Back to Journals » Patient Preference and Adherence » Volume 20
Tailored Personas for Lung Transplant Recipients’ Return-to-Work Experiences: A Secondary Analysis of Qualitative Data
Authors Huang K, Wang S, Cai L, Chen Z ![]() , Cao X, Zhou H
, Cao X, Zhou H
Received 18 February 2026
Accepted for publication 29 May 2026
Published 12 June 2026 Volume 2026:20 603119
DOI https://doi.org/10.2147/PPA.S603119
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Keyao Huang,1,* Shiyu Wang,1,* Linlin Cai,2 Zixuan Chen,3 Xiaodong Cao,1 Haiqin Zhou1
1The Affiliated Wuxi People’s Hospital of Nanjing Medical University, Wuxi People’s Hospital, Wuxi Medical Center, Nanjing Medical University, Wuxi, Jiangsu, People’s Republic of China; 2Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China; 3Wuxi Taihu University, Wuxi, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaodong Cao, The Affiliated Wuxi People’s Hospital of Nanjing Medical University, Wuxi People’s Hospital, Wuxi Medical Center, Nanjing Medical University, Wuxi, Jiangsu, People’s Republic of China, Email [email protected] Haiqin Zhou, The Affiliated Wuxi People’s Hospital of Nanjing Medical University, Wuxi People’s Hospital, Wuxi Medical Center, Nanjing Medical University, Wuxi, Jiangsu, People’s Republic of China, Email [email protected]
Background: For lung transplant recipients, going back to work is a crucial sign of improved quality of life and post-operative social rehabilitation. However, the re-employment rate for this group is typically poor. Significant individual variances result from the process, which is heavily impacted by intricate physiological, psychological, and social aspects. Support measures frequently lack specificity since there is currently a lack of thorough understanding of the distinct needs and experiences of various patient groups.
Objective: This study examines the real-life experiences, challenges, and coping mechanisms of lung transplant recipients returning to work, and develops user personas for workforce reintegration to uncover cohort diversity and inform targeted vocational rehabilitation interventions.
Methods: We conducted a secondary qualitative analysis of in-depth interviews with 38 lung transplant recipients from a tertiary hospital in Jiangsu Province. Using Graneheim and Lundman’s content analysis and persona development, we identified and visualised distinct return-to-work profiles based on shared characteristics and behaviours.
Results: Four return-to-work profiles were established: (1) Rapid Return Type – Patients who resumed work, recovered well, and actively reintegrated into society; (2) Meandering Return Type – Patients who returned to work but required ongoing balancing of health and occupational demands; (3) Life-Centred Type – Patients who voluntarily relinquished employment, prioritising health and recuperation; (4) Conflicted and Hesitant Type – Patients who have not returned to work but harbour a desire to do so, hindered by physical, psychological, and social barriers.
Conclusion: Lung transplant recipients’ return to work experiences are highly varied and impacted by a variety of circumstances, including social, psychological, physiological, and economic aspects. Finding these profiles helps policymakers, rehabilitation teams, and clinicians comprehend the internal differences in this patient population. This knowledge makes it easier to provide individualized, categorized, and stratified vocational rehabilitation assistance, which fosters long-term social and professional integration.
Keywords: lung transplantation, return to work, user profiling, quality of life, qualitative research
Introduction
Lung transplantation, as an effective treatment for end-stage lung disease, significantly improves patients’ respiratory function, prolongs survival, and enhances their quality of life.1 According to the China Organ Donation and Transplantation Development Report (2023),2 between 2015 and 2023, a total of 4,558 lung transplant procedures were performed in China, with a 30-day survival rate of 83.8%. The success of lung transplantation is not only reflected in the restoration of physiological function and extended survival time, but should also focuses on the comprehensive improvement of patients’ quality of life and the successful restoration of social functioning. Return to work (RTW) is a key indicator of a patient’s postoperative recovery and reintegration into normal social life. It relates not only to the patient’s economic independence and self-worth, but also serves as an objective measure for assessing graft function and overall rehabilitation outcomes.3,4
However, existing research indicates that the proportion of lung transplant recipients returning to work falls far short of ideal levels, and this process is fraught with challenges. Compared with other solid organ transplants, the return-to-work rate among lung transplant recipients is generally low, ranging from 30% to 38%,3,5 ranking lowest among the four major solid organ transplants.6 Returning to work is a socially ingrained process impacted by a number of interrelated elements rather than a straightforward binary result. Previous studies have predominantly focused on influencing factors such as physiological functional status, age, or educational attainment,7,8 or have described lung transplant recipients as a homogeneous group.9 Such approaches overlook variations in patients’ return-to-work experiences, intrinsic motivations, perceived barriers, and support requirements. Consequently, healthcare services frequently lack precision and specificity, making it difficult to adequately address the various difficulties that each person faces.
Against the backdrop of advancing precision medicine and personalised health management, the “user profiling” methodology offers a potent analytical tool for understanding the internal heterogeneity within patient cohorts. By systematically collecting and integrating multidimensional data, this approach constructs virtual prototypes representing distinct patient types, thereby vividly illustrating the differential characteristics, behavioural patterns, and demand structures within a group.10 User profiling has proven to be particularly useful in identifying subpopulations and directing targeted interventions in domains including chronic disease management, rehabilitative care, and health behavior interventions. For example, research in the fields of cardiac rehabilitation,11 social engagement after liver transplantation,12 and nursing education13 has effectively used persona development to uncover classification characteristics within patient or student cohorts, supporting the creation of focused support plans.
In order to develop user personas for lung transplant patients returning to employment, this study will use qualitative research methods to investigate in depth the real-life experiences of lung transplant recipients during their return to work, the main challenges they face, and their coping mechanisms. By exposing the inherent diversity and complexity within this cohort, this study aims to give clinicians, rehabilitation teams, and policymakers more nuanced insights that will help them create a tiered, categorized, and individualized occupational support system, which will ultimately improve the long-term rehabilitation outcomes and social integration levels of lung transplant recipients.
Methods
Study Design and Participants
This study employs a secondary qualitative analysis design to conduct an in-depth reanalysis of the semi-structured interview data collected in the original study regarding the experiences and barriers to returning to work among lung transplant recipients. The original study aimed to broadly explore the overall experiences, perceived barriers, and coping strategies of lung transplant patients returning to work post-surgery. It employed thematic analysis to identify core themes, resulting in a descriptive thematic framework. In contrast, this secondary analysis has the explicit analytical objective of “user profiling”, focusing on identifying patient subgroups with similar behavioral patterns and needs. It utilizes user profiling methods to produce visual patient profiles. The original study had already achieved information saturation, ensuring that the data comprehensively captured diverse patient experiences and perspectives. The user profiling method can reveal group heterogeneity that traditional thematic analysis cannot capture. Reanalyzing the existing data can generate new findings with practical implications without imposing additional burdens on lung transplant recipients.
Building on this foundation, this study employs a user profiling methodology to conduct a systematic reanalysis of the raw data. This approach not only helps to expand and deepen the initial findings but also enables the construction of a classification system based on the characteristics of different roles, thereby providing a more targeted and practice-oriented explanation for understanding this group’s re-entry into the workforce.
Participants
The participants for this secondary analysis were selected from a primary study that aimed to explore the identity formation process of lung transplant recipients returning to work from a career trajectory perspective. Specifically, participants were recruited between August and October 2025 using purposive sampling combined with a maximum variation strategy. Interview times were flexibly scheduled based on participants’ availability, and interviews were conducted via a combination of in-person and online video formats. To ensure the representativeness and diversity of the sample, we recruited participants for the qualitative interviews by distributing invitations via WeChat and during outpatient follow-up visits. These participants exhibited significant differences in terms of age, gender, educational attainment, family economic status, time since surgery, level of occupational identity, and return-to-work status.
Inclusion and Exclusion Criteria
Inclusion criteria:①≥ 2 years post-lung transplantation;② Age ≥18 years;③ Prior employment history; ④ Ability to comprehend and accurately respond to questions; ⑤ Voluntary participation in this study. Exclusion criteria: ① Patients already retired; ② Recipients of combined multi-organ transplantation; ③ Post-secondary lung transplantation.
Data Collection
Original Data Collection
The raw data were collected jointly by two researchers (Author A and Author B), neither of whom had a prior nurse-patient relationship with the participants, thereby minimizing potential bias. The interview guide was developed based on life course theory and a literature review, covering the participants’ motivations for returning to work, their postoperative rehabilitation experiences, the obstacles they encountered and their coping strategies, their family and social support, and their future career plans. Each interview lasted 30 to 60 minutes and was fully audio-recorded after obtaining informed consent from the participants. The recordings were transcribed verbatim within 24 hours and cross-checked by members of the research team to ensure accuracy. Nonverbal expressions were also documented during the interviews to enrich the depth of data interpretation. Data collection continued until information saturation was reached; this study achieved saturation at the 36th interview. To enhance the robustness of the results, two additional interviews were conducted, resulting in a final sample of 38 participants.
The research team comprises four members: one Chief Nurse in lung transplant nursing, one Deputy Chief Nurse, one Senior Nurse, and one postgraduate student. The research team analysed, synthesised, summarised, and evaluated the findings regarding behavioural decision-making experiences. Researchers explained the study’s purpose, significance, and voluntary participation nature to eligible subjects. Prior to formal interviews, general sociodemographic information was collected, including age, gender, marital status, educational attainment, employment status, disease duration, and self-reported health status.14 This information was crucial for analysing the relationship between subjects’ return-to-work behaviour and their social background.
Data Analysis
Establishing Patient Persona Label Dimensions
To construct a system of profile characteristics for the return-to-work journey of lung transplant patients, this study employed the qualitative content analysis method proposed by Graneheim and Lundman, utilising NVivo 14.0 software to analyse the interview data.15 First, the researchers (Author A and Author B) independently identified units of meaning related to the “return-to-work journey” through repeated reading of the transcribed texts. Following cross-checking, 836 units of meaning were identified. By merging semantically similar codes and through discussion and refinement by the research team, 70 standardised codes were ultimately established, forming a comprehensive and logically coherent coding framework. Subsequently, using thematic induction, the codes were categorised based on conceptual similarity and intrinsic relationships. Through continuous comparison and iterative integration, five core thematic dimensions were ultimately distilled: return-to-work status; physical function and postoperative recovery; psychological adjustment and illness identity; social and medical support systems; and family support and financial security.
Manually Extracting Features to Construct Patient Personas
When constructing user profiles, we employed the “thematic matrix analysis” method. Using 70 standardised codes as variables and 38 participants as case studies, we conducted ratings across five core dimensions. By systematically comparing the position of each case within the matrix, we grouped participants who exhibited similar identity trajectories and structural patterns. Following two rounds of independent clustering (conducted by Author A and Author B, with an initial agreement rate of 83.3%) and the resolution of discrepancies through team discussion, we ultimately distilled four distinct professional identity profiles. Each role is presented in a structured format, comprising a set of descriptions and key defining elements.
Description of Patient Personas for Self-Management
To clearly present the characteristics of different patient types, this study employs a combined approach of structuring and visualisation to construct identity profiles of lung transplant patients returning to work. Each portrait is presented as a figurative representation combined with structured labels, comprehensively illustrating typical characteristics and behavioural patterns across various dimensions of return-to-work. This presentation not only highlights the distinctiveness of different patient groups but also systematically reveals the practical approaches and diverse pathways taken by lung transplant recipients during their professional reintegration. This provides a basis for developing targeted support strategies in subsequent stages.
Rigor
To guarantee the credibility, reliability, and transferability of this study, it strictly adhered to qualitative research report standards and implemented multiple quality control measures.16 Two principal investigators collaborated during the data collection phase: one conducted semi-structured interviews, whilst the other simultaneously observed and recorded non-verbal information; following the interviews, they promptly co-authored memos to consolidate key information. During the data analysis phase, coding consistency was ensured through a triangulation mechanism, with two researchers independently completing the initial coding and categorisation; the rate of coding inconsistency was approximately 12%, and consensus was reached following joint discussion; Subsequently, inter-rater reliability was tested on a 30% random subsample. Two researchers, unaware of each other’s classifications, independently assigned participants to one of four profiles. The agreement rate was 83.3%, with a Cohen’s κ value of 0.79 (95% CI 0.65–0.93), indicating substantial agreement. All cases of disagreement were subject to in-depth team discussion and reconfirmed based on the original data.
To ensure the analysis process is fully traceable, all raw data, transcripts, analysis memos, coding manuals, labelling schemes and records of profile assignment decisions have been systematically archived, establishing a complete audit trail. The research team maintained theoretical sensitivity through regular discussions and critical reflection, ensuring that the classification system was grounded in the participants’ experiential logic and aligned with the theoretical framework of return to work following lung transplantation; all researchers had no prior nurse-patient relationships with the participants, thereby minimising potential bias. As this study is a secondary analysis, no member checking was conducted; this limitation is clearly stated in the “Limitations” section of the main text.
Ethical Considerations
This study has been approved by the Research Ethics Committee of Wuxi People’s Hospital (Approval No.: KY24037). We confirm that all organs were donated voluntarily with written informed consent, and the donation procedures were conducted in accordance with the Declaration of Istanbul. All subjects signed written informed consent forms before the study started. The informed consent explicitly stated that anonymized responses and direct quotes from participants could be published as part of the research findings. We rigorously protected the confidentiality and personal data of research participants. Interview recordings and transcribed texts were only allowed to be used for this study; they were not shared or used in any other way without the participants’ express permission. To guarantee the complete safety of participants’ names and privacy, all individually identifying information was anonymized before findings were reported and analyzed.
Results
Demographic Characteristics of Participants
This study comprised 38 patients who qualified for lung transplants. Of these, 29 were men and 9 were women; the subjects ranged in age from 18 to 60; 55.26% of the patients came from well-off families; and 36.84% of the patients had only completed primary school. Furthermore, 63.16% of the individuals went back to work following lung transplantation, and 78.95% of them were married. For more information, see Table 1.
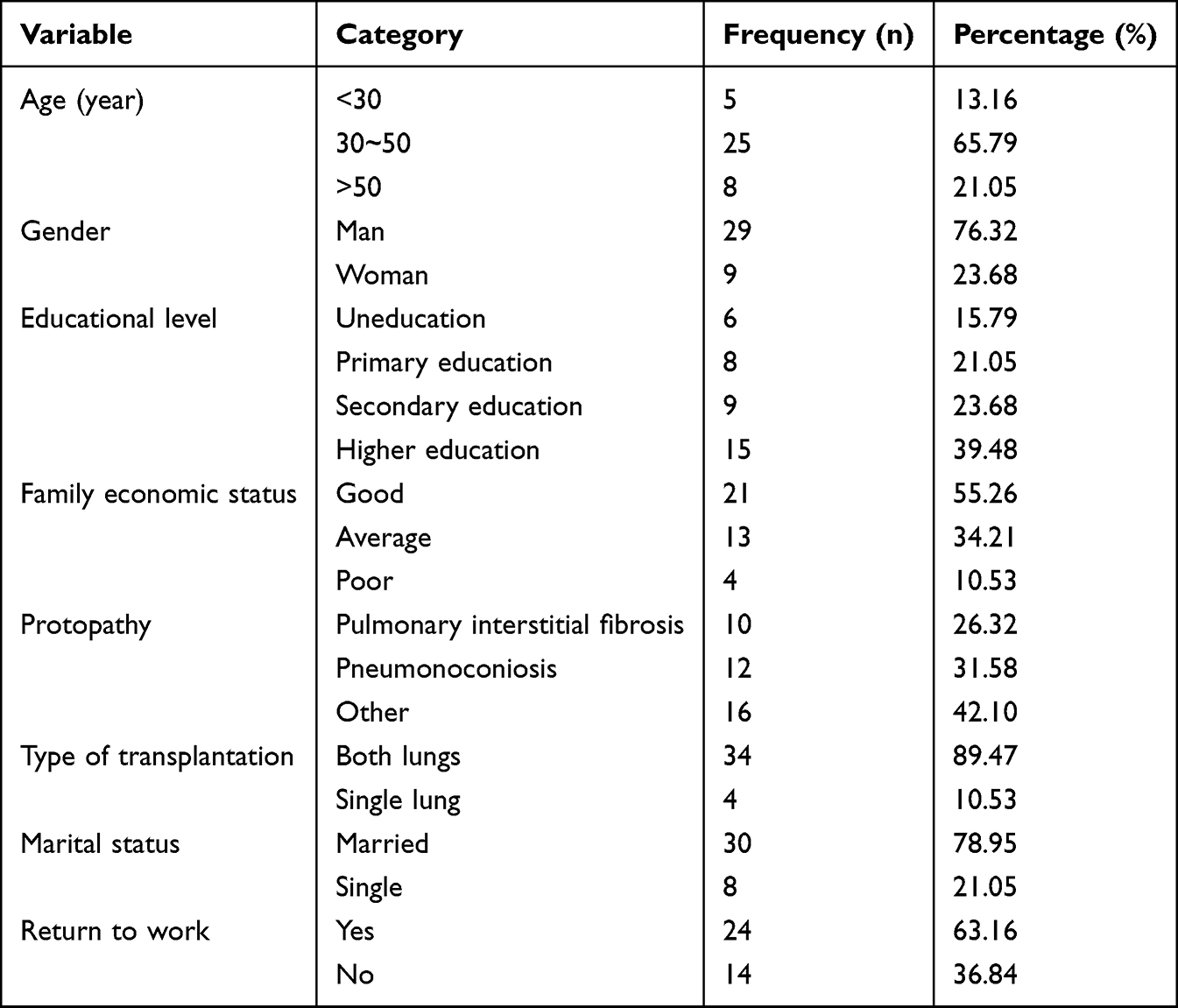 |
Table 1 Characteristics of Participants |
Tailored Personas for Return-to-Work Identity in Lung Transplant Recipients
This study employs qualitative analysis to construct four distinct occupational reintegration profiles for lung transplant recipients (see Table 2). These profiles systematically present behavioural characteristics observed during the group’s return-to-work process, while elaborating on the specific traits and needs of each patient category. The four profiles are detailed as follows:
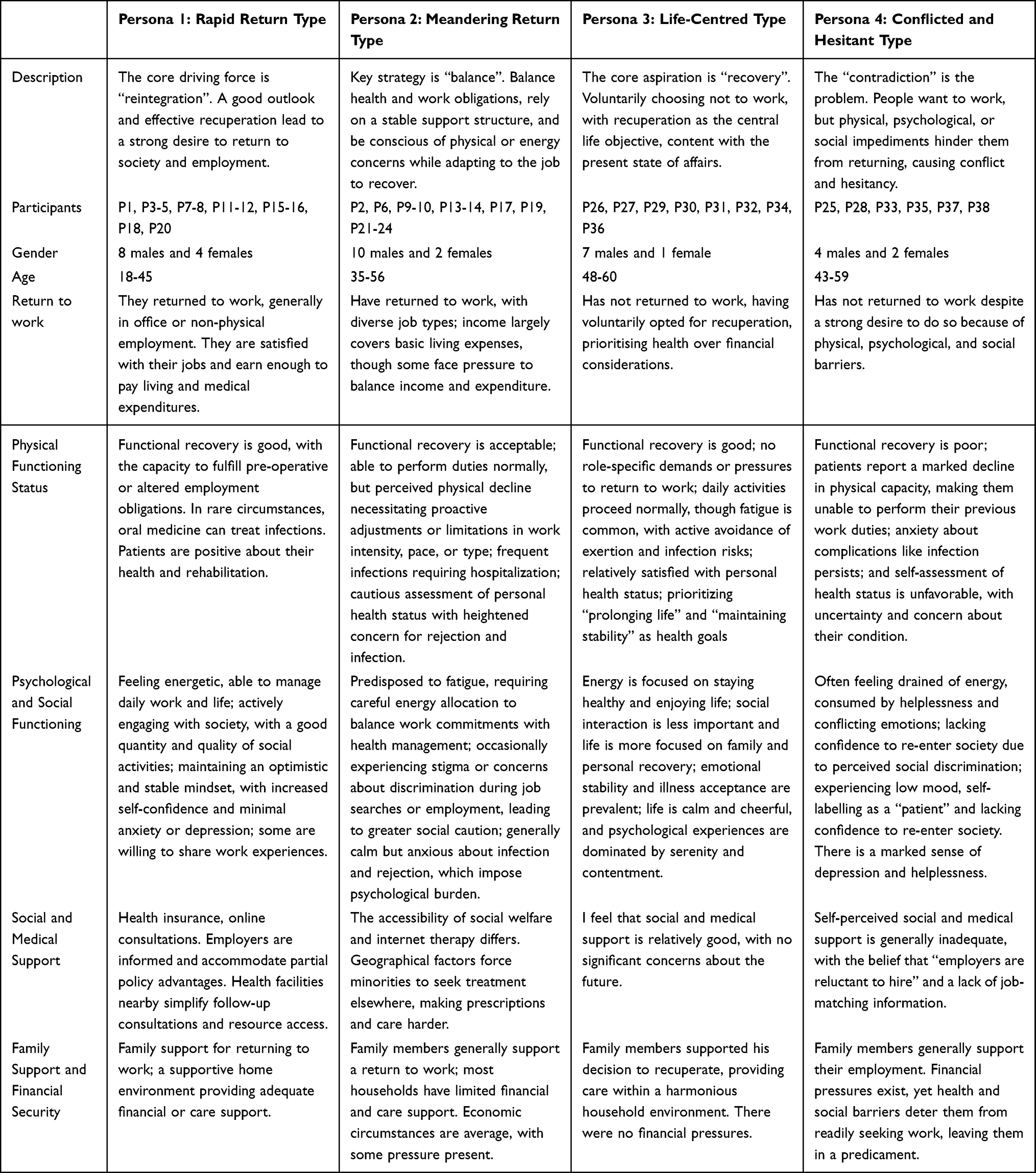 |
Table 2 Tailored Personas for Lung Transplant Recipients’ Return-to-Work Experiences |
Persona 1: Rapid Return Type
Description
The core motivation for such patients is reintegration into society and the workplace. Following successful recovery and maintaining a positive mindset, they have successfully returned to employment through various avenues, achieving effective social reintegration. They predominantly engage in office-based or light manual work, with earnings sufficient to cover living and medical expenses. They report high job satisfaction, benefit from strong family support, and experience no significant financial strain.
Key Characteristics
- Good physical recovery, able to manage work and daily activities, confident in health status.
- Positive psychological state, high energy levels, minimal impact of illness on social functioning.
- Comprehensive healthcare coverage, supportive workplace environment, and accessible medical resources.
- Family support for return to work, low financial pressure, favourable household circumstances.
Quotes
P3: Staying at home all the time made me feel like I was still an invalid. Returning to work, even part-time, made me feel useful and normal. It was a crucial part of my recovery process.
P11: My workplace was very understanding of my situation and adjusted my role. Regaining a regular routine and interacting with colleagues felt wonderful—it provided the motivation I needed during my recovery.
Persona 2: Meandering Return Type
Description
The core strategy for such patients lies in seeking a “balance” between health and work. They are able to return to work but experience a perceived decline in physical strength or energy levels, gradually adapting to the workplace environment. They must proactively adjust their pace and intensity at work, remain vigilant against risks such as infection or rejection, and endure a certain degree of ongoing psychological burden.
Key Characteristics
- Returned to work but perceive reduced physical capacity, necessitating adjustments to workload or role to maintain wellbeing, with persistent concerns about health risks.
- Simultaneously crave the sense of normalcy work provides while experiencing anxiety and burden due to physical limitations.
- Levels of workplace support vary, with some individuals facing financial strain from reduced income.
- Receive fundamental family support, though may encounter certain economic or caregiving pressures.
Quotes
P14: I can manage the work, but I don’t dare push myself like I used to. After half a day, I need to rest. I’m always worried that overexertion might trigger an infection. That worry is always at the back of my mind.
P19: When job hunting, I hesitated to mention major surgery, fearing employers might be put off. This shift is manageable, but the pay is low. Monthly medication costs remain substantial, and the pressure is considerable.
Persona 3: Life-Centred Type
The core aspiration of such patients is recuperation. They voluntarily choose not to return to work, prioritising health maintenance and quality of life above all else, content with a lifestyle centred on family and personal recuperation.
Key Characteristics
- Physical functioning permits daily activities, though fatigue is common, leading to a tendency to actively avoid exertion and infection risks.
- Emotional and psychological stability is maintained, with a high level of acceptance towards the condition and a contented, unassuming attitude towards life.
- Social engagement requirements are low, with a clear shift in life focus towards family and personal well-being.
- Family members support the decision to rest and recuperate, typically with financial security such as retirement pensions, ensuring no financial concerns.
Quotes
P29: Being given a second chance at life, I no longer want to burden myself with work. Now I spend my days taking walks, caring for flowers, and spending time with my grandchildren. It makes me feel truly content and happy.
P32: My children have all started their own families, and my spouse and I have retirement pensions. Keeping myself healthy and not becoming a burden to them is now my most important job and greatest achievement.
Persona 4: Conflicted and Hesitant Type
Description
The core dilemma for these individuals is “conflict”. They possess a strong desire to work but are constrained by significantly diminished physical capabilities, psychological barriers, or perceived social discrimination. Consequently, they remain unable to successfully re-enter the workplace, caught in a state of conflict and hesitation.
Key Characteristics
- Perceive physical limitations as incompatible with former roles, harbour persistent health anxieties, and hold low self-assessments of their condition.
- Experience low mood, frequent fatigue, self-identify as patients, and lack confidence in societal reintegration.
- Strongly perceive employment market discrimination and perceive a lack of effective vocational rehabilitation guidance.
- Face family opposition to employment driven by concern, exacerbating psychological burdens while also confronting financial pressures.
Quotes
P28: I want to work to ease the burden on my family, but after two attempts outside, my stamina simply couldn’t keep up. Feeling like a useless person is terribly distressing.
P33: My family all say, “Your health isn’t up to it, don’t struggle on.” But I’m only just over fifty – am I supposed to just stay at home? Yet I fear employers will reject me the moment they see my medical history.
Discussion
Through an in-depth exploration of the return-to-work journey of lung transplant recipients, this study identified four representative user profiles: the Rapid Return Type, the Meandering Return Type, the Life-Centred Type, and the Conflicted and Hesitant Type. The findings highlight that returning to work is not a simple “yes or no” binary outcome, but rather a dynamic and personalized process of social participation closely linked to multiple dimensions, including physical function, psychological adjustment, social support, and economic factors. To effectively enhance the level of social participation among lung transplant recipients, healthcare professionals must conduct comprehensive assessments and develop individualized, targeted intervention measures based on the social participation characteristics and barriers of different subgroups. By providing tailored social support systems and resources, they can facilitate the smooth reintegration of this population into society. The establishment of this profiling system holds significant theoretical and practical implications for building a stratified, categorized, and personalized vocational rehabilitation support system for lung transplant recipients, and it aligns with the core objectives of precision medicine and precision nursing in the fields of chronic disease management and rehabilitation. It is important to emphasize that these profiles reflect typical characteristics of patients at a specific stage; their boundaries are not strictly defined, and individuals may transition between types over time. Therefore, we recommend that the profiles from this study be viewed as tools to inspire future research and practice, rather than as established clinical classification criteria.
Patients with rapid recovery represent the cohort experiencing the smoothest transition back to work. This group demonstrates favourable postoperative recovery, maintains a positive mindset, and receives substantial support from both their workplace and family. Their successful reintegration is characterized by a combination of good physical function, a positive attitude toward their condition, and a strong social support network. Notably, their core motivation for returning to work often transcends purely economic needs, placing greater emphasis on reconstructing social identity and realising self-worth. They view work participation as an integral component of post-operative rehabilitation and normalised living. This aligns with research findings on social participation among chronic disease patients, which indicate that early functional recovery,17 positive self-efficacy,18 and environmental support7,19 are core elements facilitating successful societal reintegration. For patients who have achieved initial return-to-work success, the focus of healthcare and rehabilitation teams may shift from facilitating reintegration to consolidation and enhancement. The core objective of interventions lies in sustaining and developing their occupational engagement. Beyond ongoing health monitoring, career development counselling should be provided to assist them in realising personal fulfilment and growth through work. Psychological motivation and social support should be utilised to reinforce their positive mindset and prevent anxiety triggered by work-related stress or sudden health incidents. Concurrently, attention must be paid to the risk of neglecting physical limitations in pursuit of “normalisation”, guiding them towards establishing sustainable work-health balance patterns. Furthermore, peer support platforms should be actively established to encourage these patients to share successful experiences, leveraging their exemplary and motivational roles. This empowers the entire lung transplant patient community, inspiring greater confidence in recovery and return to work.
The profile of patients with a tortuous recovery trajectory represents an intermediate cohort facing persistent challenges in returning to work following lung transplantation. This cohort possesses the physical capacity for work resumption yet must navigate delicate compromises between health maintenance and professional obligations due to diminished post-operative stamina and energy. Core characteristics include perceived physical decline, persistent health anxiety, and economic pressures necessitating career adjustments—often stemming from inadequate workplace support and employment disclosure challenges. This profile profoundly reflects the complexity and protracted nature of the return-to-work process, aligning with the psychological states of “survivor guilt” and “health concern” commonly experienced by long-term organ transplant survivors.19 Previous studies have indicated that lung transplant recipients generally tend to overestimate health risks, and this psychological burden is associated with their occupational behavior and work experiences.20 The present study further corroborates this perspective. For this cohort, universal rehabilitation advice often proves limited in effectiveness. They require highly individualised, flexible, and forward-looking support programmes. The clinical approach focuses on providing professional guidance on physical and energy management to help patients establish a work schedule that suits their physical condition.21 Concurrently, enhanced communication and collaboration with patients’ employers are essential to facilitate flexible working arrangements such as adjustable schedules and job adjustments. Furthermore, targeted psychological counselling should be provided to alleviate health-related anxieties, transforming fear of the disease into effective self-management behaviours. This supports the development of scientifically grounded health risk awareness and helps individuals strike a balance between work commitments and rehabilitation.
The Enjoy Life Patient Profile represents individuals who proactively shift their life focus from the workplace towards personal wellbeing and family life. This group voluntarily chooses not to return to work. This decision stems from a comprehensive assessment of multiple factors including age, post-operative physical condition, stable financial resources, and robust family support. It constitutes a deliberate adaptation and redefinition of life purpose at a specific stage of their life cycle. While their physical capabilities remain sufficient for daily living, they exhibit high disease acceptance, emotional stability, and a detached attitude towards life. Their social engagement preferences lean towards low-intensity leisure activities and family interactions rather than professional involvement. Research indicates that for elderly individuals or those who have experienced significant trauma, shifting life goals from social productivity towards personal wellbeing and family relationships constitutes an effective adaptive strategy for enhancing life satisfaction.22 The findings of this study align with this conclusion. For such patients, the healthcare system should respect and support this diverse range of rehabilitation outcomes, providing a corresponding support system centred on quality of life and health maintenance. Specifically, personalised health management plans should be developed and implemented, encompassing standardised postoperative follow-ups, low-intensity rehabilitation exercises, and infection prevention guidance. Their family and social support networks must be maintained and strengthened to foster a low-stress living environment that accommodates their family-centred social participation needs. Concurrently, particular care must be taken to avoid imposing societal pressures to work. The value of their chosen path should be fully acknowledged to prevent feelings of inadequacy, thereby genuinely supporting them in achieving a quality postoperative life.
Patients exhibiting ambivalent hesitation represent the most challenging cohort in the post-lung transplant return-to-work process. They commonly harbour a strong desire to work, yet find themselves trapped by significantly diminished physical capacity, profound feelings of illness-related stigma and helplessness, perceived social employment discrimination, and family opposition stemming from health concerns. This disconnect between their desire to work and their actual capabilities forms their core conflict. It not only traps them in a prolonged state of wanting to work yet being unable or afraid to do so, but also readily triggers psychological issues such as frustration and loss of self-worth. Previous research indicates that stigma and social discrimination represent key barriers to the social reintegration of individuals with chronic illnesses and organ transplant recipients.23 Concurrently, the absence of occupational capability assessments can foster negative perceptions of one’s employability.24 This study further confirms that these intertwined physiological, psychological, and sociocultural barriers are often described by participants as factors that exacerbate the challenges they face in returning to work. At the individual level, objective vocational capability assessments and personalised skills retraining should help rebuild occupational confidence, while in-depth psychological interventions alleviate stigma and helplessness.25 At the societal level, anti-discrimination advocacy must be promoted, communication bridges established between healthcare institutions, rehabilitation specialists, and lung transplant recipients, and supportive employment programmes developed. At the family level, scientific rehabilitation education should be delivered through family meetings, guiding relatives to transform overprotection into appropriate support. Collaborative development of progressive, feasible social reintegration plans is essential, positioning families as vital pillars of support on the patient’s return journey. Furthermore, the enabling potential of information technology should be fully leveraged. Multiple studies confirm that internet usage effectively promotes individuals’ return-to-work capacity.26,27 This offers significant insights for intervention, enabling healthcare professionals to actively encourage and guide lung transplant recipients in exploring work participation through internet-based formats such as remote working and online collaboration. Such online participation models significantly reduce physical demands and eliminate commuting burdens while helping patients maintain professional identity, rebuild social connections, and accumulate successful experiences. This provides a viable buffer zone and capability-building pathway for achieving comprehensive social reintegration. For lung transplant recipients facing financial hardship, telemedicine follow-up can deliver close, accessible medical support to enhance their return-to-work prospects.
This study constructed four user personas for lung transplant patients returning to work, systematically revealing significant heterogeneity within this group during their occupational reintegration process. On the physical function dimension, improvements in objective medical indicators provide the foundation for returning to work, but patients’ subjective perceptions of functional status often become the more direct determining factor. Findings indicate that younger patients exhibit higher return rates,28 aligning with the “Rapid Return” profile. Conversely, “Tortuous Return” and “Ambivalent Observation” patients frequently experience a gap between objective improvement and subjective capability perception, this disconnect often coincides with their hesitation or feelings of frustration as they navigate their path back to recovery.29 On psychological and social dimensions, positive illness identification, high psychological resilience, and understanding support from family are key facilitators for the smooth reintegration of “rapid recovery” patients.29,30 Conversely, “conflicted and hesitant” patients are commonly burdened by stigma, fear of discrimination, and overprotective families, highlighting the necessity of psychological interventions and social advocacy. Economic factors and welfare policies intertwine to form the practical decision-making context. “Life-enjoying” patients, backed by stable financial security, can prioritize quality of life; meanwhile, many “tortuous return” and “conflicted-observing” patients face dual pressures of medical expenses and income demands. Furthermore, the lack of sustained, accessible medical rehabilitation resources further hinders occupational exploration for some patients.30 Results indicate that occupational rehabilitation following lung transplantation constitutes a multidisciplinary, full-cycle continuous support process. This necessitates establishing a multidimensional collaborative system that integrates resources from clinical medical staff, rehabilitation therapists, psychological experts, vocational counselors, and social employment services. Such a system provides patients with comprehensive support spanning preoperative assessment, early postoperative recovery, adaptation during the return-to-work process, and long-term maintenance of occupational functioning. Furthermore, digital health tools serve as critical enabling resources, particularly for patients with a meandering return pattern or ambivalent observation pattern. These tools deliver flexible, real-time, and accessible support and feedback, thereby overcoming limitations of traditional follow-up models and enhancing the continuity of support services.
Limitations
This study has several limitations. First, as a secondary analysis, the original interview data were not specifically designed for constructing return-to-work profiles, potentially limiting depth in certain dimensions and affecting the profiles’ granularity. Second, reinterpreting data within existing narratives and introducing new analytical frameworks may carry risks of overinterpretation, while the absence of participant validation may reduce the study’s confirmability. Third, participants were exclusively from a single tertiary-level hospital in one region, potentially limiting the generalizability of findings. Fourth, while the profile categorization aids in identifying typical patterns, it may oversimplify the dynamic, phased, and context-dependent nature of lung transplant recipients’ return-to-work journey. Fifth, the findings of this study fall within the scope of descriptive qualitative research and are limited in terms of the level of evidence. The discussion in this paper regarding stratified interventions and precision rehabilitation is based on theoretical inferences and preliminary hypotheses derived from profiling characteristics and has not yet been validated through clinical practice. Future research should further validate the stability and evolution of these profiles through multicenter designs, longitudinal tracking, and mixed-methods approaches, while incorporating multi-stakeholder perspectives to refine intervention strategies.
Conclusions
This study constructed four identity profiles for lung transplant recipients returning to work, systematically revealing characteristics of this group in terms of occupational return goals, physical and psychological adaptation, and social support. The findings highlight the potential value of implementing tiered, targeted support based on profiling characteristics, providing a conceptual foundation for the initial development of personalized vocational rehabilitation practices. Future longitudinal studies and intervention validation are needed to further optimize long-term social integration pathways for patients with different profiles.
Data Sharing Statement
The datasets generated and/or analyzed during the present study are available from the corresponding author, Haiqin Zhou, upon reasonable request.
Ethics Statement
The study was approved by the Research Ethical Committee of Wuxi People’s Hospital (KY24037).
Acknowledgments
We would like to express our sincere gratitude to all the patients, their families, and the hospital personnel who agreed to participate in the survey and provided valuable responses.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received funding from the Wuxi Municipal Health Commission (Youth Research Program, Grant No. Q202414), the Nanjing Medical University School Fund Project (Grant No. NMUB20250122), the Wuxi Science and Technology Bureau (Taihu Spark Program, Grant No. Y20242101).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Warrior K, Dilling DF. Lung transplantation for lymphangioleiomyomatosis. J Heart Lung Transplant. 2023;42(1):40–12. doi:10.1016/j.healun.2022.09.021
2. Jiefu H. Report on the development of organ donation and transplantation in China. 2023.
3. Suhling H, Knuth C, Haverich A, et al. Employment after lung transplantation--a single-center cross-sectional study. Dtsch Arztebl Int. 2015;112(13):213–219. doi:10.3238/arztebl.2015.0213
4. Abidi Y, Kovats Z, Bohacs A, et al. Lung transplant rehabilitation—a review. Life. 2023;13(2):506. doi:10.3390/life13020506
5. Cumming K, O’brien L, Harris J. Predictors of employment participation following lung transplant. Austra Occupl Therapy J. 2016;63(5):347–351. doi:10.1111/1440-1630.12315
6. de Baere C, Delva D, Kloeck A, et al. Return to work and social participation: does type of organ transplantation matter? Transplantation. 2010;89(8):1009–1015. doi:10.1097/TP.0b013e3181ce77e5
7. Desai RH, Hollingsworth H, Stark S, et al. Social participation of adults aging with long-term physical disabilities: a cross-sectional study investigating the role of transportation mode and urban vs rural living. Disability Health J. 2023;16(4):101503. doi:10.1016/j.dhjo.2023.101503
8. Watts AS, Mortby ME, Burns JM, Ginsberg SD. Depressive symptoms as a barrier to engagement in physical activity in older adults with and without Alzheimer’s disease. PLoS One. 2018;13(12):e0208581. doi:10.1371/journal.pone.0208581
9. Lu D, Shi L, Chen J, et al. Status and influencing factors of social participation in renal transplantation recipients: a cross-sectional study from a single center in China. Transplant Proc. 2023;55(2):354–362. doi:10.1016/j.transproceed.2023.01.021
10. Zimmermann M, Yonkers KA, Tabb KM, et al. Developing personas to inform the design of digital interventions for perinatal mental health. JAMIA Open. 2024;7(4):ooae112. doi:10.1093/jamiaopen/ooae112
11. Yang Z, Xu L, Gao Y, et al. Tailored personas for self-management in home-based cardiac rehabilitation for patients with coronary heart disease: a qualitative study. Int J Nurs Stud. 2025;163:105000. doi:10.1016/j.ijnurstu.2025.105000
12. Qi Y, Chenxiao L. The user persona study on social participation in liver transplant recipients. J Nurs Sci. 2025.
13. Han X, Duan Y, Hong S, et al. Tailored professional identity personas of male undergraduate nursing students: a secondary analysis of qualitative data. BMC Nurs. 2025;24(1):1143. doi:10.1186/s12912-025-03809-z
14. Gallagher JE, Wilkie AA, Cordner A, et al. Factors associated with self-reported health: implications for screening level community-based health and environmental studies. BMC Public Health. 2016;16(1):640. doi:10.1186/s12889-016-3321-5
15. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
16. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
17. Bourassa KJ, Memel M, Woolverton C, et al. Social participation predicts cognitive functioning in aging adults over time: comparisons with physical health, depression, and physical activity. Aging Mental Health. 2017;21(2):133–146. doi:10.1080/13607863.2015.1081152
18. Berkman LF, Glass T, Brissette I, et al. From social integration to health: durkheim in the new millennium. Soc Sci Med. 2000;51(6):843–857. doi:10.1016/S0277-9536(00)00065-4
19. Holt-Lunstad J, Smith TB, Layton JB, Brayne C. Social relationships and mortality risk: a meta-analytic review. PLoS Med. 2010;7(7):e1000316. doi:10.1371/journal.pmed.1000316
20. Kolaitis NA, Gao Y, Soong A, et al. Depressive symptoms in lung transplant recipients: trajectory and association with mortality and allograft dysfunction. Thorax. 2022;77(9):891–899. doi:10.1136/thoraxjnl-2021-217612
21. Zhu Q, Gu P, Wang Y, et al. Exploring the exercise experiences of lung transplant recipients during the waiting list period: a qualitative study. Int J Nurs Stud. 2025;170:105160. doi:10.1016/j.ijnurstu.2025.105160
22. Carstensen LL, Meeks S. Socioemotional selectivity theory: the role of perceived endings in human motivation. Gerontologist. 2021;61(8):1188–1196. doi:10.1093/geront/gnab116
23. Kurosawa S, Yamaguchi T, Mori A, et al. Resignation and return to work in patients receiving allogeneic hematopoietic cell transplantation close up. J Cancer Surviv. 2022;16(5):1004–1015. doi:10.1007/s11764-021-01092-w
24. Bhatt NS. Prevalence and determinants of return to work as a patient-centered outcome in survivors of hematopoietic cell transplantation. Curr Hematol Malig Rep. 2022;17(6):228–242. doi:10.1007/s11899-022-00678-0
25. Stellern J, Xiao KB, Grennell E, et al. Emotion regulation in substance use disorders: a systematic review and meta-analysis. Addiction. 2023;118(1):30–47. doi:10.1111/add.16001
26. Van Den Broek JM, Brunsveld-Reinders AH, Zedlitz AMEE, et al. Questionnaires on family satisfaction in the adult ICU: a systematic review including psychometric properties. Crit Care Med. 2015;43(8):1731–1744. doi:10.1097/CCM.0000000000000980
27. Wasser T, Pasquale MA, Matchett SC, et al. Establishing reliability and validity of the critical care family satisfaction survey. Crit Care Med. 2001;29(1):192–196. doi:10.1097/00003246-200101000-00038
28. Munsif M, Donnan M, Snell G, et al. Return-to-work in lung transplant recipients: an Australian perspective. Intern Med J. 2025;55(3):415–425. doi:10.1111/imj.16641
29. Petrucci L, Ricotti S, Michelini I, et al. Return to work after thoracic organ transplantation in a clinically-stable population. Eur J Heart Fail. 2007;9(11):1112–1119. doi:10.1016/j.ejheart.2007.08.002
30. Ferrario A, Verga FC, Piolatto PG, et al. Return to work after organ transplantation: a cross-sectional study on working ability evaluation and employment status. Transplant Proc. 2014;46(10):3273–3277. doi:10.1016/j.transproceed.2014.08.038
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Exploring Vision-Related Quality of Life: A Qualitative Study Comparing Patients’ Experience of Cataract Surgery with a Standard Monofocal IOL and an Enhanced Monofocal IOL
Blancafort Alias S, Del Campo Carrasco Z, Salvador-Miras I, Luna Mariné S, Gómez Prieto MJ, Liñán Martín F, Salvà Casanovas A
Clinical Ophthalmology 2022, 16:1641-1652
Published Date: 27 May 2022
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Multiple Myeloma Experiences and Preferences: A Mixed Methods Study of Patients and Care Partners in the United States
Flora DR, Byrd R, Platt DA, Hlavacek P, Hoag Goldman E, Cappelleri JC, Kennedy CT, LeBlanc TW
Patient Preference and Adherence 2025, 19:963-979
Published Date: 8 April 2025
A Qualitative Study of Migraine Headache Experience in Patients with Patent Foramen Ovale Based on the Symptom Management Theory
Li M, Feng M, Li M, Wei J, Li S, Zhang N, Li Q, Song R, Li H
Patient Preference and Adherence 2025, 19:2363-2375
Published Date: 10 August 2025