Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Tenecteplase in Ischemic Stroke: Challenge and Opportunity
Authors Li G, Wang C, Wang S ![]() , Xiong Y, Zhao X
, Xiong Y, Zhao X ![]()
Received 3 February 2022
Accepted for publication 15 April 2022
Published 11 May 2022 Volume 2022:18 Pages 1013—1026
DOI https://doi.org/10.2147/NDT.S360967
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Guangshuo Li,1 Chuanying Wang,1 Shang Wang,1,2 Yunyun Xiong,1– 3,* Xingquan Zhao1,2,*
1Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 2China National Clinical Research Center for Neurological Diseases, Beijing, People’s Republic of China; 3Chinese Institute of Brain Research, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xingquan Zhao, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, West Nansihuan Road 119, Beijing, People’s Republic of China, Email [email protected] Yunyun Xiong, China National Clinical Research Center for Neurological Diseases, Beijing, People’s Republic of China, Email [email protected]
Purpose of Review: Intravenous thrombolysis is the first-line therapy for ischemic stroke, and alteplase has been used as an intravenous thrombolysis drug for over 20 years. However, considering its low rate of recanalization and risk of intracerebral hemorrhage, alteplase may not be the optimal thrombolytic drug of choice for ischemic stroke. Tenecteplase (TNK) is a genetically engineered, mutant, tissue plasminogen activator that is a potential substitute to alteplase in ischemic stroke. The pharmacokinetic advantages of TNK include greater fibrin selectivity than alteplase and prolonged half-life time. In this review, we have summarized the clinical trials of TNK in ischemic stroke.
Recent Findings: Clinical trials showed a higher recanalization rate of TNK over alteplase without increasing the rate of intracerebral hemorrhage. However, not all clinical trials showed superiority of TNK over alteplase in functional outcomes and early neurological improvement. TNK was superior to alteplase in terms of recanalization in patients who fulfilled the imaging mismatch criteria and in those planning to undergo mechanical thrombectomy.
Summary: TNK has the potential to substitute alteplase for ischemic stroke therapy. Future TNK clinical trials that target functional outcomes are warranted.
Keywords: stroke, thrombolysis, TNK-tissue plasminogen activator, tenecteplase, clinical trial
Introduction
In the global burden of disease study 2019, stroke ranked third among the main causes of disability-adjusted life-years.1 Of all strokes, >80% are ischemic strokes due to intracranial or extracranial vessel occlusion.2 Recanalization of occluded vessels in the ultra-early period is crucial to improving functional outcomes of patients with ischemic stroke. Hence, reperfusion therapy, especially intravenous thrombolysis, has been recommended as the first-line therapy of ischemic stroke in the current guidelines.3
Clinical trials4–6 on recombinant tissue plasminogen activator (rtPA) have demonstrated its efficacy in ischemic stroke 20 years ago. In the very beginning, the National Institute of Neurological Disorders and Stroke rt-PA Stroke Study, also known as the NINDS trial,4 proved the efficacy and safety of intravenous thrombolysis alteplase in the 3-h time window of ischemic stroke onset in 1995. The European Cooperative Acute Stroke Study III trial, also known as the ECASS III trial,7 extended the time window of alteplase to 4.5 h. The Efficacy and Safety of MRI-Based Thrombolysis in Wake-Up Stroke (WAKE-UP) trial6 and the EXtending the time for Thrombolysis in Emergency Neurological Deficits (EXTEND) trial8 showed that alteplase can be used in wake-up stroke, un-witnessed stroke, and unknown-onset stroke.
Tenecteplase (TNK) is a genetically engineered, mutant, tissue plasminogen activator that has shown a greater recanalization rate than alteplase in acute myocardial infarction as well as a lower risk of hemorrhagic events.9 Several clinical trials10–19 were conducted to test the efficacy and safety of TNK in reperfusion therapy for ischemic stroke. The 2019 American Heart Association/American Stroke Association Guidelines20 recommended 0.4 mg/kg TNK as an alternative to alteplase in patients with mild neurological impairment and no major intracranial occlusion. Moreover, 0.25 mg/kg TNK was recommended in the 2019 American Heart Association/American Stroke Association Guidelines20 in patients without contraindications for intravenous (IV) fibrinolysis who were also eligible to undergo mechanical thrombectomy. Considering the limited clinical trials on TNK, the class of recommendation and level of evidence are low (IIb, B-R). The 2021 European Stroke Organisation Guidelines21 recommended 0.25 mg/kg TNK over 0.9 mg/kg alteplase before mechanical thrombectomy within 4.5 h from stroke onset. However, the recommendation of TNK over alteplase was based on expert consensus recommendation with a weak strength of recommendation and low quality of evidence. In the real-world clinic, TNK is still used cautiously to treat ischemic stroke, and more clinical trials on TNK in ischemic stroke are needed. In this review, we summarize the clinical trials on TNK in ischemic stroke (Table 1).
 |
Table 1 Clinical Trials on TNK in Ischemic Stroke |
Pharmacokinetic Comparison
Because fibrin molecules bind to each other and form the skeleton of a thrombus22,23 (Figure 1), it can be lysed through fibrinolysis. Tissue plasminogen activator (tPA) is generated in endothelial cells to convert plasminogen into plasmin. Plasmin breaks down the fibrin skeleton by converting fibrin into fibrinogen degradation products, and the thrombus is eventually dissolved to achieve recanalization of the occluded vessel.
 |
Figure 1 Mechanism of thrombosis. |
Similar to alteplase, TNK is also a 527-amino acid-modified human tissue plasminogen activator that contains the fibronectin finger, epidermal growth factor, kringle 1, kringle 2, and serine protease domains. However, three amino acids are substituted in TNK compared to alteplase: the substitution of threonine 103 with asparagine and glutamine 117 with asparagine has increased the half-life of TNK; the amino acid replacement in positions 296–299 has enhanced its resistance to plasminogen activator inhibitor-1 (PAI-1) and potentiated fibrin specificity.24 The different biomolecular structure of TNK has given it more pharmacological advantages over alteplase25 (Table 2). The prolonged half-life enables TNK to be administered as a single intravenous bolus rather than a bolus and continuous infusion. The single bolus of TNK is more convenient for “drip and ship” cases. Moreover, poor fibrin selectivity of alteplase results in excessive systematic bleeding events and disintegration of the blood–brain barrier leading to post-stroke cerebral edema and hemorrhagic transformation.26 Alteplase also causes more damage to the fibrinolytic system than TNK and increases the risk of intracerebral hemorrhage.26,27 Further, alteplase inhibits platelet aggregation and influences the coagulation process with an elevated risk of hemorrhagic events.28,29 Therefore, theoretically, TNK is a better thrombolytic agent than alteplase with lower risk of side-effects when administrated intravenously in ischemic stroke patients.25
 |
Table 2 Pharmacokinetic Comparison Between Alteplase and TNK |
Optimal Dose in Ischemic Stroke
A pilot dose-escalation safety study was conducted to investigate the safety and efficacy of TNK in ischemic stroke patients (n=88) at four doses (0.1 mg/kg, 0.2 mg/kg, 0.4 mg/kg, 0.5 mg/kg).10 The occurrence of symptomatic intracranial hemorrhage (sICH) at TNK doses of 0.1 mg/kg, 0.2 mg/kg, and 0.4 mg/kg were lower than that of alteplase (0% vs 0% vs 0% vs 15%, respectively). A phase IIb, randomized, double-blind trial was conducted in 2010 to compare the three doses of TNK (0.1 mg/kg, 0.25 mg/kg, and 0.4 mg/kg) with alteplase.12 The trial was terminated prematurely because patient enrolment was very slow, with only 112 patients being finally enrolled. The dose of 0.4 mg/kg TNK was prematurely terminated considering its poor performance in both efficacy and safety; in terms of good outcome (combining major neurological improvement and symptomatic ICH), the 0.25 mg/kg TNK group had the highest proportion (15/31, 48.4%), followed closely by the 0.1 mg/kg TNK group (14/31, 45.2%). By comparison, the rt-PA group had 41.9% (13/31) good outcomes. The difference between the 0.25 mg/kg and 0.1 mg/kg groups was not statistically significant because of the insufficient sample size after patient enrolment was terminated (n=112). Moreover, the study did not show conclusive results for an optimal dose of TNK in ischemic stroke.
The Tenecteplase VERSUS Alteplase for Acute Ischemic Stroke (TAAIS) trial enrolled patients with middle cerebral artery (MCA) occlusion on CTA and reversible penumbra on CTP (n=75) and showed the superiority of 0.25 mg/kg TNK over 0.1 mg/kg TNK among all the efficacy endpoints (mean rates of reperfusion at 24 h: 88.8% vs. 69.3%, P=0.006; complete recanalization at 24 h: 80% vs. 35%, P=0.002; median improvement in National Institutes of Health Stroke Scale score at 24 h: 11 vs. 7, P=0.0059; and mRS 0–1: 72% vs. 36%, P=0.011). However, no significant difference was detected in safety endpoints between the two doses of TNK (sICH: 4% vs. 4%, P=1.000).13 The TAAIS trial13 and another meta-analysis30 both implied that the optimal dosage of TNK in ischemic stroke may be 0.25 mg/kg, and this dosage was utilized in subsequent Phase II and Phase III trials including ATTEST (Alteplase vs. tenecteplase for thrombolysis after ischaemic stroke),15 TEMPO-1 (Tenecteplase–Tissue-Type Plasminogen Activator Evaluation for Minor Ischemic Stroke With Proven Occlusion),14 and EXTEND-IA TNK (Tenecteplase vs. Alteplase before Endovascular Therapy for Ischemic Stroke trial).17 The TEMPO-1 study also found that there were no serious drug-related adverse events in the 0.1 mg/kg TNK group. In the 0.25 mg/kg TNK group, there was one sICH (4%). Comparable risks of sICH were found between the 0.1 mg/kg TNK and 0.25 mg/kg TNK groups. Owing to a small sample size (n=100) and non-randomized study design, it was served as a safety and feasibility trial. The Norwegian tenecteplase stroke trial (NOR-TEST trial),16 a phase III trial with over 1000 enrolled patients, utilized 0.4 mg/kg TNK and failed to prove the superiority of TNK over alteplase on functional outcomes (mRS score 0–1 at 3 months: 64% vs. 63%, P=0.52). Safety outcomes were also similar between the TNK and alteplase groups (sICH: 3% vs. 2%, P=0.49; death within 3 months: 5% vs. 4%, P=0.49). The limitations of the NOR-TEST trial16 included a large proportion of TIA and stroke mimics (25%) and mild neurological impairment (median NIHSS score=4) that decreased its external validation. The EXTEND-IA TNK 2 trial failed to prove the superiority of 0.4 mg/kg TNK compared with 0.25 mg/kg TNK. Per another study,18 0.25 mg/kg was the optimal dosage for patients undergoing bridge therapy. (intravenous thrombolysis [IVT]+mechanical thrombectomy [MT])
Recanalization and Reperfusion
The TAAIS trial demonstrated that TNK was superior to alteplase in reperfusion at 24 h (79.3% vs 55.4%, P=0.004).13 The ATTEST trial failed to demonstrate the superiority of TNK over alteplase in reperfusion.15 The TAAIS trial13 only enrolled patients with a reversible penumbra on CTP and limited the percentage of hypoperfusion area volume (at least 20% greater than the infarct core lesion), whereas the ATTEST trial15 did not. While MR-DWI was used in most trials, the infarction core volume was measured via non-contrast CT in the ATTEST trial,15 which likely led to bias. The TEMPO-1 study,14 a prospective multicenter cohort study, showed that patients treated with 0.25 mg/kg TNK had a greater recanalization rate than those treated with 0.1 mg/kg TNK (52.17% vs 39.13%). TEMPO-114 enrolled patients with minor stroke (initial NIHSS score ≤5) owing to intracranial vessel occlusion and assessed the recanalization rate at 4–8 h from the administration of TNK, a timepoint earlier than those used in the TAAIS trial13 and ATTEST trial.15 Hence, the results from the TEMPO-1 study14 were more representative of patients with minor stroke. Although the ATTEST trial15 enrolled 104 patients, only 71 were included in the penumbra salvage analysis and 67 in the recanalization analysis, less than the sample size estimated to produce significant results on reperfusion and recanalization. A pooled analysis31 of the data from the TAAIS13 and the ATTEST15 trials showed that the recanalization rate of patients treated with TNK is greater than that of patients treated with alteplase, including the rate of complete (71% vs 42%, P<0.001) and partial (80% vs 57%, P<0.001) recanalization, indicating the superiority of TNK over alteplase in recanalization rate.
The EXTEND-IA TNK trial17 showed that more patients in the 0.25 mg/kg TNK group achieved substantial reperfusion (ie, restoration of blood flow to >50% of the involved territory or an absence of retrievable thrombus in the target vessel at the time of the initial angiographic assessment) than those in the alteplase group before thrombectomy, within 4.5 h after the onset of ischemic stroke (22% vs 10%, P=0.002); this indicated the superiority of TNK to alteplase in reperfusion and recanalization rate in ischemic stroke. TNK has demonstrated its superiority over alteplase in terms of recanalization rate and reperfusion in previously conducted clinical trials.13,14,17 Other imaging endpoints including infarct core volume and salvage tissue volume may warrant further investigations in future trials.
The reperfusion/recanalization rates among the TAAIS,13 ATTEST,15 and EXTEND-IA TNK17 trials were measured at different time points, and the trials also had different inclusion criteria. The reperfusion and recanalization rates were measured at 24 h after treatment in the TAAIS trial.13 The percentage of penumbra salvage and recanalization were measured at 24–48 h post treatment in the ATTEST trial.15 In the EXTEND-IA TNK trial,17 the reperfusion and recanalization rates were measured at the initial angiography or 1–2 h post thrombolysis, earlier than the measurement time in the former two trials. The TAAIS trial enrolled patients with an NIHSS score≥4 and intracranial arterial occlusion in the anterior, middle, and posterior cerebral artery, within 6 h.13 The ATTEST trial enrolled all the patients within 4.5 h after the onset of ischemia.15 In the EXTEND-IA TNK trial, the patients were enrolled if they had cerebral vascular occlusion within 4.5 h after the onset of stroke and were eligible for mechanical thrombectomy within 6 h.17 Different time points of reperfusion/recanalization rates and number of enrolled patients may have led to bias in the results of the three trials.13,15,17
Early Neurological Improvement
While only the TAAIS trial13 defined a reduction of the NIHSS score as the primary endpoint, early neurological improvement is still considered an index to assess the efficacy of TNK. The TAAIS trial13 showed that patients in the TNK group had a greater reduction of NIHSS score than patients in the alteplase group, 24 h after thrombolysis (median NIHSS reduction: 8 vs 5, P<0.001), and the percentage of NIHSS score reduction ≥8 was higher in the TNK group than the alteplase group (64% vs 36%, P=0.02). The TAAIS trial13 was the first to identify a statistically significant difference between TNK and alteplase with respect to early neurological improvement in patients with thrombolysis. The ATTEST trial15 showed non-significantly greater NIHSS score reduction in the TNK group than the alteplase group at 24 h (3 vs 2, P=0.74). The ATTEST trial15 had a similar baseline NIHSS score as the TAAIS trial, but the difference of NIHSS score at 24 h between the TNK group and alteplase group was not significant. The underlying reason may be that all enrolled patients in the TAAIS trial had proven reversible ischemic penumbra on CTP, and after recanalization of the occluded vessels, the blood supply recovered in the ischemic penumbra and neurological function improved, thereby manifesting as a greater NIHSS score reduction. The NOR-TEST trial (0.4 mg/kg TNK)16 and EXTEND-IA TNK trial (0.25 mg/kg)17 showed similar results for early neurological improvement between TNK and alteplase (NOR-TEST: 42% vs 39%, P=0.97; EXTEND-IA TNK: 71% vs 68%, P=0.70). To date, accomplished trials have failed to demonstrate whether TNK is superior to alteplase with respect to early neurological improvement.
Neurological Functional Outcome at 90 Days
The NOR-TEST trial16 is the only phase III trial among the TNK trials in ischemic stroke to investigate the efficacy of TNK in 90-day clinical outcomes, with mRS 0–1 defined as the primary endpoint. However, the NOR-TEST trial showed similar rates of mRS 0–1 at 90 days between the TNK and alteplase groups. Insufficient sample size in per-protocol analysis, lower baseline NIHSS score among the enrolled patients, and high rates of stroke mimics were likely hindrances in proving the difference between the TNK and alteplase groups on mRS score at 90 days. The TAAIS13 trial is the only clinical trial to demonstrate that patients treated with TNK had superior 90-d neurological functional outcomes than patients treated with alteplase (mRS 0–1: 72% vs 44%, P=0.02). The ATTEST trial15 showed a non-significantly higher percentage of mRS score 0–1 at 90 d in the TNK group than the alteplase group (28% vs 20%, P=0.28). A larger baseline infarction core volume was found in the TNK group compared with the alteplase group (TNK 32 mL vs alteplase 24 mL), and the final infarction core volume was larger in the TNK group than the alteplase group (total infarct volume at 24–48 h: 75 mL vs 66 mL, P=0.75), implying that patients in the TNK group had greater severity than those in the alteplase group. The EXTEND-IA TNK trial17 showed a non-significantly higher percentage of mRS score 0–1 in the TNK group (51% vs 43%, P=0.23), and the median mRS score at 90 d was also lower in the TNK group (2 vs 3, P=0.004) than the alteplase group, indicating that compared to alteplase, TNK could improve the functional outcomes in bridge therapy (IVT+MT). A pooled analysis18 of the EXTEND-IA TNK17 and EXTEND-IA TNK-218 trials (401 patients who received TNK vs 101 patients who received alteplase) showed the functional outcome difference favored TNK with a significant improvement in ordinal analysis of the mRS score (adjusted common odds ratio: 1.50, 95% CI: 1.01–2.22; P=0.04). Because TNK only proved superior in terms of the 90-day functional outcomes in some of the trials, the performance of functional outcomes of TNK and alteplase is still and it is still a debate.
Risk of Intracranial Hemorrhage
TNK has better fibrin selectivity and is less harmful to the coagulation process and blood-brain barrier than alteplase, thereby theoretically implying a lower risk of intracranial hemorrhage.27 The TAAIS13 and ATTEST15 trials showed that patients treated with TNK had similar risks of sICH (TAAIS: 4% vs 12%, P=0.33; ATTEST: 6% vs 8%, P=0.59) and parenchymal hematoma (TAAIS: 6% vs 20%, P=0.11; ATTEST: 2% vs 10%, P=0.12) as those treated with alteplase. The EXTEND-IA TNK trial17 showed that TNK (0.25 mg/kg) and alteplase had the same risk for sICH (1% vs 1%, P=0.99) and similar risk for parenchymal hematoma (6% vs 5%, P=0.76) in the bridge therapy (IVT+MT). The occurrence of parenchymal hemorrhage type 2, the most severe type of intracranial hemorrhage after intravenous thrombolysis, was lower in the TNK group than the alteplase group (0% vs 6%), as observed in the ATTEST trial.15
Similar mortality at the 90-d follow-up was noted between the TNK and alteplase groups in some of the accomplished clinical trials (TAAIS: 8% vs 12%, P=0.68; ATTEST: 17% vs 12%, P=0.51; NOR-TEST: 5% vs 5%, P=0.68)13,15,16 and a meta-analysis (7.6% vs 8.1%).32 The EXTEND-IA TNK trial showed that TNK had comparable mortality with alteplase (15% vs 17%, P=0.35) in bridge therapy.17
CT Perfusion (CTP)/MR Mismatch Group
The TAAIS trial13 added CTP mismatch to its inclusion criteria and demonstrated the superiority of TNK over alteplase. A pooled analysis33 including data from the TAAIS13 and ATTEST15 trials showed that in patients fulfilling the target mismatch criteria, those treated with TNK had greater early neurological improvement (median NIHSS reduction: 6 vs 1, P<0.001); higher recanalization rates (90% vs 33%, P<0.001), greater 90-d functional outcome (mRS 0–1, OR: 2.33, 95% CI: 1.13–5.94, P=0.032); and lower risk of parenchymal hematoma (0% vs 21%, P=0.003) and sICH (0% vs 12%, P=0.04) than patients treated with alteplase. Patients fulfilling the target mismatch criteria were more likely to have an excellent functional outcome after thrombolysis with TNK than those who failed to fulfill the target mismatch criteria (mRS 0–1, OR: 2.33 vs 1.26, P=0.044). Another pooled analysis34 that enrolled data from the TAAIS13 and ATTEST15 compared the influence of DWI (diffusion weighted imaging)-NIHSS mismatch and CTP mismatch on 90d functional outcome. Patients fulfilling CTP mismatch were more likely to have excellent functional outcomes than those fulfilling the DWI-NIHSS mismatch (90-d mRS 0–1 OR: 2.33 vs 2.15). However, patients fulfilling either DWI-NIHSS mismatch or CTP mismatch were likely to have greater early neurological improvement (median NIHSS reduction: 7 vs 2, P=0.037), higher recanalization rate (41% vs 19%, P<0.001), and lower risk of parenchymal hematoma (7% vs 13%, P=0.044) than patients who fulfilled neither of the two target mismatch criteria.
A subgroup analysis35 of the NOR-TEST trial16 showed that among patients with DWI-fluid attenuated inversion recovery (FLAIR) mismatch, those in the 0.4 mg/kg TNK group had greater early neurological improvement than patients in the alteplase group (NIHSS reduction≥4: 87.5% vs 54.2%, P=0.027). However, selection bias cannot be neglected for the small sample size and low baseline NIHSS score in this subgroup study.
Taken together, the performance of TNK is superior to alteplase in patients fulfilling target mismatch criteria. Moreover, fulfilling the target mismatch criteria indicated salvable ischemic penumbra and a greater collateral status around the infarction core. Abundant collateral circulation and higher recanalization rate owing to intravenous TNK can save the reversible penumbra around the infarction core and improve functional outcome. However, the evidence favoring TNK in patients fulfilling target mismatch criteria was mainly generated from post-hoc analysis or subgroup analysis, except in the TAAIS trial.13 Phase III randomized controlled trials are awaited to produce results that are more robust to demonstrate the superiority of TNK over alteplase in patients fulfilling the target mismatch criteria.
Minor Stroke/Stroke Mimics Group
The TEMPO-1 study14 enrolled patients with minor stroke (NIHSS≤5), wherein 76% of patients in the 0.25 mg/kg TNK group had excellent functional outcome (90-d mRS score 0–1). A post-hoc analysis that enrolled patients with NIHSS≤5 in the NOR-TEST trial16 compared the functional outcome of patients in the TNK group and alteplase group. Those in the TNK group had similar functional outcomes as the alteplase group (52.8% vs 57.1%, P=0.57). The difference was non-significant between TNK and alteplase after excluding the data of patients with stroke mimics (57.1% vs 60.6%, P=0.7). Therefore, further evidence on the efficacy of TNK in patients with minor stroke and future trials of TNK use in minor strokes is still warranted.
TEMPO-2 (A Randomized Controlled Trial of TNK-tPA vs Standard of Care for Minor Ischemic Stroke With Proven Occlusion, NCT02398656) is an ongoing phase III trial comparing 0.25 mg/kg TNK versus standard medical treatment in minor strokes (NIHSS≤5). Their results may provide more evidence of the efficacy of TNK in patients with a low NIHSS score.
Studies on the safety of TNK in patients with stroke mimics are limited. A study36 that performed subgroup analysis on 181 patients with stroke mimics (functional, 30%; migraine, 17%; seizure, 14%; without further specification, 13%; others, 26%) from the NOR-TEST trial16 showed that no patients had sICH after administration of TNK, indicating that TNK was safe in patients with stroke mimics.
Bridge Therapy with Mechanical Thrombectomy
The Direct Intra-arterial Thrombectomy in Order to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals: a Multicenter Randomized Clinical Trial (DIRECT-MT) demonstrated that primary MT was non-inferior compared to bridging MT (IVT+MT) in ischemic stroke caused by large vessel occlusion in the anterior circulation.37 However, the DIRECT-MT trial could not neglect the value of intravenous thrombolysis in bridging MT because the non-inferior margin was very broad (0.8).38 Direct endovascular treatment versus standard bridging therapy in large artery anterior circulation stroke (DEVT) trial39 again proved the non-inferiority of primary MT over bridging MT. The following trials comparing primary MT with bridging MT are ongoing: Netherlands-No-Intravenous tPA (ISRCTN80619088); DIRECT-SAFE (A Randomized Controlled Trial of DIRECT Endovascular Clot Retrieval vs Standard Bridging Thrombolysis With Endovascular Clot Retrieval Within 4.5 Hours of Stroke Onset) in Australia and China (NCT03494920); SWIFT DIRECT (Bridging Thrombolysis vs Direct Mechanical Thrombectomy in Acute Ischemic Stroke) in China (NCT03192332); TESLA (Thrombectomy for Emergent Salvage of Large Anterior Circulation Ischemic Stroke) in North America (NCT03805308). However, all the trials that compared primary MT with bridge MT used alteplase as the thrombolytic drug. Whether bridging MT with TNK is superior to direct MT is still unknown and requires further investigation. Endovascular Treatment With Versus Without Intravenous Tenecteplase in Stroke (BRIDGE-TNK, NCT04733742) is an ongoing phase III trial to compare TNK bridging MT versus primary MT in ischemic stroke caused by M1/M2 occlusion, and the results are awaited.
Discussion
To date, phase III trials with large sample size comparing TNK with alteplase are still lacking. In the accomplished trials with small sample size, TNK has been shown to be superiority to alteplase with respect to recanalization, but has similar risk of sICH in clinical studies of reperfusion therapy for ischemic stroke. TNK 0.25 mg/kg has the potential to be the optimal dose for intravenous thrombolysis and bridge therapy, and TNK may also be a promising alternative thrombolytic agent to alteplase in bridge therapy for ischemic stroke.
The number of clinical trials on TNK for ischemic stroke started to decrease. A meta-analysis32 comprising five randomized clinical trials10,13,15–17 demonstrated that TNK is non-inferior to alteplase. Heterogeneity was low (I2=0) for the efficacy and safety outcomes across the five studies,10,13,15–17 and the meta-analysis32 provided powerful evidence that TNK is non-inferior to alteplase in ischemic stroke. However, the mean NIHSS score across the included trials is 7, indicating that the non-inferiority of TNK proved in this meta-analysis32 may be more applicable in patients with low NIHSS score. Among the included studies in this meta-analysis,32 the NOR-TEST16 had the largest sample size (n>1000) and contributed to over 70% participants in the meta-analysis.32 Hence, the external generalization of the results from this meta-analysis32 may be weakened. Moreover, a generous boundary for non-inferiority margin was a major concern and decreased the generalization of non-inferiority of TNK in this meta-analysis.32 A non-inferiority margin of 5% may be more reasonable.40
At present, there are several on-going clinical trials on TNK in ischemic stroke (Table 3). Apart from the NOR-TEST trial,16 all the TNK clinical trials10–18,37 were phase II trials that focused on safety endpoints and dose comparison. Phase II trials have limited sample size as well as potential selection bias and cannot provide convincing evidence on efficacy endpoints. Phase III trials are required to demonstrate the superiority of TNK over alteplase in efficacy endpoints including functional outcomes. The PROBE (perspective, randomized, open-label, blinded outcome) study design is a limitation of all the TNK trials of ischemic stroke, except the phase IIB trial by Haley et al.12 Open-label drugs with blinded outcome assessment design are unable to eliminate information bias, and this defect in the study design may result in unconvincing conclusions. TIMELESS is a double-blinded trial of TNK in ischemic stroke among the on-going TNK trials and may provide results that are more powerful. Moreover, the phase III trial, NOR-TEST,16 failed to demonstrate the superiority of TNK over alteplase. A large percentage of stroke mimics/minor stroke cases may be one of the reasons. Another reason is the insufficient sample size based on the over-optimistic efficacy of TNK over alteplase (9%).16 The superiority of alteplase in terms of efficacy over placebo is only 10–13%, suggesting that a 9% superiority of TNK over alteplase is unrealistic.41 A large sample size is required to demonstrate the superiority of TNK over alteplase. Another method is to test the non-inferiority of TNK. Considering the single-bolus administration of TNK compared with alteplase, proving the non-inferiority of TNK enables it to be an alternative to alteplase in clinical practice. Besides, as alteplase has proven its safety and efficacy in patients with unknown onset time,42 clinical trials to investigate the efficacy and safety of TNK in an extended time window or unknown onset time are also required. The TAAIS trial13 included patients with ischemic penumbra on CTP and obtained robust results that favored TNK. The TIMELESS, TRACE III, CHABLIS-T II, and ETERNAL-LVO trials are designed to include patients with ischemic penumbra that will provide more evidence on TNK efficacy in imaging-selected patients with unknown onset time. Direct versus bridge MT in anterior circulation is also controversial. While the DIRECT-MT37 and DEVT39 trials demonstrated the non-inferiority of direct MT compared with bridge MT, the Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN-NO IV)43 and Direct Mechanical Thrombectomy in Acute LVO Stroke (SKIP)44 trials did not. All the completed clinical trials comparing direct MT and bridge MT used alteplase. Considering the outstanding recanalization rate in EXTEND-IA TNK,17 bridge MT with TNK versus direct MT may offer new evidence for this issue. A mobile stroke unit is a new intervention and transportation method that showed improved functional clinical outcomes in patients treated with IV tPA.45,46 The efficacy of a mobile stroke unit combined with TNK therapy warrant further investigation.
 | 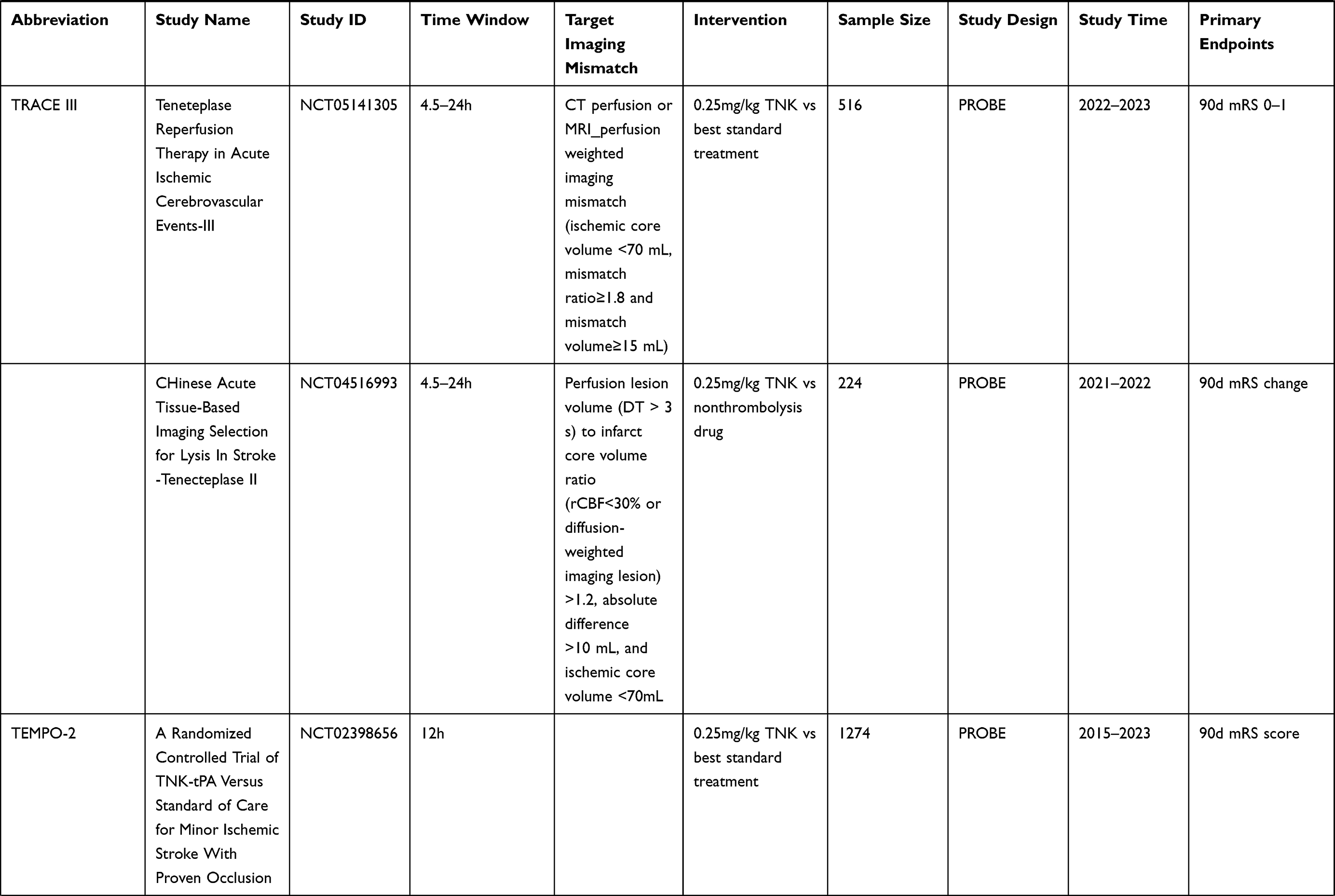 |  |
Table 3 Ongoing Trials of TNK in Ischemic Strokes |
Safety endpoints in the completed trials11,13–18,37 were common adverse events including intracranial hemorrhage of all types and mortality. Considering the degradation of the BBB, cerebral edema is another side effect for intravenous thrombolysis for ischemic stroke.26 Additional safety endpoints (eg, systematic bleeding events, cerebral infarction in a new vascular territory, and vessel re-occlusion) also need further investigation in future trials.
All the completed trials13–18 were conducted in high-income regions (North America, Europe, and Australia) and the patients enrolled were mainly of Caucasian ethnicity. Results of clinical trials in low-income regions and with east-Asian/African patients are still lacking.
Despite the limitations in study design of the aforementioned trials, they have paved the way for future trials on reperfusion therapy for ischemic stroke. Hence, subsequent trials can test the efficacy of TNK in minor stroke or bridge thrombectomy.
Studies in the real world are also crucial for the generalization of TNK. An observational study enrolled 555 patients treated with alteplase and 283 patients treated with TNK in New Zealand. Patients treated with TNK had functional clinical outcomes that were more favorable at 3 months and the median door-to-needle time was reduced by 8 min.45 Zhong et al conducted another retrospective study including 165 patients treated with TNK and 254 patients treated with alteplase across three stroke centers.48 Patients treated with TNK had a non-significantly higher proportion of 90-d functional independence and a non-significantly lower risk of sICH than patients treated with alteplase. Different proportions of large vessel occlusion and endovascular treatment may confound the treatment effects in these two real-world studies.47,48 In patients with large vessel occlusion, the TNK group showed a higher proportion of 90-d functional independence without increasing sICH risk,49 consistent with the results from the EXTEND-IA TNK.17 Real-world studies will provide information for the safety and effectiveness of TNK in ischemic stroke. However, the limitations associated with study design and potential confounders are inevitable.
During the coronavirus disease 2019 (COVID-19) pandemic, tenecteplase likely played a greater role in intravenous thrombolysis than alteplase. During the pandemic, additional sterilization measures and donning of personal protective equipment delayed the administration of intravenous thrombolytic therapy.50,51 Some neurologists were also transferred to designated COVID wards, resulting in shortage of neurovascular emergency personnel. Moreover, intravenous thrombolysis with alteplase is given as a bolus and continuous infusion for over 1 h, and neurologists tend to visit the patients several times during alteplase infusion. Multiple physician visits can lead to additional risk of exposure to stroke patients unknown of their results of nasopharyngeal swab for COVID-19. However, considering that TNK is administered as a single intravenous bolus, it could reduce the duration and frequency of intervention during intravenous thrombolysis and decrease the risk of in-hospital COVID-19 transmission in neurovascular emergency rooms.52
Conclusion
Tenecteplase is a potential alternative to alteplase in thrombolytic therapy for ischemic stroke. Future clinical trials with TNK that target the functional outcomes are warranted.
Funding
This work was supported by grants from Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (2019-I2M-5-029), Beijing Municipal Committee of Science and Technology (Z201100005620010), and Beijing Natural Science Foundation (Z200016).
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204-1222.
2. Benjamin EJ, Virani SS, Callaway CW, et al. Heart disease and stroke statistics-2018 update: a report from the American Heart Association. Circulation. 2018;137:e67–e492. doi:10.1161/CIR.0000000000000558
3. Powers WJ, Rabinstein AA, Ackerson T, et al. 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018;49:e46–e110. doi:10.1161/STR.0000000000000158
4. National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333(24):1581–1587. doi:10.1056/NEJM199512143332401
5. Boysen G; ECASS Study Group. European Cooperative Acute Stroke Study (ECASS): (rt-PA-Thrombolysis in acute stroke) study design and progress report. Eur J Neurol. 1995;1(3):213–219. doi:10.1111/j.1468-1331.1995.tb00074.x
6. Thomalla G, Simonsen CZ, Boutitie F, et al. MRI-Guided thrombolysis for stroke with unknown time of onset. N Engl J Med. 2018;379:611–622. doi:10.1056/NEJMoa1804355
7. Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359(13):1317–1329. doi:10.1056/NEJMoa0804656
8. Ma H, Campbell BCV, Parsons MW, et al. Thrombolysis guided by perfusion imaging up to 9 hours after onset of stroke. New Engl J Med. 2019;380:1795–1803. doi:10.1056/NEJMoa1813046
9. Van de Werf F. Single-bolus tenecteplase compared with front-loaded alteplase in acute myocardial infarction: the ASSENT-2 double-blind randomised trial. Lancet. 1999;354:716–722. doi:10.1016/S0140-6736(99)07403-6
10. Haley EC, Lyden PD, Johnston KC, Hemmen TM. A pilot dose-escalation safety study of tenecteplase in acute ischemic stroke. Stroke. 2005;36:607–612. doi:10.1161/01.STR.0000154872.73240.e9
11. Parsons MW, Miteff F, Bateman GA, et al. Acute ischemic stroke: imaging-guided tenecteplase treatment in an extended time window. Neurology. 2009;72(10):915–921. doi:10.1212/01.wnl.0000344168.05315.9d
12. Haley EC
13. Parsons M, Spratt N, Bivard A, et al. A randomized trial of tenecteplase versus alteplase for acute ischemic stroke. N Engl J Med. 2012;366(12):1099–1107. doi:10.1056/NEJMoa1109842
14. Coutts SB, Dubuc V, Mandzia J, et al. Tenecteplase-tissue-type plasminogen activator evaluation for minor ischemic stroke with proven occlusion. Stroke. 2015;46:769–774. doi:10.1161/STROKEAHA.114.008504
15. Huang X, Cheripelli BK, Lloyd SM, et al. Alteplase versus tenecteplase for thrombolysis after ischaemic stroke (ATTEST): a Phase 2, randomised, open-label, blinded endpoint study. Lancet Neurol. 2015;14:368–376. doi:10.1016/S1474-4422(15)70017-7
16. Logallo N, Novotny V, Assmus J, et al. Tenecteplase versus alteplase for management of acute ischaemic stroke (NOR-TEST): a Phase 3, randomised, open-label, blinded endpoint trial. Lancet Neurol. 2017;16:781–788. doi:10.1016/S1474-4422(17)30253-3
17. Campbell BCV, Mitchell PJ, Churilov L, et al. Tenecteplase versus Alteplase before Thrombectomy for Ischemic Stroke. N Engl J Med. 2018;378:1573–1582. doi:10.1056/NEJMoa1716405
18. Campbell BCV, Mitchell PJ, Churilov L, et al. Effect of intravenous tenecteplase dose on cerebral reperfusion before thrombectomy in patients with large vessel occlusion ischemic stroke: the EXTEND-IA TNK Part 2 Randomized Clinical Trial. JAMA. 2020;323:1257–1265. doi:10.1001/jama.2020.1511
19. Logallo N, Kvistad CE, Nacu A, et al. The Norwegian tenecteplase stroke trial (NOR-TEST): randomised controlled trial of tenecteplase vs. alteplase in acute ischaemic stroke. BMC Neurol. 2014;14:106. doi:10.1186/1471-2377-14-106
20. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50:e344–e418. doi:10.1161/STR.0000000000000211
21. Berge E, Whiteley W, Audebert H, et al. European Stroke Organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Euro Stroke J. 2021;6:I–LXII. doi:10.1177/2396987321989865
22. Kotb E. The biotechnological potential of fibrinolytic enzymes in the dissolution of endogenous blood thrombi. Biotechnol Prog. 2014;30:656–672. doi:10.1002/btpr.1918
23. Bivard A, Lin L, Parsonsb MW. Review of stroke thrombolytics. J Stroke. 2013;15:90–98. doi:10.5853/jos.2013.15.2.90
24. Chester KW, Corrigan M, Schoeffler JM, et al. Making a case for the right “-ase” in acute ischemic stroke: alteplase, tenecteplase, and reteplase. Expert Opin Drug Saf. 2019;18:87–96. doi:10.1080/14740338.2019.1573985
25. Logallo N, Kvistad CE, Nacu A, Thomassen L. Novel thrombolytics for acute ischemic stroke: challenges and opportunities. CNS Drugs. 2016;30:101–108. doi:10.1007/s40263-015-0307-2
26. Marshall RS. Progress in intravenous thrombolytic therapy for acute stroke. JAMA Neurol. 2015;72:928–934. doi:10.1001/jamaneurol.2015.0835
27. Huang X, Moreton FC, Kalladka D, et al. Coagulation and fibrinolytic activity of tenecteplase and alteplase in acute ischemic stroke. Stroke. 2015;46:3543–3546. doi:10.1161/STROKEAHA.115.011290
28. Gurbel PA, Hayes K, Bliden KP, Yoho J, Tantry US. The platelet-related effects of tenecteplase versus alteplase versus reteplase. Blood Coagul Fibrinolysis. 2005;16(1):1–7. doi:10.1097/00001721-200501000-00001
29. Tsikouris JP, Ii KC, Fike DS, Cox CD, Meyerrose GE, Seifert CF. Thrombolytic fibrin specificity influences activated partial thromboplastin time prolongation in vitro. Blood Coagul Fibrinolysis. 2002;13(8):725–731. doi:10.1097/00001721-200212000-00009
30. Kheiri B, Osman M, Abdalla A, et al. Tenecteplase versus alteplase for management of acute ischemic stroke: a pairwise and network meta-analysis of randomized clinical trials. J Thromb Thrombolysis. 2018;46:440–450. doi:10.1007/s11239-018-1721-3
31. Bivard A, Huang X, Levi CR, et al. Tenecteplase in ischemic stroke offers improved recanalization: analysis of 2 trials. Neurology. 2017;89(1):62–67. doi:10.1212/WNL.0000000000004062
32. Burgos AM, Saver JL. Evidence that tenecteplase is noninferior to alteplase for acute ischemic stroke: meta-analysis of 5 randomized trials. Stroke. 2019;50:2156–2162. doi:10.1161/STROKEAHA.119.025080
33. Bivard A, Huang X, McElduff P, et al. Impact of computed tomography perfusion imaging on the response to tenecteplase in ischemic stroke: analysis of 2 randomized controlled trials. Circulation. 2017;135(5):440–448. doi:10.1161/CIRCULATIONAHA.116.022582
34. Bivard A, Huang X, Levi CR, et al. Comparing mismatch strategies for patients being considered for ischemic stroke tenecteplase trials. Int J Stroke. 2020;15:507–515. doi:10.1177/1747493019884529
35. Ahmed HK, Logallo N, Thomassen L, Novotny V, Mathisen SM, Kurz MW. Clinical outcomes and safety profile of Tenecteplase in wake-up stroke. Acta Neurol Scand. 2020;142:475–479. doi:10.1111/ane.13296
36. Kvistad CE, Novotny V, Naess H, et al. Safety and predictors of stroke mimics in The Norwegian Tenecteplase Stroke Trial (NOR-TEST). Int J Stroke. 2019;14:508–516. doi:10.1177/1747493018790015
37. Yang P, Zhang Y, Zhang L, et al. Endovascular thrombectomy with or without intravenous alteplase in acute stroke. N Engl J Med. 2020;382:1981–1993. doi:10.1056/NEJMoa2001123
38. Nogueira RG, Tsivgoulis G. Large vessel occlusion strokes after the DIRECT-MT and SKIP trials: is the alteplase syringe half empty or half full? Stroke. 2020;51:3182–3186. doi:10.1161/STROKEAHA.120.030796
39. Zi W, Qiu Z, Li F, et al. Effect of endovascular treatment alone vs intravenous alteplase plus endovascular treatment on functional independence in patients with acute ischemic stroke: the DEVT Randomized Clinical Trial. JAMA. 2021;325:234–243. doi:10.1001/jama.2020.23523
40. Lin CJ, Saver JL. Noninferiority margins in trials of thrombectomy devices for acute ischemic stroke: is the bar being set too low? Stroke. 2019;50:3519–3526. doi:10.1161/STROKEAHA.119.026717
41. Wahlgren N, Ahmed N, Dávalos A, et al. Thrombolysis with alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST): an observational study. Lancet. 2007;369:275–282. doi:10.1016/S0140-6736(07)60149-4
42. Thomalla G, Boutitie F, Ma H, et al. Intravenous alteplase for stroke with unknown time of onset guided by advanced imaging: systematic review and meta-analysis of individual patient data. Lancet. 2020;396:1574–1584.
43. LeCouffe NE, Kappelhof M, Treurniet KM, et al. A randomized trial of intravenous alteplase before endovascular treatment for stroke. N Engl J Med. 2021;385:1833–1844. doi:10.1056/NEJMoa2107727
44. Suzuki K, Matsumaru Y, Takeuchi M, et al. Effect of mechanical thrombectomy without vs with intravenous thrombolysis on functional outcome among patients with acute ischemic stroke: the SKIP Randomized Clinical Trial. JAMA. 2021;325:244–253. doi:10.1001/jama.2020.23522
45. Ebinger M, Siegerink B, Kunz A, et al. Association Between Dispatch of Mobile Stroke Units and Functional Outcomes Among Patients With Acute Ischemic Stroke in Berlin. JAMA. 2021;325(5):454-466. doi:10.1001/jama.2020.26345
46. Grotta JC, Yamal JM, Parker SA, et al. Prospective, Multicenter, Controlled Trial of Mobile Stroke Units. N Engl J Med. 2021;385(11):971-981. doi:10.1056/NEJMoa2103879
47. Mahawish K, Gommans J, Kleinig T, Lallu B, Tyson A, Ranta A. Switching to tenecteplase for stroke thrombolysis: real-world experience and outcomes in a regional stroke network. Stroke. 2021;52:e590–e3. doi:10.1161/STROKEAHA.121.035931
48. Zhong CS, Beharry J, Salazar D, et al. Routine use of tenecteplase for thrombolysis in acute ischemic stroke. Stroke. 2021;52:1087–1090. doi:10.1161/STROKEAHA.120.030859
49. Gerschenfeld G, Smadja D, Turc G, et al. Functional outcome, recanalization, and hemorrhage rates after large vessel occlusion stroke treated with tenecteplase before thrombectomy. Neurology. 2021;97:e2173–e84. doi:10.1212/WNL.0000000000012915
50. Siegler JE, Zha AM, Czap AL, et al. Influence of the COVID-19 pandemic on treatment times for acute ischemic stroke: the society of vascular and interventional neurology multicenter collaboration. Stroke. 2021;52:40–47. doi:10.1161/STROKEAHA.120.032789
51. Zhou Y, Hong C, Chang J, et al. Intravenous thrombolysis for acute ischaemic stroke during COVID-19 pandemic in Wuhan, China: a multicentre, retrospective cohort study. J Neurol Neurosurg Psychiatry. 2021;92(2):226–228. doi:10.1136/jnnp-2020-324014
52. Warach SJ, Saver JL, LeCouffe NE. Stroke thrombolysis with tenecteplase to reduce emergency department spread of coronavirus disease 2019 and shortages of alteplase. JAMA Neurol. 2020;77:1203–1204. doi:10.1001/jamaneurol.2020.2396
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.