")
Back to Journals » Clinical Epidemiology » Volume 15
Temporal Trends of Inflammatory Bowel Disease Burden in China from 1990 to 2030 with Comparisons to Japan, South Korea, the European Union, the United States of America, and the World
Authors Ma T, Wan M, Liu G, Zuo X, Yang X , Yang X
Received 12 January 2023
Accepted for publication 22 April 2023
Published 8 May 2023 Volume 2023:15 Pages 583—599
DOI https://doi.org/10.2147/CLEP.S402718
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Vera Ehrenstein
Tian Ma,1– 3 Meng Wan,1– 3 Guanqun Liu,1– 3 Xiuli Zuo,1– 3 Xiaorong Yang,1– 4 Xiaoyun Yang1– 4
1Department of Gastroenterology, Qilu Hospital of Shandong University, Jinan, People’s Republic of China; 2Laboratory of Translational Gastroenterology, Qilu Hospital of Shandong University, Jinan, People’s Republic of China; 3Shandong Provincial Clinical Research Center for Digestive Disease, Qilu Hospital of Shandong University, Jinan, People’s Republic of China; 4Clinical Epidemiology Unit, Qilu Hospital of Shandong University, Jinan, People’s Republic of China
Correspondence: Xiaorong Yang, Clinical Epidemiology Unit, Qilu Hospital of Shandong University, 107 Wenhuaxi Road, Jinan, 250012, People’s Republic of China, Tel +86-531-82166951, Fax +86-531-86927544, Email [email protected] Xiaoyun Yang, Department of Gastroenterology, Laboratory of Translational Gastroenterology, Qilu Hospital of Shandong University, 107 Wenhuaxi Road, Jinan, Shandong, 250012, People’s Republic of China, Tel +86-531-82169034, Fax +86-531-86927544, Email [email protected]
Purpose: To identify and predict the epidemiological burden and trends of inflammatory bowel disease (IBD) in China and compare them globally.
Methods: We collected incidence, prevalence, deaths, years of life lost (YLLs), years lived with disability (YLDs), disability-adjusted life-years (DALYs), and the age-standardized rates (ASRs) of IBD from 1990 to 2019 in China, four developed countries and the world, from the Global Burden of Disease Study 2019. The average annual percentage change (AAPC) was calculated to evaluate the temporal trends.
Results: From 1990 to 2019, the numbers of incident and prevalent cases, age-standardized incidence rate (ASIR), and age-standardized prevalence rate (ASPR) of IBD increased in China, regardless of gender and age; decreased YLLs and increased YLDs caused a stable number of DALYs; the age-standardized mortality rate (ASMR) and age-standardized DALY rate (ASDR) decreased. In 2019, the ASIR, ASPR, ASMR, and ASDR were 3.01/100,000 person-years (/100,000) (95% UI: 2.59, 3.50), 47.06/100,000 (95% UI: 40.05, 54.99), 0.30/100,000 (95% UI: 0.24, 0.35), and 13.1/100,000 (95% UI: 10.29, 16.31), respectively; almost all disease burden data were higher in males. In 2017, the ASDR in different socio-demographic index provinces ranged from 24.62/100,000 (95% UI: 16.95, 33.81) to 63.97/100,000 (95% UI: 44.61, 91.48). When compared globally, the ASIR and ASPR in China had opposite trends and the highest AAPCs. In 2019, the ASIR and ASPR in China were in the middle of the world and lower than in some developed countries. The numbers and ASRs of incidence, prevalence, and DALYs were expected to increase by 2030.
Conclusion: The IBD burden in China significantly increased from 1990 to 2019 and was expected to rise further by 2030. China had the world’s opposite and most dramatic trends in ASIR and ASPR from 1990 to 2019. Strategies should be adjusted to adapt to the significantly increased disease burden.
Keywords: inflammatory bowel disease, China, disease burden, temporal trend, projection
Introduction
Inflammatory bowel disease (IBD), which includes ulcerative colitis (UC) and Crohn’s disease (CD), is an incurable disease with a chronic relapsing course.1,2 This disease most commonly occurs in young and middle-aged adults.3,4 Despite recent advances in treatment, IBD still has a certain mortality rate and a high disability rate.5,6 Data from follow-up studies showed that most IBD patients had intestinal or extra-intestinal complications, such as strictures, perforations, fistulas, abscesses, and thrombosis, throughout the course of the disease.7–9 Life-time surgery rates are generally 50% for CD and 20–30% for UC.1,2 The risk of postoperative recurrence is also a big issue.10 The quality of life and productivity of IBD patients are severely affected.11,12 In addition, IBD patients need lifelong medication and repeated hospitalizations, which also add significant social and economic burdens.
IBD is increasingly becoming a global health burden.5,13 Although the causes are not very clear, the incidence of IBD is closely related to the national or regional economy, industrial development level, and people’s living habits.14 China is the world’s largest developing country and has experienced a great social and economic transformation over the past 30 years, from 1990 to 2019. In China, the epidemiology of IBD has also shifted. However, pertinent studies and data are scarce, which brings great difficulties to the prevention and treatment of the disease as well as the formulation of relevant medical policies.
Based on the Global Burden of Disease (GBD) 2019 Study,15 which provides extensive data on the clinical epidemiology of IBD from 1990 to 2019, we identified and projected the national disease burden of IBD in China. In this study, we comprehensively analyzed the incidence, mortality, prevalence, years of life lost (YLLs), years lived with disability (YLDs), disability-adjusted life-years (DALYs), and the age-standardized rates (ASRs) of IBD in China from 1990 to 2019. The temporal trends in relation to age and gender were also included. We additionally made projections of disease burden until 2030. In this study, for the first time, the subnational burden of IBD in China was investigated by geographic macro-regions and the socio-demographic index (SDI), which is a comprehensive indicator of the development status of a country or region.15,16 Moreover, we also first made comparisons of the disease burden of IBD among China, Japan, South Korea, the European Union, the United States of America (USA), and the world. This study could improve the understanding of the latest epidemiological burdens of IBD in China and help the government and relevant medical decision-making departments optimize the adapted control strategies.
Materials and Methods
Data Source
The exhaustive introduction of original data sources and processing methodology of the GBD 2019 Study have been found in previous studies,15,17 and here we described the methods pertaining to the estimation of IBD in short. In the GBD 2019 Study, IBD is considered to be a digestive disorder resulting from non-infectious inflammation of the colon and gastrointestinal tract, predominantly UC and CD, which usually were diagnosed through endoscopy, imaging studies, or biopsy in patients with appropriate clinical signs and symptoms. However, the separate data for UC and CD were not provided in the GBD 2019 database. The prevalence and incidence of IBD were searched in electronic databases using the following terms: ((“crohn disease” OR (“crohn” AND “disease”) OR “colitis, ulcerative” OR (“colitis” AND “ulcerative”)) OR (“ulcerative colitis” OR (“Inflammatory” AND “Bowl”) OR (“irritable bowel syndrome” OR (“irritable” AND “bowel” AND “syndrome”) AND (“diarrhoea” OR “diarrhea”)) AND “epidemiology”. In addition to the data from literature research, available administrative data and inpatient hospital data related to IBD were further extracted as the prevalence. Based on the stipulated GBD inclusion criteria, a total of 501 original data sources about IBD burden were finally used to assess the corresponding disease burden. Mortality caused by IBD was modeled using standard Cause-of-Death Ensemble models (CODEm) based on the death database, including vital registration system and verbal autopsy data. The data from the primary studies, hospital discharges, and claims data were used to estimate the non-fatal burden of IBD using a specific Bayesian meta-regression tool, namely DisMod MR 2.1, and controlling the consistency among the incidence, prevalence, YLLs, YLDs, and DALYs. The epidemiological data for IBD by age, gender, year, and country was fitted using DisMod MR 2.1. Detailed information on the statistical methods and codes of data analysis for the IBD burden could be retrieved from the following website: http://ghdx.healthdata.org/gbd-2019/code/nonfatal-6.
We collected data on incidence, mortality, prevalence, YLLs, YLDs, and DALYs of IBD in China, Japan, South Korea, the European Union, the USA, and the world, covering the period of 1990–2019 across all age groups from the GBD 2019 Study via the Global Health Data Exchange query tool (https://ghdx.healthdata.org/gbd-results-tool). The 95% uncertainty intervals (UIs) for all estimates in the GBD Study were calculated based on the 25th and 975th-ordered number of 1000 random draws of the posterior uncertainty distribution. For fully describing the subnational disparity of IBD burden in China, available data on a total of 34 province-level administrative units, including 22 provinces, five autonomous regions, four municipalities, Hong Kong Special Administrative Region (SAR), Macao SAR, and Taiwan were retrieved from a previous study, which covered the subnational DALYs and age-standardized DALY rate (ASDR) of IBD in 34 provinces of China in 2017.18 The SDI, expressed on a scale of 0 to 1, is a comprehensive indicator reflecting the level of healthy development by integrating per capita income, average education level, and fertility rate under 25.15,16,18
Statistical Analyses
To avoid the disparity of the age composition of the populations, the ASRs of different indicators for IBD burden were used to quantify the variation among historical periods, geographical regions, and genders. We computed the average annual percentage change (AAPC) to measure the overall temporal trend in ASRs of IBD burden based on the sequencing regression model, ln (ASR)= α + β* calendar year + ϵ, and the AAPC with its 95% confidence interval (CI) were derived from the following formula: 100 × (exp (β) − 1).19–22 Compared with the smooth spline model, generalized additive model, Nordpred model, Joinpoint model, and Poisson regression, the Bayesian age-period-cohort (BAPC) model has been demonstrated to have higher accuracy in predicting the burden of non-communicable chronic diseases, especially in non-longer projection years.21,23–25 In brief, as one of the age-period-cohort models, the BAPC model applied a log-linear Poisson model to integrate the multiplicative effects of age, period, and cohort: ηij = log(λij) = μ + αi + βj+γk. In the model, λij represents the number of cases, μ is the intercept, and αi,βj, and γk are age, period, and cohort effects, respectively. i (1 ≤ i ≤ I) represents age group at time j (1 ≤ j ≤ J); k represents cohort index, k = M (I − i) + j, which depends on age, period index, and the length of age group and period interval. M indicates that the age group intervals are M times than the periodic intervals. In our study, 5-year age groups and annual data were analyzed, which meant that M was 5. Our study uses the BAPC model to project the burden of IBD in China from 2020 to 2030 within the integrated nested Laplacian approximation (R packages BAPC and INLA), assuming the inverse gamma prior distribution of age, period, and cohort effects and applying second-order random walk (RW2) to adjust for excessive dispersion. The relationship between the ASDR of IBD and the SDI of 34 provinces of China was conducted using Spearman correlation analysis. The main statistical analyses and graphing in the current study were performed using the R program version 4.0.3 (https://www.R-project.org/). Two-sided P value less than 0.05 was considered statistically significant.
Results
The National Disease Burden of IBD in 2019
In 2019, the number of incident cases and age-standardized incidence rate (ASIR) of IBD were 51.46 thousand (95% UI: 43.93, 60.47) and 3.01/100,000 person-years (/100,000) (95% UI: 2.59, 3.50) among the total Chinese population, respectively (Table 1). Overall, IBD caused 4.68 thousand (95% UI: 3.77, 5.46) deaths in China, and the age-standardized mortality rate (ASMR) was 0.30/100,000 (95% UI: 0.24, 0.35) (Table 1). Table 1 also shows that the number of prevalent cases was 911.05 thousand (95% UI: 776.35, 1069.53), while the age-standardized prevalence rate (ASPR) was 47.06/100,000 (95% UI: 40.05, 54.99). In 2019, the numbers of YLLs, YLDs, and DALYs of IBD in China were 96.56 thousand (95% UI: 75.92, 112.8), 135.91 thousand (95% UI: 89.07, 191.53), and 232.46 thousand (95% UI: 179.9, 291.09), respectively (Table 1). Meanwhile, the ASRs of YLL, YLD, and DALY were 6.02/100,000 (95% UI: 4.78, 6.95), 7.07/100,000 (95% UI: 4.65, 9.86), and 13.1/100,000 (95% UI: 10.29, 16.31) (Table 1).
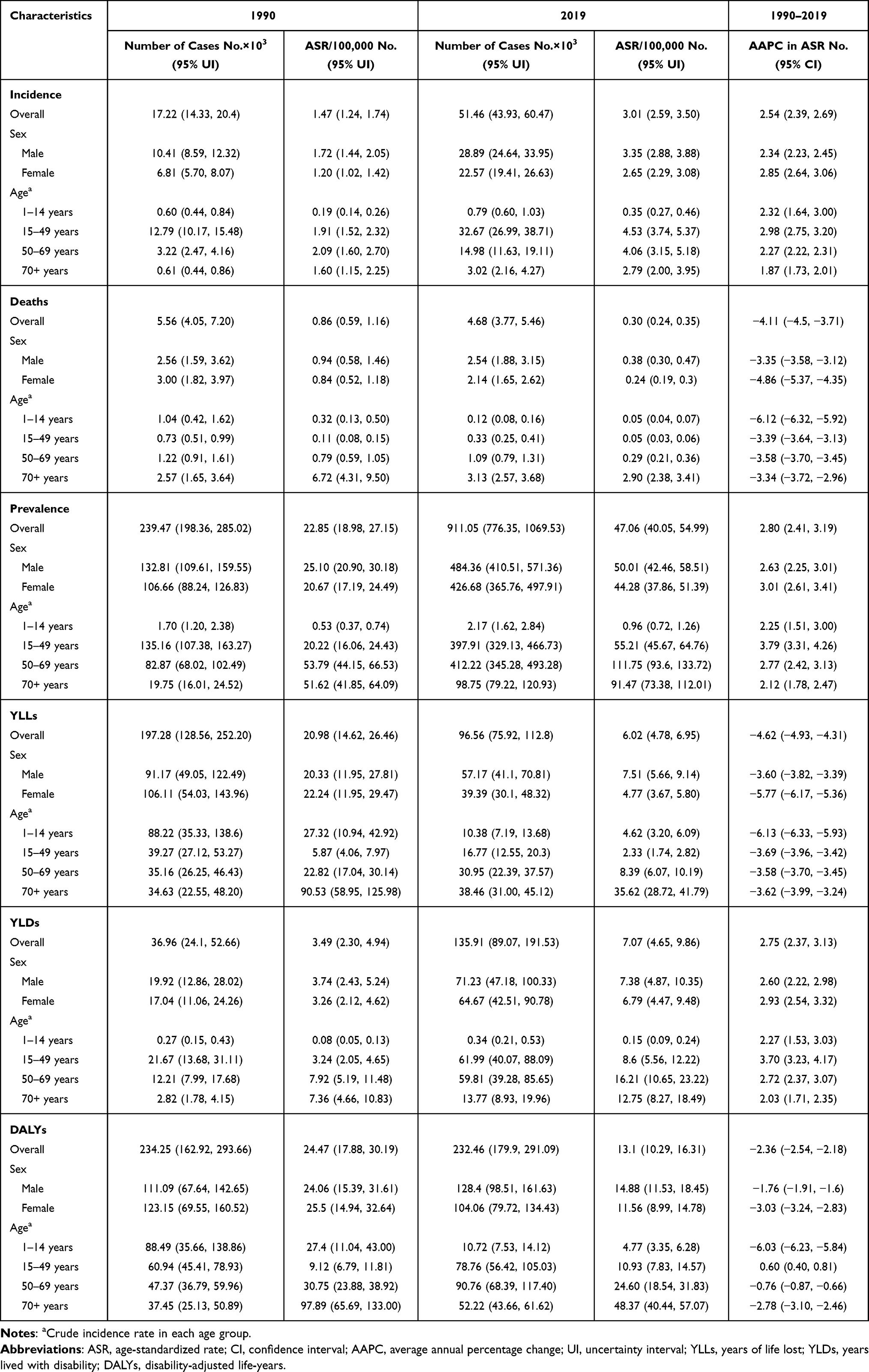 |
Table 1 The Numbers and Age-Standardized Rates of Incidence, Deaths, Prevalence, YLLs, YLDs, and DALYs of IBD in China in 1990 and 2019, and the AAPCs from 1990 to 2019 |
Temporal Trends of IBD in China from 1990 to 2019
The number of incident cases of IBD in China increased twice from 1990 [17.22 thousand (95% UI: 14.33, 20.4)] to 2019, and the ASIR also showed a growth tendency, with an AAPC of 2.54 (95% CI: 2.39, 2.69) (Table 1, Figure 1A). From 1990 to 2019, there was an overall decline in the number of deaths, but with some fluctuations (Table 1, Figure 1B). The highest number of deaths was recorded in 2004 (Figure 1B). The ASMR decreased as well, with an AAPC of −4.11 (95% CI: −4.5, −3.71) in the total population (Table 1). The number of prevalent cases almost quadrupled from 1990 [239.47 thousand (95% UI: 198.36, 285.02)] to 2019 (Table 1, Figure 1C). The ASPR also increased in 2019 when compared with 1990 [22.85/100,000 (95% UI: 18.98, 27.15)], with an AAPC of 2.80 (95% CI: 2.41, 3.19) (Table 1).
 |
Figure 1 The numbers and age-standardized rates of incidence (A), deaths (B), prevalence (C), DALYs (D), YLLs (E), and YLDs (E) of IBD in China from 1990 to 2019. Abbreviations: YLLs, years of life lost; YLDs, years lived with disability; DALYs, disability-adjusted life-years. Notes: Column chart: number; line chart: age-standardized rate; Shading: the upper and lower limits of the 95% uncertainty intervals. |
In these 30 years, IBD caused roughly the same number of DALYs in China (Table 1, Figure 1D). Nevertheless, the ASDR showed a downward trend from 1990 [24.47/100,000 (95% UI: 17.88, 30.19)] to 2019, with an AAPC of 2.36 (95% CI: −2.54, −2.18) (Table 1). In 2019, the number of YLLs of IBD in the Chinese population decreased significantly when compared to 1990, while the number of YLDs increased (Table 1, Figure 1E). The ASRs of YLL and YLD also showed opposite trends, with the AAPCs of −4.62 (95% CI: −4.93, −4.31) and 2.75 (95% CI: 2.37, 3.13), respectively.
The Changes of IBD Burden in Relation to Age and Gender from 1990 to 2019 in China
In China, the number of incident cases and ASIR of IBD increased in 2019 across all age groups and genders compared to 1990 (Table 1, Figure 2A and B). Similar to the condition in 1990, males overall had more incident cases than females in 2019 [28.89 thousand (95% UI: 24.64, 33.95) vs 22.57 thousand (95% UI: 19.41, 26.63)] (Table 1). When age was taken into account, females over the age of 85 had more incident cases than males in 2019 (Figure 3A). However, the incidence rate was higher in males than in females in almost all age groups (Figure 3A). It was found that young and middle-aged people were more likely to develop IBD in China. For both males and females, the age groups with the highest number of incident cases and incidence rate in 2019 were 30–34 years and 35–39 years, respectively (Figure 3A). From 1990 to 2019, the incidence rate doubled in the population aged 20–59 (Figure 2B). In addition, the AAPC in incidence rate was highest in the population aged 15–49 (Table 1, Figure 2A).
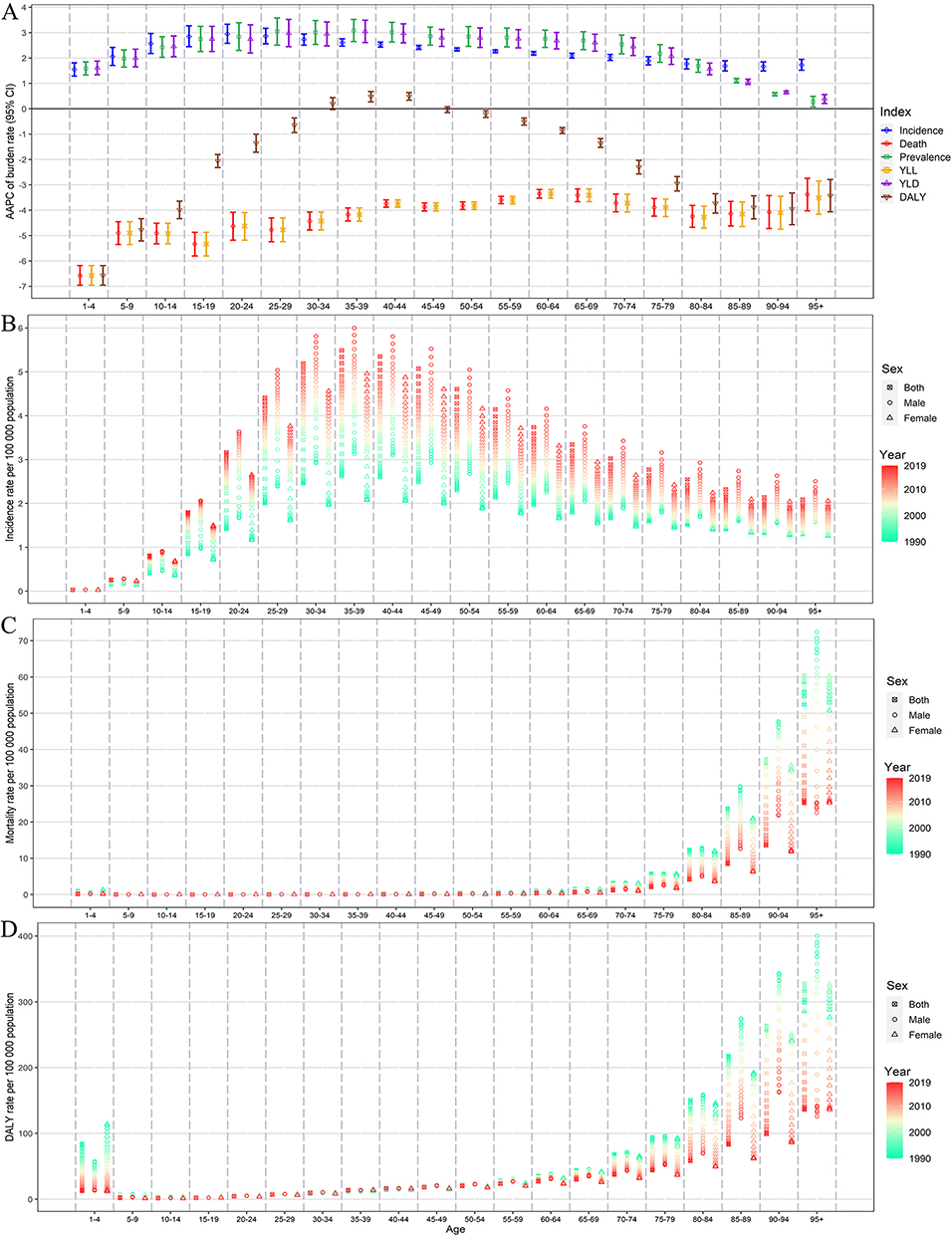 |
Figure 2 The AAPC of burden rate of IBD by age and indicators related to disease burden in China from 1990 to 2019 (A). The gradual incidence rate (B), mortality rate (C), and DALY rate (D) of IBD by age and gender in China from 1990 to 2019. The gradual change in color from green to red reflects the annual trend of the burden rate of IBD in each age group and gender from 1990 to 2019. Abbreviations: CI, confidence interval; AAPC, average annual percentage change; DALYs, disability-adjusted life-years. |
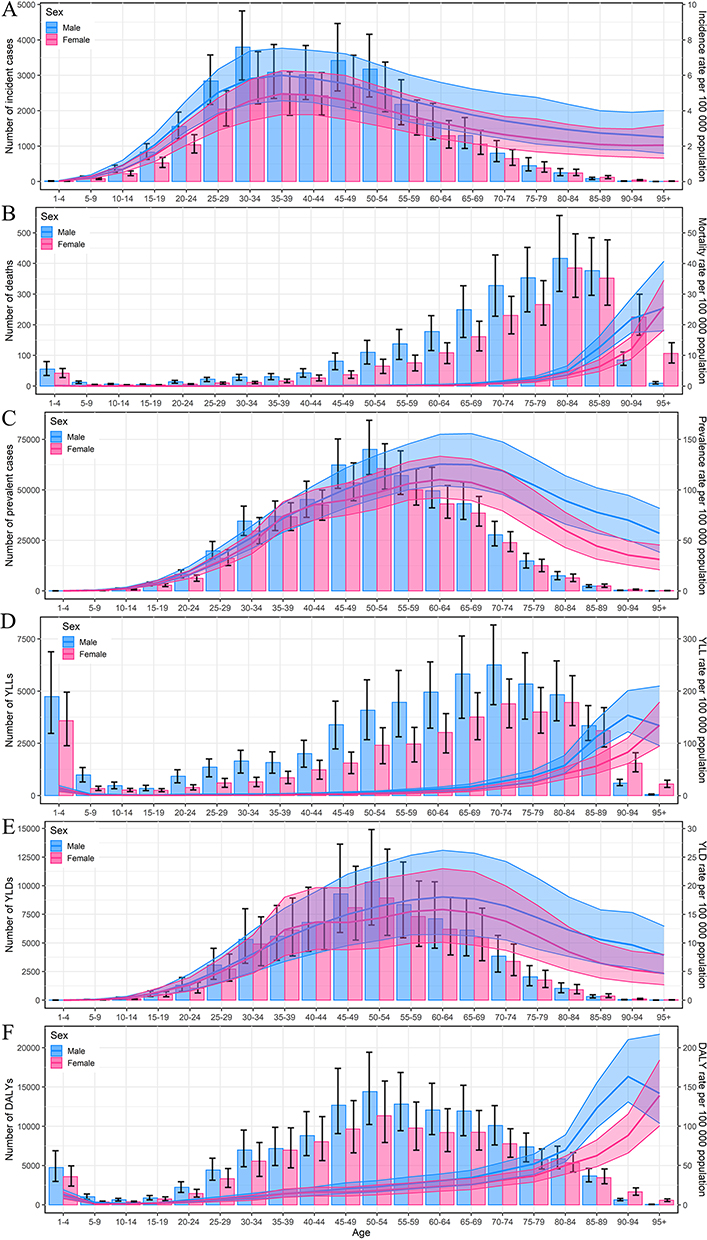 |
Figure 3 The national numbers and age-standardized rates of incidence (A), deaths (B), prevalence (C), YLLs (D), YLDs (E), and DALYs (F) of IBD by age and gender in 2019. Abbreviations: YLLs, years of life lost; YLDs, years lived with disability; DALYs, disability-adjusted life-years. Notes: Column chart: number; line chart: rate; Shading: the upper and lower limits of the 95% uncertainty intervals. |
From 1990 to 2019, the number of deaths and ASMR of IBD in China decreased in both genders. The AAPCs in ASMR of males and females were −3.35 (95%Cl: −3.58, −3.12) and −4.86 (95%Cl: −5.37, −4.35), respectively (Table 1). In 2019, more deaths were found in males than in females generally [2.54 thousand (95% UI: 1.88, 3.15) vs 2.14 thousand (95% UI: 1.65, 2.62)] (Table 1). Further analysis revealed that among people over the age of 90, there were more deaths in females in 2019, while the mortality rate was higher in males at almost all ages (Figure 3B). In 2019, there were fewer deaths in people under 70 years old and more deaths in those over the age of 70 when compared to 1990. (Table 1). Nevertheless, the mortality rate showed a downward trend at all ages. In 2019, the number of deaths increased with age among adults under the age of 85 and declined with age among those over 85 (Figure 3B). The mortality rate was significantly higher in the elderly (Figures 2C and 3B). In addition, among children and adolescents, more IBD deaths were observed in the younger group in 2019 (Figure 3B).
Similarly to the change trend of incidence, the number of prevalent cases and ASPR of IBD in China also increased in both genders and in all age groups over the last three decades (Table 1). The AAPC in ASPR was higher in females than in males (Table 1). In 2019, there were 484.36 thousand (95% UI: 410.51, 571.36) prevalent cases in males and 426.68 thousand (95% UI: 365.76, 497.91) in females in total. However, the gender-based analysis indicated that females had more prevalent cases among people over 85 years old (Figure 3C). Except for the 35–39 age group, the prevalence rate was higher in males than in females in 2019 (Figure 3C). As shown in Table 1, the age group with the highest prevalent cases was 15–49 years old in 1990, whereas it was 50–69 years old in 2019. The 50–69 age group had the highest prevalence rate in both 1990 and 2019, and the highest AAPC in prevalence rate occurred in the 15–49 age group (Table 1, Figure 2A). The more in-depth analysis showed that the number of prevalent cases increased with age among people under 50 years old, peaked in the 50–54 age group, and then decreased with age, for both males and females in 2019 (Figure 3C). Moreover, the prevalence rate peaked in males aged 65–69 and females aged 60–64 (Figure 3C).
Compared with 1990, the number and ASR of YLLs of IBD in China decreased overall in both males and females in 2019 (Table 1). When age was considered in the analysis, the number of YLLs decreased among people under 70 years old and slightly increased among those over 70 years old from 1990 to 2019, and the YLL rate decreased in all age groups (Table 1). In 2019, males and females with the highest number of YLLs were the populations aged 70–74 and 80–84, respectively (Figure 3D). Surprisingly, though the YLLs in the 1–14 age group decreased significantly from 1990 to 2019, children in the 1–4 age group still had a relatively high level of YLLs (Table 1, Figure 3D). In addition, the number of YLLs in 2019 was higher in males than in females among people under 90 years old (Figure 3D). The number and ASR of YLDs of IBD in China showed increasing trends from 1990 to 2019, regardless of gender or age (Table 1). In 2019, except for certain age groups, males had more YLDs and higher YLD rates than females (Figure 3E).
Table 1 illustrates that the number of DALYs was higher in females than in males in 1990. From 1990 to 2019, the number of DALYs decreased in females and increased in males (Table 1). As a result, the number of DALYs in males outnumbered that in females in 2019 [128.4 thousand (95% UI: 98.51, 161.63) vs 104.06 thousand (95% UI: 79.72, 134.43)] (Table 1). The ASDR showed a decreased trend during this period in both males and females, with the AAPCs of −1.76 (95%Cl: −1.91 to −1.6) and −3.03 (95%Cl: −3.24, −2.83), respectively (Table 1). In addition, while the overall ASDR of IBD decreased in China from 1990 to 2019, an increasing trend of DALY rate was observed in people aged 35–44 (Table 1, Figure 2D). More in-depth analysis showed that males had more DALYs than females among the population under 90 years old in 2019, and the DALY rate was higher in males than in females at all ages except 35–39 years old (Figure 3F). In 2019, the 50–69 age group had the highest number of DALYs (Table 1). In the adult population, the DALY rate increased with age for both genders except for males over 90 years old (Figure 3F). Moreover, among children and adolescents under 14 years old, the number of DALYs decreased with age (Figure 3F). Children aged 1–4 had a significant decline in DALYs from 1990 to 2019, whereas they still had a high level of DALYs in 2019 (Figures 2D and 3F).
The Subnational Burden of IBD in China and Its Association with SDI
The ASDR varied in Chinese provinces with different SDI levels. In 1990, the subnational ASDR of IBD ranged from 13.12/100,000 (95% UI: 9.5, 20.41) in Heilongjiang to 71.51/100,000 (95% UI: 12.14, 118.97) in Yunnan (Supplementary Table 1). Yunnan, Shanghai, Guizhou, and Hunan had the highest ASDR level, followed closely by Jiangsu, Guangxi, Beijing, Jiangxi, Xinjiang, and Qinghai (Supplementary Figure 1A and Supplementary Table 1). Meanwhile, Heilongjiang, Macau SAR, Hong Kong SAR, Tianjin, and Hainan were the provinces with the lowest ASDR level in China. There was a significant negative correlation between the ASDR in 1990 and the SDI of Chinese provinces (ρ= −0.3785, p=0.0272) (Supplementary Figure 1B). In 2017, the subnational ASDR estimates ranged from 24.62/100,000 (95% UI: 16.95, 33.81) in Heilongjiang to 63.97/100,000 (95% UI: 44.61, 91.48) in Shanghai (Supplementary Table 1). Shanghai, Jiangsu, Yunnan, and Hunan still had the highest ASDR level, while Heilongjiang, Qinghai, Fujian, and Hainan had the lowest (Figure 4A, Supplementary Table 1). In 2017, there was a positive correlation between the SDI and the ASDR of Chinese provinces, but no statistically significant difference (ρ= −0.2887, p=0.0977) (Figure 4B). From 1990 to 2017, an upward trend in ASDR was observed in most provinces except for Guangxi, Guizhou, Jiangxi, Qinghai, and Yunnan. Nonetheless, the five provinces with decreased ASDR were low-middle and middle SDI areas and all of them were among the top 10 provinces in the ASDR ranking in 1990 (Figure 4B and Supplementary Table 1).
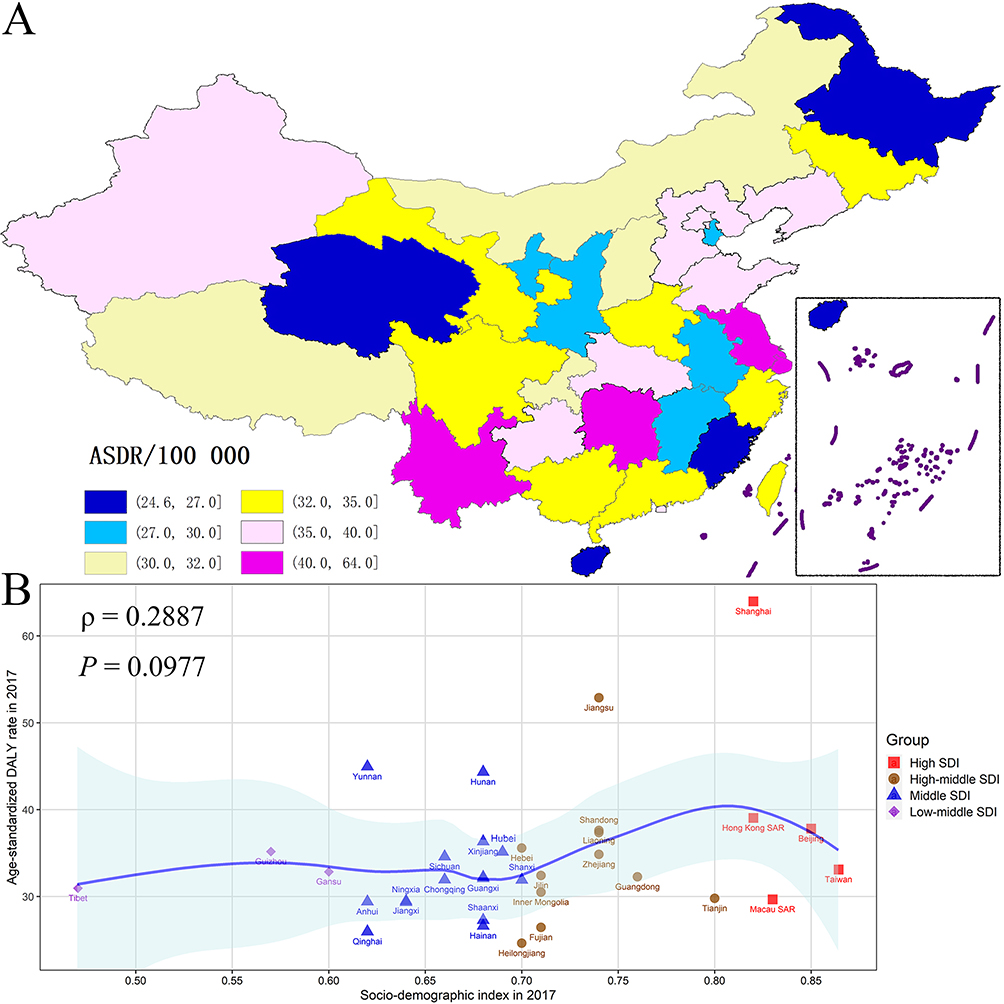 |
Figure 4 The geographical distribution of the ASDR of IBD in 2017 in China (A). The ASDR of IBD for 34 province-level administrative units by different SDI groups in 2017 (B). Abbreviations: ASDR, age-standardized DALY rate; SDI, socio-demographic Index. |
Comparisons of the IBD Burden Among China, Japan, South Korea, the European Union, the USA, and the World
Figure 5 shows the trends of the age-standardized burden rate of IBD in China, Japan, South Korea, the European Union, the USA, and worldwide from 1990 to 2019. Globally, the ASIR decreased slightly from 1990 to 2019 in general. However, China, as well as Japan, South Korea, and the European Union were all on the rise in ASIR. Over the 30-year period, the countries with the highest and lowest ASIR were the USA and China, respectively. As shown in Figure 5, the ASPR and ASR of YLD in these countries and worldwide changed in a similar way to the ASIR. From 1990 to 2019, the ASMR and ASR of YLL showed a downward trend in China, Japan, and South Korea, which differed from the trend in the European Union and the USA but was consistent with the global trend. In addition, the ASDR decreased from 1990 to 2019 worldwide. China and South Korea also showed a downward trend, while Japan and the European Union presented an upward trend. During these three decades, the ASDR of IBD was highest in the USA and lowest in China.
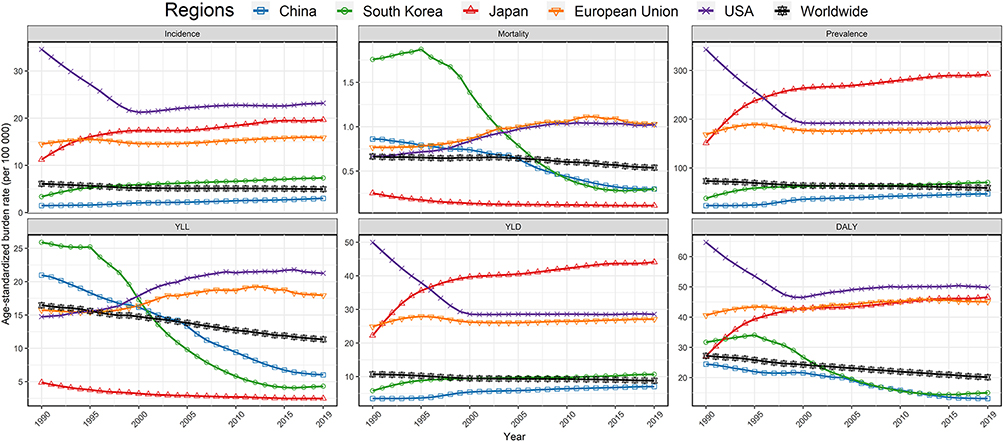 |
Figure 5 The temporal trends of age-standardized burden rates from 1990 to 2019 in China, South Korea, Japan, the European Union, the USA, and worldwide. |
The ASIR and ASPR of IBD in China were at the middle level across the world in 2019 (Figure 6A and Supplementary Figure 2A), and the AAPCs were the highest from 1990 to 2019 (Figure 6B and Supplementary Figure 2B). It can be seen that the ASIR and ASPR were positively associated with the economic level in general (Figure 6A and Supplementary Figure 2A). The ASIR and ASPR were high in the USA, Canada, Australia, New Zealand, Japan, Russia, South Korea, and most European countries, but low in Africa, South America, and most Asian countries and regions. The ASDR and ASMR in China were at a lower level worldwide in 2019 (Figure 6C and Supplementary Figure 2C), and the AAPCs in ASDR and ASMR reflected that China had the most significant downward trend across the world from 1990 to 2019 (Figure 6D and Supplementary Figure 2D).
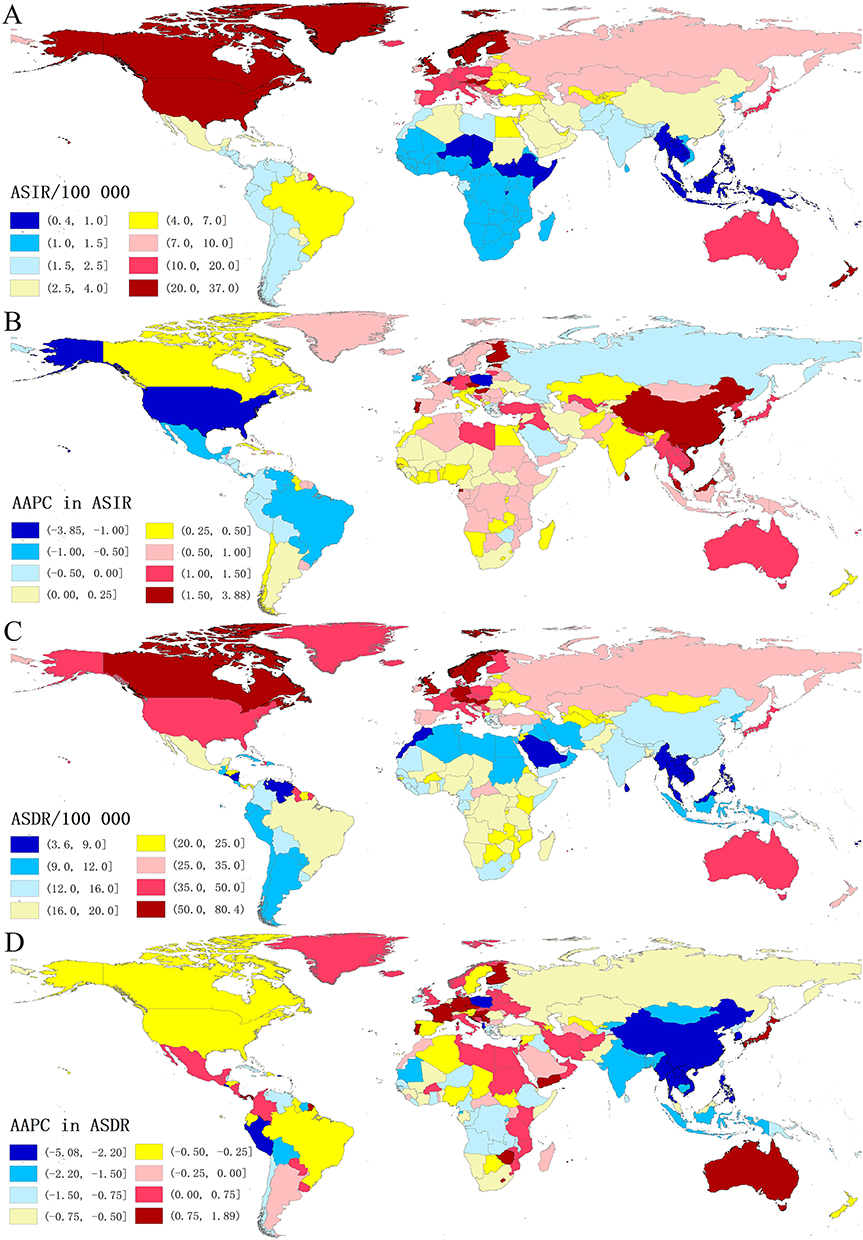 |
Figure 6 The geographical variation in IBD of ASIR (A), AAPC in ASIR (B), ASDR (C), and AAPC in ASDR (D) across countries and regions in 2019. Abbreviations: ASIR, age-standardized incidence rate; AAPC, average annual percentage change; ASDR, age-standardized DALY rate. |
Predictions of the Disease Burden of IBD in China from 2020 to 2030
Based on the GBD 2019 Study, the future disease burden of IBD in China from 2020 to 2030 was predicted in this study (Figure 7). During this decade, the ASIR and ASPR of IBD in China would be expected to continue to increase, with the AAPCs of 2.899 (95% CI: 2.824, 2.975) and 0.882 (95% CI: 0.865, 0.900), respectively (Figure 7A and C). Meanwhile, the ASMR would show a decreasing trend, with an AAPC of −1.533 (95% CI: −1.538, −1.528) (Figure 7B). Though the established ASDR decreased from 1990 to 2019, it was likely to show an upward trend from 2020 to 2030, with an AAPC of 0.735 (95% CI: 0.643, 0.826) (Figure 7D). Compared with 2020, the number of incident cases, deaths, prevalent cases, and DALYs would be higher in predictions of the disease burden of IBD in China in 2030 (Figure 7E). It is worth noting that the observed number of deaths decreased significantly from 2004 to 2015 and then increased from 2015 to 2019, and the growth was expected to continue from 2020 to 2030 (Figure 7E). In addition, except for the number of deaths, our projected number of incident cases, prevalent cases, and DALYs were higher than the pessimistic reference of an annual increase of 1%. By 2030, there would be 72,889 incident cases, 5816 deaths, 1,167,238 prevalent cases, and 329,383 DALYs (Supplementary Table 2).
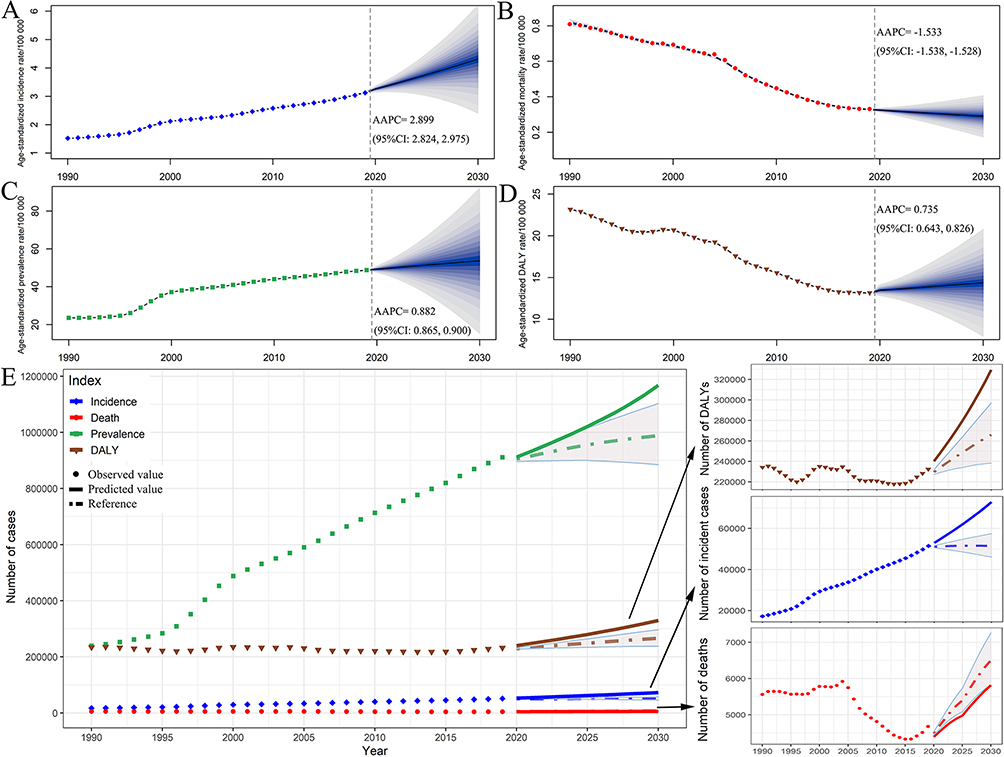 |
Figure 7 The temporal trends of the national disease burden of IBD from 1990 to 2019, and projections until 2030. Age-standardized incidence rate (A), age-standardized mortality rate (B), age-standardized prevalence rate (C), age-standardized DALY rate (D), and numbers of incident cases, deaths, prevalent cases, and DALYs (E). Abbreviations: CI, confidence interval; AAPC, average annual percentage change; DALYs, disability-adjusted life-years. Notes: Shading: a 1% decrease and increase interval based on the observed rate in 2019. |
Discussion
IBD is a costly chronic disease that causes disability and premature mortality and emerges as a major public health problem.26,27 The limited epidemiological data poses a huge challenge to China’s public healthcare system. The objective of this study is to provide an evidence-based assessment of the efficacy of current prevention and therapeutic strategies to reduce the burden of IBD in China and guide future policy planning and implementation. According to this study, the overall disease burden of IBD in China increased significantly from 1990 to 2019. The numbers and ASRs of incidence, prevalence, and YLDs all showed an upward trend during these 30 years, regardless of gender and age. Meanwhile, China had a reduction in the deaths, YLLs, ASMR, and ASDR of IBD from 1990 to 2019, which might be due to the introduction of biological agents and the reform of the healthcare system.28 It also means more medical resources and costs have been invested. According to previous studies, the direct cost of IBD has shifted from inpatient hospitalization and surgery to anti-tumor necrosis factor agents.29,30 As reported, during 2018, the mean direct and indirect costs for IBD per patient in China were about $11,668.68 and $74.90, respectively.31 The direct costs mainly included outpatient costs, hospitalization costs, biological agent costs, and surgery costs, while the indirect costs included transportation costs and accommodation costs.31 However, in China, 85.5% of IBD patients earned less than $1445 a month.31 Another study showed that 30.6% of IBD patients in China spend more than 50% of their income on medical costs.32 The changes in the epidemiological burden of IBD imply a heavier personal financial burden and greater government healthcare pressure in China. There are some suggestions for IBD prevention in China: increase dietary fiber consumption; avoid vitamin D deficiency; reduce the obesity rate; advocate breastfeeding; reduce unnecessary antibiotic exposure; and improve the quality of life, including less stress and more physical activity.33,34 Further, reducing smoking rates can help prevent IBD. However, patients with CD, not UC, should be advised to quit smoking.33,35–37
We conducted a detailed analysis of the effects of age and gender on the epidemiological burden of IBD in China, which is important for the precise formulation of IBD prevention and control strategies. In contrast to the global disease burden of IBD, where females had a higher prevalence than males,38 more prevalent cases and a higher ASPR were observed in males in both 1990 and 2019 in China. In this study, males also had more incident cases and a higher ASIR than females. One reason might be that females had a more traditional lifestyle in China. More possible causes require further investigation. In addition, the observed deaths, YLLs, YLDs, and DALYs data of IBD revealed that males had a heavier disease burden in China, and additional control strategies for males should be optimized. Females had more incident and prevalent cases but lower incidence and prevalence rates than males among people over 85 years old in 2019. Though a lower mortality rate was observed in females than in males among people over the age of 90, there were more females over the age of 90 dead from IBD when compared with males. All of this could be attributed to the fact that there were more females than males at older ages in China.39 In 2019, the number of IBD deaths in China decreased among those under 70 years old but increased among those over 70 years old when compared to 1990. However, the ASMR decreased at all ages, which is most likely due to China’s aging population.40 Canadian health administrative data indicated that the incidence of IBD in children rose rapidly from 1999 to 2010, especially in those under 5 years of age.4,41 In China, the incidence of IBD in children also increased from 1990 to 2019. Moreover, though the deaths, YLLs, and DALYs of IBD in China decreased among children aged 1–4, they remained high in 2019. This reminds us to focus on the diagnosis and treatment of IBD in young children.
In some developed countries, such as Denmark, the IBD population was shifting toward an older age.42,43 Similarly, from 1990 to 2019, the number of new cases of IBD in China significantly exceeded the number of deaths, and the age group with the most prevalent cases shifted from 15–49 to 50–69. However, consistent with previous reports,3,44 IBD still mainly affected young and middle-aged people in China according to this study. They had the most incident cases and the highest incidence rate in 2019, as well as the highest AAPCs in both the incidence and prevalence rates from 1990 to 2019. Moreover, while the overall ASDR declined from 1990 to 2019, the DALY rate in people aged 35–44 increased. There is an urgent need for the government and relevant health policymakers to make efforts in the management of IBD and formulate feasible strategies to reduce the social losses caused by loss of productivity, premature retirement, and death.
China is the world’s largest developing country, with about one-fifth of the world’s population.45,46 China is also a very large and heterogenous country with a wide disparity between rich and poor in different regions.47,48 To the best of our knowledge, this is the first study to report the subnational disease burden of IBD in China and its association with SDI. According to previous research on the global disease burden of IBD, the DALYs decreased in all countries except those with high SDI in the 1990–2017 period.38 From 1990 to 2017, the ASDR of IBD in China decreased overall, whereas detailed subnational analysis implied an upward trend in the majority of provinces. Even though there was no significant correlation between ASDR and SDI in 2017, we discovered that the five provinces with decreased ASDR were low-middle and middle SDI areas with high ASDR rankings in 1990. Strategies should be developed in Chinese provinces with high SDI to reduce the ASDR of IBD.
For the first time, we compared the disease burden of IBD in China to the global level from 1990 to 2019. According to this study, the ASIR and ASPR of IBD in China were at a global medium level and were lowest when compared with some developed countries and regions, including Japan, South Korea, the European Union, and the USA. However, while global ASIR and ASPR declined from 1990 to 2019, China showed significant upward trends and had the highest AAPCs in the world. In addition, the ASMR and ASDR of IBD in China had the sharpest decline across the world during these three decades. China appeared to be experiencing the most significant changes in the disease burden of IBD globally. Great changes have occurred in China over the last 30 years, including rapid economic development, increased industrialization, and the westernization of lifestyles. Furthermore, the changes also included the development of the healthcare system, the advancement of IBD diagnosis, and the use of biological agents. All of these were linked to shifts in the national disease burden of IBD. In addition, the ratio of prevalence to incidence figures in China was strikingly lower than in countries with high incidence rates. This is presumably due to the prevalent cases being lower because of the very low incidence rates at the start of the study period. However, with demographic changes in China, such as the rapidly aging population and low birth rate, the ratio would increase in the future.
This study also provides accurate estimates of the disease burden of IBD in China from 2020 to 2030, which would continue to increase. The projections aim to aid in the development of healthcare programs and strategies to adapt the healthcare system to the increased disease burden. This study also has some limitations. First, we could not divide IBD into UC and CD in this study because there is no separate data for these two subtypes in the GBD 2019 database. UC and CD are not only different in some risk factors, such as age and gender, but also have different epidemiological distributions in most areas of China. We expect the corresponding data to be addressed in the next iteration of the GBD study. Secondly, as is common knowledge, DALYs is composed of YLLs and YLDs. Only DALYs data were used for analysis when examining the subnational disease burden of IBD in China and its association with SDI. This might prevent the extraction of certain potentially significant results. Thirdly, we must acknowledge that the subnational data may be limited due to the absence of a centralized IBD disease recording system in China.
Conclusion
In summary, we did a comprehensive and in-depth analysis of the disease burden of IBD in China from 1990 to 2030 and compared it with Japan, South Korea, the European Union, the USA, and the world for the first time. The disease burden of IBD in China significantly increased from 1990 to 2019 and would continue to increase in predictions in 2030. In 2019, the ASIR and ASPR of IBD in China were in the middle of the world and still lower than in Japan, South Korea, the European Union, and the USA. However, China had the world’s opposite but most dramatic trends in ASIR and ASPR of IBD from 1990 to 2019. There is an urgent need to adapt the healthcare system to manage this costly and complex disease.
Data Sharing Statement
The data that support the findings of this study are openly available in Global Health Data Exchange, at http://ghdx.healthdata.org/gbd-results-tool.
Ethics Approval and Informed Consent
The GBD 2019 study is a publicly available database and all data were anonymous. Our study protocol was approved by the Institutional Review Boards of Qilu Hospital of Shandong University with approval number KYLL-202011(KS)-239.
Acknowledgments
Xiaorong Yang and Xiaoyun Yang are co-corresponding authors of this paper. We thank the countless individuals who have contributed to the Global Burden of Disease Study 2019 in various capacities.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Key Research and Development Program of China (grant numbers: 2018YFB1307700), the National Natural Science Foundation of China (grant numbers: 82270570 and 82103912), and the Emergency and Critical Care Medicine Program of Clinical Research Center of Shandong University (No. 2021SDUCRCB003); and the China Postdoctoral Science Foundation (2021M700080). The funders were not involved in the collection, analysis, or interpretation of data, or the writing or submitting of this report. The corresponding author had full access to all of the data and the final responsibility to submit it for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ordas I, Eckmann L, Talamini M, Baumgart DC, Sandborn WJ. Ulcerative colitis. Lancet. 2012;380(9853):1606–1619. doi:10.1016/S0140-6736(12)60150-0
2. Torres J, Mehandru S, Colombel JF, Peyrin-Biroulet L. Crohn’s disease. Lancet. 2017;389(10080):1741–1755. doi:10.1016/S0140-6736(16)31711-1
3. Sairenji T, Collins KL, Evans DV. An Update on Inflammatory Bowel Disease. Prim Care. 2017;44(4):673–692. doi:10.1016/j.pop.2017.07.010
4. Carroll MW, Kuenzig ME, Mack DR, et al. The impact of inflammatory bowel disease in Canada 2018: children and adolescents with IBD. J Can Assoc Gastroenterol. 2019;2(Suppl 1):S49–S67. doi:10.1093/jcag/gwy056
5. GBD 2017 Inflammatory Bowel Disease Collaborators. The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020;5(1):17–30. doi:10.1016/S2468-1253(19)30333-4
6. Na SY, Moon W. Perspectives on current and novel treatments for inflammatory bowel disease. Gut Liver. 2019;13(6):604–616. doi:10.5009/gnl19019
7. Henriksen M, Jahnsen J, Lygren I, et al. Ulcerative colitis and clinical course: results of a 5-year population-based follow-up study (the IBSEN study). Inflamm Bowel Dis. 2006;12(7):543–550. doi:10.1097/01.MIB.0000225339.91484.fc
8. Baumgart DC, Sandborn WJ. Crohn’s disease. Lancet. 2012;380(9853):1590–1605. doi:10.1016/S0140-6736(12)60026-9
9. Le Berre C, Ananthakrishnan AN, Danese S, Singh S, Peyrin-Biroulet L. Ulcerative colitis and Crohn’s disease have similar burden and goals for treatment. Clin Gastroenterol Hepatol. 2020;18(1):14–23. doi:10.1016/j.cgh.2019.07.005
10. Peyrin-Biroulet L, Loftus EV, Colombel JF, Sandborn WJ. The natural history of adult Crohn’s disease in population-based cohorts. Am J Gastroenterol. 2010;105(2):289–297. doi:10.1038/ajg.2009.579
11. Knowles SR, Graff LA, Wilding H, Hewitt C, Keefer L, Mikocka-Walus A. Quality of life in inflammatory bowel disease: a systematic review and meta-analyses-part I. Inflamm Bowel Dis. 2018;24(4):742–751. doi:10.1093/ibd/izx100
12. Shafer LA, Walker JR, Restall G, et al. Association between IBD disability and reduced work productivity (presenteeism): a population-based study in Manitoba, Canada. Inflamm Bowel Dis. 2019;25(2):352–359. doi:10.1093/ibd/izy236
13. Ng SC, Mak JWY, Pal P, Banerjee R. Optimising management strategies of inflammatory bowel disease in resource-limited settings in Asia. Lancet Gastroenterol Hepatol. 2020;5(12):1089–1100. doi:10.1016/S2468-1253(20)30298-3
14. Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. 2017;390(10114):2769–2778. doi:10.1016/S0140-6736(17)32448-0
15. GBD 2019 Diseases and Injuries Collaborator. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
16. GBD 2017 Population and Fertility Collaborators. Population and fertility by age and sex for 195 countries and territories, 1950–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1995–2051. doi:10.1016/S0140-6736(18)32278-5
17. GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1223–1249. doi:10.1016/S0140-6736(20)30752-2
18. Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;394(10204):1145–1158. doi:10.1016/S0140-6736(19)30427-1
19. Yang X, Man J, Chen H, et al. Temporal trends of the lung cancer mortality attributable to smoking from 1990 to 2017: a global, regional and national analysis. Lung Cancer. 2021;152:49–57. doi:10.1016/j.lungcan.2020.12.007
20. Yang X, Fang Y, Chen H, et al. Global, regional and national burden of anxiety disorders from 1990 to 2019: results from the Global Burden of Disease Study 2019. Epidemiol Psychiatr Sci. 2021;30:e36. doi:10.1017/S2045796021000275
21. Yu J, Yang X, He W, Ye W. Burden of pancreatic cancer along with attributable risk factors in Europe between 1990 and 2019, and projections until 2039. Int J Cancer. 2021;149(5):993–1001. doi:10.1002/ijc.33617
22. Yang X, Zhang T, Zhang H, Sang S, Chen H, Zuo X. Temporal trend of gastric cancer burden along with its risk factors in China from 1990 to 2019, and projections until 2030: comparison with Japan, South Korea, and Mongolia. Biomark Res. 2021;9(1):84. doi:10.1186/s40364-021-00340-6
23. Knoll M, Furkel J, Debus J, Abdollahi A, Karch A, Stock C. An R package for an integrated evaluation of statistical approaches to cancer incidence projection. BMC Med Res Methodol. 2020;20(1):257. doi:10.1186/s12874-020-01133-5
24. Du Z, Chen W, Xia Q, Shi O, Chen Q. Trends and projections of kidney cancer incidence at the global and national levels, 1990–2030: a Bayesian age-period-cohort modeling study. Biomark Res. 2020;8:16. doi:10.1186/s40364-020-00195-3
25. Wang H, Zhao S, Wang S, et al. Global magnitude of encephalitis burden and its evolving pattern over the past 30 years. J Infect. 2022;84(6):777–787. doi:10.1016/j.jinf.2022.04.026
26. Dulai PS, Singh S, Ohno-Machado L, Sandborn WJ. Population health management for inflammatory bowel disease. Gastroenterology. 2018;154(1):37–45. doi:10.1053/j.gastro.2017.09.052
27. Click B, Lopez R, Arrigain S, Schold J, Regueiro M, Rizk M. Shifting cost-drivers of health care expenditures in inflammatory bowel disease. Inflamm Bowel Dis. 2020;26(8):1268–1275. doi:10.1093/ibd/izz256
28. Yao LY, Shao BL, Tian F, et al. Trends in medication use and treatment patterns in Chinese patients with inflammatory bowel disease. World J Gastroenterol. 2022;28(30):4102–4119. doi:10.3748/wjg.v28.i30.4102
29. El-Matary W, Kuenzig ME, Singh H, et al. Disease-associated costs in children with inflammatory bowel disease: a systematic review. Inflamm Bowel Dis. 2020;26(2):206–215. doi:10.1093/ibd/izz120
30. van der Valk ME, Mangen MJ, Leenders M, et al. Healthcare costs of inflammatory bowel disease have shifted from hospitalisation and surgery towards anti-TNFalpha therapy: results from the COIN study. Gut. 2014;63(1):72–79. doi:10.1136/gutjnl-2012-303376
31. Yu Q, Zhu C, Feng S, et al. Economic burden and health care access for patients with inflammatory bowel diseases in China: web-based survey study. J Med Internet Res. 2021;23(1):e20629. doi:10.2196/20629
32. Luo XP, Mao R, Chen BL, et al. Over-reaching beyond disease activity: the influence of anxiety and medical economic burden on health-related quality of life in patients with inflammatory bowel disease. Patient Prefer Adherence. 2017;11:23–31. doi:10.2147/PPA.S118589
33. Ananthakrishnan AN. Epidemiology and risk factors for IBD. Nat Rev Gastroenterol Hepatol. 2015;12(4):205–217. doi:10.1038/nrgastro.2015.34
34. Piovani D, Danese S, Peyrin-Biroulet L, Nikolopoulos GK, Lytras T, Bonovas S. Environmental risk factors for inflammatory bowel diseases: an umbrella review of meta-analyses. Gastroenterology. 2019;157(3):647–659 e644. doi:10.1053/j.gastro.2019.04.016
35. Lakatos PL, Vegh Z, Lovasz BD, et al. Is current smoking still an important environmental factor in inflammatory bowel diseases? Results from a population-based incident cohort. Inflamm Bowel Dis. 2013;19(5):1010–1017. doi:10.1097/MIB.0b013e3182802b3e
36. Mahid SS, Minor KS, Soto RE, Hornung CA, Galandiuk S. Smoking and inflammatory bowel disease: a meta-analysis. Mayo Clin Proc. 2006;81(11):1462–1471. doi:10.4065/81.11.1462
37. Higuchi LM, Khalili H, Chan AT, Richter JM, Bousvaros A, Fuchs CS. A prospective study of cigarette smoking and the risk of inflammatory bowel disease in women. Am J Gastroenterol. 2012;107(9):1399–1406. doi:10.1038/ajg.2012.196
38. Piovani D, Danese S, Peyrin-Biroulet L, Bonovas S. Inflammatory bowel disease: estimates from the global burden of disease 2017 study. Aliment Pharmacol Ther. 2020;51(2):261–270. doi:10.1111/apt.15542
39. Word Health Organization. World Health Statistics 2021; 2021. Available from: https://www.who.int/publications/i/item/9789240027053.
40. Fang EF, Scheibye-Knudsen M, Jahn HJ, et al. A research agenda for aging in China in the 21st century. Ageing Res Rev. 2015;24(Pt B):197–205. doi:10.1016/j.arr.2015.08.003
41. Benchimol EI, Bernstein CN, Bitton A, et al. Trends in epidemiology of pediatric inflammatory bowel disease in Canada: distributed network analysis of multiple population-based provincial health administrative databases. Am J Gastroenterol. 2017;112(7):1120–1134. doi:10.1038/ajg.2017.97
42. Agrawal M, Christensen HS, Bogsted M, Colombel JF, Jess T, Allin KH. The rising burden of inflammatory bowel disease in Denmark over two decades: a Nationwide Cohort Study. Gastroenterology. 2022;163(6):1547–1554.e5. doi:10.1053/j.gastro.2022.07.062
43. Faye AS, Colombel JF. Aging and IBD: a new challenge for clinicians and researchers. Inflamm Bowel Dis. 2022;28(1):126–132. doi:10.1093/ibd/izab039
44. Windsor JW, Kaplan GG. Evolving Epidemiology of IBD. Curr Gastroenterol Rep. 2019;21(8):40. doi:10.1007/s11894-019-0705-6
45. Feng RM, Zong YN, Cao SM, Xu RH. Current cancer situation in China: good or bad news from the 2018 Global Cancer Statistics? Cancer Commun. 2019;39(1):22. doi:10.1186/s40880-019-0368-6
46. Zhu H, Ma X, Ye T, et al. Esophageal cancer in China: practice and research in the new era. Int J Cancer. 2022;152:1741–1751. doi:10.1002/ijc.34301
47. Yang W, Zhao R, Chuai X, et al. China’s pathway to a low carbon economy. Carbon Balance Manag. 2019;14(1):14. doi:10.1186/s13021-019-0130-z
48. Peng Z, Wu L. Association of income relative deprivation and sleep duration in China. Front Psychol. 2022;13:1008259. doi:10.3389/fpsyg.2022.1008259
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.