 At the respective campuses where they are receiving their professional education, male students provide care for male patients, while female students provide care for female patients.
Since the dental treatment is afforded for free for public in Saudi Arabia, it could be hypothesized that the restorability decisions differ in private sector rather than governmental sector. The results indicated that none of the “decision of restorability” and prognosis showed any statistical significance with place of practice. Similar findings from a study demonstrated that there was a distinction in terms of the restorative threshold between dentists who worked both in private practice and also worked as part-time practitioners in universities. When compared to those who solely worked in university clinics, those who worked in private practice had a significantly larger percentage of dentists who would restore carious lesions at an earlier stage, before they reached into the dentine.31 Other research came to similar conclusions; specifically, that dentists working in public services were more cautious and postponed the surgical intervention more than dentists working in private practices.32,33 Also, Vitaletti believes that considering the cost of establishing a private practise, it is not difficult to imagine that new practitioners would feel significant pressure to make maximum revenue on their first day of working. Practise management consultants advise dental clients that it is easier to achieve such profits by providing costly aesthetic and prosthetic services.34
Adequacy of restorability courses was significantly associated with place of graduation (p<0.05). In contrast to this finding a study conducted by Wazgar et al35 reported no significant difference among general dental practitioners according to their type of dental school. Diversity of the learning outcomes and accordingly different curricula influence graduate in the practice. The learning outcomes of undergraduate courses of developed universities are well established to prepare dentists for restorability assessment according to 75% of the graduates. On the other hand, 62.3% of the graduates from developing and recently established universities disagreed with that. Dental schools should establish dental practice training sessions and arrange regular appointments with practitioners who have adequate dental practice experiences with students and newly graduate dentists in order to improve students’ preparation for the various management facets of dental practice. Dental education is uniquely positioned to enhance the distribution of scientifically based knowledge and encourage collaboration between research and practise. Accelerated adoption of validated approaches for the diagnosis and treatment of dental diseases is required, and the dentist of today must be equipped with the knowledge and tools of tomorrow.36 This will allow students to be better prepared for the various management facets of dental practice.20 Consequently, learning outcomes and teaching measure of such topic might need to be revised in developing and recently established universities. Investigating the learning outcomes of included institutes is out of scope of this paper. However, it is highly recommended to be conducted in further studies especially in the absence of clear learning outcomes from higher authority such as Saudi Commission for Health Specialties. Dental schools and graduates need to know the learning outcomes that they need to achieve prior to dental license exam.8
When deciding whether to restore a damaged or diseased tooth, or whether to advise the patient that restoration is not feasible and the tooth may be better left alone or extracted, a comprehensive approach must be followed. Endodontic, periodontal, and structural integrity need to be evaluated, in addition to patient’s medical and dental health, as well as patient’s expectations.5 It can be observed that the respondents considered this issue when they justified their decisions with reasons. The majority of study participants agreed with the restorability decision in clinical scenario 1 as depicted in Figure 4, but they questioned the likelihood that the tooth would be restorable in the future. Decision and prognosis of the scenario 1 have not shown to be significantly associated with gender, experience, and place of practice. However, there was a statistically significant association between restorability and prognosis of scenario 1 with work place of the study participants. For example, simple root canal system, probing depth < 5.5, Furcation involvement and untreatable periodontal disease were the main four reasons mentioned by the dentists for clinical scenario 1. According to the Patel et al restorability index, this case it was assigned a score of Level 1. The dental interns’ and freshly graduated dental practitioners’ confidence in their abilities to treat this situation might represent their inability and inadequate experience to evaluate the case’s intricacies and may suggest latent incompetence. Similarly, in the second scenario, a simple root canal system, sub-gingival margin, inadequate structure, and minimal tooth structure were the main four factors indicated by the dentists for scenario 2. The decision and prognosis of clinical scenario 2 have not shown any significant association with gender, experience, place of practice and place of study. Based on the Patel et al restorability index, it received a Level 6 score. Not feasible to retain because keeping the tooth, that might or might not be repairable, would significantly impede, complicate, or jeopardize a restoration strategy that is otherwise basic and predictable. These are severe and uncommon cases that require tertiary care management. Persons with life-threatening medical problems, such as those receiving chemotherapy or having severe congestive heart failure, should only receive dental care if it relieves their discomfort.2
In clinical scenario 3, the indicated factors discovered by majority of participants were untreatable periodontal disease, probing depth >5.5 mm, minimal tooth structure, and poor ferule structure. The participants disagreed with decision of restorability and found an unfavorable prognosis of this case. No significant association has been reported between clinical scenario 3 and gender, experience, place of work and place of study. In Patel et al, index level 2 score includes a stable but constrained periodontal support/clinical attachment. In this, category are teeth with short roots (unfavorable crown/root ratio), short conical roots (unfavorable root morphology), grade 2–3 furcation involvement, and teeth with or needing root excision. Despite the fact that this case obtained a level 2 score on the Patel et al index, which indicates that the tooth can be retained with complex treatment, the participants found it extremely challenging to restore the tooth and predict its poor prognosis. When dealing with clinical complexity and uncertainty, a practitioner must determine if they can conduct the treatment and decide when and where to stop if they are unsuccessful. An overconfident practitioner may proceed with treatments without fully understanding and considering the risks, and may lack the skill to carry out the process correctly, whereas an underconfident yet capable clinician may have difficulty working independently.1
In clinical scenario 4, participants had a mixed response to the decision on tooth restorability and prognosis, and they were unsure about selecting the reasons indicated for tooth restorability. This clinical scenario presented a patient with pus discharge from the mandibular right first premolar with a chronic abscesses. It was scored as Level 2 based on the Patel et al restorability index. The participants’ inconsistent reactions could be explained by their lack of confidence in the diagnosis and treatment plans as a result of their lack of experience. A practitioner should ideally have the ability to balance the confidence with understanding of their own barriers and inadequacies, as well as be able to self-evaluate their personal competency.37 In this study, similar to clinical scenario 3, majority of participants indicated that the tooth is non-restorable with unfavorable prognosis in clinical scenario 5. This clinical scenario was presented with maxillary right first premolar, which has a normal pulp and is periodontally affected, has severe gingival recession, it received a level 2 score on the Patel et al restorability index. Most of the participants responded with reasons such as untreatable periodontal disease, probing depth greater than 5.5 mm and furcation involvement of the tooth. The treatment may not have been performed by the interns and newly graduated dental practitioners previously, making it impossible to evaluate their aptitude, or perceived competency. As a result, they would evaluate their level of confidence in their ability to provide the treatment without significant adverse effects. Therefore, confidence involved evaluating risk. Additionally, the practitioners’ confidence enable them to carry out the treatment even after its initial failure.37
The decisions are based on the dentist’s training and skill, the patient’s wishes, and the environment and resources available, such as the availability of equipment.1 Because of the constraints posed by human memory and judgement, it has been shown that there is a significant amount of bias involved in the process of making clinical decisions.38 Dental students are expected to graduate with the knowledge and abilities necessary to provide accurate diagnoses when they enter the workforce. Despite this, a number of studies have shown that general practitioners have a high level of confidence in their ability to execute the dental treatments. It is assumed that this may be the result of a number of factors, including the difficulty of the technical procedures, a lack of comprehension of the goals of treatment and the principles, inadequate teaching at the undergraduate level, and inadequate compensation for the amount of time that is required.39 Therefore, it is essential to place a greater emphasis on the educational methods utilized for students in the undergraduate level, with the goals of enhancing both their knowledge, decision-making and their self-assurance.40
Limitations
Several attempts have been used to distribute the questionnaire through schools and heads of intern and graduate units. Also, monetary incentives were used to motivate participants to respond the questionnaire and spend enough time on the survey’s questions. Since the response rate was 49%, there is a difficulty to generalize the results. However, this study could be a base line for further studies with a large sample size that includes most or all dental schools in Saudi Arabia or internationally to compare variables of the participants.
Conclusions
The inability of dental interns and freshly graduate dental practitioners to make decisions highlighted questions regarding the condition of learning outcomes and graduate attributes. The factor of absence of guidance from the higher authority in Saudi Arabia and the variety of learning outcomes might be negatively influence the ability of interns and newly graduated dental practitioners to assess tooth restorability.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the research ethics committee at Najran University, Reference No.: 443/40-50397-DS. The consent obtained from each participant prior to the commencement of the study was informed consent. The survey was anonymous and voluntary.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The author reports no conflicts of interest.
References
1. Hamer S. The impact of the dental practicality index on treatment planning. Br Dent J. 2021;1–7.
2. Dawood A, Patel S. The dental practicality index–assessing the restorability of teeth. Br Dent J. 2017;222(10):755–758. doi:10.1038/sj.bdj.2017.447
3. Zitzmann NU, Krastl G, Hecker H, et al. Strategic considerations in treatment planning: deciding when to treat, extract, or replace a questionable tooth. J Prosthet Dent. 2010;104(2):80–91. doi:10.1016/S0022-3913(10)60096-0
4. Esteves H, Correia A, Araújo F. Classification of extensively damaged teeth to evaluate prognosis. J Can Dent Assoc (Tor). 2011;77(5):305.
5. Avila G, Galindo-Moreno P, Soehren S, et al. A novel decision‐making process for tooth retention or extraction. J Periodontol. 2009;80(3):476–491. doi:10.1902/jop.2009.080454
6. Messer HH. Clinical judgement and decision making in endodontics. Austra Endodont J. 1999;25(3):124–132. doi:10.1111/j.1747-4477.1999.tb00119.x
7. Friedman S, Mor C. The success of endodontic therapy-healing and functionality. CDA J. 2004;32(6):493–503.
8. Council GD. Preparing for practice. Dental team learning outcomes for registration. 2015:16–17.
9. Tokede O, Walji M, Ramoni R, et al. Treatment planning in dentistry using an electronic health record: implications for undergraduate education. Eur J Dent Educ. 2013;17(1):e34–e43. doi:10.1111/j.1600-0579.2012.00759.x
10. Qualtrough A. Undergraduate endodontic education: what are the challenges? Br Dent J. 2014;216(6):361–364. doi:10.1038/sj.bdj.2014.227
11. Stewardson D. Endodontic standards in general dental practice--a survey in Birmingham, Part I. Eur J Prosthodont Restor Dent. 2001;9(3–4):107–112.
12. Al-Omari MA, Hazaa A, Haddad F. Frequency and distribution of root filled teeth and apical periodontitis in a Jordanian subpopulation. Oral Surg. 2011;111(1):e59–e65.
13. Kielbassa AM, Frank W, Madaus T. Radiologic assessment of quality of root canal fillings and periapical status in an Austrian subpopulation–An observational study. PLoS One. 2017;12(5):e0176724. doi:10.1371/journal.pone.0176724
14. Ray H, Trope M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int Endod J. 1995;28(1):12–18. doi:10.1111/j.1365-2591.1995.tb00150.x
15. Kim Y, Kim SK, Kim KH, et al. Degree of conversion of dual-cured resin cement light-cured through three fibre posts within human root canals: an ex vivo study. Int Endod J. 2009;42(8):667–674. doi:10.1111/j.1365-2591.2009.01565.x
16. De Moor R, Hülsmann M, Kirkevang -L-L, et al. Undergraduate curriculum guidelines for endodontology. Int Endod J. 2013;46(12):1105–1114. doi:10.1111/iej.12186
17. Eliyas S, Chana P, Briggs P. Complex dentistry in general praCtiCe–what would you do? Prim Dent J. 2019;8(3):64–74. doi:10.1308/205016819827601518
18. Ali K, Tredwin C, Kay EJ, et al. Preparedness of dental graduates for foundation training: a qualitative study. Br Dent J. 2014;217(3):145–149. doi:10.1038/sj.bdj.2014.648
19. Ali K, Slade A, Kay E, et al. Preparedness of undergraduate dental students in the United Kingdom: a national study. Br Dent J. 2017;222(6):472–477. doi:10.1038/sj.bdj.2017.272
20. Patel J, Fox K, Grieveson B, et al. Undergraduate training as preparation for vocational training in England: a survey of vocational dental practitioners’ and their trainers’ views. Br Dent J. 2006;201(5):9–15. doi:10.1038/sj.bdj.4814067
21. Oh S-L, Yang JS, Kim YJ. Discrepancies in periodontitis classification among dental practitioners with different educational backgrounds. BMC Oral Health. 2021;21(1):1–8. doi:10.1186/s12903-020-01371-5
22. Oh S, Jones D, Kim JR, et al. Comparison study of diagnosis and treatment planning for dental infections between dental students and practitioners. Healthcare. 2022;10:1393. doi:10.3390/healthcare10081393
23. Guide AD. Treatment Options for the Compromised Tooth. American endodontics association; 2011.
24. American Association of Endodontics. Endodontics: Colleagues for Excellence. Chicago, Illinois: American Association of Endodontists; 2013:1–8.
25. Heiervang E, Goodman R. Advantages and limitations of web-based surveys: evidence from a child mental health survey. Soc Psychiatry Psychiatr Epidemiol. 2011;46(1):69–76. doi:10.1007/s00127-009-0171-9
26. Nicolas E, Baptiste M, Roger‐Leroi V. Clermont‐Ferrand dental school’curriculum: an appraisal by last‐year students and graduates. Eur J Dent Educ. 2009;13(2):93–99. doi:10.1111/j.1600-0579.2008.00547.x
27. Sutton F, Ellituv ZN, Seed R. A survey of self-perceived educational needs of general dental practitioners in the Merseyside region. Prim Dent Care. 2005;os12(3):78–82. doi:10.1308/1355761054348468
28. Karaharju‐Suvanto T, Näpänkangas R, Koivumäki J, et al. Gender differences in self‐assessed clinical competence–a survey of young dentists in F inland. Eur J Dent Educ. 2014;18(4):234–240. doi:10.1111/eje.12092
29. Gilmour A, Welply A, Cowpe JG, et al. The undergraduate preparation of dentists: confidence levels of final year dental students at the School of Dentistry in Cardiff. Br Dent J. 2016;221(6):349–354. doi:10.1038/sj.bdj.2016.686
30. Alqarni MA. Assessing dental students’ professional satisfaction with operative dentistry teaching and curriculum: a study in Saudi Arabia. Medicine. 2021;100(25):e26459. doi:10.1097/MD.0000000000026459
31. Suliman A, Abdo A, Elmasmari H. Restorative treatment decisions on approximal caries among practicing dentists in the college of dentistry clinics, Ajman University, United Arab Emirates. Open Dent J. 2020;14(1):97–102. doi:10.2174/1874210602014010097
32. Vidnes-Kopperud S, Tveit A, Espelid I. Changes in the treatment concept for approximal caries from 1983 to 2009 in Norway. Caries Res. 2011;45(2):113–120. doi:10.1159/000324810
33. Espelid I, Tveit AB, Mejàre I, et al. Restorative treatment decisions on occlusal caries in Scandinavia. Acta Odontol Scand. 2001;59(1):21–27. doi:10.1080/000163501300035724
34. Vitaletti G. Treatment planning: for them or us? 2011:99–100.
35. Wazgar DY, Al-Tuwirqi A, El-Housseiny AA. Knowledge, attitude and practice of a group of dental practitioners in treating deep carious primary teeth in Saudi Arabia. Egypt Dent J. 2019;65:3259–3270. doi:10.21608/edj.2019.74002
36. Kielbassa AM, Purucker P. Dentistry--First and foremost a discipline promoting oral health. Quintessence Int (Berl). 2009;40:707.
37. Stewart J, O’Halloran C, Barton JR, et al. Clarifying the concepts of confidence and competence to produce appropriate self‐evaluation measurement scales. Med Edu. 2000;34(11):903–909. doi:10.1046/j.1365-2923.2000.00728.x
38. McCreery AM, Truelove E. Decision making in dentistry. Part I: a historical and methodological overview. J Prosthet Dent. 1991;65(3):447–451. doi:10.1016/0022-3913(91)90241-N
39. AlHamoudi SS, AlRashidi SN, AlHarbi HA, et al. Confidence in performing endodontic treatment and perception of the quality of endodontic education. Arch Pharm Pract. 2021;1:94. doi:10.51847/lWjk1PplzO
40. Awooda EM, Mudathir MS, Mahmoud SA. Confidence level in performing endodontic treatment among final year undergraduate dental students from the University of Medical Science and Technology, Sudan (2014). Saudi Endodont J. 2016;6(1):26. doi:10.4103/1658-5984.172000
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.