")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Temporal Trend and Research Focus of Injury Burden from 1998 to 2022: A Bibliometric Analysis
Authors Liu T , Li Y, Li J, Fan H, Cao C
Received 29 March 2023
Accepted for publication 12 June 2023
Published 3 July 2023 Volume 2023:16 Pages 1869—1882
DOI https://doi.org/10.2147/JMDH.S414859
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Tao Liu,1,* Yue Li,2,* Ji Li,1 Haojun Fan,1 Chunxia Cao1
1Institute of Disaster and Emergency Medicine, Tianjin University, Tianjin, People’s Republic of China; 2College of Management and Economics, Tianjin University, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chunxia Cao, Institute of Disaster and Emergency Medicine, Tianjin University, No. 92 Weijin Road, Nankai District, Tianjin, 300072, People’s Republic of China, Tel +86 02227893596, Fax +86 02227893596-307, Email [email protected]
Background: Injury is one of the leading causes of mortality and disability worldwide. It is a major contributor to the overall burden of disease. This study aimed to analyze the temporal trend, research focus and future direction of research related to injury burden.
Methods: Publications on injury burden published between January 1998 and September 2022 were extracted from the Web of Science Core Collection (WoSCC) through topic advanced search strategy. Microsoft Excel, RStudio, VOSviewer, and CiteSpace were used to extract, integrate, and visualize bibliometric information.
Results: A total of 2916 articles and 783 reviews were identified. The number of publications on injury burden showed a steady upward trend. The United States of America (USA) (n=1628) and the University of Washington (n=1036) were the most productive country and institution. High-income countries started research in this domain earlier, while research in low- and middle-income countries began in recent years. Lancet was the most influential journal. Public, environmental occupational health, general medicine and neurology were the predominant research domains. Based on keyword co-occurrence analysis, the research focus was divided into five clusters: injury epidemiology and prevention, studies related to the global burden of disease (GBD), risk factors for injury, clinical management of injury, and injury outcome assessment and economic burden.
Conclusion: The burden of injury has drawn increasing attention from various perspectives over the years. The research field on injury burden is also becoming more and more extensive. However, there are some gaps among different countries or regions, and more attention needs to be paid to low and middle-income countries.
Keywords: injury burden, bibliometric analysis, trend, focus, VOSviewer, CiteSpace
Introduction
Almost every individual is affected by traumatic experiences worldwide. These experiences might be encountered in a variety of ways, including natural disasters, war, and violence as well as road traffic accidents, falls, occupational injuries, or other injuries.1 Injury has become an international public health matter, resulting in the most frequent mortality and morbidity.2 According to the World Health Organization (WHO) statistics, about 10% of deaths and 16% of disabled are caused by injury globally.3 Injury is not only associated with an increased risk of adverse health outcomes (eg, venous thromboembolism, acute kidney injury, post-traumatic stress disorder, and sleep disorders) but also regularly poses a significant economic impact on patients’ families and society.4–8 It has been reported that the costs of injury-related care were estimated to exceed 400 billion dollars per year in the United States of America (USA) alone.9 The burden of injury could be high in regions of the world where health data are lacking.10 Consequently, the injury burden is underestimated, which is hugely challenging to understand better. Motivated by the magnitude of the situation, the research on injury burden is gaining increasing attention. A number of papers related to this field have been published. However, the issue of how trends and focus of injury burden research evolved has not been adequately addressed. In an era of rapidly growing knowledge and information, some evidence-based systematic reviews and meta-analyses would be challenging to generate a broad overview of a field from a holistic and comprehensive perspective within a relatively short time, although these methods could contribute valuable information and reliable conclusions.11
Bibliometric analysis is one of the most popular mathematical statistics-based methods for clarifying academic productivity, summarizing research trends and hotspots, and predicting the direction of a research field through qualitative and quantitative assessments.12,13 It could not only provide researchers with a comprehensive analysis and structured information to identify research frontiers but also inform research policy and management decisions. In recent years, bibliometric analysis has been increasingly used to analyze research in fields including healthcare, fracture, road traffic injury, child abuse, and disaster risk reduction.10,14–17
In this study, we aimed to analyze (i) the research trends and the focus on injury burden and predict future research directions, and (ii) the scholarly contributions and influence of different countries, institutions, authors, and journals by bibliometric method and indicators in order to contribute to the reduction of injury burden.
Materials and Methods
Data Source
The Web of Science Core Collection (WoSCC) database is a typical citation database and a frequently used database for bibliometric analysis. It is large enough to reflect the research landscape in a specific domain.18 In our study, all literature was searched and downloaded from WoSCC on October 10, 2022, to avoid bias due to database updates. Two investigators searched independently with 100% agreement (kappa = 1 > 0.75). The expressions are as follows: kappa = (P0-Pe) / (n-Pe).
Search Strategy
The search strategy was as follows: (TS = (injury OR injuries OR trauma*)) AND TS = (“cost of illness” OR “illness costs” OR “burden of illness” OR “illness burden” OR “disease burden$” OR “burden of disease$” OR “disease cost$” OR “cost$ of disease” OR “economic burden” OR “hospital burden” OR “public health burden” OR “socioeconomic burden”). The literature published from January 1, 1998 (our earliest access to the WoSCC records) to September 30, 2022, was included. Only articles and reviews were included and other types of publications (such as meeting abstracts, editorial materials, letters and early access, etc.), were excluded. No language restrictions were applied. Finally, 3699 publications were available as the ultimate dataset of further analysis (Figure 1).
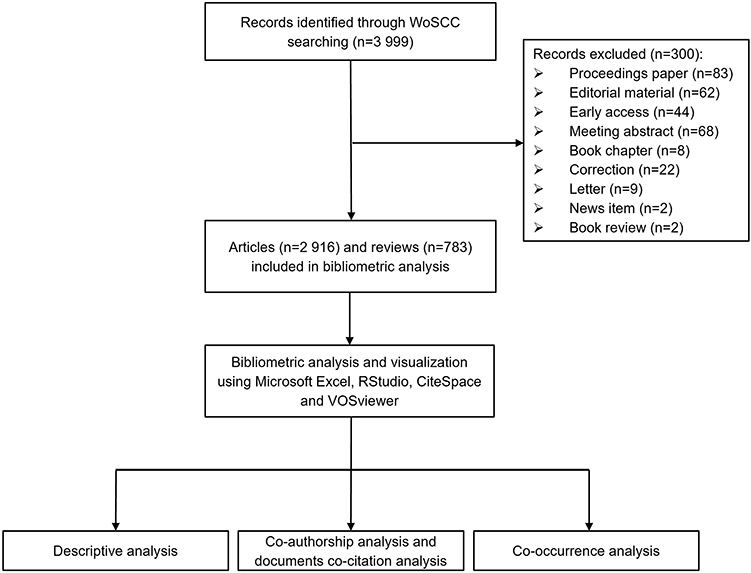 |
Figure 1 Flow chart of the literature search, selection, and analysis process. Abbreviation: WoSCC, Web of Science Core Collection. |
Data Extraction and Collection
All the information, including the number of publications and citations, titles, publication year, countries of publications, institutions, journals, authors, keywords, and references, was collected. The text format document including all bibliometric information was downloaded from the WOSCC. For more accurate bibliometric data analysis, information such as countries, institutions, and keywords, was cleaned from the above-mentioned document data to reduce the bias caused by some inherent weaknesses in the WoSCC database. The information for individual regions was incorporated into their respective countries, for example, publications for England, Northern Ireland, Scotland and Wales were merged into the United Kingdom (UK). Countries were classified by income groups using the World Bank income groupings.19 Furthermore, the impact factor (IF) (2022) and Journal citation reports (JCR) (2022) were obtained from the Web of Science.
Data Analysis
Descriptive analysis, graph plotting, and curve fitting were performed with Microsoft Excel version 2019 (Microsoft Corporation, the USA). To achieve a more comprehensive data analysis, VOSviewer version 1.6.18 (Leiden University, The Netherlands), CiteSpace version 6.1.R3 (Drexel University, USA) and RStudio version 2022.07.1 (RStudio Team, Boston MA) were used for bibliometric and visual analysis.
The number of annual and cumulative publications and the growth rate of publications over time were calculated using Microsoft Excel. Growth rate = [(number of publications in the last year ÷ number of publications in the first year) 1/(last year−first year) −1] × 100.20 To better understand the temporal trends in publications regarding injury burden, exponential and polynomial curve fits between the year and the annual number of publications were plotted. The best-fit model was picked based on the correlation coefficients (R2).
VOSviewer is a software for java based bibliometric mapping and clustering analysis by van Eck and Waltman.21 In this study, country/institution/author co-authorship analysis, author/journal co-citation analysis, journal bibliographic coupling analysis, and keywords co-occurrence analysis were conducted. Manual standardization was performed to address some countries, institutions, and keyword terms when possible because of the presence of different names, misspellings, or variations (eg, plurals, synonyms) of words.22 In the network visualization map, different nodes represented different items such as countries, institutions, authors, journals and keywords, the node size represented the number of publications, citations or frequency of appearance, and the different colors represented clusters or average years of appearance (AAY), and the thickness of the lines represented the strength of the connection between the nodes.
CiteSpace is a visualization tool for visualizing and constructing bibliometric networks developed by Professor Chen Chaomei.23 In this study, CiteSpace was used to construct a cluster analysis and presented the clusters in form of a timeline view. The modularity value (Q value) and weighted mean silhouette value (S value) were two indicators to evaluate the significance of clustering. It was generally accepted that Q > 0.30 suggests a significant clustering structure and S > 0.50 implies that the clusters are convincing.24 We also identified the top 20 references that experienced the greatest increase in the frequency of citations over a certain period, which was considered a period of popularity for the study.
Results
Basic Characteristics
Based on the selection criteria, 3699 documents (2916 articles and 783 reviews) on injury burden were published in the WoSCC from 1998 to the date and included in the study. Of these, English (97.89%) was the primary language of research, and 60.99% of publications were open access.
Publication Outputs and Trends
Figure 2 shows the number of annual and cumulative publications from 1998 to 2022 (by 30 September). The number of publications showed a steady upward trend, from 9 documents in 1998 to 495 documents in 2021, with an average annual growth rate of 64.77%, and half of the publications were published in recent 5 years. The curve fitting results showed that the annual publications satisfied the third-order polynomial, with the formula y = 0.0657×3 - 1.1452×2 + 10.968x - 7.0909 (R2=0.9921). In which y represents the number of publications and x represents the year. It could be expected that the number of publications related to the injury burden will continue to increase in the next years.
 |
Figure 2 The number of annual and cumulative publications on injury burden research from 1998 to 2022 (by 30 September). The “Annual number of publications” is referred to on the left axis and the “cumulative number of publications” is to the right axis. |
Most Productive Countries
In this study, 150 countries contributed to the publication on injury burden. Table 1 lists the 10 most productive countries. The USA published the highest number of papers (1628, 44.01%). The UK was the next leading country (727, 19.7%), followed by China (599, 16.2%). Publications from the USA were cited the most (135,572, 55.00%). Publications from Tanzania had the highest average citation per paper (291.167), followed by Switzerland (247.228). There were a large number of papers on single-country publications (SCP) and multi-country publications (MCP) from the USA.
 |
Table 1 Top 10 Most Productive Countries on Injury Burden |
The country co-authorship analysis showed the level of interaction between influential countries in this field. With a threshold of at least 5 publications per country, 86 countries were selected, forming a graph of national collaborations with 1998 links and a total link strength (TLS) of 11,405 (Figure 3). Researchers from the USA displayed the highest collaboration performance with a TLS of 2299, followed by the UK (TLS = 1496) and Australia (TLS = 1249). These relationships were driven by high and upper-middle-income countries and were lacking in low-income and lower-middle-income countries. Developed countries such as the USA, UK, Canada, Australia, and Switzerland started research in this field earlier, while the research on injury burden in developing countries such as China and India began in recent years.
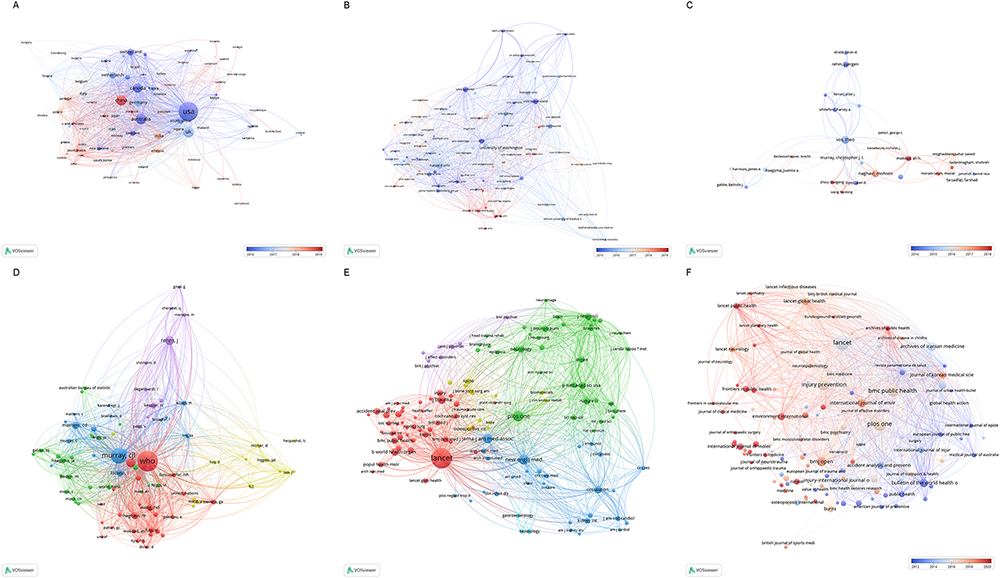 |
Figure 3 Network visualization map for (A) country collaboration, (B) institution collaboration, (C) author co-authorship (D) author co-citation (E) journal co-citation, and (F) bibliographic coupling of journals. |
Analysis of Institutional Output
Concerning the 10 most frequent institutions, the University of Washington in the USA was the leading institution, followed by Harvard University in the USA and the University of London in the UK (Table 2). Four are located in the USA, three in Australia, one in the UK, one in Canada, and one in Iran.
 |
Table 2 Top 10 Most Frequent Institutions on Injury Burden Research |
The institution collaboration network is shown in Figure 3. The most collaborative institutions included the following: the University of Washington (TLS = 618), Harvard University (TLS = 314), and the University of Queensland (TLS = 261), among others. China’s institutions, such as Chinese control disease and prevention, Peking University and Sichuan University also contributed a number of publications in this field while their studies are later, suggesting that they are paying more and more attention to this field in recent years.
Analysis of Influential Authors
In terms of the most influential authors, Vos T ranked first with 164 publications, followed by Murray CJL with 162 publications and Naghavi M with 156 publications. Vos T, Murray CJL and Naghavi M were also the most locally cited authors.
The network visualization maps for author co-authorship and author co-citation on injury burden are shown in Figure 3. Vos T had the largest TLS of 97 (Figure 3). Remarkably, several authors tended to cooperate with a small group of collaborators, generating six major clusters of authors, each usually having one or two core authors. WHO with a TLS of 15,126 and links of 89 and Murray CJL with a TLS of 12,892 and links of 88 made significant contributions to the field of injury burden (Figure 3).
Most Active Journals and Research Areas
Table 3 shows the basic information of the top 10 most productive journals on injury burden research, including journal titles, record counts, the percentage of articles, JCR, IF (2022) and journal countries (JC). Lancet published the most papers, followed by PLoS One and BMC Public Health. Lancet had the highest IF of any journal in 2022. Among these, most were classified as Q1 or Q2 according to the JCR 2022 standards. Six of 10 journals are published in the UK. The most relevant journals were identified (eg, Lancet, JAMA-the journal of the American Medical Association, New England Journal of Medicine, and PLoS One) by an analysis of co-citations (Figure 3). Those mainly appeared in journals with world-class influence. While co-citation analysis reveals more about relationships among older papers, bibliographic coupling analysis reflects more about the current research front. A total of 142 journals had at least five publications. The journal with the highest number of TLS was Lancet (TLS = 29,792), followed by PLoS One (TLS = 12,220) and Injury Prevention (TLS = 10,985) (Figure 3). Additionally, the documents in the WoS database are assigned to different research areas. The top 10 research areas ranked by publication counts are exhibited in Figure 4.
 |
Table 3 Top 10 Most Active Journals on Injury Burden |
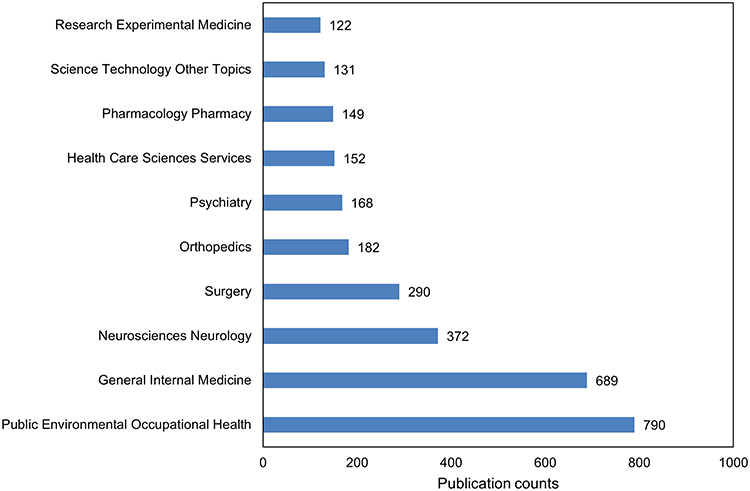 |
Figure 4 Top 10 research areas ranked by publication counts on injury burden research. |
Analysis of Highly Cited References and Reference Burst
Table 4 summarizes the characteristics of the top 10 highly cited literature within injury burden studies. These studies were systematic analyses using GBD data published in Lancet. References with strong citation bursts were explored through CiteSpace and the top 20 references with the strongest citation bursts were identified (Figure 5). The strongest burst starting from 2009 was from the paper published by WHO25, followed by Murray et al26 and Lozano et al.27
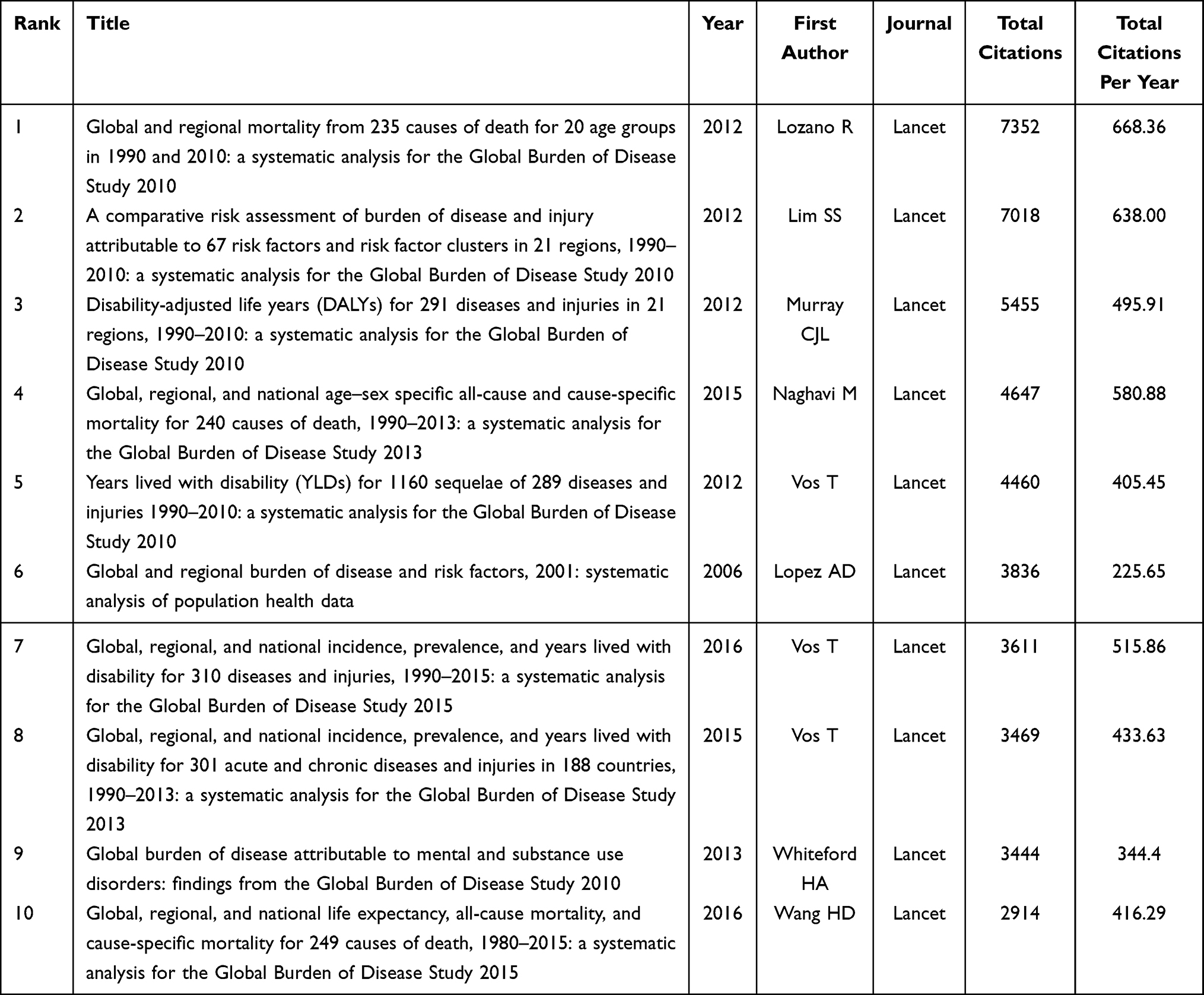 |
Table 4 Characteristics of Top 10 Highly Cited Literature on Injury Burden |
 |
Figure 5 Top 20 references with the strongest citation bursts on injury burden research. Note: *** The global burden of disease: 2004 update was a publication produced by WHO. Available at: https://www.who.int/publications/i/item/9789241563710. |
Analysis of Keywords
The keywords timeline view displays the evolution of high-frequency keywords. As shown in Figure 6, the keywords could be grouped into 6 major clusters. The modularity was 0.38, and the mean silhouette value was 0.69, reflecting the rationality of this clustering method. All these clusters were generalized and ordered by the frequency of keywords. #0 inflammation was the largest cluster, followed by #1 burden of disease, #2 post-traumatic stress disorder, #3 cost of illness, #4 meta-analysis, #5 acute kidney injury. The results reflected the increasing depth of research on the injury burden.
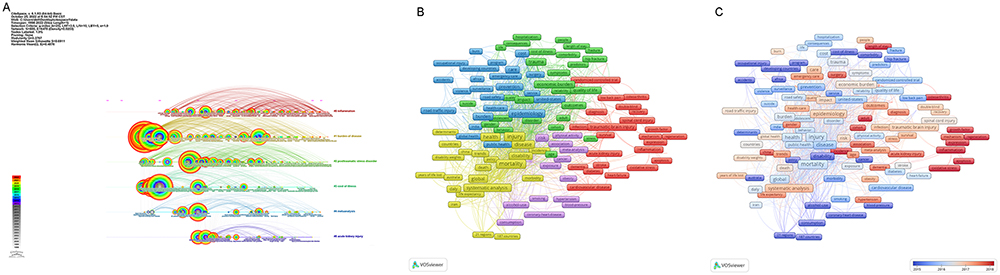 |
Figure 6 Analysis of keywords. (A) keywords timeline view; (B) keyword co-occurrence; (C) overlay visualization map. |
After merging the keywords with the same meaning, a total of 172 keywords with a minimum of 25 occurrences were extracted from the 3699 publications. A network visualization marked with different colors based on the frequency of keyword co-occurrence in the cited literature was created and the keywords were classified into 5 clusters by cluster analysis (Figure 6).
Cluster 1 (blue): Injury epidemiology and prevention.
Cluster 2 (yellow): GBD-related studies.
Cluster 3 (purple): Risk factors for injury.
Cluster 4 (green): Clinical management of injury, including injury-related disease cluster management and pathophysiological mechanisms.
Cluster 5 (red): Injury outcome assessment and economic burden.
To reflect the changes in research topics in recent years, an overlay visualization map marked with different colors based on AAY was created. The larger AAY of keywords, the closer to the present, and the higher the topic attention (Figure 6). New emerging keywords in the last 3 years were cohort, incidence, adult, China, surgery, length of stay, inflammation, oxidative stress, mechanism, etc.
Discussion
In this study, the bibliometric approach was utilized to analyze development trends and research focus of the injury burden field, as well as identify the main force and important cited publications. The results could provide insight into the injury burden research to promote ideas for future investigation and serve researchers, educators, doctors, nursing experts, and stakeholders to have a more comprehensive knowledge of this field.
Temporal Trends on Injury Burden
The change in the number of academic publications is a vital indicator of the evolving trends in a field.28 The global trend of the annual number of publications and the associated cumulative number showed a steady increase from 1998 to 2021, with half of these articles published in the last five years. The curve-fitting results also verified this trend. The results indicated that injury burden has become an increasingly important research topic and attracted a great deal of attention and academic research effort from scholars. This partly reflected the high morbidity, disability, and mortality rates and the high economic burden of injury. With this in mind, one could predict that the number of publications in this area would grow further with in-depth research on the intrinsic mechanisms and long-term effects of injury and the issuing of a series of policies or regulations on injury reduction in countries around the world.29–31
General Knowledge Structure on Injury Burden
From the perspective of countries, the total number of publications by a country is an important indicator to reflect a country’s output and productivity. The USA had an overwhelmingly dominant position in both the number of publications and citations. The USA also had a robust national and international collaboration in injury burden research with the highest SCP and MCP. In the country co-authorship map, it could be seen that the USA had the largest nodes and densest links and started research in this field earlier. The above results demonstrated a significant contribution of the USA to the research on injury burden. In economic terms, most were high-income countries and no were low-income countries of the top 10 most represented countries, which revealed the level of scientific research was closely related to the level of economic development. The developed countries would invest more in scientific research and development.32 Moreover, low- and middle-income countries may lack the capacity and financial resources to conduct research independently or have difficulty establishing collaborations with other countries.33 The overlay visualization map of country co-authorship showed that more countries, such as China and Russia, have joined the research on this field in recent years, especially in developing countries. Among the top 10 institutions, four were in the USA, three in Australia, one each in the UK and Canada, and one in Iran. The University of Washington in the USA was the most influential institution in this field, and the study on GBD was led by the Institute for Health Metrics and Evaluation at the University of Washington. Recently, institutions such as the Chinese Center for Disease Control and Prevention and Peking University have expanded their influence in the field of injury burden, likely due to the establishment of a China network on global health and the improvement of injury care systems.34,35 Yet, cross-national or cross-institutional collaboration was weak, both at the national and institutional levels, which greatly hindered the development of research on injury burden. In the context of globalization, it is an inevitable trend for researchers from different countries to join in to help the world hear more national voices. Therefore, we strongly recommend that different countries and different institutions should remove academic barriers and strengthen cooperation to boost the development of this field.
Analyzing the most influential authors could be helpful for scholars to understand the existing partnerships and identify potential collaborations at home and abroad.36 Vos T was the most productive author, followed by Murray CJL and Naghavi M. They were all GBD collaborators. They were also the core authors in the field as seen in the overlay author collaboration network map. The co-citation analysis is usually considered to be a better approach to evaluating the academic influence of a scholar.37 The author’s co-citation analysis showed that WHO and Murray CJL occupied the maximum node with the largest citations. Combining the results of the highly cited literature and the reference burst, their papers were published earlier and cited more. Thus, paying attention to their research directions could help researchers to grasp the authoritative dynamics of this field. Interestingly, this result revealed that the number of publications may not definitely reflect the academic influence of a scholar, since there were multifactor influencing the citation frequencies of a paper. We found the author collaboration presented in clusters and the whole was relatively weak. The better phenomenon is that increased authors are focusing on injury burden research and the connection between authors of different clusters is strengthening over time.
Journals are an important carrier for delivering the results of academic achievements and disseminating knowledge. In general, few researchers could be fully aware of all relevant journals in their research fields, and many are struggling to identify the appropriate journals for their research.18 The journal co-citation network map could help identify the most relevant journals in a field. This study found that most of the top 10 journals with the most outputs belonged to Q1 or Q2. The IFs of other journals were relatively low except for the lancet, indicating that the research quality in the field of injury burden needs to be improved. The journal co-citation network map showed that core journals were mainly top journals such as the Lancet, JAMA, and the New England Journal of Medicine, or journals with high annual publication volumes like PLoS One. Research related to injury burden published in these journals may have a great potential to be cited and noticed. A bibliographic coupling map of journals is useful to dig out the emerging potential journals in this field, such as Lancet public health, Frontiers in public health, and Journal of clinical medicine. In addition, the literature published in these journals also deserves special attention to obtain the latest progress in this field and to grasp future research directions.
Main Research Domains and Future Trends on Injury Burden
Keywords represent the topic and core content of a paper. The co-occurrence relationship and the AAY of keywords are important indicators to reflect the hot topics and development trends of a research field. Based on keyword co-occurrence analysis, injury burden research could be divided into five aspects: injury epidemiology and prevention, GBD-related studies, risk factors for injury, clinical management of injury, and injury outcome assessment and economic burden. Injury is a leading cause of morbidity and mortality worldwide, and injury events are in a wide range of ways, from collective and personal events to everyday injury experiences. Realizing the urgency, many countries around the world have begun to conduct injury-related research to understand injury epidemiology.38–42 The injury mechanisms mainly focused on falls, road traffic incidents, and violence.43 Exploring epidemiological characteristics of injuries is fundamental to better understanding the distribution of time, region, and population and potential influencing factors. This would facilitate improving strategies for investigation, monitoring, prevention, and control of the injury. For example, the Government of India developed a pan-India network of injury care facilities based on epidemiological data to provide immediate treatment for accident victims and address the increasing burden driven by road traffic injuries.15 Despite the growing richness of epidemiological data on injury in different nations, injury prevalence varied widely among countries. Fortunately, the GBD study has provided a comprehensive assessment of incidence, mortality, and disability for all major diseases and injuries using standardized methods since the 1990s. As shown in the keyword co-occurrence map, GBD-related studies were grouped as one of the main clusters, which suggested that GBD-related studies were still one of the main sources of data for understanding the injury burden. However, several important research questions, such as long-term health impacts, healthcare utilization, and costs, generally could not be answered by modeling estimates since GBD estimates are modeled based on real-world data. Therefore, it is essential to find out real-world data or real-world evidence to fill these gaps.
The true consequences of injury go beyond the dynamics of the occurrence or fatality and are better reflected in measures of disease burden. Because injury effects could be manifested as not only the changes in body integrity caused by external factors directly acting on the body but also the acute or chronic effects caused by the injury response. Many studies have demonstrated the association between injury and acute kidney injury, cardiovascular disease, diabetes, dementia, post-traumatic stress disorder, and other diseases.6,44–47 Thus, scholars called for considering injury as a systemic disease.48 Research on the short- and long-term health effects, potential influencing factors, and mechanisms of injury is increasingly necessary for better injury management. It has been shown that a variety of factors can affect the injury and prognosis of injury, such as smoking, alcohol consumption, obesity, and comorbidity.49–54 With the progress of medical technology and biotechnology, research related to the pathophysiology of injury has also begun to emerge, and the role of biomarkers has been highlighted to carry out more precise treatment, so as to precisely reduce the burden of injury.55,56 Moreover, as a significant public health problem that affects multiple outcome domains, injury imposes a significant economic burden on individuals, families, and society. The estimated economic cost of injury only in the USA in 2019 was as high as 4.2 trillion dollars, including 327 billion dollars in medical expenses, 69 billion dollars in work loss, and 3.8 trillion dollars in lost statistical value of life and quality of life.57
The keyword timeline chart and overlay keyword co-occurrence map reflect changes in research topics. The results showed that inflammatory, oxidative emergencies and biomarkers began to emerge and became the forefront of the injury burden field. Meanwhile, the investigation of the relationship between injury and health outcomes has intensified to promote injury prevention and management, and the main research design has gradually shifted to cohort studies. It is worth mentioning that differences in different economic levels countries and genders are also beginning to be noted.
Based on the above research focus and relevant literature, we anticipated several hot topics in injury burden research: Large observational study about injury in real-world; Injury epidemiology and burden in different injury types or populations; The pathophysiological mechanism of injury disease cluster; Injury-related research in low- and middle-income countries; Prognosis diagnosis and risk prediction of injury. Furthermore, the methods assessing the injury burden could be summarized into five phases: first, the definition of injury and injury exposure measurement; second, the construction of quantitative relationship models between injury and health outcomes; third, the identification of macro and micro risk factors for poor prognosis of injury; fourth, evaluation of economic burden based on visits/hospitalization; and fifth, conduction predictive and early warning studies on injury burden to improve injury burden in all aspects. In brief, the development trend of injury burden research has the following characteristics: (1) Wider: spatial globalization and developing countries are gradually joining in; (2) More detailed: the influencing factors develop to the micro level, from the sociodemographic level to molecular level; (3) Injury classification focuses more on subgroups; (4) Longer: paying more attention to long-term effects; (5) Full spectrum: considering injury as a systemic disease to explore broader health effects; (6) Interdisciplinary: integrating information technology, biotechnology, etc.
Strength and Limitations
This study provided a comprehensive and systematic summary of the overall overview of the field of injury burden research from 1998–2022 using a bibliometric approach, which had the advantage of covering a larger period and had richer results than previous narrative-only or systematic reviews. Then, our study also had some shortcomings. The first was that only one database, WoSCC, was searched in this study, and the information collected was limited, which may cause some bias. However, it should be noted that WoSCC was the most used database in bibliometric analysis, and the data from WoSCC could represent the status of most publications in a certain field to a certain extent. Secondly, there were intrinsic differences between the results of bibliometric analysis and real-world studies. For instance, some comparatively new publications of high quality may not attach sufficient attention due to lower citation frequency, whilst older articles tended to accumulate more citations. Third, some factors, such as the influence of certain time factors, and the database continuously updating studies, may bring about the gap existing between actual research conditions and bibliometric analysis results. Finally, whether the increasing trend in publications depicts increasing injury incidence or increased public health awareness might require further analysis.
Conclusion
This study analyzed articles published between 1998–2022 to help researchers gain a comprehensive understanding of research related to injury burden. The study found that research showed a steady growth trend and was likely to continue to increase consistently in the future. High-income countries played an important role in injury burden research, particularly the USA. The University of Washington was the most influential institution in the field. Vos T was the most contributing scholar in the field. Lancet was recognized as a high-quality journal for scholars in the field. Injury burden was more likely to focus on injury epidemiology and prevention, GBD-related studies, risk factors for injury, clinical management of injury, and injury outcome assessment and economic burden. In addition, the collaboration between different countries, institutions, and authors should be enhanced.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Consent for Publication
All authors have consented to the publication of this research.
Acknowledgments
Thanks for the National Key R&D Program of China (2021YFC260050401).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Key R&D Program of China (2021YFC260050401).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fodor K, Unterhitzenberger J, Chou C, et al. Is traumatic stress research global? A bibliometric analysis. Eur J Psychotraumatol. 2014;5(1). doi:10.3402/ejpt.v5.23269
2. Fomete B, Adebayo ET, Agbara R, Osunde DO, Abah ER. Pattern of Ocular Involvement in Midface Injuries Seen at a Tertiary Care Hospital in Northern Nigeria. Nigerian J Surgery. 2021;27(1):33–37. doi:10.4103/njs.NJS_21_20
3. Qi J, Xie Q, Li Z, Sun C. A Nomogram to Better Predict the In-Hospital Mortality of Trauma Patients with Sepsis in the Intensive Care Unit. Int J Clin Pract. 2022;2022:4134138. doi:10.1155/2022/4134138
4. Karcutskie C, Meizoso J, Ray J, et al. Association of Mechanism of Injury With Risk for Venous Thromboembolism After Trauma. JAMA Surg. 2017;152(1):35–40. doi:10.1001/jamasurg.2016.3116
5. Harrois A, Soyer B, Gauss T, et al. Prevalence and risk factors for acute kidney injury among trauma patients: a multicenter cohort study. Critical Care. 2018:22. doi:10.1186/s13054-018-2265-9
6. Sovik S, Isachsen M, Nordhuus K, et al. Acute kidney injury in trauma patients admitted to the ICU: a systematic review and meta-analysis. Intensive Care Med. 2019;45(4):407–419. doi:10.1007/s00134-019-05535-y
7. Brier Z, Connor J, Legrand A, Price M. Different trajectories of PTSD symptoms during the acute post-trauma period. J Psychiatr Res. 2020;131:127–131. doi:10.1016/j.jpsychires.2020.08.037
8. Leng Y, Byers A, Barnes D, Peltz C, Li Y, Yaffe K. Traumatic Brain Injury and Incidence Risk of Sleep Disorders in Nearly 200,000 US Veterans. Neurology. 2021;96(13):E1792–E1799. doi:10.1212/WNL.0000000000011656
9. Busse JW, Bhandari M, Guyatt GH, et al. Development and Validation of an Instrument to Predict Functional Recovery in Tibial Fracture Patients: the Somatic Pre-Occupation and Coping (SPOC) Questionnaire. J Orthop Trauma. 2012;26(6):370–378. doi:10.1097/BOT.0b013e31822421e2
10. Crowe C, Massenburg B, Morrison S, et al. Global trends of hand and wrist trauma: a systematic analysis of fracture and digit amputation using the Global Burden of Disease 2017 Study. Injury Prevention. 2020;26(SUPP_1):115–124. doi:10.1136/injuryprev-2019-043495
11. Kokol P. Meta approaches in knowledge synthesis in nursing: a bibliometric analysis. Nurs Outlook. 2021;69(5):815–825. doi:10.1016/j.outlook.2021.02.006
12. Brandt J, Hadaya O, Schuster M, Rosen T, Sauer M, Ananth C. A Bibliometric Analysis of Top-Cited Journal Articles in Obstetrics and Gynecology. JAMA Network Open. 2019;2(12). doi:10.1001/jamanetworkopen.2019.18007
13. Li X, Xiang P, Liang J, Deng Y, Du J. Global Trends and Hotspots in Esketamine Research: a Bibliometric Analysis of Past and Estimation of Future Trends. Drug Design Dev Therapy. 2022;16:1131–1142. doi:10.2147/DDDT.S356284
14. Zeng J, Xu C, Xu G, et al. The Global Status of Research in Ankle Fracture: a Bibliometric and Visualized Study. Front Surgery. 2022:9. doi:10.3389/fsurg.2022.853101
15. Sharma N, Bairwa M, Gowthamghosh B, Gupta S, Mangal D. A bibliometric analysis of the published road traffic injuries research in India, post-1990. Health Res Policy Systems. 2018;16. doi:10.1186/s12961-018-0298-9
16. Akova F, Koyuncu Z, Erol E, et al. Child Abuse as an Example of Coexistence of Emotional and Physical Trauma Among Children: an Academic Overview With Altmetric Perspective. Cureus J Med Sci. 2022;14(3). doi:10.7759/cureus.23347
17. Rana I. Disaster and climate change resilience: a bibliometric analysis. Int J Disaster Risk Reduction. 2020;50. doi:10.1016/j.ijdrr.2020.101839
18. Cheng K, Guo Q, Yang W, Wang Y, Sun Z, Wu H. Mapping Knowledge Landscapes and Emerging Trends of the Links Between Bone Metabolism and Diabetes Mellitus: a Bibliometric Analysis From 2000 to 2021. Front Public Health. 2022;10. doi:10.3389/fpubh.2022.918483
19. World Bank. World Bank country and lending groups; 2021. Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups.
20. Guo Y, Hao Z, Zhao S, Gong J, Yang F. Artificial Intelligence in Health Care: bibliometric Analysis. J Med Internet Res. 2020;22(7). doi:10.2196/18228
21. van Eck N, Waltman L. Software survey: vOSviewer, a computer program for bibliometric mapping. Scientometrics. 2010;84(2):523–538. doi:10.1007/s11192-009-0146-3
22. van Eck NJ, Waltman L. VOSviewer Manual. Leiden: Univeristeit Leiden; 2013.
23. Chen C. CiteSpace II: detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Information Sci Technol. 2006;57(3):359–377. doi:10.1002/asi.20317
24. Huang L, Xu G, He J, et al. Bibliometric Analysis of Functional Magnetic Resonance Imaging Studies on Acupuncture Analgesia Over the Past 20 Years. J Pain Res. 2021;14:3773–3789. doi:10.2147/JPR.S340961
25. World Health Organization. The global burden of disease: 2004 update; 2004. Available from:https://www.who.int/publications/i/item/9789241563710.
26. Murray C, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2197–2223. doi:10.1016/S0140-6736(12)61689-4
27. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
28. Peng C, He M, Cutrona S, Kiefe C, Liu F, Wang Z. Theme Trends and Knowledge Structure on Mobile Health Apps: bibliometric Analysis. JMIR Mhealth and Uhealth. 2020;8(7). doi:10.2196/18212
29. Waldron E, Howard K, Reinecke M. The Long-Term Effect of Trauma History on Adolescent Depression Treatment. Psychol Trauma Theory Res Practice Policy. 2019;11(7):751–759. doi:10.1037/tra0000457
30. Mitchell R, McClure R. The development of national injury prevention policy in the Australian health sector: and the unmet challenges of participation and implementation. Aust N Zealand Health Policy. 2006;3:11. doi:10.1186/1743-8462-3-11
31. Baldwin G, Sleet D, Gilchrist J, Degutis L. Fulfilling a promise: the national action plan for child injury prevention. Injury Prevention. 2012;18(3):207. doi:10.1136/injuryprev-2012-040402
32. Nafade V, Nash M, Huddart S, et al. A bibliometric analysis of tuberculosis research, 2007-2016. PLoS One. 2018;13(6). doi:10.1371/journal.pone.0199706
33. Zhao L, Cao B, Borghi E, et al. Data gaps towards health development goals, 47 low- and middle-income countries. Bull World Health Organ. 2022;100(1):40–49. doi:10.2471/BLT.21.286254
34. Liu P, Guo Y, Qian X, Tang S, Li Z, Chen L. China’s distinctive engagement in global health. Lancet. 2014;384(9945):793–804. doi:10.1016/S0140-6736(14)60725-X
35. Zhou J, Wang T, Belenkiy I, et al. Management of severe trauma worldwide: implementation of trauma systems in emerging countries: China, Russia and South Africa. Critical Care. 2021;25(1). doi:10.1186/s13054-021-03681-8
36. Wu H, Cheng K, Tong L, Wang Y, Yang W, Sun Z. Knowledge structure and emerging trends on osteonecrosis of the femoral head: a bibliometric and visualized study. J Orthopaedic Surgery Res. 2022;17(1). doi:10.1186/s13018-022-03068-7
37. Gao J, Xing D, Dong S, Lin J. The primary total knee arthroplasty: a global analysis. J Orthopaedic Surgery Res. 2020;15(1). doi:10.1186/s13018-020-01707-5
38. Polinder S, Haagsma J, Toet H, van Beeck E. Epidemiological burden of minor, major and fatal trauma in a national injury pyramid. Br J Surgery. 2012;99:114–121. doi:10.1002/bjs.7708
39. Zuraik C, Sampalis J. Epidemiology of Traumatic Injuries at an Urban Hospital in Port-au-Prince, Haiti. World J Surg. 2017;41(11):2674–2680. doi:10.1007/s00268-017-4088-2
40. Chua M, Pan D, Lee M, et al. Epidemiology and outcomes of older trauma patients in Singapore: a multicentre study. Injury Int J Care Injured. 2022;53(10):3149–3155. doi:10.1016/j.injury.2022.08.018
41. Al-Hajj S, Chahrour M, Nasrallah A, Hamed L, Pike I. Physical trauma and injury: a multi-center study comparing local residents and refugees in Lebanon. J Glob Health. 2021;11. doi:10.7189/jogh.11.17001
42. Azami-Aghdash S, Sadeghi-Bazargani H, Shabaninejad H, Abolghasem Gorji H. Injury epidemiology in Iran: a systematic review. J Inj Violence Res. 2017;9(1). doi:10.5249/jivr.v9i1.852
43. Abbafati C, Abbas K, Abbasi M, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222.
44. Davidson G, Hamlat C, Rivara F, Koepsell T, Jurkovich G, Arbabi S. Long-term Survival of Adult Trauma Patients. J Am Med Assoc. 2011;305(10):1001–1007. doi:10.1001/jama.2011.259
45. Duke JM, Randall SM, Fear MW, Boyd JH, Rea S, Wood FM. Diabetes mellitus after injury in burn and non-burned patients: a population based retrospective cohort study. BURNS. 2018;44(3):566–572. doi:10.1016/j.burns.2017.10.019
46. Barnes D, Byers A, Gardner R, Seal K, Boscardin W, Yaffe K. Association of Mild Traumatic Brain Injury With and Without Loss of Consciousness With Dementia in US Military Veterans. JAMA Neurol. 2018;75(9):1055–1061. doi:10.1001/jamaneurol.2018.0815
47. Gillikin C, Habib L, Evces M, Bradley B, Ressler K, Sanders J. Trauma exposure and PTSD symptoms associate with violence in inner city civilians. J Psychiatr Res. 2016;83:1–7. doi:10.1016/j.jpsychires.2016.07.027
48. D’Huyvetter C. The trauma disease. J Trauma Nurs. 2000;7(1):5–12. doi:10.1097/00043860-200001000-00002
49. Du J, Weinberg D, Moore T, Vallier H. Smoking Is Associated With Longer Intensive Care Unit Stays in Spine Trauma Patients. J Orthop Trauma. 2020;34(7):E250–E255. doi:10.1097/BOT.0000000000001739
50. Resnick S, Inaba K, Okoye O, et al. Impact of smoking on trauma patients. Ulusal Travma Ve Acil Cerrahi Dergisi-Turkish J Trauma Em Surgery. 2014;20(4):248–252. doi:10.5505/tjtes.2014.21737
51. Connor J, Casswell S. The burden of road trauma due to other people’s drinking. Accident Analysis Prevention. 2009;41(5):1099–1103. doi:10.1016/j.aap.2009.06.019
52. Brahmbhatt T, Hernon M, Siegert C, Plauche L, Young L, Burke P. Trauma and BMI Mortality. Curr Obes Rep. 2017;6(2):211–216. doi:10.1007/s13679-017-0264-9
53. Wardle T. Co-morbid factors in trauma patients. Br Med Bull. 1999;55(4):744–756. doi:10.1258/0007142991902754
54. Brattstrom O, Larsson E, Granath F, Riddez L, Bell M, Oldner A. Time dependent influence of host factors on outcome after trauma. Eur J Epidemiol. 2012;27(3):233–241. doi:10.1007/s10654-012-9651-4
55. Minami S, Doi T, Abe T, Takeuchi I. Neutrophil gelatinase-associated lipocalin as a biomarker for short-term outcomes among trauma patients: a single-center observational study. PLoS One. 2021;16(5). doi:10.1371/journal.pone.0251319
56. Satyam A, Andreo K, Lapchak P, et al. Complement Deposition on the Surface of RBC After Trauma Serves a Biomarker of Moderate Trauma Severity: a Prospective Study. Shock. 2020;53(1):16–23. doi:10.1097/SHK.0000000000001348
57. Peterson C, Miller G, Bartlett S, Florence C. Economic Cost of Injury - United States, 2019. Morbidity Mortality Weekly Rep. 2021;70(48):1655–1659.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.