Back to Journals » Advances in Medical Education and Practice » Volume 17
Teaching Attitude, Ethics and Communication Through the Use of An Online Escape Room for First-Year Medical Students
Authors Tomar A ![]() , Suryavanshi C
, Suryavanshi C ![]() , Pallavi LC
, Pallavi LC ![]() , Nayak KR
, Nayak KR
Received 2 April 2026
Accepted for publication 11 June 2026
Published 10 July 2026 Volume 2026:17 614137
DOI https://doi.org/10.2147/AMEP.S614137
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Supplementary video of “Online Escape Room for Medical Students” [614137].
Views: 8
Akash Tomar,1 Chinmay Suryavanshi,1 L C Pallavi,1 Kirtana Raghurama Nayak1,2
1Department of Physiology, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, KA, India; 2Department of Medical Education, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, KA, India
Correspondence: Kirtana Raghurama Nayak, Department of Physiology, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, KA, India, Email [email protected]
Background: Modern medical education requires innovative, learner-centered strategies to cultivate essential professional attributes like empathy, communication, and ethical reasoning. While the Attitude, Ethics, and Communication (AETCOM) curriculum is mandated in India, traditional lecture-based methods often struggle to engage students in the practical application of these affective-domain competencies. This study evaluated the impact of a gamified, online escape room on the engagement and learning of first-year medical students regarding AETCOM Modules 1.2 and 1.3.
Methods: A prospective interventional study was conducted with 180 students consenting first-year MBBS. Participants collaborated in small groups to navigate a 30-minute digital escape room featuring four sequential levels of increasing complexity, focused on patient perspectives, doctor-patient relationships, and ethical dilemmas. Effectiveness was measured using Kirkpatrick’s Level 1 (Reaction) via a 23-item Likert-scale and Level 2 (Learning) through pre- and post-intervention assessments. Qualitative data were analyzed using thematic analysis.
Results: Quantitative analysis revealed a statistically significant improvement in assessment scores (p < 0.001), with mean scores rising from 13.89 + 3.14 to 14.48 + 3.14. Students reported high levels of satisfaction (mean = 4.24) and perceived the activity as highly relevant to clinical practice (mean = 4.27). Thematic analysis identified three core strengths: enhanced teamwork and collaboration, high levels of interactivity and engagement, and the stimulation of critical thinking and problem-solving skills.
Conclusion: Online escape rooms serve as a scalable and effective pedagogical tool for teaching foundational professional competencies. By bridging cognitive and affective learning domains, this gamified approach fosters emotional investment and collaborative learning, better preparing early-phase medical students for the complexities of patient-centered care.
Keywords: AETCOM, medical education, escape-room, gamification, education for all
Introduction
Medical education is evolving, with a growing emphasis on interactive, learner-centric pedagogies that foster not only knowledge acquisition but also the development of critical professional competencies such as communication, ethical reasoning, collaboration, and decision-making.1 However, in the landscape of undergraduate medical education, particularly in India, there has been a growing recognition that foundational values such as those emphasized in the AETCOM (Attitude, Ethics, and Communication) framework must be explicitly taught and evaluated. This shift stems from the realization that the unstructured, observational acquisition of professional values is insufficient in the face of increasing clinical loads, shorter patient interactions, and a heightened reliance on diagnostics over dialogue.2 The National Medical Commission (NMC) in India responded by mandating the inclusion of the AETCOM module in the undergraduate curriculum.3 AETCOM modules have traditionally been taught as lecture-based teaching methods, which are foundational and often fall short in engaging students and promoting the application of knowledge in real-world scenarios.4 Teaching AETCOM requires methods that allow for experiential learning and simulation of real-world interpersonal interactions, which escape rooms can effectively provide. By immersing students in ethical dilemmas or patient-centered scenarios, educators can facilitate meaningful discussions that lectures or text-based approaches may not elicit.5
Gamification, the application of game-design elements in nongame contexts, has emerged as an innovative approach to enhance motivation, engagement, and learning outcomes in medical education.6 Originally developed for entertainment, escape rooms have increasingly been adopted in health profession education as immersive, gamified learning tools. By simulating high-pressure, time-bound scenarios, they foster experiential learning, critical thinking, and collaborative problem solving, making them promising pedagogical strategies for engaging students in active knowledge applications.7 Escape rooms, whether recreational or educational, are generally based on a combination of theoretical frameworks. This includes gamification, game-based learning, constructivism, and immersive learning. These frameworks emphasize collaboration, problem-solving, and the creation of engaging, interactive experiences that encourage learning through exploration and discovery.8 The inherent structure of an escape room requires a collaborative problem-solving mode under pressure, while navigating a narrative which directly mirrors the clinical challenges AETCOM aims to address. The need to interpret clues and make collective decisions simulates the doctor-patient-family dynamics, while the ethical dilemmas embedded in the puzzles compel students to engage in the very perspective-taking and empathetic reasoning that lectures alone cannot cultivate. As such, effective patient care depends not only on clinical acumen but also on empathy, communication, and ethical sensitivity.
Moreover, the adaptability of digital platforms has made it feasible to conduct escape rooms online, offering scalability and accessibility while maintaining interactivity. This is especially relevant in post pandemic medical education, where blended and remote learning environments are becoming standard.9,10 Escape rooms in medical education have been adapted to various learning environments, including classrooms, simulation centers, and virtual platforms. Classroom-based escape rooms use simple, low-cost puzzles and group tasks to reinforce theoretical content and teamwork within a traditional academic setting.11 Simulation center escape rooms add realism by incorporating clinical scenarios, mannequins, and medical equipment, helping learners practice hands-on skills under time constraints. Virtual escape rooms, delivered online, replicate the problem-solving and collaboration of physical formats but provide greater flexibility and accessibility for large cohorts or remote learning needs.12 In this context, online escape rooms may offer a low-cost, high-engagement solution that is adaptable across topics and learning environments, from foundational sciences to clinical rotations.
A systematic review by Veldkamp et al12 highlighted the potential of escape rooms to create active learning environments that align with problem-solving practices in healthcare, especially when designed with clear educational goals and appropriate cognitive load. Furthermore, a study by Fedorcsak in 202413 demonstrated that well-designed escape room games engage students with complex problems and challenge their clinical and teamwork skills, showing a moderate benefit for learning outcomes in medicine.
In the context of medical education, escape rooms have been effectively utilized as learning strategy in various disciplines For example, Faysal et al14 compared the effectiveness of medical escape rooms for the learning of undergraduate medical students with that of case-based learning in teaching clinical dermatology and reported that students in the escape room group performed better than those in traditional case-based learning settings. Ferns et al15 implemented an escape room for interprofessional education where a working party of five educators representing the professions of medicine, nursing, pharmacy, physiotherapy and speech pathology who shared a common interest in interprofessional education, found that using a non-clinical escape room format offered a novel way for clinicians and educators to practice skills needed for collaborative practice in an environment free from the usual hierarchies and pressures of professional roles. Another study conducted by Akatsu et al16 used escape rooms to assess 140 first year medical students in Japan in which the students were given medical interview and physical examination and this study concluded that incorporating “Escape Rooms” to the final assessment proved that this descriptive study analyzing both quantitative and qualitative data, not only achieved the intended objectives of successfully conducting comprehensive medical interview and basic physical examination skills, but also enhanced student motivation. In nursing education, Molina-Torres et al17 used an “Anatomy Escape Room” and reported that this game-based approach motivated students and provided a practical, engaging resource for learning anatomy in healthcare training.
Despite their promise, most existing studies on escape rooms focus on clinical skills or acute care training.18–20 There is a notable gap in the literature regarding their use in teaching abstracts and affective-domain content in ethics and communication. This study aims to implement an online escape room centered around AETCOM Modules assessing its impact on student learning, and exploring learner perceptions of this novel approach.3 By doing so, we seek to contribute to the growing body of literature advocating for evidence-based gamification in teaching AETCOM modules and to propose scalable, engaging solutions for addressing CBME learning outcomes in the medical curriculum.21 Thus, the objectives of this study were as follows:
- To design and implement an online escape room aligned with AETCOM modules to introduce key professional competencies to first-year MBBS students.
- To evaluate the impact of this gamified learning strategy on students’ understanding of the modules through pre- and post-assessment scores.
- To explore students’ perceptions of the escape room experience, including its effectiveness, engagement level, and perceived relevance to future clinical practice.
Materials And Methods
Study Design and Setting
This was a mixed method, quasi-experimental study using a pre-test/post-test design. The educational activity was implemented within the Phase I undergraduate medical training physiology curriculum as part of the AETCOM module delivery. In the first professional year, students study Anatomy, Physiology, Biochemistry, and Community Medicine, which includes field visits under the family adoption program. The teaching–learning methodologies encompass lectures, small group discussions, self-directed learning (SDL), skills training in laboratories, and hospital visits as part of the Early Clinical Exposure (ECE) initiative. Of the 27 AETCOM modules, five are introduced in the first year.
Module 1.2: “What it means to be a patient” and Module 1.3: “Doctor–patient relationship” are facilitated by Department of Physiology.
Module 1.5: “Cadaver as the first teacher” and Module 1.4: “Foundations of communication” are handled by Department of Anatomy.
Module 1.1: “What does it mean to be a doctor” is taught by Department of Biochemistry.
The recommended teaching approaches for AETCOM include anchoring lectures followed by case-based learning and small group discussions. This study was conducted during the hours meant for small group discussions for AETCOM in modules 1.2 and 1.3.
Study Participants and Sample Size
The study employed complete enumeration, including all students enrolled in the course during the study period as participants, thereby negating the need for a formal sample size calculation. The recruitment of the study participants was done on two days for two batches on 19/02/2025 and 20/02/2025 and the data for all the pre-post and feedback was also collected on these two days.
Inclusion and Exclusion Criteria
Inclusion Criteria
All 250 first-year medical students from the 2024–25 batch of Kasturba Medical College, Manipal, attended the small-group teaching session.
Exclusion Criteria
Students who could not attend the session were excluded.
Construction of the Educational Module
Designing the Online Escape Room
The online escape room was designed in alignment with the learning objectives of AETCOM Modules 1.2 and 1.3 addressing the competencies on developing professional qualities, roles of physician and demonstrating empathy in patient encounters. This activity was created in collaboration with Elsevier ClinicalKey®, who created the escape room on Interacty software that was structured into four sequential levels/rooms of increasing complexity:
- Level 1: “The Patient Perspective” consisted of Match-the-pair (ethics and doctor‒patient interaction terms). There were 5 such interactions in which students match the emotion felt by the patient with the dialogue that he had with the doctor.
- Level 2: “Navigating the Doctor-Patient Relationship” consisted of a crossword puzzle in which there were questions pertaining to doctor-patient. A total of 8 questions were present in this level.
- Level 3: “The Doctor Wears Multiple Coats”, consisted of different match the cards which were designed on different duties performed by a doctor.
- Level 4: “Dimensions and Implications of Human Suffering” A 9-question clinical challenge revealing a hidden image as a clue for the end.
After the end of each level, the students were given a question to solve pertaining to the topic discussed at that level. After entering the right answer, they were taken to the next round.
Each level was developed to reflect one or more intended learning outcomes of the AETCOM modules, and the students were directed to the feedback page at the end of the game. The escape room was administered online in small groups of 8 students each, with a time limit of 30 minutes. A screen-recorded demonstration of the online escape room as experienced by students is available at Video S1.
Internal Validation of the Module
The educational content and structure of the escape room were reviewed and validated by four faculty experts in medical education and ethics, as shown in Supplementary Figure 1. Feedback was incorporated from peer review prior to final deployment.
Ethical Permissions and Consent
Institutional permissions were obtained prior to implementation. Written informed consent was obtained from all the student participants which also included consent for publication of anonymized responses/direct quotes of the participants. Participation was voluntary, and anonymity and data confidentiality were ensured throughout. Ethical approval for the study was obtained from the Institutional Ethics Committee of Kasturba Medical College and Kasturba Hospital, Manipal with number [IEC1:55/2025]. Students were informed that their decision to participate or withdraw would not affect their academic standing. The study was conducted following the guidelines as declared by the Declaration of Helsinki, 2013.
Detailed Description of the Session
The AETCOM sessions in sections 1.2 and 1.3 were first taught as anchoring lectures to the students. The next day, they were called for the online escape room session which was conducted for a duration of 3 hours. A pretest on the AETCOM modules was conducted before the start of the activity. The escape room session was delivered in four demonstration rooms with each team having their own laptop/tablet for the activity. Students accessed the platform on laptops/tablets and worked in assigned groups of 8. Each group navigated the puzzle collaboratively. After game completion, each student completed a post session quiz including Multiple choice type questions and the same questions as the pre session quiz and provided feedback about the session. A plan of the lesson is shown in Figure 1.
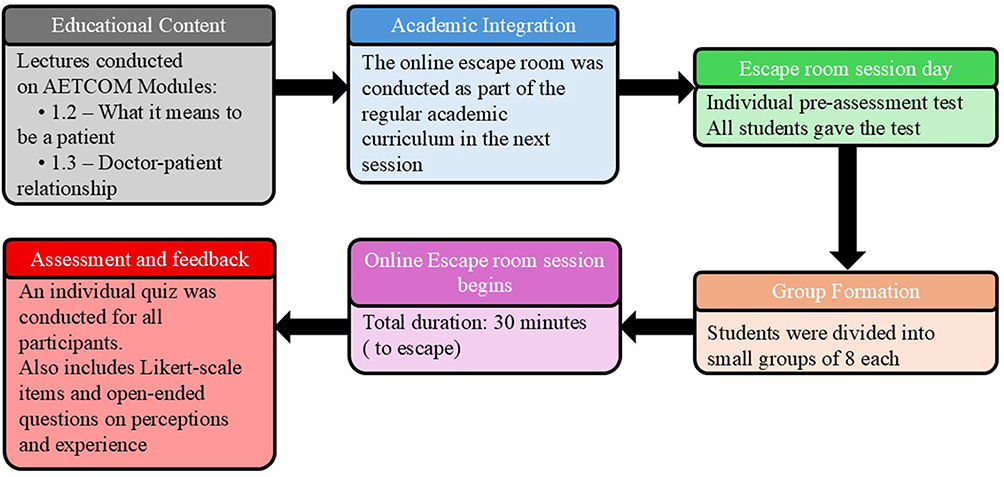 |
Figure 1 A timeline showing the session flow: Lectures → pre-quiz → escape room play (30 mins) → post-quiz → feedback. |
Session Assessment and Feedback
The session effectiveness was evaluated on the basis of the first two levels of the Kirkpatrick evaluation model.22 The first level focuses on recording learners’ reactions and rating their experience, whereas the second level captures the knowledge and insights that participants gained from the session.
Level 1 (Reaction)
The feedback of the students was gathered immediately after the educational intervention. After providing informed consent, the students were invited to answer a newly developed and validated semi structured questionnaire on the effectiveness of the session as shown in Supplementary Figure 2.
Questionnaire Validation
The questionnaire was validated for its content by five subject experts in the fields of medical education and bioethics.
After providing informed consent, the questionnaire was administered online via Microsoft Forms. Perceptions of the session were captured via a feedback form structured as follows:
- 23 Likert-scale questions (5-point scale from “Strongly Disagree” to “Strongly Agree”).
- Five open-ended questions eliciting feedback and suggestions for improvement in the escape room experience were submitted.
Level 2- (Learning)
Student learning was assessed via a pre- and post-quiz consisting of twenty multiple-choice questions based on the AETCOM session. These questions were designed, internally reviewed and validated by four faculty experts in medical education and ethics. The questions used are shown in Supplementary Table 1. These questions included:
1. 8 True or false questions
2. 8 Yes or no questions
3. 2 Match the terms questions
4. 2 Ranking or ordering questions
Data Analysis
The quantitative data were analyzed via R software. Pre- and post-test scores were compared via the Wilcoxon signed-rank test (p < 0.05 was considered significant). Questionnaire reliability was measured via Cronbach’s alpha. Descriptive statistics are presented as percentages, medians, and interquartile ranges (IQRs).
Qualitative data from the open-ended responses were analyzed via Braun and Clarke’s thematic analysis framework.23 Two independent reviewers generated initial codes inductively. A consensus on the thematic structure was reached, with 90% agreement. The final themes were reviewed and confirmed by additional members of the research team to ensure credibility and rigor.
Results
Questionnaire Validity and Reliability
The content validity ratio (CVR) was calculated for each item, and the content validity index (CVI) was calculated for the overall instrument. The CVIs for the questionnaire’s relevance, clarity, and essentiality were determined. On the basis of the reviewer’s recommendations and necessary incorporations, the final questionnaire consisted of 28 items, with the last 5 being open-ended questions. The reliability of the questionnaire was confirmed, with a Cronbach’s alpha of 0.89, ensuring reliability.
Reliability of the Assessment Tool
The reliability of the twenty-item multiple-choice pre- and post-quiz was evaluated using Cronbach’s alpha and test–retest reliability coefficients computed on the matched student data. For the pre-test to post-test matched cohort Cronbach’s alpha was 0.192 and the Pearson test–retest correlation was r = 0.131, with a Standard Error of Measurement (SEM) of 1.67 points. For the Batch B to post-test matched cohort (n = 98), Cronbach’s alpha was −0.198 and the Pearson correlation was r = −0.093 (SEM = 2.03).
Session Findings
One hundred eighty students (82 males and 98 females) consented to be part of the study out of the 250 students. The 250 students were divided in two batches of 125 each and the sessions conducted across two days. Each batch was divided into four groups and were housed in four separate demonstration rooms, so that four of 8 students each stayed in one demonstration room. The session was conducted in parallel with four facilitators in each demonstration room. The age of the participants ranged between 17 and 24 years (mean age: 19).
Findings at Level 1 – Reaction
Out of the 23 Likert scale items, four overarching themes were identified to represent students’ perceptions of the escape room-based learning activity, as shown in Table 1.
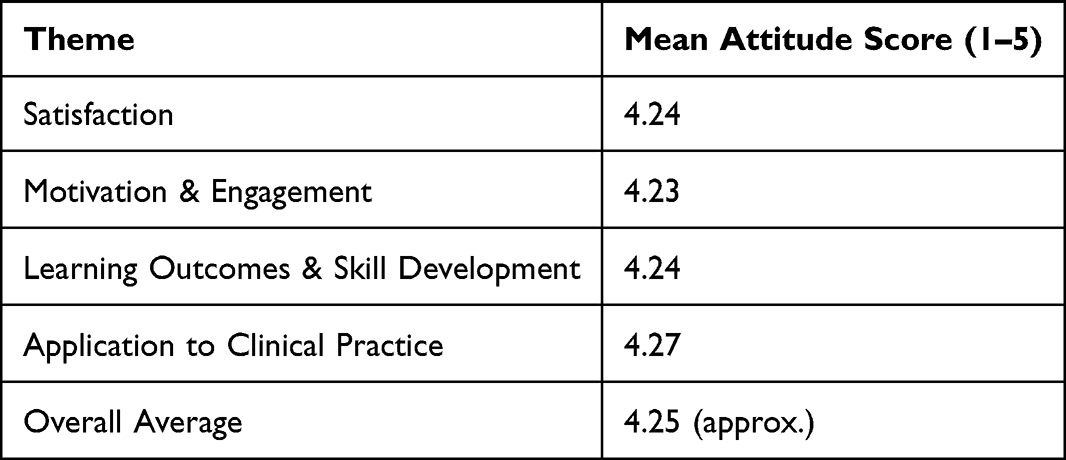 |
Table 1 Average Student Ratings for Each Key Theme Derived From 23 Likert Scale Items |
Analysis of the students’ responses to the online escape room activity revealed strong overall satisfaction across all thematic areas. The highest average rating was observed in the application to clinical practice theme (M = 4.27), indicating that participants perceived the activity as highly relevant to real-world medical decision-making. Satisfaction (M = 4.24), motivation and engagement (M = 4.23), and learning outcomes and skill development (M = 4.24) also received consistently high scores, suggesting that the escape room was not only enjoyable but also effectively supported student learning and collaboration. These results demonstrate that the gamified learning format was well received and beneficial in promoting knowledge retention, critical thinking, and team-based communication within a clinical context.
Thematic Analysis of Student Responses to the Open-Ended Questions
Three key themes were identified from the qualitative responses of students who participated in the escape room activity and completed the feedback form. These themes reflect both the perceived strengths of the learning experience and areas for future refinement.
Theme 1: Teamwork and Collaboration
The students consistently highlighted the value of collaboration during the activity. Working in teams appeared to enhance communication, coordination, and shared problem solving. Many students felt that group dynamics fostered a positive and productive learning atmosphere. One participant remarked, “The group discussion and collaboration made the activity enjoyable and productive,” illustrating how peer interaction functioned not only as a pedagogical strategy but also as a motivational factor. This aligns with the literature on cooperative learning, where teamwork has been shown to support deeper understanding through social constructivism.
Theme 2: Engagement and Interaction
The interactive nature of the escape room emerged as a key driver of student motivation. The students reported sustained attention and increased interest throughout the session. One student stated, “The interactive nature kept me interested throughout the session,” pointing to the affordances of game-based learning in maintaining engagement. This theme reinforces the pedagogical merit of gamification, suggesting that active participation and immersion are essential components in promoting learner-centered environments.
Theme 3: Critical Thinking and Problem Solving
A notable number of students appreciated the cognitive demands of the activity, indicating that the puzzles required creative and analytical thought. The escape room format challenged learners to apply previously acquired knowledge in novel ways. As one participant noted, “It made me think outside the box and apply what I learned.” This theme supports the idea that game-based learning can stimulate higher-order thinking, echoing the objectives of constructivist pedagogies.
Student Feedback on the Activity/Future Suggestions
Views on Time Constraints and Pressure
Mixed reactions were observed regarding the time limitations imposed during the activity. While some students perceived the time constraint as a source of stress, others felt it heightened their sense of urgency and collaboration. Comments such as “The time crunch made it hard to finish all questions properly,” contrasted with “The time challenge increased our collaboration,” highlight the dual role of pressure—as both a potential barrier and a motivational tool. This suggests a need to carefully calibrate time allocations in future implementations to optimize learning outcomes.
Student Views on Technical Issues
A minor yet notable concern was the presence of technical disruptions, particularly related to internet connectivity. These issues occasionally impeded student progress and disrupted group flow. One student mentioned, “Internet buffering slowed our progress.” While such challenges were not widespread, they underscore the importance of robust technological infrastructure when digital tools are integrated into learning environments.
Question Difficulty and Clarity
The students reported varying levels of difficulty with the questions, with some describing them as overly complex or ambiguously worded. Difficulty arose from syntax issues, such as plural/singular confusion. One participant reflected, “Some questions were a bit tough to guess.” This theme highlights the critical role of clear instructional design and emphasizes the need for pilot testing materials to ensure accessibility for all learners.
Suggestions for Improvement
The participants offered constructive feedback for enhancing the activity, including calls for more hints, clearer instructions, and more practical, real-world scenarios. Suggestions also included forming smaller groups and increasing the number of questions to better support learning depth. One student proposed, “Providing hints and making the cases more practical could improve the experience.” These recommendations present opportunities for iterative design improvements and responsive pedagogy.
A word cloud of the responses provided to the open-ended questions of the feedback form is shown in Figure 2.
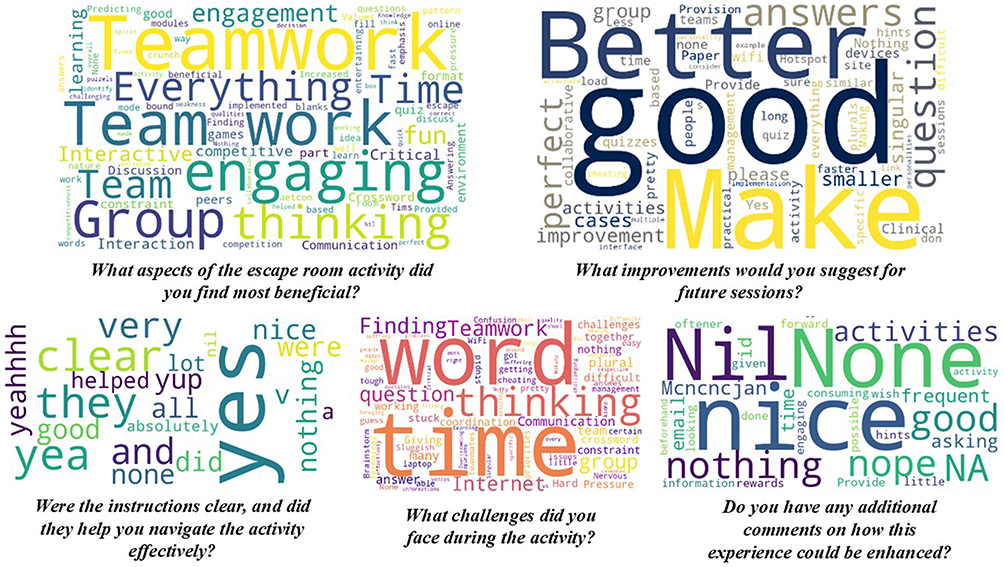 |
Figure 2 Word cloud of students’ answers to open-ended questions from the feedback form. |
As seen in the word cloud, the participants identified several key benefits of the escape room activity, most notably teamwork, interactivity, critical thinking, engagement, and fun. Terms such as time constraints, quizzes, communication, and group learning also featured prominently, indicating that students valued both the collaborative and cognitively stimulating nature of the experience.
The reported challenges included time pressure, difficulty finding words, communication gaps, and coordination issues. Technical problems such as internet connectivity and device limitations were also noted. Some students highlighted conceptual difficulties such as critical thinking and plural word forms, although many reported no significant obstacles.
While most students offered no suggestions for improvement via terms such as “nothing,” “none,” and “perfect,” some recommended more questions, similar activities, and quizzes to sustain engagement. A few requested logistical enhancements, including smaller groups, better internet access, and clearer answer formats, especially avoiding plurals or accepting alternate correct responses.
The responses to the clarity of instructions were overwhelmingly positive, with “yes” being the dominant term. Many described the instructions as very clear and helpful, with only rare instances of neutral or unclear feedback. Additional comments echo overall satisfaction, with most students suggesting no changes. Isolated suggestions included offering rewards and hints, reducing repetitive input, and providing more pre-activity guidance. These responses reaffirm the activity’s success while pointing to small opportunities for refinement.
Findings at Level 2—Learning
Descriptive analysis of pre- and post-escape room assessment scores revealed a positive shift in student performance. The mean pre-assessment score was 13.89 ± 3.14, while the mean post- assessment score increased to 14.48 ± 3.14. The median score also improved from 14 to 15. The analysis revealed a statistically significant improvement in post-assessment scores compared with the pre-assessment scores (p < 0.001) by Wilcoxon signed rank test, suggesting that escape room activity had a measurable positive effect on student learning and knowledge retention in AETCOM-related content. The pre- and post-box plots are shown in Figure 3.
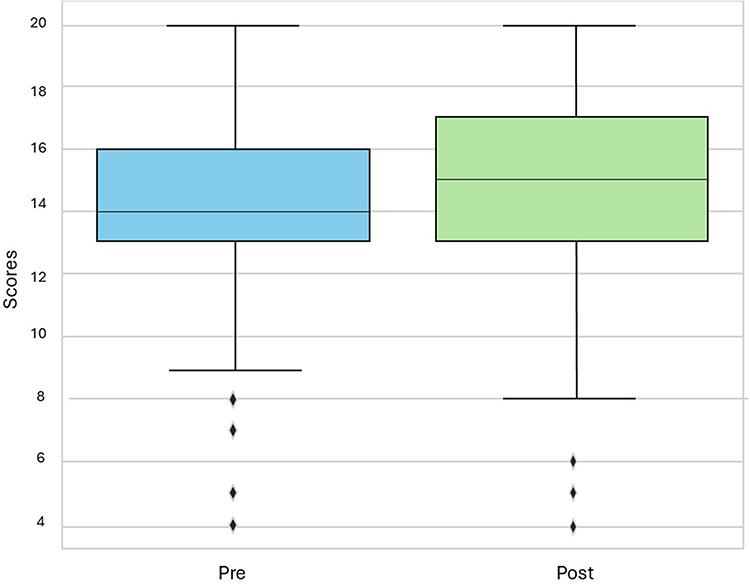 |
Figure 3 Box plot of the pre- and post-test scores of the students ((p = 0.000519) by Wilcoxon signed rank test. |
Discussion
Empathy, collaboration, and ethical sensitivity form the cornerstone of patient-centered medical practice. These attributes are traditionally nurtured through clinical exposure, role modelling, and feedback. Our study leveraged this policy shift to explore the utility of a novel pedagogical tool, an online escape room, to facilitate the learning of AETCOM competencies among first-year MBBS students. The escape room format, which is traditionally associated with entertainment, was adapted into a structured, curriculum-aligned activity that challenged learners to apply ethical reasoning, empathy, and communication principles in simulated clinical contexts. Prior studies have shown that gamified environments can promote knowledge retention, enhance motivation, and increase learner satisfaction however they were mostly conducted on various surgical skills, history taking and medical knowledge.24–26 In this study, the online escape room activity demonstrated strong evidence of validity and reliability as an instructional tool for teaching AETCOM modules. At Kirkpatrick’s Level 1 (Reaction), students reported high levels of satisfaction (mean = 4.24) aligning with our findings which focused specifically on the affective domain in medical curriculum that is on the AETCOM modules. Previous literature such as, Mirshahi et al,19 who used escape rooms to teach research ethics and use escape room as an assessment tool, and Çakmak and Kaymaz27 who explored escape rooms for technical competencies in nursing students and help enhance their critical thinking motivation have shown that escape room activity causes an increase in satisfaction and critical thinking.
In our study students also reported increased motivation, collaboration and engagement (mean = 4.23), aligning with previous studies which also reiterate that teamwork and collaboration increases when gamification techniques are used in developing teamwork competencies.28 Another study by Friedrich et al29 analyzed the teamwork of interprofessional healthcare workers in a fictitious patient case in a simulated hospital environment and found increased teamwork, motivation and engagement in the study population. This study also showed that the perceived learning outcomes and skill development (mean = 4.24) to be on the higher side and in alignment with prior studies, that have shown an increase in learning and skills development.30 A study by Antikchi et al,31 showed that gamified scenario-writing method can be an effective and dynamic learning method for developing clinical skills in nursing students.
In our study students also showed high levels of learning and application of this learning to clinical practice (mean = 4.27). Prior studies have shown the same effect in nursing students.32,33 A recent scoping review on escape rooms in medical education by Park et al34 showed that although evidence is limited on whether escape rooms can enhance knowledge retention, significant support shows their impact on fostering the ACGME (Accreditation Council for Graduate Medical Education) core competencies of interpersonal and communication skills and systems-based practice. These themes highlight the perceived relevance and authenticity of the escape room format for real-world medical scenarios and in the students who had exposure to gamified learning whether on-site or online.
Thematic analysis of open-ended feedback reinforced these quantitative results, revealing strong student appreciation for teamwork, collaboration, interactivity, and critical thinking opportunities, alongside constructive suggestions for refining question clarity, technical delivery, and time management. At Level 2 (Learning), the escape room activity produced a measurable positive impact on student knowledge. There was a clear increase in mean scores from pre-activity (13.89 ± 3.14) to post-activity (14.48 ± 3.14), with the improvement reaching statistical significance with a p-value of < 0.001. This indicates that the gamified format not only engaged students but also supported knowledge retention and application of key AETCOM concepts related to patient-centered care and doctor–patient relationships, which is in alignment with previous studies that have concluded the same.13,18,19,29,33,35,36
The use of an online format in our study allowed for scalability without compromising interaction. In line with post pandemic educational innovations,10 digital design preserves small-group engagement through embedded team tasks and timed problem solving. The students reported feeling emotionally invested in the scenarios, pointing to the potential of escape rooms to bridge the cognitive and emotional aspects of learning. The design also created opportunities for reflective discussions crucial for cultivating professional judgement in ethically complex situations.
Importantly, our study targeted first-year students’ novices still developing their understanding of the physician’s role. This early exposure to clinical scenarios grounded in empathy and ethics can serve as a scaffold for later, more complex encounters. Like the visual hermeneutic strategies used in other AETCOM studies,37,38 our activity sought to immerse students in interpretative and emotionally resonant learning. By blending cognitive challenges with collaborative storytelling, escape rooms may offer a similarly potent learning environment.
Furthermore, the escape room encouraged learners to grapple with ambiguity, manage peer dynamics, and reflect on their personal bias skills, which are critical but often underrepresented in formal assessments. As other scholars have noted, tools that foster narrative understanding and perspective-taking can cultivate tolerance for uncertainty and deepen learner engagement with professional values.39–41 While the quantitative analysis revealed a statistically significant improvement in post-assessment scores, the absolute gain was modest. This is not unexpected when measuring complex, affective competencies such as empathy and ethical reasoning, which are not easily captured by multiple-choice questions alone. Therefore, we state that the primary evidence for the intervention’s success lies in the Level 1 (Reaction) and Level 2 (learning) along with the qualitative data assessed. The strongly positive feedback on engagement, perceived relevance to clinical practice, and the development of emotional insight as seen in Figure 2 suggest that the escape room’s main impact was in the affective and social learning domains which are precisely the target of the AETCOM modules.
The students in our study not only demonstrated measurable gains in knowledge but also engaged in deep emotional and reflective learning, as evidenced by their feedback. The escape room’s high-pressure, time-bound format mirrors clinical uncertainty, whereas its gamified structure sustains motivation and fosters collaborative problem solving. These characteristics align with the educational goals of the AETCOM module: to help learners internalize the values of professionalism, patient-centric care, and ethical conduct.
Thus, our study supports the incorporation of online escape rooms as innovative and effective strategies for teaching AETCOM competencies in medical education. By fostering engagement, collaboration, and practical application of ethical and communication principles, escape rooms can enrich the learning experience and better prepare students for the complexities of clinical practice.
Limitations
This study is not without limitations. First, the absence of a control group receiving traditional AETCOM instruction constrains the ability to attribute observed gains solely to the escape room intervention. Future studies could adopt randomized or Quasi experimental designs to enable comparative analysis. Second, while the immediate post assessment results were promising, the long-term retention of competencies and their application in clinical settings were not evaluated. Longitudinal follow-up, including OSCE performance or empathy scales, would provide a fuller picture. Finally, the study was conducted in a single institution, limiting its generalizability. Implementation across multiple institutions and learner populations would provide broader validation. Future work could explore how virtual, hybrid, or AI-enhanced escape rooms compare in terms of engagement and learning outcomes.
Suggestions for Future Work
Future research could incorporate control groups to compare escape rooms with traditional lecture or case-based methods and assess long-term outcomes via objective measures of professional behavior and empathy. Triangulated qualitative approaches, including focus groups and faculty feedback, can enrich the understanding of learner experiences. Expanding escape room use to other AETCOM modules, such as medico-legal, cultural, and communication topics, offers further potential. Additionally, exploring cross-institutional and interprofessional adaptations may enhance scalability and collaborative learning.
Conclusion
Our findings support the integration of online escape rooms as an innovative and effective strategy for teaching AETCOM competencies in undergraduate medical education. The intervention fostered not only knowledge acquisition, but also emotional investment, teamwork, and feedback attributed centrally to the development of compassionate and ethical healthcare professionals. In an educational climate increasingly oriented toward active, learner-centric methods, gamified tools such as escape rooms offer a scalable, engaging, and pedagogically sound approach to preparing medical students for the complex realities of clinical care. By anchoring students in emotionally resonant, team-based, ethically grounded scenarios, escape rooms can enrich AETCOM delivery and support the formation of professional identity from the earliest stages of training. Further research is warranted to refine this approach and assess its long-term impact on learner outcomes, patient care behaviors, and curricular innovation.
Declaration of Generative AI Use
ChatGPT (Version GPT-4, Open AI) was used to check grammar and improve syntax during the preparation of this manuscript. No content was generated by the AI model with author oversight, and all intellectual content is the author’s own.
Abbreviations
AETCOM, Attitude, Ethics and Communication; AI, Artificial Intelligence; ART, Assisted Reproductive Technology; CBME, Competency-Based Medical Education; CVI, Content Validity Index; CVR, Content Validity Ratio; ECE, Early Clinical Exposure; IQR, Interquartile Range; MBBS, Bachelor of Medicine, Bachelor of Surgery; MCQ, Multiple Choice Question; NMC, National Medical Commission; OSCE, Objective Structured Clinical Examination; SDL, Self-Directed Learning.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available with the corresponding author and can be made available upon appropriate request.
Ethics Approval and Informed Consent
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki 2013 and was approved by the Institutional Ethics Committee of Kasturba Medical College and Kasturba Hospital, Manipal with number [IEC1:55/2025]. All students participated voluntarily in the study. Data confidentiality was protected. Informed written consent was obtained from all the participants.
Acknowledgments
We would like to acknowledge the support of Elsevier team especially Ms. Natasha for providing necessary arrangements for developing the online escape room.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests in this work.
References
1. Kirch SA, Sadofsky MJ. Medical education from a theory–practice–philosophy perspective. Acad Pathol. 2021;8:23742895211010236.PubMed PMID: 33959676; PubMed Central PMCID: PMC8060751. doi:10.1177/23742895211010236
2. Udgiri R, Ganganahalli P. Perceptions of Attitude, Ethics, and Communication (AETCOM) Modules Among Indian Medical Graduates in Their First Professional Year: an Educational Observational Study. Cureus. 2024;16(7):e64611.PubMed PMID: 39149658; PubMed Central PMCID: PMC11326756. doi:10.7759/cureus.64611
3. Attitude. Ethics and Communication (AETCOM) Competencies for the Indian Medical Graduate. 2018. Available from: https://www.nmc.org.in/wp-content/uploads/2020/01/AETCOM_book.pdf.
4. Alaagib NA, Musa OA, Saeed AM. Comparison of the effectiveness of lectures based on problems and traditional lectures in physiology teaching in Sudan. BMC Med Educ. 2019;19(1):365. doi:10.1186/s12909-019-1799-0
5. Andersson H, Svensson A, Frank C, Rantala A, Holmberg M, Bremer A. Ethics education to support ethical competence learning in healthcare: an integrative systematic review. BMC Med Ethics. 2022;23:29.PubMed PMID: 35305627; PubMed Central PMCID: PMC8933936. doi:10.1186/s12910-022-00766-z
6. Watsjold BK, Cosimini M, Mui P, Chan TM. Much ado about gaming: an educator’s guide to serious games and gamification in medical education. AEM Educ Train. 2022;6(4):e10794.PubMed PMID: 36034886; PubMed Central PMCID: PMC9399447. doi:10.1002/aet2.10794
7. Quek LH, Tan AJQ, Sim MJJ, et al. Educational escape rooms for healthcare students: a systematic review. Nurse Educ Today. 2024;132:106004. doi:10.1016/j.nedt.2023.106004
8. Manojlovic H. Escape room as a teaching method. Opus Educ. 2022;9(2):2. doi:10.3311/ope.504
9. Seed Ahmed M, Soltani A, Zahra D, et al. Remote online learning reimagined: perceptions and experiences of medical students in a post-pandemic world. BMC Med Educ. 2025;25(1):215. doi:10.1186/s12909-025-06815-6
10. Zhao Y, Sun T, Zhang X, Wang X, Hu W. The evolution of medical education in the era of Covid-19 and beyond: a longitudinal study. BMC Med Educ. 2024;24:1289.PubMed PMID: 39529071; PubMed Central PMCID: PMC11555806. doi:10.1186/s12909-024-06271-8
11. Nowbuth AA, Parmar VS. Escaping the ordinary: a review of escape rooms in medical and veterinary education. BMC Med Educ. 2024;24:1506.PubMed PMID: 39707331; PubMed Central PMCID: PMC11660942. doi:10.1186/s12909-024-06512-w
12. Veldkamp A, van de Grint L, Knippels MCPJ, van Joolingen WR. Escape education: a systematic review on escape rooms in education. Educ Res Rev. 2020;31:100364. doi:10.1016/j.edurev.2020.100364
13. Fedorcsak P. Moderate benefit of escape room game on learning outcome in medicine. BMC Med Educ. 2024;24(1):1353.PubMed PMID: 39580402; PubMed Central PMCID: PMC11585938. doi:10.1186/s12909-024-06352-8
14. Faysal LR, Yasmin R, Zaman A, Khan RA. Effectiveness of medical escape room on learning of undergraduate medical students in comparison with case-based learning in teaching of clinical dermatology. Rawal Med J. 2022;47(1):187.
15. Ferns J, Hawkins N, Little A, Hamiduzzaman M. The escape room experience: exploring new ways to deliver interprofessional education. Innov Educ Teach Int. 2024;61(3):516–14. doi:10.1080/14703297.2022.2158900
16. Akatsu H, Shiima Y, Gomi H, et al. Teaching “medical interview and physical examination” from the very beginning of medical school and using “escape rooms” during the final assessment: achievements and educational impact in Japan. BMC Med Educ. 2022;22(1):67. doi:10.1186/s12909-022-03130-2
17. Molina-Torres G, Cardona D, Requena M, Rodriguez-Arrastia M, Roman P, Ropero-Padilla C. The impact of using an “anatomy escape room” on nursing students: a comparative study. Nurse Educ Today. 2022;109:105205. doi:10.1016/j.nedt.2021.105205
18. Guckian J, Eveson L, May H. The great escape? The rise of the escape room in medical education. Future Healthc J. 2020;7(2):112–115. doi:10.7861/fhj.2020-0032
19. Mirshahi A, Khanipour-Kencha A, Keyvanpour S, Motlagh MK. “MORAD ESCAPE”, a novel research-based escape room approach for evaluating research competencies of health professions students. BMC Med Educ. 2025;25(1):289.PubMed PMID: 39984933; PubMed Central PMCID: PMC11846363. doi:10.1186/s12909-025-06781-z
20. Khera S, Wai A, Ford C, Yoo A, Joe D, Oyoyo U. Implementing an escape room for clinical skills practice in a paediatrics clerkship. Clin Teach. 2025;22(2):e70033. doi:10.1111/tct.70033
21. Emke AR, Torre D, Aagaard EM. Competency-based education and programmatic assessment in undergraduate medical education: describing the gateway experience of successful design and implementation. Acad Med J Assoc Am Med Coll. 2025;100(11):1268–1271.PubMed PMID: 40550132. doi:10.1097/ACM.0000000000006141
22. Bates R. A critical analysis of evaluation practice: the Kirkpatrick model and the principle of beneficence. Eval Program Plann. 27(3):341–347. doi:10.1016/j.evalprogplan.2004.04.011
23. Braun V, Clarke V. Thematic Analysis: A Practical Guide. SAGE; 2021:377.
24. Gentry SV, Gauthier A, Ehrstrom BL, et al. Serious gaming and gamification education in health professions: systematic review. J Med Internet Res. 2019;21(3):e12994. doi:10.2196/12994
25. Busca E, Caristia S, Bidone SP, et al. Serious game for the nursing assessment of home-dwelling older adults: development and validation study. JMIR Serious Games. 2024;12:e52644. PubMed PMID: 39591607; PubMed Central PMCID: PMC11632285. doi:10.2196/52644
26. Tan JW, Ng KB, Mogali SR. An exploratory digital board game approach to the review and reinforcement of complex medical subjects like anatomical education: cross-sectional and mixed methods study. JMIR Serious Games. 2022;10(1):e33282.PubMed PMID: 35006080; PubMed Central PMCID: PMC8787653. doi:10.2196/33282
27. Çakmak B, Kaymaz TT. The effect of an escape room game on students’ academic self-efficacy and motivation for critical thinking: oncology nursing course. BMC Nurs. 2024;23(1):910.PubMed PMID: 39695610; PubMed Central PMCID: PMC11658394. doi:10.1186/s12912-024-02586-5
28. Seto AV. P134: escape game as a theatre-based simulation for teamwork skills training in undergraduate medical education. Can J Emerg Med. 2018;20(S1):S104–5. doi:10.1017/cem.2018.332
29. Friedrich C, Teaford H, Taubenheim A, Boland P, Sick B. Escaping the professional silo: an escape room implemented in an interprofessional education curriculum. J Interprof Care. 2019;33(5):573–575.PubMed PMID: 30362849. doi:10.1080/13561820.2018.1538941
30. Ghafouri R, Zamanzadeh V, Nasiri M. Comparison of education using the flipped class, gamification and gamification in the flipped learning environment on the performance of nursing students in a client health assessment: a randomized clinical trial. BMC Med Educ. 2024;24(1):949.PubMed PMID: 39215281; PubMed Central PMCID: PMC11365181. doi:10.1186/s12909-024-05966-2
31. Antikchi M, Heydari S, Bakhshi F. The effect of game-based scenario writing on the clinical reasoning of internship nursing students in cardiovascular emergencies and critical care units. BMC Med Educ. 2025;25(1):597.PubMed PMID: 40269906; PubMed Central PMCID: PMC12020232. doi:10.1186/s12909-025-07079-w
32. Rushdan EE, Mohamed MAES, Abdelhalim GE, El-Ashry AM, Ali HFM. Effect of an escape room as a gamification evaluation tool on clinical reasoning and teamwork skills among nursing students: a quasi-experimental study. Nurse Educ Pract. 2025;82:104188.PubMed PMID: 39566365. doi:10.1016/j.nepr.2024.104188
33. Rafi A, Habibi A, Kalantarion M. Traditional medical education under siege: the revolutionary integration of virtual reality and gamification in medical escape rooms. BMC Med Educ. 2025;25(1):898.PubMed PMID: 40598049; PubMed Central PMCID: PMC12211356. doi:10.1186/s12909-025-07367-5
34. Park GL, Hegazy SA, Sepe J, et al. Fostering competencies: a scoping review of escape rooms in medical education. Med Sci Educ. 2025;35(2):1111–1121. doi:10.1007/s40670-024-02270-y
35. Alejandre C, Corniero P, Claret G, Alaez C, Esteban E, Jordan I. New resident training strategy based on gamification techniques: an escape room on sepsis in children. Children. 2022;9(10):10. doi:10.3390/children9101503
36. Cates AL, Krueger J, Simpson SE, et al. Comparing the effectiveness of a virtual toxicology escape room at two emergency medicine residencies. Cureus. 2020;12(10). doi:10.7759/cureus.11262
37. Rezaei S, Childress A, Kaul B, Rosales KM, Newell A, Rose S. Using visual arts education and reflective practice to increase empathy and perspective taking in medical students. MedEdPORTAL J Teach Learn Resour. 2023;19:11346.PubMed PMID: 37745278; PubMed Central PMCID: PMC10514245. doi:10.15766/mep_2374-8265.11346
38. Prabhath S, Kulkarni U, V LR, et al. Visual hermeneutics as a tool to introduce empathy and core physician attributes in doctor-patient relationship for first-year medical undergraduate students. BMC Med Educ. 2025;25(1):145. doi:10.1186/s12909-025-06742-6
39. Sturm H, Brown G, Gantwerker EA. Evaluating medical education escape rooms: a scoping review using the kirpatrick model. MedEdPublish. 2025;15:28.PubMed PMID: 41695194; PubMed Central PMCID: PMC12905535. doi:10.12688/mep.21095.3
40. Tekin M, Korkmaz G, Kılınçarslan MG, et al. Digital escape rooms in medical education: lessons learned from design and pilot implementation. BMC Med Educ. 2026;26(1):666.PubMed PMID: 41840564; PubMed Central PMCID: PMC13107658. doi:10.1186/s12909-026-09005-0
41. Thind A, Aggarwal N, Pisudde PM. Educational escape rooms for infection prevention and patient safety training in medical and nursing education: a systematic review and meta-analysis. Cureus. 2026;18(3):e105802.PubMed PMID: 42037881; PubMed Central PMCID: PMC13106903. doi:10.7759/cureus.105802
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.