Back to Journals » Cancer Management and Research » Volume 18

Systemic Inflammation Response Index, Albumin, and Hemoglobin-Albumin-Lymphocyte-Platelet Score for Stage-Stratified Esophageal Cancer Discrimination: A Retrospective Case-Control Study
Authors Li Y, Cui Y, Liu M, Zhang J, Liu Y
Received 15 April 2026
Accepted for publication 29 June 2026
Published 8 July 2026 Volume 2026:18 614276
DOI https://doi.org/10.2147/CMAR.S614276
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sanjeev K. Srivastava
Yadan Li,1,* Yanfang Cui,1,* Minmin Liu,2,* Jianfang Zhang,3 Yongshuo Liu4
1Department of Clinical Laboratory, Shandong Medical and Pharmaceutical University Hospital, Binzhou, Shandong, 256603, People’s Republic of China; 2Jinan D.A Medical Laboratory Center Co., Ltd, Jinan, Shandong, 250014, People’s Republic of China; 3Binzhou Center for Disease Control and Prevention, Binzhou, Shandong, 256603, People’s Republic of China; 4Department of Clinical Laboratory, Shandong Cancer Hospital and Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Jinan, Shandong, 250117, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yongshuo Liu, Email [email protected]
Introduction: Inflammation- and nutrition-associated biomarkers have received increasing interest in esophageal cancer research. Nevertheless, the diagnostic value of the systemic inflammation response index (SIRI), albumin (ALB), and hemoglobin-albumin-lymphocyte-platelet (HALP) score across different pathological stages has not yet been fully clarified. We evaluated the performance of SIRI, ALB, and HALP, alone and in combination, for the auxiliary discrimination of esophageal cancer (EC), and examined their associations with clinicopathological characteristics in stage-stratified analyses.
Methods: This retrospective study enrolled 168 esophageal cancer patients and 117 healthy controls (HC). SIRI and HALP were calculated preoperatively from routine hematological parameters. Cancer cases were divided into stage I/II (n = 32) and stage III/IV (n = 136) groups. ROC curve analysis evaluated the discriminatory efficacy of SIRI, ALB, HALP, and their combined model. The combined model was constructed using binary logistic regression incorporating SIRI, ALB, and HALP, and its discriminatory performance was evaluated by ROC analysis. Multivariable logistic regression adjusted for age and sex was performed, and bootstrap internal validation (1000 resamples) assessed model optimism.
Results: Compared with healthy controls, patients with esophageal cancer exhibited significantly increased SIRI levels and significantly decreased ALB and HALP levels. The combined model achieved an AUC of 0.803 for distinguishing stage III/IV disease from healthy controls and 0.746 for stage I/II disease. SIRI was significantly associated with T stage and N stage. ALB with tumor length and T stage. HALP with smoking history and T stage. After adjustment for age and sex, HALP retained significance mainly in the all-cancer and stage III/IV analyses.
Conclusion: SIRI, ALB, and HALP were associated with the occurrence and stage of esophageal cancer. Their combined model demonstrated improved discriminatory performance over single markers, particularly in stage III/IV disease, and retained additional value after adjustment for age and sex. These biomarkers may serve as convenient exploratory indicators for auxiliary assessment of esophageal cancer.
Keywords: esophageal cancer, systemic inflammation response index, albumin, HALP score, ROC analysis
Introduction
Esophageal cancer is the sixth leading cause of cancer-related death worldwide and the eighth most common cancer.1 Global cancer statistics showed that there were approximately 510,000 new cases of esophageal cancer and 450,000 deaths in 2022, with a particularly heavy burden of incidence and mortality in East Asia and other regions.2 Because early-stage esophageal cancer is often difficult to detect rapidly in clinical practice, symptoms such as dysphagia, foreign body sensation during swallowing, and obstruction usually occur late in the natural history of the disease, resulting in delayed diagnosis. Many patients are already at a locally advanced or progressive stage at the time of diagnosis, leading to an unsatisfactory overall prognosis.3 Therefore, identifying economical and reproducible biomarkers for the auxiliary detection and stratified assessment of esophageal cancer is of important clinical significance.
An increasing body of evidence suggests that the systemic inflammatory response and nutritional status of cancer patients are closely associated with tumor initiation and progression, rather than being determined solely by the biological behavior of tumor cells themselves.4,5 Because peripheral blood-based inflammatory and nutritional indicators are easily obtainable, low cost, and highly reproducible, they have attracted growing attention in recent years. The systemic inflammation response index (SIRI), which is derived from neutrophil, monocyte, and lymphocyte counts, reflects the balance between pro-tumor inflammatory responses and anti-tumor immune status.6,7 The HALP score, calculated from hemoglobin, albumin, lymphocyte, and platelet levels, integrates information on nutritional status, immune status, and inflammatory response.8 As a classic nutrition- and inflammation-related marker, albumin (ALB) is also of particular interest, and hypoalbuminemia is regarded as a signal of systemic inflammation and malnutrition in patients with cancer.9
In the field of esophageal cancer, previous studies have suggested that SIRI, HALP, and albumin-based indicators may have certain clinical value. However, the existing evidence has mainly focused on prognostic assessment, such as postoperative survival, cancer-specific survival, and the prediction of early mortality risk. For example, elevated SIRI has been associated with shorter survival in patients with esophageal cancer and is also accompanied by more advanced tumor stage, T3-T4 stage, and lymph node metastasis.10 The HALP score has been reported as a factor for predicting tumor prognosis in patients with esophageal cancer after radical resection,11 and HALP has also been identified as an independent prognostic factor in patients with unresectable esophageal squamous cell carcinoma (ESCC).12 In addition, previous studies have shown that the preoperative NLR-Alb index may be used for individualized prognostic prediction in patients with ESCC.13 However, the role of these indicators in the auxiliary diagnosis of esophageal cancer, particularly their stage-specific discriminatory value, remains unclear. However, compared with their prognostic applications, less is known about whether these routinely available inflammation- and nutrition-related biomarkers can assist in distinguishing patients with esophageal cancer from healthy individuals, especially across different pathological stages.
In this study, we compared the levels of SIRI, ALB, and HALP between patients with esophageal cancer and healthy controls to evaluate the diagnostic value of these indicators and their combined model for esophageal cancer. We further performed stage-stratified analyses to assess their discriminatory ability in early-stage (stage I/II) and advanced-stage (stage III/IV) esophageal cancer. In addition, we explored the associations of SIRI, ALB, and HALP with clinicopathological characteristics, with the aim of providing additional evidence for the auxiliary evaluation of esophageal cancer.
Methods
Patients
This retrospective study enrolled 168 patients with esophageal cancer who were diagnosed and underwent surgical treatment at the Cancer Hospital of Shandong First Medical University between 2019 and 2023, along with 117 healthy controls. Healthy controls were selected from individuals who underwent routine health examinations during the same period. Individuals with evidence of acute infection, chronic inflammatory disease, autoimmune disease, hematological disease, or malignancy were excluded according to available medical records and laboratory findings. Routine endoscopy was not performed for all healthy controls. This study was approved by the Ethics Committee of the Cancer Hospital of Shandong First Medical University (approval no. SDTHEC [202604011]). All patients were histologically diagnosed by endoscopic biopsy and further confirmed by postoperative pathological examination. Tumor classification was determined according to the postoperative pathological TNM stage based on the 8th edition of the American Joint Committee on Cancer (AJCC) staging system.14 Among the cancer cases, 32 patients were classified into the pathological stage I/II group and 136 into the pathological stage III/IV group.
The inclusion criteria were as follows: (1) histologically confirmed esophageal cancer by endoscopic biopsy with postoperative pathological confirmation; (2) no preoperative radiotherapy, chemotherapy, or immunotherapy; (3) complete data on the most recent preoperative routine hematological and biochemical parameters. The exclusion criteria were as follows: (1) severe preoperative infection, autoimmune disease, or cardiovascular disease; (2) use of antiplatelet agents or statins within 3 months before blood collection; (3) anti-inflammatory therapy and blood transfusion within 1 month before blood collection; (4) concomitant hematological disease; (5) a history of other systemic malignancies within the previous 5 years.
Laboratory Variables
Routine hematological and biochemical parameters were collected, including white blood cell count (WBC), lymphocyte count, neutrophil count, monocyte count, platelet count, hemoglobin (HB), and albumin (ALB). SIRI was defined as neutrophil count × monocyte count / lymphocyte count. HALP was defined as hemoglobin × albumin × lymphocyte count / platelet count.
Statistical Analysis
Data analysis was performed using R software. Continuous variables were tested for normality. Normally distributed variables were expressed as mean ± standard deviation (SD) and compared using the independent samples t test or one-way analysis of variance (ANOVA), as appropriate. Non-normally distributed variables were presented as median (interquartile range) [M (Q1, Q3)] and compared using the Mann–Whitney test.
Receiver operating characteristic (ROC) curve analysis was performed to evaluate the discriminatory performance of SIRI, ALB, HALP, and their combined models. To identify the optimal combination of inflammation- and nutrition-related biomarkers, several candidate models were constructed, including SIRI combined with ALB and HALP, as well as alternative models in which ALB was replaced by neutrophil, monocyte, or lymphocyte counts (SIRI + NEUT + HALP, SIRI + MON + HALP, and SIRI + LYMPH + HALP). The area under the curve (AUC) and corresponding 95% confidence intervals (CIs) were calculated. The optimal cut-off values were determined using the Youden index (defined as sensitivity + specificity − 1). The combined models were constructed using binary logistic regression.
For three-group comparisons of SIRI, ALB, and HALP among healthy controls, pathological stage I/II, and pathological stage III/IV groups, pairwise Wilcoxon rank-sum tests with Bonferroni correction were performed. For the clinicopathological association analysis, dichotomization of SIRI, ALB, and HALP was based on the optimal cut-off values derived from the ROC analysis of all cancer cases versus healthy controls, and their associations with tumor length, tumor location, smoking history, T stage, and N stage were analyzed using the chi-square test or Fisher’s exact test. Because only one patient was classified as M1, M stage was not included in the formal clinicopathological association analysis.
Because marked differences in age and sex distribution were observed between cancer cases and healthy controls, additional multivariable logistic regression analyses adjusted for age and sex were performed for all esophageal cancer cases vs. healthy controls, pathological stage III/IV vs. healthy controls, and pathological stage I/II vs. healthy controls. Odds ratios (ORs) with 95% confidence intervals were calculated for each variable in the adjusted models. ROC analyses based on model-predicted probabilities were then used to assess the incremental discriminatory value of SIRI, ALB, HALP, and their combination beyond age and sex. To further evaluate model stability, bootstrap internal validation with 1000 resamples was performed for the fully adjusted models, and optimism-corrected AUCs were calculated. To further reduce potential confounding from the age and sex imbalance between patients with esophageal cancer and healthy controls, propensity score matching was performed using age and sex as matching variables. The discriminatory performance of SIRI, ALB, HALP, and their combined model was then re-evaluated in the matched cohort by ROC analysis. Decision curve analysis (DCA) was performed to explore clinical utility by comparing three models: a clinical model including age and sex, a biomarker model including SIRI, ALB, and HALP, and a full model including all five variables. Net benefit was assessed across different threshold probabilities and compared with treat-all and treat-none strategies. All statistical tests were two-sided, and P < 0.05 was considered statistically significant.
Results
Comparison of Baseline Characteristics and Laboratory Indicators Between the Two Groups
To establish the clinical and biological context for the subsequent analyses, we first compared the baseline demographic characteristics and laboratory indicators between the esophageal cancer group and the healthy control group. Table 1 summarizes the baseline demographic characteristics and laboratory indicators of the esophageal cancer group and the healthy control group. Compared with the healthy control group, patients with esophageal cancer were older and had a higher proportion of males, with both differences being statistically significant. Analysis of laboratory parameters showed that patients with esophageal cancer had significantly higher white blood cell counts, neutrophil counts, monocyte counts, and SIRI levels, whereas lymphocyte counts, ALB levels, and HALP values were significantly lower than those in healthy controls (all P < 0.05). Overall, these findings indicate that esophageal cancer is associated with a systemic profile characterized by inflammatory activation and impaired nutritional status, thereby providing the basis for further evaluating the diagnostic performance of SIRI, ALB, and HALP.
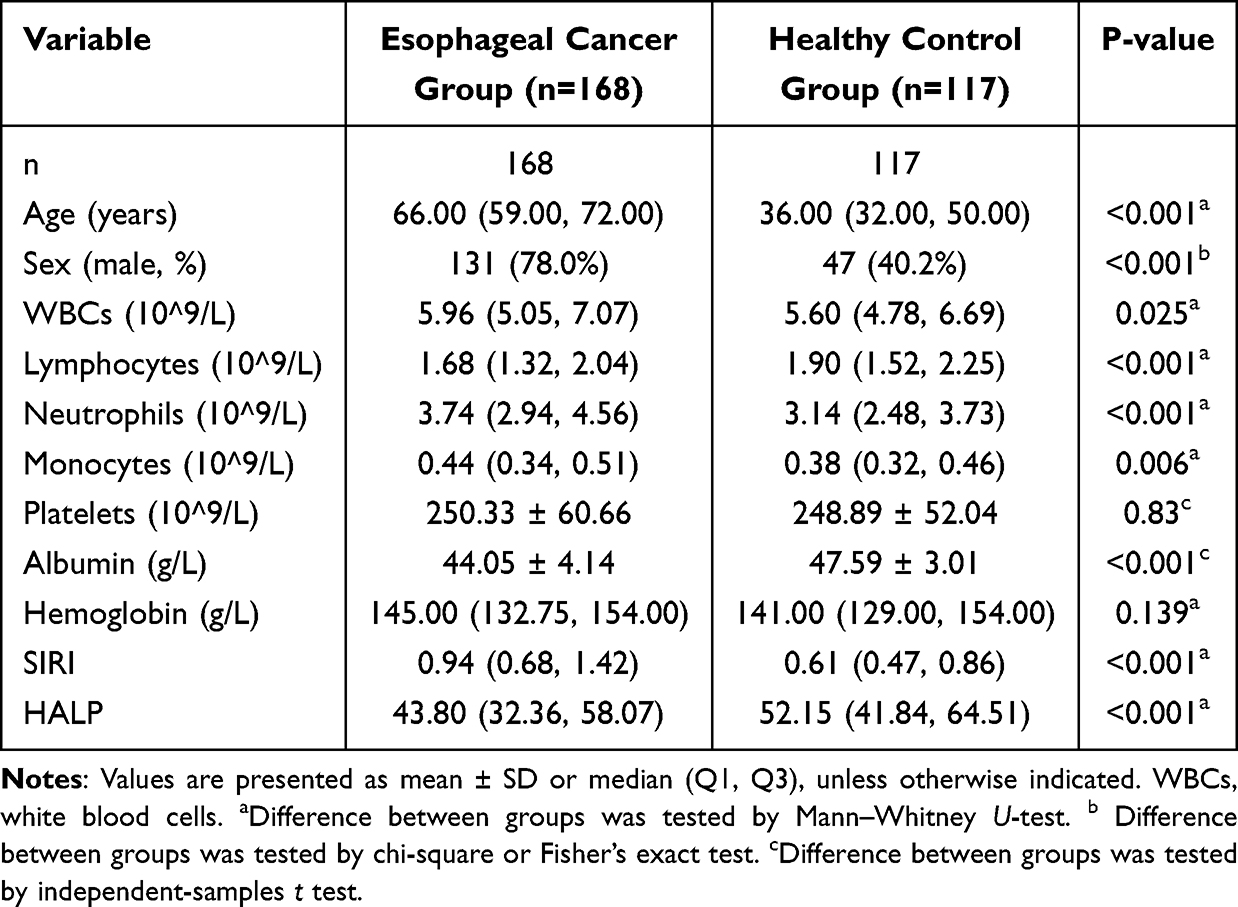 |
Table 1 Baseline Demographic Characteristics and Laboratory Parameters of Patients with Esophageal Cancer and Healthy Controls |
Diagnostic Performance of SIRI, ALB, and HALP, Alone and in Combination, for Esophageal Cancer
Building on the observed differences between patients with esophageal cancer and healthy controls, we next assessed the diagnostic performance of SIRI, ALB, and HALP, both individually and in combination. We compared the discrimination performance of multiple candidate models and selected the optimal combined model for evaluating biomarkers (Supplementary Figure S1). In the comparison between patients with pathological stage III/IV disease and healthy controls, the optimal cut-off values for SIRI, ALB, and HALP were 0.70, 44.35, and 47.68, respectively. As shown in Table 2 and Figure 1A, ALB demonstrated the best diagnostic performance among the individual indicators, with an area under the curve (AUC) of 0.767 (95% CI: 0.709–0.825), which was higher than that of SIRI [AUC = 0.732, 95% CI: 0.670–0.795] and HALP [AUC = 0.665, 95% CI: 0.599–0.732]. The combined model incorporating SIRI, ALB, and HALP showed the best overall diagnostic performance, with an AUC of 0.803 (95% CI: 0.750–0.857).
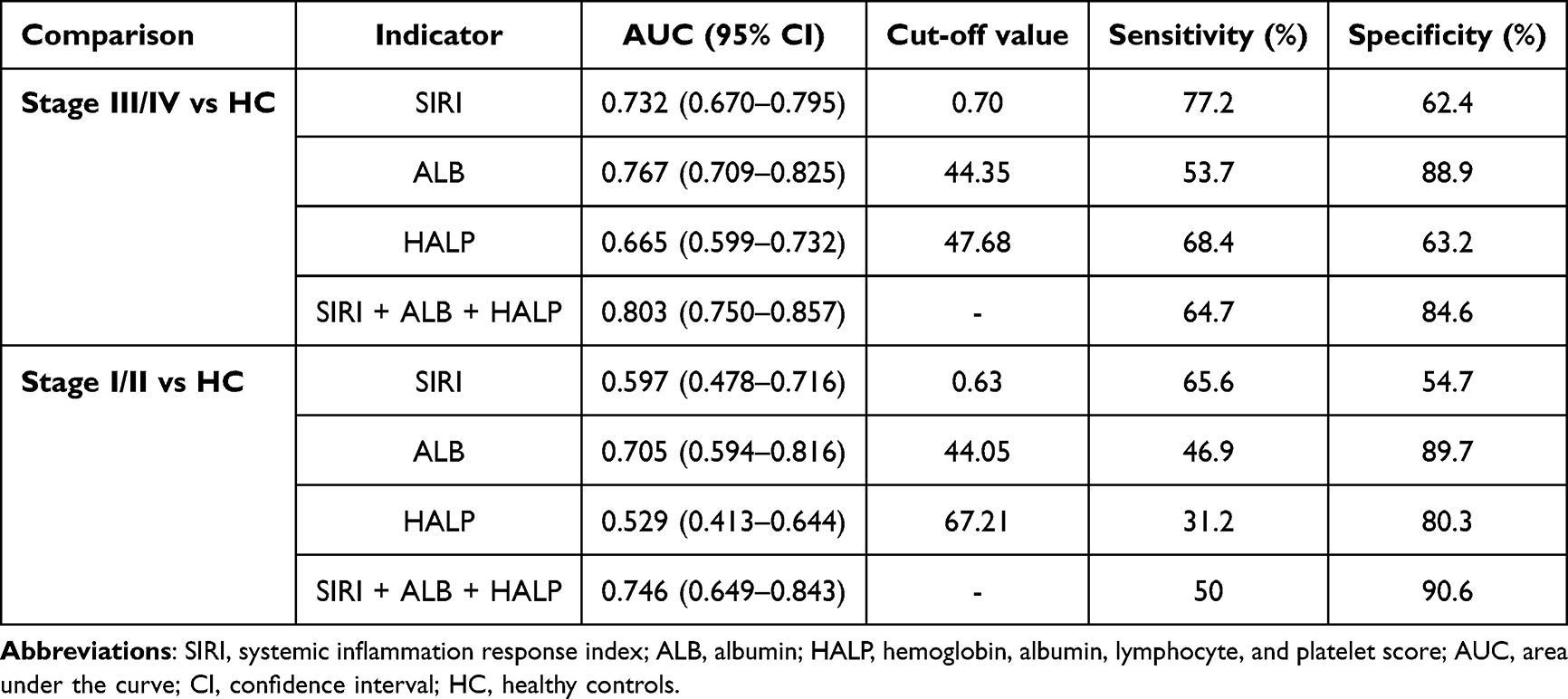 |
Table 2 Diagnostic Performance of SIRI, ALB, HALP, and Their Combination for Stage III/IV and Stage I/II Esophageal Cancer Versus Healthy Controls |
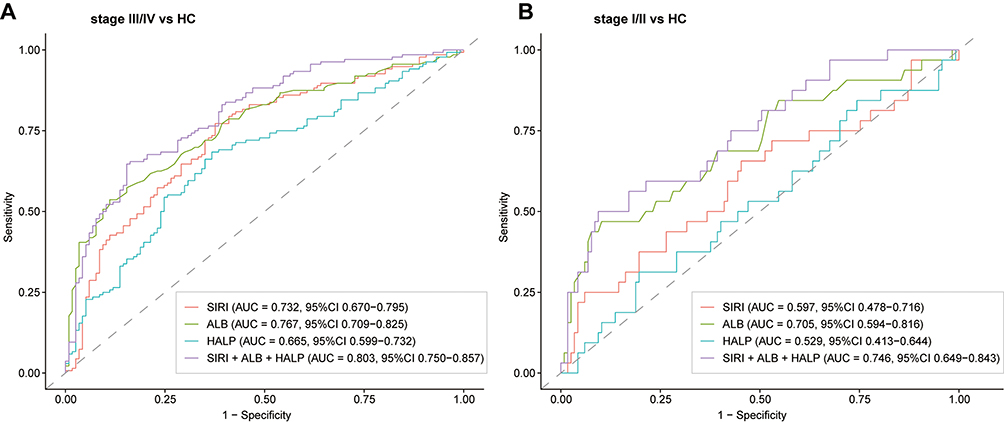 |
Figure 1 Receiver operating characteristic (ROC) curves of systemic inflammation response index (SIRI), albumin (ALB), hemoglobin–albumin–lymphocyte–platelet (HALP) score, and their combined model for discriminating esophageal cancer from healthy controls. (A) ROC curves for patients with pathological stage III/IV esophageal cancer versus healthy controls. (B) ROC curves for patients with pathological stage I/II esophageal cancer versus healthy controls. The combined model was constructed using binary logistic regression. |
To determine whether the same diagnostic pattern was present in earlier disease, we then evaluated the performance of these indicators in patients with pathological stage I/II disease. In the comparison between patients with pathological stage I/II disease and healthy controls, the optimal cut-off values for SIRI, ALB, and HALP were 0.63, 44.05, and 67.21, respectively. As shown in Table 2 and Figure 1B, ALB remained the best-performing single indicator, with an AUC of 0.705 (95% CI: 0.594–0.816). The combined model further improved the discriminatory performance, yielding an AUC of 0.746 (95% CI: 0.649–0.843). Taken together, these findings indicate that although the diagnostic performance was lower in early-stage disease than in advanced-stage disease, the combined model still improved discrimination compared with the individual markers.
Comparison of SIRI, ALB, and HALP Among the HC, Pathological Stage I/II, and Pathological Stage III/IV Groups
Given the stage-dependent differences observed in the ROC analyses, we next compared SIRI, ALB, and HALP across healthy controls, early-stage patients, and advanced-stage patients to further characterize their distribution patterns. Three study groups were included in the analysis (Table 3): the HC group (n = 117, 47 males, median age 36 years), the pathological stage I/II group (n = 32, 30 males, median age 62 years), and the pathological stage III/IV group (n = 136, 101 males, median age 68 years). Overall comparisons showed significant differences in SIRI, ALB, and HALP among the three groups (Table 3 and Figure 2A–C). Pairwise comparisons revealed that SIRI levels were significantly higher in the stage III/IV group than in the healthy control group. ALB levels were significantly lower in both stage I/II and stage III/IV patients than in healthy controls. HALP levels were significantly lower in the stage III/IV group than in both healthy controls and stage I/II patients, whereas no significant difference was observed between healthy controls and stage I/II patients. Overall, these results suggest that SIRI, ALB, and HALP vary with disease status and, to some extent, with pathological stage, particularly in advanced esophageal cancer.
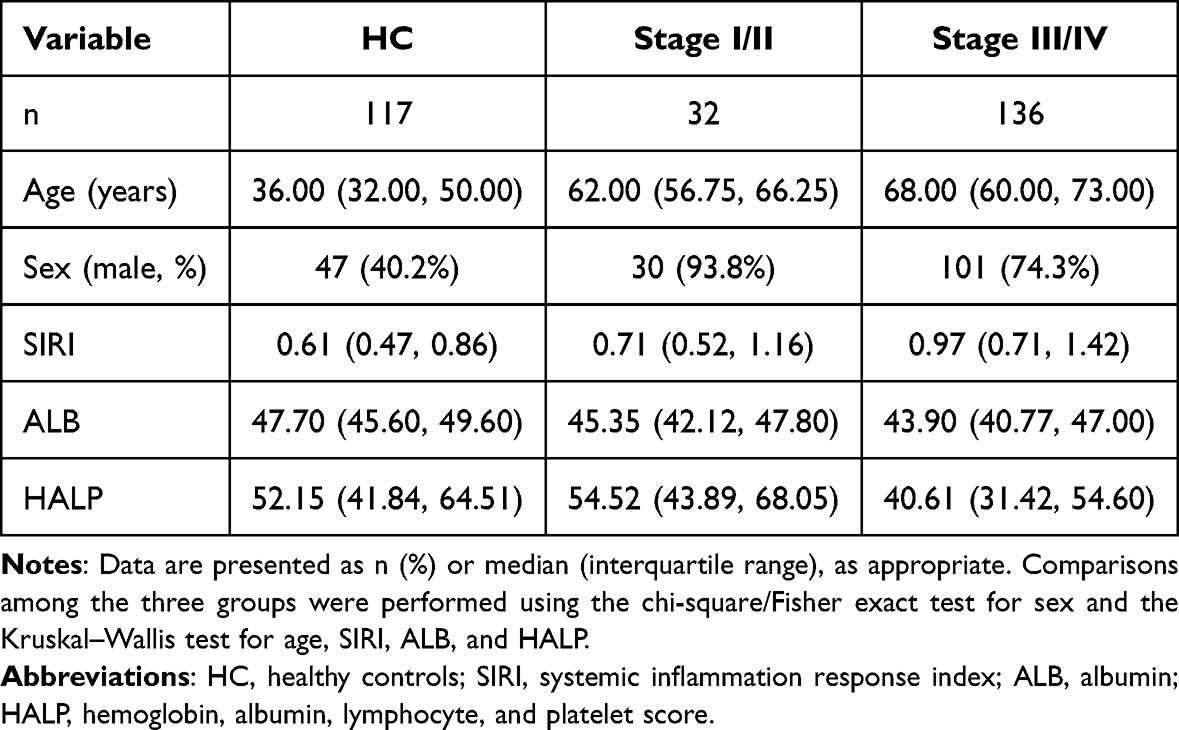 |
Table 3 Comparison of Clinical Characteristics and Inflammatory-Nutritional Indices Among HC, Stage I/II, and Stage III/IV Groups |
 |
Figure 2 Distribution of systemic inflammation response index (SIRI), albumin (ALB), and hemoglobin–albumin–lymphocyte–platelet (HALP) score across healthy controls (HC), stage I/II, and stage III/IV esophageal cancer groups. (A) Distribution of SIRI. (B) Distribution of ALB. (C) Distribution of HALP. Data are presented as boxplots showing the median and interquartile range, with individual data points overlaid. Overall comparisons were performed using the Kruskal–Wallis test, followed by pairwise Wilcoxon rank-sum tests with Bonferroni correction. NS indicates not statistically significant. |
Associations of SIRI, ALB, and HALP with Clinicopathological Characteristics in Patients with Esophageal Cancer
To further clarify the clinical relevance of these stage-related differences, we then examined the associations of SIRI, ALB, and HALP with clinicopathological characteristics in patients with esophageal cancer. According to the optimal cut-off values determined by ROC analysis, SIRI, ALB, and HALP were each categorized into high-value and low-value groups. As shown in Table 4, SIRI grouping was significantly associated with T stage (P = 0.035) and N stage (P = 0.031), but not with age, sex, tumor length, tumor location, or smoking history. ALB grouping was significantly associated with tumor length (P < 0.001) and T stage (P = 0.013), whereas no significant associations were observed with age, sex, tumor location, smoking history, or N stage. HALP grouping was significantly associated with smoking history (P = 0.006) and T stage (P = 0.004), but not with age, sex, tumor length, tumor location, or N stage.
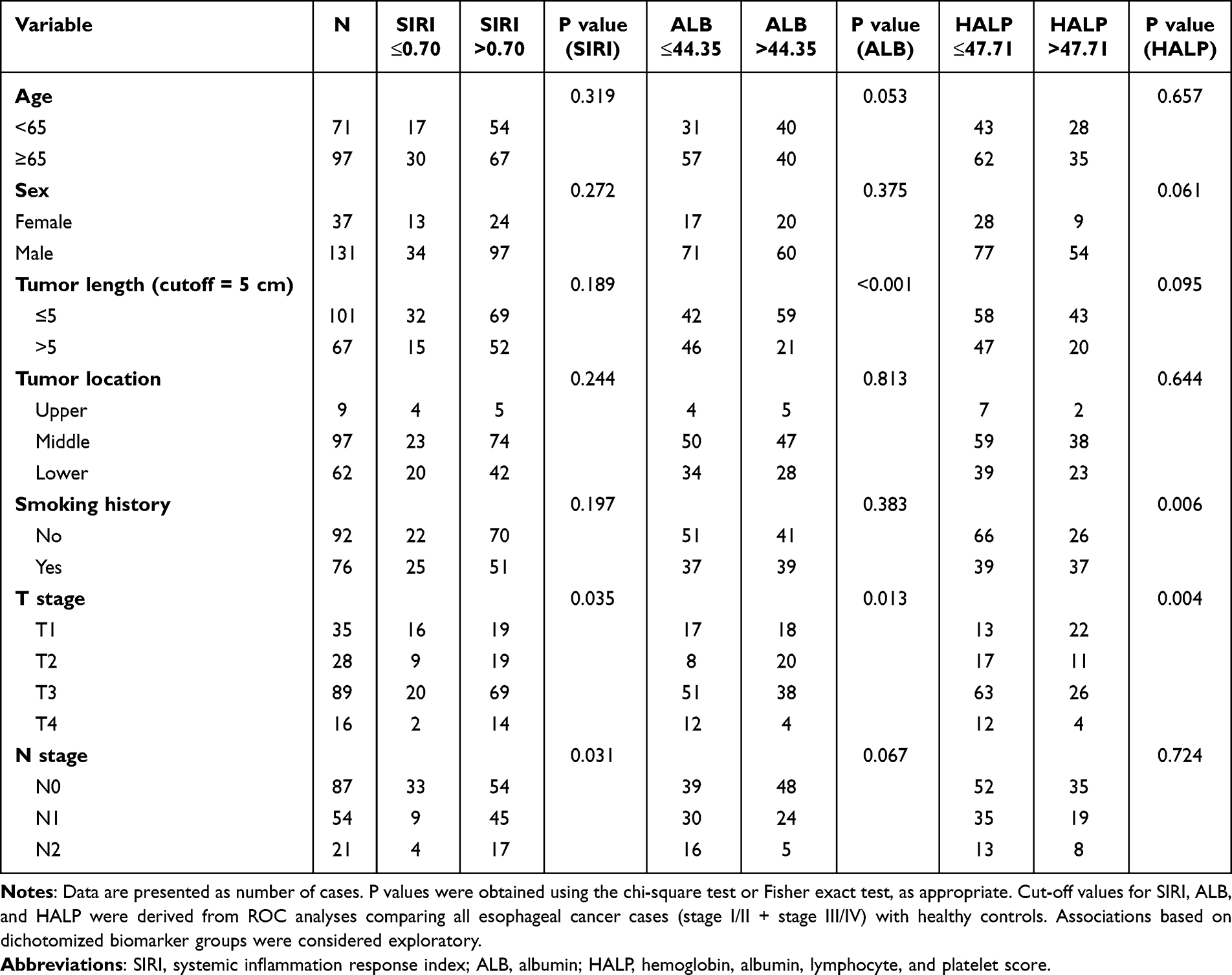 |
Table 4 Associations of SIRI, ALB, and HALP with Clinicopathological Characteristics in All Esophageal Cancer Cases |
Sensitivity and Decision Curve Analyses
Given the baseline imbalance in age and sex between esophageal cancer cases and healthy controls, additional sensitivity analyses were performed. In age- and sex-adjusted multivariable models, age remained significantly associated with esophageal cancer across all comparisons, whereas HALP retained significance mainly in the all-cancer and stage III/IV analyses. Detailed adjusted odds ratios, 95% confidence intervals, and P values are provided in Supplementary Table S1. Bootstrap internal validation demonstrated minimal optimism, with optimism-corrected AUCs of 0.966, 0.970, and 0.940 for all cancer vs. HC, stage III/IV vs. HC, and stage I/II vs. HC, respectively (Supplementary Table S2).
After age and sex matching using propensity score matching, the combined SIRI, ALB, and HALP model retained acceptable discriminatory performance, with an AUC of 0.809 (95% CI: 0.701–0.916). Among the individual biomarkers, HALP showed the highest AUC, followed by SIRI and ALB (Supplementary Table S3). Decision curve analysis showed that the full model provided greater net benefit than the biomarker-only model and the treat-all or treat-none strategies across most threshold probabilities (Supplementary Figure S2).
Discussion
In the present study, we systematically evaluated the discriminatory value of SIRI, ALB, and HALP in esophageal cancer and explored their associations with clinicopathological characteristics. Compared with healthy controls, patients with esophageal cancer had significantly increased SIRI levels, whereas ALB and HALP levels were significantly decreased, suggesting that enhanced systemic inflammation and impaired nutritional status may jointly accompany the occurrence and progression of esophageal cancer. ROC analysis showed that the combined model incorporating these three indicators demonstrated improved discriminatory performance compared with each single marker in distinguishing both advanced-stage (stage III/IV) and early-stage (stage I/II) esophageal cancer from healthy controls, with stronger performance in advanced-stage disease. The relatively lower discriminatory performance in stage I/II disease may be related to lower tumor burden and weaker systemic inflammatory and nutritional changes in early-stage patients. Three-group comparisons further showed that SIRI tended to increase with disease stage, whereas ALB and HALP were lower in advanced-stage disease. Clinicopathological analyses indicated that these biomarkers were associated with selected indicators of tumor burden and stage. After adjustment for age and sex, HALP retained significance mainly in the all-cancer and stage III/IV models.
SIRI reflects the integrated changes in systemic inflammatory response and immune status.15–17 Previous studies have shown that SIRI can predict survival outcomes in various malignancies. In pancreatic adenocarcinoma, SIRI helps clinicians improve treatment outcomes by identifying candidates for more aggressive treatment strategies.18 Similarly, SIRI has been considered a promising and novel prognostic biomarker in patients with colon cancer undergoing surgical resection.19 In gastric cancer, SIRI has also been reported as an independent prognostic factor.20 In the present study, SIRI levels were significantly higher in patients with esophageal cancer than in healthy controls, and showed an overall ascending pattern across the HC, stage I/II, and stage III/IV groups, suggesting that the degree of inflammatory activation may progressively increase with disease progression. Further clinicopathological analysis showed that SIRI was significantly associated with T stage and N stage, indicating that SIRI is related not only to the presence of the tumor itself, but also to local invasion and lymph node metastatic burden.
Several studies have shown that ALB is an appropriate marker of disease status and prognosis and is closely associated with C-reactive protein (CRP), acute phase proteins, and disease severity.21–23 In oral cancer, ALB may predict adverse reactions to chemotherapy in patients with oral malignancies.24 In patients with head and neck cancer, the impact of preoperative serum albumin on overall survival (OS) appears to be most pronounced in those with upper digestive tract involvement.25 In the present study, ALB levels were significantly lower in patients with esophageal cancer than in healthy controls, suggesting that nutritional depletion and tumor-related systemic responses may occur at an early stage of the disease. ROC analysis further showed that ALB was relatively sensitive in distinguishing patients from healthy individuals.
HALP is a composite immune-nutritional-inflammatory index with broad prognostic value across a wide range of diseases.26 The association of HALP with multiple cancers has been used to predict various clinical outcomes in different malignancies.27 In gastric cancer, HALP has been reported to be closely associated with clinicopathological characteristics and to serve as an independent prognostic factor.28 In the present study, we found that HALP had greater value in identifying advanced esophageal cancer and in reflecting disease stage progression. The observed changes in SIRI, ALB, and HALP may reflect the interaction between systemic inflammation, immune dysregulation, and nutritional impairment during esophageal cancer progression. Increased SIRI and decreased ALB and HALP are consistent with enhanced inflammatory activity, weakened antitumor immunity, and worsening nutritional status in patients with advanced disease.
Multiple studies have shown that a single biomarker is insufficient to fully capture the complex biological alterations associated with cancer, whereas integrated information on inflammation, nutritional status, and immune status may provide more comprehensive discriminatory ability.29 For example, in esophageal cancer, the systemic immune-inflammation index (SII) and prognostic nutritional index (PNI) have shown greater value in predicting overall survival (OS), and their combination can significantly improve predictive accuracy.30 In the present study, the combined model based on SIRI, ALB, and HALP consistently demonstrated improved discriminatory performance over each individual marker in the unadjusted ROC analyses, with the highest AUC observed in the comparison between stage III/IV esophageal cancer and healthy controls. After adjustment for age and sex, the AUC of the combined model remained higher than that of the base model, suggesting that SIRI, ALB, and HALP do not merely reflect differences in age and sex, but still provide incremental value beyond these demographic factors.
From a clinical perspective, SIRI, ALB, and HALP are all derived from routine hematological and biochemical tests, offering the advantages of convenient availability, low cost, and good reproducibility. In addition, these indicators were significantly associated with several clinicopathological characteristics, suggesting that they may not only help identify the presence of tumor, but also, to some extent, reflect tumor burden and disease progression. Nevertheless, this study has several limitations. Pathological subtype information was not sufficiently available for all patients. Therefore, subgroup analyses by squamous cell carcinoma and adenocarcinoma could not be performed. Given the epidemiological predominance of esophageal squamous cell carcinoma in China, the generalizability of our findings to adenocarcinoma requires further validation. A major limitation of this study was the marked baseline imbalance in age and sex between patients with esophageal cancer and healthy controls. Although age- and sex-adjusted logistic regression and matched sensitivity analyses were performed, residual confounding could not be completely excluded. The combined SIRI, ALB, and HALP model retained acceptable discriminatory performance after age and sex matching, supporting the robustness of the findings to some extent. Decision curve analysis also suggested a higher net benefit for the full model. However, because the clinical model based on age and sex alone showed substantial net benefit, the incremental clinical utility of these biomarkers should be interpreted cautiously.
Conclusion
In conclusion, SIRI, ALB, and HALP showed differential distributions between patients with esophageal cancer and healthy controls in this single-center retrospective case-control study. The combined model demonstrated improved discriminatory performance compared with individual biomarkers, particularly in patients with stage III/IV esophageal cancer, and retained acceptable performance after age- and sex-matched sensitivity analysis. These findings should be regarded as hypothesis-generating and require further validation in independent prospective cohorts.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. The data are not publicly available due to privacy restrictions, as they contain information that could compromise the privacy of research participants (patient data from the Cancer Hospital of Shandong First Medical University).
Ethical Approval
This study was approved by the Ethics Committee of the Cancer Hospital of Shandong First Medical University (approval no. SDTHEC [202604011]). This study complies with the Declaration of Helsinki. Due to the retrospective nature of the study and the use of anonymized data, the requirement for informed consent was waived by the ethics committee.
Acknowledgments
We thank the Cancer Hospital of Shandong First Medical University for providing all the samples in our study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Taishan Scholarship (tsqn202312362).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–11. doi:10.3322/caac.21660
2. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
3. Visaggi P, Barberio B, Ghisa M, et al. Modern diagnosis of early esophageal cancer: from blood biomarkers to advanced endoscopy and artificial intelligence. Cancers. 2021;13(13):3162. doi:10.3390/cancers13133162
4. Mecca M, Picerno S, Cortellino S. The killer’s web: interconnection between inflammation, epigenetics and nutrition in cancer. Int J Mol Sci. 2024;25(5):2750. doi:10.3390/ijms25052750
5. Iyengar NM, Gucalp A, Dannenberg AJ, Hudis CA. Obesity and cancer mechanisms: tumor microenvironment and inflammation. J Clin Oncol. 2016;34(35):4270–4276. doi:10.1200/JCO.2016.67.4283
6. Geng Y, Zhu D, Wu C, et al. A novel systemic inflammation response index (SIRI) for predicting postoperative survival of patients with esophageal squamous cell carcinoma. Int Immunopharmacol. 2018;65:503–510. doi:10.1016/j.intimp.2018.10.002
7. Menyhart O, Fekete JT, Győrffy B. Inflammation and colorectal cancer: a meta-analysis of the prognostic significance of the Systemic Immune-Inflammation Index (SII) and the Systemic Inflammation Response Index (SIRI). Int J Mol Sci. 2024;25(15):8441. doi:10.3390/ijms25158441
8. Zhang M, Xie C, Liu S, Fan H, Li Z, Tong X. The prognostic value of the hemoglobin, albumin, lymphocyte, and platelet (HALP) score in lung cancer: a systematic review and meta-analysis. J Clin Med. 2025;14(16):5701. doi:10.3390/jcm14165701
9. Almasaudi AS, Dolan RD, Edwards CA, McMillan DC. Hypoalbuminemia reflects nutritional risk, body composition and systemic inflammation and is independently associated with survival in patients with colorectal cancer. Cancers. 2020;12(7):1986. doi:10.3390/cancers12071986
10. Wu Z, Zhang Z, Gu C. Prognostic and clinicopathological impact of systemic inflammation response index (SIRI) on patients with esophageal cancer: a meta-analysis. Syst Rev. 2025;14(1):104. doi:10.1186/s13643-025-02847-7
11. Yamamoto S, Aoyama T, Maezawa Y, et al. The Hemoglobin, Albumin, Lymphocyte and Platelet (HALP) score as an independent prognostic factor for esophageal cancer patients who received curative treatment. In Vivo. 2025;39(2):885–893. doi:10.21873/invivo.13892
12. Shi Y, Shen G, Zeng Y, et al. Predictive values of the hemoglobin, albumin, lymphocyte and platelet score (HALP) and the modified-Gustave Roussy immune score for esophageal squamous cell carcinoma patients undergoing concurrent chemoradiotherapy. Int Immunopharmacol. 2023;123:110773. doi:10.1016/j.intimp.2023.110773
13. Lin S, Lin J, Weng J, et al. Combination of neutrophil-to-lymphocyte ratio and albumin concentration to predict the prognosis of esophageal squamous cell cancer patients undergoing esophagectomy. J Thorac Dis. 2023;15(4):2224–2232. doi:10.21037/jtd-23-333
14. Bertero L, Massa F, Metovic J, et al. Eighth edition of the UICC classification of Malignant Tumours: an overview of the changes in the pathological TNM classification criteria—what has changed and why? Virchows Arch. 2018;472(4):519–531. doi:10.1007/s00428-017-2276-y
15. Çakin Ö, Karaveli A, Yüce Aktepe M, Gümüş A, Yildirim ÖE. Comparison of inflammatory marker scoring systems and conventional inflammatory markers in patients over 65 years of age admitted to the intensive care unit: a Multicenter, Retrospective, Cohort Study. J Clin Med. 2024;13(14):4011. doi:10.3390/jcm13144011
16. Xia Y, Xia C, Wu L, Li Z, Li H, Zhang J. Systemic Immune Inflammation Index (SII), System Inflammation Response Index (SIRI) and risk of all-cause mortality and cardiovascular mortality: a 20-Year Follow-Up Cohort Study of 42,875 US adults. J Clin Med. 2023;12(3):1128. doi:10.3390/jcm12031128
17. Marchi F, Pylypiv N, Parlanti A, et al. Systemic immune-inflammation index and systemic inflammatory response index as predictors of mortality in ST-Elevation myocardial infarction. J Clin Med. 2024;13(5):1256. doi:10.3390/jcm13051256
18. Qi Q, Zhuang L, Shen Y, et al. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer. 2016;122(14):2158–2167. doi:10.1002/cncr.30057
19. Cao Y, Zheng X, Hu Y, et al. Levels of systemic inflammation response index are correlated with tumor-associated bacteria in colorectal cancer. Cell Death Dis. 2023;14(1):69. doi:10.1038/s41419-023-05602-9
20. In K, Kang S, Lee H, et al. Proportional correlation between systemic inflammation response index and gastric cancer recurrence time: a Retrospective Study. Cancers. 2025;17(9):1415. doi:10.3390/cancers17091415
21. Eckart A, Struja T, Kutz A, et al. Relationship of nutritional status, inflammation, and serum albumin levels during acute illness: a Prospective Study. Am J Med. 2020;133(6):713–722.e7. doi:10.1016/j.amjmed.2019.10.031
22. Keller U. Nutritional laboratory markers in malnutrition. J Clin Med. 2019;8(6):775. doi:10.3390/jcm8060775
23. Bretschera C, Boesiger F, Kaegi-Braun N, et al. Admission serum albumin concentrations and response to nutritional therapy in hospitalised patients at malnutrition risk: secondary analysis of a randomised clinical trial. EClinicalMedicine. 2022;45:101301. doi:10.1016/j.eclinm.2022.101301
24. Bao X, Liu F, Lin J, et al. Nutritional assessment and prognosis of oral cancer patients: a large-scale prospective study. BMC Cancer. 2020;20(1):146. doi:10.1186/s12885-020-6604-2
25. Luan CW, Yang HY, Tsai YT, Hsieh MC, Chou HH, Chen KS. Prognostic value of C-Reactive protein-to-albumin ratio in head and neck cancer: a meta-analysis. Diagnostics. 2021;11(3):403. doi:10.3390/diagnostics11030403
26. Vural A, Dolanbay T, Yagar H. Hemoglobin, albumin, lymphocyte and platelet (HALP) score for predicting early and late mortality in elderly patients with proximal femur fractures. PLoS One. 2025;20(1):e0313842. doi:10.1371/journal.pone.0313842
27. Farag CM, Antar R, Akosman S, Ng M, Whalen MJ. What is hemoglobin, albumin, lymphocyte, platelet (HALP) score? A comprehensive literature review of HALP’s prognostic ability in different cancer types. Oncotarget. 2023;14:153–172. doi:10.18632/oncotarget.28367
28. Chen XL, Xue L, Wang W, et al. Prognostic significance of the combination of preoperative hemoglobin, albumin, lymphocyte and platelet in patients with gastric carcinoma: a retrospective cohort study. Oncotarget. 2015;6(38):41370–41382. doi:10.18632/oncotarget.5629
29. Zhang J, Zhang L, Duan S, Li Z, Li G, Yu H. Single and combined use of the platelet-lymphocyte ratio, neutrophil-lymphocyte ratio, and systemic immune-inflammation index in gastric cancer diagnosis. Front Oncol. 2023;13:1143154. doi:10.3389/fonc.2023.1143154
30. Ma H, Liu Y, Ye H, Gao F, Li Z, Qin S. The prognostic value of preoperative laboratory data indicators in patients with esophageal carcinoma: an observational study. Medicine. 2024;103(24):e38477. doi:10.1097/MD.0000000000038477
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Hypoalbuminemia is Associated with Higher 90-Day Mortality and Poor Prognosis in Patients with Esophageal Squamous Cell Carcinoma and Liver Cirrhosis Receiving Radiotherapy-Based Therapy
Hua YY, Kuo MC, Chen YH, Lu HI, Lo CM, Chen Y, Wang YM, Lin YH, Li SH, Huang SY
Cancer Management and Research 2024, 16:1693-1704
Published Date: 3 December 2024