Back to Journals » OncoTargets and Therapy » Volume 16
Systemic Treatment for Gynecological Cancer Patients Undergoing Hemodialysis
Received 20 May 2023
Accepted for publication 1 July 2023
Published 8 July 2023 Volume 2023:16 Pages 545—558
DOI https://doi.org/10.2147/OTT.S419445
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Gaetano Romano
Nan Zhang,1,2,* Chang Liu,1– 3,* Wen Di1,2,4
1Department of Obstetrics and Gynecology, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 2Shanghai Key Laboratory of Gynecologic Oncology, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 3Center for Reproductive Medicine, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 4State Key Laboratory of Systems Medicine for Cancer, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wen Di, Department of Obstetrics and Gynecology, Renji Hospital, School of Medicine, Shanghai Jiao Tong University, No. 160 Pujian Road, Shanghai, 200127, People’s Republic of China, Email [email protected]
Abstract: Gynecological cancer poses a serious threat to women’s health. Chemotherapy-based systemic therapy plays a crucial role in the treatment of gynecological cancers. Many systemic therapeutic drugs are metabolized in the kidneys. Therefore, normal renal function is a prerequisite for gynecological tumor patients to complete the full course of systematic treatment and provide a guarantee for achieving an ideal prognosis. Chronic kidney disease often places restrictions on systematic treatment to different extents, such as influencing drug pharmacokinetics, increasing drug toxicity, and the risk of adverse drug reactions. Unfortunately, women undergoing renal replacement have a higher risk of developing gynecological cancers. This article summarizes the current knowledge on systemic treatment drugs for patients with gynecological cancer undergoing dialysis. We discuss the optimal choice of the systematic therapeutic protocol, administration of form and dosage, and window of chemotherapy during hemodialysis sessions to ensure both effectiveness and safety in gynecological cancer patients.
Keywords: hemodialysis, renal insufficiency, systemic treatment, gynecological cancer
Introduction
Gynecological cancer is a common disease of the female reproductive system and is among the top 10 most common cancers in women with nearly 1.4 million new cases and 700,000 deaths worldwide in 2022.1 Gynecological cancer seriously threatens the health of women and places a massive burden on their families and the society. Gynecological cancer can be roughly classified into the following categories: cervical cancer, endometrial cancer, ovarian cancer, vulvar cancer, vaginal cancer, tubal cancer, and mixed Mullerian cancer, as well as gestational trophoblastic tumor, a special type associated with pregnancy. The outcome of gynecological cancer is strongly related to the stage of diagnosis.2
According to the International Society of Nephrology (ISN) 2019 Global Kidney Health Atlas (GKHA) cross-sectional survey of 160 participating countries, the average number of newly diagnosed end-stage renal disease (ESRD) cases worldwide was 144 individuals per million people.3 Renal replacement therapy (RRT), including hemodialysis (HD), peritoneal dialysis (PD), and kidney transplantation, has been widely used to treat patients with ESRD. HD is the most common form of dialysis in most countries.3 Worldwide, the number of patients receiving long-term HD is estimated to be more than one million, and the number of newly diagnosed cases is increasing annually.4 The significance of RRT has been demonstrated to be beneficial for prolonged survival, and prolongation of life span brings ESRD patients with a higher risk of gynecological cancer in the later life cycle.4,5
However, studies on the safety and efficacy of systematic therapy in HD patients with gynecological cancer are limited. Patients undergoing HD are often excluded from the clinical trials. There are no established guidelines for the administration of cytotoxic substances in the treatment of gynecological cancer in patients undergoing dialysis. The pharmacokinetics of chemotherapeutics in patients are not unclear. Reports on actual drug administration and outcomes are usually limited to case reports and series. More attention should be paid to the formulation of chemotherapy regimens for patients with gynecological cancer receiving long-term HD.
We conducted an exhaustive review of the literature and collected existing evidence to summarize the current knowledge of drugs used in patients with gynecological cancer undergoing hemodialysis. This review aimed to optimally choose the chemotherapeutic protocol and administer the drugs at a specific time in relation to the HD procedure in this specific group of patients to ensure the most effective and safe treatment of gynecological cancer, hoping to provide guidance for the clinical treatment of these patients.
This review was based on a literature search in PubMed (published before May 2023, using the following search terms: gynecological cancer, hemodialysis, chemotherapy, systemic treatment, etc.), concerning descriptions of the cases of HD patients with gynecological malignant tumors, including data on the pharmacokinetics of chemotherapeutic agents in cancers other than gynecological malignant tumors, and comprised information given in the summary of product characteristics.
General Considerations
Gynecological cancer patients usually receive comprehensive treatment such as surgery, chemotherapy, radiotherapy, and targeted therapy. Chemotherapy plays a pivotal role in the treatment of gynecological cancers, especially in patients with advanced and recurrent cancers. With the development of precision medicine, targeted therapy has changed the traditional treatment mode of gynecological cancer and has gradually shown superiority over the traditional treatment mode, occupying an important position in the treatment of gynecological cancer.
Patients receiving HD often have multiple complications, are usually frailer than the general population, and are extremely disadvantaged in the context of chemotherapy. HD usually does not limit the possibility of surgical and radiotherapy treatment but has a significant impact on the pharmacokinetics of cytotoxic agents and targeted drugs used in oncological therapy. In addition to patient-specific characteristics, chemotherapy for HD patients requires special considerations concerning dose adjustments and timing of drug administration in relation to HD sessions.
First, in terms of drug characteristics, many drugs are predominantly eliminated by the kidneys; therefore, the standard dose may cause overdose and toxicity in HD patients. Second, the dialyzability of drugs must be considered, which means that some drugs can be removed by HD. Factors affecting drug dialyzability include molecular weight, protein binding, volume of distribution, and affinity to red blood cells. Drugs with a smaller molecular mass, low protein binding, low volume of distribution, and low affinity for red blood cells are easily removed through dialysis.6 Chemotherapy should be administered after HD if drugs are eliminated. Third, partial drug removal by HD may be purposefully performed to improve the tolerance of patients, remove remnants of the drug, and reduce side effects of the drug; sometimes, additional HD is needed depending on the patient’s condition.5 Fourth, the characteristics of drug metabolites need to be considered. If the parent drug is rapidly degraded to nontoxic metabolites, HD may not be an obstacle for the administration of such drugs.7 Finally, considering the complexity of dialysis factors involving drugs and their metabolites, it is necessary to combine actual pharmacokinetic studies in HD patients, which are relatively lacking at present.
Important HD-related factors include the duration of HD sessions (more drug is dialyzed with longer sessions), surface area, and dialyzer membrane thickness. Synthetic high-permeability membranes used in modern HD technologies can remove large molecules with molecular masses greater than 1500 Da. Owing to advances in HD technology, it is important to keep in mind that some older reports of drug dose reductions in HD patients may be outdated and inaccurate in current practice.6,8
Chemotherapy
Chemotherapy is indispensable for the comprehensive treatment of malignant gynecological tumors, especially in advanced and recurrent diseases. Platinum-based combination chemotherapy is the basic chemotherapy regimen for most malignant gynecological tumors. A summary of all the chemotherapeutics discussed in this review is listed in Table 1.
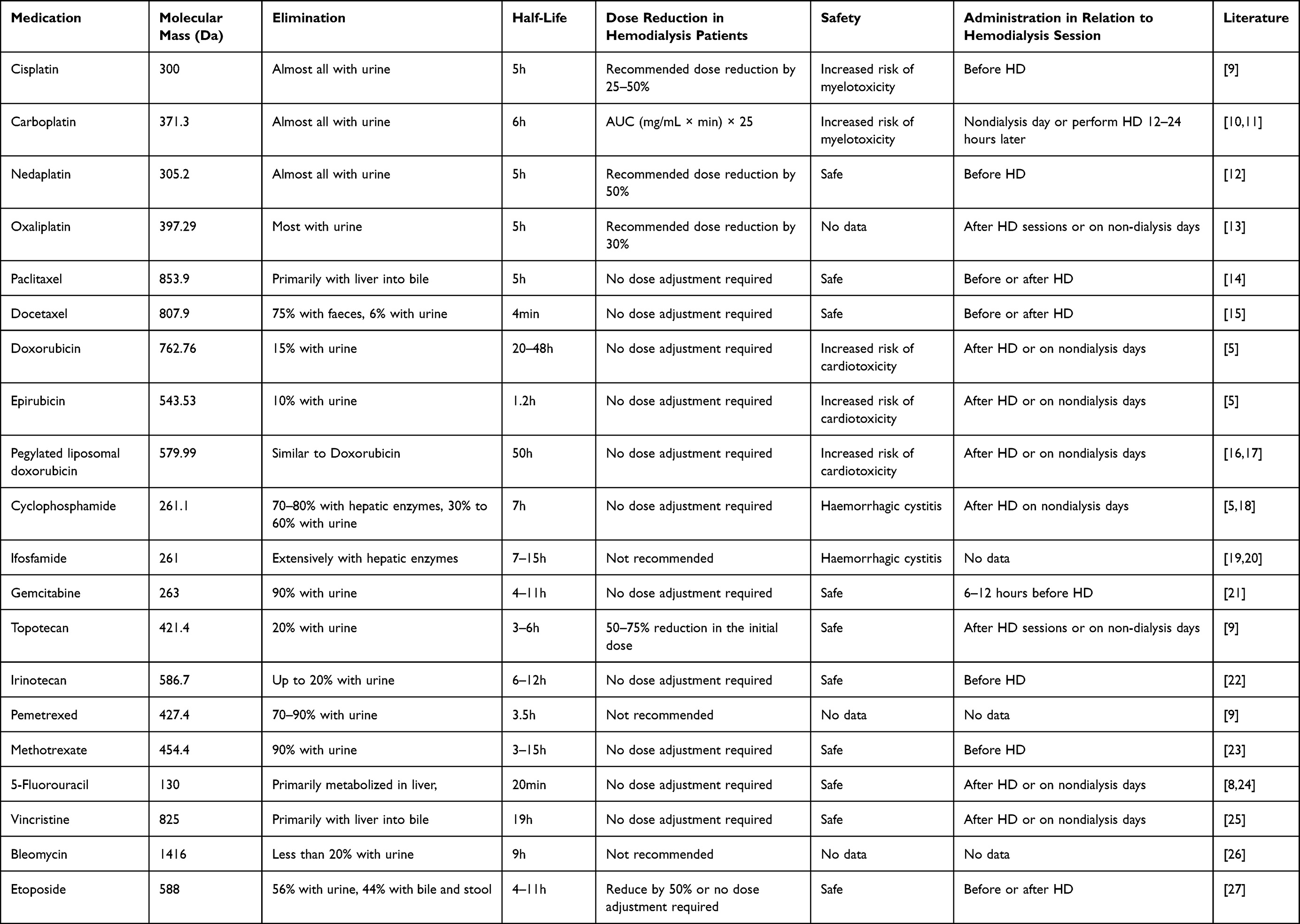 |
Table 1 Summary of the Chemotherapeutics for Gynecological Malignant Tumors in Hemodialysis Patients |
Cisplatin
Cisplatin (MM: 300 Da) is a first-generation platinum agent that is mainly eliminated through the kidney and excreted in the urine as an unchanged drug (15–75%).28 Currently, cisplatin is the most effective chemotherapeutic agent for the treatment of cervical cancer. In patients undergoing hemodialysis, the pharmacokinetic parameters of cisplatin were within the range observed in patients with normal renal function, which showed the effectiveness of hemodialysis in removing platinum. Hemodialysis was effective in removing free cisplatin and did not affect already bound cisplatin. Cisplatin (30–60 mg/m2) as a single agent or a combination regimen has been safely used in patients with gynecological cancer. A 49-year-old woman on dialysis with advanced uterine cervical cancer was administered cisplatin at a dose of 30 mg via drip infusion. The results showed that the total cisplatin clearance did not differ between dialysis patients and patients without renal impairment.29
A 66-year-old woman with metastatic ovarian cancer undergoing HD received seven cycles of chemotherapy with 60 mg/m2 cisplatin and 600 mg/m2 cyclophosphamide, and complete remission occurred after five treatment cycles.30
A 51-year-old woman with recurrent stage IIC serous papillary ovarian adenocarcinoma underwent hemodialysis and received 150 mg/m2 paclitaxel and 30 mg/m2 cisplatin. Hemodialysis was initiated 30 min after the completion of cisplatin infusion and was performed for 5 h. This combination chemotherapy was repeated twice with the same schedule at 26 days interval, and both the tolerance and reactivity were good.31 Combined with reports of other diseases, doses of cisplatin at 50–80 mg/m2 were well tolerated when starting the HD session within 30 min post-infusion.32 And, 25–50% was recommended for HD patients.
Carboplatin
Carboplatin (MM: 371.3 Da) is a second-generation, less nephrotoxic platinum analog. Unlike most other chemotherapeutics, in which body surface area (BSA) is used to calculate dosage, the Calvert formula is widely accepted for determining carboplatin dosing. In clinical practice, an acceptable way to prescribe carboplatin to HD patients is to plan its administration after an HD session. Considering that the GFR was equal to 0 mL/min after HD and that the extrarenal clearance was 25 mL/min, carboplatin dose (mg/body) = AUC (mg/mL × min) × 25,10 which is consistent with the recommended dose of the AIOM (Italian Association of Medical Oncology) guidelines.5 The majority of carboplatin becomes protein bound within 24 h, and 55–70% of the drug is excreted by the kidneys in the first 24 h.33 A 52-year-old patient with stage IVA epithelial ovarian cancer requiring HD received combination chemotherapy consisting of 150 mg/m2 paclitaxel and 100 mg carboplatin (the dose of the administered carboplatin was calculated according to the Calvert formula). HD was initiated 24 h after carboplatin administration. These results prove that determining the dose of carboplatin according to the Calvert formula and initiating HD after 24 h would ensure a favorable therapeutic effect with limited side effects.34 A 73-year-old Japanese woman with stage IC3 fallopian tube cancer underwent hemodialysis three times a week for 3 years and received 135 mg/m2 (total of 210 mg) paclitaxel for 3 h and 125 mg carboplatin (calculated according to the Calvert formula) for 1 h. The time interval between the end of carboplatin administration and hemodialysis initiation was 1 h in the first cycle, 16 h in the second cycle, and 20 h in the third cycle, and only mild side effects were observed in the third cycle. Therefore, hemodialysis was initiated 20 hours after the completion of carboplatin infusion in cycles 4–6. The planned total chemotherapy regimen was completed without any severe adverse events.11 Since carboplatin can be removed by HD, HD should be performed within 12–24 h after carboplatin infusion, when carboplatin has become bound to proteins and is not dialyzable.
Nedaplatin
Nedaplatin (MM;305.2 Da) is a third-generation platinum compound that causes DNA damage in cells via the induction of oxidative stress. It is characterized by fewer toxic side effects and no nephrotoxicity. Nedaplatin is excreted mainly through the urine. A 77-year-old woman on hemodialysis (HD) with advanced esophageal squamous cell carcinoma (ESCC) was treated with nedaplatin (45 mg/m2) and 5-fluorouracil (560 mg/m2) before initiating HD. Pharmacokinetic studies have suggested that a 50% dose of nedaplatin in HD patients is effective in obtaining pharmacokinetic data similar to those in patients with normal renal function.12 HD was performed following nedaplatin infusion.
Oxaliplatin
Oxaliplatin (MM;397.29 Da) is a third-generation platinum-based compound. Renal excretion is the primary route for platinum elimination. One HD patient with liver metastasis from colon cancer received a hepatic arterial infusion of oxaliplatin at a dose of 60 mg twice a week during HD sessions, and there were no side effects after three cycles.35 Four patients with colon cancer undergoing HD received oxaliplatin at doses ranging from 40 to 85 mg/m2. It is considered safe to perform therapy in patients by reducing doses and providing dialysis.13,36 As more than 80% of oxaliplatin can be removed by dialysis, administration of the drug might be best performed after HD sessions or on non-dialysis days. Owing to the lack of convincing data, oxaliplatin is not recommended for HD patients. However, when mandatory, this might indicate a 30% dose reduction in patients on HD.
Paclitaxel
Paclitaxel (MM: 853.9 Da) is extensively metabolized by hepatic cytochrome P450 and excreted mainly in the bile, with less than 10% excreted by the kidneys. A series of pharmacokinetic studies have shown that paclitaxel pharmacokinetics in HD patients were comparable to those in patients with normal renal function. In one case, paclitaxel was administered at a dose of 175 mg/m2 via intravenous infusion over 24h on the day without dialysis, and tolerance to treatment was acceptable.37 In another case, paclitaxel was administered at a dose of 150 mg/m2 for 3h followed by a 30 min infusion of carboplatin on a nondialysis day in a 40-year-old patient on HD with FIGO stage III ovarian cancer; the efficacy and tolerance were good.38 Therefore, because paclitaxel is not dialyzable, patients undergoing HD can receive a full-dose paclitaxel and may be used before or after HD sessions.14
Docetaxel
Docetaxel (MM: 807.9 Da) is a semisynthetic analog of paclitaxel that is metabolized in the liver by cytochrome P450 and excreted into the bile. Only 6% of the administered elimi dose remained unchanged in the urine, and the majority of docetaxel elimi was nated via fecal excretion.39 Docetaxel is also not dialyzable, which allows it to be infused before or after HD without dose adjustment, with good safety.15
Anthracyclines
Doxorubicin (MM: 762.76 Da) and epirubicin (MM: 543.53 Da) are first- and second-generation anthracycline anticancer drugs, respectively. Doxorubicin and epirubicin are metabolized mostly by the liver and, to a lesser degree, are excreted by the kidneys (15% and 10%, respectively). The pharmacokinetics of doxorubicin in HD patients are approximately 1.5 to 3 times higher than those in patients with normal kidney function. Since doxorubicin can be removed by HD, these drugs should be administered after HD or on nondialysis days.8,33 Doxorubicin must be used with caution in patients undergoing hemodialysis; however, dose reduction is not recommended. Pegylated liposomal doxorubicin (MM: 579.99 Da), a formulation of doxorubicin in poly(ethylene glycol)-coated liposome, is a second-generation pegylated liposomal doxorubicin that is comprised of distearoyl phosphatidylcholine. It has a significantly longer drug half-life (50 hours) and unique toxicity profile. Pegylated liposomal doxorubicin, in combination with carboplatin, is indicated for the first-line treatment of Uterine sarcoma and platinum sensitive recurrent ovarian cancer. In pegylated liposomal doxorubicin-treated cancer patients, the renal excretion of doxorubicin and its metabolites has a pattern similar to that reported for free doxorubicin. Only 5.5% of a single dose of pegylated liposomal doxorubicin is recovered in the urine as doxorubicin, doxorubicin or other metabolites during the 72h after injection. However, a significant reduction of total body clearance of pegylated liposomal doxorubicin was found in HD patients. A 36-year-old woman with advanced cervical cancer and ESRD due to SLE was administrated one dose of 60 mg pegylated liposomal doxorubicin i.v. Thirteen days after the chemotherapy, the patient developed high fever occurred and several erythematous to violaceous atrophic plaques, followed by generalized skin rash. Caution should be exercised to the use of pegylated liposomal doxorubicin for HD patients, and dose reduction is recommended.16,17,40,41
Cyclophosphamide
Cyclophosphamide (MM: 261.1 Da) is an alkylating agent with cytotoxic and immune suppressive effects. Approximately 70–80% of the administered cyclophosphamide dose is metabolized by hepatic enzymes, and 30–60% is eliminated by the kidneys.42 A standard dose of cyclophosphamide was safely used in anephric child undergoing dialysis, with cyclophosphamide clearance and toxicity profiles similar to those in patients with normal renal function. Cyclophosphamide should be administered after HD or on nondialysis days because it can be removed by HD.18 A 48-year-old female patient with breast cancer received 75 mg/m2 docetaxel and 600 mg/m2 cyclophosphamide postoperatively and performed hemodialysis 48h after chemotherapy. The results showed that chemotherapy with standardized dosages of cyclophosphamide was safe and effective in hemodialysis patients,43 which suggested that dose reduction may not be necessary for patients scheduled to undergo hemodialysis after cyclophosphamide infusion.
Ifosfamide
Ifosfamide (MM: 261 Da) is a parenterally administered alkylating agent similar to cyclophosphamide. Ifosfamide is mainly converted to its active metabolite by liver enzymes and excreted in the urine as an inactive metabolite.42 One case report showed that the pharmacokinetics of the parent ifosfamide did not substantially change in a patient receiving hemodialysis after ifosfamide infusion. Hemodialysis is effective in eliminating ifosfamide and some of its metabolites as well as improving ifosfamide-related neurotoxicity.19 However, the use of ifosfamide in patients was controversial, and definite recommendations cannot be made.20 Mesna (MM: 164.18Da) is a sulfhydryl compound that is used to reduce the incidence of hemorrhagic cystitis associated with certain chemotherapeutic agents. Mesna is converted to a free thiol compound in the kidney, where it binds to and inactivates acrolein and other urotoxic metabolites of ifosfamide and cyclophosphamide, thereby reducing their toxic effects on the urinary tract during urinary excretion. It can be concluded that Mesna can be dialyzed by comparing the level of Mesna in the fluid after dialysis with the level of plasma before and after dialysis. Since data on the use of ifosfamide in patients on dialysis are limited and controversial to support a clear-cut recommendation. If ifosfamide was used in patients on dialysis, Mesna should be used on non-HD days or after the HD session.44
Gemcitabine
Gemcitabine (MM, 263 Da) is a broad-spectrum antimetabolite and deoxycytidine analog with antineoplastic activity. Gemcitabine is excreted mainly through the kidneys, and the protein binding capacity of gemcitabine is less than 10%. A 64-year-old patient with pancreatic cancer received two cycles of gemcitabine at a standard dose of 1000 mg/m2 administered on days 1 and 10 and regular 3.5h hemodialysis treatment was performed 24h after each infusion. The results showed that gemcitabine treatment in patients with end-stage renal disease and intermittent standard hemodialysis was safe and well-tolerated. It is recommended that dose adjustment of gemcitabine is unnecessary, and dialysis should be started 6–12 h after gemcitabine infusion to remove the potential side effects of the metabolite of gemcitabine.21
Topotecan
Topotecan (MM: 421.4Da) binds with DNA and topoisomerase I, thus interrupting DNA replication. There are both IV and oral formulations. The IV drug is excreted by the kidneys with 51% excreted in urine, whereas only 20% of the oral formulation is excreted in urine. Topotecan has a terminal half-life of 3–6 hours following oral administration and 2–3 hours following IV administration of the drug. IV topotecan is dialyzable. One case reported one ovarian cancer patient with ESRD observed a 60% reduction of topotecan administered on nondialysis days and saw a fourfold increase in clearance while on HD and systemic clearance similar to that for patients with normal renal function. It is believed that the reduction in the initial dose of topotecan by 50–75% is recommended for ESRD patients on non-HD days or after the HD session.9
Irinotecan
Irinotecan (MM: 586.7 Da) is an antineoplastic enzyme inhibitor, which prevents relegation of the DNA strand by binding to topoisomerase I-DNA complex, preventing DNA from properly replicating and repairing itself, and causes double-strand DNA breakage and cell death. The half-life of irinotecan is about 6–12 hours. Nearly 80% of irinotecan’s elimination is done without the kidneys. After infusion, irinotecan is metabolized in serum and other tissues, like the liver and small intestine. The literature research revealed severe toxicity of irinotecan applied 24 hours before HD, even in reduced dosages, only a small fraction of up to 24% of irinotecan can be removed by using HD. Thus, usually recommend performing the HD after application of chemotherapy to mimic normal renal function.22
Pemetrexed
Pemetrexed (MM: 427.4Da) is a Folate Analog Metabolic Inhibitor. It impairs cell division by inhibiting thymidylate synthase, dihydrofolate reductase, and glycinamide ribonucleotide formyl transferase. Approximately 70–90% of unchanged pemetrexed is cleared through the urine. The elimination half-life of pemetrexed is 3.5 hours in patients with normal renal function. It can be concluded that pemetrexed cannot be dialyzed by comparing the level of pemetrexed in the fluid after dialysis with the level of plasma before and after dialysis. Pemetrexed should not be considered for patients without adequate renal function.9
Methotrexate
Methotrexate (MTX) (MM 454.4 Da) is an antimetabolite and antifolate agent with antineoplastic and immunosuppressive activities. Methotrexate is eliminated primarily by the kidneys, and its excretion depends mainly on the dose and route of administration. Approximately 90% of MTX metabolism is excreted in the urine. HD has limited effectiveness in reducing plasma MTX because the plasma protein-binding rate of MTX is relatively high, and the volume distribution is large. A 52-year-old woman with post-transplant lymphoproliferative disorder was managed with 1g/m2 MTX for 2h infusion followed by five daily 4–9h HD sessions commencing 1h following completion of MTX infusion. Hemodialysis is effective in clearing and delivering a high dose of MTX to achieve complete remission with limited and reversible toxicity.45 A 41-year-old man was initially managed with the same dose of MTX, and a total of four cycles were completed with an escalating methotrexate dose to 3g/m2 accompanied by high-flux and extended-hours hemodialysis, which showed the safety of using an escalating dosing regimen of MTX in patients with ESRD on HD.23 High-dose MTX followed by daily HD sessions could be a more rational strategy than dose reduction, when MTX is necessary for cancer treatment.
5-Fluorouracil
5-Fluorouracil (MM; 130 Da) is an antimetabolite fluoropyrimidine analog of nucleoside pyrimidine with antineoplastic activity. The administered dose of 5-fluorouracil is primarily metabolized in the liver and only 4% of fluorouracil is excreted in the urine. Since 5-fluorouracil may be removed by dialysis, it is believed that typical doses of 5-fluorouracil may be given to ESRD patients after the HD session or on nondialysis days.8,24
Vincristine
Vincristine (MM: 825 Da) is a vinca alkaloid. The local uptake or destruction of vincristine is rapid and is primarily excreted by the liver into the bile. Because of the rapid intracellular absorption of vincristine, dialysis is generally ineffective in clearing them.46 A 4-year-old boy with renal-limited primary diffuse large B-cell lymphoma received CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone) regimen chemotherapy while on hemodialysis and achieved remission at last.47 A 65-year-old man diagnosed with testicular cancer undergoing hemodialysis received two cycles of R-CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone, and rituximab) chemotherapy after hemodialysis, which was eventually discontinued owing to interstitial pneumonia. There is no need to reduce the injection volume of vincristine in hemodialysis patients, and it can be administered after HD sessions or on nondialysis days.25
Bleomycin
Bleomycin (MM: 1416 Da) is a complex of glycopeptide antibiotics from Streptomyces verticillus, consisting of bleomycin A2 and B2, which can inhibit DNA metabolism with antineoplastic activity. Bleomycin is rapidly absorbed into cells. Less than 20% of the urine is excreted by patients with moderately severe renal failure. Owing to rapid intracellular incorporation, dialysis is generally ineffective for the removal of bleomycin. According to the literature, bleomycin was administered as part of multi-agent chemotherapy for patients, and it is difficult to assess the extent to which bleomycin contributes to these adverse events.20,26
Etoposide
Etoposide (MM: 588 Da) acts by binding and inhibiting topoisomerase II and its function in ligating cleaved DNA molecules, resulting in the inhibition of DNA replication and transcription and possessing potent antineoplastic properties. Moreover, 56% of the drug is excreted in urine, and the remaining 44% is excreted in bile and stool.48 One study evaluated three patients with small cells lung cancer undergoing HD who received 50% dose reduction of the etoposide and took HD 1 hour after etoposide infusion. The plasma concentrations of etoposide were comparable to those of patients with normal renal function.9 A 30-year-old patient on HD with poor risk metastatic non-seminomatous germ cell tumor received five cycles of full dose of cisplatin and 60% dose of etoposide on days 1–5, every 21 days and strategically timed with HD. Some studies have indicated that standard-dose chemotherapy with etoposide is feasible and effective in patients undergoing hemodialysis.49 Etoposide dose reductions are still pertinent since a small amount of the drug is excreted via the urine and a prolonged half-life can be seen. On the basis of studies conducted in HD patients, the etoposide dose should be reduced by 50% and administered at a dose of 25–75 mg/m2/day.8 Since etoposide is not removed by HD, it can be administered before or after HD sessions.27
Targeted Therapy
A summary of all the targeted therapeutics discussed in this review is listed in Table 2.
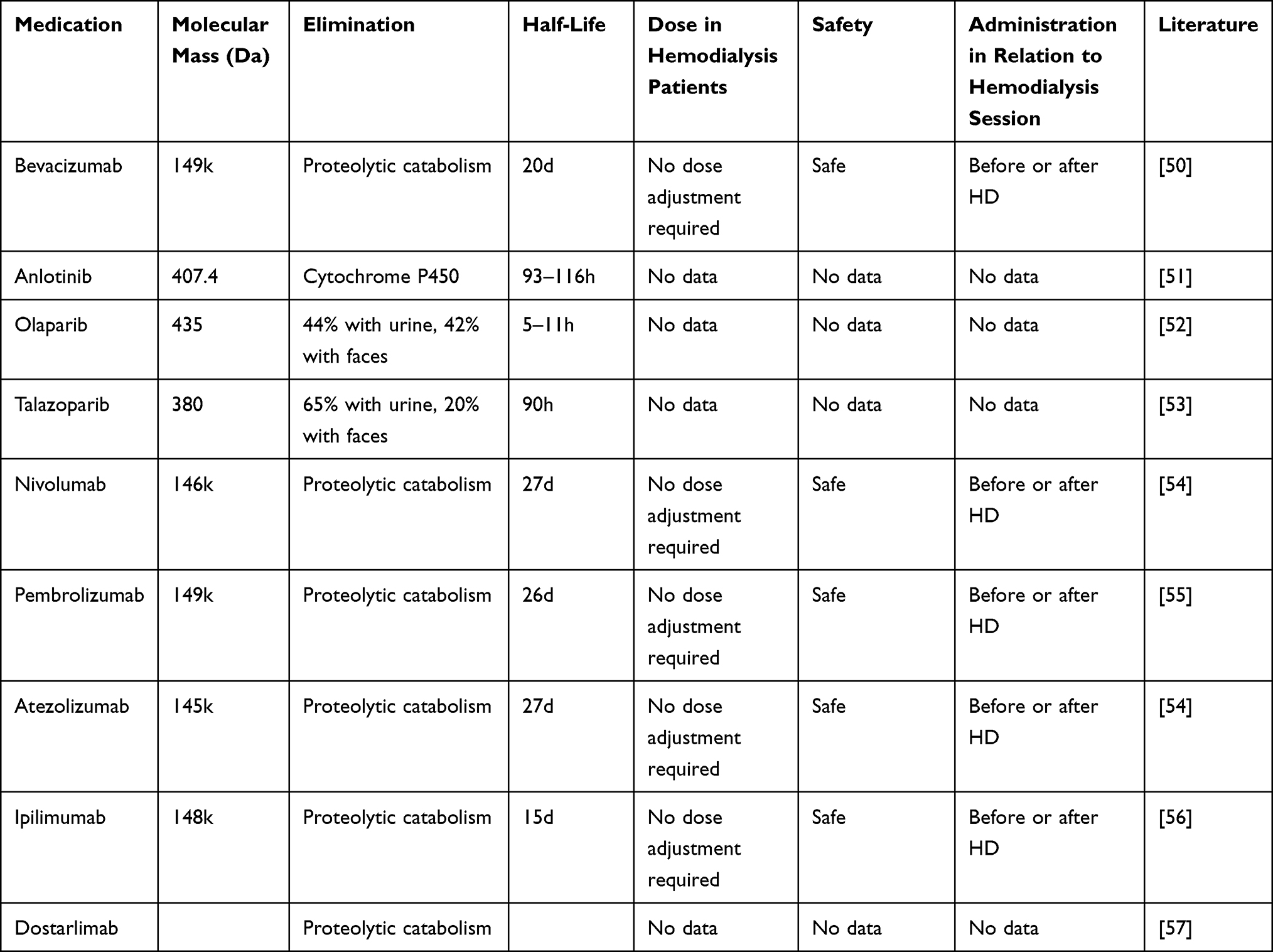 |
Table 2 Summary of the Targeted Therapeutics and Immunotherapeutic for Gynecological Malignant Tumors in Hemodialysis Patients |
Bevacizumab
Bevacizumab (MM: 149kDa) is a recombinant humanized monoclonal antibody against vascular endothelial growth factor (VEGF). The main elimination pathway of bevacizumab is proteolytic catabolism throughout the body rather than hepatic metabolism or renal excretion.58 Bevacizumab was administered at a dose of 5 mg/kg every 2 weeks for 6 months to a 23-year-old patient with metastatic renal cell carcinoma, and the patient had his disease was controlled. The pharmacokinetic parameters of bevacizumab in hemodialysis patients are similar to those reported in patients with normal renal function.59 Four patients on hemodialysis with stage IV colorectal cancer received a regular dose of bevacizumab plus a daily dose of UFT chemotherapy without serious side effects during therapy.50 Due to its large molecular mass, bevacizumab is not dialyzable and can be administered without dose reduction and performed before or after the HD session.
Anlotinib
Anlotinib (MM: 407.4 Da) is a new type of small-molecule multi-target tyrosine kinase inhibitor with potential antineoplastic and anti-angiogenic activities. Oxidation mediated by cytochrome P450 is the major anlotinib elimination pathway. A 63-year-old man on hemodialysis for small cell lung cancer was successfully treated with six cycles of concomitant oral etoposide and local radiotherapy, followed by prophylactic cranial irradiation plus anlotinib.51 No clear data are available on the dosage and safety of anlotinib in patients undergoing dialysis.
Poly ADP-Ribose Polymerase Inhibitors (PARPi)
PARP inhibitors (PARPi) are a type of anticancer treatment that prevents cancer cells from repairing DNA damage, especially those with breast cancer susceptibility gene (BRCA) variants. PARPi is currently the most important drug in maintenance therapy for ovarian cancer patients with a homologous recombination deficiency (HRD)-positive status, defined by either a BRCA1/2 mutation and/or genomic instability. PARPi maintenance treatment after chemotherapy may significantly improve PFS in women with newly diagnosed recurrent platinum-sensitive EOC.
Olaparib
Olaparib (MM: 435 Da) was strongly bound to proteins, mainly eliminated as metabolites, with 44% found in the urine and 42% in feces. In patients with mild renal impairment (creatinine clearance, 60–89 mL/min), there was no need to adjust the olaparib dose. In patients with moderate renal impairment (creatinine clearance of 30–59 mL/min), the tablet dose should be adjusted from 300 to 200 mg twice daily. Olaparib is not recommended for patients with severe renal impairment or end-stage renal disease, as its safety and pharmacokinetics have not been studied in these patients.52
Talazoparib
Talazoparib (MM: 380 Da) is metabolized via monooxidation, dehydrogenation, cysteine conjugation of a monodesfluoro metabolite, and glucuronide conjugation. Approximately 64.7% of talazoparib is excreted in the urine and 19.7% is eliminated in the feces. The mean terminal plasma half-life of Talazoparib capsules is 90 h with a standard deviation of 58 h. Talazoparib can be administered in patients with mild renal impairment (creatinine clearance 51–80 mL/min) with no dose adjustment. For patients with moderate renal impairment (creatinine clearance 31–50 mL/min), the recommended Talazoparib dose should be adjusted to 200 mg twice daily. Talazoparib is not recommended for use in patients with severe renal impairment or end-stage renal disease (creatinine clearance ≤30 mL/min), as safety and pharmacokinetics have not been studied in these patients, unless the benefit outweighs the potential risk, and the patient should be carefully monitored for renal function and adverse events.53
Immunotherapy
Immunotherapy has revolutionized the cancer treatment paradigm by harnessing the patient’s immune system to target the evading cancer cells. Immunotherapy plays an increasingly important role in cervical cancer, because most patients with cervical cancer are positive for PD-L1. The NCCN guidelines recommend PD-1 blockers plus chemotherapy as the preferred systemic treatment for advanced, metastatic, and recurrent cervical cancer. The antibodies are slowly cleared from circulation, mainly through catabolism. In general, serum immunoglobulin levels in hemodialysis patients are not altered. Considering their large molecular weights, immune checkpoint inhibitors (ICIs) are not eliminated by hemodialysis and no dose adjustments are needed.54 A summary of all the immunotherapeutics discussed in this review is listed in Table 2.
Nivolumab
Nivolumab (MM: 146 kDa) is a fully human immunoglobulin G4 (IgG4) mAb that selectively inhibits programmed cell death protein 1 (PD-1) activity by binding to the PD-1 receptor to block the ligands PD-L1 and PD-L2. A 65-year-old male with unclassified RCC received 100 mg nivolumab every 3 weeks for 12 weeks and underwent HD three times a week. A 64-year-old female with clear cell RCC received Nivolumab 3 3 mg/kg every 3 weeks for 12 weeks and underwent HD three times a week. Nivolumab was effective and well tolerated in the dialysis-dependent cancer patients.54,60 Nivolumab treatment maybe not contraindicated in hemodialysis-dependent patients.
Pembrolizumab
Pembrolizumab (MM: 149kDa) is a selective humanized IgG4-κ monoclonal antibody that inhibits the PD-1 receptor and blocks the PD-1 pathway, which plays a pivotal role in immune checkpoint regulation in the tumor microenvironment. A 63-year-old male with metastatic melanoma was treated with 10 cycles of 2 mg/kg pembrolizumab every 3 weeks while undergoing dialysis three times a week and reported complete remission.55
Atezolizumab
Atezolizumab (MM: 145 kDa) is a fully humanized monoclonal antibody immune checkpoint inhibitor that binds PD-L1 to selectively prevent the interaction between PD-1 and B7-1 (CD80) receptors. A 68-year-old male with urothelial carcinoma received two cycles of 1200 mg atezolizumab every 3 weeks and underwent HD three times a week, although eventually died of tumor progression and septic shock.54
Ipilimumab
Ipilimumab (MM: 148 kDa) is a monoclonal antibody that binds to CTLA-4, blocks the binding of CTLA-4 to its ligand (CD80/CD86), and increases the activation and proliferation of T cells. One report described two patients with ESRD undergoing hemodialysis who were safely treated with ipilimumab 3 mg/kg. These two cases demonstrate that ipilimumab can be administered safely and elicit clinical benefits in patients with ESRD undergoing hemodialysis.56
Dostarlimab
Dostarlimab is a humanized IgG4 monoclonal antibody targeting PD-1 that exerts an antitumor effect by blocking the binding of PD-1 with PD-L1 and PD-L2. Dostarlimab is approved by the FDA for use in adult patients with dMMR, relapsed, or advanced solid tumors that have progressed during or after prior therapy and do not have satisfactory alternative treatment options.57 In September 2021, the NCCN recommended guidelines for uterine and ovarian cancers.57 New guidelines continue to recommend the use of dotalizumab under certain circumstances in patients with platinum-sensitive and platinum-resistant recurrent ovarian cancer with MSI-H or dMMR. The pharmacokinetic parameters of dostarlimab were similar to those of the other anti-PD-1 antibodies. There is no available literature could be referred regarding the adjustment of dose or experience of using Dostarlimab for cancer patients undergoing dialysis.57
Hormone Therapy
Aromatase inhibitors (anastrozole, letrozole, and exemestane) can be used to treat low-grade serous ovarian and endometrioid cancers. A summary of all the endocrine therapeutics discussed in this review is listed in Table 3.
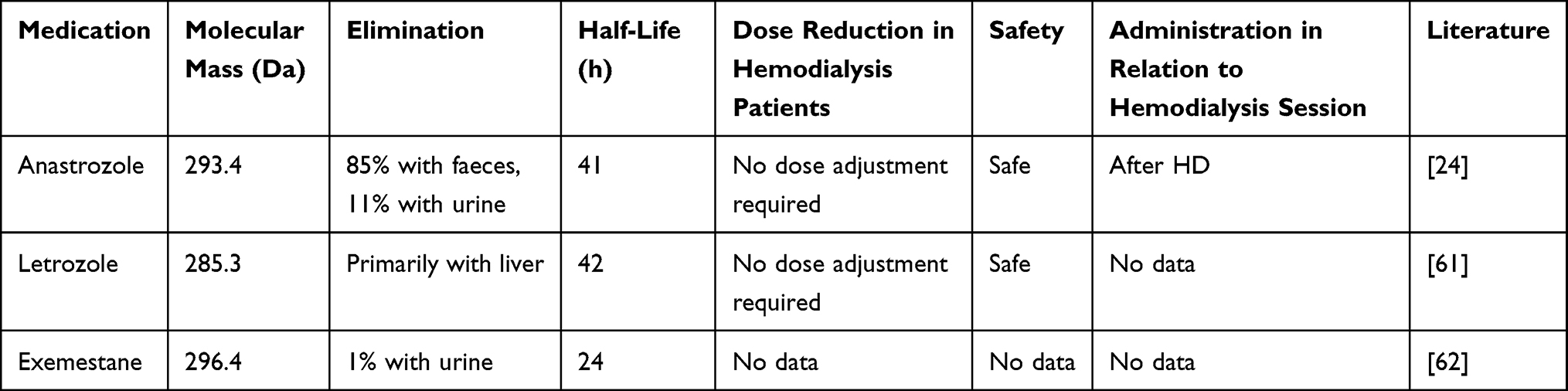 |
Table 3 Summary of the Endocrine Therapeutics for Gynecological Malignant Tumors in Hemodialysis Patients |
Anastrozole
Anastrozole (MM 293.4 Da) is a nonsteroidal aromatase inhibitor that effectively blocks estrogen synthesis. Anastrozole is rapidly absorbed and 40% of the drug is bound to plasma proteins. Hepatic metabolism accounts for approximately 85% of the anastrozole elimination. Approximately 10% of the administered dose was eliminated from the urine. Renal impairment has a negligible effect on the total drug clearance, as the renal route is a relatively minor clearance pathway for anastrozole. Serum anastrozole concentrations in HD patients are similar to those in patients with normal renal function, and the drug itself is well tolerated, which indicated that in patients with CKD/ESKD, anastrozole may be used in the same dose as in patients with normal kidney function. Owing to its low MM and moderate affinity with plasma proteins, the drug should be taken after the HD session.24
Letrozole
Letrozole (MM: 285.3 Da), a third-generation aromatase inhibitor, is a nonsteroidal inhibitor of estrogen synthesis with antineoplastic activity. Letrozole is converted into a pharmacologically inactive carbinol metabolite in the liver, followed by renal excretion of the glucuronide conjugate of this metabolite. The half-life of letrozole is 42h and there is no need to reduce the dose administered to older women. One patient was diagnosed with HER2-positive estrogen receptor-positive liver metastasis from breast cancer and received hemodialysis, and letrozole plus lapatinib without dose reduction was well tolerated.61
Exemestane
Exemestane (MM: 296.4 Da) is an irreversible steroidal aromatase inhibitor with anti-estrogen and antineoplastic activities. Exemestane binds strongly to proteins (90%) and is inactivated in the liver. Only 1% of the administered dose is excreted in urine. The mean terminal half-life of exemestane is 24 h. In patients with creatinine clearance of <30 mL/min, serum concentrations were twice as high as those in healthy volunteers. No dosage or safety data were available for the patients on renal replacement therapy. However, owing to the lack of data on pharmacokinetics and safety in dialysis patients, this drug should be used with caution only when other therapeutic options are not available.62
Conclusion
Systematic treatment in patients undergoing HD faces enormous challenges. Although those patients may have incomplete renal function and multiple medications, many drugs used in the treatment of gynecological malignant tumors can be safely administered. The selection of drugs, dose adjustments, and timing of HD with regard to the administration of chemotherapy, endocrine, targeted, and immunotherapy agents must be carefully planned, to match the distinct pharmacological traits of individual drugs and different patient’s condition. HD technology is constantly evolving, and information from previous literatures of drug administration in HD patients may not be valid in the current clinical practice. Constant updating and accumulation of experience with actual drug administration and outcomes of patients undergoing HD in real world are necessary.
Funding
This work was funded by the Natural Science Research Project of Jiading District, Shanghai (grant number JDKW-2022-0036) and the National Natural Science Foundation of China (grant number 82201846, 81974454).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Berghuis AY, Pijnenborg JFA, Boltje TJ, Pijnenborg JMA. Sialic acids in gynecological cancer development and progression: impact on diagnosis and treatment. Int J Cancer. 2022;150(4):678–687. doi:10.1002/ijc.33866
3. Thurlow JS, Joshi M, Yan G, et al. Global epidemiology of end-stage kidney disease and disparities in kidney replacement therapy. Am J Nephrol. 2021;52(2):98–107. doi:10.1159/000514550
4. Calice-Silva V, Hussein R, Yousif D, et al. Associations between global population health indicators and dialysis variables in the Monitoring Dialysis Outcomes (MONDO) consortium. Blood Purif. 2015;39(1–3):125–136. doi:10.1159/000368980
5. Pedrazzoli P, Silvestris N, Santoro A, et al. Management of patients with end-stage renal disease undergoing chemotherapy: recommendations of the Associazione Italiana di Oncologia Medica (AIOM) and the Societa Italiana di Nefrologia (SIN). ESMO Open. 2017;2(3):e000167. doi:10.1136/esmoopen-2017-000167
6. Gotta V, Dao K, Rodieux F, Buclin T, Livio F, Pfister M. Guidance to develop individual dose recommendations for patients on chronic hemodialysis. Expert Rev Clin Pharmacol. 2017;10(7):737–752. doi:10.1080/17512433.2017.1323632
7. Tomita M, Aoki Y, Tanaka K. Effect of haemodialysis on the pharmacokinetics of antineoplastic drugs. Clin Pharmacokinet. 2004;43(8):515–527. doi:10.2165/00003088-200443080-00002
8. Janus N, Thariat J, Boulanger H, Deray G, Launay-Vacher V. Proposal for dosage adjustment and timing of chemotherapy in hemodialyzed patients. Ann Oncol. 2010;21(7):1395–1403. doi:10.1093/annonc/mdp598
9. Leung TV, Hughes ME, Cambareri CG, Rubin DJ, Eaby-Sandy B. Systemic treatments for lung cancer patients receiving hemodialysis. J Adv Pract Oncol. 2018;9(6):614–629. doi:10.1111/j.1525-1438.2007.01048.x
10. Li YF, Fu S, Hu W, et al. Systemic anticancer therapy in gynecological cancer patients with renal dysfunction. Int J Gynecol Cancer. 2007;17(4):739–763. doi:10.1111/j.1525-1438.2007.00847.x
11. Wada T, Fukuda T, Kawanishi M, et al. Pharmacokinetic analyses of carboplatin in a patient with cancer of the fallopian tubes undergoing hemodialysis: a case report. Biomed Rep. 2016;5(2):199–202. doi:10.3892/br.2016.714
12. Matsuo N, Maruta M, Tsuruyama M, et al. 維持血液透析中の進行性食道がん患者にネダプラチンで化学療法を行った1症例 [A case of advanced esophageal cancer treated with nedaplatin in a patient undergoing maintenance hemodialysis]. Yakugaku Zasshi. 2020;140(3):449–453. Japanese. doi:10.1248/yakushi.19-00227
13. Gori S, Lunardi G, Inno A, et al. Pharmacokinetics of oxaliplatin in a hemodialyzed patient: chemotherapy dose adjustment and timing of dialysis. Clin Colorectal Cancer. 2014;13(4):260–263. doi:10.1016/j.clcc.2014.09.003
14. Woo MH, Gregornik D, Shearer PD, Meyer WH, Relling MV. Pharmacokinetics of paclitaxel in an anephric patient. Cancer Chemother Pharmacol. 1999;43(1):92–96. doi:10.1007/s002800050868
15. Hochegger K, Lhotta K, Mayer G, Czejka M, Hilbe W. Pharmacokinetic analysis of docetaxel during haemodialysis in a patient with locally advanced non-small cell lung cancer. Nephrol Dial Transplant. 2007;22(1):289–290. doi:10.1093/ndt/gfl498
16. Abraham SA, Waterhouse DN, Mayer LD, Cullis PR, Madden TD, Bally MB. The liposomal formulation of doxorubicin. Methods Enzymol. 2005;391:71–97. doi:10.1016/s0076-6879(05)91004-5
17. Fulton MD, Najahi-Missaoui W. Liposomes in cancer therapy: how did we start and where are we now. Int J Mol Sci. 2023;24(7):6615. doi:10.3390/ijms24076615
18. Haubitz M, Bohnenstengel F, Brunkhorst R, Schwab M, Hofmann U, Busse D. Cyclophosphamide pharmacokinetics and dose requirements in patients with renal insufficiency. Kidney Int. 2002;61(4):1495–1501. doi:10.1046/j.1523-1755.2002.00279.x
19. Carlson L, Goren MP, Bush DA, et al. Toxicity, pharmacokinetics, and in vitro hemodialysis clearance of ifosfamide and metabolites in an anephric pediatric patient with Wilms’ tumor. Cancer Chemother Pharmacol. 1998;41(2):140–146. doi:10.1007/s002800050720
20. Yasuda H, Yasuda M, Komatsu N. Chemotherapy for non-Hodgkin lymphoma in the hemodialysis patient: a comprehensive review. Cancer Sci. 2021;112(7):2607–2624. doi:10.1111/cas.14933
21. Kiani A, Kohne CH, Franz T, et al. Pharmacokinetics of gemcitabine in a patient with end-stage renal disease: effective clearance of its main metabolite by standard hemodialysis treatment. Cancer Chemother Pharmacol. 2003;51(3):266–270. doi:10.1007/s00280-003-0574-3
22. Hann A, Nosalski E, Hermann PC, Egger J, Seufferlein T, Keller F. Chemotherapeutic agents eligible for prior dosing in pancreatic cancer patients requiring hemodialysis: a systematic review. Clin Nephrol. 2018;90(2):125–141. doi:10.5414/cn109327
23. Yeung J, Vaughan E, Chadban S, Saunders J, Thiagarajah N, Brown C. High-dose intravenous methotrexate with high-flux, extended-hours haemodialysis in treatment of primary central nervous system, post-transplant lymphoproliferative disorder and end-stage kidney disease: a case report. Nephrology. 2018;23(11):1063–1064. doi:10.1111/nep.13254
24. Langenegger T, Wahl P, Schiesser D, Thurlimann B. Plasma levels of tamoxifen, N-desmethyl tamoxifen and anastrozole in a patient with metastatic breast cancer and chronic hemodialysis. Breast Cancer Res Treat. 2006;100(2):177–181. doi:10.1007/s10549-006-9243-7
25. Nakatsuji H, Sakaki M, Hamao T. 血液透析患者に発症した精巣悪性リンパ腫の1例 [Primary testicular malignant lymphoma in a hemodialysis patient: a case report]. Hinyokika Kiyo. 2015;61(2):67–70. Japanese.
26. Kimakura M, Abe T, Nagahara A, et al. Metastatic testicular cancer presenting with liver and kidney dysfunction treated with modified BEP chemotherapy combined with continuous hemodiafiltration and rasburicase. Anticancer Drugs. 2016;27(4):364–368. doi:10.1097/CAD.0000000000000334
27. Moore KJ, Snow S, Wood LA. Delivering chemotherapy to a metastatic poor risk testicular cancer patient on hemodialysis. Curr Oncol. 2022;29(3):1808–1812. doi:10.3390/curroncol29030148
28. Belt RJ, Himmelstein KJ, Patton TF, Bannister SJ, Sternson LA, Repta AJ. Pharmacokinetics of non-protein-bound platinum species following administration of cis-dichlorodiammineplatinum(II). Cancer Treat Rep. 1979;63(9–10):1515–1521.
29. Tanabe N, Goto M, Morita H, et al. Pharmacokinetics of cis-diammine-dichlor-platin in a hemodialysis patient. Cancer Invest. 1991;9(6):629–635. doi:10.3109/07357909109039874
30. Sturn W, Sanwald R, Ehninger G. Pharmakokinetik von Cisplatin bei chronischer Hämodialyse-Behandlung [Pharmacokinetics of cisplatin in long-term hemodialysis treatment]. Dtsch Med Wochenschr. 1989;114(9):337–339. German. doi:10.1055/s-2008-1066599
31. Tomita M, Kurata H, Aoki Y, Tanaka K, Kazama JJ. Pharmacokinetics of paclitaxel and cisplatin in a hemodialysis patient with recurrent ovarian cancer. Anticancer Drugs. 2001;12(5):485–487. doi:10.1097/00001813-200106000-00010
32. Watanabe R, Takiguchi Y, Moriya T, et al. Feasibility of combination chemotherapy with cisplatin and etoposide for haemodialysis patients with lung cancer. Br J Cancer. 2003;88(1):25–30. doi:10.1038/sj.bjc.6600687
33. Bednarek A, Mykala-Ciesla J, Pogoda K, et al. Limitations of systemic oncological therapy in breast cancer patients with chronic kidney disease. J Oncol. 2020;2020:7267083. doi:10.1155/2020/7267083
34. Kodama J, Sasaki A, Masahiro S, et al. Pharmacokinetics of combination chemotherapy with paclitaxel and carboplatin in a patient with advanced epithelial ovarian cancer undergoing hemodialysis. Oncol Lett. 2010;1(3):511–513. doi:10.3892/ol_00000090
35. Matoba S, Sawada T, Toda S, et al. 透析患者でのmFOLFOX6 の使用経験 [Modified FOLFOX6 in a patient on hemodialysis with metastatic colorectal cancer]. Gan To Kagaku Ryoho. 2008;35(4):673–675. Japanese.
36. Ohnishi T, Kanoh T, Shiozaki K, et al. 慢性腎不全を有する大腸癌症例に対する血液透析併用FOLFOX 4療法の1例 [FOLFOX 4 in a patient with metastatic colorectal cancer on hemodialysis due to chronic renal failure]. Gan To Kagaku Ryoho. 2007;34(8):1299–1302. Japanese.
37. Mori M, Takeda E, Sakai K, et al. 腎機能低下患者に発症した非小細胞肺癌に対しCarboplatin+Weekly Paclitaxelが著効した1例 [A case of non-small cell lung carcinoma successfully treated with carboplatin and weekly paclitaxel under renal dysfunction]. Gan To Kagaku Ryoho. 2004;31(12):2061–2064. Japanese.
38. Watanabe M, Aoki Y, Tomita M, et al. Paclitaxel and carboplatin combination chemotherapy in a hemodialysis patient with advanced ovarian cancer. Gynecol Oncol. 2002;84(2):335–338. doi:10.1006/gyno.2001.6527
39. Mencoboni M, Olivieri R, Vannozzi MO, Schettini G, Viazzi F, Ghio R. Docetaxel pharmacokinetics with pre- and post-dialysis administration in a hemodyalized patient. Chemotherapy. 2006;52(3):147–150. doi:10.1159/000092903
40. Armstrong DK, Alvarez RD, Backes FJ, et al. NCCN guidelines® insights: ovarian cancer, version 3.2022. J Natl Compr Canc Netw. 2022;20(9):972–980. doi:10.6004/jnccn.2022.0047
41. Green AE, Rose PG. Pegylated liposomal doxorubicin in ovarian cancer. Int J Nanomedicine. 2006;1(3):229–239.
42. de Jonge ME, Huitema AD, Rodenhuis S, Beijnen JH. Clinical pharmacokinetics of cyclophosphamide. Clin Pharmacokinet. 2005;44(11):1135–1164. doi:10.2165/00003088-200544110-00003
43. Yang L, Zhang XC, Yu SF, et al. Pharmacokinetics and safety of cyclophosphamide and docetaxel in a hemodialysis patient with early stage breast cancer: a case report. BMC Cancer. 2015;15:917. doi:10.1186/s12885-015-1932-3
44. Urquhart BL, Freeman DJ, Spence JD, House AA. The effect of mesna on plasma total homocysteine concentration in hemodialysis patients. Am J Kidney Dis. 2007;49(1):109–117. doi:10.1053/j.ajkd.2006.10.002
45. Mutsando H, Fahim M, Gill DS, et al. High dose methotrexate and extended hours high-flux hemodialysis for the treatment of primary central nervous system lymphoma in a patient with end stage renal disease. Am J Blood Res. 2012;2(1):66–70.
46. Olson KRE. Poisoning & Drug Overdose. In: Lange Medical Books.
47. South AM. Primary renal diffuse large B-Cell lymphoma causing haemodialysis-dependent nephromegaly in a child. BMJ Case Rep. 2018;2018. doi:10.1136/bcr-2018-226328
48. Squibb BM. Etopophos (etoposide phosphate) package insert. Available from: https://packageinserts.bms.com/pi/pi_etopophos.pdf.
49. Haraguchi N, Satoh H, Ogawa R, Hashimoto Y, Sekizawa K. Chemotherapy in a patient with small-cell lung cancer undergoing haemodialysis. Clin Oncol. 2005;17(8):663. doi:10.1016/j.clon.2005.05.003
50. Takayama T, Haga I, Nakamura A, Asami K. 血液透析患者のStage Ⅳ大腸癌に対しBevacizumab+UFT 療法が有効であった4 例 [Bevacizumab plus UFT regimen for four patients with stage colorectal cancer receiving hemodialysis]. Gan To Kagaku Ryoho. 2020;47(7):1117–1119. Japanese.
51. Gao F, Cong X, Liu Z. Successful treatment of a patient with small cell lung cancer receiving hemodialysis, with concurrent oral etoposide and radiotherapy: a case report. Medicine. 2020;99(40):e22637. doi:10.1097/MD.0000000000022637
52. Rolfo C, de Vos-Geelen J, Isambert N, et al. Pharmacokinetics and safety of olaparib in patients with advanced solid tumours and renal impairment. Clin Pharmacokinet. 2019;58(9):1165–1174. doi:10.1007/s40262-019-00754-4
53. National Center for Biotechnology Information. PubChem Compound Summary for CID 135565082, Talazoparib. Available from: https://pubchem.ncbi.nlm.nih.gov/compound/Talazoparib.
54. Cheun H, Kim M, Lee H, Oh KH, Keam B. Safety and efficacy of immune checkpoint inhibitors for end-stage renal disease patients undergoing dialysis: a retrospective case series and literature review. Invest New Drugs. 2019;37(3):579–583. doi:10.1007/s10637-018-0673-y
55. Chang R, Shirai K. Safety and efficacy of pembrolizumab in a patient with advanced melanoma on haemodialysis. BMJ Case Rep. 2016;2016. doi:10.1136/bcr-2016-216426
56. Cavalcante L, Amin A, Lutzky J. Ipilimumab was safe and effective in two patients with metastatic melanoma and end-stage renal disease. Cancer Manag Res. 2015;7:47–50. doi:10.2147/CMAR.S73389
57. Gettman L. New drug update: dostarlimab, loncastuximab tesirine, and aducanumab. Sr Care Pharm. 2022;37(1):9–16. doi:10.4140/TCP.n.2022.9
58. Panoilia E, Schindler E, Samantas E, et al. A pharmacokinetic binding model for bevacizumab and VEGF165 in colorectal cancer patients. Cancer Chemother Pharmacol. 2015;75(4):791–803. doi:10.1007/s00280-015-2701-3
59. Garnier-Viougeat N, Rixe O, Paintaud G, et al. Pharmacokinetics of bevacizumab in haemodialysis. Nephrol Dial Transplant. 2007;22(3):975. doi:10.1093/ndt/gfl664
60. Vitale MG, Baldessari C, Milella M, et al. Immunotherapy in dialysis-dependent cancer patients: our experience in patients with metastatic renal cell carcinoma and a review of the literature. Clin Genitourin Cancer. 2019;17(5):e903–e908. doi:10.1016/j.clgc.2019.06.009
61. Piacentini F, Omarini C, Barbieri E. Lapatinib and renal impairment: a case report. Tumori. 2013;99(3):e134–5. doi:10.1700/1334.14823
62. National Center for Biotechnology Information. PubChem Compound Summary for CID 3385, Fluorouracil. Available from: https://pubchem.ncbi.nlm.nih.gov/compound/3385#section=Absorption-Distribution-and-Excretion.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.