Back to Journals » OncoTargets and Therapy » Volume 13
Sustained Remission of Relapsed or Refractory Mantle Cell Lymphoma After 4-1BB-Based CD19-Directed CAR-T Therapy
Authors Yang C, Lei W, Xie H, Wu G, Wei J, Liang A, Qian W
Received 7 September 2020
Accepted for publication 6 November 2020
Published 25 November 2020 Volume 2020:13 Pages 12163—12168
DOI https://doi.org/10.2147/OTT.S280535
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Takuya Aoki
Chunmei Yang,1,* Wen Lei,1,2,* Hongqiong Xie,1,* Gongqiang Wu,3 Juying Wei,1 Aibin Liang,4 Wenbin Qian1,2,5
1Department of Hematology, The First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou 310003, Zhejiang, People’s Republic of China; 2Department of Hematology, The Second Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou 310009, Zhejiang, People’s Republic of China; 3Department of Hematology, Dongyang Hospital Affiliated to Wenzhou Medical University, Dongyang 322100, Zhejiang, People’s Republic of China; 4Department of Hematology, Tongji Hospital of Tongji University, Shanghai 200065, People’s Republic of China; 5National Clinical Research Center for Hematologic Diseases, The First Affiliated Hospital of Soochow University, Suzhou 215006, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Aibin Liang
Department of Hematology, Tongji Hospital of Tongji University, Shanghai, People’s Republic of China
Email [email protected]
Wenbin Qian
Department of Hematology, The Second Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, People’s Republic of China
Email [email protected]
Abstract: Relapsed and refractory (R/R) mantle cell lymphoma (MCL) remains an incurable lymphoma with a poor prognosis. Recently, there are a few studies demonstrating the efficacy of anti-CD19 chimeric antigen receptor T (CAR-T) cell therapy in MCL, including ZUMA-2 study in which CD28-based CAR-T cells were used. However, long-term efficacy and safety associated with 4-1BB-based CAR-T therapy in MCL are not defined well. Here, we report three male patients with R/R classical MCL, who received CD19-directed 4-1BB CAR-T therapy and achieved complete remission, showed mild symptoms of cytokine-release syndrome (CRS) and had no neurological toxicity. During a follow-up of 24– 35 months, all three patients remained in complete remission. Persistent B-cell depletion was observed in two patients. Recovery of CD19+ polyclonal B cells was detected in one patient at 6 months after CAR-T cell infusion. Recovery of serum immunoglobulin, including IgG, IgA and IgM, was not observed in two patients at the last follow-up. Only one patient developed herpes zoster, and the other two patients had no serious infection. This is the first report about the efficacy, long-term remission and safety of CD19-directed 4-1BB CAR-T therapy in R/R MCL.
Keywords: mantle cell lymphoma, CAR-T cell therapy, long-duration remission, B-cell depletion
Introduction
Mantle cell lymphoma (MCL) is a heterogeneous lymphoma that generally has a highly aggressive clinical course, accounting for 2% to 6% of non-Hodgkin lymphoma (NHL) in Asians.1,2 MCL remains an incurable disease despite the emergence of new targeted agents including Bruton’s tyrosine kinase (BTK) inhibitors that have greatly improved outcomes in patients with relapsed or refractory (R/R) disease. In the pre-BTK inhibitor era, five-year overall survival (OS) and progression-free survival (PFS) rates were 35.5% and 8.8%, respectively, in China.3 In the relapse/refractory setting, there are a number of agents now licensed for MCL treatment, which included lenalidomide, bortezomib, temsirolimus, and BTK inhibitor such as ibrutinib and acalabrutinib.4,5 Ibrutinib, a first in class BTK inhibitor, demonstrated an OR rate (ORR) of 67% with a complete remission (CR) rate of 23% leading to its FDA approval after at least one prior line of therapy.6 However, treatment with ibrutinib can provide durable remissions only in a subset of patients with R/R MCL, especially those with nonblastoid morphology non-bulky disease, good ECOG performance status (ECOG score 0–1), and low/intermediate risk MCL International Prognostic Index (MIPI).7,8 In addition, the outcomes of patients who are primary resistance to BTK inhibitors or progress after BTK inhibitor treatment are extremely poor with an ORR ranging between 25% and 42% and median OS between 6 and 10 months with salvage therapies,4 suggesting that new methods of overcoming this clinical problem are needed.
Anti-CD19 chimeric antigen receptor T (CAR-T) cells have emerged as an effective therapy for the treatment of R/R B-NHL, specifically diffuse large B-cell lymphoma (DLBCL). In a recent study, Kochenderfer et al treated nineteen DLBCL, one follicular lymphoma (FL), and one MCL patients with CD28-based CD19-CAR-T cells. This MCL patient achieved CR after CAR-T cell therapy.9 In another clinical trial, in which 4-1BB-based CD19-CAR-T cells manufactured from defined T cell subsets (1:1 CD4+:CD8+ ratio of CAR-T cells) were used to treat R/R B-cell NHL, 4 patients with MCL were enrolled.10 More recently, KTE-X19, the CD28-based anti-CD19 CAR-T-cell therapy, demonstrated durable remission in 68 patients with R/R MCL (93% ORR, 67% CR, with progression-free survival (PFS) of 61% and OS of 83% at 1 year); the majority of these patients are refractory to BTK inhibitor or relapsed after treatment with BTK inhibitor.11 Here we retrospectively analyzed 3 R/R MCL patients who underwent 4-1BB-based CD19-CAR-T therapy in our hospital, which show that all 3 patients achieved durable remissions and meaningful OS benefit after CAR-T cell treatment.
Case Reports
In this study, we performed retrospective analysis of an R/R B-cell lymphoma cohort, in which 3 patients with MCL underwent 4-1BB-based CD19-CAR-T cell therapy (NCT0253977). This study was approved by Medical Ethics Committee of the First Affiliated Hospital, College of Medicine, Zhejiang University. All enrolled MCL patients meet the inclusion and exclusion criteria that were described in Supplementary Materials and Methods section, and gave informed consent in accordance with the Declaration of Helsinki. The clinical characteristics of the patients are detailed in Table 1. Immunohistochemical staining of tumor sections showed: CD5 (+), CD20 (+), CD79a (+), CD21 (+), CD23 (+), BCL-2 (+), BCL-6 (-), CD43 (+), CycIin-D1 (+), SOX11 (+), Ki-67 (25%–50%). All patients received at least four prior line of immunochemotherapy such as R-HyperCVAD (Rituximab, cyclophosphamide, vincristine, doxorubicin, dexamethasone, alternating with high-dose methotrexate and cytarabine), VR-CAP (bortezomib, rituximab, cyclophosphamide, doxorubicin, prednisone), R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone), R-GDP (rituximab, gemcitabine, dexamethasone, cisplatin), R-DHAP (rituximab, dexamethasone, cytarabine, cisplatin), Bortezomib-GDP, lenalidomide combined with ICE (ifosfamide, carboplatin, and etoposide), ibrutinib, and autologous stem cell transplantation (ASCT). These patients received the lymphodepleting chemotherapy as described previously12 before CAR-T infusion. In this study, 4-1BB-based CD19-specific CAR construct was established in the Dr. Liang’s certified CAR-T Laboratory and the products of CD19-CAR-T were prepared in the Institute of Hematology, Zhejiang University. The nature of the CD19-CAR and manufacture of the CAR-T cells were also described in Supplementary Materials and Methods section. After conditioning therapy, the patients received a single infusion of CD19-CAR-T cells (about 2 × 106 cells/kg) at day 0. Adverse events (AEs) of special interest that might be related to CAR-T cell therapy are listed in Table 1. The most common grade 3 or grade 4 AEs observed within the first few weeks after infusion included neutropenia, fever and fatigue. Both of Patient 1 and Patient 2 experienced grade 1 cytokine-release syndrome (CRS), but Patient 3 suffered from a persistent high fever and significant drop in blood pressure that were resolved with fluid infusion. He also received tocilizumab treatment, which successfully relieved him from fever and hypotension (Table 1). Three months after CAR-T infusion, FDG-PET/CT was unable to detect any disease in all 3 patients, suggesting an achievement of CR (95% C. I. from 39% to 99%, Figure 1A). Responses are ongoing at 35, 24.5, and 24 months in 3 patients, respectively (Table 1).
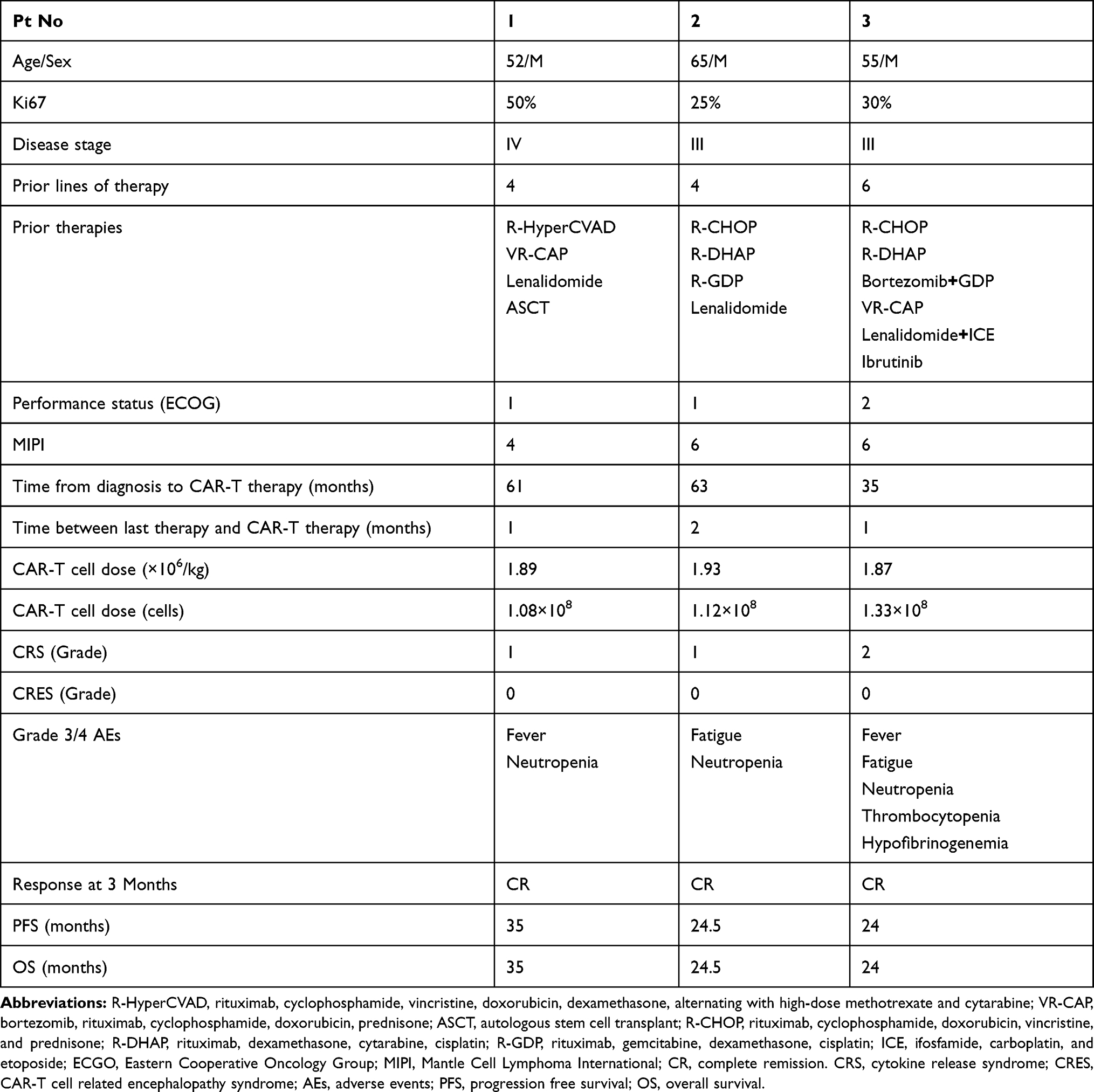 |
Table 1 Baseline Characteristics and Outcomes |
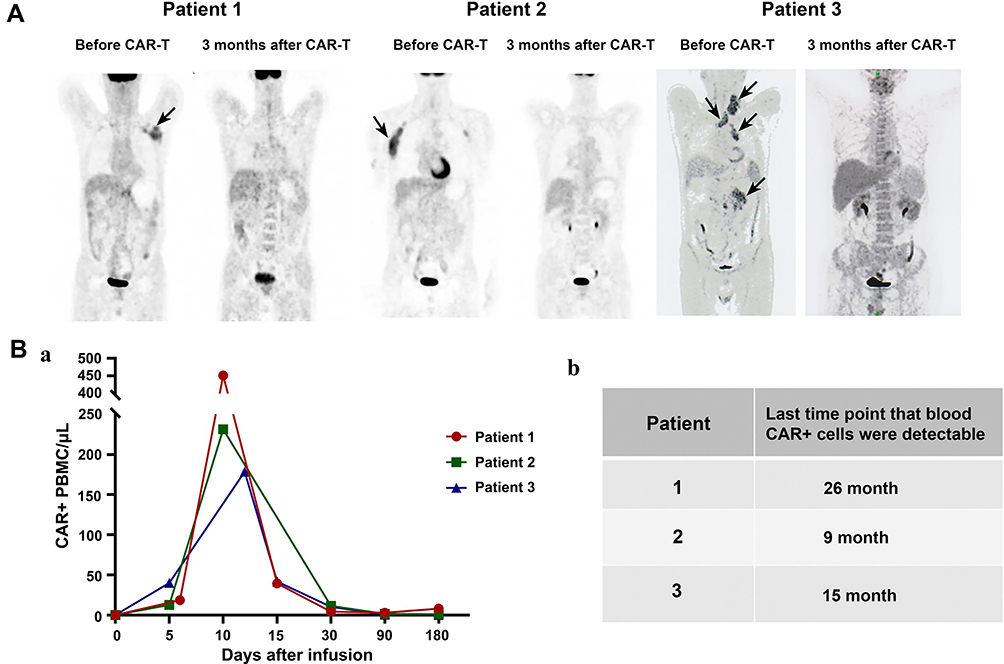 |
Figure 1 Patients with refractory or relapsed mantle cell lymphoma achieved durable remission after CD19-4-1BB CAR-T cell treatment. (A) PET-CT scans at baseline and 3 months after CAR-T infusion in three patients who responded with complete remission. Examples of sites of lymphoma in this patient are indicated by the black arrows. (B) CD19-CAR+ cells in PBMCs were detected by quantitative PCR. Limit of detection of the qPCR assay is 0.001% or 1×10−5. (a) The first 6 months after CAR-T infusion, (b) Last time that CAR+ cells were detectable. |
In the present study, the CAR-T cell levels in patients’ peripheral blood were determined by qPCR described in Supplementary Materials and Methods section. The peak number of CAR-T cells appeared in 1–2 weeks after infusion and then decreased (Figure 1B(a)). A PCR examination confirmed the long-time existence of CAR-T cells in peripheral blood of all patients. We could still detect 0.03% of CAR+ cells at 26 months after CAR-T infusion in Patient 1. The last time-point at which CAR+ cells could be detected was 9 months and 15 months for Patient 2 and Patient 3, respectively (Figure 1B(b)). CD19-CAR-T cell therapy has been reported to cause persistent B-cell depletion and hypogammaglobulinemia in patients with leukemia and lymphoma.13 We found a significant decrease of serum IgG and IgA levels after CAR-T therapy (Figure 2A). B-cell aplasia was monitored and results showed persistent B-cell depletion in Patient 1 and Patient 2, whereas we could detect 4.05% of normal B-cells in Patient 3, which indicates the recovery of B-cell at 6 months after the CAR-T therapy. We also analyzed the phenotypes of blood B cells after the recovery of B cells. The recovering B cells were polyclonal, as evidenced by a normal ratio of kappa to lambda light chains on these B cells (Figure 2B). However, the recovery of serum immunoglobulin, including IgG, IgA and IgM, was not observed in Patient 3 at the same time. He also suffered from herpes zoster that was resolved after treatment with intravenous immunoglobulin and ganciclovir. The other two patients in long-term remission did not have any other severe infections.
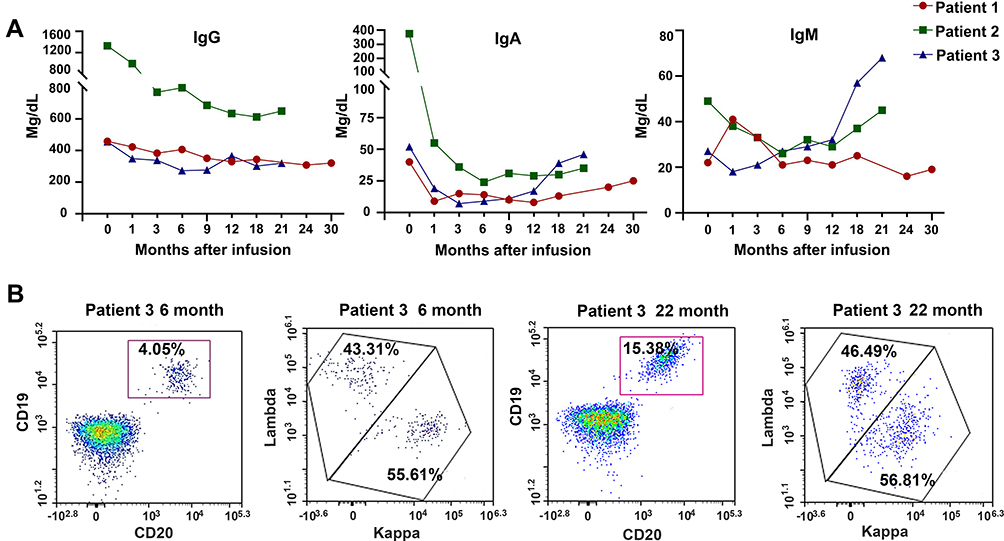 |
Figure 2 Assessment of serum immunoglobulins and B-cell recovery. (A) Immunoglobulins including IgG, IgA and IgM were monitored from all three patients before and after treatment with CD19-CAR-T cells. (B) Assessment of B cell recovery and phenotype of recovering B cells in Patient 3. |
Discussion
It was well known that CD28 and 4-1BB domain are the most commonly used costimulatory signal molecules in CD19-CAR. Milone et al14 demonstrated that human T-cells expressing CD19-CAR containing 4-1BB were significantly more effective than CD19-CAR-T cells with CD28 in leukemia model. Moreover, published clinical trial results show that CAR-T cells expressing CD28 persisted for up to 3 months, while CAR-T containing 4-1BB persisted for up to 5 years and more than 6 months in a majority of cases.15 The efficacies and adverse events of CD28-based CD19-CAR-T vs 4-1BB-based CD19-CAR-T in acute lymphoblastic leukemia (ALL) have been investigated, which showed that both CD28 CAR-T and 4-1BB CAR-T differed in response pattern, adverse events.15 Zhao et al16 manufactured 4-1BB- and CD28-based CD19-CAR-T cells using the same process and further evaluated their efficacy and safety in R/R B-ALL. In vivo experiment shows 4-1BB-based CAR-T exhibited more potent in eradicating tumor cells and longer persistence than CD28-based CAR-T cells. Moreover, retrospective analysis of a clinical study demonstrated that 4-1BB-based CAR-T resulted in higher anticancer efficacy and less severe events. However, Ying et al17 performed parallel comparison of 4-1BB or CD28 co-stimulated CD19-CAR-T cell therapy for B-NHL that included DLBCL, FL, and marginal zone B cell lymphoma. In this Phase I/II clinical trial, 4-1BB-based CAR-T was well tolerated although similar antitumor efficacies were observed between two different types of CAR-T. As mentioned above, KTE-X19, a CD28-based CD19-specific CAR-T, induced durable remissions in a majority of patients with R/R MCL. However, this therapy led to serious toxic effects that included grade 3 or higher CRS (15%) and neurologic events (31%). Infection of grade 3 or higher also occurred in 32% of the patients.11
Up to data, long-term efficacy and safety associated with 4-1BB-based CAR-T therapy in MCL are not defined well. Here, we report the results of treatment with 4-1BB CAR-T cells targeting CD19 in R/R MCL. All three patients with R/R MCL achieved a durable CR despite the small numbers in this study, suggesting that CD19 CAR-T containing 4-1BB costimulatory molecule may be a promising approach to treat MCL. Interestingly, there are no grade 3 or higher CRS occurred in all 3 patients. More importantly, any grade neurological events were also not observed in these patients (Table 1). The use of CD19-CAR-T cells resulted in prolonged B cell aplasia and resultant hypogammaglobulinemia.18 In our study, B cell aplasia was observed in all treated patients while hypogammaglobulinemia was found in 2 out of the 3 patients. Nevertheless, there were no severe infections among these patients although sustained depletion of B cells and resultant hypogammaglobulinemia can place the patient at risk of life-threatening infections.18
It is reported that in vivo expansion and persistence of CAR-T cells seem to be associated with remission in B-cell malignancies.10,19 In the present study, peak expansion of CAR-T cells in the blood occurred at 10–12 days. A longer persistence of CAR-T cells was also observed in all 3 patients. Previously, a Phase I trial reported that no CAR T cells were detected after day 68 in any patients, who received CD28-based CD19-CAR-T cells.20 Taken together, these data support that CD28-based CAR-T cells have a greater peak expansion whereas 4-1BB-based CAR-T cells show a longer persistence.21
In conclusion, although the small sample size precludes any conclusions, our study suggests that CD19-directed 4-1BB CAR-T cells elicit a potent and durable anticancer response in patients with R/R MCL. No significant toxicities, especially neurotoxicity, were observed.
Abbreviations
MCL, mantle cell lymphoma; CAR-T, chimeric antigen receptor T; R/R, relapsed and refractory; CRS, cytokine-release syndrome; OS, overall survival; PFS, progression-free survival; ORR, overall response rate; CR, complete remission; ASCT, autologous stem cell transplantation; PBMCs, peripheral blood mononuclear cells.
Ethics Approval and Informed Consent
This study was approved by Medical Ethics Committee of the First Affiliated Hospital, College of Medicine, Zhejiang University. Written informed consent was provided by all patients to have the case details and any accompanying images published.
Consent for Publication
Consent for publication was obtained from the patients.
Acknowledgment
Co-first authors: Chunmei Yang, Wen Lei, Hongqiong Xie.
Funding
This study was supported by funds from the Natural Science Foundation of Zhejiang Province (No. LY20H080006), the National Natural Science Foundation of China (No. 81830006, 81830004, 81670178), Basic Public Welfare Research Project of Zhejiang Province (No. LGF19H080001) and Translation Research Grant of HCRCH (2020ZKZC01).
Disclosure
The authors report no conflicts of interest for this work.
References
1. Miao Y, Cao L, Sun Q, et al. Spectrum and immunophenotyping of 653 patients with B-cell chronic lymphoproliferative disorders in China: a single-centre analysis. Hematol Oncol. 2018;36(1):121–127. doi:10.1002/hon.2461
2. Meng J, Chang C, Pan H, et al. Epidemiologic characteristics of malignant lymphoma in Hubei, China: a single-center 5-year retrospective study. Medicine. 2018;97(35):e12120. doi:10.1097/MD.0000000000012120
3. Yoon DH, Cao J, Chen TY, et al. Treatment of mantle cell lymphoma in Asia: a consensus paper from the Asian Lymphoma Study Group. J Hematol Oncol. 2020;13:21. doi:10.1186/s13045-020-00855-9
4. Hanel W, Epperla N. Emerging therapies in mantle cell lymphoma. J Hematol Oncol. 2020;13(1):79. doi:10.1186/s13045-020-00914-1
5. Kumar A, Sha F, Toure A, et al. Patterns of survival in patients with recurrent mantle cell lymphoma in the modern era: progressive shortening in response duration and survival after each relapse. Blood Cancer J. 2019;9(6):50. doi:10.1038/s41408-019-0209-5
6. Wang ML, Blum KA, Martin P, et al. Long-term follow-up of MCL patients treated with single-agent ibrutinib: updated safety and efficacy results. Blood. 2015;126(6):739–745. doi:10.1182/blood-2015-03-635326
7. Jain P, Romaguera J, Srour SA, et al. Four-year follow-up of a single arm, Phase II clinical trial of ibrutinib with rituximab (IR) in patients with relapsed/refractory mantle cell lymphoma (MCL). Br J Haematol. 2018;182(2):404–411. doi:10.1111/bjh.15411
8. Rule S, Dreyling M, Goy A, et al. Outcomes in 370 patients with mantle cell lymphoma treated with ibrutinib: a pooled analysis from three open-label studies. Br J Haematol. 2017;179(3):430–438. doi:10.1111/bjh.14870
9. Kochenderfer JN, Somerville RPT, Lu T, et al. Lymphoma remissions caused by anti-CD19 chimeric antigen receptor T Cells are associated with high serum interleukin-15 levels. J Clin Oncol. 2017;35(16):1803–1813. doi:10.1200/JCO.2016.71.3024
10. Turtle CJ, Hanafi LA, Berger C, et al. Immunotherapy of non-Hodgkin’s lymphoma with a defined ratio of CD8+ and CD4+ CD19-specific chimeric antigen receptor-modified T cells. Sci Transl Med. 2016;8(355):355ra116. doi:10.1126/scitranslmed.aaf8621
11. Wang M, Munoz J, Goy A, et al. KTE-X19 CAR T-cell therapy in relapsed or refractory mantle-cell lymphoma. N Engl J Med. 2020;382(14):1331–1342. doi:10.1056/NEJMoa1914347
12. Yang C, Xie M, Zhang K, et al. Risk of HBV reactivation post CD19-CAR-T cell therapy in DLBCL patients with concomitant chronic HBV infection. Leukemia. 2020;34(11):3055–3059. doi:10.1038/s41375-020-0913-y
13. Schuster SJ, Svoboda J, Chong EA, et al. Chimeric antigen receptor T cells in refractory B-cell lymphomas. N Engl J Med. 2017;377(26):2545–2554. doi:10.1056/NEJMoa1708566
14. Milone MC, Fish JD, Carpenito C, et al. Chimeric receptors containing CD137 signal transduction domains mediate enhanced survival of T cells and increased antileukemic efficacy in vivo. Mol Ther. 2009;17(8):1453–1464. doi:10.1038/mt.2009.83
15. Li S, Zhang J, Wang M, et al. Treatment of acute lymphoblastic leukaemia with the second generation of CD19 CAR-T containing either CD28 or 4-1BB. Br J Haematol. 2018;181(3):360–371. doi:10.1111/bjh.15195
16. Zhao X, Yang J, Zhang X, et al. Efficacy and safety of CD28- or 4-1BB-based CD19 CAR-T cells in B cell acute lymphoblastic leukemia. Mol Ther Oncolytics. 2020;18:272–281. doi:10.1016/j.omto.2020.06.016
17. Ying Z, He T, Wang X, et al. Parallel comparison of 4-1BB or CD28 co-stimulated CD19-targeted CAR-T cells for B cell Non-Hodgkin’s lymphoma. Mol Ther Oncolytics. 2019;15:60–68. doi:10.1016/j.omto.2019.08.002
18. Paszkiewicz PJ, Fräßle SP, Srivastava S, et al. Targeted antibody-mediated depletion of murine CD19 CAR T cells permanently reverses B cell aplasia. J Clin Invest. 2016;126(11):4262–4272. doi:10.1172/JCI84813
19. Locke FL, Ghobadi A, Jacobson CA, et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): a single-arm, multicentre, Phase 1–2 trial. Lancet Oncol. 2019;20(1):31–42. doi:10.1016/S1470-2045(18)30864-7
20. Lee DW, Kochenderfer JN, Stetler-Stevenson M, et al. T cells expressing CD19 chimeric antigen receptors for acute lymphoblastic leukaemia in children and young adults: a phase 1 dose-escalation trial. Lancet. 2015;385(9967):517–528. doi:10.1016/S0140-6736(14)61403-3
21. Kawalekar OU, O’Connor RS, Fraietta JA, et al. Distinct signaling of coreceptors regulates specific metabolism pathways and impacts memory development in CAR T cells. Immunity. 2016;44(2):380–390. doi:10.1016/j.immuni.2016.01.021
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.