Back to Journals » Clinical Ophthalmology » Volume 16
Exploring Vision-Related Quality of Life: A Qualitative Study Comparing Patients’ Experience of Cataract Surgery with a Standard Monofocal IOL and an Enhanced Monofocal IOL
Authors Blancafort Alias S, Del Campo Carrasco Z, Salvador-Miras I, Luna Mariné S, Gómez Prieto MJ, Liñán Martín F, Salvà Casanovas A ![]()
Received 31 January 2022
Accepted for publication 29 April 2022
Published 27 May 2022 Volume 2022:16 Pages 1641—1652
DOI https://doi.org/10.2147/OPTH.S358386
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sergi Blancafort Alias,1 Zoraida Del Campo Carrasco,2 Ignacio Salvador-Miras,2 Sabina Luna Mariné,2 María José Gómez Prieto,2 Francesca Liñán Martín,2 Antoni Salvà Casanovas1
1Fundació Salut i Envelliment (Health and Ageing Foundation), Universitat Autònoma de Barcelona (UAB), Barcelona, 08041, Spain; 2Service of Ophthalmology, Hospital de Sant Pau, Barcelona, 08025, Spain
Correspondence: Sergi Blancafort Alias, Fundació Salut i Envelliment (Health and Ageing Foundation), Universitat Autònoma de Barcelona (UAB), Sant Antoni Maria Claret, 171, Barcelona, 08041, Spain, Tel +34 93 433 50 30, Email [email protected]
Purpose: To explore quality of life related with intermediate vision of patients before and after cataract surgery, and to make patients’ experience available for the design of future scales that assess visual function related with intermediate distance.
Patients and Methods: A qualitative research methodology based on thematic content analysis was used to explore vision-related quality of life based on the experiences of patients with cataract. Patients were recruited at the Service of Ophthalmology of the Hospital de Sant Pau (Barcelona, Spain). Data were collected through nineteen semi-structured interviews conducted with patients diagnosed with cataract and implanted with a standard aspheric monofocal intraocular lens (IOL) (Tecnis® ZA9003) (n = 6), an enhanced monofocal IOL (Tecnis® Eyhance ICB000) (n = 6), and patients from the waiting list (n = 7). The data analysis consisted in coding, aggregation, and theme development of the transcribed audios.
Results: Patients on waiting lists reported difficulty and insecurity in performing daily and meaningful tasks related to near visual ranges (eg: threading a needle, reading price tags), intermediate (eg: using a computer or dialling numbers on a smartphone), and distant (eg: recognizing faces, walking on uneven surfaces). Patients after surgery with the standard IOL reported improvement in performing activities mainly in the distant visual range, but also the need for a better communication with clinical staff to adjust their own expectations on the results of the surgery. Finally, patients implanted with the enhanced IOL reported satisfaction and improved visual function in performing daily activities, especially those related to the intermediate visual range.
Conclusion: Our exploratory study found that patients after cataract surgery with the enhanced IOL reported a better performance in activities that require the intermediate vision. These results will inform the development of scales to assess vision-related quality of life in the intermediate visual range prioritizing outcomes according to patients’ daily and meaningful activities.
Keywords: quality of life, cataract, qualitative research, intraocular lenses
Introduction
Cataract is among the most common causes of visual impairment in older people, affecting more than 90% of those aged 65 and over.1 Visual impairment has an impact on person’s ability to perform tasks safely and easily in different functional domains, including ambulation, driving, household management, work performance, financial and legal responsibilities, and recreation and leisure activities.2 Visual impairment in older adults is also associated with reduced participation,3 mobility functions,4 falls risk5 and to a fear of falling, which restrict their physical activities and put them at risk for social isolation and disability6 and can lead to functional decline, depression, increased falls risk, and reduced quality of life.5 Moreover, visually impaired people generally have a higher prevalence of anxiety disorders and depression compared with people with good vision.7,8 Hence, visual impairment has an impact on all aspects of daily life9 and threatens the well-being of the individual.10
Cataract surgery has been shown to be cost-effective and to report consistent benefits in reducing disability, limitation in activities, anxiety, depression, risk of falls and fractures,11–17 being phacoemulsification the preferred surgical technique in the developed world and tertiary centers in developing countries to remove cataract.18–21 Several types of new intraocular lenses (IOL) have been introduced in surgical procedures during last years and reported to influence patients’ opinions about their vision after cataract extraction.22 A few studies have shown that an enhanced monofocal IOL provides, compared to other standard monofocal IOL, similar visual acuity at near and distant range and better performance at the intermediate distance range (50–100 cm).23–27 Intermediate distance range covers a zone of activities including computer work, cooking, shopping, engaging in conversation, eating, controlling the car dashboard, or organizing a desk. Hence, it may be a reasonable option for those more dependent on intermediate vision in daily activities.28
From the patient’s viewpoint, cataract and cataract surgery can influence many quality-of-life aspects affected by poor visual acuity, which may include ocular symptoms (eg, glare and halos), limitations to activities of daily living and convenience (freedom from spectacles).29 Vision-related quality of life is a growing topic of interest in the literature. It is related with patients’ concerns about coping with everyday life, incapacity to carry out ability preferred activities, and psychological distress including fear, lack of safety, frustration, annoyance, depression, embarrassment, and loneliness.30 However, vision-related quality of life in patients with cataract has been mostly assessed using ophthalmic instruments originally developed for other eye diseases or non-disease specific patient-reported outcome instruments, and hence less sensitive to change.31,32 Furthermore, few questionnaires measuring patient-reported outcomes related to visual function have been developed for cataract surgery,33,34 and no specific scales have been identified to assess visual function in the intermediate distance range. The aim of this study was to explore vision-related quality of life of patients before and after cataract surgery with different types of IOL and to highlight relevant issues for the future development of scales that assess visual function in the intermediate visual range.
Materials and Methods
The qualitative theoretical framework used in this study was phenomenology, which aims to describe the essence of a phenomenon from the perspective of those who have experienced it.35 A convenience sampling technique was used to recruit 19 patients diagnosed with cataract through the service of ophthalmology at Hospital de Sant Pau (Barcelona, Spain). Sample size determination was guided by the criterion of saturation and informational redundancy, which means that no new data is elicited by sampling more units. Participants were distributed into one of these three study groups: Patients implanted with a standard aspheric monofocal IOL (Tecnis® ZA9003) (Group 1), patients implanted with an enhanced monofocal IOL (Tecnis® Eyhance ICB000) (Group 2), and patients from the waiting list (Group 3). The difference between the two lenses is that the model of the standard IOL is exclusively monofocal, while the enhanced IOL is monofocal with an improved intermediate function. The latter features a smooth continuous power change from the center towards the lens periphery. This feature seems to increase the depth of focus, thus mitigating the effects of presbyopia and delivering sharp vision at different distances. Both models have a modified anterior surface with a sphericity of −0.27 μm across their entire optic zone of 6 mm. They also have a 360 degrees continuous posterior squared margin. Their Abbe number is 55 and refractive index is 1.47.
Inclusion criteria: Patients had to be aged 65 or over, to be diagnosed with cataract, and to be emmetrope post-operatively (Sphere ± 0,5D; CyL ≤ 0,75D) with binocular visual acuity of at least 1.0 measured on the Snellen scale (groups 1 and 2) or with binocular visual acuity of 0.5 (6/12) (minimum eyesight standard for driving) measured on the Snellen scale (group 3). To avoid recall bias, patients did not know the type of lens they had been implanted. Face-to-face interviews were conducted between June and October of 2020. Due to the outbreak of the second wave of the COVID-19 pandemic in Spain (November 2020), the research team decided to carry out phone interviews instead of face-to-face interviews, until data saturation was reached. Moreover, three health professionals (two ophthalmologists and one optometrist) from the Service of Ophthalmology of the Hospital de Sant Pau were interviewed for triangulation purposes.
A semi-structured questionnaire with open-ended questions was developed ad hoc and used for the interviews. The questionnaire explored aspects related to the difficulty perceived by participants in performing tasks at different visual ranges before and after surgery, and its impact on several aspects of their vision-related quality of life. Adjustments to the questionnaire were made according to the data collection method (face-to-face or phone interview) and to previous experience and information participants had provided. All interviews were carried out by a researcher with a background in sociology of health who was not known to the participants before the beginning of the study. Face-to-face interviews were conducted in consultation rooms located at the Service of Ophthalmology at the Hospital de Sant Pau with all measures to prevent the transmission of COVID-19 (wearing masks, physical distancing, hydroalcoholic gel and ventilation). With respect to phone interviews, they were previously scheduled so that patients could feel comfortable and have enough time to attend the call. All interviews were digitally recorded with permission from participants and transcribed onto a Microsoft Word® file. Data collected were listed, coded, and categorized by visual range adapting the framework proposed by Atkinson et al.36 Data processing occurred as an iterative process, so analysis started before data collection was completed. The study was complied with the Declaration of Helsinki and approved by the Ethics Committee of the Autonomous University of Barcelona. Participants received oral and written information about the study and signed the informed consent, which included publication of anonymised data. Participation in the study was volunteer, and participants did not receive any economic compensation.
Results
The characteristics of participants are presented in Table 1. The age of participants ranged from 63 to 85 years old. Almost twice as many participants were women (63.16%). About half of participants had completed secondary studies (42.10%), a little more than a fourth had completed higher studies (26.31%) and a little less than a third (31.58%) had completed only primary studies or had not completed any studies at all. Only four participants (21.05%) were born in the same city where they currently live (Barcelona). The majority of them were married (68%) with only one participant living alone (5.26%).
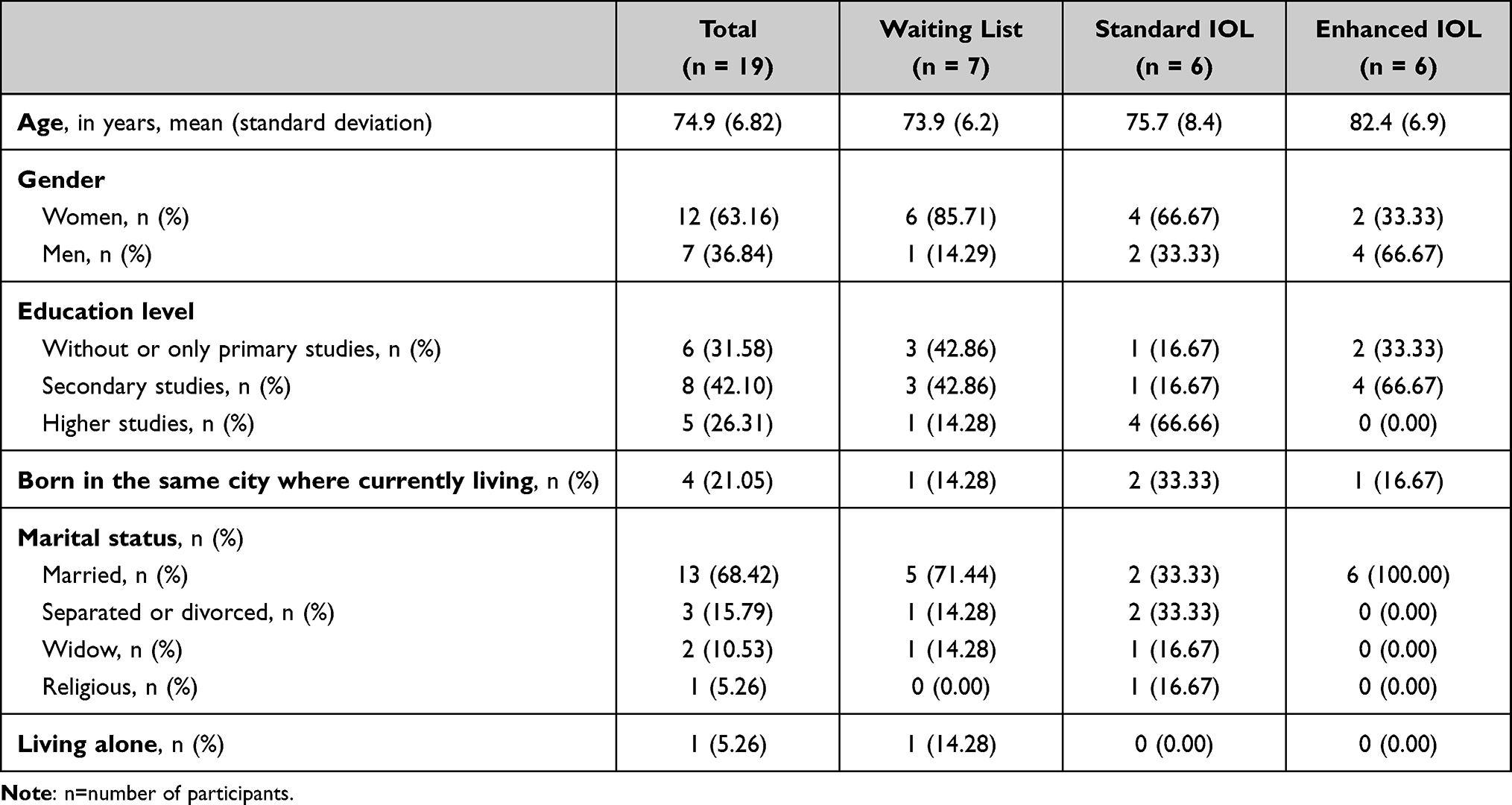 |
Table 1 Characteristics of Participants by Group |
Performance of Daily Tasks Before Surgery
Transcripts were used to create lists of vision-dependent tasks organized in continuous visual ranges. Tables 2–4 show tasks reported by patients as difficult to perform in the near, intermediate, and distant visual range before cataract surgery. Some examples of daily activities related to near vision included threading a needle and do-it-yourself tasks, while others imply strong limitations when shopping in a supermarket (see the price tags of products, read the expiration dates on nutritional labels). Reading also emerged as an important activity for patients, which was limited by cataract, causing feelings of disappointment, frustration, and sadness. Regarding the intermediate visual range, using the computer and watching TV were two of the most frequently mentioned activities. Specifically, they named problems to see the faces and read the subtitles on the screen. A second group of tasks that patients were unable to enjoy before the surgery included handcraft activities (eg, sewing and cross-stitch pattern). Thirdly, feelings of fear, insecurity, or even physical symptoms (eg, headache) emerged when patients talk about their difficulties to walk on uneven ground or to climb and/or descend steps, which clearly limit the possibility of going out from home. Finally, patients also highlighted the difficult of recognizing people at a certain approaching distance as well as facial expressions, which is something that obviously can affect social relationships. With respect to distant range, several examples were given related to the lack of safety when driving, either at night or with adverse atmospheric conditions. Other patients expressed feelings of anxiety when travelling inside a car before cataract surgery. One last example pointed to the difficulty of following small rapid balls, which means the impossibility to enjoy some sports.
 |
Table 2 Performance of Tasks in the Near Visual Range Before the Surgery |
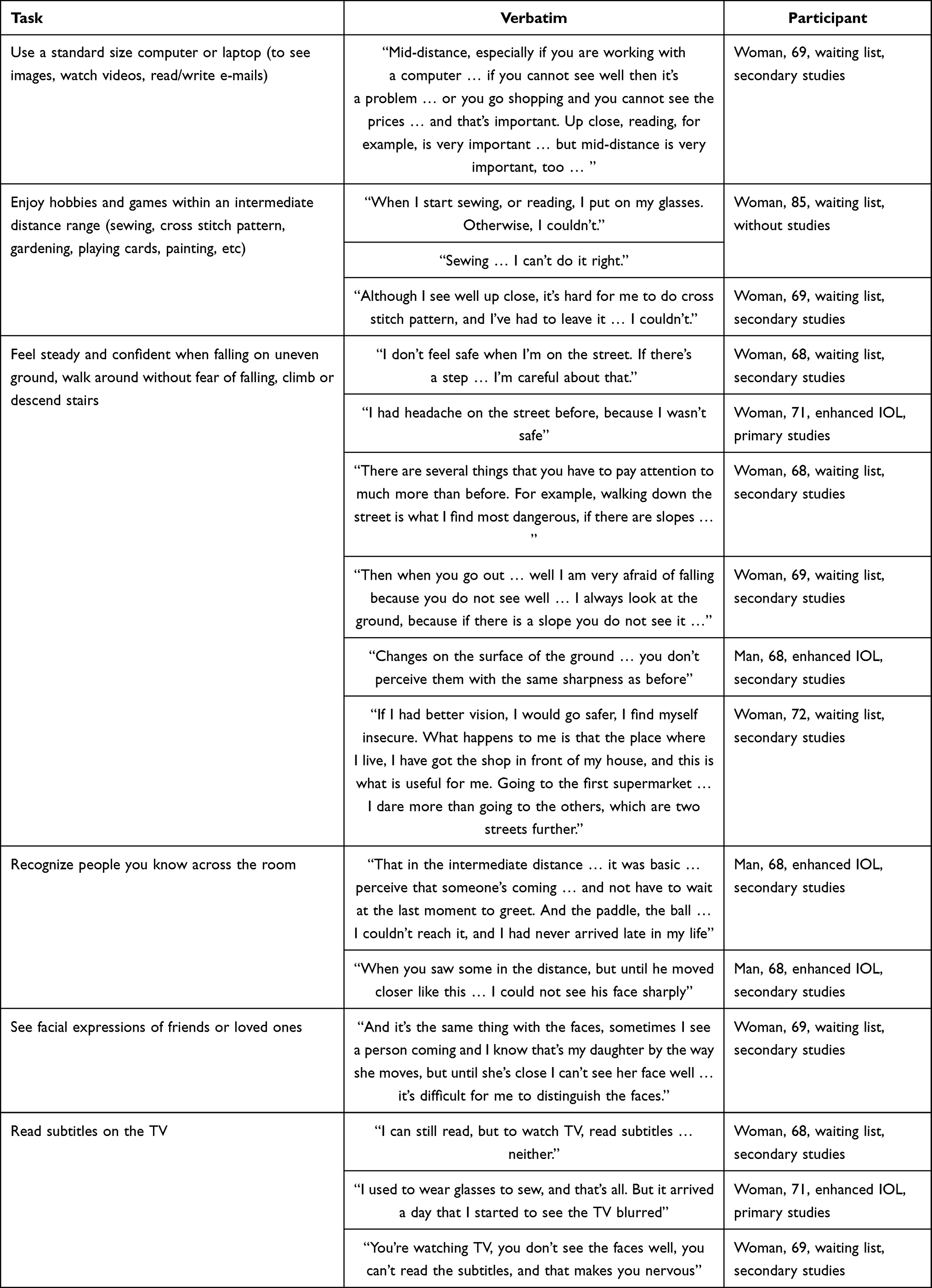 |
Table 3 Performance of Tasks in the Intermediate Visual Range Before the Surgery |
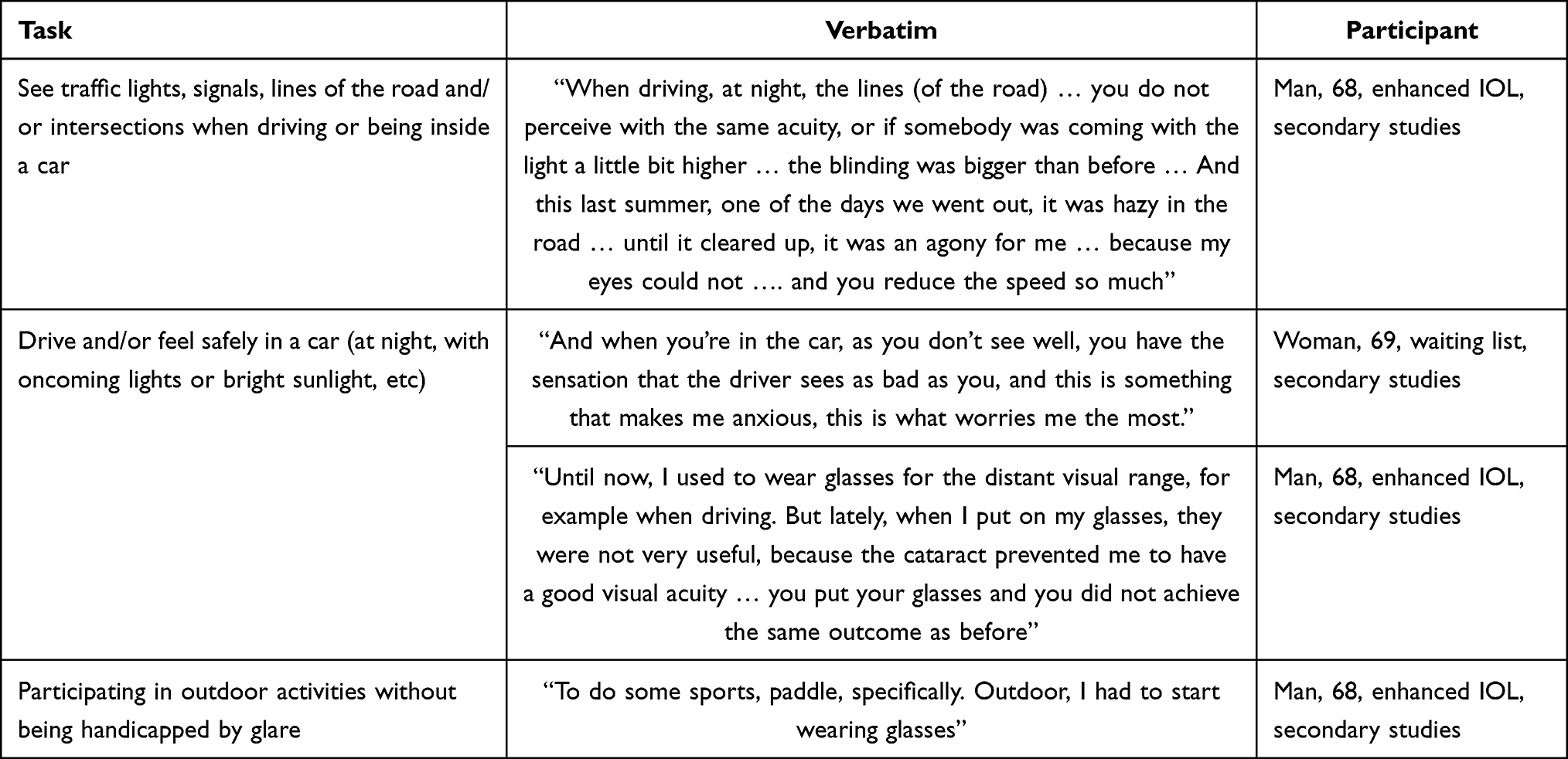 |
Table 4 Performance of Tasks in the Distant Visual Range Before the Surgery |
Impact of Cataract Surgery on the Vision-Related Quality of Life
Table 5 shows changes in the performance of vision-dependent tasks and vision-related quality of life before and after surgery. With respect to near and distant vision, improvements in the performance of tasks were found in patients who were implanted with the standard IOL as well as those implanted with the enhanced IOL. Examples given by participants referred to the possibility of seeing their own wrinkles for the first time, reading price tags, and threading a needle. They expressed their satisfaction to see things clearer, which implies that they were able to drive safer and to enjoy sightseeing. As for the intermediate visual range, only patients implanted with the enhanced IOL reported improvements in the performance of some tasks. Several examples were referred to feel safer walking on the street due to the possibility of seeing well uneven surfaces or steps. A few patients related that they had enjoyed watching the TV again because they could read the subtitles and see images. Nevertheless, it was easier for them to use the public transport because they could clearly read the numbers of the buses or the names of the stations, while others expressed their joy due to the possibility of recognizing faces, which was considered very important for social interaction. Additionally, several participants mentioned that they had gained additional comfort because they only needed to wear glasses for few tasks at a near distance. Finally, some patients implanted with the enhanced IOL made comments explicitly referring to the quality of life they have recovered after the surgery, because they did not need to accommodate the vision or wear glasses all the time, they could see clearly along different visual ranges or even help other people with vision limitations.
 |
Table 5 Changes in the Performance of Vision-Dependent Tasks and Vision-Related Quality of Life Before and After Surgery |
Discussion
This study was aimed to explore intermediate vision-related quality of life of patients before and after cataract surgery with a standard IOL and an enhanced IOL. Particularly, we identified limitations to perform vision-dependent tasks in the near, intermediate, and distant visual ranges, and assessed the degree of difficulty and importance of activities of daily living, before and after the surgery with both IOL. Furthermore, we tried to establish vision-related quality of life relevant issues for the future development of patient-reported outcomes measures of visual function, and to provide evidence of content validity for the design of future scales that assess visual tasks or functions occurring in the intermediate visual range. We used phenomenology as a valid qualitative theoretical framework to carry out the study, which has been widely used in the field of ophthalmology to explore patients’ quality of life.37–39 Data were collected through 19 semi-structured interviews conducted with patients in the waiting list for cataract surgery, implanted with a standard IOL and an enhanced IOL. Our findings showed that patients from waiting list reported difficulty in performing daily tasks related with near, intermediate, and distant visual ranges. Patients after surgery with either standard or enhanced IOL reported improvement in performing activities in the near and distant visual ranges, and the need for a better communication with clinical staff to adjust own expectations. However, only patients implanted with the enhanced IOL reported major satisfaction and improved visual function in performing daily living activities related to the intermediate and extended-intermediate visual range. Several studies have reported the same visual acuity at near and distant range and better outcomes at intermediate distance range.23–27 Visual function in patients affected by cataract has been traditionally assessed using visual acuity instruments. However, these measures do not reflect the major effects that cataract have in vision-related quality of life, caused mostly by difficulty in performing daily and meaningful tasks.40 Some researchers have evidenced how self-reported measures of vision-related quality of life can be helpful to assess the subjective wellbeing and visual disability of patients when they perform common activities in daily life41 and hence, several questionnaires examining vision-related quality of life have been developed with research purposes.42,43 Two of the questionnaires mostly used with this aim are the National Eye Institute Visual Functioning Questionnaire-25 (NEI VFQ-25)44 designed to assess quality of life in patients with visual problems, and the Visual Function Index-14 (VF-14) designed to measure functional impairment on patients due to cataract and largely used in the Spanish population.45 However, several researchers46,47 have reported problems with the utilization of both instruments, such as measurement redundancies and measurement voids, suggesting a low ability to differentiate among participants with higher levels of visual function, and concluding that neither the NEI VFQ‐25 nor VF‐14 is optimal for the assessment of vision-related quality of life in patients with cataract surgery.29 During last years, researchers have also focused their efforts on the development of cataract patient-reported outcome measures with enough characteristics in terms of brevity, precision, and responsiveness to be used in clinical practice.48 Among them, the Catquest-9SF49,50 and the most recent CAT-PROM34 have shown to be short, psychometrically robust instruments. Both have been validated in English-speaking contexts and Catquest-9F has also been validated in other languages including Spanish.51,52 The use of qualitative research to establish the basis of task-based content for patient-reported outcomes of visual function have been explored previously by other researchers36 who identified several gaps in task content and distance-specific constructs associated with visual function, including the lack of scales to assess visual tasks for the intermediate visual range, as well as to assess the use of technological devices, and the fact that there were only found two measures to assess ambulatory accident risks.
Strengths and Limitations of the Study
Our study has several limitations. First, the COVID-19 pandemic has dramatically affected the development of the study. Recruitment and availability of patients was compromised by successive outbreaks, and the final round of interviews had to be completed by phone. This is an important point to consider when it comes to interpreting the results. Secondly, the relevance of tasks and activities highlighted by patients may be considered with caution due to the diversity of profiles, the specific pandemic context, and the fact that the sample was limited, and thus sociodemographic characteristics of the participants (sex, age, educational level) may influence the kind of tasks or activities reported. For example, six of the seven patients in the waiting list group included in the study were women, and due to the generational context, examples of activities mentioned may be subjected to bias. Otherwise, the educational level achieved by participants may also influence the type of activities performed. Previous research has suggested the use of Ecological Event Monitoring methodology to identify routine tasks, which may be affected by poor vision, as well as keeping a daily event register of specific difficulties.53 Data collection and analysis were performed along six months (June 16th, 2020-December 28th, 2020) for several reasons. First, the epidemiological context due to the COVID-19 pandemic conditioned the possibility of doing interviews with patients. Second, fear of infection and workload of the clinical staff influenced the recruitment. Third, interviews with patients from Group 2 were conditioned to the availability of enhanced IOL. However, we believe that the results of our qualitative research provide rich and detailed information about the importance and meaningfulness of daily tasks influencing several domains of life. In particular, we point to the tasks performed in the intermediate visual range as potential items to consider when designing instruments to improve vision-related quality of life. Moreover, our findings provide support for the inclusion of technology tasks and task safety content in future measures of cataract patient-reported outcomes. Further research is required to examine the relationships between the visual distances required for task performance and their associations with established clinical measures of visual acuity and vision-related quality of life.
Conclusion
Our exploratory qualitative study found that patients after cataract surgery with an enhanced IOL reported a better performance of activities that require the intermediate visual range. Further research aimed to develop scales assessing vision-related quality of life in these visual ranges should prioritize outcomes according to patients’ daily and meaningful activities. In particular, our findings provide support for the inclusion of technology tasks and task safety content in future measures of cataract patient-reported outcomes.
Acknowledgments
This study has been funded by Johnson and Johnson Vision Surgical through an Independent Investigator Study (IIS) Research Grant. Johnson & Johnson Vision Surgical provided 16 Tecnis® Eyhance ICB000 Intraocular Lens free of charge for the aims of the study. The authors would like to thank the patients who participated in the study for their valuable contribution and their time. A communication (poster) of this work was presented at the congress of the European Society of Cataract and Refractive Surgery (ESCRS).
Disclosure
Dr Ignacio Salvador-Miras reports personal fees from Johnson and Johnson Vision, outside the submitted work; Dr. Sergi Blancafort Alias and Dr Antoni Salvà Casanovas report grants from Johnson and Johnson Vision Surgical, during the conduct of the study. The authors declare no other conflicts of interest in this work.
References
1. GBD 2019 Blindness and Vision Impairment Collaborators; Vision Loss Expert Group of the Global Burden of Disease Study. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the right to sight: an analysis for the Global Burden of Disease Study [published correction appears in Lancet Glob Health. 2021 Apr;9(4):e408]. Lancet Glob Health. 2021;9(2):e144–e160. doi:10.1016/S2214-109X(20)30489-7.
2. World Health Organization. Blindness and Vision impairment; October 14, 2021. Available from: http://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment.
3. Shah K, Frank CR, Ehrlich JR. The association between vision impairment and social participation in community-dwelling adults: a systematic review. Eye. 2020;34(2):290–298. doi:10.1038/s41433-019-0712-8
4. Miyata K, Yoshikawa T, Harano A, Ueda T, Ogata N. Effects of visual impairment on mobility functions in elderly: results of Fujiwara-kyo Eye Study. PLoS One. 2021;16(1):e0244997. doi:10.1371/journal.pone.0244997
5. White UE, Black AA, Wood JM, Delbaere K. Fear of falling in vision impairment. Optom Vis Sci. 2015;92(6):730–735. doi:10.1097/OPX.0000000000000596
6. Wang MY, Rousseau J, Boisjoly H, et al. Activity limitation due to a fear of falling in older adults with eye disease. Invest Ophthalmol Vis Sci. 2012;53(13):7967–7972. doi:10.1167/iovs.12-10701
7. Evans JR, Fletcher AE, Wormald RP. Depression and anxiety in visually impaired older people. Ophthalmology. 2007;114(2):283–288. doi:10.1016/j.ophtha.2006.10.006
8. Binder KW, Wrzesińska MA, Kocur J. Anxiety in persons with visual impairment. Psychiatr Pol. 2020;54(2):279–288. English, Polish. doi:10.12740/PP/OnlineFirst/85408
9. Stevelink SA, Malcolm EM, Fear NT. Visual impairment, coping strategies and impact on daily life: a qualitative study among working-age UK ex-service personnel. BMC Public Health. 2015;15(1):1118. doi:10.1186/s12889-015-2455-1
10. Weber JA, Wong KB. Older adults coping with vision loss. Home Health Care Serv Q. 2010;29(3):105–119. doi:10.1080/01621424.2010.511505
11. Bourne RRA, Flaxman SR, Braithwaite T, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(9):e888–e89. doi:10.1016/S2214-109X(17)30293-0
12. IAPB Vision Atlas. Number of people affected by vision loss; 2020. Available from: http://atlas.iapb.org/global-burden-vision-impairment/gbvi-global-cause-estimates.
13. Kupfer C. The National Eye Institute’s low vision education program: improving quality of life. Ophthalmology. 2020;107(2):229–230. doi:10.1016/S0161-6420(99)00094-9
14. Universal eye health: a global action plan 2014–2019. Geneva: World Health Organization; 2013. Available from: http://www.who.int/blindness/actionplan/en/.,
15. Vela C, Samson E, Zunzunegui MV, Haddad S, Aubin MJ, Freeman EE. Eye care utilization by older adults in low, middle, and high income countries. BMC Ophthalmol. 2012;12(1):5. doi:10.1186/1471-2415-12-5
16. Coleman AL, Yu F, Keeler E, Mangione CM. Treatment of uncorrected refractive error improves vision-specific quality of life. J Am Geriatr Soc. 2006;54(6):883–890. doi:10.1111/j.1532-5415.2006.00817.x
17. Owsley C, McGwin G Jr, Scilley K, Meek GC, Seker D, Dyer A. Effect of refractive error correction on health-related quality of life and depression in older nursing home residents. Arch Ophthalmol. 2007;125(11):1471–1477. doi:10.1001/archopht.125.11.1471
18. Gogate PM, Deshpande M, Wormald RP, Deshpande R, Kulkarni SR. Extracapsular cataract surgery compared with manual small incision cataract surgery in community eye care setting in western India: a randomised controlled trial. Br J Ophthalmol. 2003;87:667–672. doi:10.1136/bjo.87.6.667
19. Hennig A. Sutureless non-phaco cataract surgery: a solution to reduce worldwide cataract blindness? Community Eye Health. 2003;16:49–51.
20. Astbury N. Converting from ECCE to SICS. Community Eye Health. 2009;22(69):6–7.
21. Gogate P. Clinical trials of manual small incision cataract surgery and standard extracapsular cataract surgery: results of quality of life. J Community Eye Health. 2003;16:5.
22. Calladine D, Evans JR, Shah S, Leyland M, Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev. 2012;133(9):CD003169. doi:10.1002/14651858.CD003169.pub3
23. Mencucci R, Cennamo M, Venturi D, Vignapiano R, Favuzza E. Visual outcome, optical quality, and patient satisfaction with a new monofocal IOL, enhanced for intermediate vision: preliminary results. J Cataract Refract Surg. 2020;46(3):378–387. doi:10.1097/j.jcrs.0000000000000061
24. Auffarth GU, Gerl M, Tsai L, et al. Clinical evaluation of a new monofocal intraocular lens with enhanced intermediate function in cataract patients. J Cataract Refract Surg. 2020. doi:10.1097/j.jcrs.0000000000000399
25. Lopes D, Loureiro T, Carreira R, et al. Comparative evaluation of visual outcomes after bilateral implantation of an advanced or conventional monofocal intraocular lens. Eur J Ophthalmol. 2021: 229–234. doi:10.1177/1120672121995343.
26. De luis Eguileor B, Martínez-Indart L, Martínez Alday N, Sacristán Egüén C, Cuadros Sánchez C. Differences in intermediate vision: monofocal intraocular lenses vs. monofocal extended depth of focus intraocular lenses. Arch Soc Esp Oftalmol. 2020;95(11):523–527. English, Spanish. doi:10.1016/j.oftal.2020.06.009
27. Cinar E, Bolu H, Erbakan G, et al. Vision outcomes with a new monofocal IOL. Int Ophthalmol. 2021;41(2):491–498. doi:10.1007/s10792-020-01599-8
28. Yangzes S, Kamble N, Grewal S, Grewal SPS. Comparison of an aspheric monofocal intraocular lens with the new generation monofocal lens using defocus curve. Indian J Ophthalmol. 2020;68(12):3025–3029. doi:10.4103/ijo.IJO_985_20
29. Wan Y, Zhao L, Huang C, et al. Validation and comparison of the National Eye Institute Visual Functioning Questionnaire-25 (NEI VFQ-25) and the Visual Function Index-14 (VF-14) in patients with cataracts: a multicentre study [published online ahead of print, 2020 Sep 17]. Acta Ophthalmol. 2020;99(4):e480–e488. doi:10.1111/aos.14606
30. Elliott DB, Pesudovs K, Mallinson T. Vision-related quality of life. Optom Vis Sci. 2007;84(8):656–658. doi:10.1097/OPX.0b013e31814db01e
31. Longworth L, Yang Y, Young T, et al. Use of generic and condition‐specific measures of health‐related quality of life in NICE decision‐making: systematic review, statistical modelling and survey. Health Technol Assess. 2014;18(9). doi:10.3310/hta18090.
32. McAlinden C, Gothwal VK, Khadka J, Wright TA, Lamoureux EL, Pesudovs K. A head-to-head comparison of 16 cataract surgery outcome questionnaires. Ophthalmology. 2011;118(12):2374–2381. doi:10.1016/j.ophtha.2011.06.008
33. Lundstrom M, Pesudovs K. Catquest-9SF patient outcomes questionnaire; nine-item short-form Rasch-scaled revision of the Catquest questionnaire. J Cataract Refract Surg. 2009;35(3):504–513. doi:10.1016/j.jcrs.2008.11.038
34. Sparrow JM, Grzeda MT, Frost NA, et al. Cat-PROM5: a brief psychometrically robust self-report questionnaire instrument for cataract surgery. Eye. 2018;32(4):796–805. doi:10.1038/eye.2018.1
35. Teherani A, Martimianakis T, Stenfors-Hayes T, Wadhwa A, Varpio L. Choosing a qualitative research approach. J Grad Med Educ. 2015;7(4):669. doi:10.4300/JGME-D-15-00414.1
36. Atkinson MJ, Tally S, Heichel CW, Kozak I, Leich J, Levack A. A qualitative investigation of visual tasks with which to assess distance-specific visual function. Qual Life Res. 2013;22(2):437–453. doi:10.1007/s11136-012-0154-2
37. Iyigun E, Tastan S, Ayhan H, et al. Life experiences of patients with glaucoma: a phenomenological study. J Nurs Res. 2017;25(5):336–343. doi:10.1097/jnr.0000000000000172
38. Wu PX, Guo WY, Xia HO, Lu HJ, Xi SX. Patients’ experience of living with glaucoma: a phenomenological study. J Adv Nurs. 2011;67(4):800–810. doi:10.1111/j.1365-2648.2010.05541.x
39. Prem Senthil M, Lim L, Braithwaite T, et al. The impact of adult uveitis on quality of life: an exploratory study. Ophthalmic Epidemiol. 2020:1–9. doi:10.1080/09286586.2020.1856385.
40. Groessl EJ, Liu L, Sklar M, Tally SR, Kaplan RM, Ganiats TG. Measuring the impact of cataract surgery on generic and vision‐specific quality of life. Qual Life Res. 2013;22(6):1405–1414. doi:10.1007/s11136-012-0270-z
41. Fung SS, Luis J, Hussain B, Bunce C, Hingorani M, Hancox J. Patient‐reported outcome measuring tools in cataract surgery: clinical comparison at a tertiary hospital. J Cataract Refract Surg. 2016;42(12):1759–1767. doi:10.1016/j.jcrs.2016.08.037
42. Massof RW, Rubin GS. Visual function assessment questionnaires. Surv Ophthalmol. 2001;45(6):531–548. doi:10.1016/S0039-6257(01)00194-1
43. Rentz AM, Kowalski JW, Walt JG, et al. Development of a preference‐based index from the National Eye Institute Visual Function Questionnaire‐25. JAMA Ophthalmol. 2014;132(3):310–318. doi:10.1001/jamaophthalmol.2013.7639
44. Marella M, Pesudovs K, Keeffe JE, O’Connor PM, Rees G, Lamoureux EL. The psychometric validity of the NEI VFQ‐25 for use in a low‐vision population. Invest Ophthalmol Vis Sci. 2010;51(6):2878–2884. doi:10.1167/iovs.09-4494
45. Valderas JM, Rue M, Guyatt G, et al. The impact of the VF-14 index, a perceived visual function measure, in the routine management of cataract patients. Qual Life Res. 2005;14(7):1743–1753. doi:10.1007/s11136-005-1745-y
46. Gothwal VK, Reddy SP, Sumalini R, Bharani S, Bagga DK. National Eye Institute Visual Function Questionnaire or Indian Vision Function Questionnaire for visually impaired: a conundrum. Invest Ophthalmol Vis Sci. 2012;53(8):4730–4738. doi:10.1167/iovs.11-8776
47. Kovac B, Vukosavljevic M, Djokic Kovac J, et al. Validation and cross‐cultural adaptation of the National Eye Institute Visual Function Questionnaire (NEI VFQ‐25) in Serbian patients. Health Qual Life Outcomes. 2015;13(1):142. doi:10.1186/s12955-015-0330-5
48. Sparrow JM, Grzeda MT, Frost NA, et al. Cataract surgery patient-reported outcome measures: a head-to-head comparison of the psychometric performance and patient acceptability of the Cat-PROM5 and Catquest-9SF self-report questionnaires. Eye. 2018;32(4):788–795. doi:10.1038/eye.2017.297
49. Lundström M, Pesudovs K. Catquest-9SF patient outcomes questionnaire: nine-item short-form Rasch-scaled revision of the Catquest questionnaire. J Cataract Refract Surg. 2009;35(3):504–513. doi:10.1016/j.jcrs.2008.11.038
50. Lundström M, Pesudovs K. Questionnaires for measuring cataract surgery outcomes. J Cataract Refract Surg. 2011;37(5):945–959. doi:10.1016/j.jcrs.2011.03.010
51. Gothwal VK, Wright TA, Lamoureux EL, Lundström M, Pesudovs K. Catquest questionnaire: re-validation in an Australian cataract population. Clin Exp Ophthalmol. 2009;37(8):785–794. doi:10.1111/j.1442-9071.2009.02133.x
52. Lundstrom MD, Llovet F, Llovet A, et al. Validation of the Spanish Catquest-9SF in patients with a monofocal or trifocal intraocular lens. J Cataract Refract Surg. 2016;42(12):1791–1796. doi:10.1016/j.jcrs.2016.10.011
53. Stone A, Kessler R, Haythornthwaite J. Measuring daily events and experiences: decisions for the researcher. J Pers. 1991;59(3):575–607. doi:10.1111/j.1467-6494.1991.tb00260.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Visual Outcomes, Spectacle Independence, and Patient-Reported Satisfaction of the Vivity Extended Range of Vision Intraocular Lens in Patients with Early Glaucoma: An Observational Comparative Study
Kerr NM, Moshegov S, Lim S, Simos M
Clinical Ophthalmology 2023, 17:1515-1523
Published Date: 30 May 2023
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Multiple Myeloma Experiences and Preferences: A Mixed Methods Study of Patients and Care Partners in the United States
Flora DR, Byrd R, Platt DA, Hlavacek P, Hoag Goldman E, Cappelleri JC, Kennedy CT, LeBlanc TW
Patient Preference and Adherence 2025, 19:963-979
Published Date: 8 April 2025
A Qualitative Study of Migraine Headache Experience in Patients with Patent Foramen Ovale Based on the Symptom Management Theory
Li M, Feng M, Li M, Wei J, Li S, Zhang N, Li Q, Song R, Li H
Patient Preference and Adherence 2025, 19:2363-2375
Published Date: 10 August 2025
Tailored Personas for Lung Transplant Recipients’ Return-to-Work Experiences: A Secondary Analysis of Qualitative Data
Huang K, Wang S, Cai L, Chen Z, Cao X, Zhou H
Patient Preference and Adherence 2026, 20:603119
Published Date: 12 June 2026