")
Back to Journals » OncoTargets and Therapy » Volume 10
TERT-CLPTM1 locus polymorphism (rs401681) is associated with the prognosis of hepatocellular carcinoma
Authors Lee HW , Park W, Heo Y, Park TI, Park SY, Lee J
Received 17 April 2017
Accepted for publication 5 September 2017
Published 3 October 2017 Volume 2017:10 Pages 4853—4858
DOI https://doi.org/10.2147/OTT.S138956
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Geoffrey Pietersz
Hye Won Lee,1,* Won-Jin Park,2,* Yu-Ran Heo,2 Tae In Park,3 Soo Young Park,4 Jae-Ho Lee2,*
1Department of Pathology, Keimyung University School of Medicine, Daegu, Republic of Korea; 2Department of Anatomy, Keimyung University School of Medicine, Daegu, Republic of Korea; 3Department of Pathology, Kyungpook National University School of Medicine, Daegu, Republic of Korea; 4Department of Internal Medicine, Kyungpook National University School of Medicine, Daegu, Republic of Korea
*These authors contributed equally to this work
Abstract: Telomere length is associated with the development of hepatocellular carcinoma (HCC), and recent studies have focused on the genetic alteration or polymorphism in telomere-maintaining genes. We examined the clinicopathologic and prognostic value of rs401681 polymorphism, located in the TERT-CLPTM1L locus, in HCC. The relationship between rs401681 variants and telomere length was also analyzed in 156 HCC patients. The rs401681 polymorphism had the following genotype frequencies: C/C in 51.3% of the samples, C/T in 39.7%, and T/T in 9.0%. Telomeres in the tumor samples were 4.04-fold longer, on average, than the telomeres in matched normal samples (SD =1.32), and there were no differences in telomere length according to rs401681 polymorphism (p=0.802). Our results indicate that the rs401681 C allele was significantly associated with increased T and International Union for Cancer Control stages (p<0.01). Univariate and multivariate survival analyses showed that HCC with C allele had poorer prognosis (p<0.01). In conclusion, our findings suggest that rs401681 is a possible prognostic biomarker for HCC patients.
Keywords: CLPTM1L polymorphism, hepatocellular carcinoma, TERT-CLPTM1L locus, telomere length
Introduction
Telomeres are repetitive (TTAGGG)n sequences into arrays of up to 25 kb and cap the end of linear chromosomes in human cells. They play a key role in counteracting the end-replication losses that occur as a consequence of semiconservative replication of linear DNA molecules. Telomere length (TL) is maintained mainly by telomerase, a ribonucleoprotein that forms part of a protein complex that allows the addition of repetitive sequences to the 30 chain during DNA replication as a protective action against chromosome erosion. Particularly, TL showed a significant association with the prognosis of patients in various malignancies, although the prognosis according to length varies according to the type of tumor.1,2
A large number of genes and gene products are involved in this process. Specifically, the telomerase contains two key genes: telomerase reverse transcriptase (TERT) gene and cleft lip and palate transmembrane 1 like gene (CLPTM1L; alias CRR9; MIM612585). The TERT gene encodes for the telomerase enzyme, and the CLPTM1L gene product seems to participate in TERT regulation through some regions in the 30 end, called the TERT-CLPTM1L locus.3–5 According to the large single-nucleotide polymorphism (SNP) database of TERT-CLPTM1L locus, rs401681 (C.T, located in the intron 13 of CLPTM1L and 27 kb from the TERT gene) is one of the most extensively studied SNPs. However, effects of this SNP varied extremely across cancer types. In lung cancer and melanomas, T allele (minor allele) was associated with cancer risk, whereas C allele (major allele) increased the risk of lung, bladder, and prostate cancers.6
Hepatocellular carcinoma (HCC) is the most common type of primary liver cancer in adults and is a leading cause of death from cancer worldwide. Moreover, the incidence and mortality rates of HCC still continue to increase.7 Up to now, there have been many studies on diagnostic genes, prognostic factors, and genes for target therapy. There was a previous SNP study of TERT-CLPTM1 locus in HCC demonstrating that the T allele was associated with a significantly increased risk of HCC.8
In this study, we investigated whether rs401681 of TERT-CLPTM1 locus is closely associated with survival outcome in HCC, together with the clinicopathologic characteristics. The associations between this polymorphism and TERT promoter mutation and TL were also investigated based on our previous report.9
Patients and methods
Patients and tissue samples
We evaluated 156 HCC patients who underwent surgical resection as first-line treatment at the Kyungpook National University Hospital from January 2006 to December 2010. HCC was diagnosed and treated according to the American Association for the Study of Liver Diseases guidelines. The clinicopathologic parameters of the patients were re-evaluated by a review of the patients’ medical records, including age, sex, tumor size, laboratory results, and etiology of underlying liver disease. The age of the patients was based on the time of curative surgical resection. We have included this in the text. The TNM stage was evaluated according to the seventh edition of the American Joint Committee on Cancer staging system. Patients dying of causes other than HCC, patients with cancer at other sites, and patients lost to follow-up were excluded from this study. We also excluded patients who had received prior treatments such as local ablation therapy and transarterial chemoembolization. The study was approved by the institutional review board (KNUH-2014-04-056-001). All patients provided written informed consent at the time of their treatment for the use of material and medical records in future research.
SNP genotyping
Peripheral venous blood samples were collected, and DNA was extracted by using a QIAamp DNA Mini Kit (Qiagen NV, Venlo, the Netherlands). The polymerase chain reaction (PCR) amplification of the TERT-CLPTM1 locus for SNP study was performed as described previously, with minor modification.4 PCR was performed using AmpliTaq Gold (Thermo Fisher Scientific, Waltham, MA, USA). The PCR products were electrophoresed on 1.5% agarose gel and stained with ethidium bromide to confirm the size of the bands. Then, direct DNA sequencing was performed using the ABI 3730 DNA sequencer (Bionics Inc., Korea).
TERT promoter mutation and TL analysis
Surgically removed HCC specimens and corresponding nonmalignant liver tissues were formalin fixed and paraffin embedded. Paraffin blocks containing representative tumor lesions were selected after review of the corresponding hematoxylin and eosin slides. Representative lesions from each case were marked on the paraffin blocks and cored with a 3.0 mm diameter cylindrical device manually. Genomic DNA was extracted by using a QIAamp DNA Mini Kit (Qiagen). PCR amplification of the TERT promoter region was performed as described previously. Then, the PCR products were directly sequenced in both forward and reverse directions. All mutations were verified by analysis of an independent PCR isolate.
TL was examined using a real-time PCR assay. For the quantitative determination of content relative to DNA, primers for specific amplification of telomere and β-globin gene were selected according to a previous study.9 Real-time PCR was then carried out on the LightCycler 480 II system (Hoffman-La Roche Ltd., Basel, Switzerland) with a total volume of 20 μL of the reaction mixture. Each measurement was repeated in triplicate, and five serially diluted control samples were included in each experiment. The relative TL was calculated with the 2−ΔΔCT method. First, TL was normalized with β-globin gene; the TL of the tumor sample was compared with the mean level of TL in normal liver tissues and expressed as an n-fold ratio.
Statistical analysis
Chi-square, Fisher’s exact test, Mann–Whitney U test, Kruskal–Wallis, and simple correlation analysis were used to analyze the relationship between variables. Survival curves, estimated with the Kaplan–Meier method (univariate analysis), were compared by log-rank test. Overall survival (OS) was defined as the time between diagnosis and death from either disease or from other causes. Disease-free survival (DFS) was defined as the time between diagnosis and disease recurrence or development of distant metastasis. We used Cox proportional hazard modeling to calculate the hazard ratios (HRs) and 95% CIs, using time since diagnosis as the underlying time metric. For the multivariate models, we adjusted for age at diagnosis, sex, tumor size, aspartate transaminase, and alanine transaminase (ALT). All p-values <0.05 were considered statistically significant.
Results
Demographics of patients according to rs401681 genotype
The study population was composed of 117 males and 39 females with a median age of 57 years (range, 37–78 years). The genotype frequencies of rs401681 polymorphisms were as follows: C/C, 51.3%; C/T, 39.7%; T/T, 9.0%. The frequency of the rs401681 C allele was 0.71 (T allele 0.29), consistent with previously described values for Korean controls.10 The clinicopathologic characteristics of rs401681 polymorphism in HCC are presented in Table 1. The rs401681 C allele was statistically associated with T stage (p=0.003) and International Union for Cancer Control stage (p=0.008). TERT promoter mutation was found in 26.9% of the patients (42/156). TL was analyzed in 156 patients with HCC. Average of TL in HCC was 4.04-fold longer than that in matched normal tissues (SD =1.32). The mean TLs of HCC patients with C/C, T/T, and C/T alleles were 3.45-fold (SD =1.01), 2.60-fold (SD =0.83), and 5.11-fold (SD =1.56), respectively, which showed no statistical difference (p=0.802; Figure 1). The rs401681 polymorphisms did not have any relationship with other clinical parameters, TL, and TERT promoter mutation.
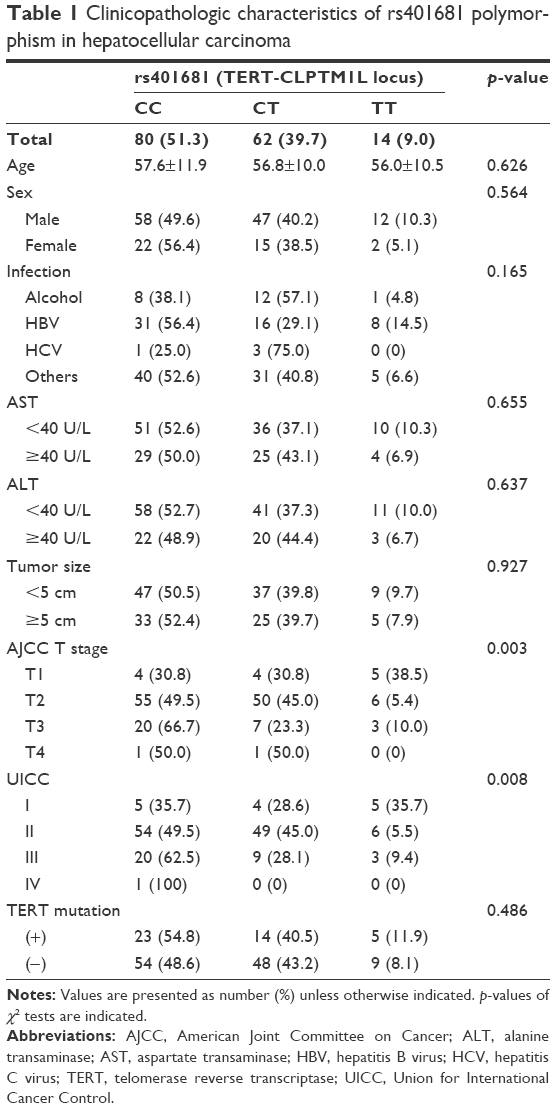 | Table 1 Clinicopathologic characteristics of rs401681 polymorphism in hepatocellular carcinoma |
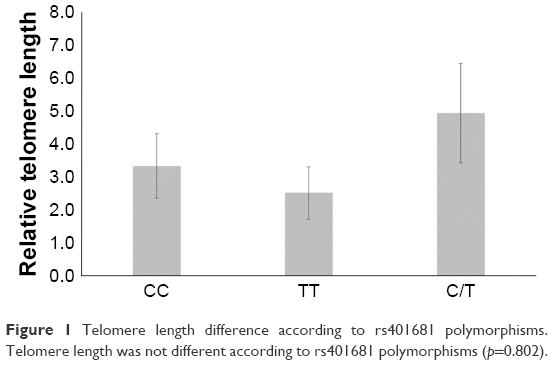 | Figure 1 Telomere length difference according to rs401681 polymorphisms. Telomere length was not different according to rs401681 polymorphisms (p=0.802). |
Prognostic value of rs401681 polymorphisms in HCC
We then conducted survival analysis to clarify the prognostic significance of rs401681 polymorphisms in HCC. The median follow-up of patients for survival analysis was 70.6 months (range, 3–101). Univariate survival analysis performed by Kaplan–Meier curve showed a shorter DFS in HCC patients with C/C allele (40.05 versus 65.7 [T/T] and 60.0 [C/T] months, χ2=8.33, p=0.016), as shown in Figure 2. However, OS was not different according to this polymorphism in HCC (67.8 [C/C] versus 50.6 [T/T] and 74.8 [C/T] months, χ2=0.68, p=0.710), as shown in Figure 2. Then, we compared the C/C genotype with T allele carriers (C/T + T/T). C allele (40.05 months) was significantly associated with poor DFS (versus 58.0 [T/T and C/T] months, χ2=7.47, p=0.006), though OS result was not different (67.8 [C/C] versus 74.1 [T/T and C/T] months, χ2=0.62, p=0.431), as shown in Figure 2.
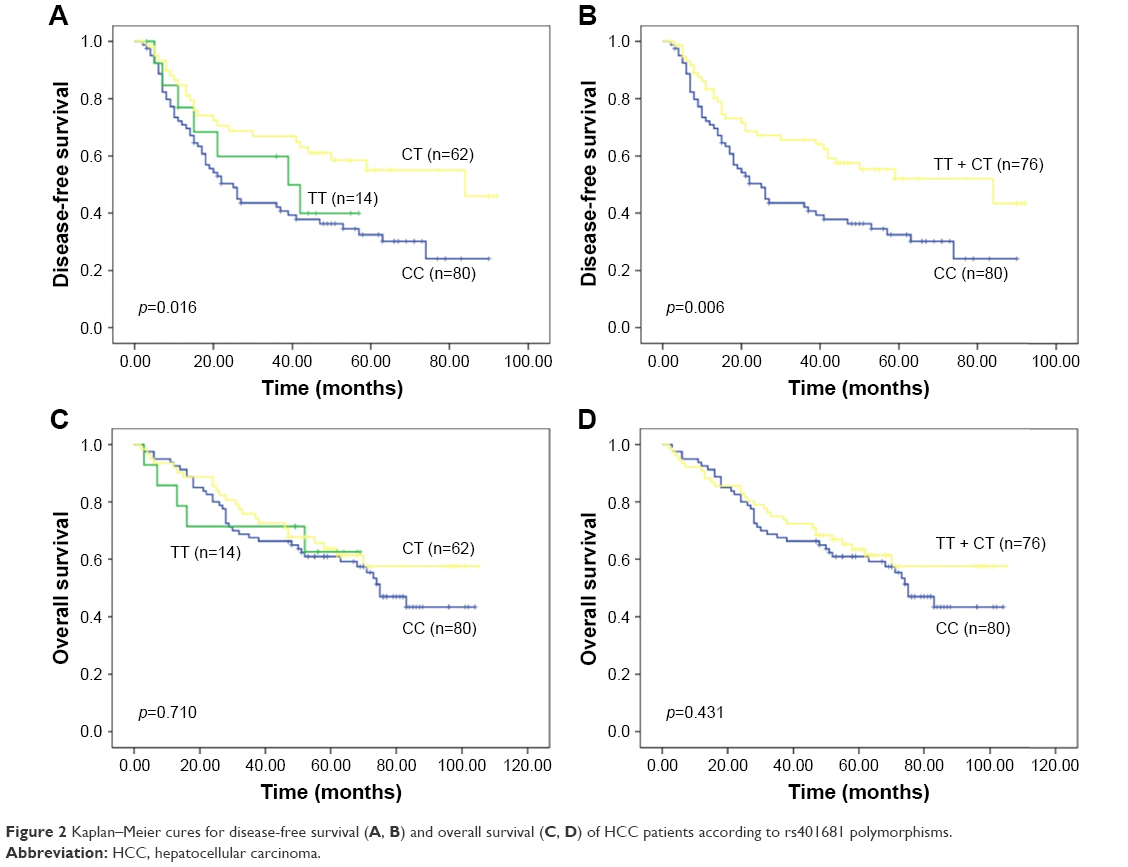 | Figure 2 Kaplan–Meier cures for disease-free survival (A, B) and overall survival (C, D) of HCC patients according to rs401681 polymorphisms. |
To evaluate whether rs401681 polymorphism is an independent prognostic predictor in HCC, we further analyzed the data by using the Cox proportional hazards regression model after adjusting for possible confounders of survival (Table 2). Multivariate analysis showed that rs401681 polymorphism is a potential marker for independent prognostic factors (HR for DFS =1.88, 95% CI: 1.03–3.44, p=0.040; HR for OS =1.07, 95% CI: 0.63–1.83, p=0.800).
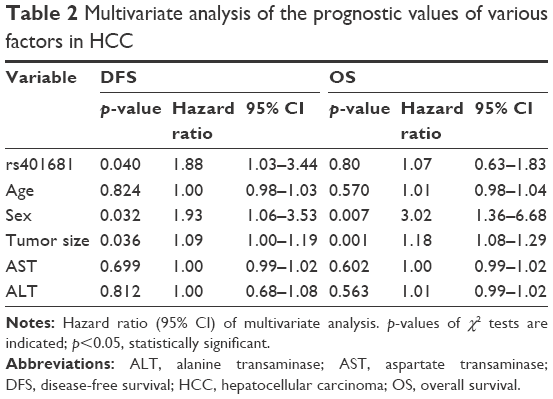 | Table 2 Multivariate analysis of the prognostic values of various factors in HCC |
Discussion
Telomeres are involved in maintaining genomic stability. Telomere biology plays a critical role in the initiation and progression of cancer in various aspects.3 There are various genes and proteins associated with the synthesis of telomerase (TERT, TERC, CLPTM1L, and so on) and telomere binding protein (such as TRF1, TRF2, POT1, TIN2, RAP1, and so on).3 The TL is controlled by the interaction of these various telomere-related genes.11 Among these, two novel telomere-associated genes, TERT and CLPTM1L, have been widely studied in cancer research.6,8 TERT gene encodes the catalytic subunit of telomerase reverse transcriptase, and this promoter mutation and dysregulated expression were proved in diverse human malignancies.3 Our previous study has demonstrated that TERT promoter mutation is frequent in HCC, and TL has some association with age, American Joint Committee on Cancer T stage, OS, and infection status. Also, TL might have a potential value as a prognostic factor in HCC. According to many reports, while shortened tumor TL shows poorer prognosis in most solid tumors, HCC has been observed with favorable prognosis as in colorectal cancer.1,9
CLPTM1L gene may be involved in apoptotic response and its expression level affects the sensitivity of cancer cell lines to anticancer drugs.4 Various genome-wide association studies have identified SNPs in the CLPTM1L-TERT gene whose locus is at chromosome 5p15.33, and rs401681 is one of the significant cancer-associated SNPs.6,8,10 It has been reported to increase the risk of various malignancies, including lung cancer, which is the most widely studied tumor type, basal cell carcinoma of skin, prostate cancer, and urinary bladder cancer.6,12 But other studies showed various genetic effects according to cancer type. The individuals with rs401681 polymorphism are rather at lower risk of melanoma and colorectal cancer.6 Also, there was no association between rs401681 and breast and endometrial cancer risk.5
However, to date, very little is known about the genetic polymorphisms of TERT-CLPTM1L on the HCC. Only one study has been conducted on the TERT-CLPTM1L HCC susceptibility variant in Chinese patients. Su et al found that rs401681 T allele of CLPTM1L was associated with a significantly increased risk of HCC (odds ratio, 1.399; 95% CI: 1.002–1.955). Also, this study showed the interaction of rs401681 polymorphism and other polymorphisms in HCC.4 This study focused on the association between rs401681 genotype and clinicopathologic parameters including survival analysis in HCC patients. To our knowledge, this is the first study describing evidence on the association between SNP rs401681 and clinical behavior of HCC.
The distribution of allele frequency in HCC was similar to that reported in a previous study conducted in Korean population.10 Another study has shown that there is a link between rs401681 C allele and telomere shortening,6 but several reports have not demonstrated an association between the risk allele and mean TL in a variety of malignancies.13,14 A recent study also suggested that the combination of the rs2853669 and TERT mutation indicates poor prognosis in HCC.15 However, we found no evidence that SNP rs401681 is associated with mean TL or TERT mutation. In our previous study, we found that ALT level and TL were significantly related.9 But in this study, aspartate transaminase and ALT were not associated with TERT-CLPTM1 locus polymorphism.
Interestingly, we did find significant associations between SNP rs401681 and TNM stage and survival, that is, worse prognosis in patients with the C allele. Our findings revealed that rs401681 C/C or C/T genotype was significantly related to an increased risk of disease relapse in HCC patients, compared with those carrying the T/T genotype. Furthermore, Cox multivariate analysis demonstrated that rs401681 polymorphism was an independent prognostic factor in HCC. In other cancers, the possibility of using it as a genetic marker has been suggested,9,16,17 and this is the first study demonstrating that in HCC. Further larger scale studies are needed to confirm the role of this possible genetic marker, and then, its molecular mechanism should be clarified.
To summarize, HCC patients with SNP rs401681 allele C had a tendency to develop advanced disease and poor DFS. Our data suggest that the genetic variant in TERT-CLPTM1L is implicated in HCC aggressiveness. This study had some limitations. TL may also be affected by lifestyle and environmental factors, such as alcohol and obesity, as well as socioeconomic factors and psychologic stress.18,19 Therefore, a carefully designed study with subdivided patients is needed. The biologic functions of rs401681 polymorphism are of great interest for HCC research.
Acknowledgments
This study was supported by grants of the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education (NRF-2014R1A6A3A04058057), and by the Korean Government (MSIP; No 2014R1A5A2010008).
Author contributions
Conceptualization: Lee HW, Lee JH; data curation: Park WJ, Heo YR, Lee HW; formal analysis: Lee HW, Lee JH; funding acquisition: Lee JH; investigation: Park WJ, Park TI, Park SY, Heo YR; methodology: Park WJ, Park TI, Park SY, Heo YR; project administration: Lee HW, Lee JH; resources: Lee HW, Park WJ, Park TI, Park SY, Heo YR; supervision: Lee JH; validation: Lee HW, Lee JH; visualization: Park WJ, Heo YR, Lee JH; writing original draft: Lee HW, Lee JH; writing review and editing: Lee HW, Park WJ, Park TI, Park SY, Heo YR, Lee JH. All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Svenson U, Roos G. Telomere length as a biological marker in malignancy. Biochim Biophys Acta. 2009;1792(4):317–323. | ||
Wentzensen IM, Mirabello L, Pfeiffer RM, Savage SA. The association of telomere length and cancer: a meta-analysis. Cancer Epidemiol Biomarkers Prev. 2011;20(6):1238–1250. | ||
Kim NW, Piatyszek MA, Prowse KR, et al. Specific association of human telomerase activity with immortal cells and cancer. Science. 1994;266(5193):2011–2015. | ||
Yamamoto K, Okamoto A, Isonishi S, Ochiai K, Ohtake Y. A novel gene, CRR9, which was up-regulated in CDDP-resistant ovarian tumor cell line, was associated with apoptosis. Biochem Biophys Res Commun. 2001;280(4):1148–1154. | ||
Mocellin S, Verdi D, Pooley KA, et al. Telomerase reverse transcriptase locus polymorphisms and cancer risk: a field synopsis and meta-analysis. J Natl Cancer Inst. 2012;104(11):840–854. | ||
Rafnar T, Sulem P, Stacey SN, et al. Sequence variants at the TERT-CLPTM1L locus associate with many cancer types. Nat Genet. 2009;41(2):221–227. | ||
Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2017. CA Cancer J Clin. 2017;67(1):7–30. | ||
Su LY, Li XL, Shen L, et al. Polymorphisms of TERT and CLPTM1L and the risk of hepatocellular carcinoma in Chinese males. Asian Pac J Cancer Prev. 2014;15(19):8197–8201. | ||
Lee HW, Park TI, Jang SY, et al. Clinicopathological characteristics of TERT promoter mutation and telomere length in hepatocellular carcinoma. Medicine. 201;96(5):e5766. | ||
Bae EY, Lee SY, Kang BK, et al. Replication of results of genome-wide association studies on lung cancer susceptibility loci in a Korean population. Respirology. 2012;17(4):699–706. | ||
Lechel A, Manns MP, Rudolph KL. Telomeres and telomerase: new targets for the treatment of liver cirrhosis and hepatocellular carcinoma. J Hepatol. 2004;41(3):491–497. | ||
Yin J, Li Y, Yin M, et al. TERT-CLPTM1L polymorphism rs401681 contributes to cancers risk: evidence from a meta-analysis based on 29 publications. PLoS One. 2012;7(11):e50650. | ||
Mirabello L, Yu K, Kraft P, et al. The association of telomere length and genetic variation in telomere biology genes. Hum Mutat. 2010;31(9):1050–1058. | ||
Pooley KA, Tyrer J, Shah M, et al. No association between TERT-CLPTM1L single nucleotide polymorphism rs4,01,681 and mean telomere length or cancer risk. Cancer Epidemiol Biomarkers Prev. 2010;19(7):1862–1865. | ||
Ko E, Seo HW, Jung ES, Kim BH, Jung G. The TERT promoter SNP rs2853669 decreases E2F1 transcription factor binding and increases mortality and recurrence risks in liver cancer. Oncotarget. 2016;7(1):684–699. | ||
Azad AK, Qiu X, Boyd K, et al. A genetic sequence variant (GSV) at susceptibility loci of 5p15.33 (TERT-CLPTM1L) is associated with survival outcome in locally advanced and metastatic non-small-cell lung cancer (NSCLC). Lung Cancer. 2014;84(3):289–294. | ||
Zhao X, Wang S, Wu J, et al. Association of TERT polymorphisms with clinical outcome of non-small cell lung cancer patients. PLoS One. 2015;10(5):e0129232. | ||
Kachuri L, Latifovic L, Liu G, Hung RJ. Systematic review of genetic variation in chromosome 5p15.33 and telomere length as predictive and prognostic biomarkers for lung cancer. Cancer Epidemiol Biomarkers Prev. 2016;25(12):1537–1549. | ||
Bisoffi M, Heaphy CM, Griffith JK. Telomeres: prognostic markers for solid tumors. Int J Cancer. 2006;119(10):2255–2260. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.