")
Back to Journals » Drug Design, Development and Therapy » Volume 16
Synergistic Effect of Combined Sub-Tenon Triamcinolone and Intravitreal Anti-VEGF Therapy for Uveitic Macular Edema
Authors Lin D , Hu J, Wu K, Feng K, Zhao X, Lu Q, Ren M, Cao J, Liu R, Dai M, Nan K, Wang Y
Received 16 December 2021
Accepted for publication 26 March 2022
Published 8 April 2022 Volume 2022:16 Pages 1055—1066
DOI https://doi.org/10.2147/DDDT.S353251
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Dan Lin,1,* Jiajiang Hu,2,* Ke Wu,1 Kemi Feng,1 Xia Zhao,1 Qingqing Lu,3 Mingxue Ren,1 Junlin Cao,1 Ruru Liu,1 Mali Dai,1 Kaihui Nan,1 Yuqin Wang1
1The Eye Hospital, School of Ophthalmology & Optometry, Wenzhou Medical University, Wenzhou, People’s Republic of China; 2Department of Ophthalmology, Shaoxing Central Hospital, Shaoxing, People’s Republic of China; 3Department of Ophthalmology, Qingpu Branch of Zhongshan Hospital Affiliated to Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kaihui Nan; Yuqin Wang, The Eye Hospital, School of Ophthalmology & Optometry, Wenzhou Medical University, Wenzhou, 325027, People’s Republic of China, Email [email protected]; [email protected]
Purpose: To investigate effects of intravitreal anti-VEGF in combination therapy with sub-Tenon triamcinolone acetonide (STA) injection for uveitic macular edema (UME).
Design: A single-center, retrospective cohort study.
Methods: The medical records were obtained for 65 eyes of 65 patients with UME. Of which, 32 eyes received combined anti-VEGF with STA injection, and 33 eyes received 40 mg of STA injection alone. The primary outcome was the reduction of central macular thickness (CMT) measured with optical coherence tomography (OCT). Resolution rate of clinical UME and changes of best corrected visual acuity (BCVA) over 24 weeks were secondary outcomes.
Results: There was a significantly greater reduction of CMT with the combination treatment than with STA alone at 1-week (β = − 157.9, P < 0.001) and 1-month (β = − 53.1, P = 0.019) after injection. The cumulative incidence of macular edema resolution of all eyes was 87.7%, with 90.6% (29/32) in the combined group and 84.8% (28/33) in the STA group, respectively. More incidence of UME resolution was observed in the combined group than the STA group after 1 week (71.9% vs 15.2%, P < 0.001) and 4 weeks (84.4% vs 54.5%, P = 0.009), respectively. BCVA was better for the combination treatment than STA alone at 1-week (β = − 0.085, P = 0.070) and 1-month (β = − 0.108, P = 0.019) after injection, respectively. Increased intraocular pressure (> 25 mmHg) was observed in 4 eyes (12.5%) in the combined group and 5 eyes (15.2%) in the STA group, respectively.
Conclusion: Combined intravitreal anti-VEGF and STA is superior to STA alone for reduction of UME and visual restoration. Addition of anti-VEGF did not increase risk for steroid-induced elevation of intraocular pressure over 6 months.
Keywords: uveitic macular edema, local combination therapy, sub-Tenon triamcinolone acetonide, intravitreal anti-VEGF
Introduction
Uveitis refers to inflammation of the uveal tract in the eye, and is the major cause of blindness. Approximately, 35% of patients with uveitis exhibit blindness or visual impairment.1 Visual loss in uveitis affects people predominantly of working age. It has been reported that uveitis accounts for 10% of blindness2 and up to 25% of cases in developing countries,3 which causes a serious socioeconomic burden.
Macular edema, cataract formation, and secondary glaucoma are the leading complications of uveitis. The prevalence of uveitic macular edema (UME) varies from 20% to 70%.4 Macular edema can cause permanent structural central retinal damage if left untreated. Therefore, effectively resolving UME is critical for preserving visual acuity of these patients. Despite the existence of severe side effects, glucocorticoids still act as the mainstay treatment for UME and are administered systemically or locally. Systemic treatments bear significant side effects and some patients suffer macular edema even with their uveitis under control.5,6 These challenges prompt physicians to explore local ocular medications as an adjuvant. Intravitreal or sub-Tenon triamcinolone acetonide (STA) is a common adjuvant treatment for UME. Recently, intravitreal anti-vascular endothelial growth factor (aVEGF) biologics have emerged as another adjuvant treatment for UME.7,8 Currently available aVEGF agents may not be suitable as a single treatment option due to the need for frequent injections.
Theoretically, over-expression of VEGF is mutually associated with inflammation in pathology,9 and such a correlation has been observed in retinal diseases.10 A few studies have focused on VEGF levels in uveitic eyes,11,12 while others have profiled inflammatory cytokines.13,14 These studies demonstrate that breakdown of the blood-retina barrier (BRB) is not only due to pro-inflammatory cytokines, but also related to increase VEGF levels. It is well recognized that steroids have strong anti-inflammatory effects but weak anti-angiogenesis effects. On the other hand, aVEGF possesses extremely weak anti-inflammatory effects.15,16 Clinical studies have shown that intravitreal administration of steroids is more effective than periocular administration in UME treatment due to the higher drug concentration.17–19 However, intravitreal steroids pose significantly higher risks, including steroid-induced cataracts and glaucoma. In previous studies, combination therapy of intravitreal aVEGF with local sustained release steroids reduced the number of additional aVEGF injections and increased visual acuity in macular edema secondary to retinal diseases such as retinal vein occlusion and diabetic macular edema.20–23 We hypothesize that a combination of STA and aVEGF therapy would benefit patients more than either therapy alone and have a synergistic effect on UME.
To verify our hypothesis, we reviewed patients with UME treated with one injection of either a combination of STA with aVEGF or traditional STA only to evaluate the effects of combined STA and aVEGF therapy in the reduction of CMT and improvement of visual acuity.
Methods
Study Population
This single-site, retrospective cohort study was conducted at the Eye Hospital of Wenzhou Medical University. Patient charts were reviewed for cases of noninfectious uveitis that were complicated by macular edema and underwent STA injection alone or combined STA with aVEGF injection between May 2013 and January 2020. Posterior sub-Tenon injection of 40 mg triamcinolone acetonide (TA) was administered for all patients using a triport cannula as previously described.24 Combined treatment cases received one of three aVEGF agents (Ranibizumab 0.5 mg, Conbercept 0.5 mg, or Bevacizumab 1.25 mg) before injection of STA. Patients meeting the following criteria at baseline were included: 1) age greater than 18 years and less than 75 years; 2) presenting with noninfectious anterior, intermediate, posterior, or panuveitis; 3) with macular edema secondary to uveitis, defined as central macular thickness (CMT) greater than 300 µm confirmed by optical coherence tomography (OCT) with intraretinal cysts and/or subretinal fluid; 4) no history of local steroid (besides of topical steroid and non-steroid anti-inflammatory drugs) therapy within the last 6 months; and 5) baseline intraocular pressure (IOP) less than 21 mmHg. Patients with macular edema caused by other diseases such as diabetic retinopathy, retinal vein occlusion, and pseudophakic macular edema were excluded. Patients with any intraocular surgery such as cataract surgery, anti-glaucoma surgery, and pars plana vitrectomy within 6 months were excluded. Patients who were pregnant or breastfeeding were also excluded. This study adhered to the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of the Eye Hospital, Wenzhou Medical University. This study was approved with waiver of informed consent by the ethic committee, since it was a retrospective study, did not involve any direct patient contact, collection of any identifiable patient information, or adversely affect the rights and health of the patients.
Data Collection
Information such as sex, age, type of uveitis, diagnosis, history of treatment, and surgical history were obtained during the initial visit. Best corrected visual acuity (BCVA) by the Chinese standard logarithm visual chart, IOP by a non-contact tonometer, slit-lamp examinations of the anterior segment and macular area, indirect ophthalmoscopy after pupil dilation, and SD-OCT (Heidelberg, Germany) for macular retina were collected at every clinic visit. Classification of uveitis and grading of inflammation were based on the Standardization of Uveitis Nomenclature criteria.25 Details of systemic and local medications in use at every clinic visit were also recorded.
Patients were divided into two treatment groups, STA group (STA injection alone) and combined group (combined injection of aVEGF and STA). In the combined group, all patients received a prior injection of aVEGF no more than 20 days before STA injection. Sequential administration of aVEGF and STA in the combined group was performed under the consideration of reducing risk of infection since steroid use can compromise local immunity. For patients with UME in both eyes, the more severe eye was included in the study. Resolution of UME was defined as normalization of macular thickness and no cysts present on OCT. To keep the same release step of TA, we started the counting days after STA injection in both groups.
Statistical Analysis
Statistical analysis of baseline parameters was performed as follows: Student’s t-test was used for normally distributed continuous variables, Mann–Whitney U-test was used for skewed distributed continuous variables, and Pearson chi-square test or Fisher’s exact test was used for discrete variables. Visual acuities were converted to logMAR (logarithm of the minimal angle of resolution) scale. To evaluate the factors associated with CMT reduction or improvement of BCVA (logMAR) at each follow-up time point, simple linear regression analysis was conducted. To assess independently associated factors, variables with a P-value less than 0.1 in the simple linear regression models and variables of treatment groups were submitted to multiple linear regression analysis. All statistical analyses were performed using SPSS software for Windows (Version 19.0; SPSS, Inc., Chicago, IL, USA). P-value <0.05 was considered statistically significant.
Results
Baseline Characteristics
Totally, 65 eyes of 65 patients including 27 men and 38 women were enrolled in this study. The baseline characteristics of treatment groups are summarized in Table 1. Of which, 11 eyes had acute anterior uveitis (five were ankylosing spondylitis related, two were HLA-B27 associated, and four were idiopathic), six eyes had intermediate uveitis, eighteen eyes had idiopathic retinal vasculitis, 12 eyes had idiopathic panuveitis, nine eyes had Behcet’s disease with panuveitis, six eyes had recurrent Vogt-Koyanagi-Harada disease, one eye had chorioretinitis, one eye had sarcoidosis-associated uveitis, and one eye had Fuchs uveitis. Five eyes received Bevacizumab 1.25 mg, 14 eyes received Ranibizumab 0.5 mg, and 13 eyes received Conbercept 0.5 mg in combined group. At baseline, totally 14 patients received systemic therapy. Two patients in combined group (n = 6) received steroids therapy only, one patient in STA group (n = 8) only received cyclosporine A therapy, and one patient with ankylosing spondylitis in STA group (n = 8) only received golimumab therapy. Other 10 patients in both groups received both steroids and immunosuppressive drugs (including cyclosporine A, azathioprine) except for one patient with Behcet’s disease in STA group received both adalimumab, steroids, cyclosporine A and acetazolamide. One patient with Vogt-Koyanagi-Harada disease in the STA group had undergone laser peripheral iridectomy about 7 months ago. Baseline characteristics including age, gender, type of uveitis, lens status, macular edema characteristics, grading of anterior chamber inflammatory cells, BCVA (logMAR), CMT, and IOP were well balanced between the two treatment groups. Injection status was not balanced: patients in the STA group were more likely to be received their first local injection of TA (57.6% of eyes) than those in the combined group (28.1% of eyes) (P = 0.024). One patient with ocular hypertension in STA group received oral methazolamide for totally 8 days from the day of STA injection.
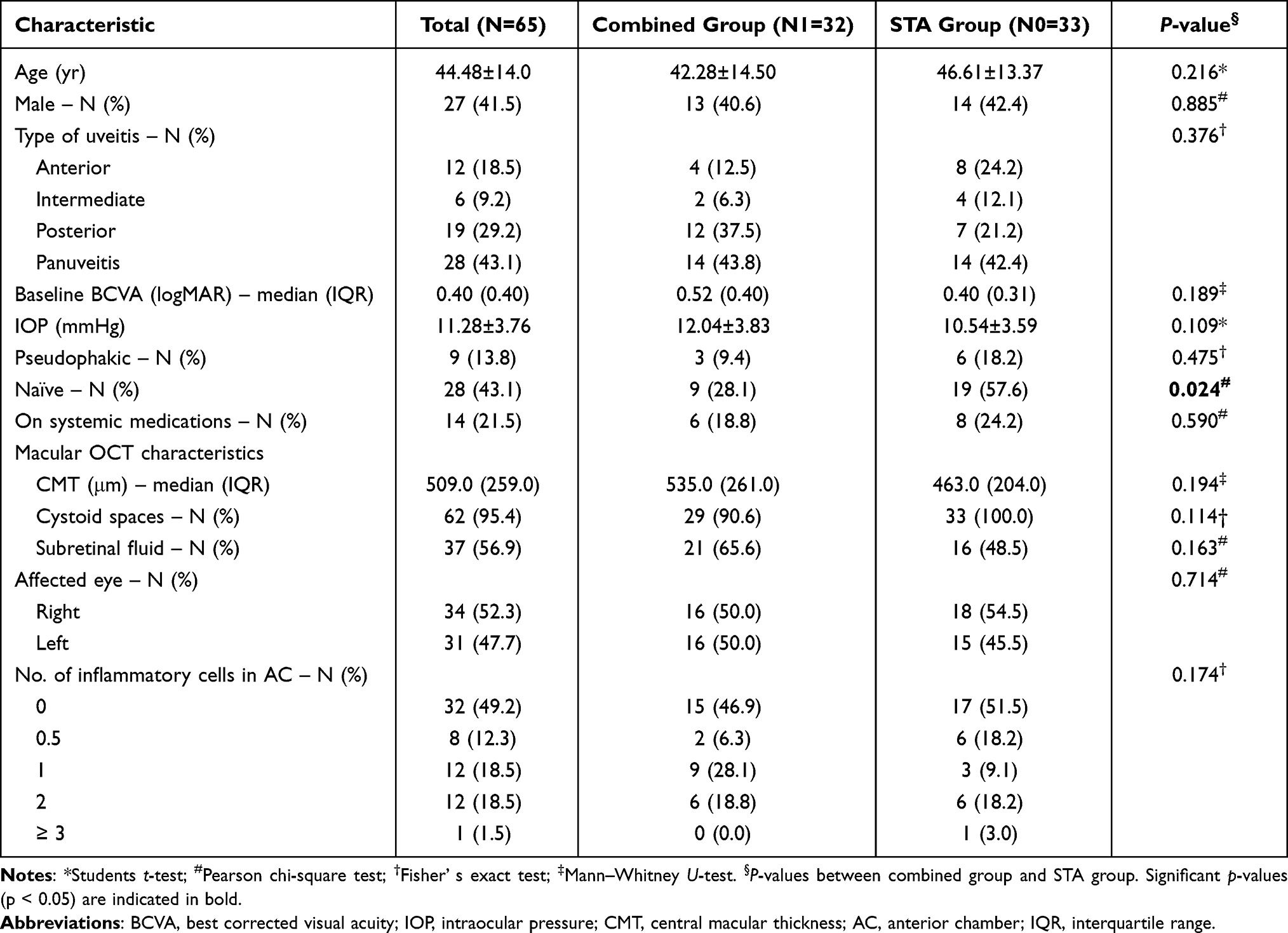 |
Table 1 Demographic and Clinical Characteristics at Baseline of Two Treatment Groups |
During the follow-up period, one patient in combined group received oral methazolamide for totally 10 days because of corticosteroid-induced ocular hypertension at 18 days after STA injection when his macular edema has already been resolved. No other patients received dorzolamide eye drops, oral diamox or methazolamide.
Reduction of Central Macular Thickness
The reduction of CMT from baseline (ΔCMT) was compared between the two treatment groups at each follow-up time point while adjusting for covariates such as baseline CMT, age, type of uveitis, lens status, injection status, systemic medication usage and UME types (Table 2). Overall, CMT improved at all follow-up visits compared with baseline for both treatment groups after one injection (Figure 1). The reduction of CMT was significantly greater (β = −157.9, P < 0.001) in the combined group (median [IQR], −288.5 [272] µm) than in the STA group (−110.0 [148] µm) at 1 week after adjusting for injection status, systemic medication usage, and baseline CMT. The same trend was observed at the 4-week visit compared after adjusting for systemic medication usage, UME type, and baseline CMT (β = −53.1, P = 0.019). The median ΔCMT (IQR) was −291.5 (235.0) µm in the combined group, and −196.0 (222.0) µm in the STA group at 4 weeks. However, by the later time-point, the strategy of combined therapy became less effective. At 12 weeks post-injection, the median decrease of CMT from baseline was −221.5 (IQR, 281) µm in the combined group and −221.0 (IQR, 246) µm in the STA group. Their difference after adjusting for baseline CMT was no longer statistically significant (β = 21.1, P = 0.475). The reduction of CMT from baseline to week 24 did not differ significantly between groups (β = −8.5, P = 0.597). Data for one outlier with a ΔCMT value of 1165 µm in the STA group was removed from the linear regression model at 12 weeks and 24 weeks, which did not affect the conclusions drawn from the results. Baseline CMT was a strong significant predictor that was negatively associated with reduction of CMT (P < 0.001) at all visits, while no other independent risk factor for ΔCMT was found in the multiple linear regression analysis.
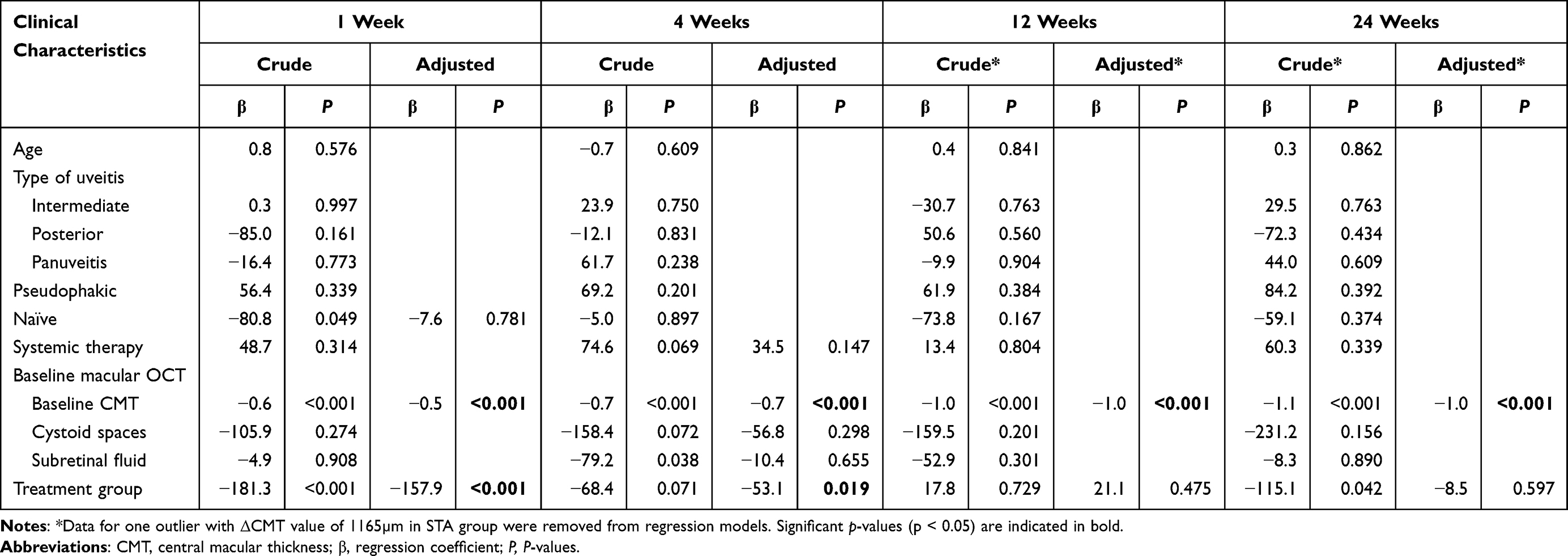 |
Table 2 Multivariable Linear Regression to Compare CMT Reduction at Each Visit Between Two Treatment Groups |
 |
Figure 1 Reduction of central macular thickness on OCT stratified by treatment groups and follow-up time points. Each error bar is constructed using 95% confidence index for the mean. ΔCMT = follow-up CMT – baseline CMT. |
Resolution of Uveitic Macular Edema
At baseline, macular cystoid spaces were observed in 87.7% (57/65) of all eyes, with 90.6% (29/32) in the combined group and 84.8% (28/33) in the STA group (P = 0.114). Macular subretinal fluid was observed in 65.6% (21/32) eyes and 48.5% (16/33) eyes of the two treatment groups, respectively (P = 0.163) (Table 1). The cumulative incidence of clinical UME resolution of all eyes was 87.7% (57/65). 90.6% (29/32) of eyes in the combined group and 84.8% (28/33) of eyes in the STA group experienced clinically resolved UME by the 24-week follow-up (Figure 2). At 1-week visit, clinical UME resolution was observed in 23 of 32 (71.9%) eyes in the combined group and only 5 of 33 (15.2%) eyes in the STA group (P < 0.001). At 4-week visit, higher cumulative incidence of UME resolution was observed in the combined group (27/32, 84.4%) compared to the STA group (18/33, 54.5%) (P = 0.009). Although the combined group (29/32, 90.6%) had more cumulative incidence of UME resolution than the STA group (27/33, 81.8%) at 12 weeks, there was no statistically significant difference (P = 0.475).
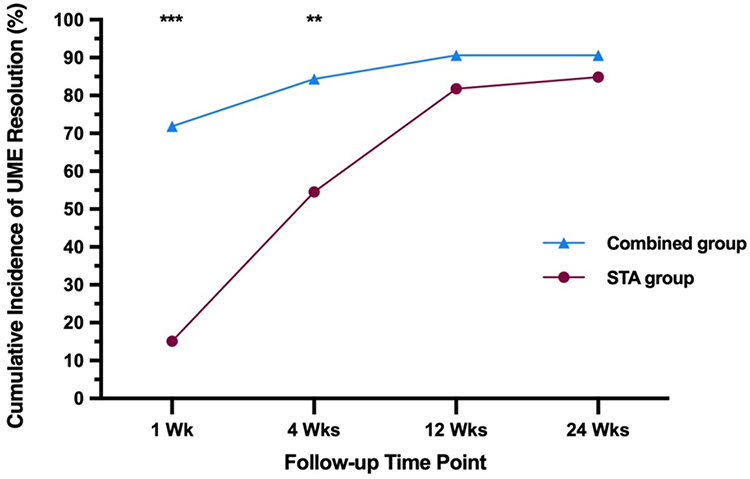 |
Figure 2 Cumulative incidence of UME resolution in OCT after injection at 1 week, 4 weeks, 12 weeks and 24 weeks follow-up time point by treatment groups. ***: P < 0.001; **: P < 0.01. |
Improvement of Visual Acuity
The analysis was conducted similarly to that for the primary outcome measurement (Table 3). Both treatment groups exhibited improved BCVA throughout follow-up (Figure 3). The combined group tended to have more visual improvement than the STA group at 1 week, though regression analysis revealed it was not statistically significant (β = −0.085, P = 0.070) after adjusting for baseline BCVA. Median difference between follow-up BCVA and baseline BCVA (ΔBCVA) [IQR] was −0.204 (0.294) in the combined group and −0.125 (0.204) in the STA group at 1 week. At 4 weeks after injection, the combined group had statistically significantly greater improvements in BCVA from baseline relative to the STA group (median [IQR], −0.301 [0.273] and −0.176 [0.278], respectively) after adjusting for baseline BCVA and UME type (β = −0.108, P = 0.019). As expected, the difference of BCVA improvement between the two treatment groups was not clinically significant at the 12-week (β = −0.057, P = 0.246) and 24-week (β = −0.014, P = 0.840) follow-up visit in the regression models. Baseline BCVA was a strong significant predictor that was negatively associated with BCVA improvement (P ≤ 0.001) at all visits, while no other covariates were significant predictors in the multivariate linear regression models.
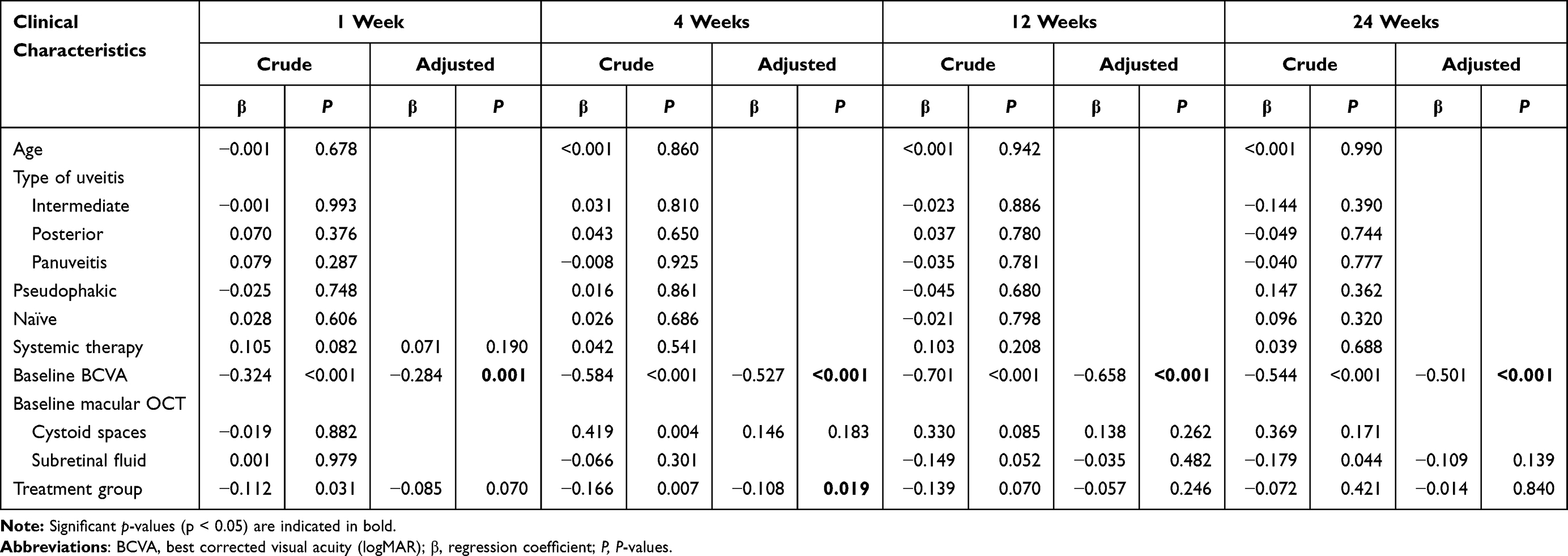 |
Table 3 Multivariable Linear Regression to Compare BCVA Improvement at Each Visit Between Two Treatment Groups |
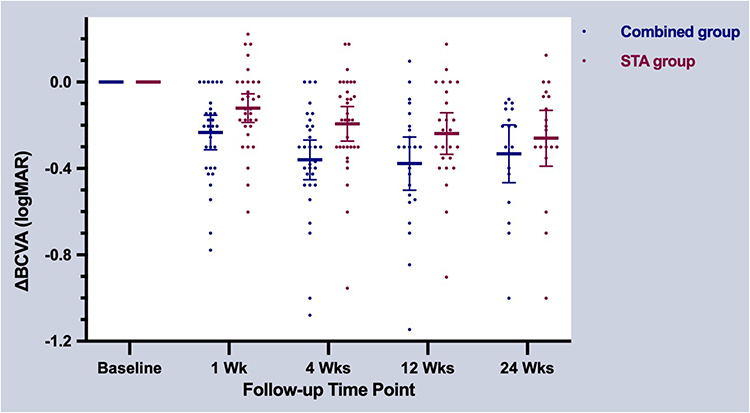 |
Figure 3 Improvement of best corrected visual acuity stratified by treatment groups and follow-up time points. Each error bar is constructed using 95% confidence index for the mean. ΔBCVA = follow-up BCVA – baseline BCVA. |
Adverse Effects
The mean IOP before injection was 12.04±3.83 mmHg in the combined group and 10.54±3.59 in the STA group (Table 1, P = 0.109). An increase of IOP (>25 mmHg) was noted in both treatment groups (four eyes in the combined group, five eyes in the STA group) and was brought under control with topical antiglaucoma medications (Figure 4). No IOP-lowering surgeries or changes in optic disk appearance were encountered in any eyes during the follow-up period. One eye in each group underwent cataract surgery for raised lens opacity. There were no cases of lid ptosis, retinal tear/detachment, sterile endophthalmitis, or vitreous hemorrhage observed in either group.
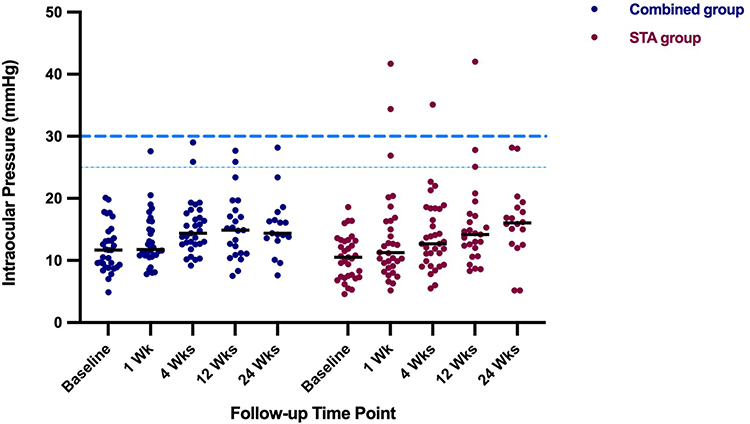 |
Figure 4 Intraocular pressure of two treatment groups at each visit. |
Management of Residual and Recurrent UME
Three eyes in the combined group and four eyes in the STA group had unresolved UME during the follow-up period. In the eyes with residual UME, three eyes were lost to follow-up, three eyes received an injection of aVEGF agent, and the remaining two eyes received the additional STA injection. Three eyes in the combined group and one eye in the STA group experienced recurrent UME, two of which resolved after conservative observation, one of which received intravitreal injection of aVEGF, and the remaining eye was lost to follow-up.
Discussion
This comparative study demonstrated that combination therapy of STA with intravitreal aVEGF can reduce UME more effectively than STA alone, with quicker improvement of visual acuity. As far as we know, no previous studies have investigated such a combination therapy for UME.
Currently, the pathogenesis of UME is not fully understood. In many uveitis eyes, a certain degree of inflammation persists even during systemic steroid therapy.26 Persistent inflammation also triggers VEGF upregulation,27 although the exact pathway by which inflammation and VEGF interact remains incompletely understood.28 It is clear that both injection of local TA and intravitreal aVEGF are somehow effective in managing UME.29,30 The disadvantage of solo intravitreal aVEGF therapy is the frequent injections that pose a great risk for opportunistic intraocular infection in patients on systemic medications.26 So far, there is still no accepted treatment for management of UME, though stepladder treatment has been described before.31 Traditionally anti-inflammatory agents including steroids and nonsteroidal inflammatory drugs are the first choice for UME. However, not all patients are responsive to these treatments. Patients often suffer persistent macular edema even in the absence of active chorioretinitis.30 Therefore, periocular or intravitreal injection of TA, intravitreal aVEGF, and intravitreal steroid implants have been used as adjunctive therapy in addition to systemic medications.26,31
In this study, CMT was significantly more reduced in the combined group than in the STA group, which was evident at the first follow-up visit. Comparing the reduction rate of CMT in both treatment groups at the 1-week follow-up visit revealed that the combined group experienced a reduction by 49.8% to a median of 243.0 µm, while the STA group experienced a reduction by only 20.8% to median of 422.5 µm. Four weeks after injection, the reduction rate of CMT in the combined group was still more (by 51.2% to median of 245.0 µm) than in the STA group (by 40.2% to median of 264.0µm). In a recent randomized clinical trial to evaluate the effectiveness of three regional corticosteroid injections for UME,17 CMT reduction at the 8-week follow-up visit was 23% for the periocular triamcinolone acetonide (PTA) group, similar to the 20.8% reduction we observed in the STA group at the 1-week follow-up visit. Regarding the effectiveness of intravitreal aVEGF on UME, a recent multicenter clinical study revealed that CMT reduction after the first intravitreal injection at the 4-week follow-up visit was 16%,8 which was between the 5%30 and 28%32 reductions reported in the other two studies. These data suggest that combination therapy is superior to single therapy, though the exact mechanism of the interaction remains unclear. We hypothesize that aVEGF quickly neutralizes VEGF to reduce retinal vessel permeability and prevent fluids from leaking into retinal tissue, while steroids downregulate inflammatory cytokines to interrupt VEGF production and to promote the stability of the retinal vascular endothelium. With these added pharmacological effects, intraretinal fluids can be quickly absorbed as shown on OCT. Steroids promote neuronal cell recovery, which is translated into visual improvement. Studies have shown that aVEGF does not possess anti-inflammatory properties while TA has weak anti-angiogenesis effects.15,33 Therefore, combination of the two drugs makes biological sense. In fact, combination therapy using both local TA and aVEGF is a superior treatment for several other ocular diseases such as age-related macular degeneration,33 diabetic macular edema,34 and retinal vein occlusion.20,35 In the current study, visual improvement was associated with greater CMT reduction for the combined group at 1-week and 4-week follow-up visits, in agreement with previous studies.17,36 The positive association between anatomic and visual function improvement may indicate a benefit of early intervention prior to unrepairable damage.
Intravitreal injection of aVEGF was conducted prior to STA in the combined group of our study. To our knowledge, no such similar study has been reported in UME for our reference to determine the order of treatment. Different treatment regimens for retinal diseases were adopted in previous studies. Eriş et al performed aVEGF injection 10 days after STA injection in the treatment of diabetic macular edema.22 Roelofs et al proceeded with intravitreal injection of TA one week before an aVEGF injection in eyes with radiation papillopathy.37 Similar strategy was adopted in an earlier randomized controlled study for macular edema due to retinal vein occlusion.35 A longer interval (two weeks) between aVEGF and Ozurdex injection was reported by Singer et al in patients with retinal vein occlusion.21 Local injection of steroids and aVEGF was performed simultaneously in other studies20,33. In addition, there is no report which has directly explored the effect in relation to the order of aVEGF and STA injection.
In a previous study, only 53% of patients treated by STA injection experienced UME resolution at the 4-week visit,38 which is comparable to our observations (54.5% of the STA group). Previous reports found that 12 weeks after STA injection, only 55.6–57% of patients experienced UME resolution.38,39 A higher proportion was observed in the current study (81.8%). At the 24-week visit, the cumulative incidence of clinical UME resolution was 77.8% in the previous study39 and 84.8% in our study. These differences may be due to 21.1% of eyes receiving orbital floor injections or a dosage of 20 mg TA in previous studies, while all patients of the STA group in our study were injected using the posterior sub-Tenon approach of 40 mg concentrated TA. Further, all eyes enrolled in our study had active uveitis with macular edema, whereas only 45% of those in the previous study had active uveitis at baseline,38 which may account for the easier resolution of UME. With combined injection of intravitreal aVEGF and STA, dramatically more clinical resolution of UME was observed at both 1-week (71.9%, compared with STA group 15.2%) and 4-week visits (84.4%).
As a method for local delivery of steroids, intravitreal TA is more effective than STA for macular edema. A recent clinical trial showed that intravitreal TA or Ozurdex achieved equivalent CMT reduction of 39% or 46%, respectively, which was significantly better than the 23% observed in the PTA group at the 8-week follow-up visit.17 However, significantly more ocular side effects were observed after intravitreal injection of TA or Ozurdex than PTA. It has been reported that intravitreal TA causes 20–65% of the incidence of IOP elevation.40 In the current study, 13.8% (9/65) eyes experienced elevation of IOP (>25 mmHg), consistent with previous reports.41,42 Thus, combined treatment may be equally or more effective in UME therapy compared with intraocular TA or Ozurdex, but with fewer side effects.
In summary, the current study demonstrated the superiority of a combined therapy in the treatment of UME. Combined STA and aVEGF therapy were well tolerated and did not show greater risks than STA therapy alone. We acknowledge that this study has some limitations such as its retrospective nature, small population size (65 eyes of 65 patients), and short follow-up period (24 weeks). Besides, a further subgroup analysis to investigate heterogeneity of different aVEGF was not carried out in this study. A long-term, randomized, and controlled trial with additional participants may be needed to further evaluate efficiency and safety of combined therapy for UME.
Acknowledgments
The authors gratefully acknowledge the study participants. This research was supported by the Zhejiang Province Natural Science Foundation of China (LQ21H180011, LY21H180004, LQ20H180006), Key R&D Program of Zhejiang Province (2021C04019) and Wenzhou Science and Technology Bureau (Y20190625).
Disclosure
The authors declare that they have no conflicts of interest with the contents of this article.
References
1. Rothova A, Suttorp-van Schulten MS, Frits Treffers W, Kijlstra A. Causes and frequency of blindness in patients with intraocular inflammatory disease. Br J Ophthalmol. 1996;80(4):332–336. doi:10.1136/bjo.80.4.332
2. Suttorp-Schulten MS, Rothova A. The possible impact of uveitis in blindness: a literature survey. Br J Ophthalmol. 1996;80(9):844–848. doi:10.1136/bjo.80.9.844
3. Thomas AS, Lin P. Local treatment of infectious and noninfectious intermediate, posterior, and panuveitis: current concepts and emerging therapeutics. Curr Opin Ophthalmol. 2020;31(3):174–184. doi:10.1097/ICU.0000000000000651
4. Accorinti M, Okada AA, Smith JR, Gilardi M. Epidemiology of macular edema in uveitis. Ocul Immunol Inflamm. 2019;27(2):169–180. doi:10.1080/09273948.2019.1576910
5. Reddy AK, Cabrera M, Yeh S, Davis JL, Albini TA. Optical coherence tomography–guided ranibizumab injection for cystoid macular edema in well-controlled uveitis: twelve-month outcomes. Retina. 2014;34(12):2431–2438. doi:10.1097/IAE.0000000000000274
6. Tsui E, Rathinam SR, Gonzales JA, et al. Outcomes of uveitic macular edema in the First-line Antimetabolites as Steroid-sparing Treatment (FAST) uveitis trial. Ophthalmology. 2022. doi:10.1016/j.ophtha.2022.02.002
7. Radosavljevic A, Agarwal M, Bodaghi B, Smith JR, Zierhut M. Medical therapy of uveitic macular edema: biologic agents. Ocul Immunol Inflamm. 2020;28(8):1239–1250. doi:10.1080/09273948.2019.1709648
8. Lasave AF, Schlaen A, Zeballos DG, et al. Twenty-four months follow-up of intravitreal bevacizumab injection versus intravitreal triamcinolone acetonide injection for the management of persistent non-infectious uveitic cystoid macular edema. Ocul Immunol Inflamm. 2019;27(2):294–302. doi:10.1080/09273948.2017.1400073
9. Fiedler U, Augustin HG. Angiopoietins: a link between angiogenesis and inflammation. Trends Immunol. 2006;27(12):552–558. doi:10.1016/j.it.2006.10.004
10. Schoenberger SD, Kim SJ, Sheng J, et al. Increased prostaglandin E2 (PGE2) levels in proliferative diabetic retinopathy, and correlation with VEGF and inflammatory cytokines. Invest Ophthalmol Vis Sci. 2012;53(9):5906–5911. doi:10.1167/iovs.12-10410
11. van Kooij B, Rothova A, Rijkers GT, de Groot-mijnes JDF. Distinct cytokine and chemokine profiles in the aqueous of patients with uveitis and cystoid macular edema. Am J Ophthalmol. 2006;142(1):192–194. doi:10.1016/j.ajo.2006.02.052
12. Paroli MP, Teodori C, D’alessandro M, et al. Increased vascular endothelial growth factor levels in aqueous humor and serum of patients with quiescent uveitis. Eur J Ophthalmol. 2007;17(6):938–942. doi:10.1177/112067210701700611
13. El‐Asrar AMA, Berghmans N, Al-Obeidan SA, et al. The CC chemokines CCL8, CCL13 and CCL20 are local inflammatory biomarkers of HLA-B27-associated uveitis. Acta Ophthalmol. 2019;97(1):e122–e128. doi:10.1111/aos.13835
14. El-Asrar AMA, Struyf S, Kangave D, et al. Cytokine profiles in aqueous humor of patients with different clinical entities of endogenous uveitis. Clin Immunol. 2011;139(2):177–184. doi:10.1016/j.clim.2011.01.014
15. Arimura S, Takamura Y, Miyake S, et al. The effect of triamcinolone acetonide or bevacizumab on the levels of proinflammatory cytokines after retinal laser photocoagulation in pigmented rabbits. Exp Eye Res. 2016;149:1–7. doi:10.1016/j.exer.2016.06.004
16. Jeon S, Lee WK, Jung Y. Changes in the intraocular cytokine levels after intravitreal bevacizumab in uveitic macular edema. Ocul Immunol Inflamm. 2012;20(5):360–364. doi:10.3109/09273948.2012.709576
17. Thorne JE, Sugar EA, Holbrook JT, et al. Periocular triamcinolone vs. intravitreal triamcinolone vs. intravitreal dexamethasone implant for the treatment of uveitic macular edema: the PeriOcular vs. INTravitreal corticosteroids for uveitic macular edema (POINT) trial. Ophthalmology. 2018;126(2):283–295.
18. Shen L, You Y, Sun S, et al. Intraocular and systemic pharmacokinetics of triamcinolone acetonide after a single 40-mg posterior subtenon application. Ophthalmology. 2010;117(12):2365–2371. doi:10.1016/j.ophtha.2010.03.033
19. Beer PM, Bakri SJ, Singh RJ, et al. Intraocular concentration and pharmacokinetics of triamcinolone acetonide after a single intravitreal injection. Ophthalmology. 2003;110(4):681–686. doi:10.1016/S0161-6420(02)01969-3
20. Moon J, Kim M, Sagong M. Combination therapy of intravitreal bevacizumab with single simultaneous posterior subtenon triamcinolone acetonide for macular edema due to branch retinal vein occlusion. Eye. 2016;30(8):1084–1090. doi:10.1038/eye.2016.96
21. Singer MA, Bell DJ, Woods P, et al. Effect of combination therapy with bevacizumab and dexamethasone intravitreal implant in patients with retinal vein occlusion. Retina. 2012;32:1289–1294.
22. Eriş E, Perente I, Vural E, et al. Evaluation of the effect of combined intravitreal ranibizumab injection and sub-tenon steroid injection in the treatment of resistant diabetic macular edema. Int Ophthalmol. 2019;39(7):1575–1580. doi:10.1007/s10792-018-0977-0
23. Nunome T, Sugimoto M, Kondo M, Suto C. Short-term results of intravitreal triamcinolone acetonide combined with cataract surgery for diabetic macular edema in Japan: in the era of anti-vascular endothelial growth factor therapy. Ophthalmol. 2018;240(2):73–80. doi:10.1159/000487548
24. Xu X, Han Y, Kong L, et al. Clinical implication of triamcinolone in aqueous humor after depository sub-Tenon application. J Cataract Refract Surg. 2017;43(11):1383–1390. doi:10.1016/j.jcrs.2017.08.010
25. Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of uveitis nomenclature for reporting clinical data. Results of the first international workshop. Am J Ophthalmol. 2005;140:509–516.
26. Butler NJ. How to manage steroid-refractory uveitic CME. Available from: https://www.reviewofophthalmology.com/article/how-to-manage-steroidrefractory-uveitic-cme.
27. Hernández Garfella ML, Palomares Fort P, Román Ivorra JA, Cervera Taulet E. Aqueous humor levels of different interleukins 1-β, 2, 6 and 10, tumor necrosis factor-α and vascular endothelial growth factor in uveitis treated with adalimumab. J Ophthalmic Vis Res. 2015;10(1):49–54. doi:10.4103/2008-322X.156110
28. Freeman G, Matos K, Pavesio CE. Cystoid macular oedema in uveitis: an unsolved problem. Eye. 2001;15:12–17.
29. Bakri SJ, Kaiser PK. Posterior subtenon triamcinolone acetonide for refractory diabetic macular edema. Am J Ophthalmol. 2005;139(2):290–294. doi:10.1016/j.ajo.2004.09.038
30. Cordero Coma M, Sobrin L, Onal S, Christen W, Foster CS. Intravitreal bevacizumab for treatment of uveitic macular edema. Ophthalmology. 2007;114(8):1574–1579.e1. doi:10.1016/j.ophtha.2006.11.028
31. Preble JM, Foster CS. Uveitic macular edema: a stepladder treatment paradigm. Clin Investig. 2015;5(5):509–517. doi:10.4155/cli.15.1
32. Mackensen F, Heinz C, Becker MD, Heiligenhaus A. Intravitreal bevacizumab (avastin) as a treatment for refractory macular edema in patients with uveitis: a pilot study. Retina. 2008;28(1):41–45. doi:10.1097/IAE.0b013e318156db75
33. Rezar-Dreindl S, Sacu S, Eibenberger K, et al. The intraocular cytokine profile and therapeutic response in persistent neovascular age-related macular degeneration. Invest Ophthalmol Vis Sci. 2016;57(10):4144–4150. doi:10.1167/iovs.16-19772
34. Lim JW, Lee HK, Shin MC. Comparison of intravitreal bevacizumab alone or combined with triamcinolone versus triamcinolone in diabetic macular edema: a randomized clinical trial. Ophthalmologica. 2012;227(2):100–106. doi:10.1159/000331935
35. Maturi RK, Chen V, Raghinaru D, Bleau L, Stewart MW. A 6-month, subject-masked, randomized controlled study to assess efficacy of dexamethasone as an adjunct to bevacizumab compared with bevacizumab alone in the treatment of patients with macular edema due to central or branch retinal vein occlusion. Clin Ophthalmol. 2014;8:1057–1064.
36. Lardenoye CWTA, van Kooij B, Rothova A. Impact of macular edema on visual acuity in uveitis. Ophthalmology. 2006;113(8):1446–1449. doi:10.1016/j.ophtha.2006.03.027
37. Roelofs K, Larocque MP, Murtha A, Weis E. The use of intravitreal anti-VEGF and triamcinolone in the treatment of radiation papillopathy. Ocul Oncol Pathol. 2018;4(6):395–400. doi:10.1159/000487543
38. Leder HA, Jabs DA, Galor A, Dunn JP, Thorne JE. Periocular triamcinolone acetonide injections for cystoid macular edema complicating noninfectious uveitis. Am J Ophthalmol. 2011;152(3):441–448.e2. doi:10.1016/j.ajo.2011.02.009
39. Choudhry S, Ghosh S. Intravitreal and posterior subtenon triamcinolone acetonide in idiopathic bilateral uveitic macular oedema. Clin Experiment Ophthalmol. 2007;35(8):713–718. doi:10.1111/j.1442-9071.2007.01578.x
40. Razeghinejad MR, Katz LJ. Steroid-Induced Iatrogenic Glaucoma. Ophthalmic Res. 2012;47(2):66–80. doi:10.1159/000328630
41. Sen HN, Vitale S, Gangaputra SS, et al. Periocular corticosteroid injections in uveitis: effects and complications. Ophthalmology. 2014;121(11):2275–2286. doi:10.1016/j.ophtha.2014.05.021
42. Thach AB, Dugel PU, Flindall RJ, Sipperley JO, Sneed SR. A comparison of retrobulbar versus sub-tenon’s corticosteroid therapy for cystoid macular edema refractory to topical medications. Ophthalmology. 1997;104(12):2003–2008. doi:10.1016/S0161-6420(97)30065-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.