Back to Journals » Infection and Drug Resistance » Volume 19
Temporal Disease Sequence and Prognostic Outcomes in Patients with Coexisting Lung Cancer and Tuberculosis: A 123-Patient Retrospective Cohort Study
Authors Yu W ![]() , Xie H, Ye B, Lv W, Yu G
, Xie H, Ye B, Lv W, Yu G ![]() , Zhong F, Chen F
, Zhong F, Chen F ![]() , Rao Y, Hu J
, Rao Y, Hu J ![]()
Received 29 October 2025
Accepted for publication 27 January 2026
Published 2 February 2026 Volume 2026:19 576692
DOI https://doi.org/10.2147/IDR.S576692
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Wenfeng Yu,1,2,* Haoran Xie,3,* Bo Ye,3 Wang Lv,1 Guocan Yu,2 Fangming Zhong,2 Fang Chen,2 Yueli Rao,4 Jian Hu1
1Department of Thoracic Surgery, The First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, Zhejiang, People’s Republic of China; 2Zhejiang Tuberculosis Diagnosis and Treatment Center, Hangzhou Red Cross Hospital, Hangzhou, Zhejiang, People’s Republic of China; 3Department of Thoracic Surgery, The Affiliated Hospital of Hangzhou Normal University, Hangzhou, Zhejiang, People’s Republic of China; 4Department of Blood Transfusion, The 903rd Hospital of PLA, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian Hu, Email [email protected]
Background: The concurrent presentation of pulmonary tuberculosis (TB) and lung cancer presents significant diagnostic and therapeutic challenges, with limited evidence guiding clinical management. To address this, we introduced a novel temporal disease-sequence classification. This study aimed to characterize clinical phenotypes and prognostic factors based on this sequence.
Methods: We conducted a retrospective cohort study of 123 patients with confirmed TB and lung cancer at our center (2017– 2023). Patients were classified by diagnostic sequence: Simultaneous Coexistence (TB-LC, n=70), Post-TB Lung Cancer (TB→LC, n=35), and Post-LC TB (LC→TB, n=18). Outcomes included demographics, symptom profiles, treatment patterns, and overall survival (OS). Statistical analyses employed Kaplan-Meier methods and Cox regression.
Results: Striking intergroup differences were observed. The TB-LC group showed the highest symptom burden (87.14, P=0.007) and chemotherapy utilization (50.00%, P=0.029). OS did not differ significantly (log-rank P=0.276), though median survival varied (TB-LC: 32 months; LC→TB: 57 months; TB→LC: not reached). Multivariable analysis identified surgery (HR=0.34, 95% CI 0.13– 0.92) and anti-TB therapy (HR=0.48, 95% CI 0.24– 0.97) as protective factors, while advanced stage predicted mortality (HR=6.24, 95% CI 2.27– 17.14).
Conclusion: Temporal disease sequence influences clinical presentation and treatment selection in TB-lung cancer patients. Surgical resection and anti-TB strategies improve outcomes, highlighting the need for integrated management protocols.
Keywords: lung cancer, tuberculosis, outcomes, temporal disease sequence
Introduction
Lung cancer and tuberculosis (TB) constitute two of the most prevalent and lethal pulmonary diseases worldwide, exhibiting elevated incidence and mortality rates.1,2 The disease burden of TB and lung cancer is disproportionately concentrated in regions with lower Socio-Demographic Index (SDI) scores.3 Collectively, China and India account for 47% of global TB-associated malignancies.3 Epidemiological evidence demonstrates that individuals with a prior TB diagnosis have a threefold elevated risk of subsequent lung cancer, potentially attributable to chronic inflammation, pulmonary fibrosis, and immune dysregulation.4 Conversely, lung cancer and its therapeutic modalities—including radiotherapy, chemotherapy, targeted therapy, and immunotherapy—may impair cellular immune function, thereby compromising host defense against Mycobacterium tuberculosis.5 Additionally, lung cancer patients often present with multiple predisposing factors, such as advanced age, smoking history, chronic pulmonary comorbidities, diabetes mellitus, and malnutrition, which collectively heighten TB susceptibility.6,7 Clinical and epidemiological data indicate that lung cancer patients face a sixfold greater TB risk relative to the general population.8,9 The co-occurrence of TB and lung cancer encompasses both synchronous and metachronous manifestations, with bidirectional pathogenic interactions that complicate diagnosis and management. In recent years, this issue has garnered increasing attention within academic circles. It is worth emphasising that clinical practice and epidemiological evidence suggest that different temporal sequences and causal relationship patterns may exist between lung cancer and tuberculosis.10
Despite increasing recognition of the co-occurrence of tuberculosis and lung cancer, prior research has predominantly concentrated on epidemiological associations and risk factor enumeration, leaving critical gaps in clinical stratification and management guidance. Evidence indicates that survival outcomes are superior when the interval between TB and lung cancer diagnoses exceeds six months, suggesting a potential prognostic impact of temporal sequence.11 A standardized framework to classify this sequence is lacking. To bridge this gap, we recently established a three-category classification system: (1) Simultaneous Coexistence (TB-LC), defined as concurrent diagnosis of both conditions within a six-month window; (2) Post-Tuberculosis Lung Cancer (TB→LC), referring to lung cancer developing against a backdrop of prior TB sequelae; and (3) Post-Lung Cancer Tuberculosis (LC→TB), denoting active TB occurring during or following lung cancer treatment. The association of this framework with distinct imaging phenotypes, baseline clinical characteristics, or treatment distribution patterns remains uninvestigated.
To elucidate the clinical relevance of this classification system, we retrospectively analyzed clinical data from 123 patients with pathologically confirmed lung cancer and microbiologically or histologically confirmed pulmonary tuberculosis at our center. The study objectives were as follows: (1) to classify patients according to the proposed temporal causal mo (2) to compare baseline data, clinical characteristics, and treatment regimens across phenotypes; and (3) to identify prognostic factors. This analysis aims to guide the development of phenotype-specific management strategies and establish a reference for future prospective cohort studies.
Method
Study Design and Participants
We conducted a retrospective cohort study at a single tertiary care center in China to evaluate survival outcomes and identify prognostic factors among patients with concurrent or sequential tuberculosis (TB) and lung cancer. The study included patients hospitalized between December 2017 and December 2023. Patients were eligible if they met all of the following criteria: (1) age ≥18 years; (2) a pathologically confirmed diagnosis of lung cancer and a microbiologically or clinically confirmed diagnosis of pulmonary TB, consistent with the Chinese WS 288–2017 diagnostic criteria; (3) a clearly documented temporal sequence between the two diagnoses; and (4) availability of complete clinical data covering diagnosis, treatment, and follow-up (including at least 1 year of follow-up or documented survival status at the last contact). Exclusion criteria were: (1) a concurrent diagnosis of other active malignancies or hematologic cancers, or (2) incomplete medical records or loss to follow-up without definitive survival status documentation.
Based on the temporal relationship, patients were categorized into three predefined groups: (1) Simultaneous Coexistence (TB-LC), defined as the diagnosis of both conditions within a six-month window; (2) Post-Tuberculosis Lung Cancer (TB→LC), referring to lung cancer diagnosed in a patient with a history of prior TB sequelae; and (3) Post-Lung Cancer Tuberculosis (LC→TB), denoting active TB diagnosed during or after the completion of lung cancer treatment.
Diagnostic Criteria
The diagnosis of lung cancer was histologically confirmed via specimens obtained from bronchoscopy biopsy, CT-guided needle biopsy, surgical resection, or cytology. Histological subtypes included adenocarcinoma, squamous cell carcinoma, and others. The diagnosis of pulmonary tuberculosis was established in accordance with the Chinese WS 288–2017 criteria. Confirmatory diagnosis was preferentially based on microbiological evidence (positive culture, PCR, or nucleic acid test for Mycobacterium tuberculosis from sputum, bronchoalveolar lavage fluid, or tissue) or pathological evidence (identification of granulomas with caseous necrosis on biopsy). In the absence of confirmatory tests, a clinical diagnosis was made based on a combination of typical chest imaging findings (eg, upper-lobe cavities, miliary nodules) along with compatible chronic symptoms and a documented response to anti-tuberculosis therapy.
Data Collection
Data were abstracted from electronic medical records and supplemented by structured telephone follow-up. The following variables were collected: (1) Demographics: Age, sex, smoking history, alcohol use, height, weight; (2) Comorbidities: Pre-existing chronic diseases (eg, diabetes, Hypertension); (3) TB Characteristics: Number of lesions, involved lung lobes, treatment history (eg, prior anti-TB therapy), imaging features; (4) Lung Cancer Characteristics: Primary site, histological subtype, TNM stage (8th edition AJCC criteria), treatment modalities (surgery, radiotherapy, chemotherapy, immunotherapy); (5) Temporal Sequence: Diagnostic order of TB and lung cancer (as defined above); (6) Survival Outcomes: Vital status (alive/dead) and date of last follow-up or death.
Statistical Analysis
All statistical analyses were performed using R software (version 4.2.0; R Foundation) with the survival package. Continuous variables are presented as mean ± SD or median (IQR), and were compared using t-tests/Mann–Whitney U-tests (two groups) or ANOVA/Kruskal–Wallis tests (three groups), as appropriate. Categorical variables are expressed as numbers (percentages) and compared using the Chi-square or Fisher’s exact test. Survival curves were generated by the Kaplan-Meier method and compared with the Log rank test. Prognostic factors were identified using Cox proportional hazards regression. Variables with P < 0.10 in univariable analysis were entered into a backward stepwise multivariable model (retention criterion: P < 0.05). The proportional hazards assumption was checked with Schoenfeld residuals. A two-sided P < 0.05 defined statistical significance.
Results
Patient Inclusion Process
This retrospective study included 123 patients diagnosed with concurrent pulmonary tuberculosis and lung cancer between December 2017 and December 2023. Participants were stratified into three groups based on diagnostic sequence: Simultaneous Coexistence Group (TB-LC, n=70), Post-Tuberculosis Lung Cancer Group (TB→LC, n=35), and Post-Lung Cancer Tuberculosis Group (LC→TB, n=18), as illustrated in Figure 1.
 |
Figure 1 Study the flowchart of patients with tuberculosis and lung cancer. |
Baseline Characteristics
Table 1 presents the demographic and clinical characteristics across study groups. The overall cohort had a median age of 64 years (IQR 56.00–69.00), with the TB-LC group demonstrating a comparable median age of 63.50 years (IQR 55.00–68.00; P=0.374 for intergroup comparison). Male predominance was observed across all groups (TB-LC: 75.71%; TB→LC: 62.86%; LC→TB: 77.78%; P=0.327). No statistically significant differences were detected in smoking, alcohol consumption, body mass index (BMI), or hypertension, diabetes mellitus, or chronic pulmonary disease (COPD) among the groups (all P>0.05).
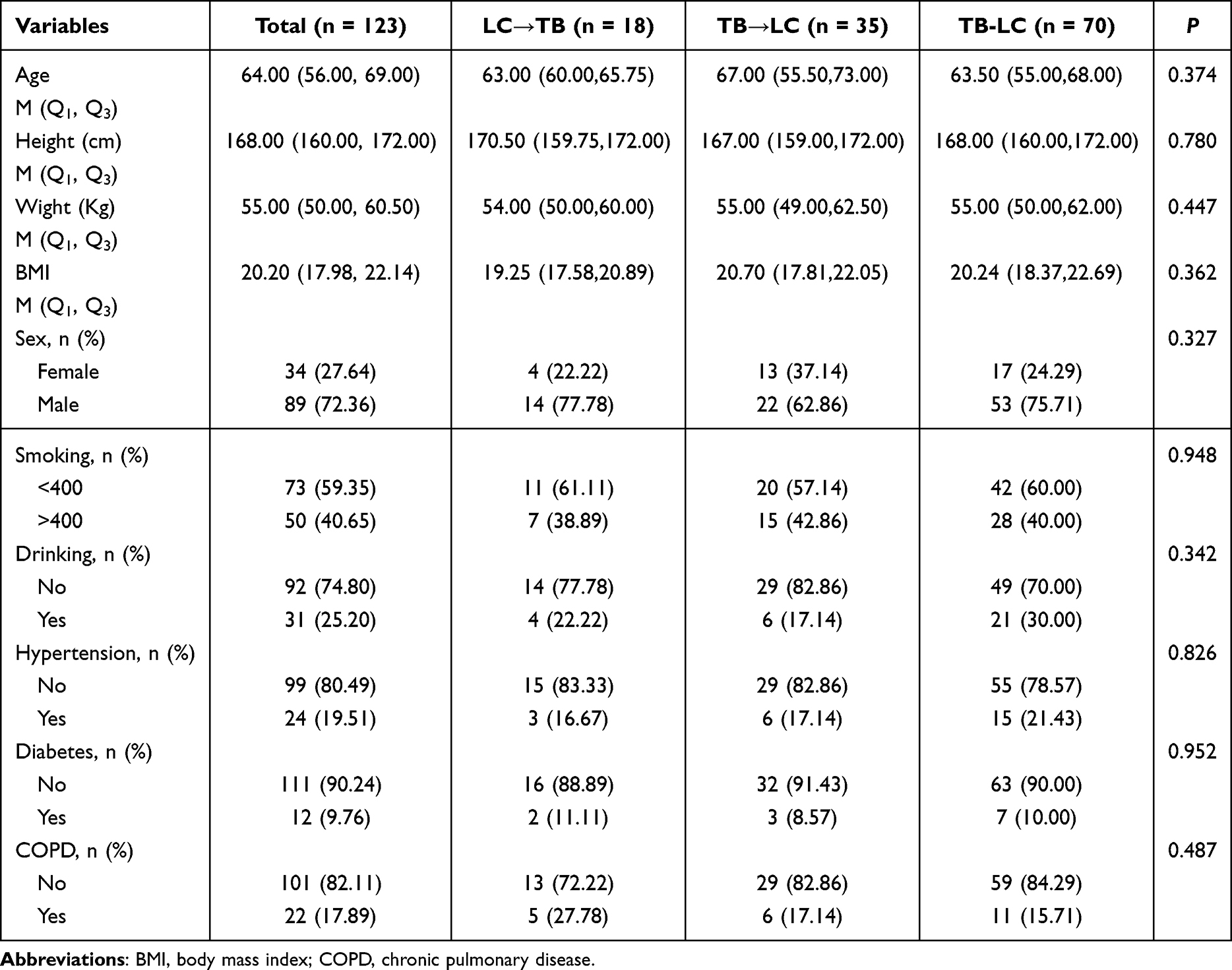 |
Table 1 Baseline Characteristics of the Study Population |
Clinical Characteristics and Therapeutic Approaches
Table 2 demonstrates that symptomatic presentation was most frequent in the TB-LC group (87.14%), followed by LC→TB (77.78%) and TB→LC (60.00%) groups (P=0.007). The most common symptoms were cough (37.40%) and hemoptysis (14.63%). Table 3 reveals the histopathological and staging distribution: adenocarcinoma (52.85%), squamous cell carcinoma (40.65%), stage I (34.96%), stage II (27.64%), stage III (21.14%), and stage IV (16.26%) disease. Radiological evaluation showed >3 tuberculous lesions in 72.36% of cases, with 66.67% exhibiting co-localization in the same pulmonary lobe. No significant differences were observed among groups regarding lesion topography, tumor location, histological subtype, tumor stage, or pleural effusion presence (all P>0.05). Figure 2 outlines the therapeutic landscape, documenting twelve distinct treatment modalities, including operation (41.46%), chemotherapy (17.89%), and chemoradiotherapy. Conservative treatment was elected in 10.57% of cases(Table S1). Table 4 details treatment comparisons: received antitumor therapy rates (LC→TB: 94.44%; TB→LC: 85.71%; TB-LC: 90.00%), surgical rates (LC→TB: 72.22%; TB→LC: 65.71%; TB-LC: 50.00%), and chemotherapy rates (LC→TB: 50.00%; TB-LC: 44.29%; TB→LC: 20.00%; P=0.029). Immunotherapy utilization was minimal (4.07%, n=5/123). Anti-tuberculosis treatment completion rates (88.89%, 77.14%, 74.29%; P=0.420) and median treatment durations (9.00 [IQR 8.00–12.00], 12.00 [8.00–12.00], 9.00 [6.00–12.00] months; P=0.093) showed no significant intergroup differences.
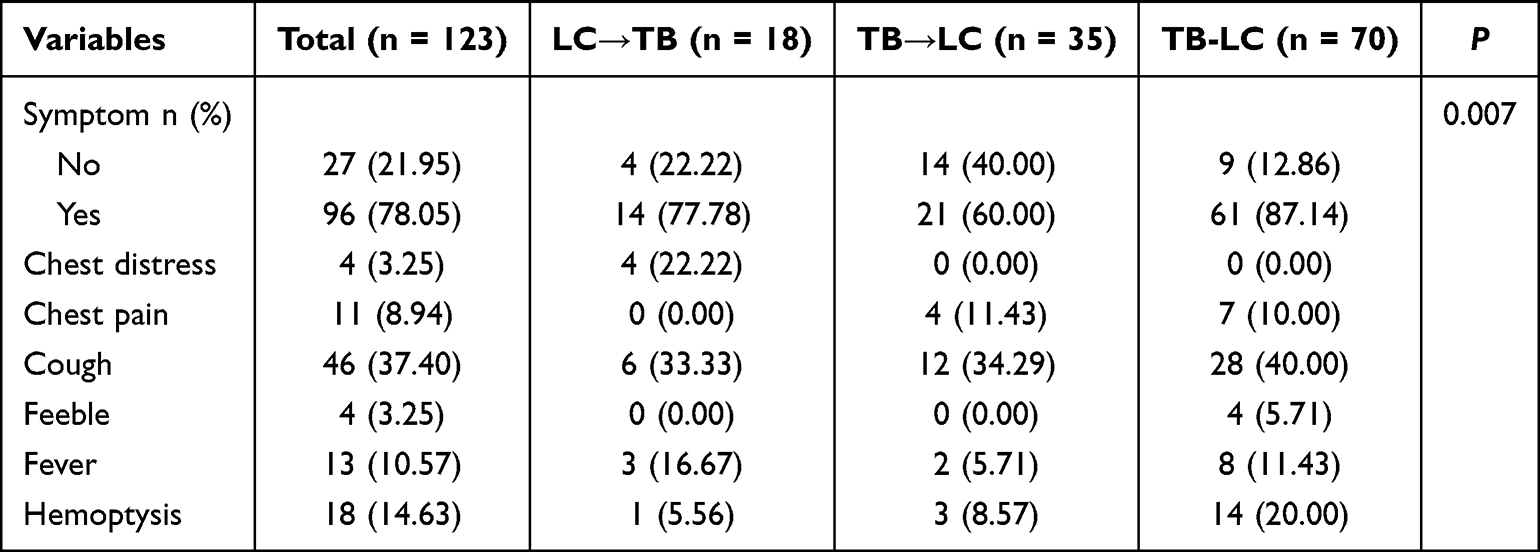 |
Table 2 The Symptoms of the Study Population |
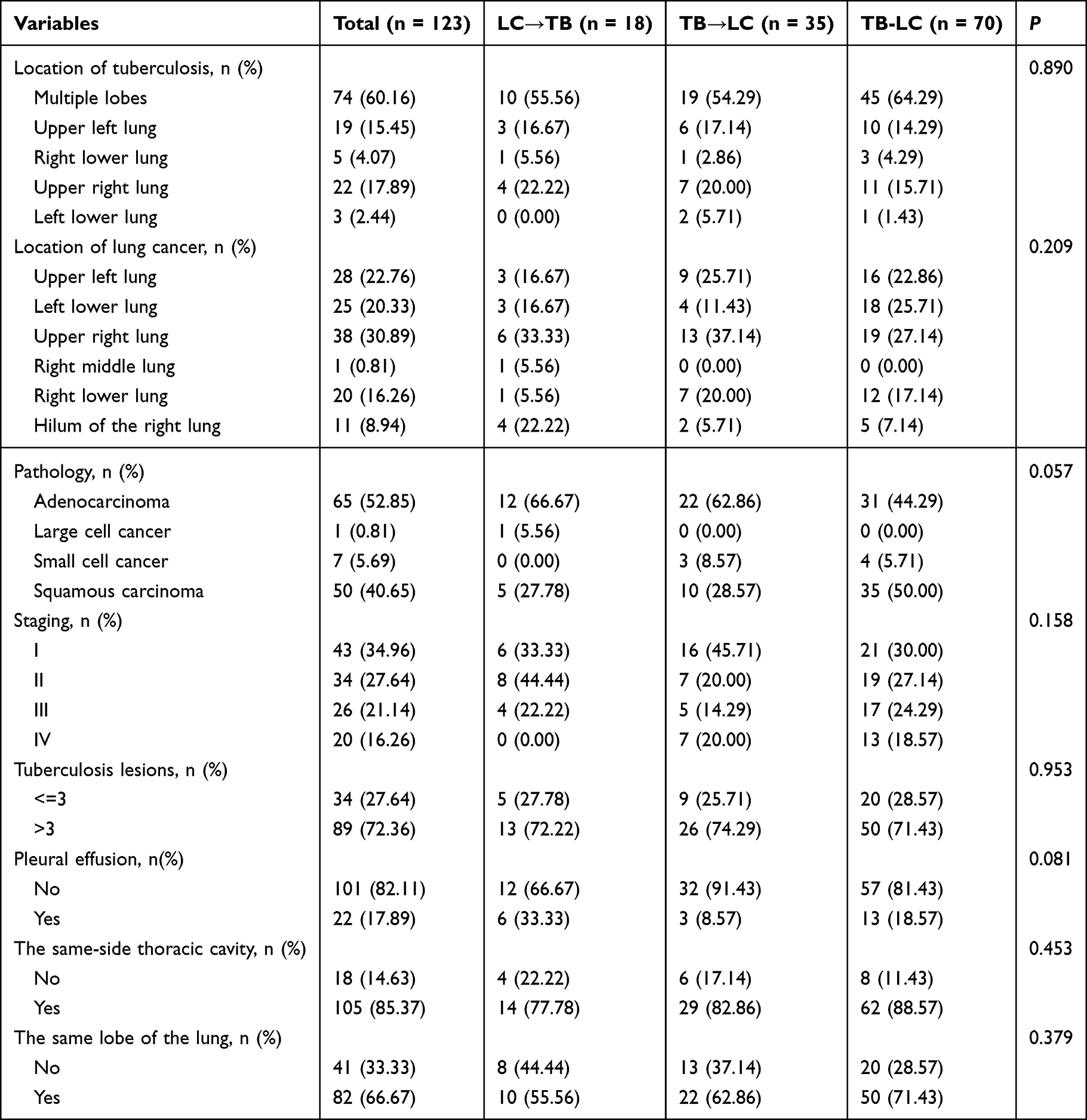 |
Table 3 Clinical Characteristics of the Study Population |
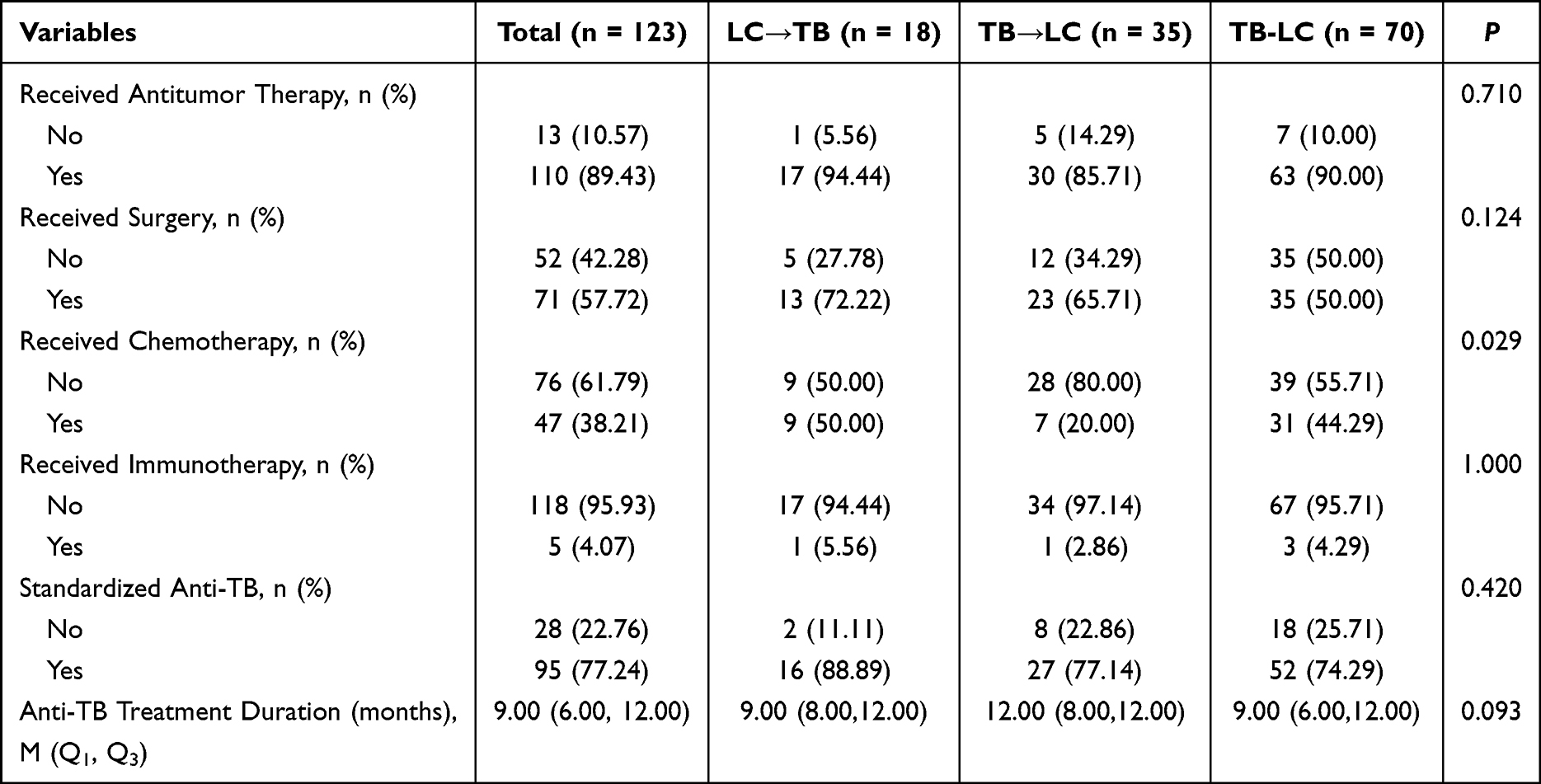 |
Table 4 Anti-TB and Anti-Cancer Therapy Profile |
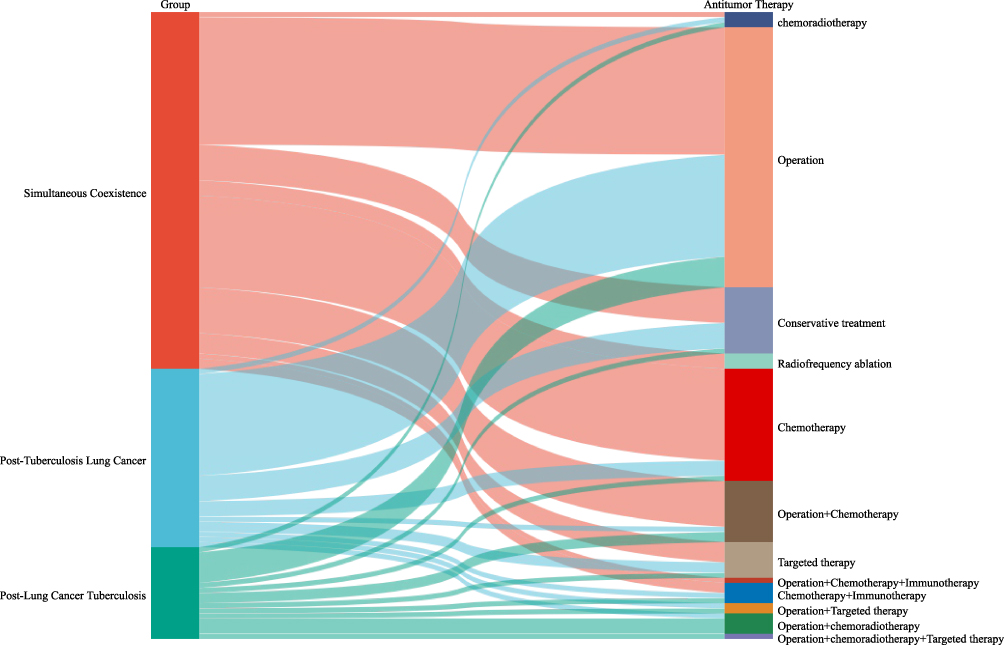 |
Figure 2 The Sangitu chart illustrates the process of the patient’s anti-tumor treatment. The width of the bars represents the number of patients; the colors represent the treatment categories. |
Survival Outcomes
Figure 3 demonstrates comparable overall survival across groups by Kaplan-Meier analysis (log-rank P=0.276). Median survival durations were 32 months (TB-LC), 57 months (LC→TB), and not reached (TB→LC).
 |
Figure 3 Kaplan-Meier curves of OS of the groups. |
Prognostic Determinants
Table 5 presents Cox regression analyses. Multivariable modeling identified surgical intervention (HR=0.34, 95% CI 0.13–0.92; P=0.034) and standardized anti-tuberculosis therapy (HR=0.48, 95% CI 0.24–0.97; P=0.041) as independent protective factors, while advanced tumor stage (III–IV: HR=6.24, 95% CI 2.27–17.14; P<0.001) conferred worse prognosis. Age, sex, BMI, chemotherapy, and anti-tuberculosis duration showed no significant associations.
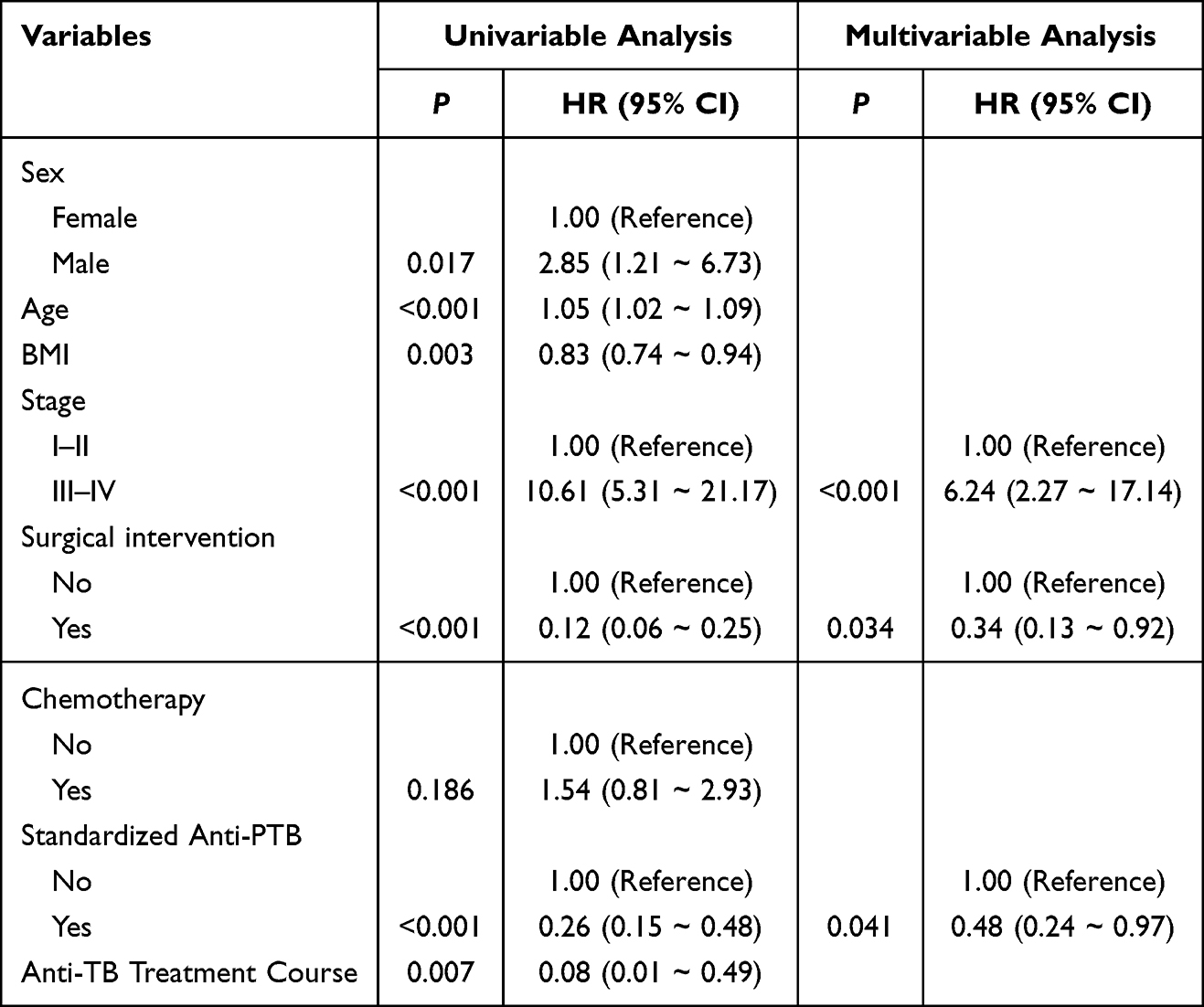 |
Table 5 Predictors of Overall Survival in Patients |
Discussion
This study represents one of the most comprehensive analyses to date of patients with coexisting tuberculosis and lung cancer, examining their clinical characteristics and long-term prognosis through a disease chronological stratification system. The findings reveal heterogeneous manifestations of the two diseases across different temporal sequence groups, providing crucial evidence-based support for formulating clinical management strategies.
Key Findings and Clinical Implications
Cohort analysis indicated that 78.05% of patients presented with clinical symptoms, with cough (37.40%) and haemoptysis (14.63%) being the most prevalent manifestations. These findings align closely with prior studies,12,13 confirming substantial symptom overlap between TB and lung cancer. Compared to patients with TB alone, those with coexisting conditions were more likely to experience irritative cough but less likely to experience night sweats.14,15 Notably, distinct clinical characteristics emerged across diagnostic sequence groups: the concurrent coexistence group (TB-LC) exhibited significantly higher symptom burden (87.14%, P=0.007). This phenomenon may stem from multiple pathophysiological mechanisms: Firstly, the coexistence of active tuberculosis infection and lung cancer may induce a cumulative inflammatory state, thereby exacerbating respiratory symptoms. Secondly, tuberculosis-related inflammation can both mask and amplify cancer-related symptoms.16,17 This finding carries important clinical implications: tuberculosis patients who remain persistently coughing or haemoptising after sputum conversion to smear-negative status following anti-tuberculosis therapy should be vigilant for the possibility of coexisting lung cancer; conversely, when respiratory symptoms worsen during treatment in lung cancer patients, the possibility of coexisting tuberculosis should be considered.
Analysis of Treatment Patterns
Treatment analysis revealed two key findings: 1) High tumour treatment rates were maintained across all three groups (LC→TB group: 94.44%; TB→LC group: 85.71%; TB-LC group: 90.00%). Notably, the TB-LC group achieved a high rate of concurrent treatment for both conditions, fully aligning with current tuberculosis and lung cancer diagnostic and treatment guidelines18 — where anti-tuberculosis therapy should be conducted without delaying lung cancer treatment. For newly diagnosed, untreated, and advanced lung cancer patients, efficacy assessment is recommended one month after initiating anti-tuberculosis therapy. Should tuberculosis be effectively controlled, oncological treatment should commence promptly to improve prognosis.19–21 2) Differentiated treatment plans must be tailored to individual patient circumstances. Within our cohort, 12 distinct tumour treatment patterns were observed. Existing evidence indicates that co-morbid patients present significantly greater treatment challenges than those with lung cancer alone. Increased complication risks, compromised physical condition, and drug interactions may all contribute to treatment failure. Therefore, personalised precision medicine should be implemented alongside standardised treatment protocols.22 Notably, the chemotherapy utilisation rate was markedly higher in the LC→TB subgroup (50.00%, P=0.029), potentially reflecting: first, more advanced tumour staging in this subgroup (despite no significant intergroup differences in staging distribution); next, the higher incidence of tuberculosis during cancer treatment among patients receiving chemotherapy/immunotherapy, consistent with research concluding that chemotherapy-induced immunosuppression increases tuberculosis infection risk.23,24 Given that immunotherapy recipients constituted only 4.07% of this cohort (due to sample size limitations), definitive conclusions could not be drawn. However, prior studies indicate that for lung cancer patients with concurrent latent tuberculosis, immunotherapy is relatively safe and non-inferior in efficacy compared to non-infected individuals. Nevertheless, rigorous tuberculosis screening before treatment is essential, and enhanced monitoring for immune-related adverse events (irAEs) is required in those with active tuberculosis infection.25 Consequently, it is recommended that immune checkpoint inhibitors (ICIs) be incorporated into comprehensive treatment regimens at an appropriate time following effective control of pulmonary tuberculosis.
Survival Outcomes and Prognostic Factors
Survival analysis revealed: although the Log rank test did not detect a statistically significant difference in overall survival (OS) (P=0.276), median survival times exhibited numerical differences across groups (TB-LC group: 32 months; LC→TB group: 57 months; TB→LC group: not reached), suggesting potential biological differences warranting further investigation. This discrepancy between statistical and clinical significance may stem from insufficient statistical power due to sample size limitations, particularly pronounced in the LC→TB subgroup (n=18). This constitutes a key limitation of the present study, necessitating larger sample sizes in future research to yield more reliable conclusions.
Multivariate Analysis Identified Two Modifiable Protective Factors
Surgical resection (HR=0.34, 95% CI 0.13–0.92) and standardised anti-tuberculosis therapy (HR=0.48, 95% CI 0.24–0.97). Their clinical significance includes:
1. Persistence of surgical benefit: After adjusting for tumour stage, the survival advantage conferred by surgery remained significant, indicating that surgically suitable patients may benefit from resection regardless of tuberculosis status. This finding aligns closely with prior studies.26 For patients with smear-positive or severe pulmonary tuberculosis combined with resectable NSCLC, it is recommended to initiate anti-tuberculosis therapy first, followed by surgery once the condition is controlled. If tuberculosis proves difficult to control within a short period, neoadjuvant therapy should be initiated. Lung cancer surgery/neoadjuvant therapy should be conducted within one month of anti-tuberculosis treatment. For patients with smear-negative or focal lesions (eg, tuberculomas) combined with stage I–IIIa NSCLC, surgery may proceed after short-term (2-week) anti-tuberculosis therapy. Conversely, lung cancer patients with old tuberculosis require no additional anti-tuberculosis treatment; surgical planning should be determined directly by lung cancer staging.27
2. Protective effect of anti-tuberculosis therapy: Survival benefits from standardised anti-tuberculosis treatment underscore the importance of tuberculosis control for cancer patient prognosis, fully aligning with existing literature and guideline recommendations.18,28
Conversely, advanced tumour stage (stages III–IV) was confirmed as the strongest negative prognostic factor (HR=6.24, 95% CI 2.27–17.14), consistent with prior lung cancer studies.29 The unique contribution of this study lies in confirming that this negative association remains significant even in the context of tuberculosis infection.
Clinical Implications: The Findings Provide the Following Key Guidance
1. Diagnostic Optimisation: Particularly in endemic regions, diagnostic protocols for patients suspected of TB-lung cancer comorbidity should be refined. The high symptom burden among these cases (87.14%) indicates a need to lower the clinical threshold for comprehensive assessment.
2. Dual Management: Treatment strategies should emphasise a dual approach combining surgical resection with standardised anti-tuberculosis therapy, as both independently improve patient outcomes.
3. Chemotherapy Optimisation: Inter-group disparities in chemotherapy application patterns suggest potential treatment selection bias, which could be mitigated through standardised protocols.
Research Limitations: The Following Limitations Must Be Objectively Acknowledged
1. Inherent limitations in causal inference due to retrospective design and potential selection bias (particularly in treatment allocation).
2. Geographical limitations of single-centre data may affect the generalisability of results across settings with differing tuberculosis prevalence and cancer treatment patterns.
3. Sample size constraints (especially n=18 in the LC→TB subgroup) impacted the power to detect potentially important differences.
4. The low immunotherapy utilisation rate (4.07%) limits the generalisability of findings to current widespread checkpoint inhibitor applications.
5. Missing data on key confounders (including socioeconomic status and treatment adherence details).
Future Research Directions
Based on current findings, the following studies are proposed:
1. Prospective multicentre studies: Validate the universality of this classification system and prognostic model in larger, more heterogeneous populations.
2. Mechanistic exploration: Investigate biological interactions between TB infection and lung cancer progression, with a focus on tumour microenvironment regulatory mechanisms.
3. Clinical trials: Systematically evaluate optimal sequential combinations and integrated strategies for anti-tuberculosis and anti-cancer therapies (including modern immunotherapy regimens).
In summary, this study employs rigorous time-stratified analysis to confirm that disease sequence significantly influences clinical phenotypes and treatment patterns in patients with TB-lung cancer comorbidity. The identification of surgical intervention and standardised anti-tuberculosis treatment as independent protective factors provides scientific rationale for implementing integrated management strategies. Although preliminary and requiring validation, these findings highlight the potential of a time-stratified approach to inform more precise diagnosis and treatment guidelines, especially in regions heavily burdened by both diseases. Although these findings require prospective validation, they offer crucial evidence for evidence-based treatment decisions in this high-risk patient cohort. Future research should focus on elucidating underlying biological mechanisms and optimising combined treatment regimens.
Conclusion
This study proposes and validates a novel temporal-sequence classification model (TB-LC, TB→LC, LC→TB) for patients with coexisting TB and lung cancer. Our findings demonstrate that the diagnostic sequence shapes distinct clinical phenotypes and influences therapeutic decisions. Critically, we identify surgical resection and timely anti-TB therapy as independent, modifiable factors for improving survival, underscoring the imperative for integrated management protocols. As an exploratory study, this work primarily establishes the clinical relevance and utility of the temporal-classification framework. Future prospective, multi-center studies are warranted to confirm its prognostic precision and to guide the development of sequence-specific treatment algorithms in high-burden settings.
Ethics Approval and Consent to Participate
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. This study was approved by the Clinical Research Ethics Committee of the Hangzhou Red Cross Hospital (No. 031-001, 2025) and conducted in accordance with the Declaration of Helsinki (as revised in 2013) and Good Clinical Practice Guidelines. Due to the retrospective nature of the study and without any specific intervention, informed consent has been agreed to be waived. The data were maintained with confidentiality.
Acknowledgments
I would like to thank everyone who contributed to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Zhejiang Provincial Medical and Health Science and Technology Project (2025KY1121). The National Key Research and Development Program of China (2022YFC2407303); Key R&D Program of Zhejiang (2025C01136); Research Center for Lung Tumor Diagnosis and Treatment of Zhejiang Province (JBZX-202007).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA. 2024;74(1):12–12. doi:10.3322/caac.21820
2. Lin CH, Lin CJ, Kuo YW, et al. Tuberculosis mortality: patient characteristics and causes. BMC Infect Dis. 2014;14:5. doi:10.1186/1471-2334-14-5
3. Leung CY, Huang HL, Rahman MM, et al. Cancer incidence attributable to tuberculosis in 2015: global, regional, and national estimates. BMC Cancer. 2020;20(1):412. doi:10.1186/s12885-020-06891-5
4. Yu YH, Liao CC, Hsu WH, et al. Increased lung cancer risk among patients with pulmonary tuberculosis: a population cohort study. J Thorac Oncol. 2011;6(1):32–37. doi:10.1097/JTO.0b013e3181fb4fcc
5. Su S, Ye MF, Cai XT, et al. Assessment of anti-PD-(L)1 for patients with coexisting malignant tumor and tuberculosis classified by active, latent, and obsolete stage. BMC Med. 2021;19(1):322. doi:10.1186/s12916-021-02194-z
6. Liao KM, Shu CC, Liang FW, et al. Risk factors for pulmonary tuberculosis in patients with lung cancer: a retrospective cohort study. J Cancer. 2023;14(4):657–664. doi:10.7150/jca.81616
7. Qin Y, Chen Y, Chen J, Xu K, Xu F, Shi J. The relationship between previous pulmonary tuberculosis and risk of lung cancer in the future. Infect Agent Cancer. 2022;17(1):20. doi:10.1186/s13027-022-00434-2
8. Dobler CC, Cheung K, Nguyen J, Martin A. Risk of tuberculosis in patients with solid cancers and haematological malignancies: a systematic review and meta-analysis. Europ Resp J. 2017;50(2):1700157. doi:10.1183/13993003.00157-2017
9. Suárez I, Fünger SM, Kröger S, Rademacher J, Fätkenheuer G, Rybniker J. The diagnosis and treatment of tuberculosis. Deutsches Arzteblatt Int. 2019;116(43):729–735. doi:10.3238/arztebl.2019.0729
10. Cabrera-Sanchez J, Cuba V, Vega V, Van der Stuyft P, Otero L. Lung cancer occurrence after an episode of tuberculosis: a systematic review and meta-analysis. Eur Respir Rev. 2022;31(165):220025. doi:10.1183/16000617.0025-2022
11. Xiong M, Xie S, Wang Y, et al. The diagnosis interval influences risk factors of mortality in patients with co-existent active tuberculosis and lung cancer: a retrospective study. BMC Pulm Med. 2023;23(1):382. doi:10.1186/s12890-023-02674-3
12. Kontsevaya I, Cabibbe AM, Cirillo DM, et al. Update on the diagnosis of tuberculosis. Clin Microbiol Infect. 2024;30(9):1115–1122. doi:10.1016/j.cmi.2023.07.014
13. Riely GJ, Wood DE, Ettinger DS, et al. Non-small cell lung cancer, version 4.2024, NCCN clinical practice guidelines in oncology. J Natl Comprehens Cancer Netw. 2024;22(4):249–274. doi:10.6004/jnccn.2204.0023
14. Uchida Y, Soejima K. Clinical characteristics of patients simultaneously diagnosed with lung cancer and active pulmonary tuberculosis in countries where tuberculosis is moderately endemic. Transl Cancer Res. 2022;11(8):2480–2482. doi:10.21037/tcr-22-1904
15. Zhang F, Qi F, Han Y, et al. Clinical and imaging features of co-existent pulmonary tuberculosis and lung cancer: a population-based matching study in China. BMC Cancer. 2025;25(1):89. doi:10.1186/s12885-024-13350-y
16. Yang L, Zhuang L, Ye Z, Li L, Guan J, Gong W. Immunotherapy and biomarkers in patients with lung cancer with tuberculosis: recent advances and future directions. iScience. 2023;26(10):107881. doi:10.1016/j.isci.2023.107881
17. Cao S, Li J, Lu J, Zhong R, Zhong H. Mycobacterium tuberculosis antigens repress Th1 immune response suppression and promotes lung cancer metastasis through PD-1/PDl-1 signaling pathway. Cell Death Dis. 2019;10(2):44. doi:10.1038/s41419-018-1237-y
18. Ho JC, Leung CC. Management of co-existent tuberculosis and lung cancer. Lung Cancer. 2018;122:83–87. doi:10.1016/j.lungcan.2018.05.030
19. Hirashima T, Tamura Y, Han Y, et al. Efficacy and safety of concurrent anti-cancer and anti-tuberculosis chemotherapy in cancer patients with active Mycobacterium tuberculosis: a retrospective study. BMC Cancer. 2018;18(1):975. doi:10.1186/s12885-018-4889-1
20. Chai M, Shi Q. The effect of anti-cancer and anti-tuberculosis treatments in lung cancer patients with active tuberculosis: a retrospective analysis. BMC Cancer. 2020;20(1):1121. doi:10.1186/s12885-020-07622-6
21. Ye MF, Su S, Huang ZH, et al. Efficacy and safety of concurrent anti-tuberculosis treatment and chemotherapy in lung cancer patients with co-existent tuberculosis. Ann Translat Med. 2020;8(18):1143. doi:10.21037/atm-20-5964
22. Lee CS, Shu CC, Chen YC, Liao KM, Ho CH. Tuberculosis treatment incompletion in patients with lung cancer: occurrence and predictors. Int J Infect Dis. 2021;113:200–206.
23. Cheng MP, Abou Chakra CN, Yansouni CP, et al. Risk of active tuberculosis in patients with cancer: a systematic review and meta-analysis. Clin Infect Dis. 2017;64(5):635–644. doi:10.1093/cid/ciw838
24. Yang ZM, Qin XY, Lu YY, et al. Pathogen spectrum and clinical characteristics of lung cancer patients: a 10-year retrospective study. Int J Cancer. 2025;156(7):1470–1479. doi:10.1002/ijc.35272
25. Shi J, Li J, Wang Q, et al. The safety and efficacy of immunotherapy with anti-programmed cell death 1 monoclonal antibody for lung cancer complicated with Mycobacterium tuberculosis infection. Transl Lung Cancer Res. 2021;10(10):3929–3942. doi:10.21037/tlcr-21-524
26. Evman S, Baysungur V, Alpay L, et al. Management and surgical outcomes of concurrent tuberculosis and lung cancer. Thorac Cardiovasc Surgeon. 2017;65(7):542–545. doi:10.1055/s-0036-1583167
27. Tang A, Ahmad U, Raja S, et al. How much delay matters? How time to treatment impacts overall survival in early stage lung cancer. Ann Surg. 2023;277(4):e941–e7. doi:10.1097/SLA.0000000000005307
28. Zhou ZJ, Xie HY, Bertolaccini L, Xia N, Zhang Y. Research progress on lung cancer complicated with pulmonary tuberculosis: a narrative review. Transl Lung Cancer Res. 2025;14(6):2272–2280. doi:10.21037/tlcr-2025-450
29. Asamura H, Nishimura KK, Giroux DJ, et al. IASLC lung cancer staging project: the new database to inform revisions in the ninth edition of the TNM classification of lung cancer. J Thorac Oncol. 2023;18(5):564–575. doi:10.1016/j.jtho.2023.01.088
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.