Back to Journals » Biologics: Targets and Therapy » Volume 19
Switch from Intravenous to Subcutaneous Formulation of Tocilizumab in Rheumatoid Arthritis: Retrospective Cohort Analysis and Systematic Literature Review
Authors Galoppini G ![]() , Garaffoni C, Lotesoriere A, Nogarin F, Bortoluzzi A, Govoni M, Silvagni E
, Garaffoni C, Lotesoriere A, Nogarin F, Bortoluzzi A, Govoni M, Silvagni E ![]()
Received 21 July 2025
Accepted for publication 29 October 2025
Published 4 December 2025 Volume 2025:19 Pages 713—727
DOI https://doi.org/10.2147/BTT.S555169
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Shein-Chung Chow
Giorgio Galoppini, Carlo Garaffoni, Andrea Lotesoriere, Federico Nogarin, Alessandra Bortoluzzi, Marcello Govoni, Ettore Silvagni
Department of Medical Sciences, Rheumatology Unit, University of Ferrara and Azienda Ospedaliero-Universitaria S. Anna, Cona (Ferrara), Italy
Correspondence: Marcello Govoni, Rheumatology Unit, Department of Medical Sciences, University of Ferrara and Azienda Ospedaliero-Universitaria S. Anna, 8 Aldo Moro Street, Cona (Ferrara), Italy, Tel +39 0532 236807, Email [email protected]
Purpose: Subcutaneous tocilizumab (SC-TCZ) is approved for rheumatoid arthritis (RA) management. During Severe Acute Respiratory Syndrome CoronaVirus 2 (SARS-CoV2) pandemics, experiences of intravenous (IV)-to-SC TCZ switch in RA patients spread. We aimed to determine SC-TCZ maintenance, efficacy and safety in IV-to-SC TCZ switchers, combining a single center, retrospective cohort study and a systematic literature review (SLR).
Patients and Methods: We included RA patients undergoing IV-to-SC TCZ switch (2015– 2024); patients were grouped and evaluated according to maintenance of SC-TCZ (“Go on SC” group, GoS) or returning to IV-TCZ within 12 months (T2) (“Back IV” group, BI). SC-TCZ maintenance, disease activity, adverse events (AEs) were evaluated; a univariate regression analysis was performed to evaluate factors associated with a successful switch. The SLR was performed in accordance with PRISMA 2.0 guidelines and registered in PRSPERO (ID CRD42024523714), to search for relevant articles regarding maintenance of SC-TCZ after IV-to-SC switch, efficacy (assessed both clinically and with clinimetric tools) and safety of this strategy, as well as predictors of a successful IV-to-SC switch.
Results: According to the success of SC-TCZ switch (T2), SC-TCZ maintenance rate was 43.3% (13/30 patients). A switch back to IV-TCZ was more likely if patients had higher baseline GH score (OR 1.05, 95% CI 1.01– 1.10), and less likely if the IV-to-SC switch was agreed with treating physician (0.03, 0.00– 0.21). At first visit after baseline, the mean DAS28 value diminished in GoS (− 0.3) versus BI (+0.5), p < 0.001. No treatment-related serious AEs were reported. The SLR retrieved 12 articles (3626 patients), including 2 open-label randomized controlled trials (RCTs) and 10 observational studies. By the end of follow-up, SC-TCZ maintenance in our cohort was lower than in other experiences (25.9% versus 78.7%), but with a longer follow-up (up to 4.5 years).
Conclusion: Intravenous to subcutaneous tocilizumab switch is an effective and safe option in rheumatoid arthritis management, especially in the case of a shared decision.
Keywords: non-therapeutical switch, biologic therapy, rheumatoid arthritis management, healthcare policies, systematic literature review
Introduction
Tocilizumab (TCZ) is a humanized monoclonal antibody directed against the human interleukin-6 receptor (IL-6R). In rheumatoid arthritis (RA), IL-6 has a pivotal role; synovial and serum IL-6 levels have been demonstrated to be increased compared to controls, correlating with disease course and articular bone damage.1 Through years, TCZ has accumulated relevant evidence in terms of efficacy in RA, at first as intravenous (IV) administration.2 To simplify patients’ management and reduce healthcare structures burden, a self-administrable subcutaneous (SC) formulation of TCZ was developed.3 Two randomized clinical trials (RCTs), SUMMACTA (worldwide)4 and MUSASHI (Japanese),5 demonstrated the non-inferiority of SC-TCZ with respect to IV-TCZ as part of a combination therapy or as monotherapy, respectively. Similar effectiveness of IV- and SC-TCZ was confirmed through a comprehensive analysis of data from European national registries.6 Although the most recent European Alliance of Associations for Rheumatology (EULAR) recommendations for the management of RA patients equally advise the use of biologic disease-modifying anti-rheumatic drugs (bDMARDs) with different mechanisms of action,7 in real world clinical practice rheumatologists start from tumor necrosis factor α (TNFα) inhibitors (TNFis) after methotrexate (MTX) failure,8,9 while other bDMARDs targeting T/B cells co-stimulation, CD20, or IL-6R are adopted after the failure of TNFis. Janus kinase (Jak) inhibitors prescription, instead, requires greater caution due to alerts on cardiovascular safety.10,11 Therefore, unless contraindications to TNFis exist, such as concomitant interstitial lung disease (ILD) or congestive heart failure (CHF), which drive the choice towards other bDMARDs,12 TCZ or sarilumab (SAR) are reserved for TNFis insufficient-responder patients. Accordingly, in this kind of patients, TCZ proved comparable efficacy with other non-TNFis bDMARDs, even without concomitant MTX,13,14 and safer than Jak inhibitors.15 Moreover, TCZ seems preferable when impaired kidney function, infectious and malignancy risks are a concern, while caution should be adopted for patients at risk of lower intestinal perforation. This is possibly due to the strong TCZ-mediated suppression of C-reactive protein (CRP), which may delay the diagnosis of acute diverticulitis.16 Attention should be paid also to decreased neutrophil and platelet counts, as well as cholesterol levels increases (although overall cardiovascular risk improves during TCZ therapy).17,18
Recently, TCZ has been licensed for the treatment of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) disease (COVID-19), among other indications.19 Indeed, SARS-CoV-2 can infect upper and lower airways, but the most dramatic cases are those characterized by an abnormal inflammatory response, which can lead to acute respiratory distress syndrome (ARDS) or cytokines release storm (CRS).20 Fostered by clinical trials and reports worldwide, the World Health Organization (WHO) promoted a metanalysis of past and ongoing trials exploring the role of TCZ in the management of severe COVID-19, demonstrating that IV-TCZ administration, along with glucocorticoids (GCs), reduced mortality and the need for invasive mechanical ventilation.21,22 This unprecedented request of IV-TCZ for patients in intensive care units caused shortage of stocks; therefore, clinicians, in accordance with national and local Health Authorities, suggested to switch rheumatological patients (mainly RA), treated with IV-TCZ, to SC-TCZ, to maintain disease control, avoiding therapy administration interruptions, as well as to keep immune-compromised patients away from potential in-hospital sources of SARS-CoV-2 infection.23,24 COVID-19 vaccines and remote contacts with patients by telemedicine interventions helped clinicians to this purpose,25 and, accordingly, this approach was adopted in a significant number of patients. However, the assessment of the outcome of this “non-therapeutical” switch has not been thoroughly investigated. Therefore, we combined a single center observational study with a systematic review of the literature (SLR), with the primary objective to assess the maintenance of SC-TCZ in RA patients with stable disease switching from IV-TCZ (for reasons different from inadequate disease control), along with the identification of clinical and demographic factors associated with a successful switch. Secondly, we explored the efficacy and safety of IV-to-SC TCZ switch and switch back to IV-TCZ.
Materials and Methods
Study Design
This study combined a single center, retrospective, observational study, and an SLR.
Ethics Considerations
The present study was performed following the principles of the Declaration of Helsinki Ethical Principles for Medical Research Involving Human Patients. The Independent Ethics Committee of the Area Vasta Emilia Centrale (AVEC) approved the study protocol (CE-AVEC 493–2023-Oss-AOUFe). All the patients enrolled signed the informed consent. Patients reported their ethnicity during personal history interviews.
Study Setting
We included patients with a clinical diagnosis of RA (according to expert opinion, satisfying 2010 ACR/EULAR classification criteria26), both male and female (sex distinction made for biological reports), over 18 years old, on treatment with monthly IV-TCZ for at least six-month, attending the tertiary-referral level Rheumatology Unit, Azienda Ospedaliero-Universitaria St. Anna, Ferrara (Italy). Patients enrolled switched to SC-TCZ at least once in their clinical history (between 2015 and 2024) for non-therapeutical reasons, and they were expected to attend at least one clinical visit during the subsequent follow-up period.
Study Procedures, Demographic and Clinical Variables Collected
Baseline demographics (age, sex, smoking habit), clinical (body mass index (BMI), disease duration, previous/concomitant GCs, conventional synthetic (cs-) or biological (b-) disease modifying anti-rheumatic drugs (DMARDs) use, IV-TCZ dose and starting date, main comorbidities), serological (autoantibodies (ie, rheumatoid factor (RF) and anti-cyclic citrullinated peptides (ACPA)), CRP, erythrocyte sedimentation rate (ESR), lipid profile), and instrumental (hands/feet radiographic erosions) characteristics were collected. Reasons for TCZ formulation modification included patients’ choice (in accordance with treating rheumatologist), or National Health Authorities dispositions (due to shortage of IV-TCZ stocks during COVID-19 pandemics). The main time-points considered were T0, defined as the time of IV-to-SC TCZ switch; T1 (first visit after the switch); T2 (visit of eventual switching back to IV-TCZ, if different from T1, within 12 months from T0); and T3 (end of follow-up and database lock, 15th September 2024) (Supplementary Figure S1).
Endpoints
We prospectively evaluated maintenance (expressed as the proportion of patients still receiving a specific medication at a definite timepoint, elsewhere referred to as “proportion of patients covered”)27 of SC-TCZ with respect to switch-back to IV-TCZ within 12 months from T0 (T2). Therefore, we grouped our patients according to their maintenance of SC-TCZ at T2 (“Go on SC” group, GoS) or their need to revert to IV-TCZ (“Back IV”, BI). If the treatment with TCZ had not been discontinued earlier, we censored retention at T3. Efficacy was measured as changes in disease activity score on 28 joints (DAS28)-ESR (or simply DAS28), a composite measure used in clinical practice as a proxy for RA course; it has been considered globally as well as in its sub-items (number of swollen and tender joints, ESR values, patient-reported global health (GH) assessment), in order to capture discrepancies between objectively assessable and patient-dependent outcomes. GH is assessed asking a patient how much RA has affected his/her health status in the last week; the score is expressed on a 100 mm visual analogue scale; higher values refer to worse health status.28 Here, DAS28 was calculated adopting ESR instead of CRP, because CRP values are normally within the range of normality during TCZ therapy even in patients with persistent synovitis, due to TCZ effects on IL-6-dependent inflammation. Safety was assessed measuring adverse events (AEs) and severe AEs (SAEs) incidence rates. An AE was defined as any clinical/laboratory abnormality, occurring during the treatment, whether or not it is considered related to the drug; an AE was deemed severe if life- threatening, organ-threatening or requiring hospitalization.29 Injection site reaction (ISR) was defined as any cutaneous lesion occurring within 4 hours on site of drug delivery.3
The efficacy of switch back to IV-TCZ was defined as achievement of a state of DAS28-ESR low-disease activity (LDA)/remission (REM), defined as DAS28 ≤2.6 and 2.6 ≤ 3.2, respectively, after switch-back to IV-TCZ.
Statistical Analysis
Continuous variables were reported as mean (standard deviation, SD) or as median (interquartile range, IQR) for non-normally distributed data, tested with Saphiro–Wilk test. Categorical variables were reported as absolute and relative frequencies. Baseline characteristics were compared using Wilcoxon sum rank test or Fisher’s exact test, according to their distribution; Chi-square or McNemar test, for categorical variables. Follow-up between groups differences in outcome measures have been analyzed through Wilcoxon signed rank test for continuous variables and McNemar test for categorical variables. A univariable logistic regression analysis was performed to explore the associations between baseline characteristics and switch back to IV-TCZ, and results were reported as odds ratios (ORs) and 95% confidence intervals (95% CI). Statistical analysis was performed with RStudio©.30
Systematic Literature Review
An SLR was conducted according to the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA 2.0) statements (Supplementary Table S1).31 The SLR was registered in PROSPERO (ID CRD42024523714) on 25th March 2024.
The search was performed in Medline and Embase databases, using the keywords “rheumatoid arthritis”, “intravenous tocilizumab”, “subcutaneous tocilizumab”, “switch route of administration”, “maintenance”, “efficacy”, “safety”. Review questions regarded the maintenance, efficacy and safety of IV-to-SC TCZ switch (and SC-to-IV TCZ switch back), and the search for clinical predictors of successful switch. To measure these outcomes, we considered the following variables in the included studies: (i) proportion of patients still on SC-TCZ at the end of study for maintenance,27 (ii) DAS28-ESR/-CRP, Clinical Disease Activity Index (CDAI) or Simplified Disease Activity Index (SDAI) for efficacy,28 (iii) AEs/SAEs incidence rate for safety.29 To maximize the inclusivity, articles were screened according to three Population, Intervention, Comparison/Control, Outcome, and Study design (PICOs) frameworks (Supplementary Methods).
Reports published until 25th March 2024 were included, in English or Italian. Types of studies included SLRs and meta-analyses, RCTs, non-controlled trials, cohort studies, cross-sectional studies, case-control studies, case series (>5 patients), conference abstracts (back to 2022) (Supplementary Methods). Risk of bias was assessed according to the National Heart, Lung and Blood Institute (NHLBI) risk-of-bias tool32 for any type of study, and rated as high, low or unclear.
Articles retrieved were managed with a dedicated software, Zotero;33 after duplicates deletion, retained articles were screened based on (i) title and abstract, (ii) full text and (iii) screening of the reference lists from the selected studies by three independent reviewers (GG, FN, AL); in case of disagreement, a fourth reviewer (ES) was asked to solve the dispute. Data retrieved from included articles, organized in tables, pertained to study characteristics, clinical-demographic population characteristics, outcomes (drug maintenance, predictive factors, switch efficacy, safety).
Study characteristics and outcomes were extracted based on “summary of evidence” tables. Since included studies showed high heterogeneity in terms of groups of patients compared, times of assessment, and endpoints considered, a metanalysis of the outcome measures was not deemed feasible.
Results
Patients’ Characteristics and Maintenance of SC-TCZ
As of 15th September 2024, 45 RA patients had been in treatment with IV-TCZ for at least 6 months; 30 of them met inclusion criteria and were evaluated at baseline (T0) and after mean (SD) 4.6 (2.4) months from the IV-to-SC switch (T1). At T1, 33.3% (10/30) patients switched back to IV-TCZ, followed by 7 patients after 0.7 months (IQR 0.5–1.8). Therefore, within 12 months (T2), 13/30 patients still maintained SC route and were grouped as GoS, while 17/30 patients needed to switch back to IV route of administration (BI group). At T2, SC-TCZ maintenance rate was 43.3% (13/30 patients).
Baseline demographic and clinical characteristics did not significantly differ between the two groups (Table 1). However, reasons for switching route of administration significantly differed, being “personal preference” prevalent among GoS (9/13, 69.2%), while “IV-TCZ shortage during COVID-19 pandemics” prevailed among BI patients (16/17, 94.1%), p < 0.001. By the end of data collection (T3), SC-TCZ maintenance was 25.9% (7/27 patients; 3 patients were lost to follow-up and 2 of them died (unknown cause)). Overall, SC-TCZ retention rate was 0.4 (IQR 0.3–2.8) years, significantly conditioned by the need to revert IV-TCZ at an average 3.7 (3.0–4.0) months. On the other hand, GoS patients continued to receive SC-TCZ for average 4.5 (1.9–4.9) years.
 |
Table 1 Baseline Characteristics of Ferrara Cohort. Data Refers to RA Patients Switching from IV-TCZ to SC-TCZ Between 2015 and 2024 (N = 30) |
Clinical-Demographic Factors Associated with IV-TCZ Switch Back
Patients were less likely to revert to IV-TCZ if the decision of the IV-to-SC switch was agreed with the treating rheumatologist per personal preference (OR 0.03, 95% CI 0.00–0.21, p = 0.003); higher baseline GH values associated with a greater risk of switching back to IV-TCZ (OR 1.05, 1.01–1.10, p = 0.034). BMI, combination therapy with MTX or GCs, and the other clinical factors assessed did not significantly associate with the need to revert to IV-TCZ (Figure 1 and Table S2).
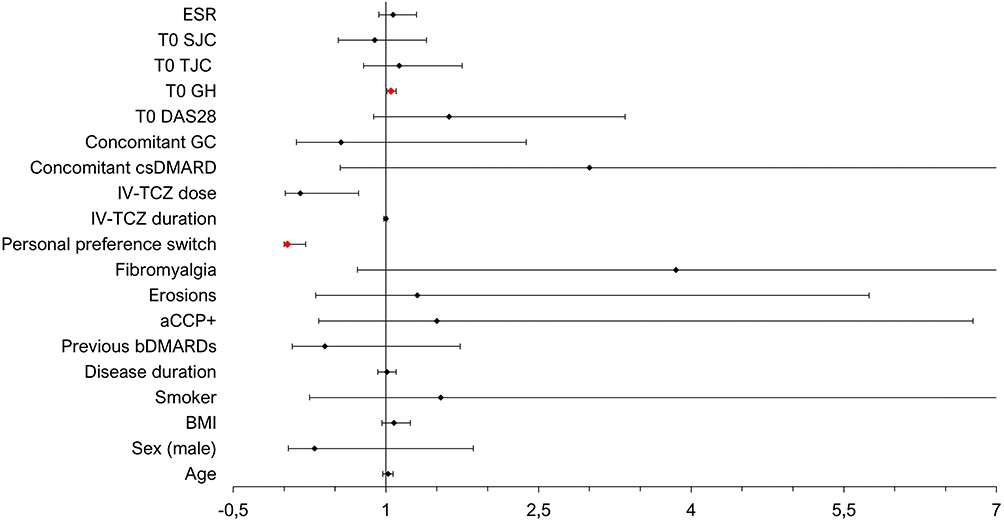 |
Figure 1 Univariate analysis showing odds ratios (with 95% confidence intervals) for switching back to IV-TCZ (lower probability towards left side, higher probability towards right side). Red dots represent statistically significant associations. |
Efficacy
At baseline, 24/30 (80.0%) were on remission or low disease activity (LDA) according to DAS28 definition. Mean (SD) DAS28 values changed from 2.0 (1.3) at T0 to 2.1 (1.3) at T1. In GoS group, mean (SD) DAS28 decreased from T0 to T1 (1.6 (1.4) vs 1.3 (0.9)), while mean DAS28 increased in BI in the same timeframe (2.3 (1.1) vs 2.8 (1.1)) (Figure S2). T1 DAS28 values significantly differed between GoS and BI groups (p < 0.001). Focusing on DAS28 sub-items, we found they all decreased in GoS, while they increased in BI group; this difference was statistically significant when patient-dependent parameters were considered (GoS vs BI: GH 23.8 (24.7) vs 55.9 (13.7), p = 0.01; average TJC 0.0 (IQR 0.0–0.0) vs 2.0 (1.0–4.0), p = 0.01). At T3, DAS28 values were consistent with a state of remission in both groups (2.0 (1.2) for GoS, 2.2 (0.9) for BI).
Safety
Overall, AEs incidence rate was low (28.8/100 PY). The interval between T1 and T3 was considered for GoS patients, to evaluate specifically the safety of SC-TCZ after the switch; we registered an AEs rate of 10.3/100 PY (of which 2.6/100 PY of infectious nature).
The interval T2-T3 allowed us to evaluate the safety of IV-TCZ after the switching back; we observed 42.9/100 PY AEs (27.3/100 PY were infections) in this group.
No SAEs related to TCZ were recorded.
Efficacy of SC-to-IV Switch Back
At T1, 19 (63.3%) patients formally kept disease control, although 8 switched back to IV-TCZ, while 5 patients worsened to MDA and all reverted to IV-TCZ (Figure 2). Two patients improved from MDA at T0 to LDA/REM at T1; nonetheless, 1 patient returned to IV route. Eventually, 4 patients persisted in MDA at T1; 3 switched back to IV-TCZ by T1, while the last one subsequently developed an injection site reaction and switched to SAR.
 |
Figure 2 Flow chart of patients’ disease course, according to DAS28 value, and ongoing treatment at different timepoints, throughout the observation timeframe. 3 patients were lost to follow up: among those, 1 was lost to follow up after T2 (*), 2 patients died for unknown cause before T3 (**). |
Among the 8 out of 17 patients (47.1%) who were in MDA at T1 and switched back to IV-TCZ, 6 out of 8 achieved LDA at T3 while still receiving IV-TCZ. 2 out of 8 patients were receiving other b/tsDMARDs at T3; however, these treatment changes occurred approximately 1.6 years after the switch back to IV-TCZ. 1/8 patient was lost to follow up. The 9/17 (52.9%) patients already in LDA/REM at T1 maintained disease control at T3, except for 1/9 patient who therefore switched to baricitinib after 2.1 years; 1/9 patient switched to SAR after 3.7 years from T2.
Systematic Literature Review
The search retrieved 582 non-duplicated references (Pubmed 65, Embase 577), and 12 articles were included (five from Embase,6,24,34–36 one from PubMed,37 six from both4,5,38–41), with a total of 3626 patients (1364 underwent IV-to-SC switch) (Figure 3). Agreement between reviewers was judged qualitatively and considered acceptable for the purposes of this study. Extracted data were summarized in Supplementary Tables S3, S4 and S5.
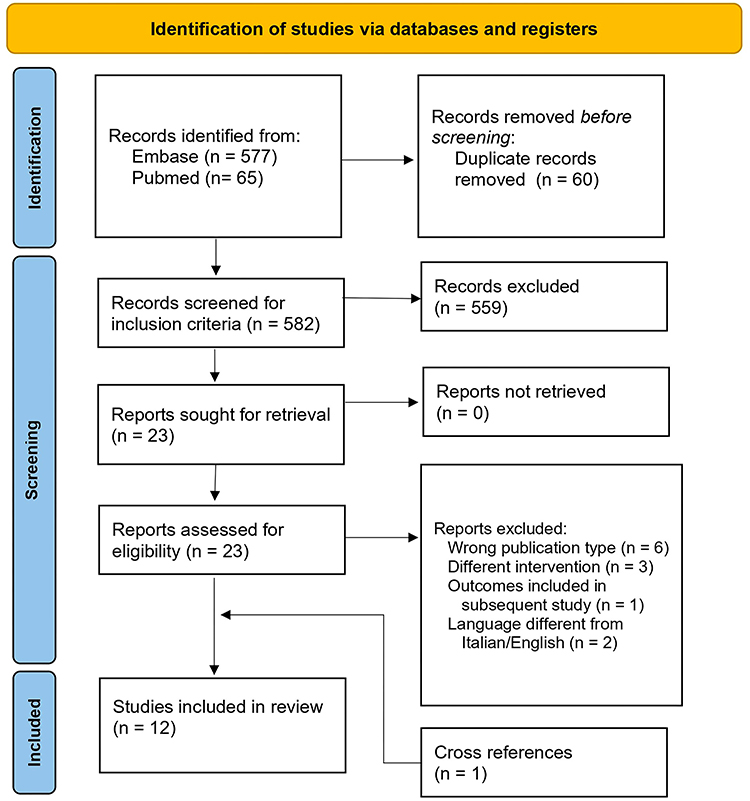 |
Figure 3 PRISMA 2.0 flow-chart of records inclusion strategy. |
According to the NHLBI risk of bias tool, the quality of included records was acceptable (Figure 4). Included observational studies (10/12 (83.3%)) lacked especially a thorough baseline case series/cohort description, the application of objective and standardized outcome measures; methodological explanations (eg, significance thresholds). As expected by the open label design, in none of the 2 RCTs included neither the patients nor the physicians were blinded to the assignment group.
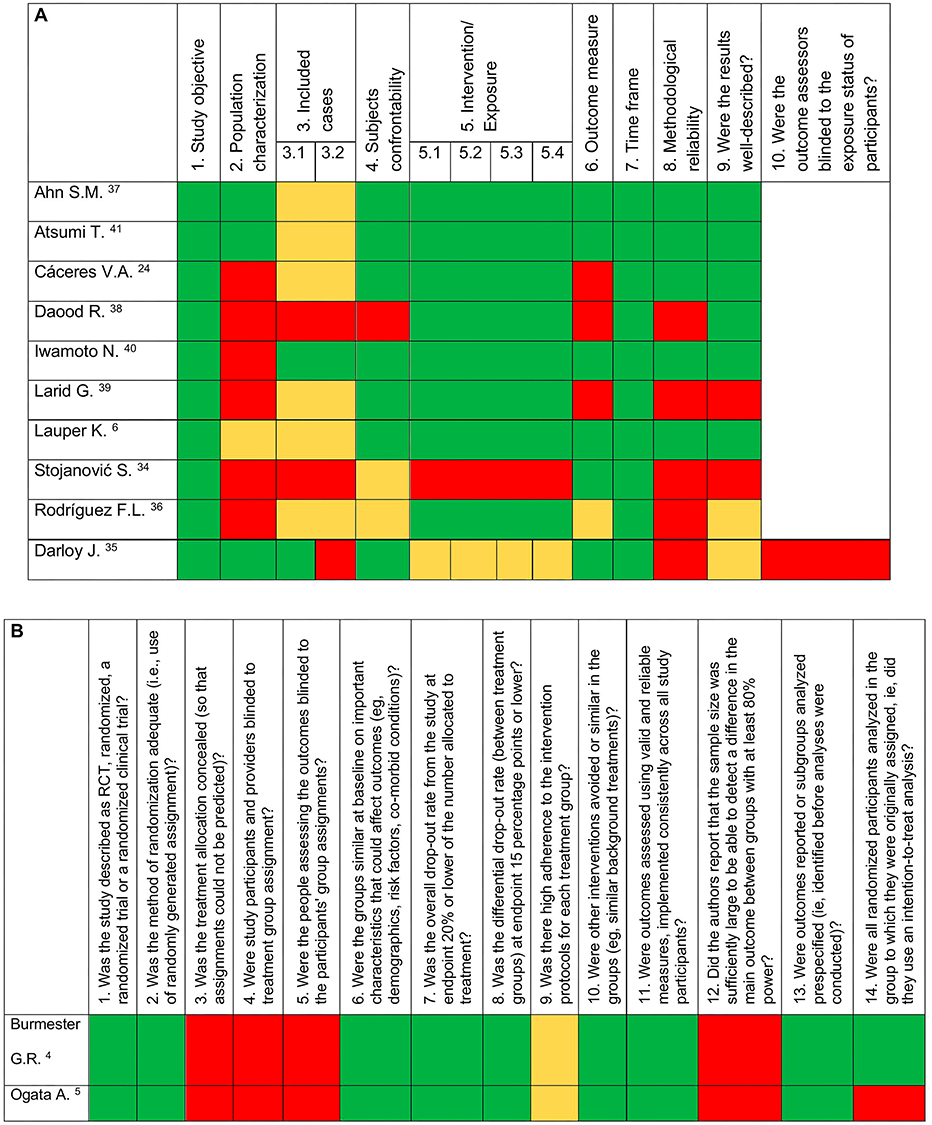 |
Figure 4 Risk of bias assessment (assessed adopting National Heart, Lung and Blood Institute risk-of-bias tool) for observational studies (A) and RCTs (B). (A) Some questions have different meanings whether referring to generic observational (a) or cohort (b) studies: 1. (a, b) Was the study question or objective clearly stated? 2. (a) Was the study population clearly and fully described, including a case definition? (b) Was the study population clearly specified and defined? 3. (a) Were the cases consecutive? 3.1 (b) Was the participation rate of eligible persons at least 50%? 3.2 (b) Was loss to follow-up after baseline 20% or less? 4. (a) Were the subjects comparable? (b) Were all the subjects selected or recruited from the same or similar populations (including the same period)? (a, b) Were inclusion and exclusion criteria for being in the study prespecified and applied uniformly to all participants? 5. (a) Was the intervention clearly described? 5.1 (b) For the analyses in this paper, were the exposure(s) of interest measured prior to the outcome(s) being measured? 5.2 (b) Was the exposure(s) assessed more than once over time? 5.3 (b) For exposures that can vary in amount or level, did the study examine different levels of exposure as related to the outcome (eg, categories of exposure, or exposure measured as continuous variable)? 5.4 (b) Were the exposure measures (independent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? 6. (a) Were the outcome measures clearly defined, valid, reliable, and implemented consistently across all study participants? (b) Were the outcome measures (dependent variables) clearly defined, valid, reliable, and implemented consistently across all study participants? 7. (a) Was the length of follow-up adequate? (b) Was the timeframe sufficient so that one could reasonably expect to see an association between exposure and outcome if it existed? 8. (a) Were the statistical methods well-described? (b) Was a sample size justification, power description, or variance and effect estimates provided? 9. (a) Were the results well-described? (b) Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)?. |
Maintenance
A descriptive synthesis of the main outcomes, compared to our cohort, is provided in Table 2; We reported SC-TCZ retention rate after switching from studies for which maintenance was not available. The proportion of patients still on SC-TCZ after a period (variable according to specific study) from non-therapeutic switch was reported in 9/12 studies, assessed after mean (SD) 10.1 (5.3) months, varying from 30.0% to 100.0% (mean 78.7, SD 21.2%). Maintenance was equal to/higher than 75th centile (93.7%) in 2 studies conducted between 2010 and 2015,5,40 and 1 in 2021,34 while it was equal to/lower than 25th centile (72.1%) in 3 retrospective observational studies, all conducted between 2022 and 2023.24,37,38 IV-to-SC switch happened during COVID-19 pandemics in 4/12 cases:24,34,36,38 maintenance varied from 30.0% to 100.0%. In 8/12 cases, the switch occurred for reasons other than pandemics: while efficacy outcomes varied greatly, drug maintenance was ≥70.3%.
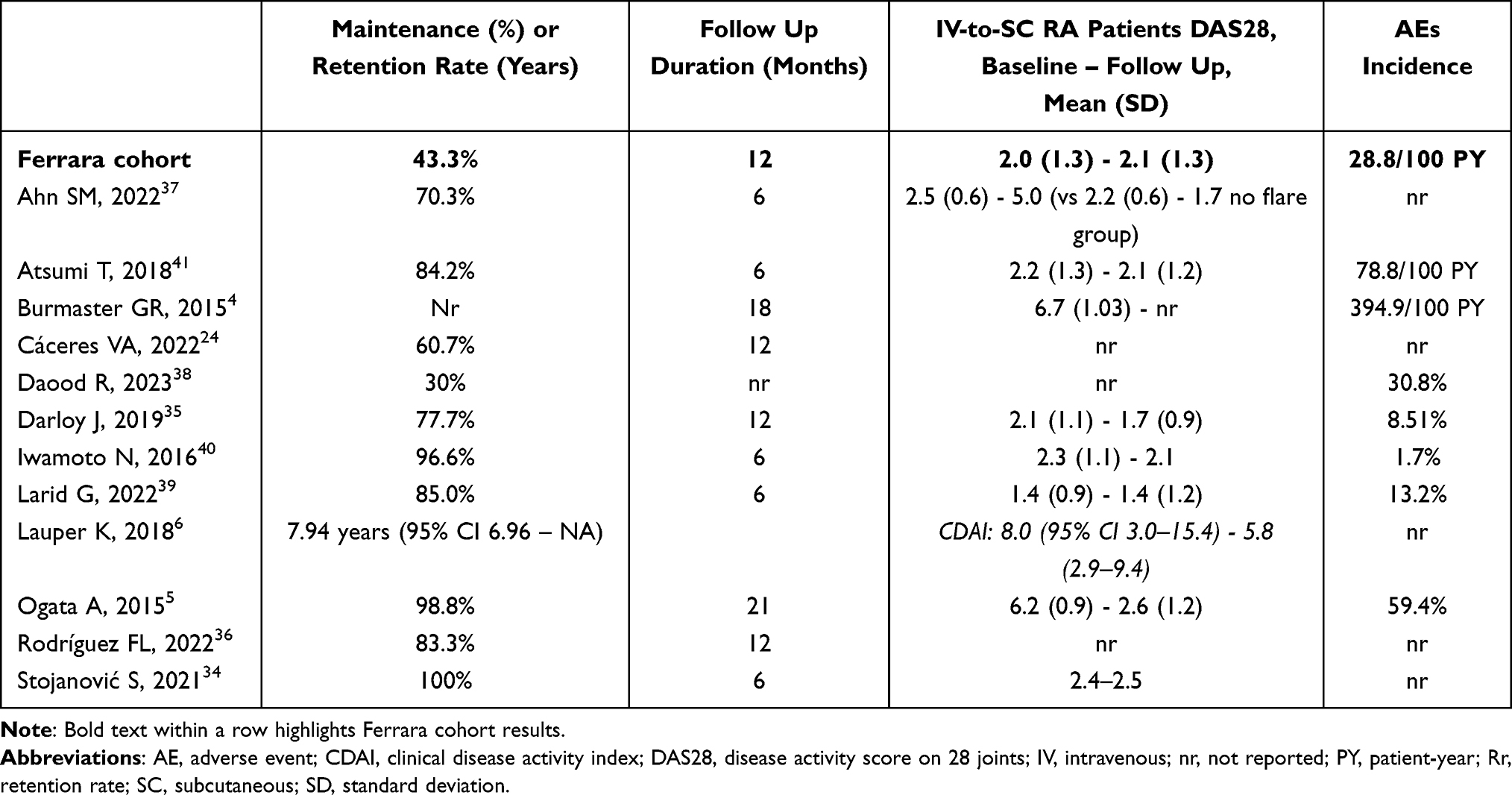 |
Table 2 Comparison of Outcomes Between Our Cohort and Studies from the SLR |
Factors Associated with IV-TCZ Switch Back
In only 1 out of 4 studies exploring the role of body mass or mass index, the proportion of patients in clinical remission decreased in those patients weighting more than 70 kg (from a baseline 72.7% to 27.3% at the end of follow-up) and/or BMI >25 kg/m2 (from 66% to 46%), while the proportion remained stable in other weight groups.5 Two studies confirmed that patients receiving SC-TCZ monotherapy were more likely to have an arthritic flare (OR, 8.53; 95% CI, 1.21–60.40; p = 0.03)37 or to switch back to IV-TCZ,24 with respect to those receiving combination therapy with MTX.
On the other hand, 2 studies found the presence of rheumatoid nodules, duration of IV-TCZ therapy, baseline DAS28 > 3.2,35 as well as male sex, high body mass and concomitant GCs39 to be associated with a physician propensity to continue TCZ intravenously.
Efficacy
In included studies, efficacy was defined according to different definitions, like REM/LDA maintenance, DAS28 or CDAI response, disease flare occurrence, symptoms worsening. In 2/4 studies, the proportion of efficaciously treated patients diminished in switching group (from 82.5% to 79.4%5 and from 81.9% to 73.3%35), compared to an increase in the control SC-to-SC (from 66.5% to 71.5%5), and IV-to-IV (from 59.5% to 70.3%35) groups. In 1/4 study, efficacy trend was confirmed both in IV-to-SC switching (from about 37% to 55.6%) and control groups (IV-to-IV patients; from 37% to 46.4%).4 Three out of 12 studies reported that IV-TCZ was successfully re-established in >80.0% of unsatisfied IV-to-SC switching patients.24,36,37
Safety
Overall, incidence of AEs in IV-to-SC switchers was reported in 8/12 studies, varying from 1.7% (1 common flu among 58 patients)40 to 59.4% (mainly of infectious nature).5 When a comparator group was present, incidence of AEs in switching group was equal/inferior to the former, except for a higher incidence of ISR (which brought to drug withdrawal in only 1 case4). Incidence of SAEs was even lower, reported in only 4/8 studies, varying between 4.1%41 and 5.3%.39 Even when incidence of SAEs was higher in IV-to-SC group than in control group (ie, IV-to-IV patients),4 the difference was non statistically significant.
Discussion
The massive adoption of IV-TCZ for severe COVID-19 has recently stimulated the spreading of studies regarding the safety and effectiveness of IV-to-SC TCZ switch in the context of autoimmune diseases, included RA. We assessed the maintenance rate of SC-TCZ following the switch, demonstrating that higher baseline GH values, as well as a superimposed “not therapeutical” condition for switching, associated with the necessity to revert to IV-TCZ. However, as demonstrated by the SLR performed, IV-to-SC TCZ switch remains a safe and efficacious option, particularly if a shared decision pathway is guaranteed.
The SARS-CoV-2 disease pandemic significantly impacted on IV-TCZ persistence. Six out of 11 records retrieved by this SLR dated after January 2021, while 3 out of the remaining 5 dated before 2016, likely fostered by the availability of SC-TCZ in Europe. Even in our cohort, most IV-to-SC switches (66.7%) took place between 2020 and 2021: this context, which forced a therapeutic strategy not completely shared with patients, may have conditioned a 1-year maintenance of 43.3%, as a nocebo effect.23 Likewise, studies published after 2020 report a maintenance lower than the global mean of 78.7%; the only exception is represented by the work by Stojanović at al. with a retention rate of 100%.34 However, this study lacked a thorough population characterization, as well as the description of baseline and follow-up characteristics of the IV-to-SC subgroup. Adherence to therapy is a significant determinant of maintenance, even more pivotal than the therapy decision itself, frequently influenced by patient’s opinions and thoughts. In a previous study, patients were asked why they preferred IV route of administration over SC (or vice versa); surprisingly, when patients had the possibility to share therapeutic decisions and their opinions with clinicians, they preferred to continue receiving the drug through the same administration route they have been thus far, without any significant socio-economic/educational predictive factor for this preference.42 This substantially confirms the experience described in our study, highlighting a lower IV-to-SC TCZ switch success for cases occurring under healthcare rules super-imposition. Of course, since the two routes of administration already proved pharmacodynamic overlap,3 we expected clinical response to SC-TCZ to differ from IV-TCZ for non-pharmacological reasons. Patients could make mistakes in self-administering SC formulation, which could impair drug’s pharmacokinetic properties; on the other hand, the possibility to self-administer TCZ at home could avoid the risk of missing an infusion due to logistic reasons (ie, inability to reach the hospital).
According to previous meta-analyses which confirmed that TCZ and abatacept (ABA) efficacy is not conditioned by fat tissue distribution, our analysis confirmed a lack of association between BMI and the need to revert to IV-TCZ. This was confirmed also in the studies included in the SLR, with one only exception.5
As expected from RCTs and observational studies, and confirmed by this SLR, TCZ effectiveness was retained after switching from IV to SC formulation, with mean DAS28 values stably lower than 3.2, the threshold for MDA. However, taking into account GoS and BI groups separately, we showed a decrease in DAS28 values in the former, and an increase in the latter group, with 5 patients reaching the MDA status, mostly driven by TJC and GH sub-items. This finding specifically reinforces the impact of patient reported outcomes, like GH, and their potentially confounding effects on disease activity assessment and treatment decisions-making.43,44 Furthermore, this was confirmed by the finding that baseline GH significantly associated with the need to revert to IV-TCZ during the follow-up.
Since public health policies seek to lighten the load on major hospitals by moving most services to outpatient facilities, it appears reasonable to question whether IV-bDMARDs will still be an option, given the availability of similarly efficacious SC analogues. In fact, the TOCERRA project highlighted a preference toward SC instead of IV route for RA patients starting TCZ since 2015.6 However, the problem for the patient could be the change of administration route in the case of successful treatment, rather than the administration route itself. This was demonstrated with IV-to-SC ABA, as well, since, in a single center study, 27.5% of RA patients switched to SC-ABA returned to IV-ABA within 90 days, and this permitted to regain disease control in 1 month.45 On the other hand, the necessity to switch back could be due to the lower presence of MTX co-therapy.45 Accordingly, also in one study retrieved by this SLR, RA patients in SC-TCZ monotherapy flared more frequently than those in combination therapy.37 Conversely, in our cohort, no significant difference was retrieved in the case of TCZ monotherapy or combination with MTX or GCs. It should be underlined that the comparative effectiveness of TCZ and ABA as monotherapy differs widely, and our analysis was not powered to demonstrate a difference between combination with csDMARDs and monotherapy.46 Besides, it is noteworthy that all willful switches in our cohort happened before COVID-19 pandemics. Among those who started IV-TCZ after the end of the pandemics, only one switched to SC-TCZ and was able to maintain SC-TCZ till T3. This low rate of switch proposal could be explained by clinicians’ feeling of a low success rate, as well as by the decision not to modify an effective treatment strategy for patients demonstrating to tolerate it. On the other hand, IV formulation still maintains its rationale for difficult or comorbid patients, for whom a tighter follow-up is optioned.47
Another option for IL-6 interception in RA includes SAR, structurally similar to TCZ and with a similar mechanism of action. However, being TCZ-responders did not predict a response to SAR. In a prospective study, in fact, TCZ-to-SAR switch, not compelled by a clinical need (eg, loss of disease control), resulted in increase in disease activity and low persistence rates.48 In a pandemic scenario, the possibility of switching patients receiving IV-TCZ to SAR was intriguing, since SAR is not as effective for the treatment of COVID-19 affected patients as it is for rheumatologic patients,49 but performed in only 2 patients of our cohort, precluding a formal comparison.
Given the comparable safety between IV and SC TCZ from international studies, we did not expect an increase in AEs rate after the non-therapeutical switch. Accordingly, the rate of AEs in GoS patients was in line with results from the SLR regarding TCZ switchers, except for ISR, which was observed in only one case in our cohort. AEs incidence was higher in BI patients; a tighter follow up, with monthly outpatient visits, in IV-TCZ treated RA patients, compared to an average 6-monthly schedule for SC-TCZ treated patients, might explain this disproportion: therefore, a reporting bias could be present, particularly for infections.50 A similar reporting disproportion between IV and SC formulation of a bDMARD emerged also in one study on infliximab.51
Our study has some limitations. First, we were not able to grant patients’ compliance to SC-TCZ, since a low adherence rate could explain the relief after the re-establishment of IV route. Second, the lag between T2 and T3 did not allow us to weigh the short-term effect of the switch back to IV-TCZ against a placebo effect. Moreover, we did not measure other composite measures like CDAI, nor the patient’s satisfaction with disease control52 or the function,53 therefore we are not able to objectively quantify the impact of more subjective facets of disease. We neither documented using ultrasound whether there was active synovitis in the case of flares, despite this technique gained superiority over clinical assessment in recognizing synovitis.54 Again, the sample size of the single center analysis was low, and we included 6/30 patients with moderate disease activity at baseline, in apparent opposition to treat-to-target strategy.55 However, all but one of these patients switched to SC-TCZ during pandemics, which interfered with routine treat-to-target strategy.56 We did not include a control group with patients continuing IV TCZ, since it was out of the scope of this work. Though the IV-to-SC switch is not actually recommended by guidelines, during the pandemic breakout (from March 2020 to December 2022) it was proposed to all the patients for whom TCZ was deemed appropriate. Between 2015 and 2020, instead, 15 RA patients received IV-TCZ but were not proposed to switch to SC formulation: (i) one had switched from SC-to-IV TCZ; (ii) 5 were lost to follow up; (iii) 9 changed mechanism of action because of primary (2/9) or secondary (5/9) insufficient response, or for other clinical reasons (2/9). Regarding the SLR, outcome measures were heterogeneous, study designs of included articles were mainly observational and retrospective, and IV-to-SC switch was not always the main focus.
Overall, the included studies were well-conducted and did not report significant limits due to application of the study protocols to real life, not even those studies conducted during SARS-CoV2 pandemic. Therefore, neither our work was affected by real world issues.
Nonetheless, strengths of our study rely on a thorough examination of clinical characteristics of the patients and associations with a successful switch, as well as on the long follow-up available. Moreover, to the best of our knowledge, this is the first systematization of available evidence regarding IV-to-SC TCZ switch in RA, thus it will provide a useful reference for clinicians in the management of RA patients treated with IV-TCZ willing to simplify their therapeutic strategy. This will provide a cornerstone for future research as well, pointing out the limits of using heterogeneous efficacy measures and the advisability/importance of focusing on non-pharmacological ways to improve patients’ adherence to a specific treatment. Besides the clinical consequences of this SLR, we emphasize the importance of reporting both medication maintenance and retention rate, since the latter surely addresses both therapy efficacy and safety, but does not inform on the number of patients who will likely get these therapeutic benefits (as maintenance does).
Conclusions
Intravenous to subcutaneous tocilizumab switch emerges as a strategy that needs to be shared with the patient: this is more crucial than other clinical factors supposed to predict the success of this therapeutic strategy. Despite heterogeneity in efficacy assessments and outcomes among retrieved literature studies, patients undergoing intravenous to subcutaneous tocilizumab switch are able to maintain the subcutaneous route of administration in a significant proportion of cases. This is of utmost importance to avoid changing a useful drug, especially for difficult-to-treat RA patients who have already failed other therapeutic options. Switching remains an efficacious and safe option and switching back to intravenous route allows to regain disease control for patients unwilling to continue subcutaneous tocilizumab or experiencing a worsening of disease activity measures.
Abbreviations
ABA, abatacept; ACPA, anti-cyclic citrullinated peptides; (S)AE, (severe) adverse event; ARDS, acute respiratory distress syndrome; b, biologic; BI, back (to) intravenous tocilizumab; BMI, body mass index; CI, confidence interval; CRP, C reactive protein; CRS, cytokines release storm; cs, conventional synthetic; DAS28, disease activity score on 28 joints; DMARD, disease modifying anti-rheumatic drugs; ESR, erythrocyte sedimentation rate; GC(s), glucocorticoid(s); GH, global health; GoS, go on subcutaneous tocilizumab; IQR, interquartile range; ISR, injection site reaction; IV, intravenous; Jak, Janus kinase; LDA, low disease activity; MDA, moderate disease activity; MTX, methotrexate; OR, odds ratio; PY, person year; RA, rheumatoid arthritis; RCT, randomized clinical trial; REM, remission; RF, rheumatoid factor; SAR, sarilumab; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; SC, subcutaneous; SD, standard deviation; SLR, systematic literature review; TCZ, tocilizumab; WHO, World Health Organization.
Data Sharing Statement
All data are available on appropriate request from the corresponding author.
Ethics Approval and Informed Consent
The present study was performed following the principles of the Declaration of Helsinki Ethical Principles for Medical Research Involving Human Patients. The Independent Ethics Committee of the Area Vasta Emilia Centrale (AVEC) approved the study protocol (CE-AVEC 493-2023 Oss-AOUFe).
Consent for Publication
All the patients enrolled signed the informed consent. No personal picture no video of included patients has been recorded for this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. All the authors agree to be personally accountable for the author’s own contributions and for ensuring that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and documented in the literature.
Funding
No specific funding was received from any bodies in the public, commercial or not-for-profit sectors to carry out the work described in this article.
Disclosure
Prof. Dr. Alessandra Bortoluzzi reports speaker fee from GSK and AstraZeneca, outside the submitted work. ES has received research support from AbbVie and Lilly and consulting/speaker’s fees from AbbVie, Alfa-Sigma, Lilly, UCB, Novartis, Astra Zeneca.
MG has received fees for sponsorized lectures from Alfa-Sigma, Abbvie, Eli Lilly, Astra Zeneca, GSK, UCB. The other authors declare no conflicts of interest.
References
1. Baillet A, Gossec L, Paternotte S, et al. Evaluation of serum interleukin-6 level as a surrogate marker of synovial inflammation and as a factor of structural progression in early rheumatoid arthritis: results from a French national multicenter cohort. Arthritis Care Res. 2015;67(7):905–912. doi:10.1002/acr.22513
2. Zhang X, Peck R. Clinical pharmacology of tocilizumab for the treatment of patients with rheumatoid arthritis. Expert Rev Clin Pharmacol. 2011;4(5):539–558. doi:10.1586/ecp.11.33
3. Zhang X, Chen YC, Fettner S, et al. Pharmacokinetics and pharmacodynamics of tocilizumab after subcutaneous administration in patients with rheumatoid arthritis. Int J Clin Pharmacol Ther. 2013;51(8):620–630. doi:10.5414/CP201904
4. Burmester GR, Rubbert-Roth A, Cantagrel A, et al. A randomised, double-blind, parallel-group study of the safety and efficacy of subcutaneous tocilizumab versus intravenous tocilizumab in combination with traditional disease-modifying antirheumatic drugs in patients with moderate to severe rheumatoid arthritis (SUMMACTA study). Ann Rheum Dis. 2014;73(1):69–74. doi:10.1136/annrheumdis-2013-203523
5. Ogata A, Tanimura K, Sugimoto T, et al. Phase III study of the efficacy and safety of subcutaneous versus intravenous tocilizumab monotherapy in patients with rheumatoid arthritis. Arthritis Care Res. 2014;66(3):344–354. doi:10.1002/acr.22110
6. Lauper K, Santos MJ, Ianonne F, et al. Comparative effectiveness of subcutaneous versus intravenous tocilizumab in a paneuropean collaboration of registries. Ann Rheum Dis. 2018;77((Lauper K.; Courvoisier D.S.; Gabay C.) Rheumatology, University Hospitals of Geneva, Geneva, Switzerland):606. doi:10.1136/annrheumdis-2018-eular.2886
7. Smolen JS, Landewé RBM, Bergstra SA, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheum Dis. 2023;82(1):3–18. doi:10.1136/ard-2022-223356
8. Zhao SS, Kearsley-Fleet L, Bosworth A, Watson K, Hyrich KL. Effectiveness of sequential biologic and targeted disease modifying anti-rheumatic drugs for rheumatoid arthritis. Rheumatology. 2022;61(12):4678–4686. doi:10.1093/rheumatology/keac190
9. Carrara G, Argnani L, Zanetti A, et al. Persistence of bDMARD therapy in rheumatoid arthritis after first-line TNF-inhibitor failure: the RECORD study of the Italian Society for Rheumatology. Scand J Rheumatol. 2022;51(5):363–367. doi:10.1080/03009742.2021.2003033
10. Tian Z, Kearsley-Fleet L, Galloway J, et al. Potential impact of European Medicines Agency measures to minimize risk of serious side effects on JAKi prescribing and utilization in the UK. Rheumatology. 2025;64(3):1453–1458. doi:10.1093/rheumatology/keae279
11. Silvagni E, Bortoluzzi A, Occhino G, et al. Frailty and cardiovascular safety of JAK inhibitors versus TNF inhibitors in rheumatoid arthritis: a real-world comparative study of drug effects and patient profiles. Front Pharmacol. 2025:16. doi:10.3389/fphar.2025.1565909
12. Antoniou KM, Distler O, Gheorghiu AM, et al. ERS/EULAR clinical practice guidelines for connective tissue disease-associated interstitial lung diseaseDeveloped by the task force for connective tissue disease-associated interstitial lung disease of the European Respiratory Society (ERS) and the European Alliance of Associations for Rheumatology (EULAR)Endorsed by the European Reference Network on rare respiratory diseases (ERN-LUNG). Eur Respir J. 2025:2500896. doi:10.1183/13993003.02533-2024
13. Gottenberg JE, Brocq O, Perdriger A, et al. Non–TNF-targeted biologic vs a second anti-TNF drug to treat rheumatoid arthritis in patients with insufficient response to a first anti-TNF drug: a randomized clinical trial. JAMA. 2016;316(11):1172–1180. doi:10.1001/jama.2016.13512
14. Sparks JA, Harrold LR, Simon TA, et al. Comparative effectiveness of treatments for rheumatoid arthritis in clinical practice: a systematic review. Semin Arthritis Rheum. 2023;62:152249. doi:10.1016/j.semarthrit.2023.152249
15. Miyazaki Y, Nakayamada S, Tanaka H, et al. Comparison of anti-IL-6 receptor and JAK inhibitors in patients with rheumatoid arthritis from the real-world practice FIRST registry. Rheumatology. 2025;64(4):1627–1636. doi:10.1093/rheumatology/keae334
16. Sepriano A, Kerschbaumer A, Bergstra SA, et al. Safety of synthetic and biological DMARDs: a systematic literature review informing the 2022 update of the EULAR recommendations for the management of rheumatoid arthritis. Ann Rheum Dis. 2023;82(1):107–118. doi:10.1136/ard-2022-223357
17. Generali E, Carrara G, Selmi C, et al. Comparison of the risks of hospitalisation for cardiovascular events in patients with rheumatoid arthritis treated with tocilizumab and etanercept. Clin Exp Rheumatol. 2018;36(2):310–313.
18. Pugliesi A, Oliveira DGC, Filho VA de S, et al. Cardiovascular safety of the class of JAK inhibitors or tocilizumab compared with TNF inhibitors in patients with rheumatoid arthritis: systematic review and a traditional and Bayesian network meta-analysis of randomized clinical trials. Semin Arthritis Rheum. 2024;69:152563. doi:10.1016/j.semarthrit.2024.152563
19. Kishimoto T, Kang S. IL-6 revisited: from rheumatoid arthritis to CAR T cell therapy and COVID-19. Annu Rev Immunol. 2022;40:323–348. doi:10.1146/annurev-immunol-101220-023458
20. Gusev E, Sarapultsev A, Solomatina L, Chereshnev V. SARS-CoV-2-specific immune response and the pathogenesis of COVID-19. Int J Mol Sci. 2022;23(3):1716. doi:10.3390/ijms23031716
21. Saadoun D, Vieira M, Vautier M, et al. SARS-CoV-2 outbreak in immune-mediated inflammatory diseases: the Euro-COVIMID multicentre cross-sectional study. Lancet Rheumatol. 2021;3(7):e481–e488. doi:10.1016/S2665-9913(21)00112-0
22. The WHO Rapid Evidence Appraisal for COVID-19 Therapies (REACT) Working Group. Association between administration of IL-6 antagonists and mortality among patients hospitalized for COVID-19: a meta-analysis. JAMA. 2021;326(6):499–518. doi: 10.1001/jama.2021.11330
23. Gupta R, Shipa M, Yeoh SA, Buck P, Ehrenstein MR. An unfavourable outcome following switching intravenous Abatacept and tocilizumab to subcutaneous forms during the COVID-19 pandemic. Rheumatol Oxf Engl. 2021;60(2):977–979. doi:10.1093/rheumatology/keaa653
24. Cáceres VA, Piñeiro ML, Ibáñez-Beróiz B, Enguita-Germán M. Mass switch from intravenous to subcutaneous tocilizumab in rheumatic diseases during the SARS-COV-2 pandemic. J Clin Rheumatol. 2022;28(7):346–348. doi:10.1097/RHU.0000000000001862
25. Garaffoni C, Adinolfi A, Bortoluzzi A, et al. Novel insights into the management of rheumatoid arthritis: one year in review 2022. Clin Exp Rheumatol. 2022;40(7):1247–1257. doi:10.55563/clinexprheumatol/1sjgyr
26. Aletaha D, Neogi T, Silman AJ. Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheumat. 2010. 62(9):2569–2581. doi:10.1002/art.27584
27. Rasmussen L, Pratt N, Hansen MR, Hallas J, Pottegård A. Using the “proportion of patients covered” and the Kaplan-Meier survival analysis to describe treatment persistence. Pharmacoepidemiol Drug Saf. 2018;27(8):867–871. doi:10.1002/pds.4582
28. Buzatu C, Moots RJ. Measuring disease activity and response to treatment in rheumatoid arthritis. Expert Rev Clin Immunol. 2019;15(2):135–145. doi:10.1080/1744666X.2019.1559050
29. Adverse event | European medicines agency (EMA). Available from: https://www.ema.europa.eu/en/glossary-terms/adverse-event.
30. R: the R project for statistical computing. 2024. Available from: https://www.r-project.org/.
31. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
32. Study quality assessment tools | NHLBI, NIH. Available from: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
33. Zotero | your personal research assistant. Available from: https://www.zotero.org/.
34. Stojanović S, Stamenković B, Nedović J, Aleksić I, Cvetković J. Effectiveness of tocilizumab after switching from intravenous to subcutaneous formulation in patients with rheumatoid arthritis: a single-centre experience. Acta Fac Medicae Naissensis. 2021;38(3):247–257. doi:10.5937/afmnai38-31264
35. Darloy J, Segaud N, Salmon JH, et al. Tocilizumab effectiveness after switching from intravenous to subcutaneous route in patients with rheumatoid arthritis: the RoSwitch study. Rheumatol Ther. 2019;6(1):61–75. doi:10.1007/s40744-018-0138-y
36. Rodríguez de Francisco L, Acosta García HL, Fernández González M, Soriano Martínez M, Ciudad Gutierrez P. Evaluation of the effectiveness and safety of switching from intravenous to subcutaneous tocilizumab. Eur J Hosp Pharm. 2022;29(SUPPL 1):A115. doi:10.1136/ejhpharm-2022-eahp.240
37. Ahn SM, Oh JS, Heo HM, et al. Predictive factors for rheumatoid arthritis flare after switching from intravenous to subcutaneous formulation of tocilizumab in real-world practice. J Korean Med Sci. 2022;37(17):e138. doi:10.3346/jkms.2022.37.e138
38. Daood R, Toledano K, Markovits D, et al. Switching from intravenous tocilizumab to subcutaneous administration during COVID-19 pandemic: impact on treatment efficacy and patient satisfaction. Clin Exp Rheumatol. 2023;41(3):744–746. doi:10.55563/clinexprheumatol/lxfy2v
39. Larid G, Joffres L, Ricard E, et al. Stable efficacy and safety after switching from intravenous to subcutaneous tocilizumab in a cohort of 200 patients in real life conditions. Joint Bone Spine. 2022;89(4). doi:10.1016/j.jbspin.2022.105347
40. Iwamoto N, Fukui S, Umeda M, et al. Evaluation of switching from intravenous to subcutaneous formulation of tocilizumab in patients with rheumatoid arthritis. Mod Rheumatol. 2016;26(5):662–666. doi:10.3109/14397595.2015.1129692
41. Atsumi T, Fujio K, Yamaoka K, Tomobe M, Kuroyanagi K, Kameda H. Safety and effectiveness of subcutaneous tocilizumab in patients with rheumatoid arthritis in a real-world clinical setting. Mod Rheumatol. 2018;28(5):780–788. doi:10.1080/14397595.2017.1416760
42. Desplats M, Pascart T, Jelin G, et al. Are Abatacept and tocilizumab intravenous users willing to switch for the subcutaneous route of administration? A questionnaire-based study. Clin Rheumatol. 2017;36(6):1395–1400. doi:10.1007/s10067-017-3587-8
43. Nikiphorou E, Radner H, Chatzidionysiou K, et al. Patient global assessment in measuring disease activity in rheumatoid arthritis: a review of the literature. Arthritis Res Ther. 2016;18(1):251. doi:10.1186/s13075-016-1151-6
44. Maranini B, Bortoluzzi A, Silvagni E, Govoni M. Focus on sex and gender: what we need to know in the management of rheumatoid arthritis. J Pers Med. 2022;12(3). doi:10.3390/jpm12030499
45. Reggia R, Franceschini F, Tincani A, Cavazzana I. Switching from intravenous to subcutaneous formulation of Abatacept: a single-center Italian experience on efficacy and safety. J Rheumatol. 2015;42(2):193–195. doi:10.3899/jrheum.141042
46. Silvagni E, Bortoluzzi A, Carrara G, Zanetti A, Govoni M, Scirè CA. Comparative effectiveness of first-line biological monotherapy use in rheumatoid arthritis: a retrospective analysis of the RECord-linkage on rheumatic diseases study on health care administrative databases. BMJ Open. 2018;8(9):e021447. doi:10.1136/bmjopen-2017-021447
47. Huynh TK, Ostergaard A, Egsmose C, Madsen OR. Preferences of patients and health professionals for route and frequency of administration of biologic agents in the treatment of rheumatoid arthritis. Patient Prefer Adherence. 2014;8:93–99. doi:10.2147/PPA.S55156
48. den Broeder N, den Broeder AA, Verhoef LM, van den Hoogen FHJ, van der Maas A, van den Bemt BJF. Non-medical switching from tocilizumab to sarilumab in rheumatoid arthritis patients with low disease activity, an observational study. Clin Pharmacol Ther. 2023;114(4):810–814. doi:10.1002/cpt.2999
49. Swets MC, Moss RJ, Kor F, et al. A comparison of the effectiveness of different doses of tocilizumab and sarilumab in the treatment of severe COVID-19: a natural experiment due to drug shortages. Int J Infect Dis. 2023;129:57–62. doi:10.1016/j.ijid.2023.01.041
50. McLaughlin M, Östör A. Safety of subcutaneous versus intravenous tocilizumab in combination with traditional disease-modifying antirheumatic drugs in patients with rheumatoid arthritis. Expert Opin Drug Saf. 2015;14(3):429–437. doi:10.1517/14740338.2015.998198
51. Baraliakos X. Comparative evaluation of adverse events associated with subcutaneous infliximab (CT-P13 SC) and intravenous infliximab: a real-world analysis of post-marketing surveillance data. ACR Meeting Abstracts. Available from: https://acrabstracts.org/abstract/comparative-evaluation-of-adverse-events-associated-with-subcutaneous-infliximab-ct-p13-sc-and-intravenous-infliximab-a-real-world-analysis-of-post-marketing-surveillance-data/.
52. Pham T, Tubach F. Patient acceptable symptomatic state (PASS). Joint Bone Spine. 2009;76(4):321–323. doi:10.1016/j.jbspin.2009.03.008
53. Bruce B, Fries JF. The Stanford Health Assessment Questionnaire: a review of its history, issues, progress, and documentation. J Rheumatol. 2003;30(1):167–178.
54. Silvagni E, Zandonella Callegher S, Mauric E, et al. Musculoskeletal ultrasound for treating rheumatoid arthritis to target—a systematic literature review. Rheumatology. 2022;61(12):4590–4602. doi:10.1093/rheumatology/keac261
55. Smolen JS, Breedveld FC, Burmester GR, et al. Treating rheumatoid arthritis to target: 2014 update of the recommendations of an international task force. Ann Rheum Dis. 2016;75(1):3–15. doi:10.1136/annrheumdis-2015-207524
56. Yeoh SA, Ehrenstein MR. Are treat-to-target and dose tapering strategies for rheumatoid arthritis possible during the COVID-19 pandemic? Lancet Rheumatol. 2020;2(8):e454–e456. doi:10.1016/S2665-9913(20)30175-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.