Back to Journals » Journal of Pain Research » Volume 18
Targeting Kinesiophobia After Thoracic Surgery with an Integrated Protection Motivation and Exposure Intervention: A Randomized Controlled Trial
Authors Peng J, Luo Y ![]() , Feng L, Xiao J, Feng F, Zheng Y, Bao L, Yang S, Wu X
, Feng L, Xiao J, Feng F, Zheng Y, Bao L, Yang S, Wu X
Received 18 June 2025
Accepted for publication 18 November 2025
Published 19 December 2025 Volume 2025:18 Pages 6911—6920
DOI https://doi.org/10.2147/JPR.S544205
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Jiao Peng,1,* Yang Luo,2,* Lijuan Feng,2 Juan Xiao,2 Fang Feng,2 Yi Zheng,2 Lihong Bao,3 Sai Yang,3 Xiao Wu2
1Department of Respiratory and Critical Care Medicine, Wuhan Fourth Hospital, Wuhan, Hubei Province, People’s Republic of China; 2Department of Thoracic Surgery, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 3Department of Nursing, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiao Wu; Sai Yang, Email [email protected]; [email protected]
Background: Kinesiophobia is a significant barrier to recovery after thoracic surgery. We aimed to determine the efficacy of an integrated intervention combining Protection Motivation Theory (PMT) and exposure therapy for reducing kinesiophobia and improving postoperative outcomes.
Methods: In this single-center, randomized, double-blind, controlled trial, we enrolled 144 patients with kinesiophobia (Tampa Scale for Kinesiophobia [TSK-17-C] score ≥ 37) following thoracoscopic pulmonary surgery. Participants were randomized 1:1 to receive either a structured PMT-based psychological and graded exposure-behavioral intervention on postoperative day 1 (POD1) (experimental group, n=72) or routine care with standard pain education (control group, n=72). The primary outcome was the TSK-17-C score on POD3.
Results: The experimental group exhibited a significantly lower adjusted mean TSK-17-C score on POD3 compared to the control group (28.26 vs 36.13, respectively; adjusted mean difference, − 7.86; 95% CI, − 8.37 to − 7.35; P < 0.001). The intervention also led to a more improved pain trajectory (P=0.048 for time-by-group interaction) and superior cough capacity on POD3 (P < 0.001). The intervention was safe and well-tolerated.
Conclusion: An integrated psychological-behavioral intervention combining PMT and exposure therapy effectively reduces kinesiophobia, alleviates pain, and improves cough capacity in the early postoperative period for patients undergoing thoracic surgery. This nurse-led protocol provides a non-pharmacological approach that may enhance recovery and help mitigate the “pain-fear-avoidance” cycle.
Keywords: kinesiophobia, thoracic surgery, protection motivation theory, exposure therapy, postoperative recovery, pain management, randomized controlled trial
Introduction
Postoperative pain is a significant clinical challenge, frequently instigating kinesiophobia—a fear of movement-related pain that adversely impacts patient prognosis across diverse surgical populations. Its prevalence is particularly striking in major orthopedic and cardiac surgeries, with reported incidence rates ranging from 35% after total knee arthroplasty1,2 to over 80% following spinal and cardiac procedures.3–6 In patients undergoing thoracic surgery, kinesiophobia often culminates in the avoidance of essential recovery behaviors like deep breathing, coughing, and early ambulation.7 This avoidance not only impedes recovery but also elevates the risk of severe complications, such as pulmonary infections and deep vein thrombosis (DVT), thereby prolonging hospitalization and compromising long-term quality of life.8–10
The Fear-Avoidance Model provides a framework for this phenomenon, positing that catastrophic pain interpretation fosters a self-perpetuating cycle of fear, avoidance, and functional decline.11 While extinction theory suggests that breaking this cycle requires disrupting the anticipated link between movement and pain—the core principle of exposure therapy—initiating this process is challenging, as profound fear prevents patients from attempting the necessary activities in the first place.12 Traditional management, relying on pharmacological analgesia and generic health education, often fails to address this core psychological barrier.13,14
To overcome this clinical impasse, our study introduces an innovative intervention that integrates Protection Motivation Theory (PMT) with graded exposure therapy. PMT aims to enhance patients’ intrinsic motivation for rehabilitation by reinforcing their appraisal of both the threats of inactivity and their own coping capacity.15 This motivational enhancement serves as a crucial prerequisite for graded exposure therapy, which, administered under preemptive analgesia, allows patients to safely experience that movement does not lead to catastrophic pain. This “expectancy violation” directly challenges maladaptive cognitions and facilitates the extinction of kinesiophobia.16
To our knowledge, research systematically combining PMT with exposure therapy in thoracic surgery patients remains scarce. We therefore hypothesized that this integrated intervention, compared to routine care, would more effectively reduce kinesiophobia, alleviate postoperative pain, and improve functional recovery. Accordingly, this randomized controlled trial was designed to evaluate the efficacy of our protocol.
Methods
Study Design and Ethics
This was a prospective, single-center, randomized, double-blind (patient and assessor), parallel-controlled clinical trial conducted at Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China. This study was approved by the Medical Ethics Committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (Approval No.: 20230987; Approval Date: January 1, 2024). Written informed consent was obtained from all participants prior to enrollment. The trial was registered with the Chinese Clinical Trial Registry (Registration No.: ChiCTR2400080205; Registration Date: January 23, 2024).
Study Participants
Participants were enrolled from January 23, 2024, to May 31, 2024.
Inclusion Criteria
(1) Age ≥18 years; (2) Scheduled for elective thoracoscopic pulmonary surgery; (3) Score ≥37 on the Chinese version of the Tampa Scale for Kinesiophobia (TSK-17-C)17 on the morning of postoperative day 1 (POD1); (4) Conscious and capable of effective verbal communication and questionnaire comprehension; (5) Voluntarily agreed to participate and provided signed informed consent.
Exclusion Criteria
(1) Postoperative admission to the Intensive Care Unit (ICU); (2) Requirement for a second surgery during the study period; (3) Postoperative contraindications to ambulation, such as circulatory instability, severe dyspnea or hypoxemia, active bleeding, or unimmobilized fractures; (4) Known or newly diagnosed psychiatric disorders or cognitive impairments precluding cooperation; (5) Concomitant systemic pain treatments or other pain etiologies that could confound results; (6) Concurrent participation in other clinical trials or a history of major surgery within the past 3 months; (7) Investigator judgment of other conditions likely to cause result bias or poor compliance.
Randomization and Blinding
Eligible patients were randomly assigned in a 1:1 ratio to either the experimental or control group using a computer-generated random number sequence. A researcher independent of recruitment and intervention managed the allocation sequence via a centralized randomization system to ensure concealment. Both participants and outcome assessors were blinded to group assignments throughout the study.
Interventions
All patients received standardized perioperative management, including consistent surgical, anesthetic, and basic postoperative analgesia protocols (eg, patient-controlled analgesia [PCA], rectal and intravenous analgesics).
Control Group
Patients in the control group received standard pain-related health education. This included information on the causes and importance of postoperative pain, assessment methods, analgesic effects and side effects, and a brief introduction to non-pharmacological pain relief methods. The content was delivered via a booklet and a one-time explanation by a research nurse.
Experimental Group
In addition to routine care, patients in the experimental group received an integrated psychological-behavioral intervention combining PMT and graded exposure therapy. The intervention was delivered by a specially trained research nurse following a standardized operating procedure (SOP) on the afternoon of POD1, after eligibility was confirmed by the morning TSK-17-C assessment. The intervention aimed to facilitate safe and effective completion of key early activities through cognitive restructuring and behavioral experiences, and to collaboratively establish daily postoperative activity goals. Intervention materials included a PMT education manual, a pain management leaflet, and a graded exposure activity card.
Intervention Introduction and Collaborative Goal Setting
- Personalized Communication: The research nurse initiated a therapeutic dialogue based on the patient’s TSK score, encouraging them to express specific concerns about pain, coughing, and ambulation.
- PMT-Integrated Cognitive Restructuring:
- Threat Appraisal: Using the PMT manual, the nurse clarified that postoperative pain is normal and manageable, corrected misconceptions (eg, “coughing will tear the stitches”), and emphasized the real risks of inactivity (eg, pulmonary complications, DVT), using visual aids and statistics to underscore their severity and prevalence.
- Coping Appraisal: The nurse reinforced the efficacy of multimodal analgesia, instructed on the preemptive use of PCA, and taught correct techniques for coughing (eg, incision splinting) and ambulation to bolster self-efficacy.
Graded Exposure Behavioral Intervention
After cognitive preparation and ensuring the patient’s Numerical Rating Scale (NRS) score was ≤3 (administering preemptive PCA if higher), the following activities were performed sequentially:
(1) Exposure for Coughing: The intervention progressed from psychological preparation and guided imagery to gentle huffing, and finally to effective, splinted coughing. Immediate positive feedback was provided to reinforce the cognition that coughing is safe and controllable. A goal of coughing at least once every half-hour while awake was set.
(2) Exposure for Ambulation: The intervention proceeded from in-bed preparatory movements to sitting at the bedside, standing with support, marching in place, and finally, short-distance walking. The nurse provided continuous monitoring and support. Positive feedback was used to reinforce the cognition that early ambulation is safe and beneficial. A goal of ambulating more than twice daily for a total of 20–30 minutes was established.
Consolidation and Progressive Support
On POD2 and POD3, the research nurse followed up to review progress, address any new concerns, and provide tailored education (eg, reframing increased pain as a sign of lung re-expansion). The nurse reinforced PMT cognitions and assisted with progressive activities, collaboratively adjusting daily goals to promote independence.
Outcome Measures and Assessment
All outcomes were assessed by trained personnel blinded to group allocation.
Primary Outcome Measure
Kinesiophobia: Assessed using the TSK-17-C.17 Scores range from 17 to 68, with higher scores indicating more severe kinesiophobia. Assessments were conducted on the morning of POD1 (baseline) and the afternoon of POD3.
Secondary Outcome Measures
(1) Daily Pain Intensity: Assessed using the NRS (0=no pain, 10=worst imaginable pain), recording average and worst pain over the past 24 hours. Assessments were performed on POD1 AM (baseline) and daily from POD1 PM to POD3 PM.
(2) Cough Capacity: Assessed using the Semi-Quantitative Cough Strength Score (SCSS)18 (0=no cough to 5=strong, effective cough). Assessed on POD1 AM and POD3 PM. Refusal to cough due to pain was scored as 0.
Safety and Psychological Status Outcomes
(1) Anxiety: Assessed using the Generalized Anxiety Disorder 7-item scale (GAD-7).19 Assessed at admission and on POD3 PM.
(2) Depression: Assessed using the Patient Health Questionnaire-9 (PHQ-9).20 Assessed at admission and on POD3 PM. For POD3 assessments, the timeframe prompt for both scales was modified to “since your surgery.”
Sample Size Calculation
Based on a moderate effect size (Cohen’s d = 0.5) for the primary outcome (TSK), a two-sided significance level of 0.05, and 80% power, G*Power21 3.1.9.7 indicated a required sample size of 64 participants per group. To account for a potential 10% dropout rate, we aimed to enroll 72 participants per group, for a total of 144.
Statistical Analysis
Data were analyzed using SPSS 26.0 following the intention-to-treat (ITT) principle, with multiple imputation for missing data. The primary outcome (TSK-17-C at POD3) was analyzed using ANCOVA with baseline TSK as a covariate. Daily pain intensity (NRS) was analyzed using a mixed-effects model for repeated measures (MMRM). Cough capacity (SCSS) was analyzed using the Mann–Whitney U-test. Anxiety (GAD-7) and depression (PHQ-9) at POD3 were analyzed using ANCOVA with baseline scores as covariates. A two-sided p < 0.05 was considered statistically significant.
Results
Participant Flow and Baseline Characteristics
From January 23 to May 31, 2024, 436 patients were screened. Of these, 276 (63.3%) were excluded for not meeting the TSK-17-C criterion (<37). Of the 160 eligible patients, 16 were excluded for other reasons. Ultimately, 144 patients were randomized (72 per group) and included in the ITT analysis (Figure 1). The two groups were well-balanced at baseline regarding demographic, clinical, and psychological characteristics (all p>0.05), ensuring comparability (Table 1).
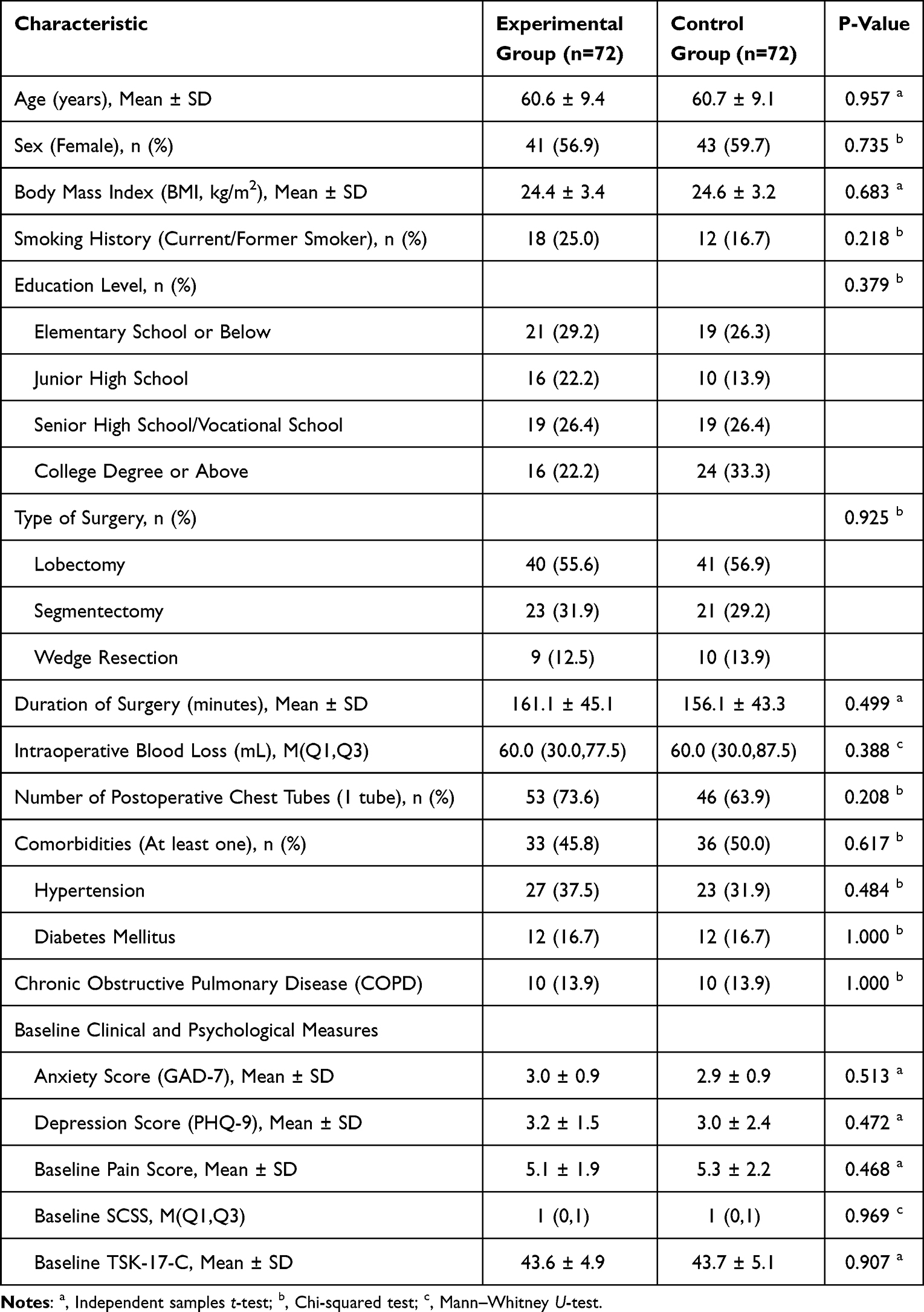 |
Table 1 Baseline Demographic and Clinical Characteristics of Participants |
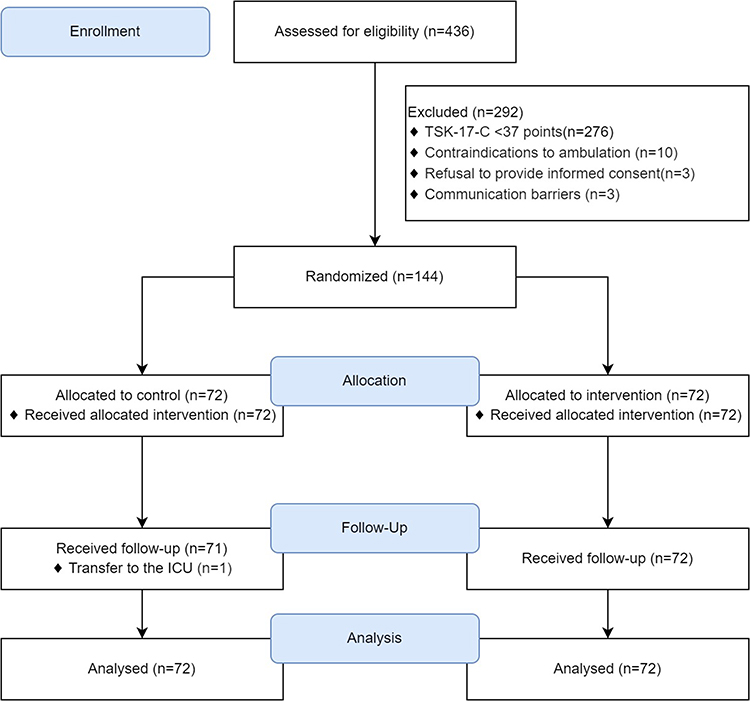 |
Figure 1 Participant Flow. |
Primary Outcome Measure
After adjusting for baseline TSK-17-C scores, ANCOVA revealed a significant main effect of the intervention on POD3 TSK-17-C scores (F(1, 141) = 927.290, P < 0.001), with the model explaining 88.0% of the adjusted variance (Adjusted R2 = 0.880). The adjusted mean TSK-17-C score was significantly lower in the experimental group (28.26 ± 0.18) than in the control group (36.13 ± 0.18). The adjusted mean difference was −7.86 (95% CI [−8.37, −7.35]; P < 0.001) (Table 2).
 |
Table 2 Comparison of Primary Outcome (TSK-17-C) at POD3, Adjusted for Baseline |
Secondary Outcome Measures
Comparison of NRS Changes Over Time
The MMRM analysis revealed significant main effects for time (F(2.81, 398.58) = 29.94, P < 0.001) and group (F(1, 142) = 6.18, P = 0.014). Crucially, a significant time × group interaction was observed (F(2.81, 398.58) = 2.71, P = 0.048), indicating different pain trajectories between groups. Pain scores in the experimental group showed a steady decline, whereas scores in the control group decreased until POD2 before slightly increasing at POD3 (Figure 2).
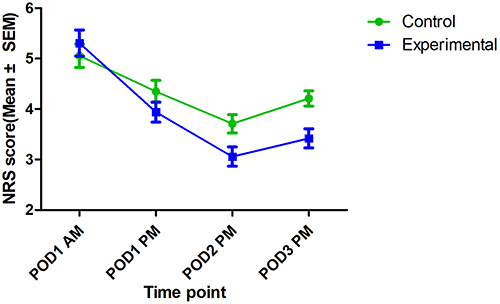 |
Figure 2 Comparison of NRS score changes over time between the two groups. |
Comparison of Cough Capacity
At POD3, the experimental group demonstrated significantly higher SCSS scores than the control group (Mann–Whitney U = 1078.500, Z = −6.200, P < 0.001), indicating superior cough capacity (Table 3).
 |
Table 3 Comparison of Cough Capacity Between Groups (POD3 PM) |
Comparison of Psychological Status (POD3 PM)
After adjusting for baseline scores, ANCOVA showed no significant between-group differences in GAD-7 scores (F(1, 141) = 0.265, P = 0.608) or PHQ-9 scores (F(1, 141) = 0.426, P = 0.515) at POD3 (Table 4).
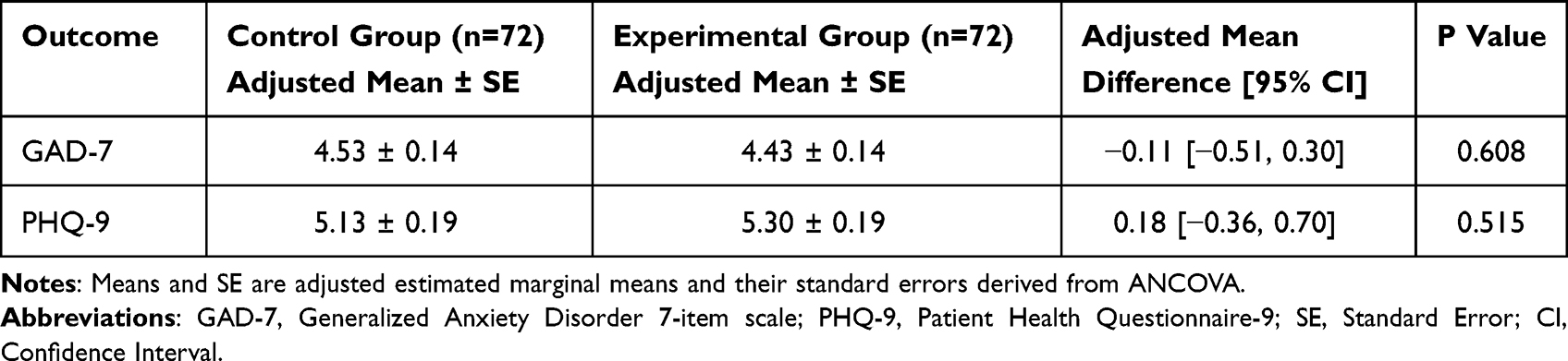 |
Table 4 Comparison of Psychological Status Between Groups on Postoperative Day 3 PM, Adjusted for Baseline (ANCOVA Results) |
Adverse Events
The incidence of minor adverse events was comparable between the experimental group (13 events, 18.1%) and the control group (11 events, 15.3%) (P > 0.05). No serious adverse events related to the study intervention occurred.
Discussion
This study demonstrates that an integrated intervention combining PMT and exposure therapy significantly reduces kinesiophobia, alleviates daily pain, and improves cough capacity in patients following thoracic surgery, strongly supporting our primary hypothesis. These findings offer a novel evidence-based approach to perioperative rehabilitation.
Mechanism of the Integrated Intervention in Mitigating Kinesiophobia
The intervention disrupts the vicious cycle of the Fear-Avoidance Model11 on two distinct levels. First, PMT augmented patients’ intrinsic motivation by enhancing their appraisal of the threats posed by inactivity (eg, DVT) and bolstering their coping appraisal and self-efficacy. This motivational foundation is crucial for overcoming the initial resistance to engage in rehabilitation, a common limitation of standard education. Second, graded exposure therapy, conducted under preemptive analgesia, provided positive “expectancy violation” experiences. By allowing patients to discover that movement does not inevitably lead to catastrophic pain, this component directly challenged maladaptive cognitions and facilitated the extinction of learned fear associations.22,23 It is crucial to note that our intervention targeted not the nociceptive pain signal itself, but the maladaptive psychological response to it. By demonstrating that movement is safe despite the presence of pain, the intervention effectively decouples the sensation of pain from the fear of harm.24
Impact of the Integrated Intervention on Pain and Cough Capacity
The divergent pain trajectories suggest the intervention promoted more adaptive pain coping strategies, such as proactive analgesic use. The slight increase in pain scores at POD3, observed in both groups, is an anticipated phenomenon likely related to lung re-expansion and pleural irritation from the chest tube.25 Our intervention prepared patients for this, reframing the discomfort as a positive sign of healing, which may explain why the experimental group maintained overall lower pain scores compared to the control group, whose interpretation of this pain may have been colored by unaddressed kinesiophobia.26 The significant improvement in cough capacity is a critical finding, as effective coughing is vital for preventing postoperative pulmonary complications.27 The targeted exposure component empowered patients to overcome their fear and perform this essential rehabilitation task effectively.28
Impact of the Integrated Intervention on Psychological Status
The intervention did not significantly alter anxiety or depression levels at POD3. This null finding may be attributable to several factors. First, the short 3-day follow-up may be insufficient to detect changes in more stable emotional states. Second, the intervention was specifically tailored to kinesiophobia, not generalized anxiety or depression. Third, the baseline anxiety and depression levels of our cohort were generally mild, limiting the potential for significant improvement. Importantly, the intervention did not exacerbate these negative emotions, suggesting that the supportive framework, particularly the enhancement of self-efficacy via PMT, may have buffered the potential stress associated with the demands of early mobilization.29
Clinical Significance and Contribution
This study validates a safe and effective non-pharmacological intervention that can be implemented by trained nurses, suggesting good clinical feasibility. By integrating motivation enhancement with behavioral exposure, the protocol effectively promotes early engagement in crucial recovery activities, which is key to preventing postoperative complications. This approach may also reduce reliance on opioids and potentially mitigate the risk of chronic postoperative pain, a hypothesis that warrants long-term investigation. While comprehensive cognitive restructuring requires time, our brief intervention served as a critical catalyst, creating an early “expectancy violation” that empowered patients to break the initial barrier of avoidance and embark on a positive recovery trajectory.
Study Limitations
This study has several limitations. First, as a single-center trial, its generalizability to other healthcare settings requires further validation through multicenter studies. Second, the short follow-up period precludes assessment of long-term effects on chronic pain, functional recovery, and quality of life. Third, the implementation by dedicated research nurses raises questions about scalability, including staff training requirements and time costs in routine clinical practice. Fourth, the exclusion of critically ill patients limits the applicability of these findings to higher-risk populations. Finally, we did not assess the potential influence of postoperative cognitive dysfunction on patient engagement, and while no serious safety events occurred, the intervention was conducted under close supervision, highlighting the need for a monitored environment.
Conclusion
The findings of this randomized controlled trial indicate that an integrated psychological-behavioral intervention based on Protection Motivation Theory and exposure therapy can significantly reduce kinesiophobia, alleviate daily pain intensity, improve cough capacity, and promote early functional recovery in patients after thoracic surgery. This safe and feasible protocol offers a promising new strategy to break the “pain-fear-avoidance” cycle, enhance perioperative management, and accelerate the recovery process for this patient population.
Data Sharing Statement
Deidentified individual participant data that underlie the results reported in this article (including text, tables, figures) will be made available upon reasonable request to the corresponding authors. Data will be available beginning 6 months and ending 36 months following article publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alsaleem MK, Alkhars AM, Alalwan HA, Almutairi A, Alonayzan A, AlYaeesh IA. Kinesiophobia Post Total Hip Arthroplasty: a Retrospective Study. Cureus. 2021;13(6):e15991. doi:10.7759/cureus.15991
2. Du X, Shao Y, Xue J, Kong J. Prevalence and influencing factors of kinesiophobia after total knee arthroplasty: a systematic review and meta-analysis. J Orthop Surg Res. 2025;20(1):332. doi:10.1186/s13018-025-05752-w
3. Chen Y, Zhong G, Zhong S, Lin J, Lin Y. Effect of kinesiophobia on postoperative rehabilitation outcomes in patients with cervical spondylotic myelopathy: a cross-sectional study. J Orthop Surg Res. 2024;19(1):469. doi:10.1186/s13018-024-04819-4
4. Zeng Z, Shen Y, Wan L, et al. Kinesiophobia in patients after cardiac surgery: a scoping review. BMC Cardiovasc Disord. 2024;24(1):469. doi:10.1186/s12872-024-04140-2
5. Liu Y, Ye F, Liu J, Yu J, Fan L, Yang Q. Study of factors influencing early kinesiophobia in older patients after coronary artery bypass grafting in China. Heart Surg Forum. 2024;27(5):E504–E510. doi:10.59958/hsf.7377
6. Pan Y, Qi Q, Yang C, et al. Fear of movement in patients after lumbar spine fusion and an analysis of factors: a cross-sectional study. Front Neurol. 2025;16:1467843. doi:10.3389/fneur.2025.1467843
7. Li C, Lin Y, Xiao X, et al. Development and validation of a risk prediction model for kinesiophobia in postoperative lung cancer patients: an interpretable machine learning algorithm study. Sci Rep. 2025;15(1):19412. doi:10.1038/s41598-025-03575-7
8. Luo Y, Li S, Feng L, Zheng J, Peng C, Bao L. Impact of psychological resilience on the fear of pain and activity recovery in postsurgical patients: observational cohort study. JMIR Form Res. 2025;9:e63556. doi:10.2196/63556
9. Bao L, Peng C, He J, Sun C, Feng L, Luo Y. The relationship between fear avoidance belief and threat learning in postoperative patients after lung surgery: an observational study. Psychol Res Behav Manag. 2023;16:3259–3267. doi:10.2147/prbm.s420724
10. Sayilan AA, Saltan A, Mert S, Ankarali H. Identifying relationships between kinesiophobia, functional level, mobility, and pain in older adults after surgery. Aging Clin Exp Res. 2022;34(4):801–809. doi:10.1007/s40520-021-02011-w
11. Vlaeyen JWS, Crombez G, Linton SJ. The fear-avoidance model of pain. Pain. 2016;157(8):1588–1589. doi:10.1097/j.pain.0000000000000574
12. Nelson S, Borsook D, Bosquet Enlow M. Targeting the stress response in pediatric pain: current evidence for psychosocial intervention and avenues for future investigation. Pain Rep. 2021;6(3):e953. doi:10.1097/PR9.0000000000000953
13. Padovan AM, Kuvačić G, Gulotta F, et al. A new integrative approach to increase quality of life by reducing pain and fear of movement in patients undergoing total Hip arthroplasty: the IARA model. Psychol Health Med. 2018;23(10):1223–1230. doi:10.1080/13548506.2018.1488080
14. Huysmans E, Goudman L, Coppieters I, et al. Effect of perioperative pain neuroscience education in people undergoing surgery for lumbar radiculopathy: a multicentre randomised controlled trial. Br J Anaesth. 2023;131(3):572–585. doi:10.1016/j.bja.2023.05.007
15. Balla J, Hagger MS. Protection motivation theory and health behaviour: conceptual review, discussion of limitations, and recommendations for best practice and future research. Health Psychol Rev. 2025;19(1):145–171. doi:10.1080/17437199.2024.2413011
16. De Baets L, Meulders A, Van Damme S, Caneiro JP, Matheve T. Understanding discrepancies in a person’s fear of movement and avoidance behavior: a guide for musculoskeletal rehabilitation clinicians who support people with chronic musculoskeletal pain. J Orthop Sports Phys Ther. 2023;53(5):307–316. doi:10.2519/jospt.2023.11420
17. Wei X, Xu X, Zhao Y, Hu W, Bai Y, Li M. The Chinese version of the Tampa Scale for Kinesiophobia was cross-culturally adapted and validated in patients with low back pain. J Clin Epidemiol. 2015;68(10):1205–1212. doi:10.1016/j.jclinepi.2015.07.003
18. Ibrahim AS, Aly MG, Abdel-Rahman KA, Mohamed MA, Mehany MM, Aziz EM. Semi-quantitative cough strength score as a predictor for extubation outcome in traumatic brain injury: a prospective observational study. Neurocrit Care. 2018;29(2):273–279. doi:10.1007/s12028-018-0539-3
19. Tong X, An D, McGonigal A, Park SP, Zhou D. Validation of the Generalized Anxiety Disorder-7 (GAD-7) among Chinese people with epilepsy. Epilepsy Res. 2016;120:31–36. doi:10.1016/j.eplepsyres.2015.11.019
20. Wang W, Bian Q, Zhao Y, et al. Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. Gen Hosp Psychiatry. 2014;36(5):539–544. doi:10.1016/j.genhosppsych.2014.05.021
21. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
22. Paré C, Sullivan MJL. Pain catastrophizing and fear of movement: detection and intervention. Clinical Pain Management. 2022;282–290. doi:10.1002/9781119701170.ch27
23. Naqvi WM, Vaidya L, Kumar K. Impact of low back pain on fear of movement and functional activities. Int J Res Pharm Sci. 2020;11(3):4830–4835. doi:10.26452/ijrps.v11i3.2779
24. Vandael K, Vervliet B, Peters M, Meulders A. Excessive generalization of pain-related avoidance behavior: mechanisms, targets for intervention, and future directions. Pain. 2023;164(11):2405–2410. doi:10.1097/j.pain.0000000000002990
25. Wei S, Zhang G, Ma J, et al. Randomized controlled trial of an alternative drainage strategy vs routine chest tube insertion for postoperative pain after thoracoscopic wedge resection. BMC Anesthesiol. 2022;22(1):27. doi:10.1186/s12871-022-01569-w
26. Herrero-Montes M, Fernández-de-las-Peñas C, Ferrer-Pargada D, et al. Association of Kinesiophobia with Catastrophism and Sensitization-Associated Symptoms in COVID-19 Survivors with Post-COVID Pain. Diagnostics. 2023;13(5):847. doi:10.3390/diagnostics13050847
27. Rachmasari A, Suryani RL, Nur Adriyani FH. Implementasi latihan batuk efektif dalam upaya pembersihan jalan nafas pada pasien pasca anestesi umum di ruang pemulihan. Kolaborasi J Pengabdi Masy. 2024;4(5):351–363. doi:10.56359/kolaborasi.v4i5.407
28. Traxler J, Glombiewski J, Vlaeyen JWS. Den teufelskreis durchbrechen – das fear avoidance model und seine therapieansätze. Physiopraxis. 2022;20(2):30–35. doi:10.1055/a-1737-8399
29. Yao X, Zhang L, Du J, Gao L. Effect of Information-Motivation-Behavioral Model Based on Protection Motivation Theory on the Psychological Resilience and Quality of Life of Patients with Type 2 DM. Psychiatr Q. 2021;92(1):49–62. doi:10.1007/s11126-020-09783-w
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comprehensive Review on Personalized Pain Assessment and Multimodal Interventions for Postoperative Recovery Optimization
Xu J, Liu X, Zhao J, Zhao J, Li H, Ye H, Ai S
Journal of Pain Research 2025, 18:2791-2804
Published Date: 5 June 2025
Effectiveness of Combining Thoracic Paravertebral Nerve Block and Serratus Anterior Plane Block in Non-Intubated Spontaneous-Ventilation Video-Assisted Thoracoscopic Surgery: A Retrospective Case-Control Study
Shi Z, Shao G, Zhang X, Shi Y, Rong G, Xu D, Zhu H, Yin D
Journal of Inflammation Research 2025, 18:11125-11137
Published Date: 14 August 2025
Single- versus Multiple-Injection Intertransverse Process Block for VATS: A Randomized Trial on Dermatomal Sensory Blockade
Supphapipat K, Samerchua A, Leurcharusmee P, Lapisatepun P, Pipanmekaporn T, Konkarn N, Prapussarakul K, Jinadech T, Wanvoharn M
Journal of Pain Research 2025, 18:4791-4800
Published Date: 15 September 2025