Back to Journals » Advances in Medical Education and Practice » Volume 13
Teaching About Intergenerational Dynamics: An Exploratory Study of Perceptions and Prevalence in US Medical Schools
Authors Talmon GA ![]() , Nasir S, Beck Dallaghan GL
, Nasir S, Beck Dallaghan GL ![]() , Nelson KL
, Nelson KL ![]() , Harter DA, Atiya S, Renavikar PS, Miller M
, Harter DA, Atiya S, Renavikar PS, Miller M ![]()
Received 28 July 2021
Accepted for publication 5 January 2022
Published 29 January 2022 Volume 2022:13 Pages 113—119
DOI https://doi.org/10.2147/AMEP.S329523
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Geoffrey A Talmon,1,2 Seif Nasir,2 Gary L Beck Dallaghan,3 Kari L Nelson,2,4 Daniel A Harter,1 Samir Atiya,1 Pranav S Renavikar,1 Michael Miller5
1Department of Pathology and Microbiology, University of Nebraska Medical Center, Omaha, NE, USA; 2Office of Medical Education, College of Medicine, University of Nebraska Medical Center, Omaha, NE, USA; 3Office of Medical Education, University of North Carolina, Chapel Hill, Chapel Hill, NC, USA; 4Office of Graduate Medical Education, University of Nebraska Medical Center, Omaha, NE, USA; 5Department of Psychiatry and Behavioral Sciences, University of Texas Medical Branch, Galveston, TX, USA
Correspondence: Kari L Nelson, Email [email protected]
Purpose: Prior studies suggest a role for promoting recognition of generational differences as a part of workplace ethics. To our knowledge, there is no published comprehensive analysis demonstrating how commonly or by what methods intergenerational dynamics are taught as structured coursework in medical school curricula. To address this gap, we carried out a survey of curriculum leaders of US medical schools to assess the current practices and attitudes toward content related to generational differences in medical school coursework.
Methods: A survey consisting of 23 closed- and open-ended questions that aimed to assess the presence, characteristics, and attitudes of participants towards intergenerational dynamics in medical school coursework was disseminated via email. Curriculum deans at 154 allopathic medical schools were invited to complete the survey and sent one reminder email. Quantitative responses were descriptively analyzed, and qualitative responses were thematically analyzed.
Results: The response rate was 38.3%, with the majority (58%) of responding institutions stating that their curriculum did not include coursework on intergenerational dynamics. When taught, the most frequent method of instruction was small-group activities. Most stated that the educational content for intergenerational dynamics has been part of their curriculum for fewer than five years. In total, 34% of respondents agreed that some form of education about intergenerational dynamics should be required during medical education as they felt that content could improve cultural competence. Those that were less supportive of inclusion of intergenerational material stated concerns about stereotyping and the value of generational descriptions.
Conclusion: Our findings show a heterogeneity of responses on the perceptions and practice of curriculum leaders regarding inclusion of content related to intergenerational differences in medical school education. In summary, we present the first work assessing current practices and attitudes toward content related to the inclusion of material on intergenerational dynamics in undergraduate medical education in US allopathic medical schools.
Keywords: intergenerational dynamics, medical school, teaching, curriculum
Introduction
The concept of intergenerational dynamics is an examination of how differences in generations’ perspectives, preferences, and expectations impact how individuals interact. The role that generational differences play in many work settings has received increasing attention in both the popular press and academic literature.1–3 Discussions about potential generational differences may be of particular importance as institutions strive to foster a more inclusive, collaborative workforce.4
The theory behind viewing interactions through a generational lens is predicated on the belief that shared experiences, with relation to popular culture, world events, and emerging technologies during youth have a common impact on adult preferences and expectations. While differences between generations’ views and the challenges these engender is nothing new, we currently live in an unprecedented time in which at least five generational groups are regularly interacting in society. These groups are generally considered, traditionalists (born 1925–1945), baby boomers (born 1946–1964), generation X (born 1965–1980), millennials (born 1981–2000), and generation Z (born 2001–2020).4 Multiple surveys have suggested that workplace conflict could be attributed to or exacerbated by generational differences.4–7 However, others have expressed concerns about formally recognizing or teaching about intergenerational dynamics as it could lead to stereotyping.2
Due to the criticality of effective interpersonal interactions, there is likely no area in which an understanding of generational differences is more imperative than in the health professions. The ability of providers and patients to communicate effectively, determine goals, and develop a shared plan for promoting health and managing disease requires a fundamental understanding of each other’s point of view.8 As such, knowledge of potential generational tendencies may be of value for healthcare providers.
Prior studies point toward creating an awareness of generational descriptions and/or areas of potential intergenerational tension amongst residents and faculty by inclusion in formal curricula (eg, workshops, lectures, etc.). Sharing descriptions of possible generation-specific traits was shown to be an effective strategy to solve student-teacher as well as doctor-patient communication challenges.8–11 While these studies suggest a role for promoting intergenerational dynamics as a part of workplace ethics, there has not been a comprehensive analysis to demonstrate how commonly or by what methods intergenerational dynamics are taught as structured coursework in medical school curricula.
To address this gap, we carried out a survey of curriculum leaders of allopathic US medical schools that aimed to evaluate the current trends and attitudes toward content related to generational differences in medical school coursework. Therefore, the goal of this exploratory study was to better understand the current practices and perceptions of incorporating intergenerational dynamics material into medical school curricula.
Methods
Previously conducted surveys related to medical education curricula and attitudes toward curricular change were reviewed.7–11 Using these instruments as a guide, we developed a survey to explore the extent to which intergenerational dynamics are incorporated into medical school curricula. The survey inquired about curricular content, source materials, modality of content delivery, and number of hours in the curriculum. Participants were also asked to indicate their agreement on a number of questions using a 1 to 5 Likert scale (1=strongly disagree to 5=strongly agree). For those participants who indicated they did not include this content, questions were posed to better understand why.
Prior to distributing the survey, the authors invited content and survey experts to review the questions for clarity. The 23-item survey consisted of multiple choice, multiple answer, and open-ended questions. The survey is available as Supplement File 1 . The study was approved by the Institutional Review Board of the University of Nebraska Medical Center (873-19-Ex) and conducted in accordance with the Declaration of Helsinki. By completing the survey, respondents were notified they were consenting to the use of their de-identified data in the study, which was stated in the introductory statement of the survey.
Curriculum deans from 154 allopathic medical schools were invited to respond to the survey via email. Medical schools were identified using the Liaison Committee on Medical Education (LCME) listing of accredited medical schools. From this list, contacts and email addresses were obtained from their public website. The survey was distributed via the SurveyMonkey online platform. One follow-up email was sent two weeks after the invitation and data collection was closed four weeks after the survey link was initially emailed. Introductory comments on the survey included details regarding the information it was intended to collect, a definition of intergenerational dynamics, as well as a statement regarding the anonymity of responses at the beginning of the questionnaire. Survey items were not set to require completion in case the question was not relevant for the respondent’s institution. Multiple choice and multiple answer responses were analyzed using descriptive statistics. The responses were summarized using IBM SPSS v. 26 (Armonk, NY). Thematic analysis was used to identify patterns derived from the open-ended comments.12 Guidelines established by Braun and Clarke were used to identify themes.13
Results
Of the 154 medical institutions that were contacted, 59 participants responded (response rate 38.3%) and respondents could answer as many or few questions as they wished. Within the respondent cohort, 38 (64%) had class sizes between 101–200; 12 (20%) had class sizes greater than 200, 6 (10%) had class sizes between 51–100, and 3 (5%) had class sizes less than 50.
The majority 34 (58%) stated that their curriculum did not include coursework on intergenerational dynamics, 17 (29%) did have such coursework, and 8 (14%) were unsure if such an element existed within their curriculum. Most 9 (82%) stated that content has been part of their curriculum for less than five years (Figure 1 n=11 respondents). Twelve respondents provided additional information about the nature of their education related to this content; the results below reflect the practices of these institutions.
 |
Figure 1 Time integrational training has been included in curricula at respondents’ institutions. Values in parentheses represent the number of respondents (n=11 respondents total). |
Of the institutions that taught intergenerational dynamics content (n=12 respondents, could select more than one answer), the methods of instruction varied, with the most frequent being small-group activities 10 (83%), followed by didactic lectures 6 (50%), asynchronous modules 3 (25%), and independent coursework 2 (17%). Most respondents 9 (75%) stated that such coursework was required.
Of the responses that included this content (n=12 respondents, could select more than one answer), most 10 (83%) incorporated content into the preclinical curriculum while some 6 (50%) placed this work in the clerkship or elective phases of their curricula. Respondents reported that the material used to teach intergenerational dynamics at their institutions included self-designed materials 8 (67%), online resources 6 (50%), textbooks 1 (8%), or a combination of these resources. Over half 7 (58%) of the institutions that had intergenerational dynamics coursework included 5 hours or less of content per academic year, with the number of programs, in general, decreasing as the hours spent per year increased (Figure 2).
 |
Figure 2 Hours of content. Number of hours included for teaching intergenerational dynamics in the curricula of respondent medical schools per year. Values in parentheses represent the number of respondents (n=12 respondents total). |
Examining information provided by 44 respondents, 21 (48%) felt that the time dedicated to teaching about intergenerational dynamics was appropriate, 17 (38%) said that such coursework should increase, while 6 respondents (14%) felt it should decrease. For the following questions, n=44. Only 12 (27%) agreed or strongly agreed with the statement “I feel that our program does an adequate job of teaching concepts related to intergenerational dynamics to medical students” (Figure 3). Fewer than half 20 (45%) agreed or strongly agreed that some form of education about intergenerational dynamics should be required during medical education, while 15 (34%) of respondents were neutral. The majority 27 (61%) agreed that understanding intergenerational dynamics makes medical students better clinicians. Similarly, most respondents 30 (68%) agreed that faculty should receive training in generational differences and intergenerational dynamics. Of note, only 50% stated that they, themselves had received such instruction.
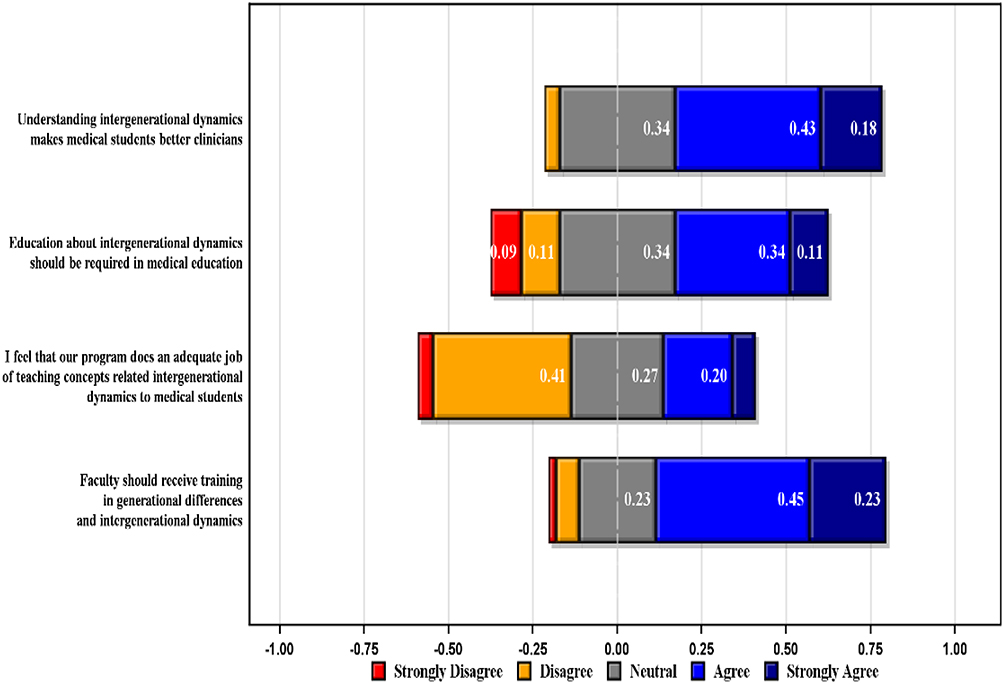 |
Figure 3 Likert-type item survey responses regarding the importance of understanding and teaching intergenerational dynamics to medical students and faculty, as well as the quality of that teaching at respondents’ institutions. Numbers are proportions of respondents. As depicted, 0.00 (gray) indicates the respondents were neutral, while negative values (yellow and red) indicate disagreement and positive values (light blue and dark blue) indicate agreement with the respective statements. |
Eighteen participants (31%) shared additional thoughts regarding teaching about intergenerational dynamics in medical education via open-ended responses. Thematic analysis resulted in four primary themes, detailed in Table 1. Respondents who supported inclusion of education about generational tendencies felt that content could improve cultural competence and noted that it would require time within the curriculum. Among those who were less supportive of inclusion of this material indicated concerns about stereotyping, questions regarding the value of generational descriptions, and possible subsumption of this content into general education about interpersonal communication.
 |
Table 1 Open-Ended Text Responses to the Survey Question “What Additional Thoughts Do You Have Regarding Teaching About Intergenerational Dynamics in Medical Education?” |
Discussion
Few studies exist in the literature that examine the utility of, or practices related to, teaching about generational differences in the health professions curricula in general, or medical school specifically. Studies on generational characteristics in healthcare are based on surveys and direct interviews.4,6,14 Generational differences analyzed through this approach are largely subjective and rely on accumulated experiences. Despite this fact, several institutions have found success in utilizing discussions of intergenerational dynamics in small settings, such as within a subspecialty residency class.7–9 Our study sought to provide a baseline understanding of the current practices of and attitudes among medical education leaders related to incorporating intergenerational dynamics in the medical school curriculum.
We found that more than 50% of responding institutions do not currently include coursework on intergenerational dynamics. Amongst the institutions that had such coursework, the favored methods of instruction were small group activities and didactic lectures. Of note, many institutions incorporated content in the preclinical curriculum. While some respondents felt that intergenerational education should be required for students and faculty, the responses were mixed. These findings show a heterogeneity of responses and perspectives on the perceptions, practice, and intentions of medical curriculum leaders regarding the subject of inter-generational differences and how, or if, it should be included in medical education.
Amongst those who supported inclusion of this content, respondents suggested that utilizing both pre-clinical and clinical years in part to teach intergenerational dynamics, with generation-specific representatives as facilitators, could prove effective. The most common concern observed amongst those against incorporating this material was the potential for generational stereotyping and divisiveness or even discrimination. Others may value the teaching of intergenerational dynamics, but think that developing an entire set of curricula is not necessary. The broad range of responses in this survey was expected. Intergenerational dynamics has enjoyed a vigorous and polarized history.2 While the coursework on professionalism and communication continues to grow in the medical school curriculum, it primarily focuses on the dynamics and teaching related to ethnicity, gender identity, or socioeconomic strata among members of the healthcare profession.15 It is interesting to note that while only most respondents were at best neutral about the need for inclusion in the curricula, the majority believed that knowledge of generational dynamics would make students better physicians.
There are limitations to the current study. Of note, the relatively low response rate and non-response bias may have impacted the results. Further, participants were limited to allopathic, US medical schools.
In summary, we present the first work assessing current practices and attitudes toward content related to intergenerational dynamics in undergraduate medical education in US allopathic medical schools. While it is outside the scope of this paper to discuss the underlying validity of intergenerational dynamics as a subject in health professions education, prior successes make it challenging to argue that the benefits generated by its adoption are entirely lacking.16 It is our hope that the current study will provide more opportunities for dialogue related to the teaching of intergenerational dynamics in medical school. For those who are interested in including this material in their teaching, the current study may provide some ideas regarding where to incorporate this content. Moving forward, additional research regarding the method, utility, and value of intergenerational dynamics as a component of medical school curriculum may prove useful.
Ethical Approval
The study was reviewed and approved by the University of Nebraska IRB (INSTITUTIONAL REVIEW BOARD) (873-19-Ex).
Acknowledgments
The authors want to thank the Alliance for Clinical Education for their support in distributing the survey.
Funding
There is no funding to report.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Urick MJ, Hollensbe EC, Masterson SS, Lyons ST. Understanding and managing intergenerational conflict: an examination of influences and strategies. Work Aging Retire. 2017;3(2):166–185.
2. Becton JB, Walker HJ, Jones-Farmer A. Generational differences in workplace behavior. J Appl Soc Psychol. 2014;44(3):175–189. doi:10.1111/jasp.12208
3. Sirias D, Karp HB, Brotherton T. Comparing the levels of individualism/collectivism between baby boomers and generation X. Manag Res News. 2007;30(10):749–761. doi:10.1108/01409170710823467
4. Stutzer K. Generational differences and multigenerational teamwork. Crit Care Nurse. 2019;39(1):78–81. doi:10.4037/ccn2019163
5. Boysen PG, Daste L, Northern T. Multigenerational challenges and the future of graduate medical education. Ochsner J. 2016;16(1):101–107.
6. Christensen SS, Wilson BL, Edelman LS. Can I relate? A review and guide for nurse managers in leading generations. J Nurs Manag. 2018;26(6):689–695. doi:10.1111/jonm.12601
7. Kelly AM, Mullan PB. Designing a curriculum for professionalism and ethics within radiology: identifying challenges and expectations. Acad Radiol. 2018;25(5):610–618. doi:10.1016/j.acra.2018.02.007
8. Moreno-Walton L, Brunett P, Akhtar S, DeBlieux PMC. Teaching across the generation gap: a consensus from the Council of Emergency Medicine Residency Directors 2009 Academic Assembly. Acad Emerg Med. 2009;16(s2):S19–S24. doi:10.1111/j.1553-2712.2009.00601.x
9. Krishnaraj A, Pesch AJ. Navigating generational differences in radiology. RadioGraphics. 2018;38(6):1672–1679. doi:10.1148/rg.2018180051
10. Maurer MS, Costley AW, Miller PA, et al. The Columbia Cooperative Aging Program: an interdisciplinary and interdepartmental approach to geriatric education for medical interns. J Am Geriatr Soc. 2006;54(3):520–526. doi:10.1111/j.1532-5415.2005.00616.x
11. Higgins MF, O’Gorman C. What we can learn from generational gaps; 2014.
12. Kiger ME, Varpio L. Thematic analysis of qualitative data: AMEE guide no. 131. Med Teach. 2020;429(8):846–854. doi:10.1080/0142159X.2020.1755030
13. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101. doi:10.1191/1478088706qp063oa
14. Lorio AK, Huggins CF, Leo SA, Wheeler JM, Housley SN. Smartphones and generational differences … are smartphones a barrier to successful patient interactions in the physical therapy clinic? J Phys Ther Educ. 2018;32(2):151–158. doi:10.1097/JTE.0000000000000034
15. Flores G, Gee D, Kastner B. The teaching of cultural issues in U.S. and Canadian Medical Schools. Acad Med. 2000;75(5):451–455. doi:10.1097/00001888-200005000-00015
16. Talmon G, Beck Dallaghan G, editors. Mind the Gap: Generational Differences in Medical Education. Syracuse, NY: Gegensatz Press; 2017.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.