Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
TACE Sequential to Radiofrequency Ablation versus RFA Alone in Hepatocellular Carcinoma Within Milan Criteria
Authors Yan H, Zhao C ![]() , Liu M, Liu H, Mu L
, Liu M, Liu H, Mu L ![]() , Xiang Z, Huang M
, Xiang Z, Huang M ![]()
Received 14 May 2025
Accepted for publication 18 July 2025
Published 12 August 2025 Volume 2025:12 Pages 1795—1805
DOI https://doi.org/10.2147/JHC.S534039
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ali Hosni
Huzheng Yan,1,* Chenghao Zhao,1,* Mingming Liu,2,* Huan Liu,1 Luwen Mu,1 Zhanwang Xiang,1,* Mingsheng Huang1,*
1Department of Interventional Radiology, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China; 2Department of Radiology, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mingsheng Huang, Email [email protected] Zhanwang Xiang, Email [email protected]
Objective: This study aimed to compare the efficacy and safety of transarterial chemoembolization followed by radiofrequency ablation (cTACE-RFA) versus RFA alone in patients with early-stage hepatocellular carcinoma (HCC) within the Milan criteria.
Methods: A retrospective analysis included 343 patients with Milan criteria-compliant HCC. After 1:1 propensity score matching (PSM), 93 patients underwent cTACE-RFA, and 93 received RFA alone. Primary endpoints were overall survival (OS) and local progression-free survival (LPFS).
Results: The TACE-RFA group demonstrated significantly superior 1-, 3-, and 5-year LPFS rates (84.9%, 58.1%, 36.6%) compared to the RFA group (75.3%, 44.1%, 16.1%; HR=0.54, 95% CI: 0.37– 0.79, P=0.001). However, no significant 1-, 3-, and 5-year OS difference (HR = 1.06, 95% CI: 0.61– 1.83, p = 0.843) was observed between cTACE-RFA (95.7%, 80.6%, 59.1%) and RFA alone group (96.8%, 78.5%, 61.3%). Subgroup analyses revealed significant OS improvements with cTACE-RFA in tumor with high-risk locations (HR = 0.38; 95% CI: 0.17– 0.85, p = 0.018) and diameter 3– 5 cm: (HR = 0.28; 95% CI: 0.12– 0.64, p = 0.003). cTACE-RFA group also was observed significant LPFS improvements for tumors in high-risk locations (HR=0.48, 95% CI: 0.30– 0.77, p=0.002) or 3– 5 cm in size (HR=0.25, 95% CI: 0.15– 0.41, p< 0.001). Complication rates were comparable, with no procedure-related mortality and similar severe adverse event incidences (P=0.516).
Conclusion: cTACE-RFA significantly prolongs LPFS compared to RFA alone in early HCC, particularly for tumors > 3 cm or in high-risk locations, without increasing major complications.
Keywords: hepatocellular carcinoma, radiofrequency ablation, transarterial chemoembolization
Introduction
Hepatocellular carcinoma (HCC) ranks as the third leading cause of cancer-related mortality worldwide, with its incidence rising steadily against the backdrop of chronic liver disease.1–3 For early-stage HCC meeting the Milan criteria (single tumor ≤5 cm or ≤3 tumors each ≤3 cm), surgical resection, liver transplantation, and radiofrequency ablation (RFA) serve as primary curative therapies.4,5 However, RFA alone is associated with a notably high local recurrence rate of 20–30%, particularly for subcapsular tumors or those adjacent to major vessels, where incomplete ablation may result from the heat sink effect or overly conservative ablation strategies.6
Transarterial chemoembolization (TACE), the standard treatment for intermediate- to advanced-stage HCC, occludes tumor vasculature while delivering chemotherapeutic agents.7–9 This dual mechanism not only reduces tumor burden but also mitigates the heat sink effect within the ablation zone, potentially enhancing RFA efficacy.10–12 Accumulating evidence suggests that TACE combined with microwave ablation (MWA) or RFA significantly improves survival and local control in patients with HCC >3 cm.13,14 Nevertheless, the therapeutic value of TACE followed by RFA (TACE-RFA) for early-stage HCC within the Milan criteria—especially tumors ≤3 cm located in high-risk anatomical regions (eg, near the diaphragm or major vessels)—remains contentious. For instance, Lee et al reported that TACE-RFA achieved a markedly lower 5-year local tumor progression rate compared to TACE alone (16.5% vs 37.0%) in ultrasound-invisible HCC,15 whereas Cao et al found no significant long-term survival advantage of TACE-RFA over RFA monotherapy for HCC ≤3 cm, except in high-risk subgroups (eg, tumors >2 cm or perivascular lesions).16
Against this unresolved debate, our study aims to compare the prognostic differences between TACE-RFA and RFA alone in Milan criteria-adherent HCC, with the goal of providing evidence-based insights for personalized interventional strategies in early-stage HCC management.
Materials and Methods
Study Population
A retrospective analysis was conducted on patients with early-stage hepatocellular carcinoma (HCC) within the Milan criteria (single tumor ≤5 cm or ≤3 tumors each ≤3 cm, absence of macrovascular invasion and extrahepatic metastasis) treated between January 1, 2017, and December 31, 2021. Patients receiving radiofrequency ablation (RFA) alone as curative therapy were assigned to the RFA group, while those undergoing conventional transarterial chemoembolization (cTACE) followed by RFA 4–6 weeks later were assigned to the cTACE-RFA group. Key inclusion criteria were: (1) Milan criteria-compliant HCC; (2) age 18–70 years; (3) Eastern Cooperative Oncology Group (ECOG) performance status 0–1; (4) Child-Pugh class A/B; and (5) ineligibility or refusal of surgical resection or liver transplantation. Exclusion criteria included: (1) HCC beyond Milan criteria; (2) recurrent HCC or extrahepatic metastasis; (3) prior ablation therapy; and (4) incomplete data. Initially, 141 patients were enrolled in the RFA group and 202 in the cTACE-RFA group. After 1:1 propensity score matching (PSM) to balance baseline characteristics, 93 matched pairs were included in the final analysis.
The diagnosis of HCC was based on the European Association for the Study of the Liver. The study protocol was approved by the Ethics Committee of the Third Affiliated Hospital of Sun Yat-sen University, with waived informed consent due to its retrospective nature. This retrospective study was conducted in accordance with the Declaration of Helsinki. Patient data confidentiality was strictly maintained, and all data were anonymized for analysis.
TACE Procedure
Patients were placed in the supine position. Under local anesthesia, the Seldinger technique was used to puncture the femoral artery and insert a 5F introducer sheath (Terumo, Japan). A 5F hepatic artery catheter (Cook Medical, USA) was advanced into the celiac trunk under digital subtraction angiography (DSA) guidance to map tumor-feeding arteries. A 2.7F microcatheter (Progreat, Terumo) was then superselectively navigated into tumor-afferent branches using a 0.014-inch microguidewire (Asahi Intecc, Japan), with adjunctive cone-beam CT (CBCT) for three-dimensional localization of tumor vasculature and satellite lesions. An emulsion of epirubicin (30–50 mg) and lipiodol (Guerbet, France) at a 1:2–1:3 ratio was slowly infused through the microcatheter. For hypervascular tumors, additional embolization was performed using gelatin sponge particles (100–300 μm, Gelfoam, Pfizer) or polyvinyl alcohol microspheres (Embosphere, Merit Medical) until complete devascularization or stasis was achieved. Post-embolization DSA or CBCT confirmed satisfactory lipiodol deposition. All procedures adhered to the European Association for the Study of the Liver (EASL) guidelines and were performed by interventional radiologists with ≥10 years of experience.4 Epirubicin dosage was adjusted by body surface area (50 mg/m²), and embolization endpoints were defined as complete occlusion of tumor vasculature.
RFA Procedure
Patients were positioned supine or laterally, with local anesthesia (2% lidocaine) and intravenous sedation (midazolam 0.05 mg/kg). Ablation trajectories were planned using preprocedural contrast-enhanced CT/MRI. A 17-gauge cooled-tip electrode (Cool-tip™ RF System, Boston Scientific, USA) was deployed under CT guidance. For tumors ≤3 cm, single-needle single-point ablation was performed, while tumors 3–5 cm required multi-needle overlapping or umbrella-shaped ablation (needle spacing: 1.0–2.0 cm). Manufacturer-recommended parameters included power output 60–120 W, ablation duration 10–15 minutes per session, and target temperature 90–100°C. Post-ablation tract coagulation was performed to prevent bleeding and tumor seeding. Immediate post-procedural contrast-enhanced CT assessed ablation margins, with supplemental ablation applied for residual viable tissue. Patients were monitored for 24 hours for complications (eg, pain, fever). All RFA procedures followed EASL guidelines4 and were conducted by experienced interventional radiologists (≥10 years). Ablation zones were designed to encompass the tumor with a 5–10 mm safety margin, and prolonged ablation (15–20 minutes) was applied for perivascular tumors to counteract the heat sink effect.
Follow-up and Outcomes
In the cTACE-RFA group, technical success was evaluated via contrast-enhanced CT/MRI at 1 month post-TACE using mRECIST criteria. All patients underwent follow-up contrast-enhanced CT/MRI or contrast-enhanced ultrasound (CEUS), alpha-fetoprotein (AFP) testing, liver function, and coagulation profiles at 1 month post-RFA, then every 3 months for 3 years, and biannually thereafter. Suspected recurrence prompted intensified imaging (1–2 month intervals). Multidisciplinary teams determined salvage therapies (eg, repeat ablation, TACE, and targeted/immunotherapy) for recurrent or new lesions. Primary endpoints were local progression-free survival (LPFS) and overall survival (OS), OS was defined as the interval from enrollment in the study until the death or the last follow-up record. LPFS was defined as the time interval from enrollment in the study to local tumor recurrence or the last review. LPFS was selected as the primary endpoint to specifically evaluate the efficacy of locoregional treatments (TACE-RFA vs RFA) in controlling local tumor progression, which is the most direct measure of ablative success. Distant progression was excluded from this endpoint to avoid confounding by extrahepatic metastasis, which may be influenced by systemic factors beyond local treatment control. Tumor response was classified per mRECIST (complete/partial response, stable/progressive disease).
High-risk location refers to the organ that may be damaged by radiofrequency ablation, and the tumor is within 2cm from gastrointestinal tract, gallbladder, hilar region, diaphragm, heart and liver capsule.Technical success required absence of enhanced tissue in the ablation zone on 1-month imaging. Adverse events (eg, liver abscess, hemorrhage) were graded using CTCAE v5.0.
Statistical Analysis
Data were analyzed using SPSS 26.0 (IBM, USA) and GraphPad Prism 8.0 (GraphPad Software, USA). Continuous variables are expressed as mean ± SD, and categorical variables as frequencies (%). Intergroup comparisons utilized independent t-tests, Mann–Whitney U-tests, or chi-square/Fisher’s exact tests. Survival curves were generated via Kaplan–Meier method with Log rank testing. Multivariate Cox regression identified independent prognostic factors (variables with P<0.10 in univariate analysis). Propensity scores were calculated using logistic regression (covariates: age, sex, etiology, tumor size/location, Child-Pugh class, AFP, albumin, bilirubin), matched 1:1 with a caliper of 0.02. Standardized mean differences (SMD < 0.10) confirmed post-matching balance.
Results
Patient Baseline Characteristics
The study flow chart was shown in Figure 1. A total of 343 patients with early-stage hepatocellular carcinoma (HCC) within the Milan criteria were included, comprising 141 patients in the cTACE-RFA group and 202 in the RFA group. After 1:1 propensity score matching (PSM), 93 matched pairs were analyzed. Baseline characteristics of the patients were shown in Table 1. Prior to matching, significant baseline differences existed between groups in age (cTACE-RFA: 56.9 ± 11.9 years vs RFA: 56.5 ± 10.9 years, P = 0.030), maximum tumor diameter (30.4 ± 17.6 mm vs 23.3 ± 14.2 mm, P = 0.002), high-risk anatomical locations (67.4% vs 40.1%, P < 0.001), and Child-Pugh class B proportion (12.8% vs 5.9%, P = 0.017). Post-PSM, baseline variables were well balanced, with no significant differences in age (55.9 ± 11.3 vs 54.5 ± 10.6 years, P = 0.332), tumor diameter (24.0 ± 11.3 vs 19.9 ± 9.5 mm, P = 0.417), high-risk locations (58.1% vs 48.4%, P = 0.186), or other key parameters (all standardized mean differences [SMD] < 0.10). Etiology (hepatitis B: 86.0% vs 87.1%), AFP levels (≤100 ng/mL: 74.2% vs 71.0%), and liver function markers (ALT, albumin, bilirubin) were also comparable post-matching (P > 0.05).
 |
Table 1 Patient Characteristics |
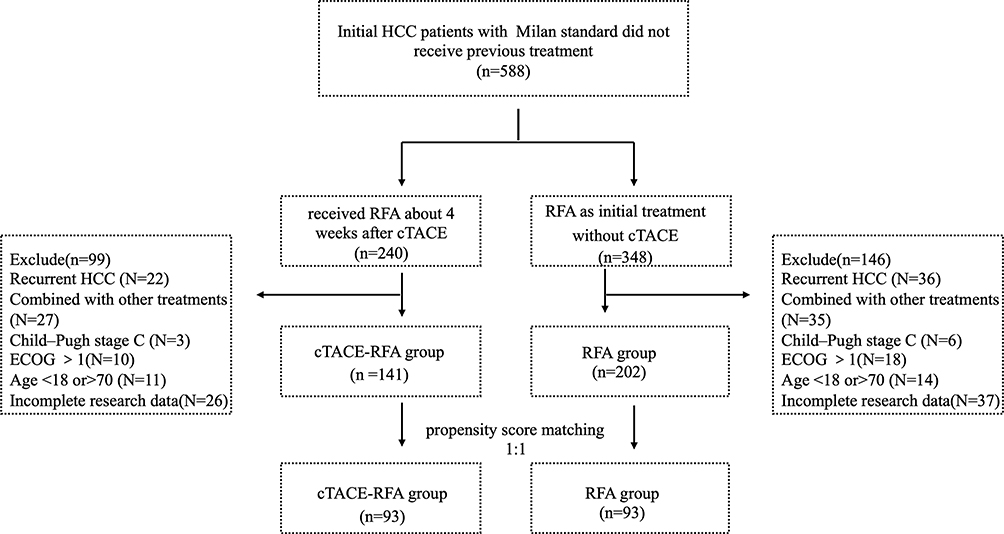 |
Figure 1 Flow chart of enrolled patient selection. Abbreviations: HCC, Hepatocellular carcinoma; TACE, Transarterial chemoembolization; RFA, Radiofrequency ablation. |
Technical Success and Efficacy
In the cTACE-RFA group, all patients underwent RFA 4–6 weeks after TACE. A total of 103 lesions (93 patients: 85 with 1 lesion, 6 with 2 lesions, and 2 with 3 lesions) were ablated in the cTACE-RFA group, compared to 104 lesions (93 patients: 85 with 1 lesion, 5 with 2 lesions, and 3 with 3 lesions) in the RFA group. Technical success rates were similar between groups (98.9% vs 97.8%, P = 1.00). The cTACE-RFA group required an average of 1.3 ablation needles (range: 1–3), with a power of 120.6 W (80–160 W) and ablation duration of 16.4 minutes (8–30 minutes), whereas the RFA group used 1.4 needles (1–3), 125.2 W (80–140 W), and 16.2 minutes (7–28 minutes).
Overall Survival (OS)
The median follow-up duration was 42 months (range: 24–90 months). The 1-, 3-, and 5-year overall survival (OS) rates were 95.7%, 80.6%, and 59.1% for the cTACE-RFA group, compared to 96.8%, 78.5%, and 61.3% for the RFA group, respectively. No significant intergroup difference was observed (HR = 1.06, 95% CI: 0.61–1.83, p = 0.843). As detailed in Table 2 and Figure 2, univariate analysis identified the following predictors of improved prognosis: age ≤60 years (p = 0.002), maximum tumor diameter ≤3 cm (p = 0.007), solitary tumor (p = 0.006), Child-Pugh class A (p = 0.023), albumin ≥35 g/dL (p = 0.001), and non-high-risk tumor location (p = 0.034).
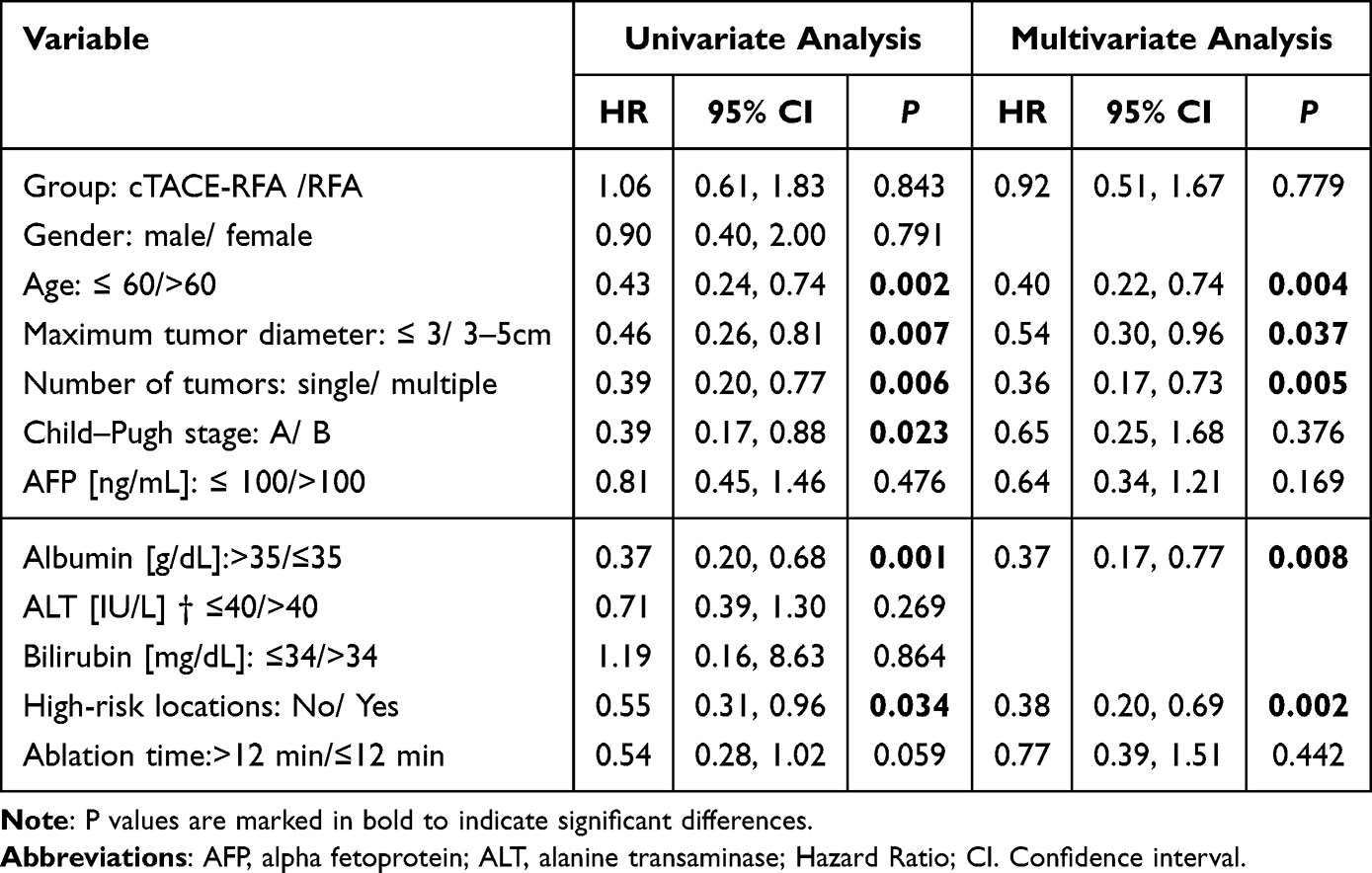 |
Table 2 Univariate Analysis and Cox Proportional Hazards Regression Analysis Related to OS |
 |
Figure 2 Overall survival (Kaplan–Meier analysis). (A) Overall survival between groups. (B) Subgroup analysis for tumors in high-risk locations. (C) Subgroup analysis for tumors with a maximum diameter of 3–5 cm. |
Multivariate Cox regression demonstrated no OS benefit for cTACE-RFA over RFA alone (HR = 0.92, p = 0.779). Notably, age ≤60 years (HR = 0.40, 95% CI: 0.22–0.74, p = 0.004), maximum tumor diameter ≤3 cm (HR = 0.54, 95% CI: 0.30–0.96, p = 0.037), solitary tumor (HR = 0.36, 95% CI: 0.17–0.73, p = 0.005), and albumin ≥35 g/L (HR = 0.37, 95% CI: 0.17–0.77, p = 0.008) emerged as independent protective factors for OS. Additionally, non-high-risk tumor location was associated with superior survival (HR = 0.38, 95% CI: 0.20–0.69, p = 0.002). Subgroup analyses revealed significant OS improvements with cTACE-RFA in tumor with high-risk locations (HR = 0.38; 95% CI: 0.17–0.85, p = 0.018) and diameter 3–5 cm: (HR = 0.28; 95% CI: 0.12–0.64, p = 0.003).
Local Progression-Free Survival (LPFS)
The cTACE-RFA group demonstrated superior 1-, 3-, and 5-year LPFS rates (84.9%, 58.1%, and 36.6%) compared to the RFA group (75.3%, 44.1%, and 16.1%; HR = 0.54, 95% CI: 0.37–0.79, P = 0.001). As detailed in Table 3 and Figure 3, Multivariate Cox regression confirmed the LPFS advantage of cTACE-RFA (HR = 0.50, P = 0.001), alongside tumor size ≤3 cm (HR = 0.61, P = 0.023) and non-high-risk locations (HR = 0.58, P = 0.007). Prolonged ablation time (>12 minutes) showed marginal LPFS benefit (HR = 0.70, P = 0.076). Subgroup analyses highlighted significant LPFS improvements for tumors in high-risk locations (HR=0.48, 95% CI: 0.30–0.77, p=0.002) or 3–5 cm in size (HR=0.25, 95% CI: 0.15–0.41, p<0.001) with cTACE-RFA.
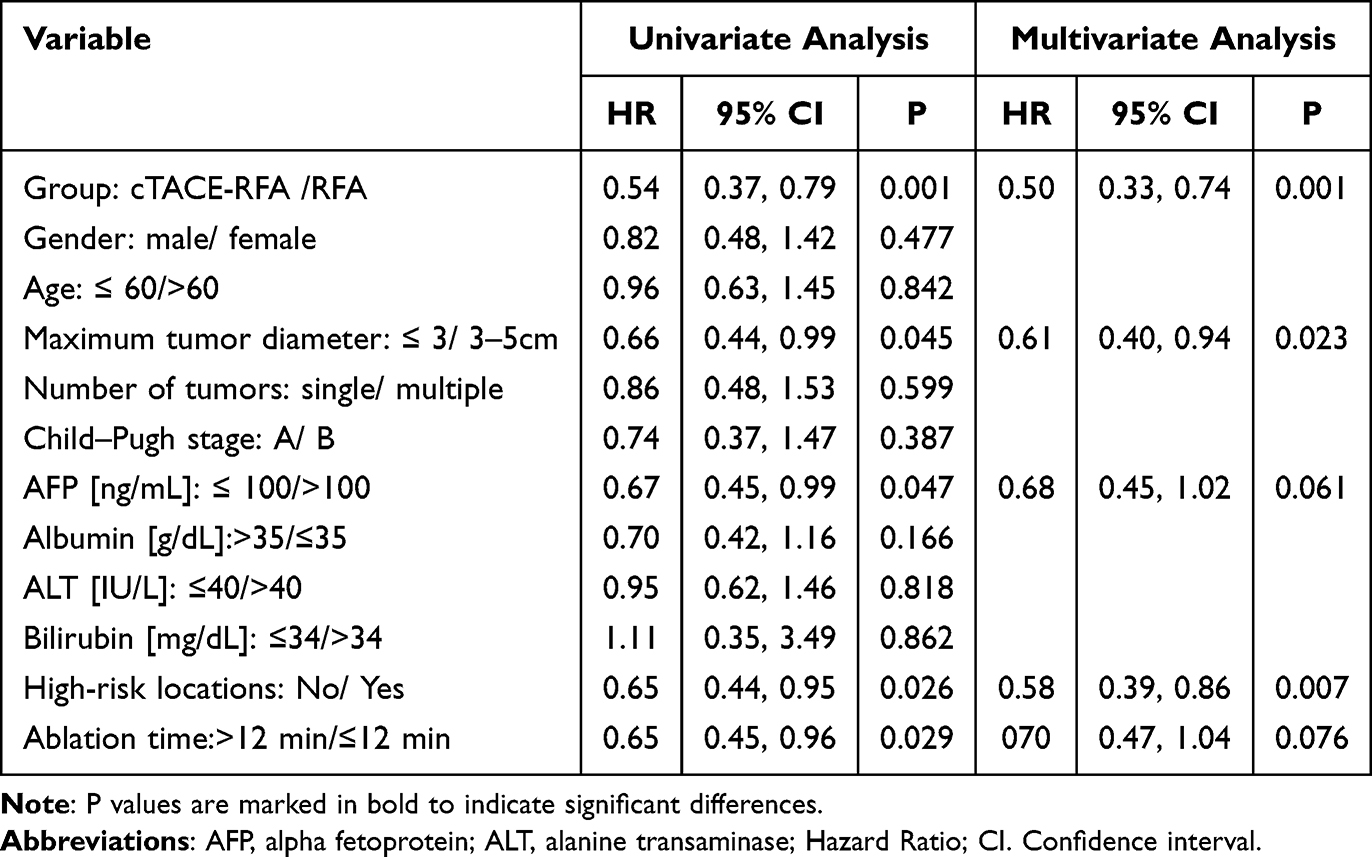 |
Table 3 Univariate Analysis and Cox Proportional Hazards Regression Analysis Related to LPFS |
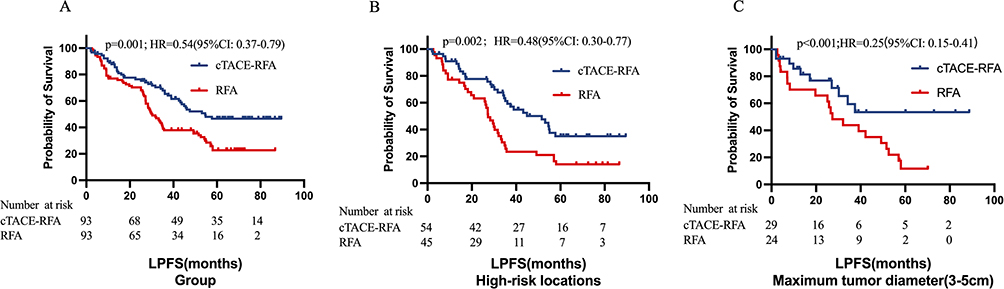 |
Figure 3 Local progression-free survival (Kaplan–Meier analysis). (A) Progression-free survival between groups. (B) Subgroup analysis for tumors in high-risk locations. (C) Subgroup analysis for tumors with a maximum diameter of 3–5 cm. |
Complications
No procedure-related mortality occurred. Common adverse events included transient pain, fever, and elevated transaminases, managed conservatively. Perihepatic hemorrhage occurred in 2 cTACE-RFA and 4 RFA patients (P = 0.678), with one cTACE-RFA case requiring embolization. Minor pneumothorax (2 cases) and liver abscess (1 RFA case) resolved without intervention. Biliary injury causing obstructive jaundice (1 cTACE-RFA case) necessitated percutaneous transhepatic cholangial drainage (PTCD). Severe complication rates did not differ significantly between groups (P = 0.516).
Discussion
This propensity score-matched analysis evaluates the comparative efficacy of cTACE followed by RFA (cTACE-RFA) versus RFA monotherapy in patients with early-stage HCC within the Milan criteria. Our findings demonstrate that the combined therapy significantly improved local tumor control, as evidenced by superior LPFS, though no overall survival (OS) benefit was observed. Subgroup analyses further revealed that cTACE-RFA conferred pronounced advantages in tumors located at high-risk anatomical sites (eg, adjacent to major vessels or the diaphragm, as shown in Figure 4) or with diameters of 3–5 cm. These results provide critical insights for optimizing individualized therapeutic strategies in early-stage HCC.
 |
Figure 4 A case of RFA for HCC in high-risk anatomical locations. (A and B) Pre-procedural T2-weighted and contrast-enhanced arterial phase MRI showing a lesion (As indicated by the white arrow) in hepatic segments S2/S3, adjacent to the liver capsule, spleen, and diaphragm. The white arrow shows the ablation range immediately after radiofrequency ablation. (C and D) CT-guided radiofrequency ablation procedure. (E and F) Post-RFA imaging at 1 month: T2-weighted and contrast-enhanced MRI confirming complete necrosis of the lesion (As indicated by the white arrow). |
The superior LPFS in the cTACE-RFA group aligns with prior studies and may be attributed to TACE’s dual mechanism of vascular embolization and lipiodol-mediated delineation of tumor margins.17 By occluding tumor-feeding arteries, TACE reduces intraprocedural heat-sink effects—a major contributor to incomplete ablation in perivascular tumors.18,19 Furthermore, lipiodol deposition enhances intraoperative visualization, minimizing residual disease risk.20 These synergies likely explain the marked LPFS improvement in high-risk subgroups, where conventional RFA alone often fails to achieve adequate ablation margins.
The absence of OS differences between groups may reflect several factors. First, early-stage HCC patients inherently exhibit prolonged survival, necessitating longer follow-up to discern survival disparities. Second, salvage therapies (eg, repeat ablation and systemic agents) post-recurrence may attenuate initial treatment-related survival advantages.4,21 This observation corroborates meta-analyses suggesting that OS benefits of combined therapies are more pronounced in intermediate/advanced HCC, whereas early-stage cohorts often exhibit comparable survival due to favorable prognoses.22
Subgroup analyses identified tumor location and size as pivotal determinants of therapeutic outcomes. For tumors in high-risk regions, cTACE-RFA’s ability to downsize lesions and optimize ablation conditions likely underlies its LPFS advantage.23 Similarly, the enhanced efficacy in tumors measuring 3–5 cm supports the notion that Milan-criteria HCC is a heterogeneous entity requiring tailored approaches. These findings resonate with Yang et al’s meta-analysis, which highlighted the superiority of combined therapies in tumors >3 cm.24
Multivariate analysis identified age ≤60 years, solitary tumors, albumin ≥35 g/dL, and non-high-risk locations as independent predictors of favorable OS. Albumin levels, reflective of hepatic functional reserve, are strongly associated with treatment tolerance and survival—a finding consistent with recent prognostic models.25–27 Additionally, non-high-risk anatomical positions reduced LPFS risk by 42% (HR=0.58, p=0.007), suggesting that RFA monotherapy suffices for these lesions, whereas high-risk subgroups demand aggressive combinations. Although our cohort did not receive concurrent immune checkpoint inhibitors or tyrosine kinase inhibitors, recent studies suggest that combining locoregional therapies with systemic agents may enhance outcomes in intermediate-stage HCC.28 The potential synergy of TACE-RFA with such therapies in early-stage HCC warrants future investigation.
Safety profiles were comparable between groups, with no significant difference in severe complications (p=0.516). The low incidence of major adverse events (eg, biliary injury and abscess) underscores the feasibility of sequential TACE-RFA,19,29 aligning with Zhao et al’s conclusion that combined therapies do not substantially elevate procedural risks.30
This study has limitations. First, the retrospective single-center design introduces potential selection bias, despite rigorous propensity score matching. Second, the modest sample size, particularly in high-risk subgroups, may limit statistical power. Third, the median follow-up of 42 months precludes assessment of long-term survival (eg, 10-year OS). Lastly, technological advancements such as microwave ablation (MWA)—which offers superior thermal efficacy for larger tumors—may influence generalizability. Future research should focus on TACE monotherapy, TACE-MWA and TACE-RFA.31
Conclusion
In early-stage HCC within the Milan criteria, TACE-RFA offers superior LPFS over RFA alone, particularly for tumors with maximum tumor diameter 3–5cm or in high-risk locations, without compromising safety. While OS benefits remain elusive, this combined approach represents a rational strategy to optimize local control in select subgroups. Our findings advocate for personalized treatment algorithms guided by tumor anatomy, size, and hepatic reserve.
Abbreviations
HCC, Hepatocellular carcinoma; OS, Overall survival; RFA, Radiofrequency ablation; MWA, Microwave ablation; TACE, Transarterial chemoembolization; ECOG, Eastern Cooperative Oncology Group; PSM, Propensity score matching; LPFS, Local Progression-Free Survival; RECIST, Response Evaluation Criteria in Solid Tumors; AFP, Alpha fetoprotein.
Data Sharing Statement
Requests for access to the data should be directed to the corresponding author, who will provide the necessary information and materials to ensure proper use and interpretation of the data.
Acknowledgments
We would like to express our sincere gratitude to the Department of Interventional Radiology and the Department of Radiology at the Third Affiliated Hospital of Sun Yat-sen University for their support and assistance throughout this study.
Author Contributions
Huzheng Yan: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Writing – original draft
Mingsheng Huang: Conceptualization, Project administration, Resources, Supervision, Writing – review and editing
Zhanwang Xiang: Conceptualization, Project administration, Resources, Supervision, Writing – review and editing
Chenghao Zhao: Conceptualization, Methodology, Project administration, Resources, Writing – review and editing
Mingming Liu: Data curation, Formal analysis, Writing – original draft, Writing – review and editing
Huan Liu: Data curation, Formal analysis, Project administration, Software, Supervision, Writing – review and editing
Luwen Mu: Formal analysis, Software, Project administration
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Beijing iGandan Foundation: i GandanF-1082025-YLPS010.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. doi:10.3322/caac.21660
2. Gordan John D, Kennedy Erin B, Abou-Alfa Ghassan K, et al. Systemic therapy for advanced hepatocellular carcinoma: ASCO guideline. J Clin Oncol. 2020;38:4317–4345. doi:10.1200/JCO.20.02672
3. Vogel A, Cervantes A, Chau I, et al. Hepatocellular carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29:iv238–iv255. doi:10.1093/annonc/mdy308
4. European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of hepatocellular carcinoma. J Hepatol. 2025;82:315–374. doi:10.1016/j.jhep.2024.08.028
5. Xi M, Yang Z, Hu L, et al. Radiofrequency ablation versus stereotactic body radiotherapy for recurrent small hepatocellular carcinoma: a randomized, open-label, controlled trial. J Clin Oncol. 2025;43:1073–1082. doi:10.1200/JCO-24-01532
6. Kang TW, Lim HK, Lee MW, et al. Long-term therapeutic outcomes of radiofrequency ablation for subcapsular versus nonsubcapsular hepatocellular carcinoma: a propensity score matched study. Radiology. 2016;280:300–312. doi:10.1148/radiol.2016151243
7. Da-Long Y, Lin Y, Fan-Jian Z, et al. Multicenter, retrospective GUIDANCE001 study comparing transarterial chemoembolization with or without tyrosine kinase and immune checkpoint inhibitors as conversion therapy to treat unresectable hepatocellular carcinoma: survival benefit in intermediate or advanced, but not early, stages. Hepatology. 2025. doi:10.1097/HEP.0000000000001229
8. Ma T, Bai X, Zhang Q, et al. Adjuvant transarterial chemoembolization for hepatocellular carcinoma following curative resection: a randomized, open-label, Phase 3 trial. Hepatology. 2025. doi:10.1097/HEP.0000000000001233
9. Fan W, Zhu B, Chen S, et al. Survival in patients with recurrent intermediate-stage hepatocellular carcinoma: sorafenib plus TACE vs TACE alone randomized clinical trial. JAMA Oncol. 2024;10:1047–1054. doi:10.1001/jamaoncol.2024.1831
10. Zhang Y-J, Chen J, Zhou Z, et al. Transarterial chemoembolization with radiofrequency ablation versus surgical resection for small late-recurrence hepatocellular carcinoma. Radiology. 2025;314:e241096. doi:10.1148/radiol.241096
11. Krupa K, Fudalej M, Cencelewicz-Lesikow A, et al. Current treatment methods in hepatocellular carcinoma. Cancers. 2024;16:4059. doi:10.3390/cancers16234059
12. Patel Krishnan R, Hari M, Patel Roshal R, et al. Locoregional therapies for hepatocellular carcinoma: a systematic review and meta-analysis. JAMA Network Open. 2024;7:e2447995. doi:10.1001/jamanetworkopen.2024.47995
13. Shin SW, Ahn KS, Kim SW, et al. liver resection versus local ablation therapies for hepatocellular carcinoma within the Milan criteria: a systematic review and meta-analysis. Ann Surg. 2021;273:656–666. doi:10.1097/SLA.0000000000004350
14. Shi F, Lian S, Mai Q, et al. Microwave ablation after downstaging of hepatocellular carcinoma: outcome was similar to tumor within Milan criteria. Eur Radiol. 2020;30:2454–2462. doi:10.1007/s00330-019-06604-y
15. Hyukjoon L, Jin YC, Jong SN, et al. Comparison of combined therapy using conventional chemoembolization and radiofrequency ablation versus conventional chemoembolization for ultrasound-invisible early-stage hepatocellular carcinoma (Barcelona Clinic Liver Cancer Stage 0 or A). Korean J Radiol. 2018;19:1130–1139.
16. Cao S, Zou Y, Lyu T, et al. Long-term outcomes of combined transarterial chemoembolization and radiofrequency ablation versus RFA monotherapy for single hepatocellular carcinoma ≤3 cm: emphasis on local tumor progression. Int J Hyperthermia. 2022;39:1–7. doi:10.1080/02656736.2021.1998660
17. Zaitoun Mohamed MA, Elsayed Saeed B, Zaitoun Nahla A, et al. Combined therapy with conventional trans-arterial chemoembolization (cTACE) and microwave ablation (MWA) for hepatocellular carcinoma >3-<5 cm. Int J Hyperthermia. 2021;38:248–256. doi:10.1080/02656736.2021.1887941
18. Chen L, Ren Y, Sun T, et al. The efficacy of radiofrequency ablation versus cryoablation in the treatment of single hepatocellular carcinoma: a population-based study. Cancer Med. 2021;10:3715–3725. doi:10.1002/cam4.3923
19. Yan H, Xiang Z, Zhao C, et al. Long-term outcomes of patients with hepatocellular carcinoma who underwent microwave ablation after downstaging with transarterial chemoembolization to Barcelona clinic liver cancer stage. A J Vasc Interv Radiol. 2023;34:768–776. doi:10.1016/j.jvir.2022.12.466
20. Tsai Y-C, Shih J-H, Hwang H-E, et al. Early prediction of 1-year tumor response of hepatocellular carcinoma with lipiodol deposition pattern through post-embolization cone-beam computed tomography during conventional transarterial chemoembolization. Eur Radiol. 2021;31:7464–7475. doi:10.1007/s00330-021-07843-8
21. Salem R, Padia SA, Toskich BB, et al. Radiation segmentectomy for early hepatocellular carcinoma is curative. J Hepatol. 2025;82:1125–1132. doi:10.1016/j.jhep.2025.01.005
22. Wang L, Ke Q, Lin N, Huang Q, Zeng Y, Liu J. The efficacy of transarterial chemoembolization combined with microwave ablation for unresectable hepatocellular carcinoma: a systematic review and meta-analysis. Int J Hyperthermia. 2019;36(1):1287–1295. doi:10.1080/02656736.2019.1692148
23. Zhang G, Ren Y, Liu J, et al. Transarterial chemoembolization plus radiofrequency ablation and Iodine-125 seed implantation for hepatocellular carcinoma in high-risk locations: a propensity score-matched analysis. J Hepatocell Carcinoma. 2025;12:15–27. doi:10.2147/JHC.S499763
24. Yao Y, Hongli Y, Lingyu Q, et al. Combined radiofrequency ablation or microwave ablation with transarterial chemoembolization can increase efficiency in intermediate-stage hepatocellular carcinoma without more complication: a systematic review and meta-analysis. Int J Hyperthermia. 2022;39:455–465. doi:10.1080/02656736.2022.2048095
25. Lee CH, You GR, Jo HG, et al. Albumin-Bilirubin grade as a valuable predictor of recurrence and prognosis in patients with hepatocellular carcinoma following radiofrequency ablation. Cancers. 2025;16.
26. Liuhaonan Z, Yixun T, Xiaoling H, et al. Combined impact of prognostic nutritional index, fibrinogen-to-albumin ratio, and neutrophil-to-lymphocyte ratio on surgical outcomes and prognosis in hepatocellular carcinoma. Am J Cancer Res. 2025;15:439–451. doi:10.62347/RTMF3105
27. Hu G-J, Zheng Q-Y, Tsai F-G, et al. Ablative margin assessment for recurrence prediction in patients with hepatocellular carcinoma receiving radiofrequency ablation. J Formos Med Assoc. 2025.
28. Ronit J, Pannaga M, Ashish M, et al. The combined use of lenvatinib and locoregional therapies for the management of hepatocellular carcinoma. Cancers. 2025;17.
29. Li L-Q, Su T-S, Wu Q-Y, et al. Therapeutic outcome of stereotactic body radiotherapy for small hepatocellular carcinoma lesions - a systematic review and network meta-analysis. Clin Oncol. 2023;35:652–664. doi:10.1016/j.clon.2023.07.002
30. Zhao J, Wu J, He M, et al. Comparison of transcatheter arterial chemoembolization combined with radiofrequency ablation or microwave ablation for the treatment of unresectable hepatocellular carcinoma: a systemic review and meta-analysis. Int J Hyperthermia. 2020;37:624–633. doi:10.1080/02656736.2020.1774667
31. Hao L, Thomas J, Vogl TJ, et al. A comparison of the efficacy and safety of US-, CT-, and MR-guided radiofrequency and microwave ablation for HCC: a systematic review and network meta-analysis. Cancers. 2025;17.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Transarterial Chemoebolization in Hepatocellular Carcinoma: A Binational Japanese-German Study
Auer TA, Sofue K, Ueshima E, Rauer N, Yamaguchi T, Gebauer B, Hamm B, Murakami T, Althoff CE
Journal of Hepatocellular Carcinoma 2022, 9:695-705
Published Date: 1 August 2022
PD-1 Inhibitors Combined with Antiangiogenic Therapy with or Without Transarterial Chemoembolization in the Treatment of Hepatocellular Carcinoma: A Propensity Matching Analysis
Li H, Su K, Guo L, Jiang Y, Xu K, Gu T, Chen J, Wu Z, Wang P, Zhang X, Yan Y, Li S, Wu X, Han L, He K, Wen L, Li B, Han Y
Journal of Hepatocellular Carcinoma 2023, 10:1257-1266
Published Date: 29 July 2023