Back to Journals » International Journal of General Medicine » Volume 19
Tamoxifen Combined with Hormone Replacement in Women with Thin Endometrium Receiving Frozen-Thawed Embryo Transfer for Promoting Endometrial Growth: A Double-Blinded, Randomized Controlled Trial
Authors Shi Q ![]() , Mei J, Yan G, Kong N
, Mei J, Yan G, Kong N ![]() , Liu J, Shen X, Sun Y, Lu F, Jiang Y, Sun H, Huang C
, Liu J, Shen X, Sun Y, Lu F, Jiang Y, Sun H, Huang C ![]()
Received 23 December 2025
Accepted for publication 6 May 2026
Published 13 May 2026 Volume 2026:19 587828
DOI https://doi.org/10.2147/IJGM.S587828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kenneth Adler
Qingqing Shi,* Jie Mei,* Guijun Yan,* Na Kong, Jingyu Liu, Xiaoyue Shen, Yanxin Sun, Feifei Lu, Yue Jiang, Haixiang Sun, Chenyang Huang
Center for Reproductive Medicine and Obstetrics and Gynecology, Drum Tower Clinic Medical College of Nanjing Medical University, Nanjing, 210008, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haixiang Sun, Email [email protected] Chenyang Huang, Email [email protected]
Background: Thin endometrium continues to pose a significant challenge in assisted reproductive technology (ART) cycles, necessitating further exploration of therapeutic approaches. Tamoxifen (TMXF) has been primarily used in ovarian stimulation therapy and can also be implemented as an endometrial preparation protocol, potentially improving endometrial thickness. Does TMXF combined with hormone replacement therapy (HRT) in women with thin endometrium receiving frozen-thawed embryo transfer (FET) improve the endometrial thickness and pregnancy outcome compared to hormone replacement alone?
Methods: This single-centre prospective double-blind randomized controlled trial ran between March 2020 and October 2022. In it, 120 patients with thin endometrium were randomized to TMXF-HRT and control HRT groups at a 1:1 ratio. The primary outcome was endometrium thickness. The secondary outcomes include embryo implantation rate, miscarriage rate and live birth rate. This trial is registered at the ClinicalTrials.gov, number NCT04292886 (Registration Date: March 1, 2020).
Results: Endometrial thickness was significantly greater in the TMXF-HRT group than in the HRT alone group (7.80 ± 0.93 vs 6.93 ± 0.80 mm, P < 0.001), and multivariate analysis confirmed a positive effect of TMXF supplementation on endometrial thickness. However, no significant differences were observed between the two groups in embryo implantation rate or live birth rate.
Conclusion: TMXF combined with HRT can significantly increase endometrial thickness and has the potential to improve clinical pregnancy outcomes (the difference was not statistically significant).
Keywords: thin endometrium, tamoxifen, hormone replacement, frozen-thaw embryo transfer, endometrial thickness
Background
Successful assisted reproductive technology (ART) depends on high-quality embryos, good endometrial receptivity, and their synchronization. Endometrial thickness measured by trans-vaginal ultrasound is the most commonly used non-invasive indicator of receptivity.1–3 Thin endometrium, often defined as thickness less than 7 mm or 8 mm before transformation, leads to cycle cancellation and pregnancy loss. Its causes include uterine surgery, inflammation, infection, endocrine disorders, congenital anomalies, and unknown factors.4–6 It has been reported that the incidence of thin endometrium in ART has reached 1.5–9.1%.7,8 Although various treatments (eg, exogenous estrogen, vitamin E, aspirin, sildenafil, pentoxifylline, stem cells, growth hormone) have been tried, their efficacy remains controversial and suboptimal.9–12 Thin endometrium is still a very difficult problem in ART cycles, and therapeutic methods still need to be explored.
Tamoxifen (TMXF) is a selective estrogen receptor modulator that exerts estrogenic or antiestrogenic effects depending on the target tissue. In 1971, Klopper and Hall first reported its role in inducing ovulation in anovulatory infertile women.13 Previous study showed that tamoxifen significantly increased endometrial thickness, pregnancy rate and live birth rate during intrauterine insemination in patients with thin endometrium.14 And the application of TMXF in the frozen embryo transfer (FET) cycle can improve the serum estrogen level and the endometrial thickness, which showed obvious advantages in clinical pregnancy.15 Although another study showed that TMXF had little effect on pregnancy outcomes, while TMXF could achieve the similar follicle development and pregnancy rate with less gonadotropin (Gn), which was more economical for patients.16 Our previously published retrospective study suggested that adding TMXF to hormone replacement therapy (HRT) improved endometrial thickness in thin endometrium patients undergoing FET, but did not significantly enhance clinical pregnancy or reduce miscarriage rates.17 Given the inherent limitations of retrospective designs, a prospective randomized controlled trial is needed to determine whether TMXF combined with HRT can not only increase endometrial thickness but also translate into improved pregnancy outcomes. This trial aims to address that specific evidence gap.
Methods
Patients
The patients were recruited between March 2020 and October 2022. The first patient in our study was enrolled on 20 March 2020. This trial is registered at the ClinicalTrials.gov, number NCT04292886. This randomized controlled trial was conducted/reported in accordance with the CONSORT 2010 Statement (www.consort-statement.org).
Inclusion criteria: (1) basal serum FSH level < 10 IU/L and younger than 38 years old; (2) endometrium thickness < 8 mm6 for at least 2 FET cycles with different endometrial preparation protocols (ovulation induction cycle/natural cycle/HRT cycle, etc).; (3) at least one high-quality embryo remains; (4) patients agreed to the clinical randomized controlled study of tamoxifen for thin endometrium and sign the informed consent.
Exclusion criteria: (1) abnormal chromosome karyotype; (2) accompanied by other uterine diseases, such as intramural myoma affecting uterine cavity morphology, adenomyosis, serious endometriosis, congenital uterine malformations, endometrial tuberculosis, etc.; (3) contraindications to HRT; (4) participating in other clinical studies; (5) previous history of fundus diseases.
Randomization and Blinding
This prospective, double-blind, randomized controlled trial used random numbers generated by Stata 15.0 to assign eligible participants in a 1:1 ratio to either the TMXF-HRT group (receiving TMXF plus estrogen from day 2 of the menstrual cycle for five days) or the control group (receiving vitamin C plus estrogen instead). Both patients and treating physicians were blinded to group allocation. We encapsulated TMXF and vitamin C tablets to eliminate any differences in appearance and taste. Prior to trial initiation, all investigators completed standardized operating procedure (SOP) training to ensure proper understanding of the protocol and successful implementation of blinding.
Power Calculation
Reviewing the previous data of our centre, the average endometrial thickness of patients with thin endometrium was 7.14 ± 0.8 mm. We expected the endometrial thickness after TMXF addition to be increased by 1 mm at least, which could be considered effective. Accepting a type 1 error (α factor) of 0.05 and type 2 error (β factor) of 10%, the allocation ratio was determined to be 1:1 between the two groups, and at least 60 subjects needed to be enrolled in each arm to allow for a dropout rate of 10%.
Efficacy
The primary outcome was the endometrial thickness. The secondary outcomes were the embryo implantation rate (defined as the ratio of the gestational sac number to the number of transferred embryos), early miscarriage rate (defined as the ratio of the miscarriage number to the patients receiving embryo transfer before 12 weeks of gestation) and live birth rate (defined as the ratio of the number of normal fetuses delivered after 28 weeks of gestation to patients receiving embryo transfer).
Study Procedure
Figure 1 illustrates the enrollment process, including numbers of included and excluded patients and reasons for exclusion. All participants provided written informed consent during screening visits.
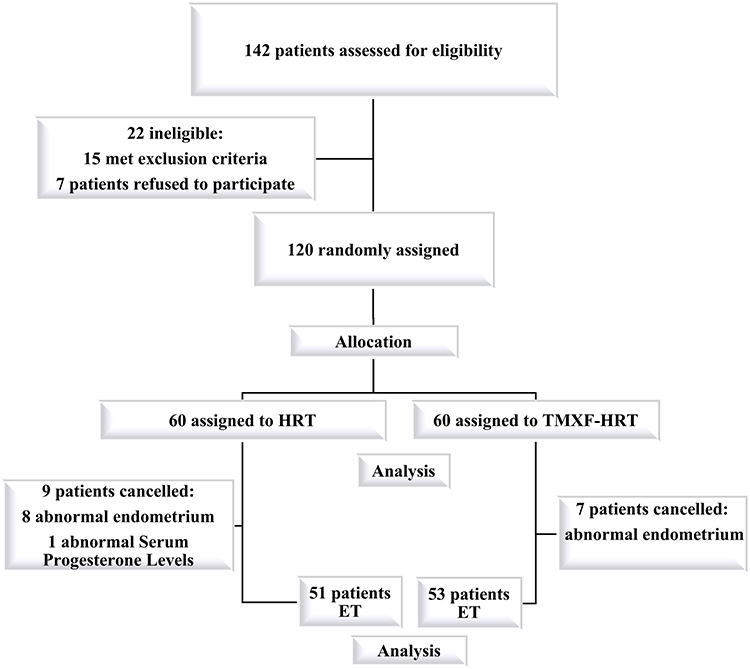 |
Figure 1 A flow chart of the study. |
Patients were randomized to receive either TMXF (10 mg po bid) or vitamin C (10 mg po bid) for five days, starting on day 2 of the menstrual cycle. From the same day, both groups also received estradiol tablets (Femoston, 2 mg po tid).
On cycle day 10, endometrial thickness and serum hormone levels (estrogen and progesterone) were measured. Subsequent treatment was stratified based on endometrial thickness:
If thickness ≥ 8 mm (12 patients in the vitamin C group): Oral estradiol (Femoston) was continued. On cycle day 18, endometrial transformation to the secretory phase was induced using Femoston (estradiol and dydrogesterone tablets) combined with progesterone injection.
If thickness < 8 mm (60 patients in the tamoxifen group and 48 in the vitamin C group): Oral estradiol was increased to 4 mg twice daily, with additional vaginal estradiol (Femoston 2 mg once daily). Endometrial transformation was performed on day 18 using the same regimen (Femoston estradiol/dydrogesterone tablets plus progesterone injection).
After endometrial transformation, embryo transfer was scheduled: cleavage-stage embryos on day 5 and blastocysts on day 6. Ultrasound was performed 30 days after transfer for women with positive β-hCG; clinical pregnancy was defined as the presence of a gestational sac. Luteal support was continued until two months after embryo transfer.
Statistics
The endometrial thickness in the two groups was compared with the Student’s t-test. The embryo implantation rate, early miscarriage rate and live birth rate in patients receiving FET of the two groups were compared using Chi-squared or Fisher’s exact tests as appropriate. Univariate and multivariate analyses were performed using logistic regression models. P < 0.05 was considered statistically significant. All analyses were performed with R (http://www.R-project.org) and EmpowerStats software (www.empowerstats.com, X&Y solutions, Inc. Boston MA).
Results
A total of 120 patients were randomly assigned to the control group (group A, HRT, n = 60) or TMXF-HRT group (group B, n = 60). The following study course is presented in Figure 1. All patients in both groups were treated according to the study protocol. In Group A, 8 patients did not receive FET according to the study protocol because of abnormal endometrium, and 1 patient abandoned FET due to the early increase of serum progesterone level. In group B, 7 patients abandoned embryo transfer due to endometrial factors. Therefore, the analysis of endometrial thickness was performed on all 120 patients, while pregnancy outcome analysis was performed on 104 patients (51 in Group A and 53 in Group B).
The baseline characteristics of patients in these two groups were similar. There was no significant difference in female age, number of previous treatment cycles and body mass index (BMI) between the two groups. The type of infertility (primary or secondary) and the duration of infertility were similar. In addition, similar total number of oocyte picked, and available embryos were observed in the previous IVF/ICSI cycles of the two groups (Table 1). We compared the difference of the major outcome (endometrial thickness) between these two groups. The endometrial thickness of patients in TMXF-HRT group (Group B) was significantly higher than that of HRT group (Table 1, 7.80 ± 0.93 mm vs 6.93 ± 0.80 mm, P < 0.001). Further univariate analysis (Table S1) and multivariate regression analysis (Table 2) were conducted to explore the correlation between TMXF addition and endometrial thickness. After adjusting for potential confounding factors, the results showed that TMXF supplementation had a significantly positive effect on the endometrial thickness (Table 2, β: 0.871, 95% CI: 0.585, 1.158, P = 0.001). Although the endometrial thickness showed significant improvement, it is important to note that the increase was only approximately 0.9 mm, and its clinical significance should be interpreted with caution.
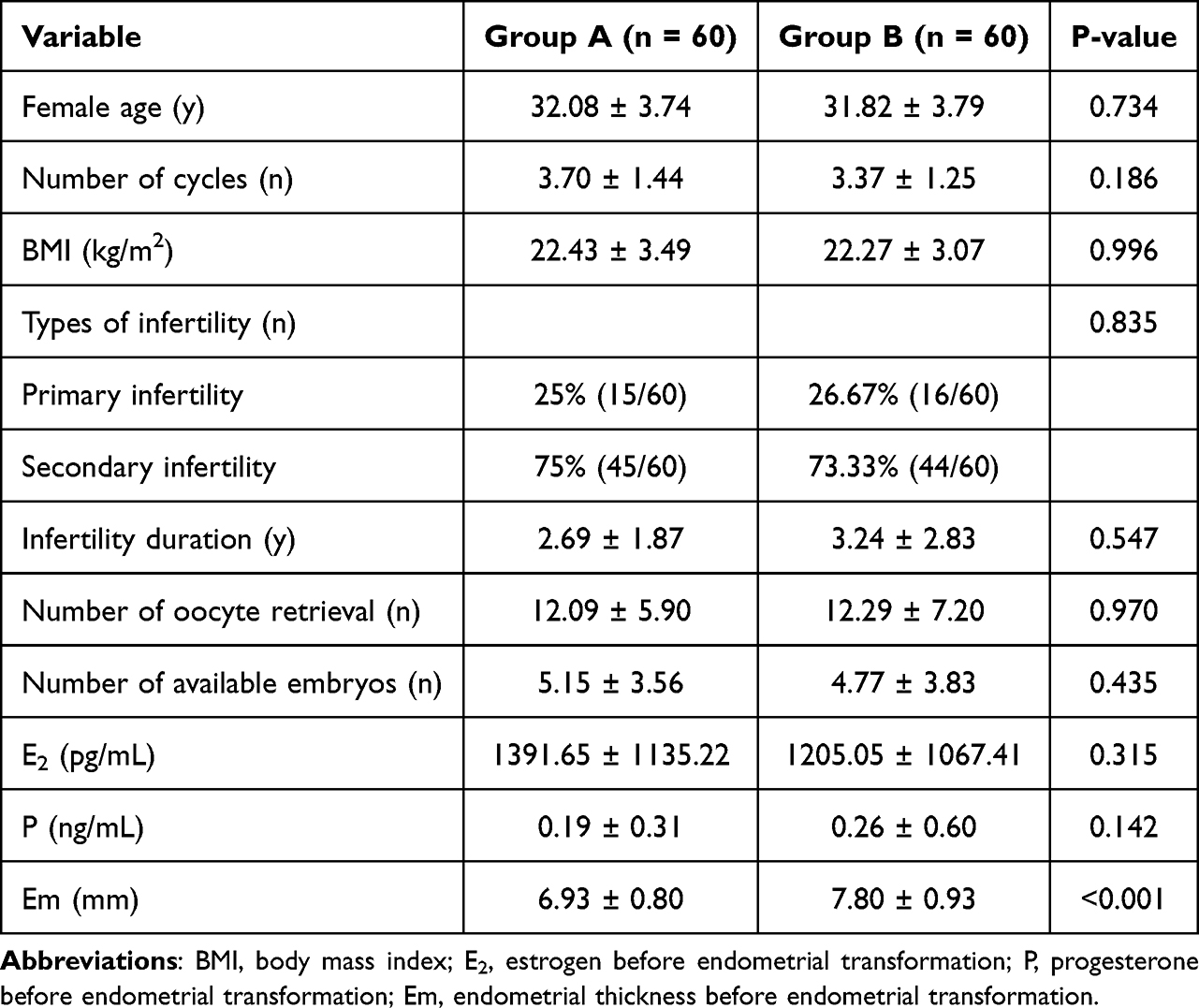 |
Table 1 Patient Characteristics at Baseline and in FET Cycles Between the Two Groups |
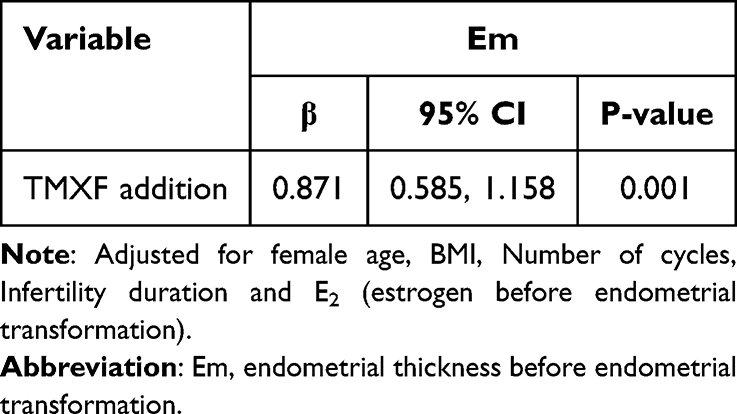 |
Table 2 Multivariate Analysis for the Endometrial Thickness |
We compared the differences between the two groups of the secondary outcomes (embryo implantation rate, clinical pregnancy rate, early miscarriage rate and live birth rate) in further analysis. There was no significant difference between the two groups in female age, number of previous treatment cycles, serum estrogen and progesterone level before endometrial transformation, the number and type of transferred embryos. The embryo implantation rate, clinical pregnancy rate and live birth rate of patients in TMXF-HRT-FET group (group B, n = 53) were higher than those in HRT-FET group (Table 3, embryo implantation rate: 47.06% vs 34.85%; clinical pregnancy rate: 50.94% vs 39.22%; live birth rate: 43.40% vs 29.41%, P > 0.05) and the early miscarriage rate was lower in the TMXF-HRT FET cycles (20.00% vs 11.11%, P > 0.05) with no statistical significance. Further multivariable regression analysis was conducted and the results showed that there was no significant correlation between TMXF supplementation and clinical pregnancy outcomes in HRT cycles (Table 4).
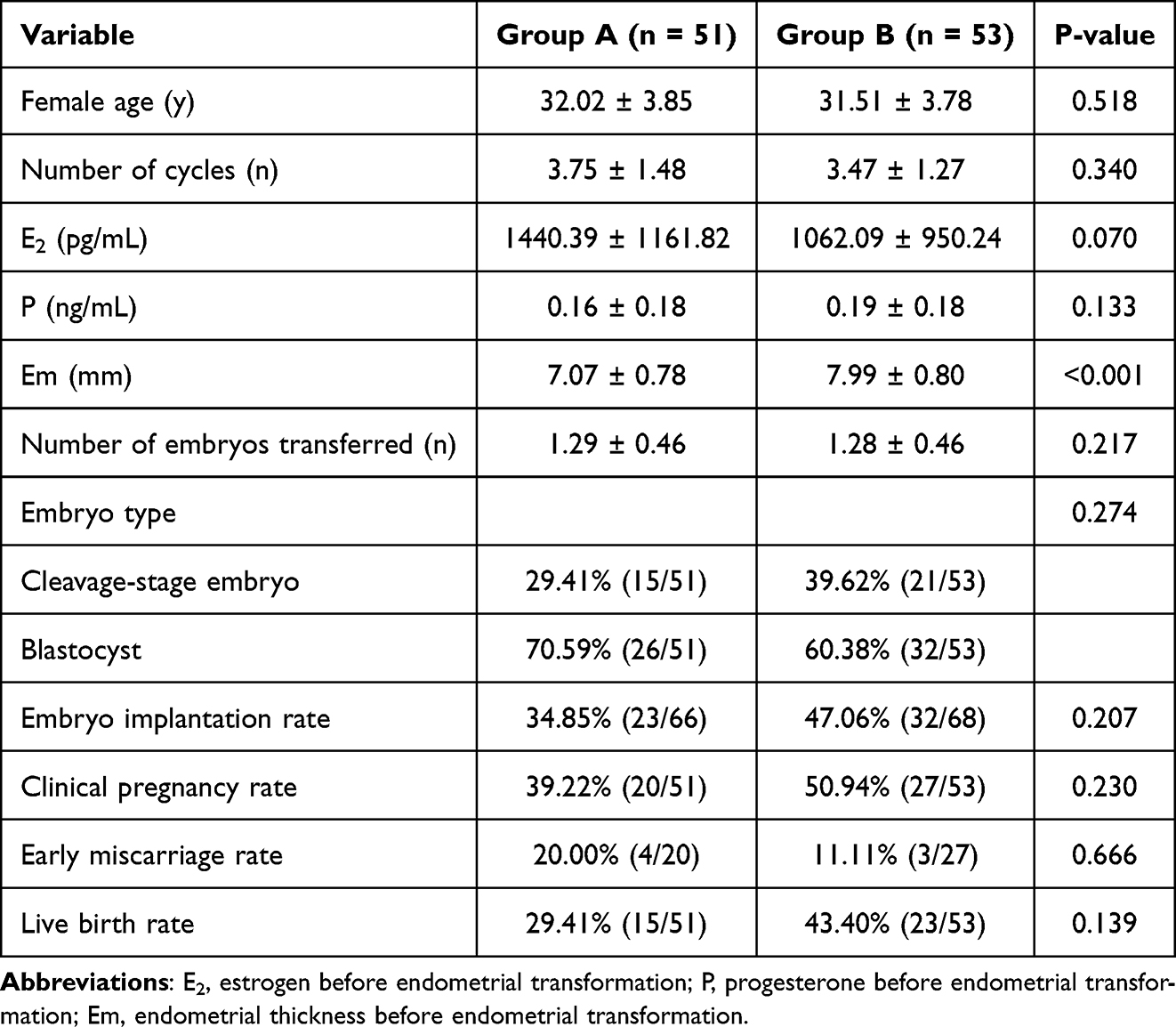 |
Table 3 Clinical Pregnancy Outcomes in FET Cycles Between the Two Groups |
 |
Table 4 Multivariate Analysis for the Clinical Outcomes |
Discussion
Since the first successful frozen-thawed embryo transfer (FET) in 1983, FET has become an integral part of assisted reproductive technology. Successful embryo implantation depends on both embryo quality and endometrial receptivity. Endometrial preparation for FET, which aims to promote endometrial growth using endogenous or exogenous estrogen followed by progesterone-induced transformation, is therefore critical. Common preparation protocols include natural cycle, modified natural cycle, HRT cycle (with or without downregulation), and ovarian stimulation cycle. Current evidence does not favor any single protocol, and clinical selection is typically individualized.18
The endometrial basal layer contains spiral arteries that supply the functional layer, where proliferation, secretion, and degeneration occur to support implantation. After ovulation, spiral artery constriction reduces blood flow to the functional layer, lowering oxygen partial pressure to facilitate embryo implantation. In a very thin endometrium, implantation occurs closer to the basal layer, which has higher blood flow and oxygen tension, leading to reactive oxygen species (ROS) production that may impair embryo development and implantation.19 The etiology of thin endometrium remains unclear but includes iatrogenic or drug-induced injury, endocrine disorders, age, and idiopathic factors. Pathophysiologically, thin endometrium is characterized by limited glandular epithelial proliferation, high uterine blood flow resistance, and reduced vascular endothelial growth factor (VEGF) expression.20 Additionally, significantly decreased estrogen receptor (ER) expression in thin endometrium impairs estrogen response, leading to endometrial dysplasia.21 In HRT cycles, patients with thin endometrium often fail to respond adequately to high-dose estrogen, possibly due to reduced ER activity.22
Tamoxifen, a selective estrogen receptor modulator, acts by competitively binding to estrogen receptors, exerting either estrogenic or antiestrogenic effects depending on the target tissue. In 1971, Klopper and Hall first reported its use for ovulation induction.13 Tamoxifen has similar ovulation-inducing effects as clomiphene citrate (CC) but acts as an agonist on the endometrium and cervical mucus, significantly improving endometrial thickness and pregnancy outcomes.8,23,24 Tamoxifen increases total estrogen metabolites and, through synergy with other estrogen‑induced genes, upregulates ER expression. Combined application of TMXF can markedly improve endometrial ER responsiveness. As a G protein‑coupled estrogen receptor (GPER) agonist, TMXF activates epidermal growth factor receptor (EGFR)-mediated signaling pathways, induces aromatase expression, and forms a positive feedback loop that promotes endometrial proliferation and growth. It also enhances endometrial estrogen biosynthesis and metabolism, raising estrogen levels and increasing endometrial thickness. Furthermore, TMXF directly affects the endometrium by increasing expression of VEGF, insulin‑like growth factor 1 (IGF-1), cell proliferation markers, and cytokines, thereby improving endometrial capillary density and microenvironment.14,25,26 Reported side effects of tamoxifen include hot flashes, menstrual irregularities, uterine cancer, thromboembolic events, lymphedema in premenopausal women, and significant bone density loss.27 Its safety for offspring remains controversial. Animal studies using much higher doses than human clinical practice have suggested potential fetal toxicity (eg, intrauterine growth restriction, fetal death), but recent human studies have not observed teratogenic effects following tamoxifen exposure during pregnancy.28,29 Long-term use of tamoxifen may increase the risk of early menopause.30
Previous applications of tamoxifen in ART mainly focused on ovarian stimulation, which requires more clinic visits, is less convenient than oral HRT, and carries a higher risk of ovarian hyperstimulation syndrome (OHSS) that should be avoided in FET cycles. In the present study, tamoxifen was administered at a low dose (20 mg/day) for only 5 days. Given its plasma half‑life of 7–14 days,31 the interval between drug discontinuation and embryo transfer exceeded 14 days, ensuring safety. Tamoxifen was used to induce endometrial estrogen receptors alongside exogenous estrogen supplementation, thereby enhancing local estrogen activity, stimulating endometrial cell proliferation, and promoting angiogenesis. Consequently, tamoxifen improved endometrial thickness in HRT cycles. Although the TMXF-HRT group showed numerically higher embryo implantation, clinical pregnancy, and live birth rates, as well as a lower early miscarriage rate, these differences were not statistically significant. The primary outcome of this study was endometrial thickness, and the sample size was calculated accordingly. The lack of significant differences in pregnancy outcomes may be attributable to the limited sample size, warranting further prospective studies with larger cohorts.
Several limitations of this study should be acknowledged. First, the sample size was calculated based on the primary outcome of endometrial thickness rather than on reproductive outcomes. Consequently, the study was under-powered to detect potentially clinically meaningful differences in secondary endpoints such as embryo implantation rate, miscarriage rate, and live birth rate. The numerically higher live birth rates observed in the tamoxifen group did not reach statistical significance, which may be at least partly attributable to limited statistical power. Second, this was a single‑center trial, which may limit the generalizability of our findings to other populations with different demographic characteristics or clinical practices. Third, although the trial followed a standardized protocol, the possibility of protocol heterogeneity over time cannot be excluded, particularly in the management of dose adjustments and endometrial transformation criteria based on serial thickness measurements. Such variations could have introduced unintended bias despite rigorous training and blinding procedures. Fourth, we did not assess molecular or histologic markers of endometrial receptivity, such as estrogen receptor expression, vascular endothelial growth factor levels, or integrin profiles. The absence of these mechanistic endometrial markers limits our ability to elucidate how tamoxifen exerts its effects on endometrial growth beyond morphological changes. Future multi-center studies with larger sample sizes, predefined subgroup analyses for pregnancy outcomes, and inclusion of endometrial biomarker assessments are warranted to validate and extend our findings. Therefore, the present results do not support the routine clinical application of TMXF-HRT for patients with thin endometrium.
Conclusions
The present study demonstrates that tamoxifen combined with hormone replacement therapy significantly increased endometrial thickness. However, this morphological improvement did not translate into superior pregnancy outcomes, as there were no statistically significant differences in clinical pregnancy outcomes between the intervention and control groups. These findings suggest that endometrial thickness alone may be insufficient as a reliable predictor of reproductive success. Additionally, the clinical pregnancy outcome indicators (clinical pregnancy rate and live birth rate) in the intervention group were higher than those in the control group (no significant difference), suggesting a potential ameliorating effect of TMXF-HRT on patients with thin endometrium. Notably, the statistical power of this trial was compromised by inadequate sample size, resulting in wide confidence intervals that cannot definitively exclude clinically meaningful effects. Future investigations should prioritize adequately powered, multi-center randomized controlled trials to validate these observations.
Abbreviations
TMXF, tamoxifen; ART, assisted reproductive technology; HRT, hormone replacement therapy; FET, frozen-thawed embryo transfer; Gn, gonadotropin; SOP, standard operating procedure; BMI, body mass index; ROS, reactive oxygen species; CC, clomiphene citrate; ER, estrogen receptor; GPER, G protein coupling estrogen receptors; EGFR, epidermal growth factor receptor; IGF-1, insulin-like growth factor 1; OHSS, ovarian hyperstimulation syndrome.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available due to the special requirements of our hospital and our reproductive medicine center for the disclosure of patients’ clinical data but are available from the corresponding author (Chenyang Huang) on reasonable request via E-mail.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Nanjing Drum Tower Hospital Affiliated to Nanjing University Medical School (NO. 2019-224-02). It was registered on 1 March 2020 and the registry number is NCT04292886. It was carried out at the Reproductive Medicine Centre of Nanjing Drum Tower Hospital affiliated to Nanjing University Medical School. Informed consent was obtained from each patient before treatment. All methods were carried out in accordance with relevant guidelines and regulations. Our study fully protects the privacy of patient data and strictly complies with the Declaration of Helsinki.
Acknowledgment
The abstract of this paper was presented at the ASRM 2024 Scientific Congress & Expo Conference name Tamoxifen combined with hormone replacement in women with thin endometrium receiving Frozen-Thawed embryo transfer for promoting endometrial growth: a double-blinded, randomized controlled trial as a poster presentation talk with interim findings. The poster’s abstract was published in “Poster Abstracts”: https://prod.asrm.org/globalassets/_asrm/news-events/asrm-scientific-congress/asrm2024/2024-final-program.pdf
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Fertility Research Program of Young and Middle-aged Physicians-Clinical Research In 2022 and 2023 (Beijing Health Promotion Association, BJHPA-2022-SHZHYXZHQNYJ-LCH-002, BJHPA-2023-SZHYXZHQN-006), fundings for Clinical Trials from the Affiliated Drum Tower Hospital, Medical School of Nanjing University (2021-LCYJ-MS-20), National Natural Science Foundation of China (82071646), Scientific research project of Jiangsu Province Association of Maternal and Child Health (No. FYX202203), Open project of the Affiliated Jiangning Hospital of Nanjing Medical University Immune Cell Transformation Research Center (JNYYZXKY202213) and Nanjing Drum Tower Hospital Medical Center Project (2022-YXZX-FC-03).
Disclosure
The authors declare that they have no competing interests.
References
1. Zhang T, Li Z, Ren X, et al. Endometrial thickness as a predictor of the reproductive outcomes in fresh and frozen embryo transfer cycles: a retrospective cohort study of 1512 IVF cycles with morphologically good-quality blastocyst. Medicine. 2018;97(4):e9689. doi:10.1097/MD.0000000000009689
2. Koo HS, Park CW, Cha SH, Yang KM. Serial evaluation of endometrial blood flow for prediction of pregnancy outcomes in patients who underwent controlled ovarian hyperstimulation and in vitro fertilization and embryo transfer. J Ultrasound Med. 2018;37(4):851–9. doi:10.1002/jum.14418
3. Chan JM, Sukumar AI, Ramalingam M, Ranbir Singh SS, Abdullah MF. The impact of endometrial thickness (EMT) on the day of human chorionic gonadotropin (hCG) administration on pregnancy outcomes: a 5-year retrospective cohort analysis in Malaysia. Fertility Res Pract. 2018;4(1):5. doi:10.1186/s40738-018-0050-8
4. Yuan X, Saravelos SH, Wang Q, Xu Y, Li TC, Zhou C. Endometrial thickness as a predictor of pregnancy outcomes in 10787 fresh IVF-ICSI cycles. Reprod Biomed Online. 2016;33(2):197–205. doi:10.1016/j.rbmo.2016.05.002
5. Vaegter KK, Lakic TG, Olovsson M, Berglund L, Brodin T, Holte J. Which factors are most predictive for live birth after in vitro fertilization and intracytoplasmic sperm injection (IVF/ICSI) treatments? Analysis of 100 prospectively recorded variables in 8400 IVF/ICSI single-embryo transfers. Fertil Sterility. 2017;107(3):641–648e642. doi:10.1016/j.fertnstert.2016.12.005
6. Liu KE, Hartman M, Hartman A, Luo ZC, Mahutte N. The impact of a thin endometrial lining on fresh and frozen-thaw IVF outcomes: an analysis of over 40 000 embryo transfers. Hum Reprod. 2018;33(10):1883–1888. doi:10.1093/humrep/dey281
7. Wu Y, Gao X, Lu X, et al. Endometrial thickness affects the outcome of in vitro fertilization and embryo transfer in normal responders after GnRH antagonist administration. Reproduct Biol Endocrinol. 2014;12(1):96. doi:10.1186/1477-7827-12-96
8. Mahajan N, Sharma S. The endometrium in assisted reproductive technology: how thin is thin? J Human Reprod Sci. 2016;9(1):3–8. doi:10.4103/0974-1208.178632
9. Dogra Y, Singh N, Vanamail P. Autologous platelet-rich plasma optimizes endometrial thickness and pregnancy outcomes in women with refractory thin endometrium of varied aetiology during fresh and frozen-thawed embryo transfer cycles. JBRA Assist Reprod. 2022;26(1):13–21. doi:10.5935/1518-0557.20210037
10. Rocha MNC, Florencio RS, Alves RRF. The role played by granulocyte colony stimulating factor (G-CSF) on women submitted to in vitro fertilization associated with thin endometrium: systematic review. JBRA Assist Reprod. 2020;24(3):278–282. doi:10.5935/1518-0557.20200025
11. Santamaria X, Cabanillas S, Cervello I, et al. Autologous cell therapy with CD133+ bone marrow-derived stem cells for refractory Asherman’s syndrome and endometrial atrophy: a pilot cohort study. Hum Reprod. 2016;31(5):1087–1096. doi:10.1093/humrep/dew042
12. Li X, Luan T, Zhao C, et al. Effect of sildenafil citrate on treatment of infertility in women with a thin endometrium: a systematic review and meta-analysis. J Int Med Res. 2020;48(11):300060520969584. doi:10.1177/0300060520969584
13. Klopper A, Hall M. New synthetic agent for the induction of ovulation: preliminary trials in women. Br Med J. 1971;1(5741):152–154. doi:10.1136/bmj.1.5741.152
14. Sharma S, Rani G, Bose G, Saha I, Bathwal S, Chakravarty BN. Tamoxifen is better than low-dose clomiphene or gonadotropins in women with thin endometrium (<7 mm) after clomiphene in intrauterine insemination cycles: a prospective study. J Human Reprod Sci. 2018;11(1):34–39. doi:10.4103/jhrs.JHRS_9_17
15. Ke H, Jiang J, Xia M, Tang R, Qin Y, Chen ZJ. The effect of tamoxifen on thin endometrium in patients undergoing frozen-thawed embryo transfer. Reprod Sci. 2018;25(6):861–866. doi:10.1177/1933719117698580
16. Pourmatroud E, Zargar M, Nikbakht R, Moramazi F. A new look at tamoxifen: co-administration with letrozole in intrauterine insemination cycles. Arch Gynecol Obstetrics. 2013;287(2):383–387. doi:10.1007/s00404-012-2556-3
17. Shi Q, Huang C, Liu J, et al. Hormone replacement therapy alone or in combination with tamoxifen in women with thin endometrium undergoing frozen-thawed embryo transfer: a retrospective study. Front Endocrinol. 2023;14:1102706. doi:10.3389/fendo.2023.1102706
18. Liu X, Wang H, Pan R, Li Q, Shi J, Zhang S. Comparison of the method of endometrial preparation prior to frozen-thawed embryo transfer: a retrospective cohort study from 9733 cycles. Reprod Sci. 2021;28(11):3155–3163. doi:10.1007/s43032-021-00603-5
19. Xu Z, Zhang Y, Zhang S, et al. Novel half-sandwich iridium O^C (carbene)-Complexes: in vitro and in vivo tumor growth suppression and pro-apoptosis via ROS-mediated cross-talk between mitochondria and lysosomes. Cancer Lett. 2019;447:75–85. doi:10.1016/j.canlet.2019.01.018
20. Miwa I, Tamura H, Takasaki A, Yamagata Y, Shimamura K, Sugino N. Pathophysiologic features of “thin” endometrium. Fertil Sterility. 2009;91(4):998–1004. doi:10.1016/j.fertnstert.2008.01.029
21. Gao M, Cao C, Zhang X, et al. Abnormal expression of estrogen receptor is associated with thin endometrium. Gynecol Endocrinol. 2019;35(6):544–547. doi:10.1080/09513590.2018.1554035
22. Yu K, Huang ZY, Xu XL, Li J, Fu XW, Deng SL. Estrogen receptor function: impact on the human endometrium. Front Endocrinol. 2022;13:827724. doi:10.3389/fendo.2022.827724
23. Hu R, Hilakivi-Clarke L, Clarke R. Molecular mechanisms of tamoxifen-associated endometrial cancer (Review). Oncol Lett. 2015;9(4):1495–1501. doi:10.3892/ol.2015.2962
24. Elkas J, Armstrong A, Pohl J, Cuttitta F, Martinez A, Gray K. Modulation of endometrial steroid receptors and growth regulatory genes by tamoxifen. Obstetrics Gynecol. 2000;95(5):697–703. doi:10.1016/s0029-7844(99)00660-2
25. Cano A, Hermenegildo C. Modulation of the oestrogen receptor: a process with distinct susceptible steps. Human Reprod Update. 2000;6(3):207–211. doi:10.1093/humupd/6.3.207
26. Sa SI, Maia J, Bhowmick N, et al. Uterine histopathological changes induced by acute administration of tamoxifen and its modulation by sex steroid hormones. Toxicol Appl Pharmacol. 2019;363:88–97. doi:10.1016/j.taap.2018.11.015
27. Mikelman S, Mardirossian N, Gnegy ME. Tamoxifen and amphetamine abuse: are there therapeutic possibilities? J Chem Neuroanat. 2017;83-84:50–58. doi:10.1016/j.jchemneu.2016.08.004
28. Schuurman TN, Witteveen PO, van der Wall E, et al. Tamoxifen and pregnancy: an absolute contraindication? Breast Cancer Res Treat. 2019;175(1):17–25. doi:10.1007/s10549-019-05154-7
29. Buonomo B, Brunello A, Noli S, et al. Tamoxifen exposure during pregnancy: a systematic review and three more cases. Breast Care. 2020;15(2):148–156. doi:10.1159/000501473
30. Furukawa S, Hayashi S, Usuda K, Abe M, Ogawa I. The impairment of metrial gland development in tamoxifen exposed rats. Exp Toxicol Pathol. 2012;64(1–2):121–126. doi:10.1016/j.etp.2010.07.004
31. Hussain T, Kneeshaw PJ. Stopping tamoxifen peri-operatively for VTE risk reduction: a proposed management algorithm. Int J Surg. 2012;10(6):313–316. doi:10.1016/j.ijsu.2012.05.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.