Back to Journals » International Journal of General Medicine » Volume 16
Systemic Immune-Inflammation and Systemic Inflammation Response Indices are Predictive Markers of Mortality in Inpatients Internal Medicine Services
Authors Çavuşoğlu Türker B, Ahbab S, Türker F ![]() , Hoca E, Çiftçi Öztürk E, Kula AC, Öztürk H, Urvasızoğlu AÖ, Bulut M
, Hoca E, Çiftçi Öztürk E, Kula AC, Öztürk H, Urvasızoğlu AÖ, Bulut M ![]() , Yasun Ö
, Yasun Ö ![]() , Ataoğlu HE
, Ataoğlu HE
Received 16 May 2023
Accepted for publication 21 July 2023
Published 26 July 2023 Volume 2023:16 Pages 3163—3170
DOI https://doi.org/10.2147/IJGM.S420332
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Betül Çavuşoğlu Türker,1 Süleyman Ahbab,1 Fatih Türker,1 Emre Hoca,1 Ece Çiftçi Öztürk,1 Atay Can Kula,2 Hüseyin Öztürk,3 Ayşe Öznur Urvasızoğlu,1 Merve Bulut,4 Özge Yasun,5 Hayriye Esra Ataoğlu1
1Department of Internal Medicine, University of Health Sciences, Haseki Health Training and Research Hospital, İstanbul, Turkey; 2Internal Medicine Department, Ivrindi State Hospital, Balıkesir, Turkey; 3Department of Internal Medicine, University of Health Sciences, Başakşehir Çam ve Sakura City Hospital, İstanbul, Turkey; 4Department of Internal Medicine, University of Health Sciences, Gaziosmanpaşa Taksim Health Training and Research Hospital, İstanbul, Turkey; 5Internal Medicine Department, Hakkari State Hospital, Hakkari, Turkey
Correspondence: Fatih Türker, University of Health Sciences, Haseki Health Training and Research Hospital, Internal Medicine Clinic, Aksaray, Dr. Adnan Adıvar Cd. No: 9, İstanbul, 34130, Turkey, Tel +905364721656, Fax +90212 453 20 00, Email [email protected]
Purpose: Internal medicine services serve the patient population with many chronic diseases. Therefore, it is high mortality rates compared to other departments of the hospital. Estimating the prognostic risk of hospitalized patients may be useful in mortality for patients. İn this study, we evaluated the level of Systemic Immune Inflammation Index (SII) and Systemic Inflammation Response Index (SIRI) and its association with mortality in inpatients.
Patients and methods: This study was performed in 2218 patients who were hospitalized between January 1st–December 31th of 2019. Patients were followed up for three years about primary endpoint as all-cause (except for unnatural deaths) mortality. Participants were divided into 4 equal groups according to their increasing levels of SII and SIRI. (Quartile 1– 4) Age, gender, diabetes mellitus, hypertension, coronary artery disease, chronic kidney disease, malignancies (solid), white blood cell, neutrophil, lymphocyte, monocytes, hemoglobin, hematocrit, platelet, CRP, albumin, Systemic Inflammation Response Index (Quartile 1– 4), Systemic Immune Inflammation Index (Quartile 1– 4) were compared between survival and non-survival groups.
Results: There were 1153 female and 1065 male participants enrolled. Compared with surviving patients, patients who died were older and had a higher prevalence of diabetes mellitus, hypertension, malignancy, chronic kidney disease and coronary artery disease (p < 0.001). There was a lower proportion of female patients among the patients who died. Compared to the survivor group, group who died exhibited a significant increase in CRP level, neutrophil, white blood cell and monocyte counts, but had a lower lymphocyte count, albumin level and hemoglobin count (P < 0.001). Results of Cox regression analysis showed that age, chronic kidney disease, malignancy, SIRI quartile 3, 4 and SII quartile 3, 4 pointed out a close relationship with mortality risk. (P < 0.001).
Conclusion: The SIRI and SII have indicated the clinical importance of as novel markers for predicting mortality in inpatients.
Keywords: internal medicine inpatients, mortality, SIRI, SII
Introduction
Internal medicine clinicians serve a patient population that suffers from many chronic diseases. As such, those patients have higher mortality rates than those empanelled to other departments in a hospital,1,2 owing to factors of high infection rates and advanced age.3–5 Various prognostic risk scoring systems and parameters have been developed to predict internal medicine patient mortality6 so that those with worse prognoses can be treated earlier and monitored more closely. Notably, there is growing evidence to suggest that inflammation markers can be used to make such predictions.7
Evidence has suggested that chronic low-grade inflammation leads to vascular endothelial injury, oxidative stress, and thrombosis, which may be the underlying cause of mortality.8 One important predictive inflammatory response indicator is the measured change in peripheral blood cell composition.9 Because this measurement is inexpensive and easily made, it is widely used in clinical practice. Previous studies have shown that neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR) and platelet-to-lymphocyte ratio (PLR) are important predictors of various diseases (eg cerebrovascular and coronary artery) and other malignancies.10–15
As more complex peripheral blood inflammatory markers are now understood, systemic inflammation response index (SIRI) and systemic immune-inflammation (SII) metrics have been established.16,17 SIRI is derived from neutrophil, lymphocyte and monocyte data, and SII is derived from neutrophil, lymphocyte and platelet data. Both indices were developed to determine the prognoses of neoplastic diseases.18–20 Subsequent studies reported that SII could be used as an inflammatory indicator for autoimmune illnesses, such as Behçet’s disease,21 and other studies showed that a high SIRI rating is associated with an increased risk of acute coronary syndrome (patients with chest pain) and increased risk of stroke (patients with supraventricular tachycardia).22,23 Because only a few studies have utilised SIRI and SII indices to prognosticate on malignancies and other chronic diseases,24 this study investigates the utility of SII and SIRI indices in evaluating the mortality of patients in internal medicine clinics.
Methods
Study Design, Patient Selection and Endpoints
This retrospective cohort study was conducted at the Internal Medicine Clinic of the Haseki Health Training and Research Hospital utilising medical health and clinical data records of 2218 hospitalised and discharged patients between 1 January and 31 December 2019. The informed consent was obtained from all patients who were hospitalized at our clinic. All data were collected anonymously and without any patient-identifying information, and the study protocol was reviewed and approved by the Institutional Review Board of the University of Health Sciences at the Haseki Health Training and Research Hospital (Ref. No. 23R/2018). Moreover, the study was conducted in accordance with the Key Principles of Good Clinical Practices and the Declaration of Helsinki.
Readmissions, patients with insufficient data and intensive-care transfers were excluded, as were patients with haematological malignancy, pregnancy and end-stage liver disease, as well as those taking nonsteroidal anti-inflammatory agents, anti-inflammatories and immunosuppressives (eg steroids), owing to the risk of hemogram parameters being affected. Patients’ whose primary endpoints and all-cause mortalities, apart from unnatural deaths (eg accidents, suicides or murders), fell within the three-year follow-up period were also excluded. All follow-up data were collected from the Haseki Training and Research Hospital data processing system, and the Turkish National Mortality Registry was used to confirm all death reports.
Specific variables of age, gender, diabetes mellitus, hypertension, coronary artery disease, chronic kidney disease, malignancies (solid), white blood cell, neutrophil, lymphocyte, monocyte, haemoglobin, haematocrit, platelet, CRP and albumin were recorded. SIRI scores were formulated for all participants as the neutrophil × (monocyte / lymphocyte) count, and SII scores reflected the platelet × (neutrophil / lymphocyte) count. Participants were divided into 4 equal groups according to their increasing levels of SII and SIRI. (Quarter 1 to 4 incrementally) The quartiles of SII and SIRI levels were compared between the survival and non-survival groups.
Laboratory Measurements
Routine blood samples for all laboratory tests were taken after a 12-h fasting period between 6 and 7 am. Blood samples were taken on the first day of hospitalisation prior to the start of drug treatment and were analysed immediately. Laboratory findings were obtained from patients’ electronic medical records. The listed biochemical parameters were measured for all participants. During the follow-up period, 920 participants died.
Statistical Method
IBM SPSS Statistics for Windows (Version 25.0, IBM Corp., Armonk, NY, USA) was used for the statistical analyses. Continuous data were presented as means and standard deviations over Q1–Q4, and all categorical variables were represented as percentages. The ratios per group were compared using the chi-square test between survivors and non-survivors. The Student’s t-test was used to compare the groups based on normally distributed numerical data. In the case of abnormal distribution of numerical data, the Mann–Whitney-U test was used to compare the two groups. The Cox proportional-hazards regression model was used to analyze the effects of the variables on event-free survival. The predictive performance of age, chronic kidney disease, malignancy SIRI and SII was assessed by Cox regression. Parameter found to be different between outcomes (non-survivor) were included in the regression models to find out parameters showing independent relationship with these outcomes. A p-value of less than 0.05 was considered significant.
Results
A total of 2218 patients (1153 females and 1065 males) who were hospitalized between January 1st–December 31th, 2019, were included in this study (Figure 1). The baseline characteristics of the survivor and exitus groups are presented (Table 1). Compared with surviving patients, patients who died were older and had a higher prevalence of diabetes mellitus, hypertension, malignancy, chronic kidney disease, and coronary artery disease (p <0.001 and p <0.001, respectively). Moreover, there was a lower proportion of female patients among those who died (p = 0.019). CRP levels were higher, whereas albumin levels were lower, in patients who died. Compared to the survivor group, the group that died exhibited a significant increase in neutrophil, white blood cell, and monocyte counts but had a lower lymphocyte count and hemoglobin count (P <0.001, <0.001, <0.001, <0.001, and <0.001, respectively).
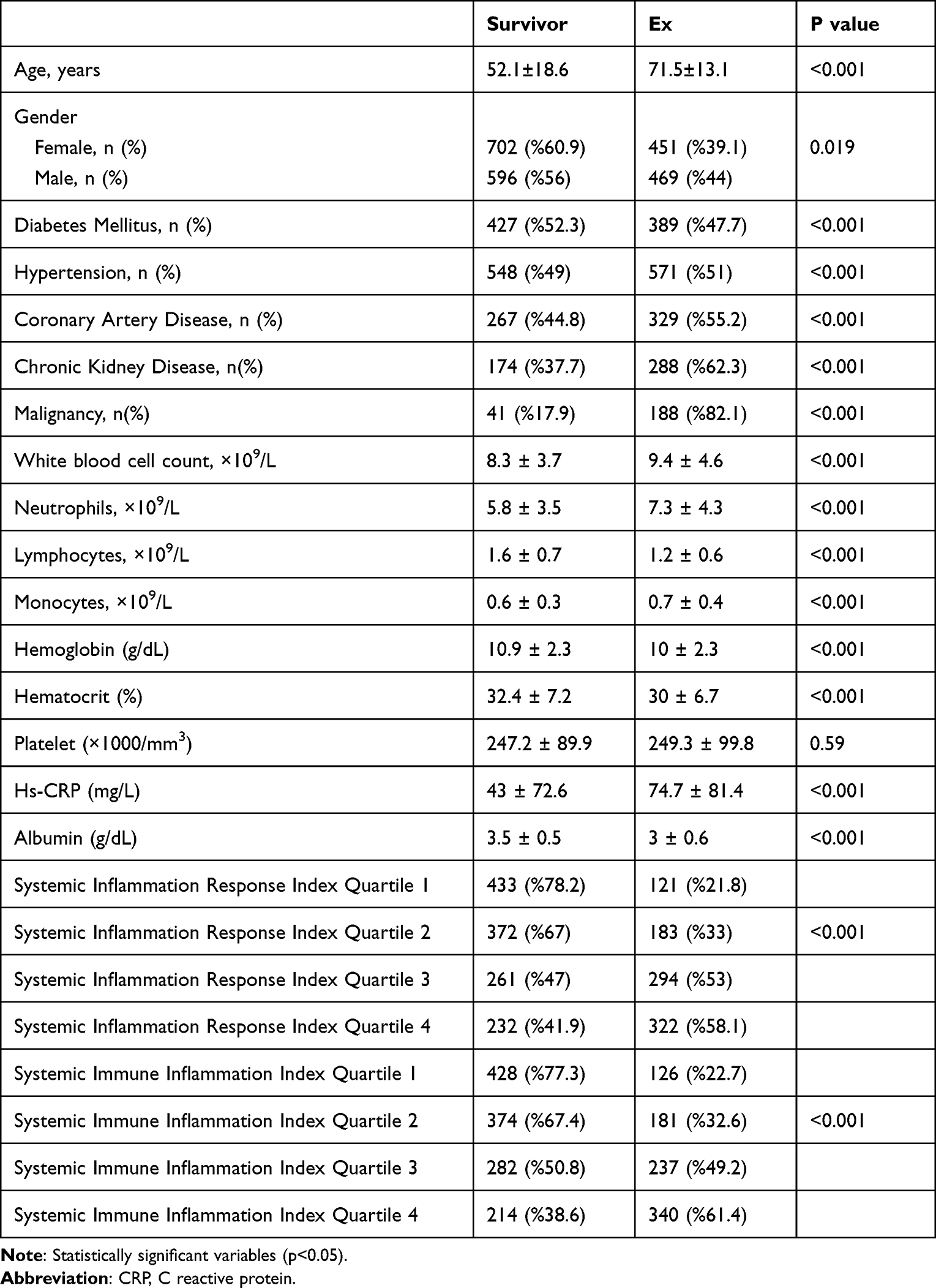 |
Table 1 Baseline Characteristics of Patients |
 |
Figure 1 Flow chart for patients’ selection. |
A multivariate Cox proportional hazards model was used to evaluate the mortality risk between groups. The results of the Cox regression analysis with age, chronic kidney disease, malignancy SIRI, and SII are presented (Table 2 and Table 3). SIRI quartiles 3 and 4 and SII quartiles 3 and 4 indicated a close relationship for the mortality risk (SII: [Quartile 3 – Quartile 1] OR:1.72, 95% CI = 1.14–2.60, P = 0.01; SII: [Quartile 4 – Quartile 1] OR:2.41, 95% CI = 1.62–3.57, P <0.001 Table 2). (SII: [Quartile 3 – Quartile 1] OR: 2.08, 95% CI = 1.40–3.07 p<0.001; SII: [Quartile 4 – Quartile 1] OR: 2.02, 95% CI = 1.37–2.94, P <0.001 Table 3). Moreover, the mortality risk was higher for those with malignancy, chronic kidney disease, and advanced age (p <0.001 and p <0.001, respectively).
 |
Table 2 Cox Regression Analysis for Systemic Immune Inflammation Index |
 |
Table 3 Cox Regression Analysis for Systemic Inflammation Response Index |
In both quartiles 1 and 2, the proportion of patients who died was lower than that of patients who survived (SIII: [Q1] 77.3% to 22.7%; SIRI: [Q1] 78.2% to 21.8%; SIII: [Q2] 67.4% vs 32.6% SIRI: [Q2] 67% vs 33%). The number of patients who died in quartiles 3 and 4 of the SIRI was higher (SIRI: [Q3] 47% to 53%; [Q4] 41.9% to 58.1%) (Figure 2). While the number of surviving patients was higher in quartile 3 of the SII, the number of patients who died in quartile 4 was higher (SII: [Q3] 50.8% to 49.2%; [Q4] 38.6% to 61.4%) (Figure 3).
 |
Figure 2 Number of survivors and nonsurvivors according to SIRI’s quartiles. |
 |
Figure 3 Number of survivors and nonsurvivors according to SII’s quartiles. |
Discussion
Internal medicine professionals face a significant burden on the health system due to increased patient burden, complicated patients, and increased mortality rates. In this study, age, chronic kidney disease, malignancy, and elevated SIII and SIRI scores were independently associated with mortality in hospitalized patients in the Department of Internal Medicine.
In our study, age, chronic kidney disease, and malignancy were associated with mortality. Studies have shown that advanced age, malignancy, and chronic kidney disease are strongly associated with mortality, as in our study.3–5 Apart from these known factors, various markers have been put forward to predict mortality.
As a new type of inflammatory index, the systemic inflammatory response index (SIRI) and systemic immune-inflammation (SII) indexes are based on the components of CBC, such as neutrophils, platelets, lymphocytes, and monocytes. Clinically, the SII and SIRI can be easily obtained from routine blood screening results, which is cost-effective for patients. These indices have been used to predict mortality in various diseases. Studies on mortality using these indices are relatively new and limited. Yun et al while doing this study in patients with aneurysmal subarachnoid hemorrhage; other investigators have investigated the relationship between the Systemic Inflammation Response Index and the Systemic Immune-inflammation index and mortality in various cancer patients.25–28
We found a strong correlation between SIRI, SII, and all-cause mortality and determined that mortality increased as the SII and SIRS quartiles increased. Studies have suggested that neutrophils play an important role in the inflammatory response in atherosclerosis.29–31 When the monocytes activate, they transform to lipid-laden macrophages. This transformation is an essential process in the formation of atherosclerotic lesions.32 Lymphocytes have a regulatory function in inflammation and an inhibitory effect on atherosclerosis.33 That’s why studies suggest that the SII has high prognostic value in patients with cardiovascular disease.34 Moreover, high levels of SII are associated with elevated levels of cytokines such as interleukin-6, interleukin-8, and interleukin-10, which are implicated in the systemic chronic inflammation response.35,36 The increased mortality in participants with a higher SII was thought to be due to chronic inflammation, which could produce reactive oxygen and nitrogen species, increasing the risk of death.37 An increase in SII and SIRI quartiles may be associated with an increase in atherosclerosis and chronic inflammation. Therefore, an increase in the SIRI and SII quartiles was closely associated with an increase in mortality.
However, research on this topic is new and limited research has been conducted on this topic. When the literature was examined, it was observed that the studies were generally related to a single disease. The feature that distinguishes our study from other studies is the high number of cases, the long follow-up period, and the inclusion of patients with various chronic diseases. In our study, unlike others, we found that as SIRI and SII levels increased, all cause of mortality increased inpatients in correlation with SIRI and SII levels.
Conclusion
Chronic inflammation is associated with various health problems including cardiovascular diseases, cancer, and mortality.
Our study indicates the clinical importance of SIRI and SII as novel markers for predicting mortality in inpatients in internal medicine clinics. It was found that the SIRI and SII at the time of admission were significantly related to the prognosis of hospitalized patients in the internal medicine clinic. Elevated SIRI and SII indices independently predicted poor prognosis. The systemic immune inflammation index and systemic inflammation response index have been identified as novel prognostic markers for all-cause mortality. The SIRI and SII may serve as useful, low-cost, and noninvasive prognostic mortality markers for inpatients. Further studies are necessary to validate our findings.
Acknowledgments
We would like to thank the editorial team and the participants who contributed to our study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bai AD, Srivastava S, Tomlinson GA, et al. Mortality of hospitalised internal medicine patients bedspaced to non-internal medicine inpatient units: retrospective cohort study. BMJ Qual Saf. 2018;27(1):11–20. doi:10.1136/bmjqs-2017-006925
2. Bogler O, Liu J, Cadesky B, et al. Quality of care and outcomes in internal medicine patients bedspaced to noninternal medicine units. Medicine. 2021;100(18):e25737. doi:10.1097/MD.0000000000025737
3. Urhoj SK, Jespersen LN, Nissen M, et al. Advanced paternal age and mortality of offspring under 5 years of age: a register-based cohort study. Hum Reprod. 2014;29(2):343–350. doi:10.1093/humrep/det399
4. Lavie CJ, Lee DC, Sui X, et al. Effects of running on chronic diseases and cardiovascular and all-cause mortality. Mayo Clin Proc. 2015;90(11):1541–1552. doi:10.1016/j.mayocp.2015.08.001
5. Dauer CC. Mortality from infections. Public Health Rep. 1961;76(2):159–165. doi:10.2307/4591084
6. Guo G, Chen X, Cai X, et al. Inflammation-based markers can predict the prognosis of geriatric patients with metastatic colorectal cancer receiving first-line chemotherapy. Transl Cancer Res. 2019;8(4):1137–1147. doi:10.21037/tcr.2019.06.27
7. Tong-Minh K, Welten I, Endeman H, et al. Predicting mortality in adult patients with sepsis in the emergency department by using combinations of biomarkers and clinical scoring systems: a systematic review. BMC Emerg Med. 2021;21(1):70. doi:10.1186/s12873-021-00461-z
8. Jin Z, Wu Q, Chen S, et al. The associations of two novel inflammation indexes, SII and SIRI with the risks for cardiovascular diseases and all-cause mortality: a ten-year follow-up study in 85,154 individuals. J Inflamm Res. 2021;14:131–140. doi:10.2147/JIR.S283835
9. Macrez R, Ali C, Toutirais O, et al. Stroke and the immune system: from pathophysiology to new therapeutic strategies. Lancet Neurol. 2011;10(5):471–480. doi:10.1016/S1474-4422(11)70066-7
10. Cushman M, Arnold AM, Psaty BM, et al. C-reactive protein and the 10-year incidence of coronary heart disease in older men and women: the cardiovascular health study. Circulation. 2005;112(1):25–31. doi:10.1161/CIRCULATIONAHA.104.504159
11. Wheeler JG, Mussolino ME, Gillum RF, et al. Associations between differential leucocyte count and incident coronary heart disease: 1764 incident cases from seven prospective studies of 30,374 individuals. Eur Heart J. 2004;25:1287–1292. doi:10.1016/j.ehj.2004.05.002
12. Anrather J, Iadecola C. Inflammation and stroke: an overview. Neurotherapeutics. 2016;13(4):661–670. doi:10.1007/s13311-016-0483-x
13. Ohno Y. Role of systemic inflammatory response markers in urological malignancy. Int J Urol. 2019;26(1):31–47. doi:10.1111/iju.13801
14. Kim HS, Ku JH. Systemic inflammatory response based on neutrophil-to-lymphocyte ratio as a prognostic marker in bladder cancer. Dis Markers. 2016;2016:8345286. doi:10.1155/2016/8345286
15. Dolan RD, McSorley ST, Horgan PG, Laird B, McMillan DC. The role of the systemic inflammatory response in predicting outcomes in patients with advanced inoperable cancer: systematic review and meta-analysis. Crit Rev Oncol Hematol. 2017;116:134–146. doi:10.1016/j.critrevonc.2017.06.002
16. Geng Y, Zhu D, Wu C, et al. A novel systemic inflammation response index (SIRI) for predicting postoperative survival of patients with esophageal squamous cell carcinoma. Int Immunopharmacol. 2018;65:503–510. doi:10.1016/j.intimp.2018.10.002
17. Xie QK, Chen P, Hu WM, et al. The systemic immune-inflammation index is an independent predictor of survival for metastatic colorectal cancer and its association with the lymphocytic response to the tumor. J Transl Med. 2018;16:273. doi:10.1186/s12967-018-1638-9
18. Qi Q, Zhuang L, Shen Y, et al. A novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapy. Cancer. 2016;122:2158–2167. doi:10.1002/cncr.30057
19. Fest J, Ruiter R, Mulder M, et al. The systemic immune-inflammation index is associated with an increased risk of incident cancer-a population-based cohort study. Int J Cancer. 2020;146:692–698. doi:10.1002/ijc.32303
20. Jomrich G, Paireder M, Kristo I, et al. High systemic immune-inflammation index is an adverse prognostic factor for patients with gastroesophageal adenocarcinoma. Ann Surg. 2021;273:532–541. doi:10.1097/SLA.0000000000003370
21. Tanacan E, Dincer D, Erdogan FG, et al. A cutoff value for the systemic immune-inflammation index in determining activity of behçet disease. Clin Exp Dermatol. 2021;46(2):286–291. doi:10.1111/ced.14432
22. Dziedzic EA, Gąsior JS, Tuzimek A, et al. Investigation of the associations of novel inflammatory biomarkers-Systemic Inflammatory Index (SII) and Systemic Inflammatory Response Index (SIRI)-with the severity of coronary artery disease and acute coronary syndrome occurrence. Int J Mol Sci. 2022;23:9553. doi:10.3390/ijms23179553
23. Lin KB, Fan FH, Cai MQ, et al. Systemic immune inflammation index and system inflammation response index are potential biomarkers of atrial fibrillation among the patients presenting with ischemic stroke. Eur J Med Res. 2022;27:106. doi:10.1186/s40001-022-00733-9
24. Xia Y, Xia C, Wu L, et al. Systemic Immune Inflammation Index (SII), System Inflammation Response Index (SIRI) and risk of all-cause mortality and cardiovascular mortality: a 20-year follow-up cohort study of 42,875 US adults. J Clin Med. 2023;12(3):1128–1131. doi:10.3390/jcm12031128
25. Yun S, Yi HJ, Lee DH, et al. Systemic inflammation response index and systemic immune-inflammation index for predicting the prognosis of patients with aneurysmal subarachnoid hemorrhage. J Stroke Cerebrovasc Dis. 2021;30(8):105861. doi:10.1016/j.jstrokecerebrovasdis.2021.105861
26. Huang H, Liu Q, Zhu L, et al. Prognostic value of preoperative systemic immune-inflammation index in patients with cervical cancer. Sci Rep. 2019;9(1):3284. doi:10.1038/s41598-019-39150-0
27. Huang Y, Chen Y, Zhu Y, et al. Postoperative Systemic Immune-Inflammation Index (SII): a superior prognostic factor of endometrial cancer. Front Surg. 2021;8:704235. doi:10.3389/fsurg.2021.704235
28. He K, Si L, Pan X, et al. Preoperative Systemic Immune-Inflammation Index (SII) as a superior predictor of long-term survival outcome in patients with stage I–II gastric cancer after radical surgery. Front Oncol. 2022;12:829689. doi:10.3389/fonc.2022.829689
29. Su G, Zhang Y, Xiao R, et al. Systemic immune-inflammation index as a promising predictor of mortality in patients with acute coronary syndrome: a real-world study. J Int Med Res. 2021;49(5):3000605211016274. doi:10.1177/03000605211016274
30. Chan SL, Wong LL, Chan KA, et al. Development of a novel inflammation-based index for hepatocellular carcinoma. Liver Cancer. 2020;9:167–181. doi:10.1159/000504252
31. Motomura T, Shirabe K, Mano Y, et al. Neutrophil-lymphocyte ratio reflects hepatocellular carcinoma recurrence after liver transplantation via inflammatory microenvironment. J Hepatol. 2013;58:58–64. doi:10.1016/j.jhep.2012.08.017
32. Furman D, Campisi J, Verdin E, et al. Chronic inflammation in the etiology of disease across the life span. Nat Med. 2019;25(12):1822–1832. doi:10.1038/s41591-019-0675-0
33. Azab B, Zaher M, Weiserbs KF, et al. Usefulness of neutrophil to lymphocyte ratio in predicting short- and long-term mortality after non-ST-elevation myocardial infarction. Am J Cardiol. 2010;106(4):470–476. doi:10.1016/j.amjcard.2010.03.062
34. Huh JY, Ross GW, Chen R, et al. Total and differential white blood cell counts in late life predict 8-year incident stroke: the Honolulu Heart Program. J Am Geriatr Soc. 2015;63(3):439–446. doi:10.1111/jgs.13298
35. Shah AD, Denaxas S, Nicholas O, et al. Neutrophil counts and initial presentation of 12 cardiovascular diseases: a CALIBER Cohort Study. J Am Coll Cardiol. 2017;69(9):1160–1169. doi:10.1016/j.jacc.2016.12.022
36. Ghattas A, Griffiths HR, Devitt A, et al. Monocytes in coronary artery disease and atherosclerosis: where are we now? J Am Coll Cardiol. 2013;62(17):1541–1551. doi:10.1016/j.jacc.2013.07.043
37. Kim JH, Lee YJ, Park B. Higher monocyte count with normal white blood cell count is positively associated with 10-year cardiovascular disease risk determined by Framingham risk score among community-dwelling Korean individuals. Medicine. 2019;98:e15340. doi:10.1097/MD.0000000000015340
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.