Back to Journals » International Journal of Women's Health » Volume 15
Survival Status and Predictors of Mortality Among Women with Uterine Rupture at Public Hospitals of Eastern Ethiopia. Semi-Parametric Survival Analysis
Authors Alemu A, Yadeta E ![]() , Deressa A
, Deressa A ![]() , Debella A
, Debella A ![]() , Birhanu A
, Birhanu A ![]() , Heluf H, Mohammed A
, Heluf H, Mohammed A ![]() , Ahmed F, Beyene A
, Ahmed F, Beyene A ![]() , Getachew T
, Getachew T ![]() , Eyeberu A
, Eyeberu A ![]()
Received 27 December 2022
Accepted for publication 13 March 2023
Published 25 March 2023 Volume 2023:15 Pages 443—453
DOI https://doi.org/10.2147/IJWH.S402885
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Addisu Alemu,1 Elias Yadeta,2 Alemayehu Deressa,1 Adera Debella,2 Abdi Birhanu,3 Helina Heluf,2 Ahmed Mohammed,3 Fila Ahmed,1 Andinet Beyene,3 Tamirat Getachew,2 Addis Eyeberu2
1School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 2School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 3School of Medicine, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Addis Eyeberu, School of Nursing and Midwifery, Haramaya University, 138, Dire Dawa, Harar, Ethiopia, Tel +251910005436, Email [email protected]
Background: Uterine rupture is the most dangerous complication of labor and contributes to high maternal mortality. Despite efforts to improve basic and comprehensive emergency obstetric treatment, women continue to suffer from disastrous maternal outcomes.
Purpose: This study aimed to assess the survival status and predictors of mortality among women with uterine rupture at public hospitals in the Harari Region, Eastern Ethiopia.
Patients and Methods: We conducted a retrospective cohort study among women with uterine rupture in public hospitals in Eastern Ethiopia. All women with uterine rupture were followed for 11 years retrospectively. Statistical analysis was conducted with STATA version 14.2. Kaplan–Meier curves together with a Log rank test were used to estimate the survival time and show the presence of differences among groups. Cox Proportion Hazard (CPH) model was used to determine the association between independent variables and survival status.
Results: There were 57,006 deliveries in the study period. We found that 10.5% (95% CI: 6.8– 15.7) of women with uterine rupture have died. The median recovery and death time for women with uterine rupture were 8 and 3 days with interquartile range (IQR) of 7– 11 days and 2– 5 days, respectively. Antenatal care follow-up (AHR: 4.2, 95% CI: 1.8– 9.79), education status (AHR: 0.11; 95% CI: 0.02– 0.85), visiting health center (AHR: 4.89; 95% CI: 1.05– 22.88), and admission time (AHR: 4.4; 95% CI: 1.89– 10.18) were the predictors of survival status of women with uterine rupture.
Conclusion: One out of ten study participants died due to uterine rupture. Factors including not having ANC follow-up, visiting health centers for treatment, and being admitted during the night time were predictors. Thus, a great emphasis has to be given to the prevention of uterine rupture and the linkage within health institutions has to be smooth to improve the survival of patients with uterine rupture with the help of different professionals, health institutions, health bureaus, and policymakers.
Keywords: emergency obstetrics, uterine rupture, predictors, mortality, Ethiopia
A Letter to the Editor has been published for this article.
Introduction
A uterine rupture is defined as a partial or complete disruption to all three layers of the uterus, which most commonly occurs in pregnant women, but can occur in non-pregnant women if the uterus is exposed to trauma, diseased, or malignant.1–3 It is a sign of poor obstetric management and limited access to comprehensive emergency obstetric care facilities. The global incidence of uterine rupture is 0.07%, which is substantially lower than what is in Africa’s 1.3%. Evidence shows that 60% of uterine ruptures occur spontaneously, with the remaining 29% being scar ruptures and 11% being traumatic ruptures.4
Uterine rupture is one of the most dangerous complications of labor, endangering both the mother and the fetus and contributing to high maternal and perinatal mortality and morbidity.5 Uterine rupture is a significant public health concern, accounting for 13% of maternal death and 74–92% of perinatal mortality in sub-Saharan Africa, as well as 36% of maternal mortality in Ethiopia.6 A study done in Bahir Dar showed that maternal mortality due to uterine rupture is 2.1%.7 While a study was done in Tigray showed that 9.6% and 74.8% of the women and the fetuses died due to uterine rupture, respectively.8
Several studies conducted around the world found that rural residents, gravidity, having a history of cesarean section scar, maternal education, increased maternal age, distance from a health-care facility, high parity, not having antenatal care, mal-presentation, prolonged labor, obstructed labor, inappropriate usage of uterotonic drugs, induction or augmentation, congenital uterine anomalies, previous myomectomy, and Cephalopelvic disproportion(CPD) are risk factors of uterine rupture.9–13 In Ethiopia, the most serious consequences of uterine rupture are anemia, blood transfusion, vesicovaginal fistula, wound infection, maternal death, relaparotomy, puerperal sepsis, and stillbirth.14
Uterine rupture is managed usually with a surgical procedure. Despite the fact that surgical intervention reduces maternal morbidity associated with uterine rupture, many maternal and newborn complications have been documented.15 To reduce maternal mortality and morbidity, Ethiopia’s government is working substantially on basic emergency obstetric and newborn care. Despite this effort, the maternal death rate (412 per 100,000 live births) is among the highest in the world, with uterine rupture continuing to be a leading cause of maternal morbidity and mortality.
Despite efforts to improve the healthcare system and provide basic and comprehensive emergency obstetric treatment, women continue to suffer from disastrous maternal and fetal outcomes.16,17 Evidence-based data regarding survival status and predictors of uterine rupture are important to improve the accessibility and provision of emergency obstetric care, as well as to provide counseling and support to the women to enable them to cope with physical, social, psychological, and economic consequences.18,19 Therefore, this study aimed to assess the survival status and predictors of uterine rupture among women at public hospitals in the Harari Region, Eastern Ethiopia.
Materials and Methods
Study Design, Area, and Time Frame
We conducted a retrospective cohort study from October 1, 2012 to October 1, 2022 in public hospitals of Harar city. The Harar city is the capital city of Harari National Regional State, which is located 526 km east of Addis Ababa. Jugal Hospital and Hiwot Fana Specialized University Hospital (HFSUH) are the two public hospitals in Harari Regional State. In Harari Region, there are 45 health facilities (34 health posts, 8 health centers, and 5 hospitals). Among the 5 hospitals found in the Harar Regional State, only two of them are giving service as public hospitals. These two hospitals currently provide different services for more than 5.8 million populations in the catchment area.
Populations and Eligibility Criteria
All women who had uterine rupture at Jugal Hospital and HFSUH were the source population while all women who had uterine rupture at Jugal Hospital and HFSUH from October 1, 2012 to October 1, 2022 were the study population.
All medical records of women who had uterine ruptures at Jugal Hospital and HFSUH were included in the study. Women with incomplete medical records or patients whose records were lost were excluded from the study.
Sample Size Determinations and Sampling Procedure
The sample size was calculated using the double population proportion formula using Epi Info version 7 software. The predictors used to calculate sample size were history of previous cesarean section, induced labor, and prolonged labor. We obtained the largest sample size using the variable history of previous cesarean section20 compared to other covariates, and this was considered the final sample size of the study. Using a proportion of exposed (35.7%) and non-exposed (15.3%), one-to-one exposed-to-non-exposed ratio (1:1), 95% level of the confidence interval and power of 80%; with the non-retrieval rate of 10% and design effect 1.5, the final sample size became 248. However, the total number of uterine ruptures in the 11 years was 287 and we include all of the cases.
In the Harari Region, there are 5 governmental hospitals. Of those, Jugol Hospital and HFSUH were selected randomly. The maternal registration logbook was reviewed to obtain medical registration numbers. The 11 years of data from October 1, 2012 to October 1, 2022, were reviewed. A total of 287 women with uterine rupture medical registration numbers were obtained over these years. All women with uterine rupture were included in the study.
Data Collection and Quality Control
A checklist was developed after reviewing available relevant literature and used to collect information on socio-demographic factors, clinical characteristics of uterine rupture, causes and intervention-related characteristics, and management outcome of uterine rupture and obstetric-related factors. A pretest was conducted on 5% of the sample size at Haramaya general hospital. Data were collected by trained BSc midwives and supervised by experienced midwives. Double data entry was made by two data clerks to maintain the consistency of the data by comparing the two separately entered data.
Study Variables and Their Measurement
In this study, the event was death. The time variable was time from admission to the occurrence of the event coded as one otherwise zero. The independent variables were socio-demographic characteristics like age, address, educational status, and marital status; obstetrics characteristics like gravidity, parity, antenatal care follow-up, and visiting health facility; clinical characteristics of study participants and causes and intervention-related characteristics.
Statistical Analysis
Data were cleaned, checked for consistency and completeness, and then entered into Epi data version 3.1, and exported to Stata software version 14.2 for statistical analysis. Descriptive statistics such as percentages, medians, and interquartile ranges (IQRs) were computed. The median time to death and recovery was estimated using the Kaplan–Meier (KM) curve. The Log rank test was used to compare survival status between groups of categorical variables. Cox proportional hazards regression with the Efron method was used to detect the independent predictors of uterine rupture. All variables with p < 0.25 in the bivariate analysis were included in the multivariable model analysis. The Kaplan–Meier curve graph and Schoenfeld residuals were used to check the proportional hazard assumptions (glob test = 0.8484). The model fitness was assessed and the p-value was less than 0.001. The adjusted Hazard ratios (AHRS) with 95% confidence intervals (CIs) were used to identify the association between independent variables and uterine rupture. The final statistical significance was declared at P < 0.05 for final analyses.
Results
Sociodemographic and Obstetrics Characteristics of Study Participants
A total of 57,006 deliveries were conducted in the study period. A total of 287 women developed uterine rupture, 10 medical cards were incomplete and the study included 277 follow-ups. The mean (±SD) age of the mothers was 28.1 years (±5.4 years) with the range of 15–46 years and more than half 170 (61.4%) of the study participants were in the age group of 25–34 years. Of the total participants, 210 (75.8%) had formal education, 189 (68.2 %) were residing in rural areas, and 265 (95.6%) of them were married. The majority of 232 (83.8%) of the study participants were multigravida, around three-third 179 (64.6%) of them had ANC follow-up, and 212 (77.1%) visited health centers for treatment. A chi-square test was done to determine the association between survival status from uterine rupture and the independent variables. Accordingly, variables including age (p-value: 0.001), educational status (p-value: 0.006), ANC follow-up (p-value: 0.001), and health facility visit (p-value: 0.03) were associated with survival status (Table 1).
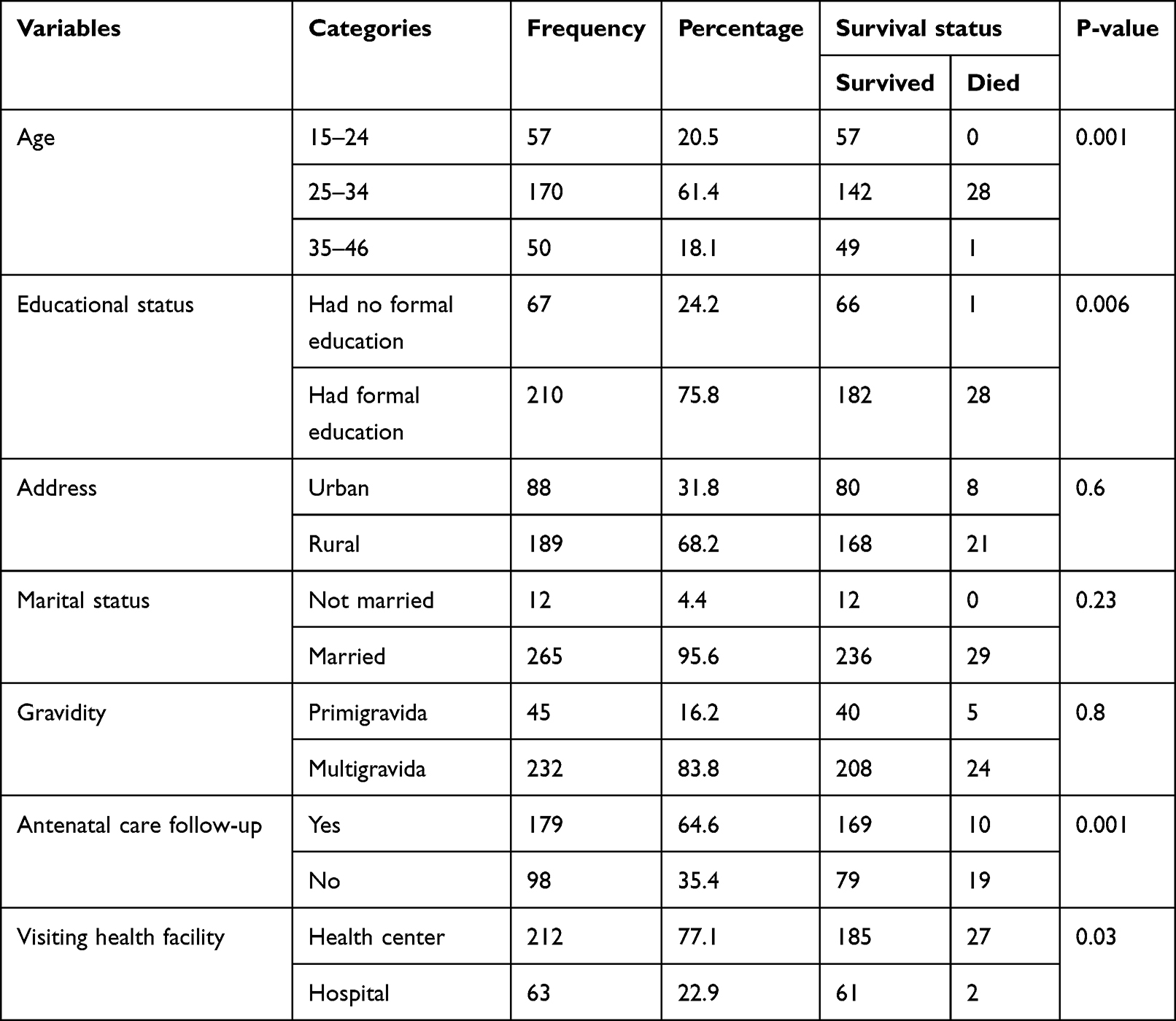 |
Table 1 The Association Between Sociodemographic and Obstetrics Characteristics with Survival Status from Uterine Rupture Among Women in Public Hospitals of Harari Region, Ethiopia, 2022 |
Clinical Characteristics of Study Participants
Of the total participants, around two-thirds 185 (66.8%) of them were admitted during the daytime, only 42 (15.2%) of them had labor initiated by induction, and there was an excessive uterine contraction for 20.2% of the mothers. The majority (89.5%) of the study participants had abdominal pain. Of the total participants, 58.5% of them had tachycardia, half (51.3%) of them had a temperature >37°C, and 48.4% had a sign of shock. Based on the chi-square test, variables including time of admission (P-value: 0.002), labor initiated by induction (P-value: 0.016), presence of excessive uterine contraction (P-value: 0.001), having abdominal swelling (P-value: 0.001), and a sign of shock (P-value: 0.001) were associated with survival status from uterine rupture (Table 2).
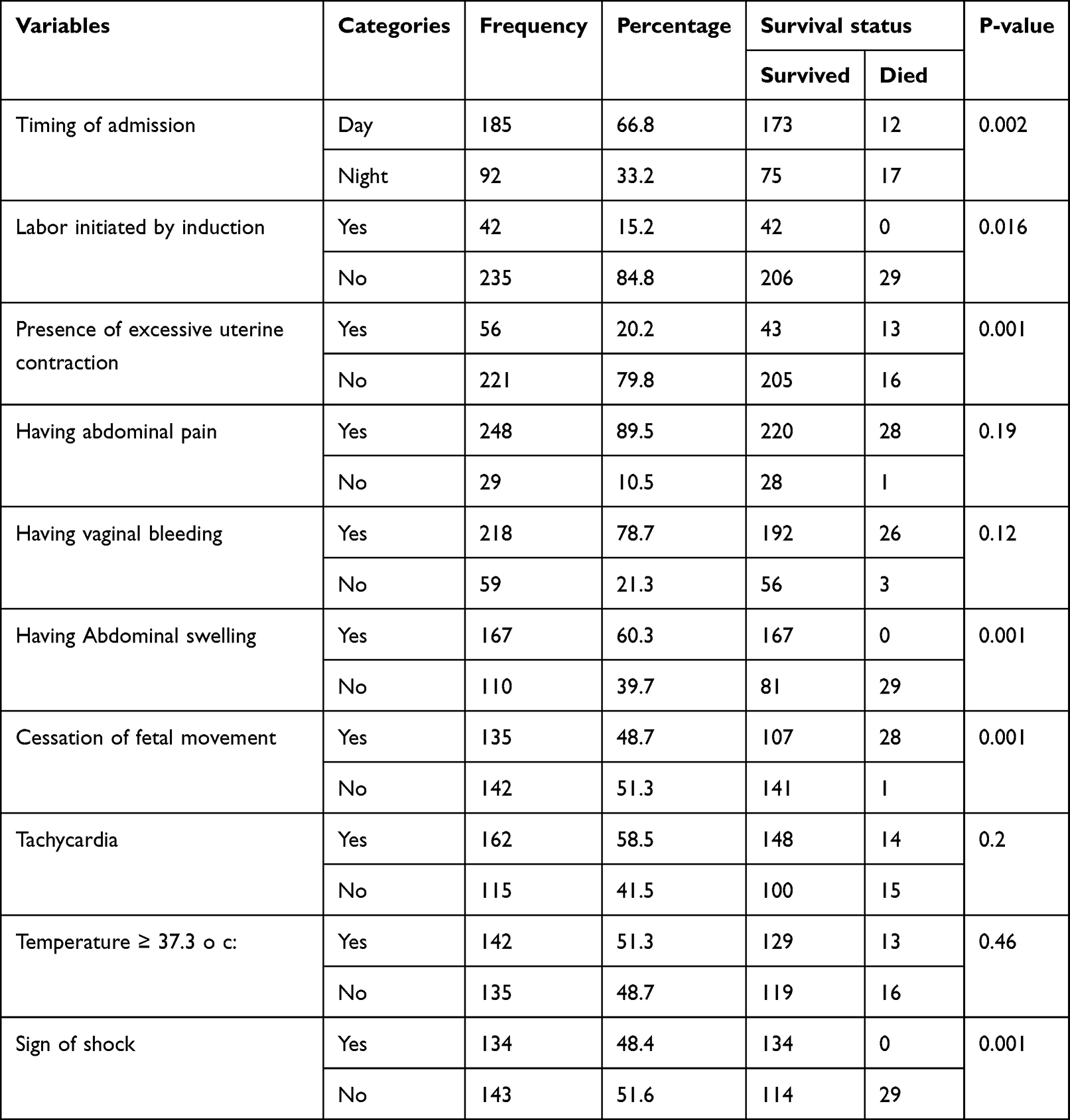 |
Table 2 The Association Between Clinical Characteristics and Survival Status from Uterine Rupture Among Women in Public Hospitals of Harari Region, Ethiopia, 2022 |
Causes and Interventions
The most commonly identified causes of uterine rupture were obstructed labor 124 (44.8%) and previous cesarean section 66 (23.8%) (Figure 1). Regarding previous cesarean sections, the majority of the cesarean sections were lower segment incisions 51 (77.3%) while cesarean sections were classical incisions. Regarding the number of cesarean sections performed, 43 (65.2%) of cesarean sections were performed once while 23 (34.8%) of the cesarean sections were performed more than two times.
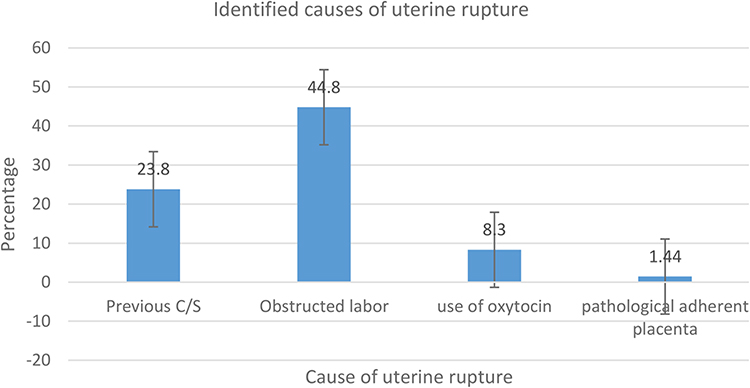 |
Figure 1 Identified causes of uterine rupture among women in public hospitals of Harari region, Ethiopia. 2022. |
Regarding the treatments provided for the study participants, 123 (44.4%) of the cases were managed by surgical repair. While 68 (24.5%) were managed by bilateral tubal ligation and 86 (31.1%) by hysterectomy. Two hundred six (74.4%), 270 (97.5%), and 126 (45.5%) of the cases needed a blood transfusion, fluid resuscitation, and oxygen, respectively.
Survival Status of Women with Uterine Rupture
Of the 277 follow-ups, 248 (89.5) with 95% CI (85.5–92.6) women with uterine rupture have recovered. Meanwhile, 10.5% of women who had uterine rupture died. This finding showed that the median recovery time for women with uterine rupture was 8 days with an interquartile range (IQR) of 7–11 days. The median time to death for women with uterine rupture was 3 days with an interquartile range (IQR) of 2–5 days. The total person-day risk estimated was 2467 person days. The total rate of recovery of women with uterine rupture was 100.53 per 100 person days.
The Kaplan–Meier survival curve shows that the survival plot decreases as time elapses. So, there is a decrease in the survival of women with uterine rupture as the number of days increases. The cumulative probability of failure at the end of the first day was 0.4% (95% CI: 0.05–2.6), at 8–9 days was 50.4% (95% CI: 44.4–56.7), at 12–13 days was 83.4% (95% CI: 78.9–88.1), and at the end of the follow-up was 98.1% (Figure 2).
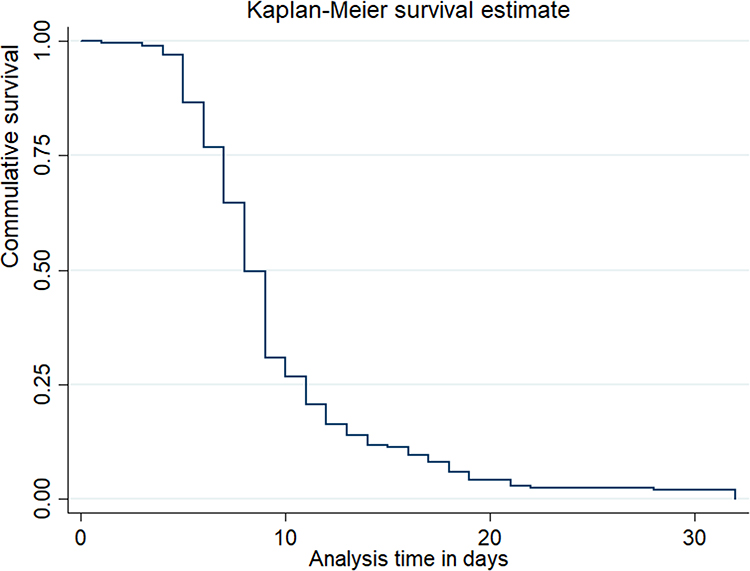 |
Figure 2 Kaplan Meier survival estimate of recovery time of women with uterine rupture in public hospitals of Harari Region, Ethiopia, 2022. |
Test for Equality of Survival Function
A Log rank test was run to see the difference in survival time between different predictors. Accordingly, variables including ANC follow-up, education, time of admission, and visiting health centers than hospitals had significant survival differences. On the other hand, age, gravida, abdominal pain, temperature >37°C, and address did not have significant survival differences. Graphically, there was a significant survival difference between those who had formal education and who did not have formal education. Additionally, there was also a significant survival difference between those who had a body temperature of >37°C and ≤37°C (Figures 3 and 4).
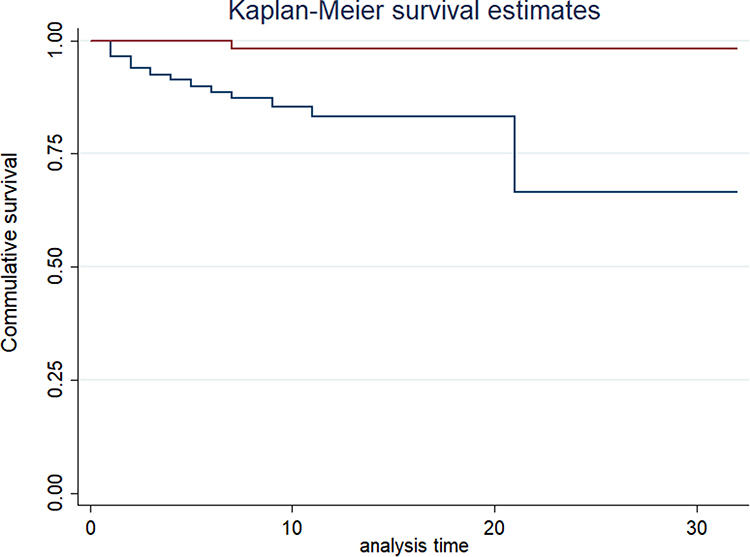 |
Figure 3 Kaplan Meier survival estimate of recovery time by antenatal care follow of women with uterine rupture in public hospitals of Harari Region, Ethiopia, 2022. Notes: ________ ANC = Yes, __________ ANC = No. |
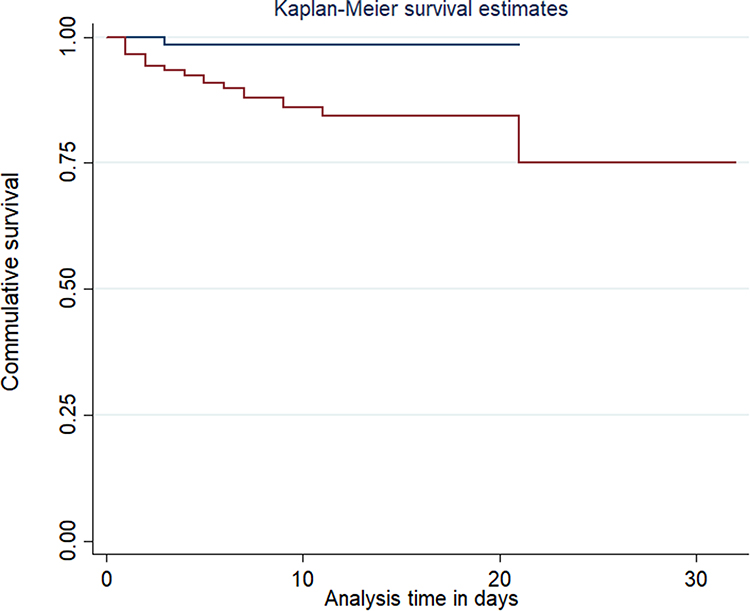 |
Figure 4 Kaplan Meier survival estimate of recovery time by the educational status of women with uterine rupture in public hospitals of Harari Region, Ethiopia, 2022. Notes: ________ Educational status = No formal education, __________ Educational status = had formal education. |
Predictors of Mortality Among Mothers with Uterine Rupture
In the multivariable cox regression model, variables including ANC follow-up, educational status, visiting health facility, and admission time were predictors of mortality among mothers with uterine rupture.
Mothers who did not have ANC follow-up were 4.2 more likely to die than those who had ANC follow-up (AHR: 4.2, 95% CI: 1.81–9.79). Compared to those who did not have formal education, those mothers who had formal education were 88.8% less likely to die (AHR: 0.11; 95% CI: 0.02–0.85). The tendency to die was almost 5 times higher among mothers who visited health centers compared to those who visited hospitals (AHR: 4.89; 95% CI: 1.05–22.88). Mothers who were admitted during nighttime were 4.4 times more likely to die compared to those admitted during the daytime (AHR: 4.4; 95% CI: 1.89–10.18) (Table 3).
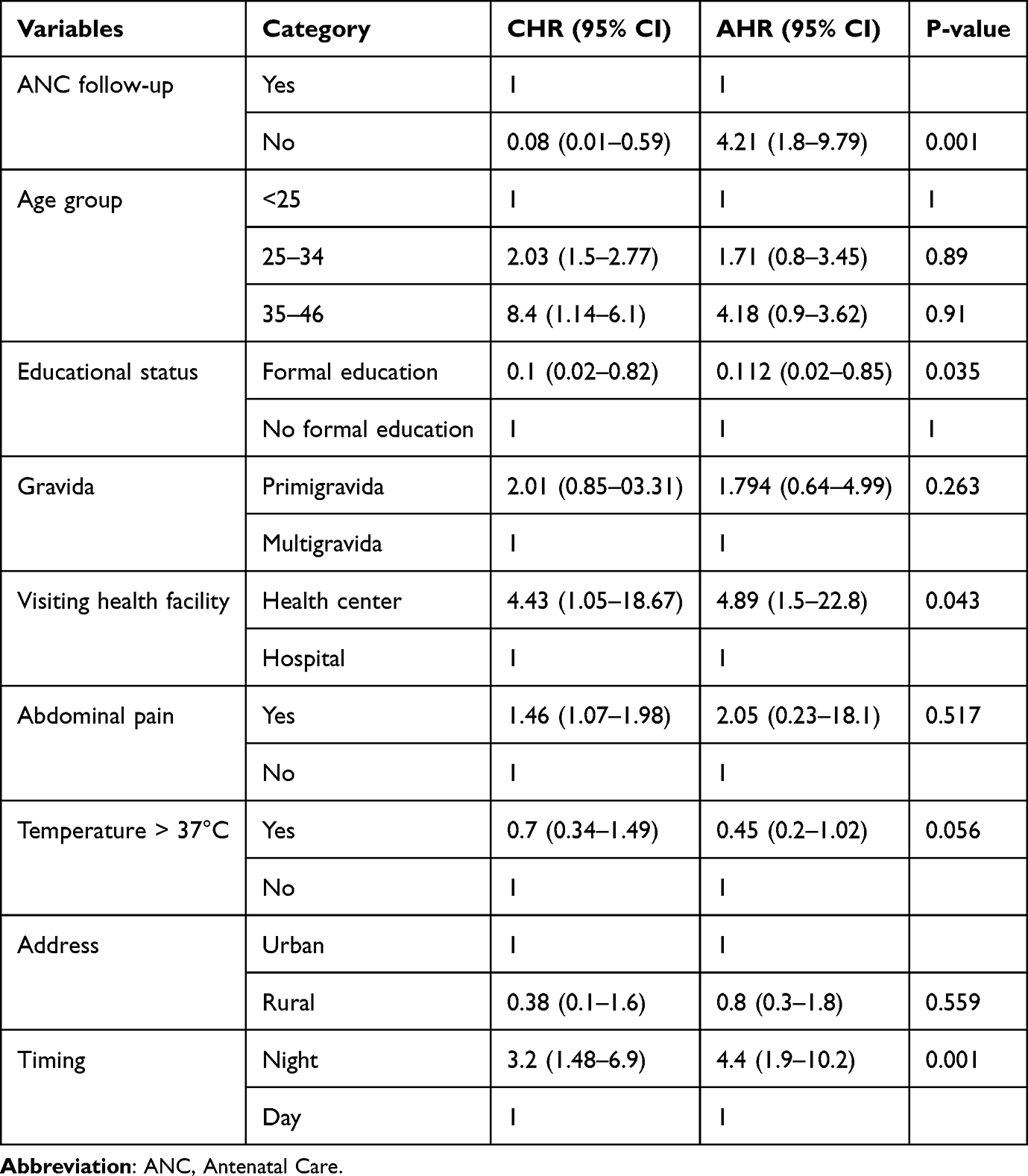 |
Table 3 Predictors of Mortality from Uterine Rupture Among Women in Public Hospitals of Harari Region, Ethiopia, 2022 |
Discussion
This study has assessed the survival status of women with uterine rupture and its predictors. In this study, the median time to death for women with uterine rupture was 3 days with interquartile range (IQR: 2–5 days) and around 10.5% (95% CI: 6.8–15.7%) of women with uterine rupture have died. This study identified that ANC follow-up, educational status, visiting health facility, and admission time were predictors of mortality among mothers with uterine rupture.
In this study, the median time for death for women with uterine rupture was 3 days with interquartile range (IQR: 2–5 days) and around 10.5% (95% CI: 6.8–15.7%) of women with uterine rupture have died. This is in line with studies conducted in Nigeria and at Liaquat University Hospital in Pakistan where the maternal case fatality rate due to uterine rupture was 14.7%.21 and 8.19%,1 respectively. However, this finding is different from studies conducted in Italy22 where there was only one death due to uterine rupture, in the UK where there were only 2 deaths,23 5(2.1%) deaths in Felege Hiwot referral Hospital, Bahir Dar,24 13 (3.7%) deaths in Yirgalem general and teaching hospital, southern Ethiopia,7 and 16 (6.6%) deaths in Debre Markos referral Hospital.25 Additionally, it was also different from studies conducted in New Delhi, India,15 Suhul General Hospital, Shire Town, North West Tigray, Ethiopia,26 Masaryk University Hospital Brno, Czech Republic,27 four health institutions found in the United States,28 France,29 and Massachusetts, United States30 that there was no maternal death associated with uterine rupture. The reason for this discrepancy might be that in the study done in the Czech Republic only 15 uterine rupture cases were identified during the study period but 277 uterine rupture cases were included in this study and the United States, France, and Italy are developed countries with a better health-care delivery system compared to our study site which is a developing country and where around three-fourth of the study participants visited health centers or health institutions with no specialists for treatment prior to going to the hospitals. This implied that there is a delay in referral from health centers to hospitals. The referral linkage should be improved to increase the survival chance of women with uterine rupture.
As revealed in this study result, mothers who did not have ANC follow-up were 4.2 times more likely to die than those who had ANC follow-up. This finding is different from studies conducted at Felege Hiwot referral hospital in Bahir Dar, Ethiopia31 and Yirgalem general and teaching hospital, southern Ethiopia25 where ANC follow-up was not associated with the undesired maternal outcome including death. In another study done in Debre Markos referral hospital, Northwest Ethiopia25 ANC follow-up was not associated with maternal death due to uterine rupture. This might be due to the fact that in the other studies only a small proportion of women did not have ANC follow-up but in our study, more than a quarter of the study participants did not have ANC follow-up. Thus, the tendency to miss the risk factors for uterine rupture is high leading for a higher association with death. It is important to advocate the importance of antenatal care in the identification of high-risk pregnancies and the prevention of undesired maternal outcomes.
In this study, compared to those who did not have formal education, those mothers who had formal education were 88.8% less likely to die due to uterine rupture. This finding is different from the one conducted in Debre Markos referral hospital, Northwest Ethiopia15 where educational status was not associated with death due to uterine rupture. The possible explanation for this difference might be that in the study done in Debre Markos referral hospital, almost three-fourth of the study participants cannot read and write thus this reduces its tendency to associate with death due to uterine rupture since the magnitude of death was only 6.6%. The other reason could be that not having formal education might indirectly lead the mothers not to have ANC follow-up and, in our study, more than a quarter of the participants did not have ANC follow-up and there was a significant association between not having ANC follow-up and death due to uterine rupture.
The study found that the tendency to die was almost 5 times higher among mothers who visited health centers compared to those who visited the hospital. This finding is different from the one conducted at Felege Hiwot referral hospital, Ethiopia where the source of referral to the hospital was not associated with the undesired maternal outcome including death.26 Around three-fourth of the participants were rural residents where their access to hospitals is limited. The health centers found in the area do not have a specialist for the acute management of uterine rupture and the mothers had to be referred to the hospitals found in the city. The risk of dying due to uterine rupture increases as the time between the onset and treatment prolongs. It takes a long time to get to the hospitals so the tendency for them to die after traveling for hours for better management is higher for those who visited health centers at first.
Furthermore, mothers who were admitted during nighttime were 4.4 times more likely to die compared to those who were admitted during the daytime. This finding is different from the one conducted at Felege Hiwot referral hospital, Ethiopia where the time of arrival to the hospital was not associated with the undesired maternal outcome including death.26 The possible explanation for this difference might be that in the other study, the undesired maternal outcomes included not only death but also permanent organ injury, obstetric fistula, wound dehiscence, Sepsis, and ICU admission but in our study, the survival analysis was computed. The other possible explanation could be that most of the specialists are not available in the hospitals during the night time and this might result in a delay in the treatment of uterine rupture which might, in turn, lead the mothers to die.
Generally, this study will be useful for policymakers, and health bureaus to plan and implement a healthcare delivery system that helps to identify risk factors for uterine rupture and address uterine rupture cases as early as possible to prevent death and improve the outcome. It also helps the health institutions to work on enhancing women’s knowledge about uterine rupture by planning and incorporating the issue of uterine rupture in the health education that is provided for the women during ANC follow-up.
Strength and Limitation
One of the strengths of this study is that it included all uterine rupture cases in the study period making the study more representative. Additionally, it is a retrospective cohort study. However, these study findings are not without limitations, since a card review was done to collect the data, we were not able to get all the variables from the card because there were missing values and incomplete records.
Conclusion
More than one-tenth of the study participants died due to uterine rupture. Not having ANC follow-up, not having a formal education, visiting health centers for treatment, and being admitted during the night time were all associated with death due to uterine rupture. Thus, a great emphasis has to be given to the prevention and management of uterine rupture and the linkage within health institutions has to be smooth to improve the survival of patients with uterine rupture with the help of different professionals, health institutions, health bureaus, and policymakers. Multi-sector collaborations can play a vital role in decreasing the mortality rate.
Data Sharing Statement
All relevant data are included in this manuscript. However, additional data will be available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Ethical approval was secured from the Institutional Health Research Ethics Review Committee (IHRERC) of the College of Health and Medical Sciences of Haramaya University, IRB number was IHRERC/106/2022. All methods were carried out in accordance with the national ethical declarations and international ethical declarations (Helsinki declarations).
Before the study commenced, hospital administrators provided informed, voluntary, written, and signed consent. There was no direct contact with patients because the study was based on secondary data. As a result, anonymity was maintained by using the identified number rather than the patients’ names. Furthermore, all extracted data was kept confidential and was not used for any purpose other than the stated objective.
Acknowledgments
We would like to extend our thanks to Haramaya University, College of Health and Medical Science for facilitating this study and for availing working space for this activity.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Haramaya University. The funder has no role in designing the study and reporting the findings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Togioka BM, Tonismae T. Uterine rupture. StatPearls [Internet]. StatPearls; 2021.
2. Herrera FA, Hassanein AH, Bansal V. Atraumatic spontaneous rupture of the non-gravid uterus. J Emerg Trauma Shock. 2011;4(3):439. doi:10.4103/0974-2700.83896
3. Manoharan M, Wuntakal R, Erskine K. Uterine rupture: a revisit. Obstet Gynecol. 2010;12:223–230.
4. Rizwan N, Abbasi RM, Uddin SF. Uterine rupture, frequency of cases, and fetomaternal outcome. J Pak Med Assoc. 2011;61(4):322–324.
5. Kaye DK, Kakaire O, Osinde MO. A systematic review of the magnitude and case fatality ratio for severe maternal morbidity in sub-Saharan Africa between 1995 and 2010. BMC Pregnancy Childbirth. 2011;11:65.
6. Desta M, Amha H, Anteneh Bishaw K, et al. Prevalence and predictors of uterine rupture among Ethiopian women: a systematic review and meta-analysis. PLoS One. 2020;15(11):e0240675.
7. Ahmed DM, Mengistu TS, Endalamaw AG. Incidence and factors associated with outcomes of uterine rupture among women delivered at Felegehiwot referral hospital, Bahir Dar, Ethiopia: a cross-sectional study. BMC Pregnancy Childbirth. 2018;18(1):447.
8. Mengesha MB, Weldegeorges DA, Hailesilassie Y, et al. Determinants of uterine rupture and its management outcomes among mothers who gave birth at public hospitals of Tigrai, North Ethiopia: an unmatched case-control study. J Pregnancy. 2020;2020:8878037.
9. Ashimi AO, Omole-Ohonsi A, Ugwa AE, Amole TG. Prospective surveillance of ruptured uterus in a rural tertiary health facility in Northwest Nigeria. J Matern Fetal Neonatal Med. 2014;27(16):1684–1687.
10. Abebe F, Mannekulih E, Megerso A, Idris A, Legese T. Determinants of uterine rupture among cases of Adama city public and private hospitals, Oromia, Ethiopia: a case-control study. Reprod Health. 2018;15(1):161. doi:10.1186/s12978-018-0606-4
11. Mukasa PK, Kabakyenga J, Senkungu JK, Ngonzi J, Kyalimpa M, Roosmalen VJ. Uterine rupture in a teaching hospital in Mbarara, western Uganda, unmatched case-control study. Reprod Health. 2013;10(1):1–6. doi:10.1186/1742-4755-10-29
12. Omole-Ohonsi A, Attah R. Risk factors for ruptured uterus in a developing country. Gynecol Obstetric. 2011;1(102):2161–2932.
13. Berhan Y, Berhan A. Causes of maternal mortality in Ethiopia: a significant decline in abortion-related death. Ethiop J Health Sci. 2014;24:15–28. doi:10.4314/ejhs.v24i0.3S
14. Dagne Addisu MM, Melkie A, Necho W. The burden of uterine rupture and its determinant factors in Ethiopia: a systematic review and meta-analysis. Hindawi. 2020;2020:1–2.
15. Astatikie G, Limenih MA, Kebede M. Maternal and fetal outcomes of uterine rupture and factors associated with maternal death secondary to uterine rupture. BMC Pregnancy Childbirth. 2017;17(1):117. doi:10.1186/s12884-017-1302-z
16. Abrahams Z, Jacobs Y, Mohlamonyane M, et al. Implementation outcomes of health systems strengthening intervention for perinatal women with common mental disorders and experiences of domestic violence in South Africa: pilot feasibility and acceptability study. BMC Health Serv Res. 2022;22(1):641. doi:10.1186/s12913-022-08050-x
17. Pattinson RC, Makin JD, Pillay Y, Van den Broek N, Moodley J. Basic and comprehensive emergency obstetric and neonatal care in 12 South African health districts. S Afr Med J. 2015;105(4):256–260. doi:10.7196/SAMJ.9181
18. Committee opinion no. 590: preparing for clinical emergencies in obstetrics and gynecology. Obstet Gynecol. 2014;123(3):722–725. doi:10.1097/01.AOG.0000444442.04111.c6
19. Pattinson RC, Bergh AM, Makin J, et al. Obstetrics knowledge and skills training as a catalyst for change. S Afr Med J. 2018;108(9):748–755. doi:10.7196/SAMJ.2018.v108i9.13073
20. Getahun WT, Solomon AA, Kassie FY, Kasaye HK, Denekew HT. Uterine rupture among mothers admitted for obstetrics care and associated factors in referral hospitals of Amhara regional state, institution-based cross-sectional study, Northern Ethiopia, 2013–2017. PLoS One. 2018;13(12):e0208470. doi:10.1371/journal.pone.0208470
21. Ali AA, Adam I. Maternal and perinatal outcomes of uterine rupture in the Kassala Hospital, east Sudan: 2006–2009. J Obstet Gynaecol. 2011;31(1):48–49. doi:10.3109/01443615.2010.522268
22. Aziz N, Yousfani S. Analysis of uterine rupture at university teaching hospital Pakistan. Pak J Med Sci. 2015;31(4):920–924. doi:10.12669/pjms.314.7303
23. Donati S, Fano V, Maraschini A. Uterine rupture: results from a prospective population-based study in Italy. Eur J Obstet Gynecol Reprod Biol. 2021;264:70–75. doi:10.1016/j.ejogrb.2021.07.001
24. Fitzpatrick KE, Kurinczuk JJ, Alfirevic Z, Spark P, Brocklehurst P, Knight M. Uterine rupture by intended mode of delivery in the UK: a national case-control study. PLoS Med. 2012;9(3):e1001184. doi:10.1371/journal.pmed.1001184
25. Gebretsadik A, Hagos H, Tefera K. Outcome of uterine rupture and associated factors in Yirgalem general and teaching hospital, southern Ethiopia: a cross-sectional study. BMC Pregnancy Childbirth. 2020;20(1):256.
26. Marwah S, Singh S, Bharti N, Gupta PK, Factors R. Outcome analysis in rupture of gravid uterus: lessons for obstetricians. Cureus. 2022;14(2):e21890.
27. Marie Bereka T, Mulat Aweke A, Eshetie Wondie T. Associated factors and outcome of uterine rupture at Suhul General Hospital, Shire Town, North West Tigray, Ethiopia 2016: a Case-Control Study. Obstet Gynecol Int. 2017;2017:8272786.
28. Andonovova V, Hruban L, Gerychova R, Janku P, Ventruba P. Uterine rupture during pregnancy and delivery: risk factors, symptoms, and maternal and neonatal outcomes - retrospective cohort. Ceska Gynekol. 2019;84(2):121–128.
29. Finnsdottir SK, Maghsoudlou P, Pepin K, et al. Uterine rupture and factors associated with adverse outcomes. Arch Gynecol Obstet. 2022;22:1–8.
30. Markou GA, Muray JM, Poncelet C. Risk factors and symptoms associated with maternal and neonatal complications in women with uterine rupture. 16 years of multicentric experience. Eur J Obstet Gynecol Reprod Biol. 2017;217:126–130.
31. Barger MK, Nannini A, Weiss J, et al. Severe maternal and perinatal outcomes from uterine rupture among women at term with a trial of labor. J Perinatol. 2012;32(11):837–843.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Thrombocytopenia Among Pregnant Women in Southwest Ethiopia: Burden, Severity, and Predictors
Haile K, Kebede S, Abera T, Timerga A, Mose A
Journal of Blood Medicine 2022, 13:275-282
Published Date: 26 May 2022
COVID-19 Case Fatality Rate and Factors Contributing to Mortality in Ethiopia: A Systematic Review of Current Evidence
Girma D, Dejene H, Adugna L, Tesema M, Awol M
Infection and Drug Resistance 2022, 15:3491-3501
Published Date: 4 July 2022
Incidence and Predictors of Recurrence and Mortality Following First Venous Thromboembolism Among the Saudi Population: Single-Center Cohort Study
AlEidan FAS, AlManea RK, AlMoneef AT, Shalash NA, AlRajhi NA, AlMousa SF, Al Raizah A, Abuelgasim KA
International Journal of General Medicine 2022, 15:7559-7568
Published Date: 28 September 2022
Incidence and Predictors of Cardiac Arrest Among Patients Admitted to the Intensive Care Units of a Comprehensive Specialized Hospital in Central Ethiopia
Ashine TM, Heliso AZ, Babore GO, Ezo E, Saliya SA, Muluneh BB, Alaro MG, Adeba TS, Sebro SF, Hailu AG, Abdisa EN
Patient Related Outcome Measures 2024, 15:31-43
Published Date: 15 February 2024