Back to Journals » Cancer Management and Research » Volume 14
Systematic Immunological Level Determined the Prognosis of Leptomeningeal Metastasis in Lung Cancer
Authors Hong Y ![]() , Duan P, He L, Li Q, Chen Y, Wang P
, Duan P, He L, Li Q, Chen Y, Wang P ![]() , Fu Y, Liu T
, Fu Y, Liu T ![]() , Ding Z
, Ding Z ![]()
Received 2 November 2021
Accepted for publication 3 March 2022
Published 15 March 2022 Volume 2022:14 Pages 1153—1164
DOI https://doi.org/10.2147/CMAR.S347323
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Antonella D'Anneo
Ye Hong,1 Ping Duan,2 Lang He,3 Qing Li,1 Yueyun Chen,1 Peipei Wang,1 Yang Fu,1 Ting Liu,1 Zhenyu Ding1
1Department of Biotherapy, Cancer Center, West China Hospital, West China Medical School, Sichuan University, Chengdu, People’s Republic of China; 2Department of Oncology, Cheng Du First People’s Hospital, Chengdu, People’s Republic of China; 3Department of Oncology, The Fifth People’s Hospital Affiliated to Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China
Correspondence: Zhenyu Ding, Department of Biotherapy, Cancer Center, West China Hospital, West China Medical School, Sichuan University, Chengdu, 610041, People’s Republic of China, Tel +86 28 8542 2562, Fax +86 28 8516 4059, Email [email protected]
Background and Purpose: Leptomeningeal metastases (LM) is the end-event of lung cancer and the prognosis is dismal. Few studies explored the prognostic performance of systematic immunological levels in lung cancer patients with LM. Our study aimed to explore the possible relationship between the prognosis of LM and systematic immunological level and other clinical characteristics.
Methods: This retrospective, multi-institutional, observational study was conducted in 4 tertiary centers in China. Patients were screened from January 2009 to May 2019. Patients with radiographically or histologically confirmed LM were enrolled. The data of systematic immunological level and other clinical characteristics of each patient were extracted and statistically analyzed to establish a prognostic model based on statistical analysis results. The predictive accuracy and discriminative capability of the model were evaluated by the calibration curve and concordance index (C-index).
Results: A total of 109 patients were enrolled in the study. Patients with adenocarcinoma, tumors harboring EGFR mutation, at their age of 50– 59, with either bone, brain, or lung metastases, were enriched in this cohort. The median overall survival (OS) was 20.4 months (95% CI: 15.2– 25.6). Cox univariate and multivariate analysis revealed better PS (0– 1), no distant lymph nodes metastasis (DLNM), simultaneous diagnosis of lung cancer and leptomeningeal metastasis (SDLL), and lower neutrophil to lymphocyte ratio (NLR), were associated with better OS. Based on these independent prognostic variables, a prognostic nomogram model with a C-index for OS prediction of 0.71, was constructed. The actual probability of survival at 1-, 2- and 3-year showed good concordance with the prediction curve of our nomogram.
Conclusion: The systematic immunological level was an independent prognostic factor of lung cancer patients with LM. The prognostic model based on statistical analysis had a good ability to predict the OS of patients.
Keywords: leptomeningeal metastases, lung cancer, prognosis, survival, nomogram model
Introduction
Lung cancer is a lethal disease affecting millions of people worldwide.1 Most patients are diagnosed at a late stage, losing the opportunity of surgery. For those who suffered from advanced non-small cell lung cancer (NSCLC), the prognosis is significantly improved with the advent of targeted therapy and immunotherapy.2,3 Leptomeningeal metastasis (LM), affecting 3–5% of patients, is considered a late-stage event. The outcome remains dismal in these patients,4,5 with a median overall survival (OS) of 3–11 months.6,7 Notably, with modern imaging technology, the incidence of LM has remarkably increased.8,9 There is increasing interest in the prognostic predictors of LM patients. Most reports focused on clinical characteristics (age, performance score, EGFR mutation, and extracranial metastasis), few studies investigated the influence of systematic inflammatory level.4,10–15
The systematic inflammatory reaction is a reflection of the immune response, which acts as the interface between the immune system and cancer. Accumulating evidence revealed the correlation between systematic immunity and cancer occurrence, evolution, and prognosis.16–19 However, it is hard to evaluate the status of systematic immunity comprehensively and precisely. Because the immune system is mainly composed of different types of immune cells and factors both locally and in circulation, measuring circulating immune cells such as lymphocytes, or neutrophils, is a simple and feasible way to reflect the local immunological response. Currently, few, if any, studies on the association between the prognosis of patients with LM and the systematic inflammatory level were reported. In this study, we explored the possible relationship between the prognosis of LM and the neutrophil to lymphocyte ratio (NLR), which stood as an indicator of systematic inflammatory reaction.
Patients and Methods
Patients
This retrospective, multi-institutional, observational study was conducted in 4 tertiary centers in China. Patients were screened through the Hospital Information System electronic files from January 2009 to May 2019. Patients with pathologically confirmed, metastatic lung cancer were screened. LM was defined as either abnormal leptomeningeal appearance on gadolinium-contrast magnetic resonance imaging (MRI) or positive cytology findings in cerebrospinal fluid (CSF).9,20 Suspected cases with only clinical symptoms or signs were excluded due to unreliable diagnosis.
Data Collection
Medical records of enrolled patients were reviewed. Retrieved data regarding demographic features, date of lung cancer and LM diagnosis, lung cancer histology and driver mutation status, treatment history, clinical outcomes and imaging examination results were collected.
We collected the data of complete blood count including white blood cell, platelet, neutrophil, lymphocyte, eosinophil, basophil, monocyte, and also biochemistry data including albumin, globulin, at the time of LM diagnosis. Here, neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), monocyte-to-lymphocyte ratio (MLR), albumin-to-globulin ratio (AGR) were calculated. The cut-off values of these factors were based on ROC analysis. All these baseline data were plotted for each patient (Figure 1).
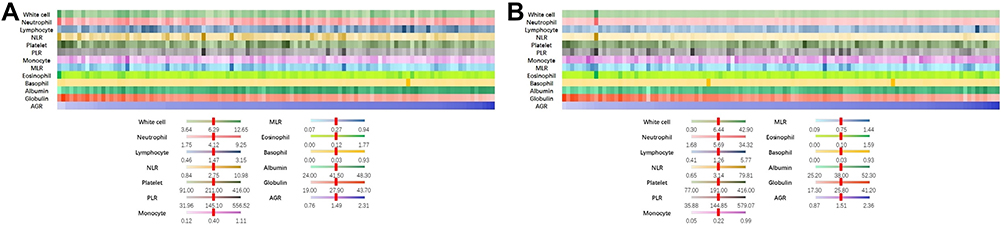 |
Figure 1 The distribution of circulating blood composition. (A) The distribution of circulating blood composition at the time of diagnosis of advanced lung cancer. (B) The distribution of circulating blood composition at the time of diagnosis of lung cancer with leptomeningeal metastases. Abbreviations: NLR, neutrophil to lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; MLR, monocyte-to-lymphocyte ratio; AGR, albumin-to-globulin ratio. |
Genetic Testing
Genetic testing was performed on tumor tissues. EGFR mutation or ALK rearrangement was detected in our domestic, College of American Pathologists-certified lab in West China Hospital. Tumor content was assessed by board-certified pathologists using hematoxylin and eosin staining. All specimens contained more than 10% of tumor content. DNA was extracted using the QIAamp DNA mini kit (Qiagen). In some patients, comprehensive genomic profiling was performed by Next Generation Sequencing (NGS) with 56 cancer-related gene panels covering the whole exons of the EGFR or ALK gene at a mean coverage depth of >800X. The genomic alterations including single base substitution, insertions/deletions, copy number variations, as well as gene rearrangement and fusions were assessed.
Outcome Measurement
The treatment response of LM was commonly evaluated based on Response Assessment in Neuro-Oncology (RANO) working group consensus.9,21 Due to the clinical application of the RANO criteria is complex, the evaluation is difficult to unify, and there is lack of objective criteria. To avoid the influence of these factors, this study used OS as only outcome, which was mostly objective. OS was defined as the period from the diagnosis of LM to death of any cause.
Statistical Analysis
All statistical analysis was performed on SPSS (ver. 25, IBM Inc, IL) and R software (ver. 3.6.1; http://www.Rproject.org). Chi-square test, Spearman, and Kendall’s tau-b test were used for correlation analysis. For analysis, continuous variables except for age were dichotomized into low or high-risk categories according to the cut-off values from receiver operating characteristic (ROC) analysis or the median value. The cut-off value of age was categorized according to a previous study, where the age < 60 years predicted a better survival.5,11 Univariate and multivariate analysis were used to identify independent variables that were associated with OS and construed a prognostic nomogram model. We also used a prognostic model named molecular graded prognostic assessment model (molGPA) constructed by three factors including PS, EGFR mutation, and extracranial lesions to analyze patients in this study. P < 0.05 upon two-sided testing was considered significant for all analyses.
Results
Demographic Characteristics
A total of 109 patients were enrolled from 4 referral centers. The demographic characteristics were listed in Table 1. The median age was 56 (range: 32–86). Most patients were female (61.5%), non-smokers (72.5%), relative fit (ECOG performance score, PS≤2, 81.7%), and had adenocarcinoma (96.3%). EGFR mutation (70.6%) was the most frequent driver mutation. And further analysis revealed a slightly higher frequency of L858R mutation (38.5%) than exon 19 deletion (31.2%). The median time to the onset of LM from the diagnosis of LC was 8.0 months (range: 0–83.0). The aberrant appearance was common in MRI imaging (89.9%) except in only 11 patients no signs were found, Cerebellum was the most commonly involved site. Most patients had neurological symptoms (66.1%). Patients were diagnosed either at the baseline (n=38, 34.9%) or during the treatment course. For the latter, most patients had sudden onset of LM, when their extra-cranial lesions were well controlled (55/71, 77.4%). In this study, patients received the following treatments: tyrosine kinase inhibitors (TKI) for EGFR or ALK, chemotherapy, and whole-brain radiotherapy.
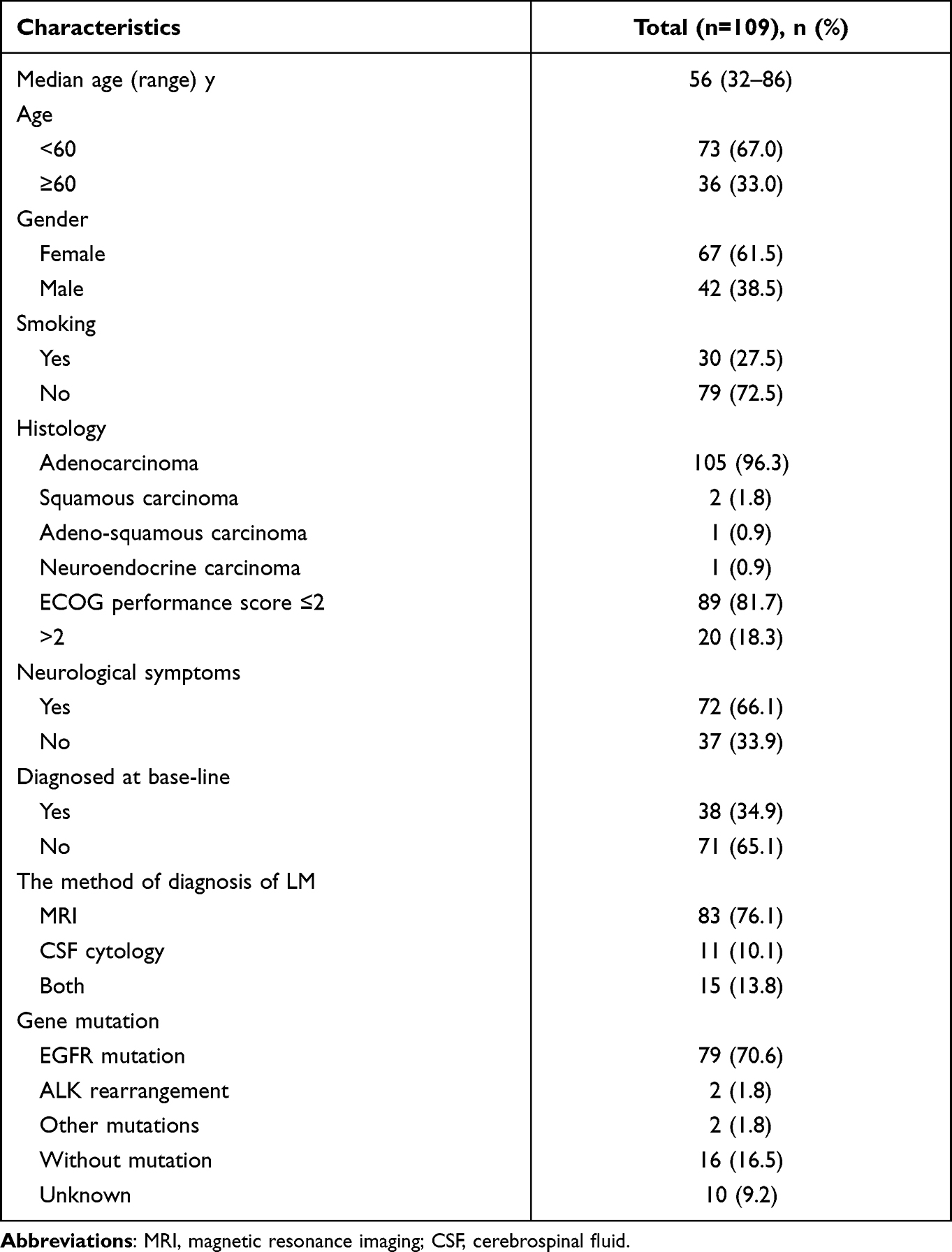 |
Table 1 Characteristics of the 109 Lung Cancer Patients with Leptomeningeal Metastasis |
Clinical and Genetic Features
Further analysis revealed this cohort of patients was enriched for patients aged 50–59 (n=46, 42.2%). Most patients were neither very old nor very young (age 40–79, n=103, 94.5%, Figure 2A). Patients were prone to multiple metastases. The most common metastatic site was bone, followed by the lung, brain, pleural, adrenal gland, and liver. (Figure 2B). The time from the onset of lung cancer to the occurrence of metastases (Time 1) was positively associated with the time from metastases to LM development (Time 2) (relative score=0.16, P=0.033), while the latter was inversely associated with the survival after the diagnosis of LM (relative score=−0.20, P=0.003, Figure 2C). This study also tried to explore possible genetic aberrations associated with LM. At this time, 16 patients had the NGS data of the primary tumors. We compared the data with those from 36 advanced lung cancer patients harboring EGFR mutation without LM. Commonly involved genes were TP53 and CDK4, etc. No significant difference in genetic aberrations between groups was observed (Figure 3).
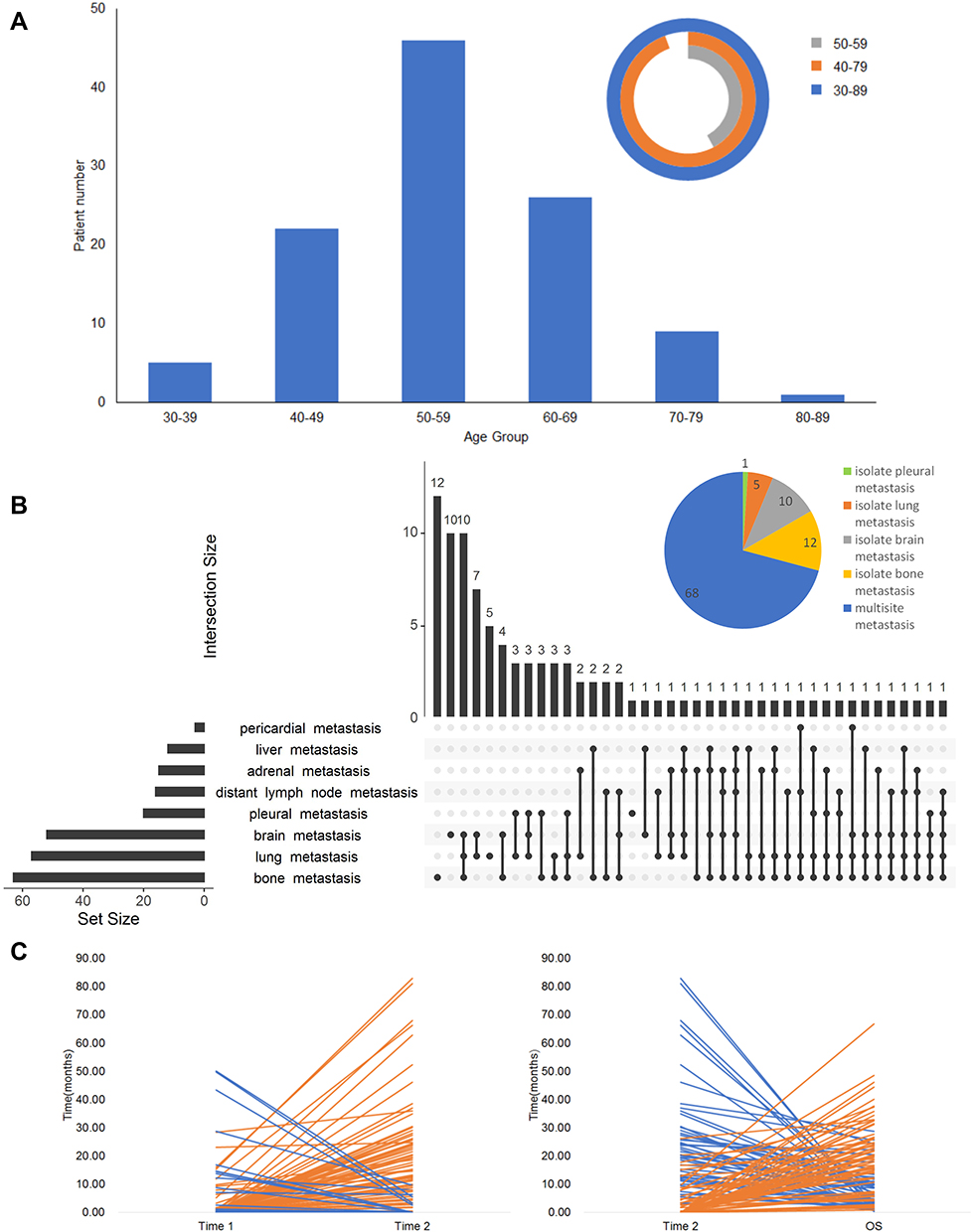 |
Figure 2 Clinical features of patients. (A) The distribution of age when patient diagnosed as leptomeningeal metastases. (B) The distribution of common metastatic sites. (C) The time from the initiation of metastases to the involvement of leptomeningeal metastases (Time 2) was related positively to the time from the onset of lung cancer to the metastases (Time 1), while negatively to the survival after leptomeningeal metastases. |
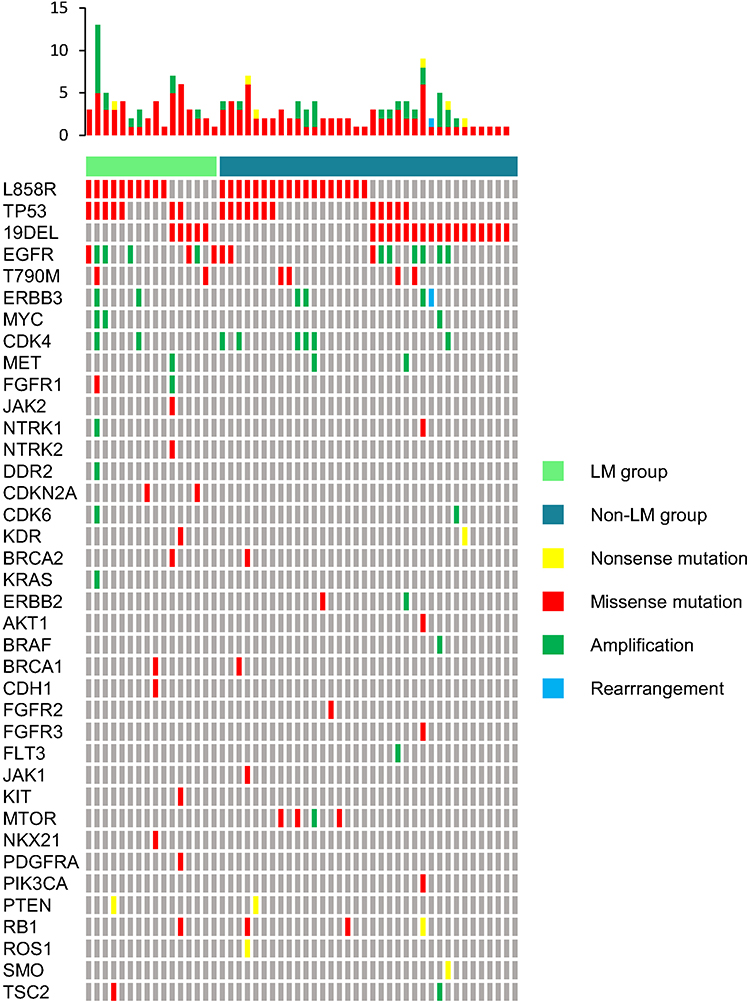 |
Figure 3 The comparison of genetic aberrations of 16 leptomeningeal metastases patients with EGFR mutation and 36 similar advanced lung cancer patients harboring EGFR mutation without leptomeningeal metastases. Abbreviation: LM, leptomeningeal metastasis. |
Prognostic Factors
The median OS of our patients was 20.4 months (95% CI: 15.2–25.6), and the median follow-up was 35.73 months (95% CI: 22.67–48.80, Figure 4). Here we found PS, distant lymph node metastasis (DLMN), simultaneous diagnosis of lung cancer, and leptomeningeal metastasis (SDLL), were related to survival. Also, NLR, MLR, PLR were related to poor prognosis. Neither chemotherapy (p=0.091), or TKI (p=0.392), or whole brain radiotherapy (WBRT) (p=0.592) was statistically associated with survival. Osimertinib is believed to improve the control of intracranial lesions, but in our patients receiving osimertinib (n=33), no survival benefit was observed (p=0.444) compared with those receiving other EGFR TKI (n=41).
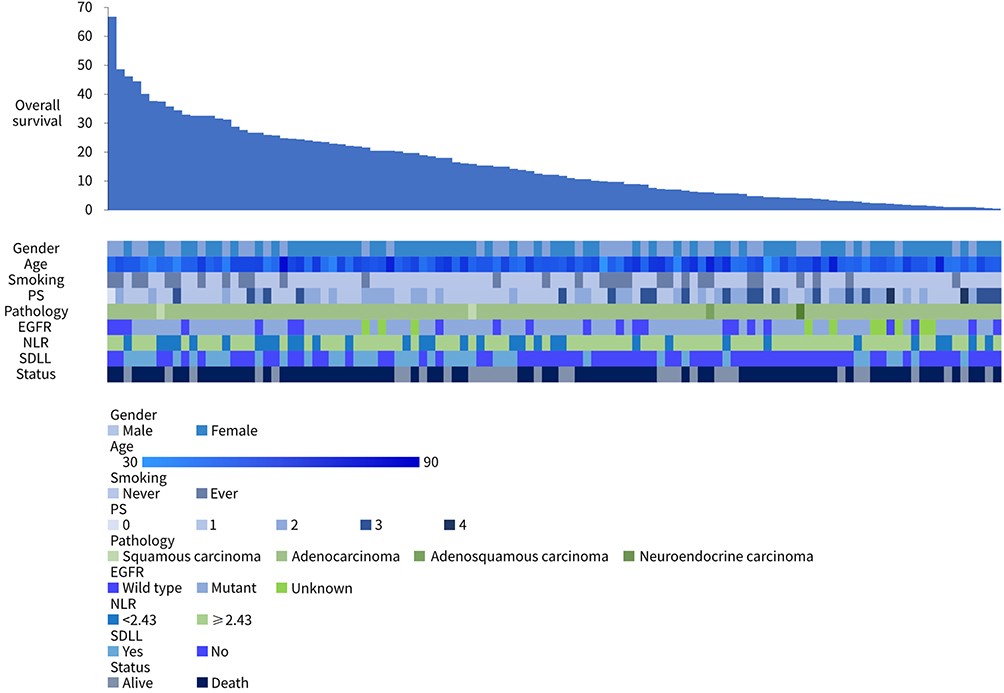 |
Figure 4 Summary of patients’ survival and the association between survival and clinical features including gender, age, smoking, PS, pathology, EGFR, NLR, and SDLL. Abbreviations: NLR, neutrophil to lymphocyte ratio; SDLL, simultaneous diagnosis of lung cancer and leptomeningeal metastasis. |
Cox Regression Model
Here both univariate and multivariate analyses were performed. In univariate analysis, NLR, PLR, MLR, PS, DLNM, and SDLL were significantly associated with survival (Figure 5). In multivariate analysis, NLR remained an independent survival factor, together with PS, DLNM, SDLL (Figure 6A).
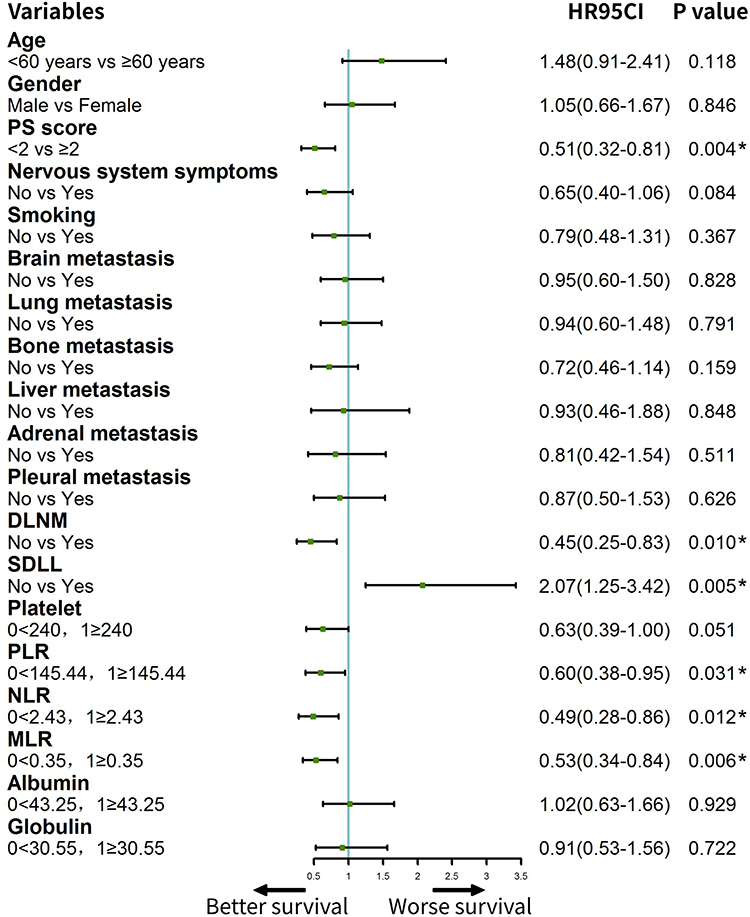 |
Figure 5 The forest plot for cox univariate analysis. In univariate analysis, NLR, PLR, MLR, PS, DLNM, and SDLL were significantly associated with overall survival. Abbreviations: NLR, neutrophil to lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; MLR, monocyte-to-lymphocyte ratio; DLNM, distant lymph nodes metastasis; SDLL, simultaneous diagnosis of lung cancer and leptomeningeal metastasis. Note: *Demonstrated that variables were significantly associated with overall survival. |
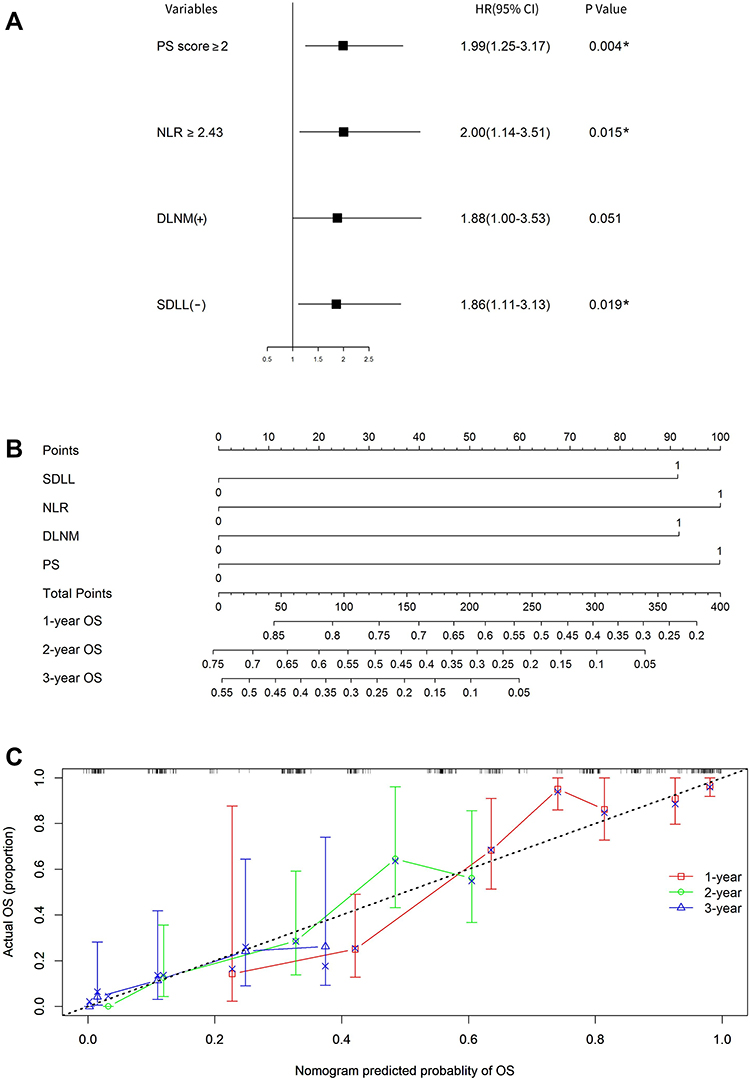 |
Figure 6 The independent prognostic factors and nomogram model for leptomeningeal metastasis. (A) Multivariate analysis showed NLR together with PS, DLNM, and SDLL were independent survival factor for leptomeningeal metastasis. (B) Establishment of a nomogram to predict the likelihood of 1-, 2- and 3-year survival. To use the nomogram, the value attributed to an individual patient is located on each variable axis, and a line is drawn upwards to determine the number of points received for each variable value. The sum of these numbers is located on the total points axis, and a line is drawn downward to the survival axis to determine the likelihood of 1-, 2- and 3-year survival. The 0 and 1 values of SDLL represented yes and no, respectively. The 0 and 1 values of NLR represented < 240 and ≥ 240, respectively. The 0 and 1 values of DLNM represented no and yes, respectively. The 0 and 1 values of PS represented < 2 and ≥ 2, respectively. (C) the calibration curve for OS at 1-, 2- and 3-year. Abbreviations: NLR, neutrophil to lymphocyte ratio; DLNM, distant lymph nodes metastasis; SDLL, simultaneous diagnosis of lung cancer and leptomeningeal metastasis; OS, overall survival. Note: *Demonstrated that variables were significantly associated with overall survival. |
Nomogram Establishment and Validation
Based on the previous Cox model, four variates (PS, NLR, DLNM, and SDLL) were integrated into the nomogram to predict the 1-, 2, 3-year OS (Figure 6B). The concordance index (C-index) for OS prediction was 0.71. The calibration plot for the probability of survival at 1, 2, and 3 years after diagnosis of LM showed a good correlation between the prediction by nomogram and actual observation (Figure 6C).
The Prognostic Performance of molGPA
We exploratively analyzed the predictive value of the molGPA model for the prognosis of 99 evaluable patients, and finally concluded that only patients in the high-risk group (0 points, 6 patients) and low-risk groups (1.5–2 points, 48 patients) had significant difference in OS (4.8 months vs 22.67 months, P=0.003). There was no statistically difference in overall survival between the high- and intermediate-risk groups (0.5 −1 points, 45 patients), the intermediate- and low-risk groups. Notably, the intermediate-risk group was numerically superior to the high-risk group (17.97 months vs 4.8 months) in OS, and the low-risk group was better than the intermediate-risk group (22.67 months vs 17.97 months) in OS.
Discussion
Lung cancer has the highest incidence and mortality among all malignancies.1 Its prognosis is improved with novel treatments, but those with leptomeningeal involvement still had poor life expectance.9,22 It is critical to screen the patients with a high risk of leptomeningeal metastases. Previous studies indicated patients with adenocarcinoma, with EGFR mutation, esp. L858R point mutation might be highly susceptible to this complication.11,12 Our cohort of LM patients also have high proportion of these patients. And we further found patients at their age of 50–59, with either bone, brain, or lung metastases were enriched in this cohort. Our results argued the clinical features of leptomeningeal metastases were unique.
Our study comprehensively evaluated the prognostic factors of these patients, both from clinical aspects and laboratory parameters. Our results showed better PS (0–1), no DLNM, SDLL, and lower NLR, were associated with better OS. Based on these variables, an integrated nomogram was constructed, with a C-index for OS prediction of 0.71. The actual probability of survival at 1-, 2- and 3-year showed good concordance with the prediction curve of our nomogram. The nomogram further supported the prognostic value of these factors.
Different prognostic factors of lung cancer with LM were proposed in previous reports, including age, gender, EGFR status, PS score, systematic metastasis, and TKI treatment4,10–13,21,23–26 (Figure 7). We tested these factors in our cohort, but most failed to be validated to be prognostic. On the other hand, our findings of DLNM, SDLL, PS were supported by most reports. We believe the seemingly discordant results might be due to the heterogeneity of these patients in different studies.
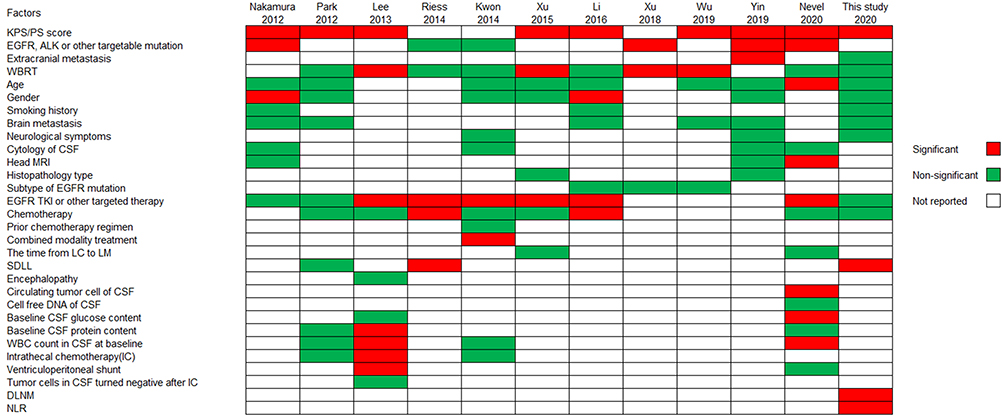 |
Figure 7 Summary of prognostic factors of leptomeningeal metastases in literature and this study. Abbreviations: WBRT, whole brain radiation therapy; CSF, cerebrospinal fluid; MRI, magnetic resonance imaging; TKI, tyrosine kinase inhibitors; LC, lung cancer; LM, leptomeningeal metastasis; SDLL, simultaneous diagnosis of lung cancer and leptomeningeal metastasis; DLNM, distant lymph nodes metastasis; NLR, neutrophil to lymphocyte ratio. |
Besides our prognostic model, other models were suggested before. One model was constructed according to PS, neurological deficits, systemic disease, and encephalopathy differentiate patients to good or poor prognosis. Three factors including PS, EGFR mutation, and extracranial lesions were included in another model, the molecular graded prognostic assessment model, namely the molGPA model.10 We analyzed our cohort by using this model, but with unsatisfactory prognosis discriminating capability. This might be due to the limited patient number, but it also argued the application of this model would not be universal. Compared with the above models, our nomogram model was based on laboratory results besides clinical characteristics and might be comprehensive.
Our study revealed the systemic inflammatory status significantly influenced the survival of patients with leptomeningeal metastases. Circulating neutrophils, lymphocytes were components of system immunity. Not surprisingly, circulating hematological compositions such as NLR were related to the occurrence, progression, and prognosis of many tumors.16,27–30 Our finding was interesting because whether the onset of leptomeningeal metastases was related to immunity remained unknown, and our results provided clues to this problem. Recently, two clinical trial where immune checkpoint inhibitors were used to treat lung cancer patients with LM were reported.31,32 The results of two trials both suggested some patients with LM do benefit from immune checkpoint inhibitors treatment. This supported the notion that the immune system may play a role in the control of LM. These trials, together with our results, supported the immunological aspect of leptomeningeal metastases.
This study had its limitations. Firstly, due to the nature of the retrospective study, the bias was almost inevitable. Secondly, although we performed a multi-center study, the sample size was still limited. Also, the genetic aberrations were only available for a few patients. Thus, the conclusion of our results should be interpreted with caution, and prospective large sample-sized studies are urgently needed for leptomeningeal metastases.
In summary, our study suggested a high-risk population might be susceptible to leptomeningeal metastases. Good PS, no DLNM, SDLL, and lower NLR were significantly associated with better OS. Our study may contribute to the identification and management of leptomeningeal metastases in the clinic.
Data Sharing Statement
All data analyzed during this study are included in this published article.
Ethical Statement
This retrospective study was approved by the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University (2021年审(1076) 号). The requirement for written informed consent was waived by the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University. The study was performed in accordance with the ethical standards of the Declaration of Helsinki (1964) and its subsequent amendments.
Author Contributions
ZYD, PD, and LH designed the research. YH, QL, YYC, and PPW collected and analyzed data. YH, YF, and TL wrote and revised the manuscript. All authors contributed to data analysis, drafting or revising the article, agreed on the journal to which the article has been submitted, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding
No funding or sponsors involved.
Disclosure
All authors declared no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68(6):394–424. doi:10.3322/caac.21492
2. Yoneda K, Imanishi N, Ichiki Y, Tanaka F. Treatment of non-small cell lung cancer with EGFR-mutations. J Univ Occup Environ Health. 2019;41(2):153–163. doi:10.7888/juoeh.41.153
3. Pacheco JM, Camidge DR, Doebele RC, Schenk E. A changing of the guard: immune checkpoint inhibitors with and without chemotherapy as first line treatment for metastatic non-small cell lung cancer. Front Oncol. 2019;9:195. doi:10.3389/fonc.2019.00195
4. Park JH, Kim YJ, Lee J-O, et al. Clinical outcomes of leptomeningeal metastasis in patients with non-small cell lung cancer in the modern chemotherapy era. Lung Cancer. 2012;76(3):387–392. doi:10.1016/j.lungcan.2011.11.022
5. Kuiper JL, Hendriks LE, van der Wekken AJ, et al. Treatment and survival of patients with EGFR-mutated non-small cell lung cancer and leptomeningeal metastasis: a retrospective cohort analysis. Lung Cancer. 2015;89(3):255–261. doi:10.1016/j.lungcan.2015.05.023
6. Liao BC, Lee JH, Lin CC, et al. Epidermal growth factor receptor tyrosine kinase inhibitors for non-small-cell lung cancer patients with leptomeningeal carcinomatosis. J Thorac Oncol. 2015;10(12):1754–1761. doi:10.1097/JTO.0000000000000669
7. Umemura S, Tsubouchi K, Yoshioka H, et al. Clinical outcome in patients with leptomeningeal metastasis from non-small cell lung cancer: Okayama lung cancer study group. Lung Cancer. 2012;77(1):134–139. doi:10.1016/j.lungcan.2012.03.002
8. Remon J, Le Rhun E, Besse B. Leptomeningeal carcinomatosis in non-small cell lung cancer patients: a continuing challenge in the personalized treatment era. Cancer Treat Rev. 2017;53:128–137. doi:10.1016/j.ctrv.2016.12.006
9. Cheng H, Perez-Soler R. Leptomeningeal metastases in non-small-cell lung cancer. Lancet Oncol. 2018;19(1):e43–e55. doi:10.1016/S1470-2045(17)30689-7
10. Yin K, Li Y-S, Zheng -M-M, et al. A molecular graded prognostic assessment (molGPA) model specific for estimating survival in lung cancer patients with leptomeningeal metastases. Lung Cancer. 2019;131:134–138. doi:10.1016/j.lungcan.2019.03.015
11. Nakamura Y, Takahashi T, Tsuya A, et al. Prognostic factors and clinical outcome of patients with lung adenocarcinoma with carcinomatous meningitis. Anticancer Res. 2012;32(5):1811–1816.
12. Wu YL, Zhao Q, Deng L, et al. Leptomeningeal metastasis after effective first-generation EGFR TKI treatment of advanced non-small cell lung cancer. Lung Cancer. 2019;127:1–5. doi:10.1016/j.lungcan.2018.11.022
13. Xu Q, Chen X, Qian D, et al. Treatment and prognostic analysis of patients with leptomeningeal metastases from non-small cell lung cancer. Thorac Cancer. 2015;6(4):407–412. doi:10.1111/1759-7714.12188
14. Clarke JL, Perez HR, Jacks LM, Panageas KS, Deangelis LM. Leptomeningeal metastases in the MRI era. Neurology. 2010;74(18):1449–1454. doi:10.1212/WNL.0b013e3181dc1a69
15. Waki F, Ando M, Takashima A, et al. Prognostic factors and clinical outcomes in patients with leptomeningeal metastasis from solid tumors. J Neurooncol. 2009;93(2):205–212. doi:10.1007/s11060-008-9758-3
16. Schreiber RD, Old LJ, Smyth MJ. Cancer immunoediting: integrating immunity’s roles in cancer suppression and promotion. Science. 2011;331(6024):1565–1570.
17. Shankaran V, Ikeda H, Bruce AT, White JM, Swanson PE, Old LJ. IFNgamma and lymphocytes prevent primary tumour development and shape tumour immunogenicity. Nature. 2001;410(6832):1107–1111. doi:10.1038/35074122
18. Tan TT, Coussens LM. Humoral immunity, inflammation and cancer. Curr Opin Immunol. 2007;19(2):209–216. doi:10.1016/j.coi.2007.01.001
19. Mapara MY, Sykes M. Tolerance and cancer: mechanisms of tumor evasion and strategies for breaking tolerance. J Clin Oncol. 2004;22(6):1136–1151. doi:10.1200/JCO.2004.10.041
20. Grossman SA, Krabak MJ. Leptomeningeal carcinomatosis. Cancer Treat Rev. 1999;25(2):103–119. doi:10.1053/ctrv.1999.0119
21. Xu Y, Hu M, Zhang M, et al. Prospective study revealed prognostic significance of responses in leptomeningeal metastasis and clinical value of cerebrospinal fluid-based liquid biopsy. Lung Cancer. 2018;125:142–149. doi:10.1016/j.lungcan.2018.08.017
22. Herbst RS, Morgensztern D, Boshoff C. The biology and management of non-small cell lung cancer. Nature. 2018;553(7689):446–454. doi:10.1038/nature25183
23. Li Y-S, Jiang B-Y, Yang -J-J, et al. Leptomeningeal metastases in patients with NSCLC with EGFR mutations. J Thorac Oncol. 2016;11(11):1962–1969. doi:10.1016/j.jtho.2016.06.029
24. Riess JW, Nagpal S, Iv M, et al. Prolonged survival of patients with non-small-cell lung cancer with leptomeningeal carcinomatosis in the modern treatment era. Clin Lung Cancer. 2014;15(3):202–206. doi:10.1016/j.cllc.2013.12.009
25. Nevel KS, DiStefano N, Lin X, et al. A retrospective, quantitative assessment of disease burden in patients with leptomeningeal metastases from non-small-cell lung cancer. Neuro Oncol. 2020;22(5):675–683. doi:10.1093/neuonc/noz208
26. Kwon J, Chie EK, Kim K, et al. Impact of multimodality approach for patients with leptomeningeal metastases from solid tumors. J Korean Med Sci. 2014;29(8):1094–1101. doi:10.3346/jkms.2014.29.8.1094
27. Bottazzi B, Riboli E, Mantovani A. Aging, inflammation and cancer. Semin Immunol. 2018;40:74–82. doi:10.1016/j.smim.2018.10.011
28. Shinko D, Diakos CI, Clarke SJ, Charles KA. Cancer-related systemic inflammation: the challenges and therapeutic opportunities for personalized medicine. Clin Pharmacol Ther. 2017;102(4):599–610. doi:10.1002/cpt.789
29. Silva TH, Schilithz AOC, Peres WAF, Murad LB. Neutrophil-lymphocyte ratio and nutritional status are clinically useful in predicting prognosis in colorectal cancer patients. Nutr Cancer. 2020;72(8):1345–1354. doi:10.1080/01635581.2019.1679198
30. Diem S, Schmid S, Krapf M, et al. Neutrophil-to-Lymphocyte ratio (NLR) and Platelet-to-Lymphocyte ratio (PLR) as prognostic markers in patients with non-small cell lung cancer (NSCLC) treated with nivolumab. Lung Cancer. 2017;111:176–181. doi:10.1016/j.lungcan.2017.07.024
31. Hendriks LEL, Bootsma G, Mourlanette J, et al. Survival of patients with non-small cell lung cancer having leptomeningeal metastases treated with immune checkpoint inhibitors. Eur J Cancer. 2019;116:182–189. doi:10.1016/j.ejca.2019.05.019
32. Zheng MM, Tu HY, Yang JJ, et al. Clinical outcomes of non-small cell lung cancer patients with leptomeningeal metastases after immune checkpoint inhibitor treatments. Eur J Cancer. 2021;150:23–30. doi:10.1016/j.ejca.2021.03.037
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.