Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
Symptom Improvement Following Treatment with the Inhaled Dual Phosphodiesterase 3 and 4 Inhibitor Ensifentrine in Patients with Moderate to Severe COPD – A Detailed Analysis
Authors Watz H, Rickard K ![]() , Rheault T, Bengtsson T, Singh D
, Rheault T, Bengtsson T, Singh D
Received 29 May 2020
Accepted for publication 20 August 2020
Published 16 September 2020 Volume 2020:15 Pages 2199—2206
DOI https://doi.org/10.2147/COPD.S263025
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Henrik Watz,1 Kathleen Rickard,2 Tara Rheault,2 Thomas Bengtsson,3 Dave Singh4
1Pulmonary Research Institute at Lung Clinic Grosshansdorf, Airway Research Center North (ARCN), Member of the German Center for Lung Research (DZL), Grosshansdorf, Germany; 2Verona Pharma Plc, Raleigh, NC, USA; 3StatMind AB, Lund, Sweden; 4Medicines Evaluation Unit, University of Manchester & Manchester University NHS Foundation Trust, Manchester, UK
Correspondence: Henrik Watz
Pulmonary Research Institute at LungenClinic Grosshansdorf, Airway Research Centre North (ARCN), German Centre for Lung Research (DZL), Wöhrendamm 80, Grosshansdorf 22927, Germany
Tel +49-4102-8881-0
Fax +49-4102-8881-114
Email [email protected]
Introduction: Ensifentrine is an inhaled first-in-class dual inhibitor of phosphodiesterase (PDE) 3 and 4. In a four-week randomized, double-blind, placebo-controlled, parallel-group study in patients with chronic obstructive pulmonary disease (COPD), nebulized ensifentrine 0.75 to 6mg twice daily significantly improved bronchodilation and symptoms, with all doses being well tolerated. Here, we report data for a number of prespecified exploratory and post hoc endpoints from this study that help to further profile the effect of ensifentrine on symptoms.
Methods: Eligible patients were males or females aged 40– 75 years with COPD, post-bronchodilator forced expiratory volume in 1 second 40– 80% predicted. Other than being clinically stable for at least four weeks prior to entry, there were no symptomatic inclusion or exclusion criteria. The outcome measures reported in this manuscript are the Evaluating Respiratory Symptoms [E-RS™:COPD] questionnaire total score and subscales (breathlessness, cough/sputum and chest symptoms) at Weeks 1– 4, Transition Dyspnea Index (TDI) focal score at Weeks 2 and 4, and St George’s Respiratory Questionnaire – COPD Specific (SGRQ-C) total score and domain data (symptoms, activity and impacts) at Week 4.
Results: There was a gradual improvement versus placebo with all ensifentrine doses for all three E-RS™:COPD subscales from Week 1 to Week 4, with the greatest ensifentrine effect on the breathlessness subscale, and all four doses superior to placebo from Week 2 onwards (p< 0.05). For TDI focal score, all ensifentrine doses were superior to placebo at Weeks 2 and 4 (p< 0.05). In the individual SGRQ-C domains at Week 4, ensifentrine had the greatest effect on the symptoms domain, with ensifentrine 6mg superior to placebo (p< 0.05).
Conclusion: In these analyses, ensifentrine demonstrated a notable early and meaningful effect on dyspnea, with this effect observed across two different assessment tools.
Keywords: phosphodiesterase inhibitors, chronic obstructive pulmonary disease, signs and symptoms, respiratory, drug therapy
Introduction
Although a range of effective therapies are available for chronic obstructive pulmonary disease (COPD), many patients still experience daily symptoms,1–3 even when receiving maximal combined inhaled therapy. Novel treatment options are therefore needed that will target symptoms, along with lung function and exacerbations.
Phosphodiesterases (PDEs) are enzymes that impact a range of cellular functions by modulating levels of cyclic nucleotides, with PDE3 inhibition resulting in airway smooth muscle relaxation,4–6 and PDE4 inhibition having anti-inflammatory effects.4–6 There is evidence to suggest that combined inhibition of PDE3 and PDE4 can have additive (or perhaps synergistic) effects with respect to anti-inflammatory and bronchodilator activity.4 Ensifentrine is an inhaled first-in-class dual inhibitor of PDE3 and PDE4 that has previously demonstrated bronchodilator and anti-inflammatory efficacy in healthy volunteers, and in patients with asthma or COPD.7–10 In particular, in a four-week randomized, double-blind, placebo-controlled, parallel-group Phase IIb study in patients with COPD, ensifentrine 0.75 to 6 mg twice daily (BID) significantly improved bronchodilation and symptoms, with all doses being well tolerated.11 In the current manuscript, we used data from this study to further profile the effect of ensifentrine on symptoms by evaluating the individual domains of the patient reported outcome instruments used. This included prespecified exploratory endpoints describing the effect of ensifentrine on the Evaluating Respiratory Symptoms (E-RS™:COPD) questionnaire subscales and St George’s Respiratory Questionnaire – COPD Specific (SGRQ-C) questionnaire domains, and post hoc analyses of E-RS™:COPD and Transition Dyspnea Index (TDI) responders.
Materials and Methods
Trial Design and Patients
The design of the study (including full inclusion and exclusion criteria) has been previously reported in detail.11 In brief, eligible patients were males or females aged 40–75 years with a diagnosis of COPD and post-bronchodilator forced expiratory volume in 1 second (FEV1) 40–80% predicted normal. Other than requiring all patients to be clinically stable for at least four weeks prior to entry, there were no symptomatic inclusion or exclusion criteria. Patients receiving inhaled corticosteroids (ICSs) prior to the study were permitted to continue their ICS medication throughout the study, providing the dose was stable from at least four weeks prior to entry and throughout. Inhaled long-acting β2-agonists and long-acting muscarinic antagonists were not permitted during the study, and for at least 48 h (once-daily medications) or 24 h (twice daily) prior to entry. All patients provided written informed consent prior to any study-related procedure. The study was approved by the independent ethics committees at each institution (see supplement), and was performed in accordance with the principles of the Declaration of Helsinki, and the International Conference on Harmonization notes for guidance on Good Clinical Practice (ICH/CPMP/135/95). The study is registered at ClinicalTrials.gov (NCT03443414) and EudraCT (2016–005205-40).
After a 7–14-day run-in period, eligible patients were randomized equally to five treatment groups, to inhale nebulized ensifentrine 0.75, 1.5, 3 or 6 mg or placebo BID for four weeks. Daily throughout the study (including between screening and randomization [baseline]) patients used an e-diary to record COPD symptoms (using the E-RS™:COPD questionnaire). In addition, at the randomization visit, baseline (pre-dose) data were collected for Baseline Dyspnea Index and SGRQ-C, with TDI assessed at Weeks 2 and 4 and SGRQ-C at Week 4.
We present the mean treatment-placebo differences for E-RS™:COPD total score and subscales (breathlessness, cough/sputum and chest symptoms) at Weeks 1 to 4, TDI focal score at Weeks 2 and 4, and SGRQ-C total score and domains (symptoms, activity and impacts) at Week 4. In addition, we report the responder analyses at Week 4 for the E-RS™:COPD subscales, TDI, and SGRQ-C total score.
Sample Size and Statistical Methods
The study was powered for the primary endpoint, which was to investigate the placebo-corrected effect of ensifentrine on change from baseline in peak FEV1 on Week 4. The analyses in this manuscript were not formally powered.
The mean values reported in this manuscript were analyzed using a restricted maximum likelihood-based mixed model for repeated measures, including fixed effects for treatment, visit and treatment by visit interaction, patient as random effect, baseline value as covariate and covariance structure by visit. E-RS™:COPD total score data were averaged to give weekly scores (with a minimum requirement of four days of data). To control for the familywise error rate, a fixed-sequence testing strategy was employed, with the highest ensifentrine dose tested first versus placebo. Results are presented for the full analysis set, which included all randomized patients who received at least one dose of study medication and who had at least one post-treatment efficacy data assessment. Supportive data are presented for the per-protocol set, which included all patients in the full analysis set who did not have pre-specified major protocol deviations that could have affected the efficacy outcome or the patient’s treatment.
The percentages of responders were analyzed in the full analysis set only, using a logistic regression model adjusting for treatment and country, with treatment differences expressed as the odds ratio. A responder was defined as a patient with at least a 1 unit improvement (ie, decrease) in E-RS™:COPD breathlessness subscale,12 at least a 0.7 unit improvement (decrease) in E-RS™:COPD cough/sputum subscale or chest symptoms subscale,12 a TDI focal score of at least 1,13 or at least a 4 unit improvement (decrease) in SGRQ-C total score.14
Results
The study took place between 10 July 2017 and 7 February 2018. Of 616 patients recruited into the study, 405 were randomized, with 403 receiving at least one dose of study medication (81, 81, 82, 80 and 79 in the ensifentrine 0.75, 1.5, 3, and 6 mg and placebo groups, respectively) and who were therefore included in the full analysis set used for the current analyses. The per-protocol set included 54, 72, 62, 65 and 50 patients, respectively, with the most common major protocol deviation leading to exclusion from the full analysis set being plasma ensifentrine concentrations being out of expected range (with detectable levels of ensifentrine in patients in the placebo group). The mean (SD) age of the patients randomized into the study was 63.2 (6.61) years, 60.5% of whom were male, with mean post-bronchodilator FEV1 55.8% predicted, ranging from 40.2 to 79.9%. Baseline mean E-RS:COPD™ total scores were 13.6, 12.3, 12.0, 12.2 and 11.5 in the ensifentrine 0.75, 1.5, 3, and 6 mg and placebo groups, respectively, with Baseline Dyspnea Index focal scores of 5.9, 6.4, 6.4, 6.4 and 6.4, and SGRQ-C total scores of 49.9, 43.4, 42.1, 44.1 and 42.3.
E-RS™:COPD
We previously reported the results for mean E-RS™:COPD total score, in which there was a progressive improvement over the duration of the study for all four ensifentrine doses compared to placebo (Figure 1A).11 Consistent with these total score results, in the full analysis set there was a gradual increase in all mean ensifentrine versus placebo differences for all three subscales from Week 1 to Week 4 – in other words, a relative improvement in symptoms in the ensifentrine groups (Figure 1B to D). The greatest ensifentrine effect was on the breathlessness subscale (indicating a relative improvement in dyspnea), for which the mean differences versus placebo were statistically significant for all four doses from Week 2 onwards, reaching an effect size of approximately –1 by Week 4. Ensifentrine also improved the cough/sputum and chest symptoms subscales mean scores, with significant differences versus placebo from Week 3 onwards for all doses. The relative effect of ensifentrine versus placebo was generally greater in the per-protocol set than in the full analysis set – again with the greatest effect on the breathlessness subscale (Supplementary Figure 1). For the responder analyses at Week 4, a higher proportion of patients met the definition of response in the four ensifentrine groups than placebo in all three domains, although the odds ratios were not consistently statistically significant (Table 1).
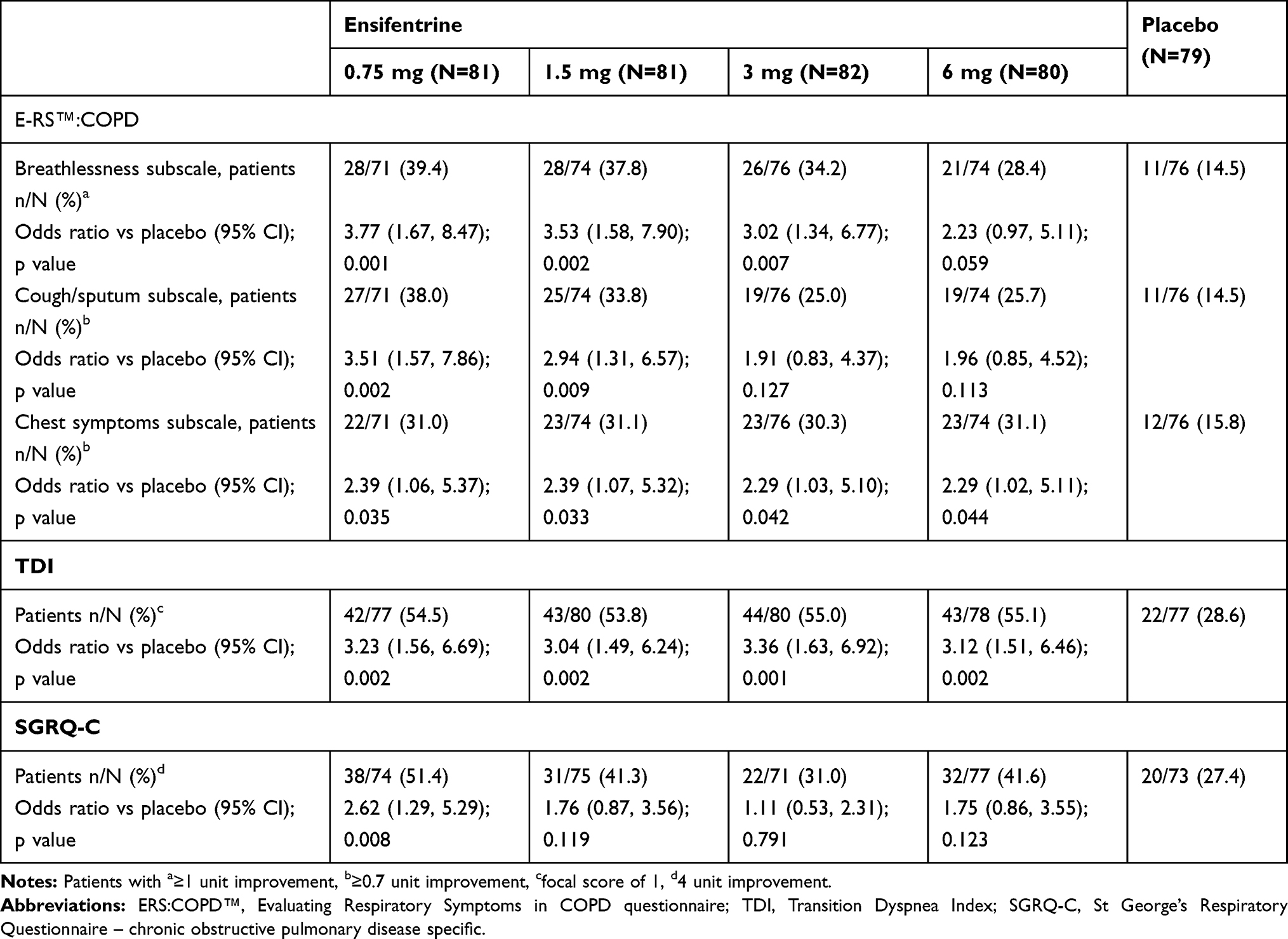 |
Table 1 E-RS™:COPD Subscales, TDI Focal Score, and SGRQ-C Total Score Responder Analyses at Week 4 (Full Analysis Set) |
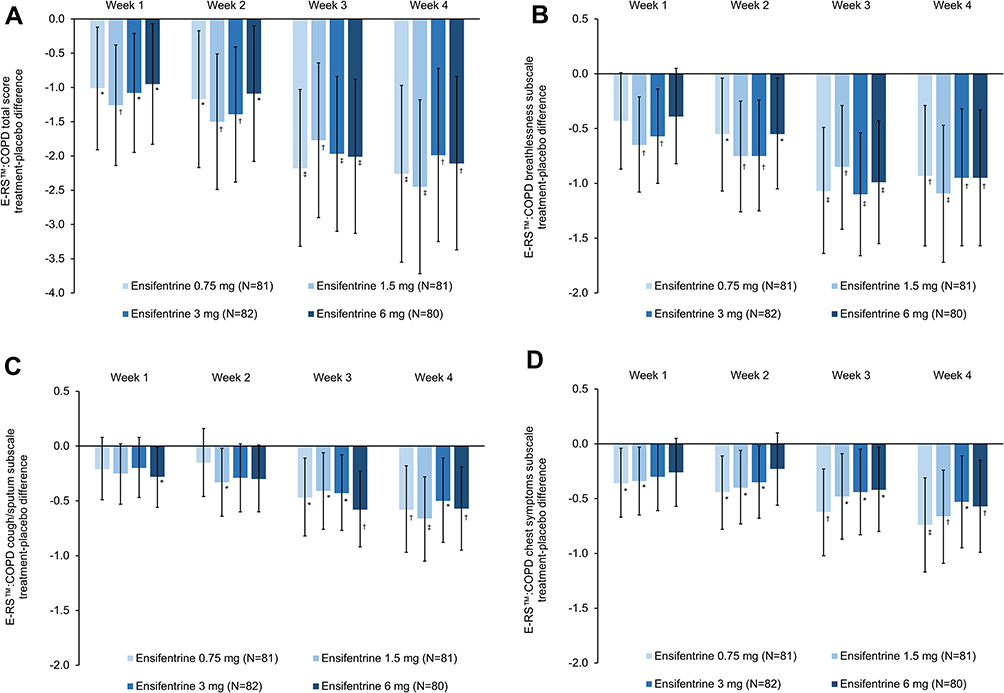 |
Figure 1 E-RS™:COPD: (A) total score; (B) breathlessness subscale; (C) cough/sputum subscale; (D) chest symptoms subscale (full analysis set). Panel 1A is reproduced from Singh D, Martinez FJ, Watz H, Bengtsson T, Maurer BT. A dose-ranging study of the inhaled dual phosphodiesterase 3 and 4 inhibitor ensifentrine in COPD. Respir Res. 2020;21(1):47. Creative commons license and disclaimer available from: (http://creativecommons.org/licenses/by/4.0/).11 Data are least squares means treatment–placebo differences and 95% confidence intervals. *p<0.05; †p<0.01; ‡p<0.001 vs placebo. Least squares mean changes from baseline in the placebo group (N=79) were 0.38, 0.57, 1.11 and 1.19 at Weeks 1, 2, 3 and 4, respectively for the total score, 0.11, 0.25, 0.53 and 0.47 for the breathlessness subscale, 0.14, 0.13, 0.30 and 0.36 for the cough/sputum subscale, and 0.12, 0.18, 0.26 and 0.35 for the chest symptoms subscale. Data analyzed for 71, 74, 76, 74 and 76 patients in the ensifentrine 0.75, 1.5, 3 and 6 mg and placebo groups, respectively. |
TDI
TDI was measured at Weeks 2 and 4; we previously reported Week 4 mean TDI focal score values for the full analysis set.11 Data at Week 2 were similar to the Week 4 values, with all four ensifentrine doses superior to placebo, and with differences that exceeded the minimum clinically important difference (MCID) of 1 (Figure 2). Again the relative effect of ensifentrine versus placebo was generally greater in the per-protocol set than in the full analysis set (Supplementary Figure 2). In the responder analyses at Week 4, a significantly higher proportion of patients in all four ensifentrine groups had a clinically relevant improvement from baseline than in the placebo group (Table 1).
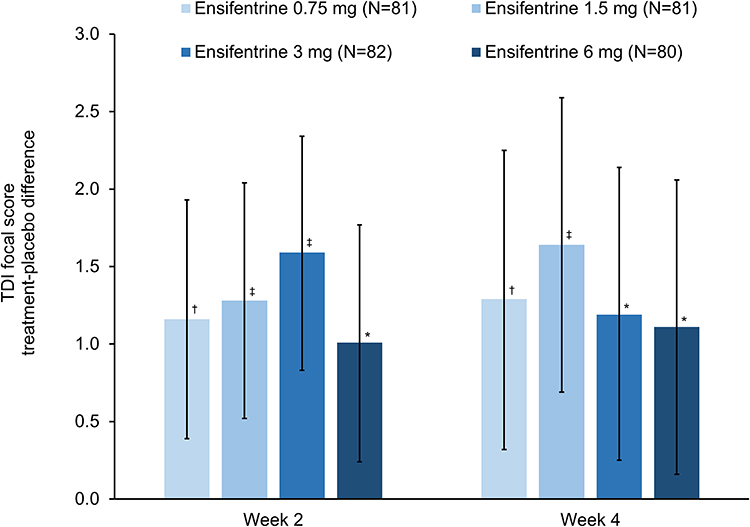 |
Figure 2 TDI focal score at Weeks 2 and 4 (full analysis set). Data are least squares means treatment–placebo differences and 95% confidence intervals. *p<0.05; †p<0.01; ‡p<0.001 vs placebo. Least squares mean TDI total scores in the placebo group (N=79) were 0.10 and 0.31 at Weeks 2 and 4, respectively. Data analyzed for 75, 80, 80, 78 and 76 patients in the ensifentrine 0.75, 1.5, 3 and 6 mg and placebo groups, respectively. |
SGRQ-C
For mean SGRQ-C total score at Week 4 in the full analysis set, there were numerical improvements versus placebo with all four ensifentrine doses, although the differences were not statistically significant (Figure 3).11 In the individual domains at Week 4, ensifentrine had the greatest effect on the SGRQ-C symptoms domain, with the mean difference versus placebo reaching statistical significance for the 6 mg dose and nominal significance (due to the hierarchy) for the 0.75 mg dose (Figure 3). Numerical improvements versus placebo were observed for all doses in the impacts domain. A similar pattern was also seen in the per-protocol set – again with the relative effect of ensifentrine versus placebo generally greater in the per-protocol set than in the full analysis set (Supplementary Figure 3). In the responder analysis at Week 4, a higher proportion of patients met the definition of response in the four ensifentrine groups than placebo in all three domains, although the odds ratios were not consistently statistically significant (Table 1).
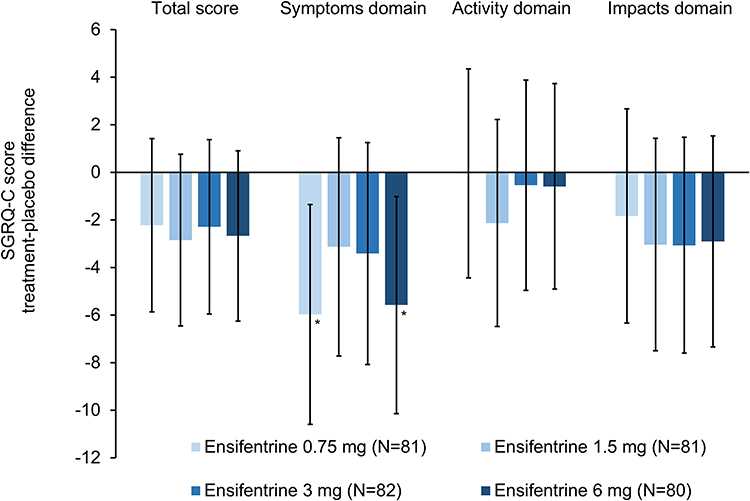 |
Figure 3 SGRQ-C total score and domains at Week 4 (full analysis set). Data are least squares means treatment–placebo differences and 95% confidence intervals. *p<0.05 vs placebo. Least squares mean changes from baseline in the placebo group (N=79) were –0.33, 1.25, –2.16 and 0.11 for the total score and the symptoms, activity and impacts domains, respectively. Data analyzed for 74, 75, 71, 77 and 73 patients in the ensifentrine 0.75, 1.5, 3 and 6 mg and placebo groups, respectively. |
Discussion
In these analyses, the different domains of the patient reported outcome instruments were evaluated to further understand the effects of ensifentrine on different components of symptoms and quality of life. Ensifentrine demonstrated a notable early and meaningful effect on dyspnea, with this effect observed across two different scales (E-RS™:COPD breathlessness subscale and TDI). The SGRQ-C domain analysis also indicated a benefit of ensifentrine on symptoms. These benefits were demonstrated despite the relatively short (four week) treatment duration, and is of particular interest as breathlessness has a substantial impact on overall health-related quality of life in COPD,1,15 and is one of the key reasons for patients to seek medical care.16
The previously published primary and secondary analyses, which focused on lung function, confirmed the bronchodilator effect of ensifentrine, which was apparent from the first dose, with a more gradual effect on symptoms (as assessed using the E-RS™:COPD total score).11 In the current analyses, the effect of ensifentrine on all three of the E-RS™:COPD subscales showed a similar pattern to the total score with gradual improvement over the study period. Whereas many questionnaires only have defined MCIDs for their total scores, the E-RS™:COPD has recognized MCID values for the total score (–2.0) and for each of the subscales. In a detailed analysis using results from three clinical trials, MCIDs for the subscales were defined as –1.0 for the breathlessness subscale and –0.7 for both the cough/sputum and chest symptoms subscales.12 In our analyses, whereas the greatest effect on the cough/sputum and chest symptoms subscales was noted in the Week 4 analyses (at or near the MCID12), interestingly the effect of ensifentrine on the breathlessness subscale was similar at Weeks 3 and 4 (again at or near the MCID), with significant improvements versus placebo seen with all ensifentrine doses at Week 2. This suggests that the rapid bronchodilator effect of ensifentrine could be translating into an early patient-perceived improvement in breathlessness, whereas the effect of ensifentrine on cough/sputum and chest symptoms may due (at least in part) to a more gradual anti-inflammatory effect. In contrast, in a previous study the effect of the long-acting muscarinic antagonist aclidinium on E-RS™:COPD was predominantly driven by the breathlessness subscale even by Week 24.17 In addition, although care should be taken with indirect comparisons between studies, the effect of ensifentrine on symptoms in this study seems numerically greater than the PDE4 inhibitor roflumilast in other studies18,19 – again supporting the dual mechanism of action.
The effect of ensifentrine on TDI total score, which predominantly assesses the impact of COPD symptoms such as breathlessness on daily activities, was similar at Weeks 2 and 4 (and exceeded the MCID of113), again suggesting that patients perceived an early reduction in their symptoms as was seen with the E-RS™:COPD breathlessness subscale. In contrast, SGRQ-C assesses the broad impact of COPD on an individual’s life, and it is possible that the study duration was insufficient to demonstrate a clear impact on this endpoint. Despite this, at Week 4 ensifentrine 6 mg had a significant effect versus placebo on the SGRQ-C symptoms domain (with nominal significance for the 0.75 mg dose, given the hierarchy), although the effect overall and on the activity and impacts domain was less marked. We acknowledge that the wide confidence intervals on these data mean that the results should be interpreted with caution. Unfortunately, the symptoms domain of the SGRQ-C does not distinguish between the impact of breathlessness, cough, and sputum, and thus detailed cross-comparisons are not possible on the specific symptom improvement as is possible with the E-RS™:COPD.
The main analyses were conducted in the full analysis set – those patients who received at least one dose of study medication and who had at least one post-baseline efficacy evaluation available. When we excluded patients with major protocol deviations (ie, in the per-protocol set), the relative effect of ensifentrine versus placebo was generally greater than in the full analysis set. As a consequence, the improvements versus placebo in the per-protocol set for the E-RS™:COPD and SGRQ-C supported clinically meaningful effects that were somewhat diluted in the full analysis set.
The main limitation of these analyses is that although most of the endpoints were prespecified, the study was powered for lung function and not to evaluate the effect of ensifentrine on symptoms. In addition, the four-week duration of the study is relatively short when evaluating the effect of therapy on these endpoints – especially TDI and SGRQ-C, for which a behavioral change is needed if a patient is to perceive maximal benefits from either bronchodilation or reduced inflammation. Finally, since randomization into the study did not stratify patients by symptoms, there were some differences in baseline criteria across ensifentrine doses, such that patients in the 0.75 mg group had the highest (ie, most severe) baseline E-RS™:COPD and SGRQ-C values. This may explain why this group benefited from therapy as much as the higher doses.
Conclusion
In these analyses ensifentrine demonstrated a notable early and meaningful effect on dyspnea, with this effect observed across two different assessment tools.
Data Sharing Statement
Deidentified data from this study are available on request, following submission of a valid research protocol to the corresponding author.
Ethics Approval and Informed Consent
The study was approved by independent ethics committees at each institution (see supplement). All patients provided written informed consent prior to any study-related procedure.
Acknowledgments
Dave Singh is supported by the National Institute for Health Research (NIHR) Manchester Biomedical Research Centre (BRC). The authors would like to thank the investigators and patients at the investigative sites for their support of this study. Writing support was provided by David Young of Young Medical Communications and Consulting Ltd. This support was funded by Verona Pharma plc.
Disclosure
HW reports personal fees from AstraZeneca, Bayer, BerlinChemie, Boehringer Ingelheim, GlaxoSmithKline, Novartis, and Roche, all outside the submitted work. KR and TR are employees of Verona, the sponsor of the study. TB reports personal fees from Verona, both during the conduct of the study and outside the submitted work. DS reports personal fees from Verona during the conduct of the study. Outside the submitted work, he reports personal fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, Genentech, GlaxoSmithKline, Glenmark, Menarini, Mundipharma, Novartis, Peptinnovate, Pfizer, Pulmatrix, Theravance, and Verona. The authors report no other conflicts of interest in this work.
References
1. Punekar YS, Mullerova H, Small M, et al. Prevalence and burden of dyspnoea among patients with chronic obstructive pulmonary disease in five European countries. Pulm Ther. 2016;2(1):59–72. doi:10.1007/s41030-016-0011-5
2. Kessler R, Partridge MR, Miravitlles M, et al. Symptom variability in patients with severe COPD: a pan-European cross-sectional study. Eur Respir J. 2011;37(2):264–272. doi:10.1183/09031936.00051110
3. Gruenberger J-B, Vietri J, Keininger DL, Mahler DA. Greater dyspnea is associated with lower health-related quality of life among European patients with COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:937–944. doi:10.2147/COPD.S123744
4. Banner KH, Press NJ. Dual PDE3/4 inhibitors as therapeutic agents for chronic obstructive pulmonary disease. Br J Pharmacol. 2009;157(6):892–906. doi:10.1111/j.1476-5381.2009.00170.x
5. de Boer J, Philpott AJ, van Amsterdam RG, Shahid M, Zaagsma J, Nicholson CD. Human bronchial cyclic nucleotide phosphodiesterase isoenzymes: biochemical and pharmacological analysis using selective inhibitors. Br J Pharmacol. 1992;106(4):1028–1034. doi:10.1111/j.1476-5381.1992.tb14451.x
6. Page CP, Spina D. Phosphodiesterase inhibitors in the treatment of inflammatory diseases. Francis S, Conti M, Houslay M, editors. In Phosphodiesterases as Drug Targets. Handbook of Experimental Pharmacology. Berlin, Heidelberg: Springer; 2011. 391–414. http://link.springer.com/10.1007/978-3-642-17969-3_17.:
7. Franciosi LG, Diamant Z, Banner KH, et al. Efficacy and safety of RPL554, a dual PDE3 and PDE4 inhibitor, in healthy volunteers and in patients with asthma or chronic obstructive pulmonary disease: findings from four clinical trials. Lancet Respir Med. 2013;1(9):714–727. doi:10.1016/S2213-2600(13)70187-5
8. Singh D, Abbott-Banner K, Bengtsson T, Newman K. The short term bronchodilator effects of the dual PDE3 and PDE4 inhibitor RPL554 in COPD. Eur Respir J. 2018;52(5):1801074. doi:10.1183/13993003.01074-2018
9. Bjermer L, Abbott-Banner K, Newman K. Efficacy and safety of a first-in-class inhaled PDE3/4 inhibitor (ensifentrine) vs salbutamol in asthma. Pulm Pharmacol Ther. 2019;58:101814. doi:10.1016/J.PUPT.2019.101814
10. Singh D, Abbott-Banner KH, Reid F, Newman K, Phase A. I, randomised, double blind, placebo controlled, study to assess the safety, tolerability and pharmacokinetics of multiple inhaled doses of RPL554 administered by nebuliser to healthy male subjects and stable COPD patients. Am J Respir Crit Care Med. 2016;193:A6838.
11. Singh D, Martinez FJ, Watz H, Bengtsson T, Maurer BT. A dose-ranging study of the inhaled dual phosphodiesterase 3 and 4 inhibitor ensifentrine in COPD. Respir Res. 2020;21(1):47. doi:10.1186/s12931-020-1307-4
12. Leidy NK, Murray LT, Monz BU, et al. Measuring respiratory symptoms of COPD: performance of the EXACT- Respiratory Symptoms Tool (E-RS) in three clinical trials. Respir Res. 2014;15(1):124. doi:10.1186/s12931-014-0124-z
13. Mahler DA, Witek TJ. The MCID of the Transition Dyspnea Index is a total score of one unit. COPD. 2005;2(1):99–103. doi:10.1081/COPD-200050666
14. Jones PW. St. George’s Respiratory Questionnaire: MCID. COPD. 2005;2(1):75–79. doi:10.1081/COPD-200050513
15. Janson C, Marks G, Buist S, et al. The impact of COPD on health status: findings from the BOLD study. Eur Respir J. 2013;42(6):1472–1483. doi:10.1183/09031936.00153712
16. Punekar YS, Wurst K, Shukla A. Resource use and costs up to two years post diagnosis among newly diagnosed COPD patients in the UK primary care setting: A retrospective cohort study. COPD J Chronic Obstr Pulm Dis. 2015;12(3):267–275. doi:10.3109/15412555.2014.933953
17. Jones PW, Leidy NK, Hareendran A, Lamarca R, Chuecos F, Garcia Gil E. The effect of aclidinium bromide on daily respiratory symptoms of COPD, measured using the Evaluating Respiratory Symptoms in COPD (E-RS: COPD) diary: pooled analysis of two 6-month Phase III studies. Respir Res. 2016;17(1):61. doi:10.1186/s12931-016-0372-1
18. Martinez FJ, Calverley PMA, Goehring U-M, Brose M, Fabbri LM, Rabe KF. Effect of roflumilast on exacerbations in patients with severe chronic obstructive pulmonary disease uncontrolled by combination therapy (REACT): a multicentre randomised controlled trial. Lancet. 2015;385(9971):857–866. doi:10.1016/S0140-6736(14)62410-7
19. Martinez FJ, Rabe KF, Sethi S, et al. Effect of roflumilast and inhaled corticosteroid/long-acting β2-agonist on chronic obstructive pulmonary disease exacerbations (RE2SPOND). A randomized clinical trial. Am J Respir Crit Care Med. 2016;194(5):559–567. doi:10.1164/rccm.201607-1349OC
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.