Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Taurine Regulates the Expression of Interleukin −17/10 and Intestinal Flora and Protects the Liver and Intestinal Mucosa in a Nonalcoholic Fatty Liver Disease Rat Model
Authors Zhu FL, Huang T, Lv ZL, Liang G, Yao Z, Lan LC, Qadir A, Chen XQ, Shan QW
Received 17 October 2023
Accepted for publication 9 January 2024
Published 9 February 2024 Volume 2024:17 Pages 675—689
DOI https://doi.org/10.2147/DMSO.S440978
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Fu-Li Zhu,1,2 Ting Huang,3 Zi-Li Lv,4 Gang Liang,5 Zhen Yao,2 Lian-Cheng Lan,2 Abdul Qadir,2 Xiu-Qi Chen,2 Qing-Wen Shan2
1Department of Pediatrics, the First College of Clinical Medical Science, China Three Gorges University, Yichang Central People’s Hospital, Yichang, Hubei, 443000, People’s Republic of China; 2Department of Pediatrics, First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, 530021, People’s Republic of China; 3Guangxi Key Laboratory of Aquatic Genetic Breeding and Healthy Aquaculture, Guangxi Academy of Fishery Science, Nanning, Guangxi, 530021, People’s Republic of China; 4Department of Pathology, First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, 530021, People’s Republic of China; 5Department of Pathophysiology, School of Basic Medical Sciences of Guangxi Medical University, Nanning, Guangxi, 530021, People’s Republic of China
Correspondence: Qing-Wen Shan; Xiu-Qi Chen, Department of Pediatrics, First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, 530021, People’s Republic of China, Email [email protected]; [email protected]
Purpose: To investigate the intestinal inflammatory response and the abundance of intestinal bacteria in rats with high-fat diet (HFD)-induced nonalcoholic fatty liver disease (NAFLD) and assess the intervention effects of taurine (TAU).
Methods: Forty male Sprague-Dawley rats were randomly divided into five groups: group I, normal diet and normal saline gavage; group II, normal diet and TAU gavage; group III, HFD and normal saline gavage; group IV, HFD and TAU gavage (from the 1st week); group V, HFD and TAU gavage (from the 10th week). At the end of the 16th week, all the animals were sacrificed. Body weight, liver weight, liver function, and serum lipid levels were measured. The histopathologies of the liver and ileum were observed. The mRNA and protein expression levels of interleukin 17 (IL-17) and IL-10 in the ileum were detected by reverse transcription quantitative polymerase chain reaction (qPCR) and immunohistochemistry. Three types of bacteria were detected in intestinal feces using the 16S rDNA qPCR method.
Results: The ileal IL-17 level in group III was significantly higher than those in the other four groups (P < 0.01). The ileal IL-10 mRNA levels in group IV was significantly higher than those in groups III and V (P < 0.05), and IL-10 protein MOD levels in group III was significantly lower than those in the other four groups (P < 0.01). The numbers of Lactobacillus in group III were significantly lower than those in the other four groups (P < 0.01 or P < 0.05). The numbers of Bifidobacteria in groups IV and V were significantly increased compared with that in group III (P < 0.05).
Conclusion: TAU may down-regulate the expression of IL-17, up-regulate the expression of IL-10 and regulate the intestinal flora, and alleviate the liver and intestinal damage in rats with HFD-induced NAFLD.
Keywords: taurine, non-alcoholic fatty liver disease, interleukin 17, interleukin 10, intestinal barrier, gut microbiota
Introduction
With the increasing prevalence of obesity and metabolic syndrome, nonalcoholic fatty liver disease (NAFLD) has become a serious public health problem worldwide. A meta-analysis in 2022 revealed that the overall prevalence of NAFLD worldwide was estimated to be 32·4%, with a prevalence of 31.6% in Asia, 32·6% in Europe, 47·8% in North America, and 56·8% in Africa.1 In particular, the epidemiology of NAFLD in children from 2015 to 2020 showed that the estimated prevalence of NAFLD in children with obesity was 26%.2 NAFLD is a systemic and multifactorial disease that involves multiple organs, including the liver, adipose tissue and intestine, as well as organelles such as the endoplasmic reticulum and mitochondria.3,4
The pathogenesis of NAFLD is complex and ambiguous, and no approved standardized treatment for the disease is currently available. Dietary and lifestyle interventions remain the primary non-pharmacological treatments for NAFLD. Therefore, novel therapies with high efficacy and fewer side effects must be explored. Taurine (TAU; 2-amino ethane sulphonic acid) is a sulfur-containing amino acid involved in various physiological functions such as bile salt conjugation, cell membrane stabilization, antioxidation, and immunomodulation.4,5 Global epidemiological studies have demonstrated that consumption of large amounts of seafood containing TAU reduces the risk of metabolic diseases such as obesity, hyperlipidemia, and diabetes.4,6 Experiments have revealed that TAU has certain preventive and therapeutic effects on NAFLD.7,8 The research by Branco RC et al9 and the available data on the anti-obesity effects of TAU are conflicting and probably influenced by species, strain, dietary background, as well as the methods, concentration, dosage, and duration of supplementation. In addition, TAU can alleviate duodenal mucosal inflammatory injury in chickens by regulating the intestinal barrier function10 and reduce the expression levels of bowel inflammatory factors in the impaired small intestinal mucosae of broilers.11 The gut-liver axis is closely associated with the progression of NAFLD, for which the gut microbiota and intestinal barrier have been considered a two critical factors.12 The occurrence of an inflammatory cytokine imbalance in NAFLD has been reported in a previous study.13 Therefore, we hypothesized that TAU might prevent and treat NAFLD by regulating intestinal cytokine levels and the barrier function, on the basis of the gut-liver axis theory. Interleukin 17 (IL-17), an important proinflammatory cytokine secreted mainly by Th17 cells, mediates the inflammatory response of the body. IL-10 is mainly secreted by Treg cells with negative immune regulation and serves an immunosuppressive role in the body. The present research examined the protective effect of TAU on the intestine in a NAFLD rat model. The aim of this study was to develop a novel formulation for clinical guidance in the prevention and treatment of NAFLD by analyzing the regulatory effect of TAU on intestinal IL-17 and IL-10 expression levels and the intestinal flora of NAFLD rats.
Materials and Methods
Animals and Diet
Forty male Sprague-Dawley rats (7–8 weeks old, weighing 180–200 g) were purchased from the Experimental Animal Center of Guangxi Medical University (Nanning, China). The composition of the high-fat feed given to the rats was as follows: 82.5% normal feed, 10% lard, 2% cholesterol, 5% yolk powder, and 0.5% sodium cholate. The animal feed was purchased from Jiangsu Xietong Pharmaceutical Bio-engineering Co., Ltd (Nanjing, China). TAU was supplied by Sigma (St. Louis, MO, USA) and dissolved in 0.9% saline for gavage. The rats in each group were housed in individually ventilated cages (with four animals per cage) with a controlled environment (temperature, 22–24°C; relative humidity, 60–65%) under a regular 12/12-h light/dark cycle at the Experimental Animal Center of Guangxi Medical University. All the animals had ad libitum access to a chow diet without allergens that was sterilized by high-pressure sterilization and to purified water. The pad material was changed 2 or 3 times a week. One week before the start of the experiment, all the rats were fed the normal diet to allow them to acclimatize to their surroundings.
The animal usage and protocol were reviewed and approved by the Guangxi Medical University Ethical Review Committee. The experimental operations and procedures were in accordance with the regulations on the administration of experimental animals and the ethical requirements of the People’s Republic of China.
Animal Experiment Design
The rats were randomly divided into five groups (the treatments were allocated by cage, eight rats/group) (The groups are shown in Table 1): group I (normal control group), rats fed with the normal diet and received normal saline (400 mg/kg/d) by gavage for 16 weeks; group II (normal prevention group), rats maintained with the normal diet and TAU (400 mg/kg/d)4 by gavage for 16 weeks; group III (HFD model group), rats received normal saline (400 mg/kg/d) by gavage in addition to HFD for 16 weeks; group IV (TAU prevention group), rats received TAU (400 mg/kg/d)4 by gavage in addition to HFD for 16 weeks; and group V (TAU treatment group), rats fed with HFD for 10 weeks, and one rat in group III was dissected to confirm the success of the fatty liver model with hematoxylin-eosin (H&E) staining, followed by TAU (400 mg/kg/d)4 gavage until the 16th week. During the experiment, three rats (two from group I and one from group V) were sacrificed due to gavage. The whole study lasted 16 weeks, during which all the animals were regularly weighed once a week.
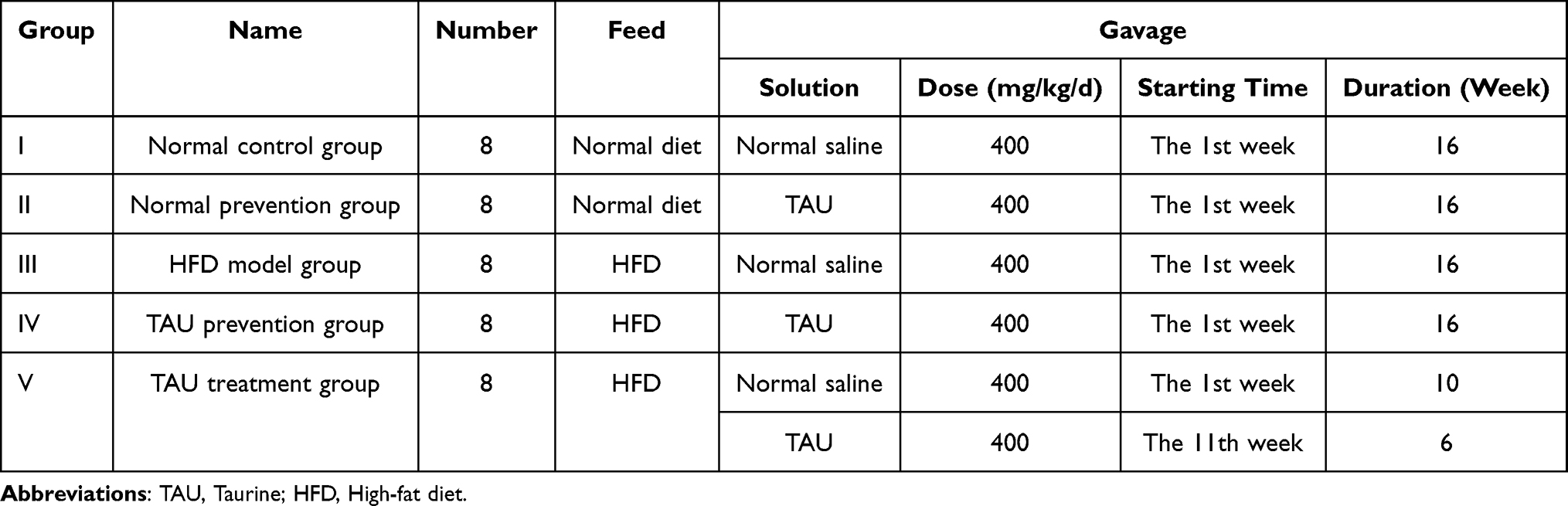 |
Table 1 Design Table of Rat Models in Five Groups |
At week 16, all rats were anesthetized by intraperitoneal injection of 20% urethane (1g/kg· BW). All the animals were intentionally exsanguinated under anesthesia. The collected blood samples were centrifuged at 3000 rpm for 15 min at 4°C to obtain serum. In addition, their livers were quickly removed and weighed. A portion of the liver was fixed in 10% formalin neutral buffer solution for H&E staining. Approximately 2.5 cm of the ileum (the distal part of the intestine located 2 cm from the ileocecal valve) was divided into three segments. One section of 1 cm was fixed in 10% formalin neutral buffer solution at room temperature for H&E and immunohistochemical stainings, one section of 1 cm was stored at −80°C for reverse transcription quantitative polymerase chain reaction (RT-qPCR), and another section at 0.5 cm of the ileum was trimmed to a size of 1 mm3 to fix in 3% glutaraldehyde solution for transmission electron microscopy (TEM) specimen preparation. Fresh stool samples from the terminal ileum were collected and stored immediately at −80°C for subsequent analysis. The above experimental design is shown in Figure 1.
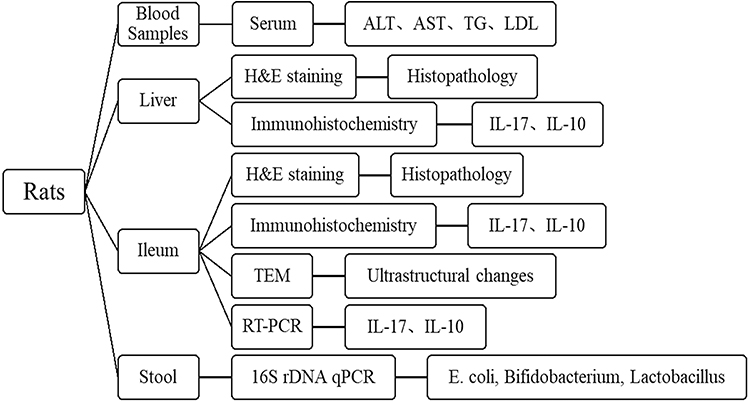 |
Figure 1 Schematic diagram of experimental design process. Abbreviations: ALT, alanine transaminase; AST, aspartate transaminase; TG, triglyceride; LDL, low-density lipoprotein.IL, interleukin; H&E, hematoxylin-eosin; TEM, transmission electron microscopy; RT-qPCR, reverse transcription quantitative polymerase chain reaction. |
Serum Biochemical Analysis
The serum levels of alanine transaminase (ALT), aspartate transaminase (AST), triglycerides (TGs), and low-density lipoprotein (LDL) were determined using an automatic biochemical analyzer, with the assistance of the clinical laboratory of the First Affiliated Hospital of Guangxi Medical University.
Histopathological Analyses of the Liver and Ileum
The liver and ileal specimens fixed in 10% formalin neutral solution were routinely dehydrated, embedded in paraffin, sectioned (at a thickness of 4 μm), and then stained with a H&E solution. Then, we examined the histopathological changes under light microscopy. The NAFLD activity score (NAS) was used for scoring liver histology by a blinded observer in accordance with the published criteria.14 The ileum histopathology was scored from 0 to 40, and the detailed criteria were described previously.15
Ultrastructural Changes of the Ileum
Small slices of the ileum were prefixed with 3% glutaraldehyde, postfixed with 1% osmium tetroxide, rinsed, gradient dehydrated, soaked, solidified, sectioned (70 nm) using an ultramicrotome, stained with lead citrate, and examined for ultrastructural changes of the ileal mucosal epithelial cells and extracellular matrix on TEM.
mRNA Expression Analysis
Total mRNA was isolated from the ilea by using a commercially available kit (TIANGEN, Inc., Beijing, China), and 2ug of RNA was reverse-transcribed into cDNA by using a high-efficiency cDNA reverse transcription kit (TIANGEN, Inc.) in accordance with the manufacturer’s instructions. The mRNA levels were quantified by quantitative PCR with the SYBR Green I chimeric fluorescence method using a US ABI 7500 fluorescence quantitative PCR instrument. The reaction systems for qPCR were as follows: 2×SuperReal PreMix Plus 10.0ul, cDNA Template 2.0ul, Forward primer (10uM) 0.6ul, Reverse primer(10uM) 0.6ul, 50×ROX Reference Dye 0.4ul, RNase-Free ddH2O 6.4u. The thermocycling conditions for qPCR were as follows: One cycle of pre-denaturation at 95°C for 15 min, followed by 40 cycles of denaturation at 9°C for 10 sec and annealing/extension at 60°C for 32 sec.The relative mRNA expression levels of IL-17 and IL-10 were finally calculated by 2−ΔΔCt relative quantitative analysis and normalized by the β-actin gene. The primer pairs used in the study are listed in Table 2.
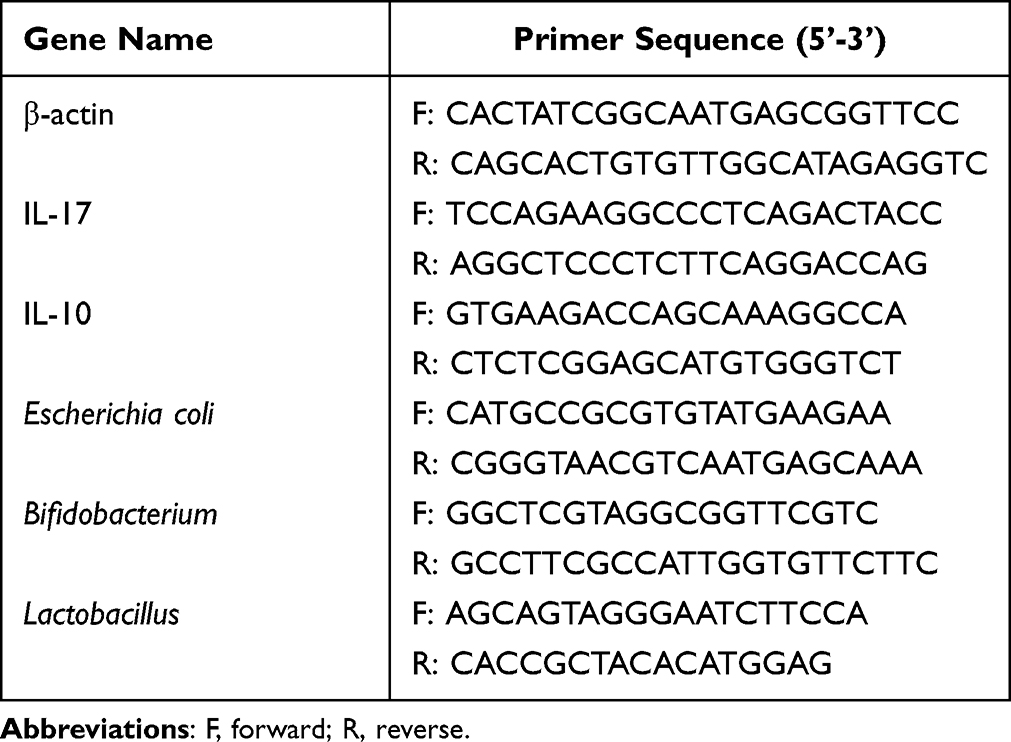 |
Table 2 Primers Used for Reverse Transcription-Quantitative PCR |
Protein Expression Analysis
The paraffin sections were immunohistochemically stained using the streptavidin-biotin method to detect the protein expressions of IL-17 and IL-10 in the ileal tissues, using primary antibodies from Bioss, Beijing, China (catalogue number: bs-1183R, bs-0698R) and secondary antibodies from ZSGB-BIO, Beijing, China (catalogue number: SP-0023). The staining results were observed and analyzed under a light microscope. After two double-blind readings by two senior pathologists, five discontinuous fields (original magnification, ×400) were randomly selected from each section. The Image-Pro Plus 6.0 pathological image analyzer (Media Cybernetics Inc.) was used to measure the fields using the optical density value method, and then the mean value was obtained, which was the mean optical density (MOD).
Quantitative Analysis of Bacteria
Rat fecal samples of 0.2 g were weighed on an electronic balance, and total DNA was extracted in accordance with the instructions of the manufacturer of the TIANamp Stool DNA Kit (TIANGEN, Inc.). After the standard strain was revived, inoculated, and cultured, DNA was obtained using the TIANamp Bacteria DNA Kit (TIANGEN, Inc.) as the standard. The primer sequences used for the bacteria genes are shown in Table 2. In accordance with the DNA absorbance (A260 value) of the three standard strains, the copy number of the 1 mL standard was calculated. The concentrations of E. coli were 4.74x1014copies/mL, Bifidobacteria 2.28x1014copies/mL and Lactobacillus 2.18x1014copies/mL. The stock solution of three standard strains was diluted by a gradient of 10X, and the standard samples were prepared with five different gradient concentrations (109–1013copies/ mL) of each bacterial DNA. qPCR amplification was performed with a PCR instrument using the absolute quantitative standard curve method. The thermocycling conditions were set as follows: One cycle of predenaturation at 95°C for 30 sec, followed by 40 cycles of denaturation at 95°C for 10 sec and annealing/extension at 60°C for 30 sec. At the end of the amplification, the standard curve equation was established in accordance with the standard curve and the correlation coefficient generated by the 7500 PCR instrument analysis system (Escherichia coli: Y = −3.208X + 53.244, R2 = 0.994, Eff% = 104.98%; Bifidobacterium: Y = −3.318X + 69.615, R2 = 0.992, Eff% = 100.15%; Lactobacillus: Y = −3.484X + 64.011, R2 = 0.994, Eff% = 93.643%). The quantities of the three major bacteria in each fecal sample were obtained by comparing the number of cycles (CT value) with the standard curve. The results were expressed as the logarithm of the bacterial gene copies per gram of stool (base 10).
Statistical Analyses
All statistical analyses were performed using the SPSS version 22.0 software. The data in this study were expressed as mean ± standard deviation (SD). Among them, NAS and ileum histological score were analyzed using Kruskal–Wallis H-tests followed by Dunn’s multiple comparison test. All the variables were compared using one-way analysis of variance, followed by the Tukey’s HSD post hoc test for multiple comparison. The correlations between the degree of intestinal inflammation and the cytokine mRNA and protein levels were analyzed using the Pearson correlation test. P values < 0.05 were considered statistically significant.
Results
Effects of TAU on Body and Liver Weights, Liver Index, Serum Lipid Profiles, and Liver Function Test results
We found no significant differences in the initial body weights among the five groups (P > 0.05) (Figure 2A). At the end of the 16th week, the body weight of the rats in group III was greater than those of the other four groups, but the difference was not statistically significant (P > 0.05) (Figure 2A). The results showed that the liver weight and index (liver weight/body weight) increased significantly in groups III, IV, and V compared with groups I and II (P < 0.05 and P < 0.01, respectively). However, no significant differences were found between groups III, IV, and V (P > 0.05) (Figure 2B and C). Furthermore, the serum ALT, AST, TG, and LDL levels of the rats that were fed a HFD increased significantly compared with those of the rats fed a normal diet (P < 0.01 or P < 0.05). When compared with group III, the serum AST and TG in group IV were significantly decreased, and the serum TG in group V was significantly decreased (P < 0.01 or P < 0.05), whereas the serum ALT and LDL levels were not significantly improved, as illustrated in Figure 2D and E.
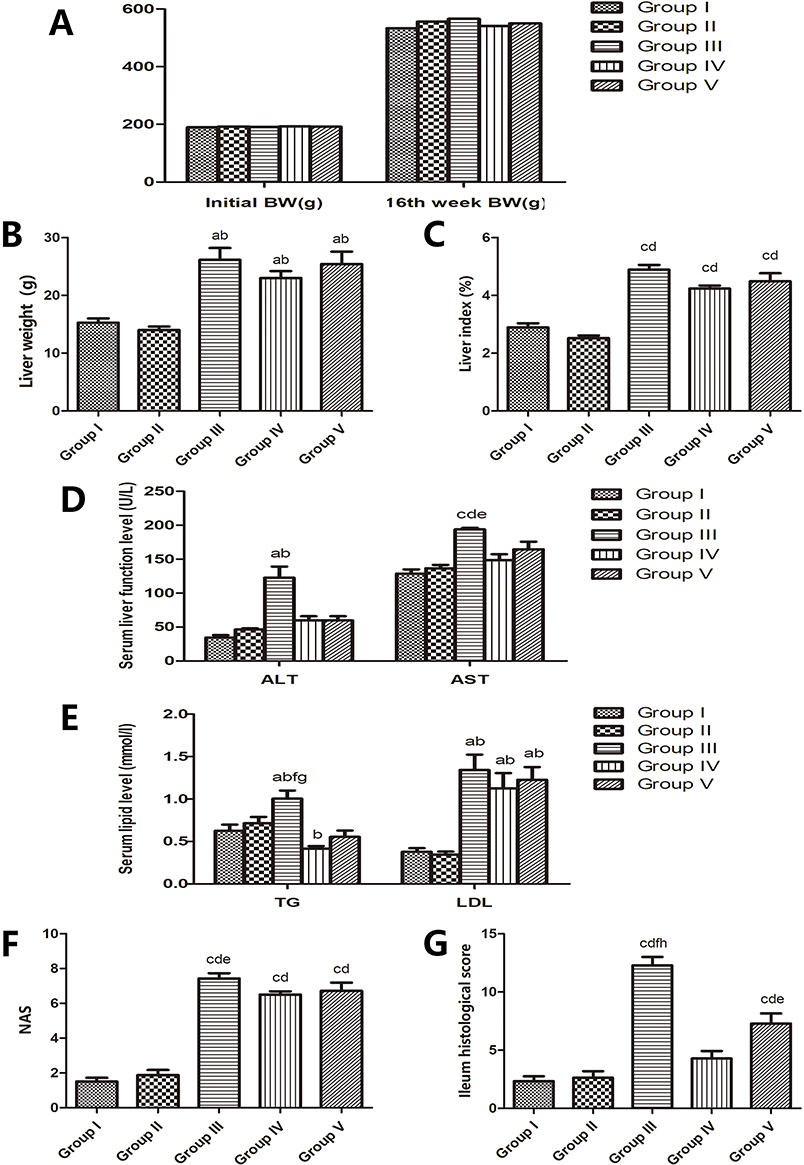 |
Figure 2 The effects of taurine administration on the physiological and serum laboratory indexes, NAS, and ileal histological scores of the rats with non-alcoholic fatty liver disease. (A) The effect on BW. (B) The effect on liver weight. a, P<0.05 compared with group I;b, P<0.05 compared with group II. (C) The effect on liver index. c, P<0.01 compared with group I; d, P<0.01 compared with group II. (D) The effect on serum liver function level. a, P<0.05 compared with group I; b, P<0.05 compared with group II; c, P<0.01 compared with group I; d, P<0.01 compared with group II; e, P<0.05 compared with group IV. (E) The effect on serum lipid level. a, P<0.05 compared with group I; b, P<0.05 compared with group II; f, P<0.01 compared with group IV; g, P<0.01 compared with group V. (F) The effect on NAS. c, P<0.01 compared with group I; d, P<0.01 compared with group II; e, P<0.05 compared with group IV. (G) The effect on ileal histological scores. c, P<0.01 compared with group I; d, P<0.01 compared with group II; e, P<0.05 compared with group IV; f, P<0.01 compared with group IV; h, P<0.05 compared with group V. Abbreviations: BW, body weight; ALT, alanine transaminase; AST, aspartate transaminase; TG, triglyceride; LDL, low-density lipoprotein; NAS, non-alcoholic fatty liver disease activity score. |
Effect of TAU on the Histopathology of the Liver
Macropathological observation revealed ruddy-colored livers in groups I and II and yellow hepatomegaly in group III. When the NAFLD rats were treated with TAU, the color of the liver turned red, more or less. When compared with that in group V, the color of the livers in group IV appeared redder (Figure 3A).
 |
Figure 3 The effects of taurine administration on the high-fat diet-fed rats. (A) Naked-eye view of the liver in the five groups. Histological appearance of the liver (B) and ileal (C) sections from the five experimental groups (original magnification, ×400). In (B) the white arrow refers to hepatic cord, the black arrow refers to normal hepatocytes, the purple arrow refers to infiltration of inflammatory cells, the green arrow refers to ballooning degeneration of hepatocytes, the yellow arrow refers to steatosis, and the blue arrow refers to focal necrosis. In (C) the black arrow refers to the infiltration of inflammatory cells in the lamina propria gland, and the red arrow refers to the breakage and loss of villi. |
Histological examinations revealed normal livers without inflammatory infiltration or fibrosis in groups I and II. Severe macrovesicular and microvesicular steatosis, infiltration of mild lobular mixed neutrophilic and mononuclear cells, even focal necrosis, marked collagen fiber deposition around the central vein and portal tracts, and severe ballooning degeneration of hepatocytes were observed in group III. After treatment with TAU, histological examinations revealed remarkable improvements in the steatosis, inflammatory, ballooning, and fibrosis compared with those in group III. In addition, the histological improvements in group IV were more remarkable than those in group V (Figure 3B).
To further examine the severity of NAFLD, the NAS was assessed in accordance with the criteria of Kleiner et al.14 The NAS in group III was significantly higher than those of groups I and II (P < 0.01) but was remarkably reduced after TAU preventive administration (P < 0.05; Figure 2F).
Effect of TAU on the Histopathology of the Ileum
Under light microscopy, the ileal mucosae of the rats in groups I and II were slender and tidy, with a complete surface structure and no inflammatory cell infiltration. However, in group III, the ileal mucosa was broken and missing, the gap was widened, and the epithelial cells were shed, showing serious infiltration of inflammatory cells mainly composed of neutrophils and lymphocytes. Compared with group III, after treatment with TAU, the ileal mucosae of the rats in groups IV and V were neat, and deletion and fracture were rare, showing less inflammatory cell infiltration (Figure 3C).
On the basis of the grading criteria of Zhao et al15 for inflammation, the histological score of the ileal mucosa was higher in group III than in groups I and II (P < 0.01) but was significantly decreased after TAU administration (P < 0.01 or P < 0.05), especially in group IV (Figure 2G).
Effect of TAU on the Ultrastructural Pathology of the Ileum
Neat and tight villi of ileal mucosal epithelial cells, long tight junctions, and normal mitochondria and endoplasmic reticulum were observed on TEM in groups I and II (Figure 4A, B, F and G). However, sparse or even missing ileal villi, shortening or disappearance of the tight junctions (Figure 4C), mitochondrial edema, endoplasmic reticulum expansion, and even completely destroyed cell structures were found in group III (Figure 4H). We also found that the ileal mucosal villi were rich and orderly, the tight junction morphology was restored, and the organelle structure was relatively complete in groups IV and V (Figure 4D, E, I and J).
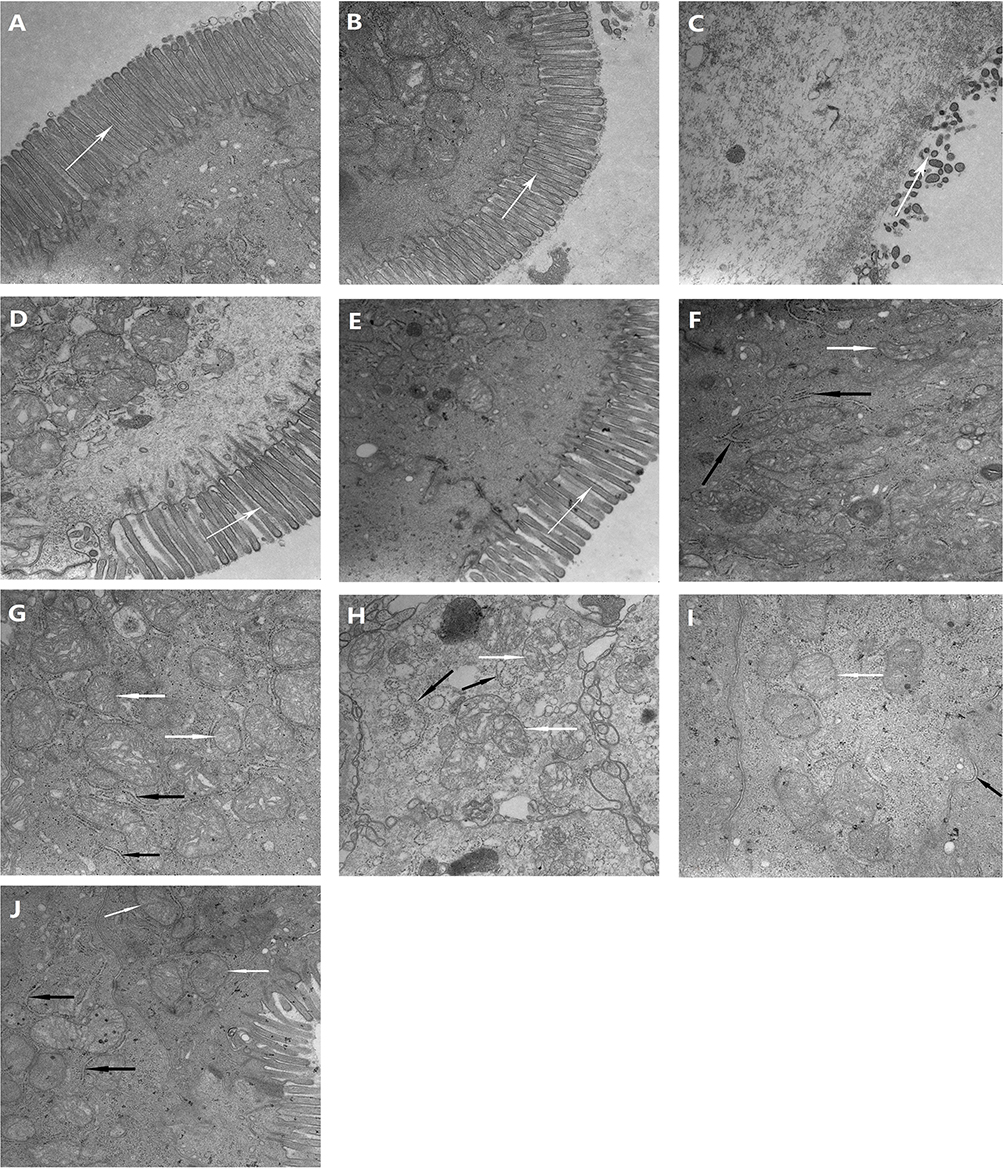 |
Figure 4 The effects of taurine administration on the ileal ultrastructure under transmission electron microscopy (TEM) (original magnification, ×30,000). (A and F) Group I; (B and G) Group II; (C and H) Group III; (D and I) Group IV; (E and J) Group V. The white arrow refers to the mitochondria, and the black arrow refers to the endoplasmic reticulum. |
Effect of TAU on the mRNA Expression Levels of Ileal Cytokines
In this study, we found that the mRNA expression level of IL-17 was increased in group III compared with groups I and II but was significantly reduced with TAU administration in groups IV and V compared with group III (P < 0.01; Figure 5A). We also found that the mRNA expression level of IL-10 was significantly increased in group IV compared with groups III and V (P < 0.05), as shown in Figure 5B.
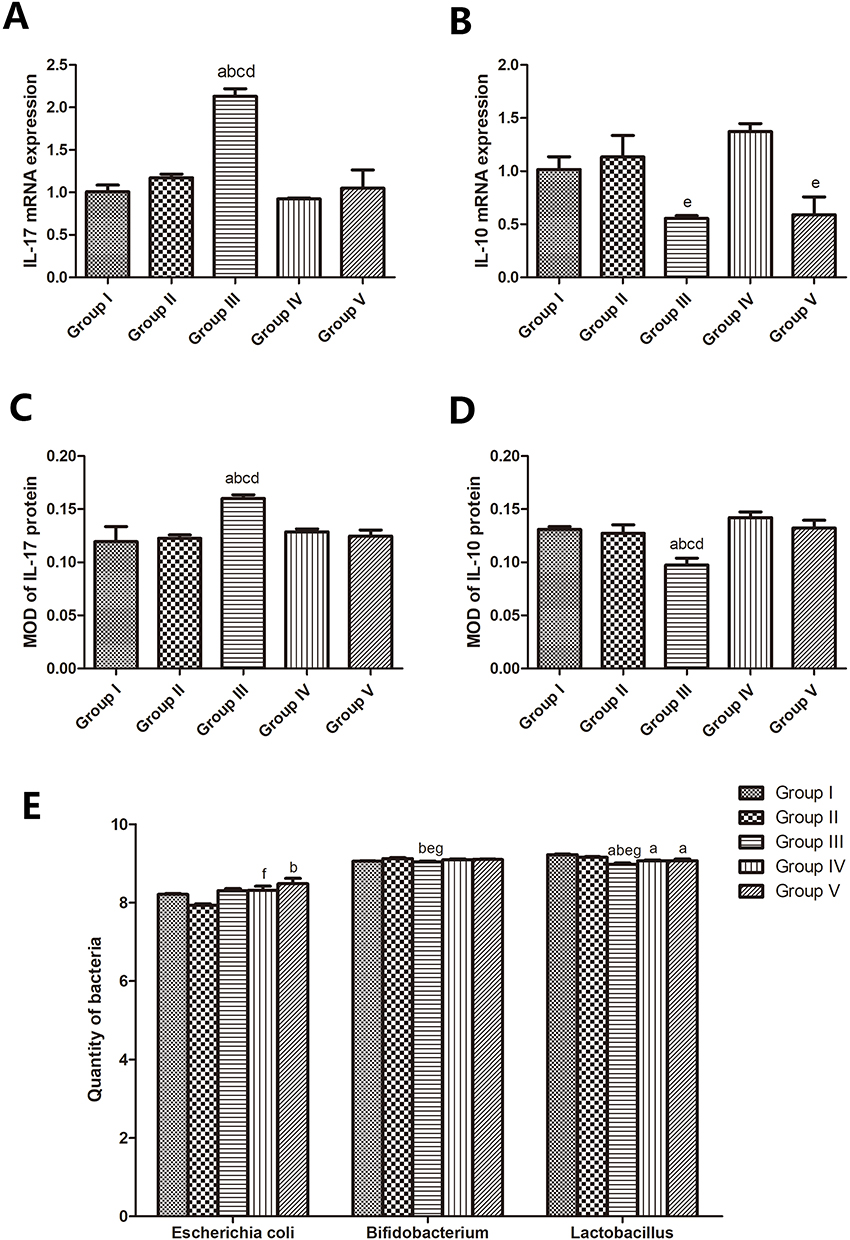 |
Figure 5 The effects of taurine administration on the mRNA expression levels and MODs of IL-17/ IL-10 in ileum, and on the quantities of the three bacteria in the intestinal fecal samples. (A) Comparison of IL-17 mRNA expression. a, P< 0.01 compared with group I; b, P<0.01 compared with group II; c, P<0.01 compared with group IV; d, P<0.01 compared with group V. (B) Comparison of IL-10 mRNA expression. e, P<0.05 compared with group IV. (C) MOD of IL-17 protein expression. a, P< 0.01 compared with group I; b, P<0.01 compared with group II; c, P<0.01 compared with group IV; d, P<0.01 compared with group V. (D) MOD of IL-10 protein expression. a, P< 0.01 compared with group I; b, P<0.01 compared with group II; c, P<0.01 compared with group IV; d, P<0.01 compared with group V. (E) Quantity of bacteria comparison. a, P< 0.01 compared with group I; b, P<0.01 compared with group II; e, P<0.05 compared with group IV; f, P<0.05 compared with group II; g, P<0.05 compared with group V. |
Effect of TAU on the Protein Expression Levels of Ileal Cytokines
Immunohistochemical staining showed that the IL-17 and IL-10 expressions were mainly distributed in the mucosal epithelial cells in the ileal mucosa. The positive protein expression was localized in the cytoplasm and cell membrane, which appeared as pale brown or tan particles. Moreover, the optical density analysis revealed that the MOD of IL-17 in group III was significantly higher than that in groups I and II, but the MOD of IL-10 in group III was significantly lower than those in the two groups (P < 0.01). However, the administration of TAU for prevention and treatment significantly reversed the increase in IL-17 expression level and the decrease in IL-10 expression level (P < 0.01; Figure 6A and B; Figure 5C and D).
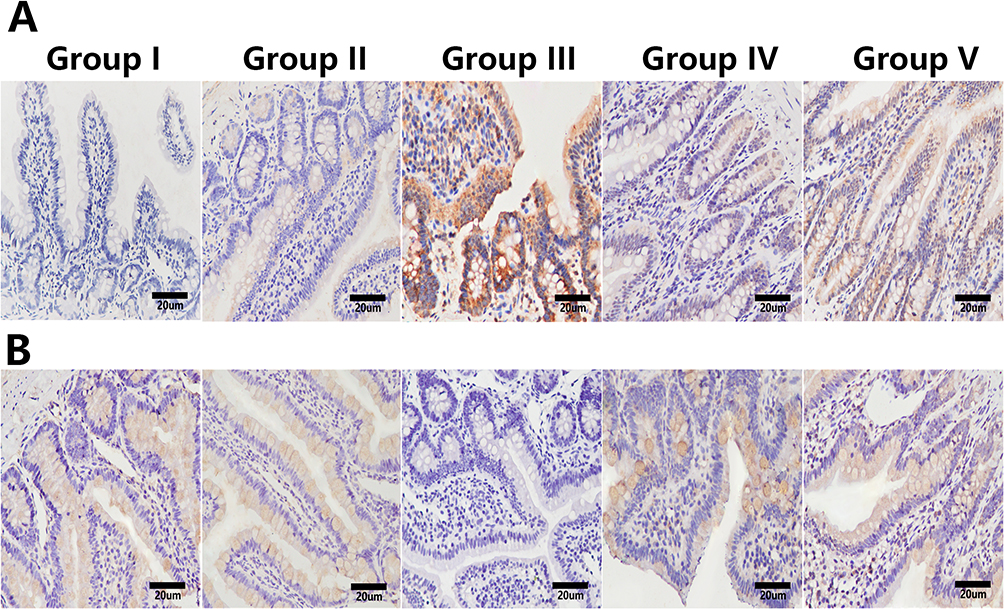 |
Figure 6 The effects of taurine administration on the protein expression levels of IL-17 and IL-10 in the ileum. Immunohistochemical stainings for IL-17 (A) and IL-10 (B) in the ileal tissues in the five groups (original magnification, ×400). IL-17 and IL-10 were mainly expressed in the cytoplasm of ileal mucosal epithelial cells, which were brownish yellow or brown when positive, but not stained when negative. |
Effect of TAU on the Gut Microbiota
Escherichia coli, as the dominant flora in G- bacteria, is an opportunistic infection bacterium that exist in the intestines of healthy people. This bacterium is also one of the harmful species most closely related to NAFLD that has been widely studied. Both Bifidobacterium and Lactobacillus are the most abundant G+ probiotics in the human intestine, and they are also beneficial bacteria that have attracted much attention in NAFLD research. In this study, three representative strains of E. coli, Bifidobacterium, Lactobacillus, and those closely related to NAFLD were screened as the research objects for quantitative detection. The quantities of Bifidobacterium and Lactobacillus were reduced in group III compared with group I (P > 0.05 and P < 0.01, respectively) and group II (P < 0.01), and remarkably increased in groups IV and V compared with group III (P < 0.05). The quantity of E. coli in group III was higher than those in groups I and II, but no significant change was observed after TAU administration in groups IV and V (P > 0.05; Figure 5E).
Correlation Analysis Between the Cytokine Expression Levels and Ileal Inflammation
The IL-17 mRNA and protein expression levels positively correlated with intestinal inflammation (r = 0.76, P = 0.001 and r = 0.714, P = 0.000, respectively), with statistically significant differences. The IL-10 mRNA and protein expression levels negatively correlated with intestinal inflammation (r = −0.612, P = 0.015 and r = −0.637, P = 0.000, respectively), with statistically significant differences.
Discussion
NAFLD, a liver disease associated with genetics-environment-metabolic stress, is becoming one of the most important public health problems in the world. NAFLD is a multifactorial and complex liver disease that is related with insulin resistance (IR) and genetic predisposition, but the underlying molecular mechanisms involved in disease development have not been fully elucidated. In a previous study, the anatomical and functional interrelationship between the intestinal mucosal barrier and the liver, also named as gut-liver axis, is increasingly recognized to be implicated in NAFLD onset and progression.16 Imbalance of gut-liver axis may arise from changes in microbiome composition and intestinal permeability.17 NAFLD is closely related to increased intestinal mucosal permeability, intestinal microbiota disorders, and intestinal immune dysfunction.18 Although accumulating evidence has shown that TAU administration could prevent NAFLD in different animal models,4,19,20 the mechanisms are still not fully understood.
In the present study, NAFLD was successfully replicated by feeding with HFD for 16 weeks, in a similar manner as described in previous studies.21,22 In addition, the level of the proinflammatory factor IL-17 in the intestinal mucosa was significantly increased, and that of the anti-inflammatory factor IL-10 was significantly decreased, consistent with the report of Liu et al23 of changes in the expression levels of the inflammatory factors in the liver of a NAFLD model, thus proving that NAFLD is associated with intestinal immune dysfunction. The pathological score and inflammation of the ileal mucosa increased with the changes in the expression levels of IL-17 and IL-10. This indicates significant differences in the expression levels of inflammatory cytokines in the intestine of the NAFLD rats and that the occurrence and development of the disease were related to intestinal inflammatory response. According to our analysis, due to the reduced secretion of intestinal mucus and antimicrobial peptides, impaired tight junctions and increased intestinal permeability in NAFLD,24 pathogenic agents cross the barrier, enter the liver through the gut-liver circulation, activate Kupffer cells to release a series of inflammatory cytokines, and finally induce inflammation of intestinal and liver.
The experimental results showed that liver steatosis was also observed in the rats in groups IV and V, which were given TAU intervention. However, The decrease of NAS suggested that TAU had a role in alleviating hepatic inflammatory injury, and the reduction of AST and TG levels indicated that TAU had a good effect on reducing enzymes and improving lipid metabolism, which may have been related to the role of TAU in bile salt binding, antioxidation and immune regulation. Notably, the serum levels of ALT and LDL were not significantly reduced by TAU, which might be related to the sample size, which was indeed a potential limitation of the present study and needs to be improved in future studies. Furthermore, the intestinal pathological score and degree of inflammation were reduced, indicating that TAU administration could not only alleviate liver damage but also delay the progression of intestinal inflammation in the rats by regulating the expression levels of IL-17/IL-10. This might be because TAU could directly induce the polarization of adipose tissue macrophages toward an M2-like phenotype, thereby reducing the expression levels of proinflammatory factors and increasing the expression levels of anti-inflammatory factors.25 Second, TAU neutralized the hypochlorous acid in the inflammatory site to generate TAU chloramine, which directly inhibited the polarization of M1 macrophages and expression of proinflammatory mediators.25 Therefore, TAU may serve an immunomodulatory role by directly or indirectly regulating the polarization of macrophages in adipose tissue in NAFLD to inhibit the inflammatory response of the body and reduce inflammatory injuries to the liver and intestine.
Intestinal barrier dysfunction is associated with various liver diseases.26 The mechanical barrier is mainly composed of intact intestinal mucosal epithelial cells, and the biological barrier is composed of the intestinal microbiota. In the present study, light microscopy, TEM and quantitative detection of intestinal bacteria were used to observe changes in the ileal epithelium morphology, ultrastructure, and number of intestinal bacteria to detect intestinal mechanical and biological barrier dysfunctions in NAFLD. In group III, on TEM, the intestinal villi, tight junctions, and organelles were damaged to varying degrees, or even missing. Additionally, the epithelial structure of the ileal mucosa was significantly damaged under light microscopy, indicating that the mechanical barrier function of the intestinal mucosa was damaged, and the intestinal permeability was increased, which was consistent with previous reports.27 Through the quantitative determination of the three main bacteria in the intestine, it was found that the number of Lactobacilli in the HFD group was significantly lower than that in the normal diet group (groups I and II), but the number of E. coli was not significantly changed, and the number of Bifidobacteria was not significantly different from that in group I, which is not consistent with a previous report.28 In addition to considering the limitations of sample size and testing methods, this discrepancy may also be related to the different sample sources and conditions. Moreover, because of the grouping by cage, different microecosystems were established between the rats in each cage and the environment, which also affected the composition of the gut microbiota. Therefore, in order to reduce the interference of external environment and sampling conditions on samples, the stool specimens in the present study were collected from fresh feces from the terminal ileum.This may be an advantage of the present study; however, it lacks theoretical support at present and needs further verification by future experiments.
After the TAU intervention, in groups IV and V, complete intestinal mucosal villi were observed under a light microscope. On TEM, the morphology and structure of the intestinal villi, tight junctions, and organelles were improved. According to Lopez-Escalera et al,24 the increased intestinal permeability in patients with fatty livers was related to the interruption of tight junctions. Thus, we hypothesize that TAU can repair the intestinal mucosal epithelial structure and reduce intestinal permeability, thereby repairing the damaged intestinal mechanical barrier. TAU can directly scavenge oxygen free radicals at the membrane level, inhibit membrane lipid peroxidation and stabilize cell membranes.29 By conducting experiments and analyses, it was revealed that the mechanism of action of TAU to protect the intestinal mucosa from oxidation and free radicals may be based on the antioxidant effect, thereby repairing the intestinal mucosa. Second, the numbers of Bifidobacteria and Lactobacilli in groups IV and V were significantly higher than those in group III. However, the number of E. coli in groups IV and V was not significantly different from that in group III. We hypothesize that TAU may partially regulate the composition of intestinal microbes to protect the intestinal biological barrier. The intervention effect of TAU on the intestinal microecology of NAFLD has rarely been reported, and the specific mechanism and reasons need further study. In previous years, intestinal inflammation and increased permeability of intestinal epithelial cells have been reported to possibly lead to increased translocation of numerous intestinal microorganisms associated with NAFLD progression.24,30 From these findings, it can be inferred that TAU administration may indirectly affect the intestinal flora by repairing the intestinal mechanical barrier and reducing intestinal permeability and bacterial translocation. In the present study, only single genes of three bacteria were used as research objects instead of metagenomes, and the impact of different cage living environment on intestinal microecology was ignored, which are indeed potential limitations of the current study. In future research, the above experimental design will be improved and high-throughput sequencing for metagenomics of gut microbes will be performed.
In the present study, in terms of ileum pathological score and IL-10 mRNA expression, the TAU prevention group showed more advantages than the treatment group. In addition to the intervention course, it might also be related to the long-term antioxidant and immunomodulatory effects of TAU. Oxidative stress and immune inflammation are important links in the pathogenesis of NAFLD.31 The preventive use of TAU may prevent further progression of the disease by alleviating oxidative stress and reducing the expression of inflammatory cytokines, but the specific mechanism remains to be further studied.
Conclusion
In summary, the present study demonstrated that TAU has protective effects on HFD-induced NAFLD, such as reduction of the liver weight and index, liver steatosis, and inflammation. Furthermore, TAU may down-regulate the expression of IL-17, up-regulate the expression of IL-10 and regulate the intestinal flora, and alleviate the liver and intestinal damage in rats with HFD-induced NAFLD.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval
The animal usage and protocol were reviewed and approved by the Guangxi Medical University Ethical Review Committee (no. 2019 KY-126). The experimental operations and procedures were in accordance with the regulations on the administration of experimental animals and the ethical requirements of the People’s Republic of China.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Key Laboratory of Children’s Disease Research in Guangxi’s Colleges and Universities, Education Department of Guangxi Zhuang Autonomous Region and the Development and Promotion Application Project of Guangxi Medical and Health Appropriate Technology of China (S2017035).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Riazi K, Azhari H, Charette JH, et al. The prevalence and incidence of NAFLD worldwide: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2022;7(9):851–861. doi:10.1016/S2468-1253(22)00165-0
2. Shapiro WL, Noon SL, Schwimmer JB. Recent advances in the epidemiology of nonalcoholic fatty liver disease in children. Pediatr Obes. 2021;16(11):e12849. doi:10.1111/ijpo.12849
3. Li X, Wang H. Multiple organs involved in the pathogenesis of non-alcoholic fatty liver disease. Cell Biosci. 2020;10(1):140. doi:10.1186/s13578-020-00507-y
4. Abd Elwahab AH, Ramadan BK, Schaalan MF, et al. A novel role of sirt1/ fgf-21 in taurine protection against cafeteria diet-induced steatohepatitis in rats. Cell Physiol Biochem. 2017;43(2):644–659. doi:10.1159/000480649
5. Rafiee Z, García-Serrano AM, Duarte JMN. Taurine Supplementation as a Neuroprotective Strategy upon Brain Dysfunction in Metabolic Syndrome and Diabetes. Nutrients. 2022;14:1292. doi:10.3390/nu14061292
6. Sagara M, Murakami S, Mizushima S, et al. Taurine in 24-h urine samples is inversely related to cardiovascular risks of middle aged subjects in 50 populations of the world. Adv Exp Med Biol. 2015;803:623–636.
7. San J, Hu J, Pang H, et al. Taurine Protects against the Fatty Liver Hemorrhagic Syndrome in Laying Hens through the Regulation of Mitochondrial Homeostasis. Int J Mol Sci. 2023;24(12):10360. doi:10.3390/ijms241210360
8. Yu Z, Cheng M, Luo S, et al. Comparative Lipidomics and Metabolomics Reveal the Underlying Mechanisms of Taurine in the Alleviation of Nonalcoholic Fatty Liver Disease Using the Aged Laying Hen Model. Mol Nutr Food Res;2023. e2200525. doi:10.1002/mnfr.202200525
9. Branco RC, Batista TM, Camargo RL, et al. Long-term taurine supplementation leads to enhanced hepatic steatosis, renal dysfunction and hyperglycemia in mice fed on a high-fat diet. Adv Exp Med Biol. 2015;803:339–351.
10. Xiao M, Mi Y, Liu L, et al. Taurine regulates mucosal barrier function to alleviate lipopolysaccharide-induced duodenal inflammation in chicken. Amino Acids. 2018;50(11):1637–1646. doi:10.1007/s00726-018-2631-6
11. Yang Q, Wang Z, Cui Y, et al. Effects of taurine on bowel inflammatory factor of small intestinal mucosa impaired by heat stress in broilers. Adv Exp Med Biol. 2019;1155:1049–1056.
12. Han H, Jiang Y, Wang M, et al. Intestinal dysbiosis in nonalcoholic fatty liver disease (NAFLD): focusing on the gut-liver axis. Crit Rev Food Sci Nutr. 2023;63(12):1689–1706. doi:10.1080/10408398.2021.1966738
13. Duan Y, Pan X, Luo J, et al. Association of Inflammatory Cytokines With Non-Alcoholic Fatty Liver Disease. Front Immunol. 2022;13:880298. doi:10.3389/fimmu.2022.880298
14. Kleiner DE, Brunt EM, Van Natta M, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology. 2005;41(6):1313–1321. doi:10.1002/hep.20701
15. Zhao H, Zhang H, Wu H, et al. Protective role of 1,25(oh)2 vitamin d3 in the mucosal injury and epithelial barrier disruption in DSS-induced acute colitis in mice. BMC Gastroenterol. 2012;12(1):57. doi:10.1186/1471-230X-12-57
16. Han H, Jiang Y, Wang M, et al. Intestinal dysbiosis in nonalcoholic fatty liver disease (NAFLD): focusing on the gut-liver axis. Crit Rev Food Sci Nutr. 2023;63(12):1689–1706.
17. Hu H, Lin A, Kong M, et al. Intestinal microbiome and NAFLD: molecular insights and therapeutic perspectives. J Gastroenterol. 2020;55(2):142–158. doi:10.1007/s00535-019-01649-8
18. Hyun CK. Molecular and Pathophysiological Links between Metabolic Disorders and Inflammatory Bowel Diseases. Int J Mol Sci. 2021;22(17):9139. doi:10.3390/ijms22179139
19. Yu Z, Cheng M, Luo S, et al. Comparative Lipidomics and Metabolomics Reveal the Underlying Mechanisms of Taurine in the Alleviation of Nonalcoholic Fatty Liver Disease Using the Aged Laying Hen Model. Mol Nutr Food Res. 2023;67:e2200525.
20. Kim SH, Seo H, Kwon D, Yuk DY, Jung YS. Taurine Ameliorates Tunicamycin-Induced Liver Injury by Disrupting the Vicious Cycle between Oxidative Stress and Endoplasmic Reticulum Stress. Life. 2022;12(3):354. doi:10.3390/life12030354
21. Shang Z, Gao Y, Xue Y, et al. Shenge Formula attenuates high-fat diet-induced obesity and fatty liver via inhibiting ACOX1. Phytomedicine. 2023;123:155183. doi:10.1016/j.phymed.2023.155183
22. Yalcin EB, Tong M, Cao K, et al. High Fat Diet Mediated Alterations in Serum Sphingolipid Profiles in An Experimental Mouse Model Measured by Matrix-Assisted Laser Desorption/Ionization-Time of Flight Mass Spectrometry. Eur J Biol Biotechnol. 2023;4:25–32. doi:10.24018/ejbio.2023.4.1.135
23. Liu J, Li W, Zhu W, et al. Chronic intermittent hypoxia promotes the development of experimental non-alcoholic steatohepatitis by modulating treg/th17 differentiation. Acta Biochim Biophys Sin. 2018;50(12):1200–1210. doi:10.1093/abbs/gmy131
24. Lopez-Escalera S, Lund ML, Hermes GDA, et al. In Vitro Screening for Probiotic Properties of Lactobacillus and Bifidobacterium Strains in Assays Relevant for Non-Alcoholic Fatty Liver Disease Prevention. Nutrients. 2023;15:2361. doi:10.3390/nu15102361
25. Murakami S. The physiological and pathophysiological roles of taurine in adipose tissue in relation to obesity. Life Sci. 2017;186:80–86. doi:10.1016/j.lfs.2017.08.008
26. Shi L, Jin L, Huang W. Bile Acids, Intestinal Barrier Dysfunction, and Related Diseases. Cells. 2023;12(14):1888. doi:10.3390/cells12141888
27. Mao JW, Tang HY, Zhao T, et al. Intestinal mucosal barrier dysfunction participates in the progress of nonalcoholic fatty liver disease. Int J Clin Exp Pathol. 2015;8:3648–3658.
28. Zhou Y, Zhao S, Jiang Y, et al. Regulatory function of buckwheat-resistant starch supplementation on lipid profile and gut microbiota in mice fed with a high-fat diet. J Food Sci. 2019;84:2674–2681. doi:10.1111/1750-3841.14747
29. Zuhal Y, Nedret K, Cigdem O, et al. Effects of taurine in cellular responses to oxidative stress in young and middle-aged rat liver. Ann N Y Acad Sci. 2007;1100:553–561. doi:10.1196/annals.1395.061
30. Di Ciaula A, Baj J, Garruti G, et al. Liver Steatosis, Gut-Liver Axis, Microbiome and Environmental Factors. A Never-Ending Bidirectional Cross-Talk. J Clin Med. 2020;9(8):2648. doi:10.3390/jcm9082648
31. Clare K, Dillon JF, Brennan PN. Reactive Oxygen Species and Oxidative Stress in the Pathogenesis of MAFLD. J Clin Transl Hepatol. 2022;10(5):939–946. doi:10.14218/JCTH.2022.00067
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Therapeutic Effects of HLA-G5 Overexpressing hAMSCs on aGVHD After Allo-HSCT: Involving in the Gut Microbiota at the Intestinal Barrier
Bu X, Pan W, Wang J, Liu L, Yin Z, Jin H, Liu Q, Zheng L, Sun H, Gao Y, Ping B
Journal of Inflammation Research 2023, 16:3669-3685
Published Date: 24 August 2023
Portulaca Oleracea L. as a Potential Therapeutic Drug Intervention in Ulcerative Colitis: Mechanisms of Action and Clinical Studies
Liu XY, Liu ZX, Tan WW, Zhang WB, Zhang YL, Zheng L, Que RY, Wen HZ, Dai YC
Drug Design, Development and Therapy 2024, 18:5931-5946
Published Date: 11 December 2024
Metagenomic Sequencing Combined with Metabolomics to Explore Gut Microbiota and Metabolic Changes in Mice with Acute Myocardial Infarction and the Potential Mechanism of Allicin

Gao Y, Qin G, Liang S, Yin J, Wang B, Jiang H, Liu M, Luo F, Li X
Drug Design, Development and Therapy 2025, 19:771-791
Published Date: 3 February 2025
Coix Seed Oil Alleviates DSS-Induced Ulcerative Colitis via Intestinal Barrier Repair and Ferroptosis Regulation
Zeng YX, Li NR, Deng BY, Gu YF, Lu SF, Liu Y
Journal of Inflammation Research 2025, 18:2557-2581
Published Date: 20 February 2025
Si-Ni Decoction as a Potential Treatment for Ulcerative Colitis: Modulation of Gut Microbiota and AKT1 Inhibition Through Network Pharmacology and in vivo Validation
Shi L, Chen L, Jin G, Yang Y, Zhu F, Zhou G
Journal of Inflammation Research 2025, 18:6263-6280
Published Date: 14 May 2025