")
Back to Journals » Cancer Management and Research » Volume 11
Survival and intracranial control outcomes of whole-brain radiotherapy (WBRT) alone versus WBRT plus a radiotherapy boost in non-small-cell lung cancer with brain metastases: a single-institution retrospective analysis
Authors Lu F , Hou Y, Xia YX, Li L, Wang L, Cao K, Chen HX, Chang L, Li WH
Received 30 January 2019
Accepted for publication 9 April 2019
Published 8 May 2019 Volume 2019:11 Pages 4255—4272
DOI https://doi.org/10.2147/CMAR.S203461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Fei Lu,1,2 Yu Hou,1 Yaoxiong Xia,1 Lan Li,1 Li Wang,1 Ke Cao,1 Haixia Chen,1 Li Chang,1 Wenhui Li1
1Department of Radiation Oncology, The Third Affiliated Hospital of Kunming Medical University, Tumor Hospital of Yunnan Province, Kunming, Yunnan, People’s Republic of China; 2Department of Oncology and Hematology, The First People’s Hospital of Honghe State, Mengzi, Yunnan, People’s Republic of China
Purpose: To compare the differences in survival and intracranial local control between patients treated with whole-brain radiotherapy (WBRT) and WBRT plus a radiotherapy boost (RTB) in non-small-cell lung cancer (NSCLC) patients with brain metastases (BMs).
Patients and methods: Between May 2010 and October 2017, 206 NSCLC patients with BMs were treated with brain radiotherapy; among these patients, 140 patients underwent WBRT alone (group A) and 66 patients underwent WBRT plus RTB (group B). The endpoints included intracranial local progression-free survival and regional progression-free survival time (iLPFS and iRPFS, respectively) and overall survival (OS).
Results: Between the two groups, not all baseline clinical factors were well-balanced. The median iLPFS was 17.9 months in group A and 22.3 months in group B. The 2-year iLPFS rates were significantly lower in group A than in group B (34.5% vs 49.3%, P=0.041); however, no significant differences were observed in OS or iRPFS. Multivariate analyses revealed that epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKIs) therapy was significantly associated with good OS, iLPFS, and iRPFS. Among the patients treated with TKIs (n=62), there were no differences in OS (P=0.190), iLPFS (P=0.334), or iRPFS (P=0.338) between groups A and B. In the patients without TKI treatment (n=102), the median iLPFS was significantly longer in group B than in group A (16.7 vs 12.0 months, P=0.032), but no significant differences were found in OS (p=0.182) or iRPFS (P=0.837) between the two groups.
Conclusion: WBRT plus RTB significantly improved iLPFS compared with WBRT alone, especially in patients without EGFR-TKI treatment. However,there were no significant differences in iRPFS or OS between the two groups. Patients treated with EGFR-TKIs may not benefit from WBRT plus RTB.
Keywords: non-small-cell lung carcinoma, brain metastases, brain radiotherapy, radiotherapy boost, tyrosine kinase inhibitor
Introduction
Lung cancer is the most common cause of cancer death throughout China and the world.1,2 Non-small-cell lung cancer (NSCLC) accounts for 87% of lung cancer cases, and up to 30% of NSCLC patients will present with or develop brain metastases (BMs) at some point in their disease course.3,4 Patients with BMs commonly have poor prognoses, and untreated patients have a median survival of just 2–3 months.5,6
Radiotherapy, as an important treatment for controlling neurologic symptoms and prolonging survival, is widely used in patients with BMs. During the past 50 years, whole-brain radiotherapy (WBRT) has been the standard treatment for BMs, but WBRT alone has an unsatisfactory effect with an intracranial control rate (ICR) of 60% and a median survival of just 3–6 months.7,8 Several studies have shown that WBRT plus an in-field radiotherapy boost (RTB) for BMs could improve ICR versus WBRT alone, and select patients could experience significant survival benefits.9–12
Currently, there is increasing evidence that epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKIs) alone or EGFR-TKIs plus brain radiotherapy can effectively control intracranial metastases in patients with EGFR-mutant NSCLC.13–17 EGFR-TKIs have recently been considered as a first-line treatment option for advanced metastatic mutated NSCLC patients, and an increasing number of patients are receiving EGFR-TKI treatment.18 Among the research on WBRT plus RTB mentioned above, only one single-arm study analyzed targeted therapy and identified that a history of EGFR-TKI treatment indicated good survival. However, this study lacked a control group and included only 11 patients who received EGFR-TKIs.11 In the era of targeted therapy, there are few case–control studies to reevaluate the efficacy of WBRT versus WBRT plus RTB. Therefore, the aim of this single-center retrospective study was to reassess the survival and intracranial control differences between WBRT and WBRT plus RTB.
Material and methods
Study design and patients
In total, 860 patients diagnosed with lung cancer with BMs between May 2010 and October 2017 in the Third Affiliated Hospital of Kunming Medical University (Kunming, China) were retrospectively reviewed. The eligibility criteria were as follows: 1) patients with age ≥18 years old, 2) patients with cytologically or histologically proven NSCLC, 3) patients with BMs confirmed by gadolinium-enhanced MRI or contrast-enhanced CT, 4) patients treated with brain radiotherapy, and 5) patients with enough information available. Patients were excluded if they had cytologically or histologically proven small-cell lung cancer (SCLC), interrupted treatment for more than 1 week during brain radiotherapy, or presented with other tumors. This study was approved by the Ethics Committee of the Third Affiliated Hospital of Kunming Medical University. Informed consent was waived by the committee because of the retrospective nature of this study. This trial was conducted in accordance with the Declaration of Helsinki. We confirm that patient data confidentiality was maintained.
Clinical and treatment data, including sex, age, Karnofsky Performance Scale (KPS) score, history of smoking, histology, number of BMs, location and maximum diameter of the brain lesions, treatment regimen before and after the detection of BMs, extracranial metastases (EMs) status when the BMs were confirmed, number of organs with EMs, the time interval from cancer diagnosis to confirmed BMs and from the diagnosis of BMs to the initiation of brain radiotherapy, epidermal growth factor receptor (EGFR) mutation status, targeted treatment regimen, brain radiotherapy information, data on recursive partitioning analysis (RPA),19,20 graded prognostic assessment (GPA),21,22 and treatment responses, were recorded.
Radiation treatment planning and delivery
In total, 206 patients were eligible for this study (Figure 1). All patients underwent WBRT with a median dose of 40 Gy/20f (range, 16–56 Gy/8-28f, 5 f/week). Among the patients, 33 patients (16%) received 30 Gy/10f, 24 patients (11.7%) received 36 Gy/18f, 76 patients (36.9%) received 40 Gy/20f, 41 patients (19.9%) received 46 Gy/23f, and 32 patients (15.5%) received a median dose of 41.4 Gy/23f. For the radiotherapy technology of WBRT, 2DCRT was used for 127 patients (61.7%), 3DCRT was used for 62 patients (30.1%), and IMRT was used for 17 patients (8.3%). Of the 206 patients, based on the judgment of radiation oncologists according to the tumor volume, tumor location, and neurological symptoms, 66 patients (32%) underwent concurrent or sequential local lesion RTB with a median dose of 11 Gy (range, 6–21.6 Gy) with 3DCRT (n=36) or IMRT (n=30). The PTV boost was defined as a 3 mm margin to the GTV boost. Of these 66 patients, 31 patients (47.0%) received concurrent RTB and 35 patients (53.0%) received sequential RTB.
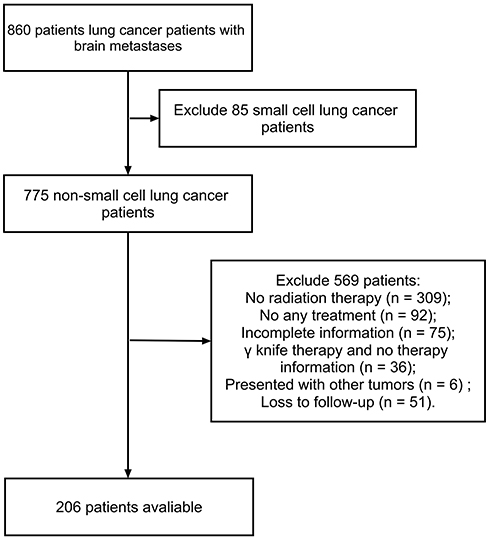 | Figure 1 Trial profile. |
Follow-ups and endpoints
All patients underwent clinical follow-up examinations, including contrast-enhanced MRI or contrast-enhanced CT of the head 1 month after the end of radiotherapy and every 3 months thereafter. The intracranial response was assessed by the new Response Evaluation Criteria in Solid Tumors (RECIST) 1.1.23 Overall survival (OS) was calculated from the day of BM confirmation to death or the last day of follow-up. Intracranial local progression-free survival (iLPFS) was the time from the end of brain radiotherapy to the progression of previously treated brain lesions or the last day of follow-up. Intracranial regional progression-free survival time (iRPFS) was defined as the time from the completion of brain radiotherapy to the day of new BM diagnoses or the last day of follow-up.
Statistical analyses
Survival curves were generated using the Kaplan–Meier method and compared using the log-rank test. The log-rank test was also used for univariate analyses of prognostic factors. The variables with P-values of <0.1 from univariate analyses were further analyzed in the multivariate analyses using the Cox proportional hazards regression model to assess prognostic factors related to OS, iLPFS, and iRPFS. The characteristics of the patients in the two groups were compared using the Chi-square test for categorical variables and the independent sample Student’s t-test for continuous variables. Tests were two-sided, and P<0.05 was considered statistically significant. The statistical analyses were conducted with SPSS (version 22.0; IBM Corp., Armonk, NY, USA) and STATA (version 12.0; Stata Corporation LP, College Station, TX, USA).
Results
Baseline characteristics of the patients
Patients were divided into two groups based on their brain radiotherapy method: one group was treated with WBRT alone (WBRT-alone group) and another group was treated with WBRT plus RTB (WBRT plus RTB group). Patient characteristics in both treatment groups are described in Table 1. For the entire cohort, the median age was 54 years (range, 28–76 years). There were 119 males (57.8%) and 87 females (42.2%). A total of 98 patients (47.6%) had detected BMs at the time of their initial diagnosis of NSCLC and 155 patients (75.2%) had confirmed BMs within the first year. The majority of patients (88.8%) had a pathological type of adenocarcinoma. More than half of the patients (61.7%) had EMs at the baseline of the BMs. In total, 51.5% (106/206) of the patients received targeted therapy, 104 patients were treated with EGFR-TKIs, and 7 patients received vascular endothelial growth factor receptor (VEGFR) inhibitors. Several patients used more than one drug, and 2 patients only used VEGFR inhibitors. 47 patients received first-line EGFR-TKI treatment. However, EGFR-mutant information was only available for 62 patients, and the EGFR status of 42 patients who received EGFR-TKI treatment was unknown. The patients without EGFR information were mainly diagnosed before 2014. At that time, EGFR mutation testing relied mainly on tumor tissue, but liquid biopsy or circulating-free tumor DNA was not be used, so some patients were unable to perform genetic testing due to the small tumor samples.24–26 For this reason, some patients continued to use TKIs after clinically confirmed effectiveness of the treatment without EGFR gene sequencing.
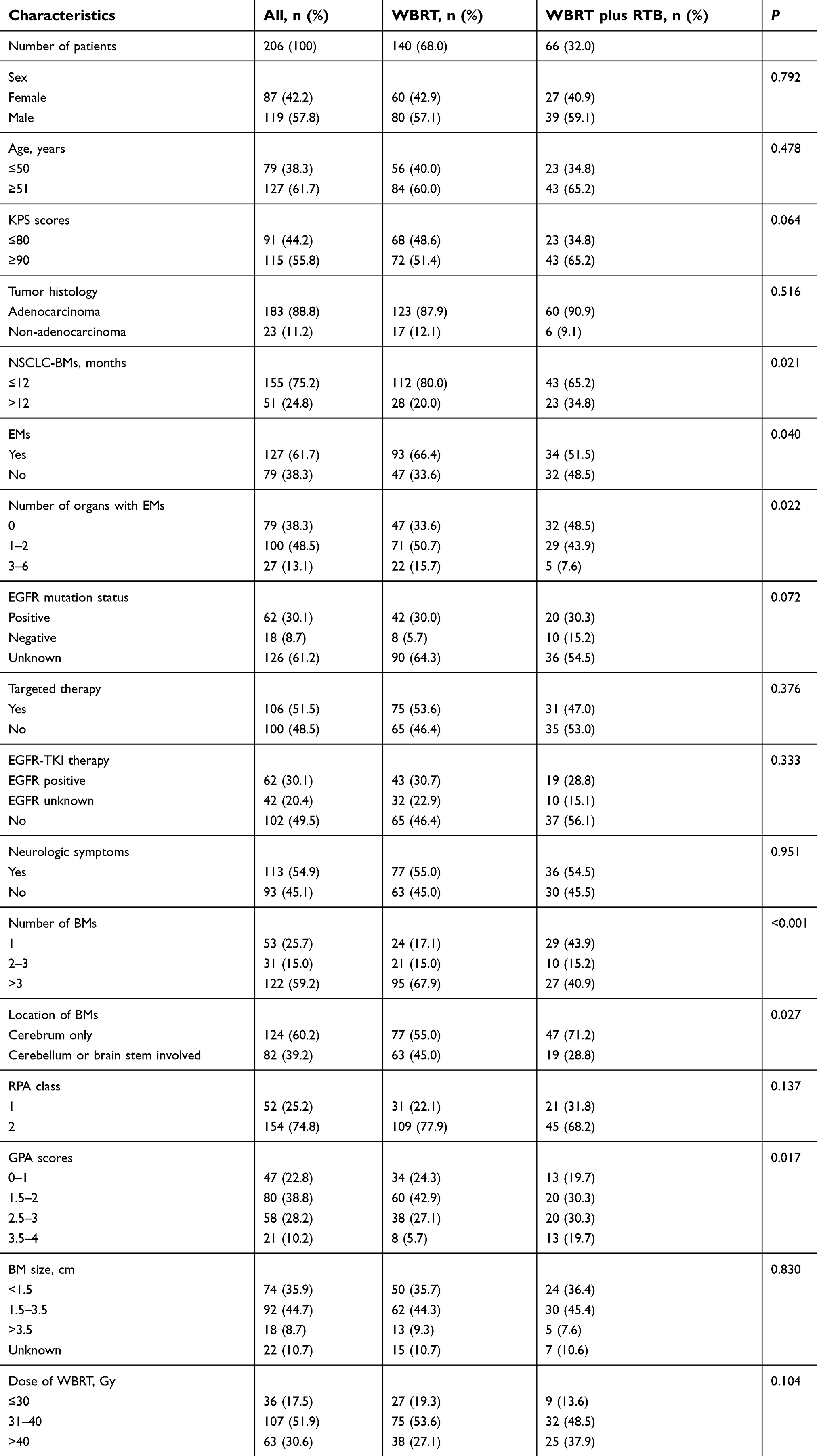 | Table 1 Patient baseline characteristics |
Compared with patients in the WBRT plus RTB group, more patients were diagnosed BMs within the first year of disease (80.0% vs 65.2%, P=0.021) and more patients had EMs (66.4% vs 51.5%, P=0.040) and more than 3 brain lesions (67.9% vs 40.9%, P=0.000) in the WBRT-alone group. The WBRT-alone group also included more patients with BMs located in the cerebellum or brain stem (45% vs 28.8%, P=0.027) and more patients with lower GPA scores (P=0.017) than the WBRT plus RTB group. Other clinical features, including sex, age, KPS score, pathological type, number of organs with EMs, EGFR status, targeted therapy regimen, neurological symptoms, RPA class, maximum diameter of the brain lesions, and radiation dose of WBRT, were well-balanced between the two study groups.
Overall survival
The median follow-up time was 22.7 months (range, 0.5–98.4 months). By the last follow-up visit, 97 patients (47.1%) had died, which included 74 patients in the WBRT-alone group and 23 patients in the WBRT plus RTB group.
For the entire cohort, the median OS was 25.8 months, and the 6-, 12-, and 24-month OS rates were 95.6%, 79.2%, and 55.7%, respectively (Figure 2A). The median OS in the WBRT-alone group was 25.8 months, and the median OS in the WBRT plus RTB group was 37.6 months. The 6-, 12-, and 24-month OS rates in the WBRT-alone group were 95.0%, 75.6%, 54.9%, and 97.0%, 86.9%, 56.4% in the WBRT plus RTB group, respectively (P=0.200; Figure 2D).
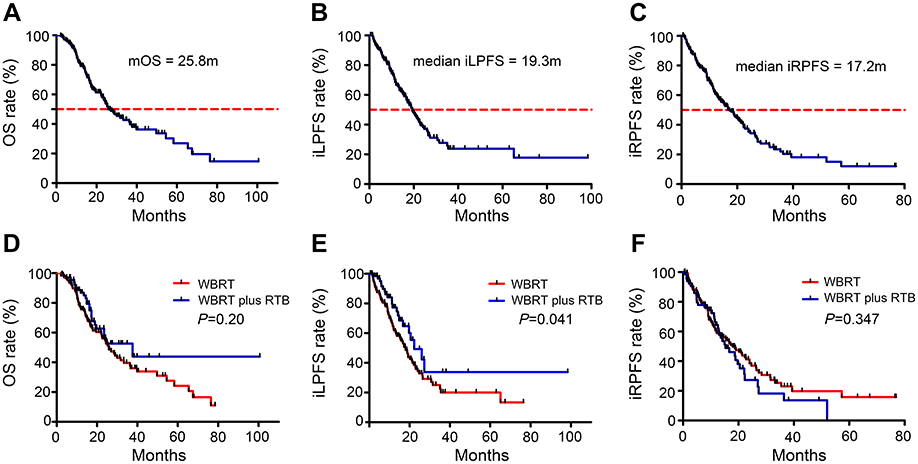 | Figure 2 Cumulative incidence of OS (A), iLPFS (B), and iRPFS (C) for all patients; comparison of cumulative incidence of OS (D), iLPFS (E), and iRPFS (F) between WBRT-alone group and WBRT plus RTB group. Abbreviations: mOS, median overall survival; iLPFS, intracranial local progression-free survival; iRPFS, intracranial regional progression-free survival; WBRT, whole-brain radiotherapy; RTB, radiotherapy boost. |
Univariate and multivariate analyses were performed to determine the prognostic predictors for OS (Table 2). The univariate analysis revealed that ages ≤50 years (P=0.050), treatment with EGFR-TKIs therapy (P<0.001), absence of neurologic symptoms (P=0.027), RPA class 1 (P=0.005), good GPA scores (P=0.049), and no chemotherapy treatments during or after brain radiotherapy (P=0.020 and 0.045, respectively) were significantly associated with a better OS. The multivariate analysis found that RPA class 2 (HR: 1.914, 95% CI: 1.027–3.567, P=0.041), smoking (HR: 1.619, 95% CI: 1.027–2.552, P=0.038), poor GPA score (P=0.039), and treatment without EGFR-TKI therapy (HR: 3.402, 95% CI: 1.920–6.027, P<0.001) were independent factors associated with worse OS. The median OS of patients treated with EGFR-TKIs regardless of EGFR status was significantly better than patients treated without targeted therapy, and EGFR mutation-positive patients had a surprising median OS of 58.3 months.
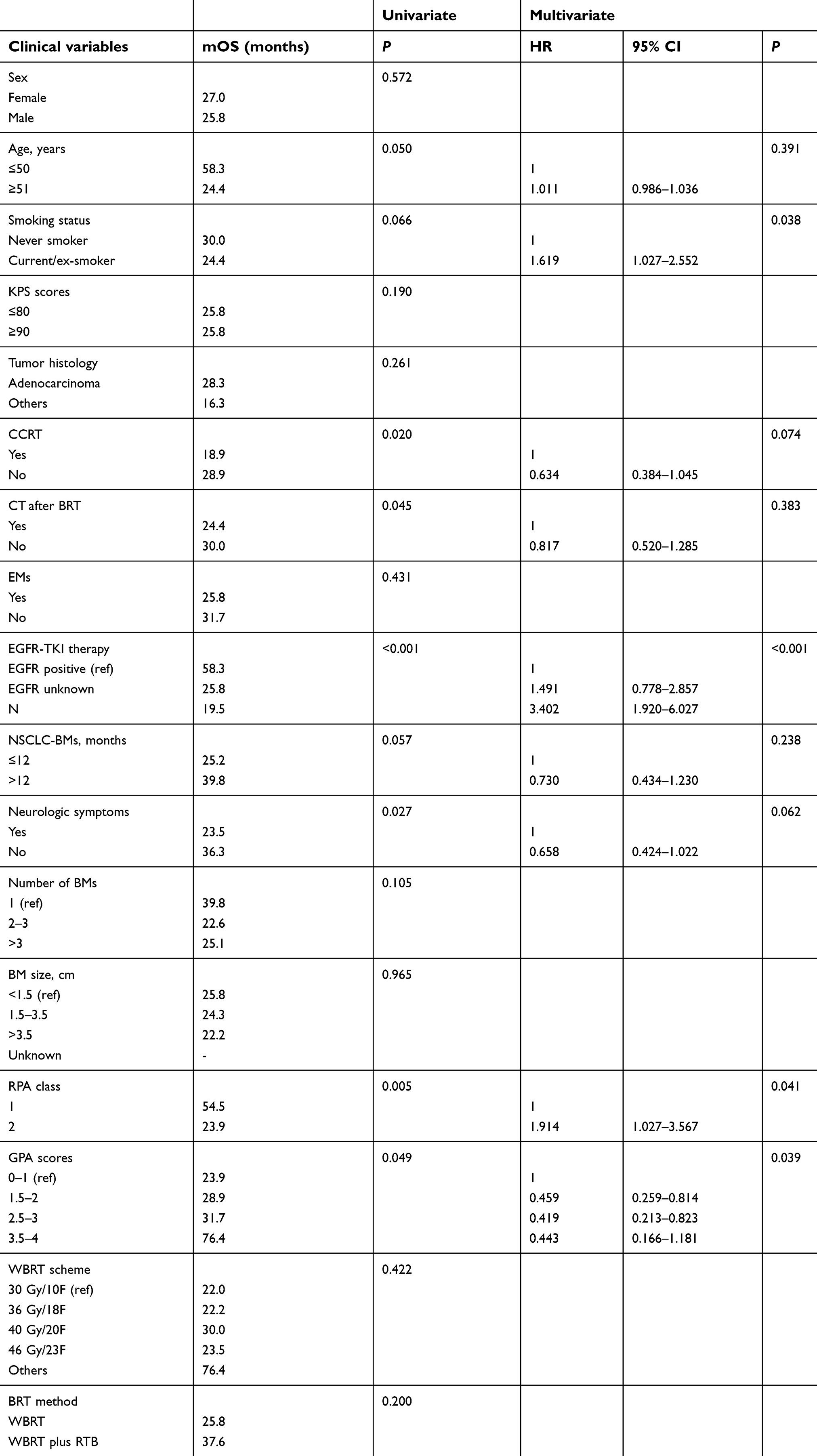 | Table 2 Univariate and multivariate analyses for OS |
Intracranial local progression-free survival
In all patients, the median iLPFS was 19.3 months, and the 1- and 2-year iLPFS rates were 67.3% and 38.4%, respectively (Figure 2B). The median iLPFS was 17.9 months in the WBRT-alone group and 22.3 months in the WBRT plus RTB group. The 2-year iLPFS rates were significantly lower in the WBRT-alone group than in the WBRT plus RTB group (34.5% vs 49.3%, P=0.041, Figure 2E).
The univariate analysis revealed that treatment with EGFR-TKI therapy (P=0.004), few brain lesions (P=0.016), good GPA score (P=0.006), and treatment with WBRT plus RTB (P=0.041) were significantly associated with better iLPFS. Multivariate analysis indicated that the independent favorable prognostic factors for iLPFS were treatment with EGFR-TKI therapy (P=0.001), RPA class 1 (P=0.034), and good GPA scores (P=0.002, Table 3). However, the difference in iLPFS between brain radiotherapy methods in the multivariate analysis was not significant (P=0.354). The WBRT scheme was significant in the univariate but not significant in multivariate analyses (P=0.054). Due to the complexity of radiotherapy schemes, the most appropriate radiotherapy scheme could not be established.
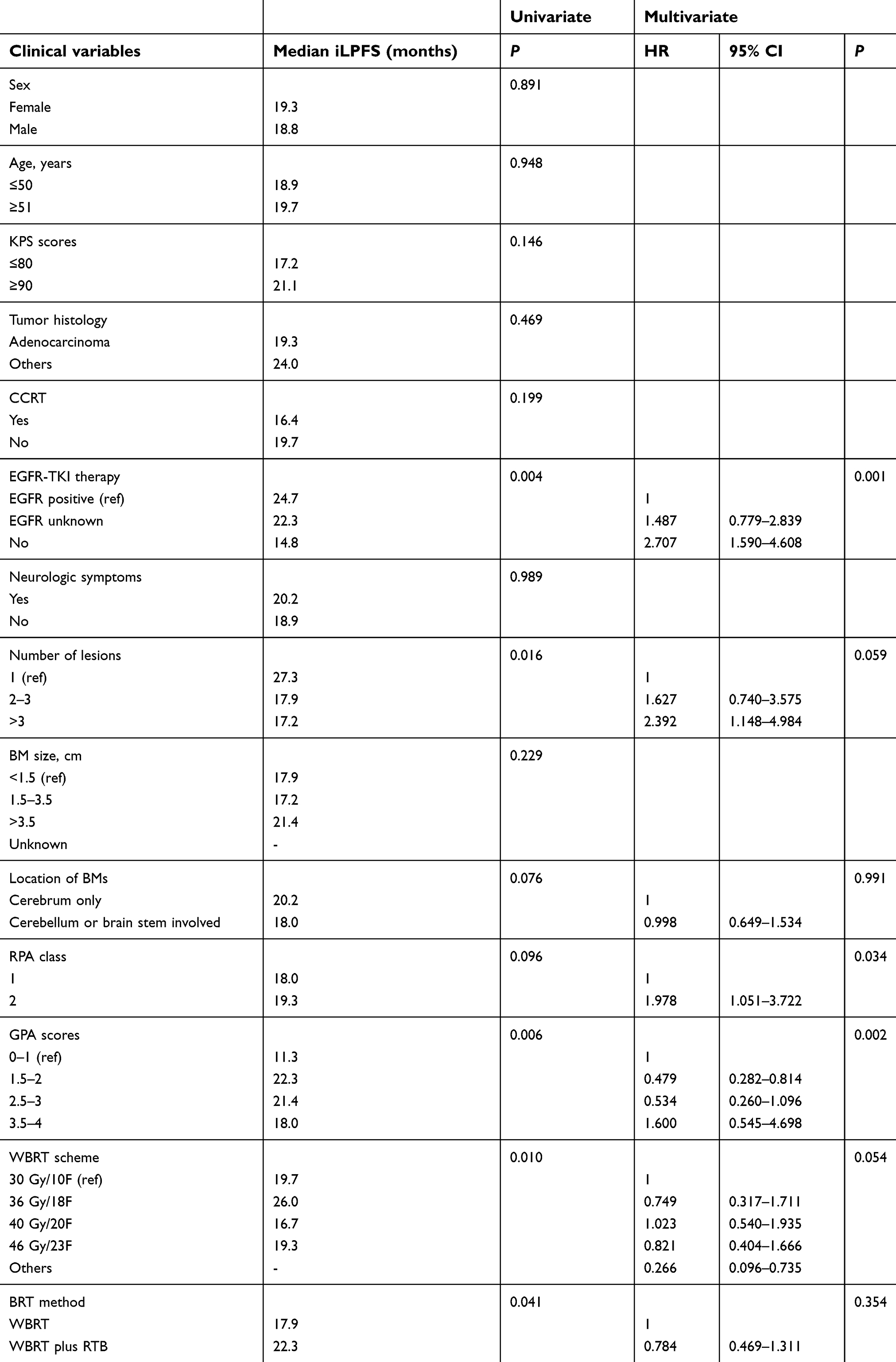 | Table 3 Univariate and multivariate analyses for iLPFS |
Intracranial regional progression-free survival
The median iRPFS was 17.2 months among all patients, 17.9 months in the WBRT-alone group, and 15.3 months in the WBRT plus RTB group. The 2-year iRPFS rates were 35.3% among all patient subgroups (Figure 2C). The 2-year iRPFS rate was not significantly different between the two groups (38.4% for the WBRT-alone group and 27.3% for the WBRT plus RTB group, P=0.347, Figure 2F).
In univariate analysis, no chemotherapy treatments during brain radiotherapy (P=0.005), no EMs at baseline (P=0.037), treatment with EGFR-TKI therapy (P=0.011), RPA class 1 (P=0.030), and good GPA scores (P=0.013) were significant predictors for better iRPFS. Multivariate analysis indicated that no chemotherapy during brain radiotherapy (P=0.002), few brain lesions (P=0.025), treatment with EGFR-TKI therapy (P<0.001), and good GPA scores (P=0.025) were independent favorable risk factors for iRPFS (Table 4). The method of brain radiotherapy showed no significant difference in the univariate analysis (P=0.347) and was not analyzed in the multivariate analysis.
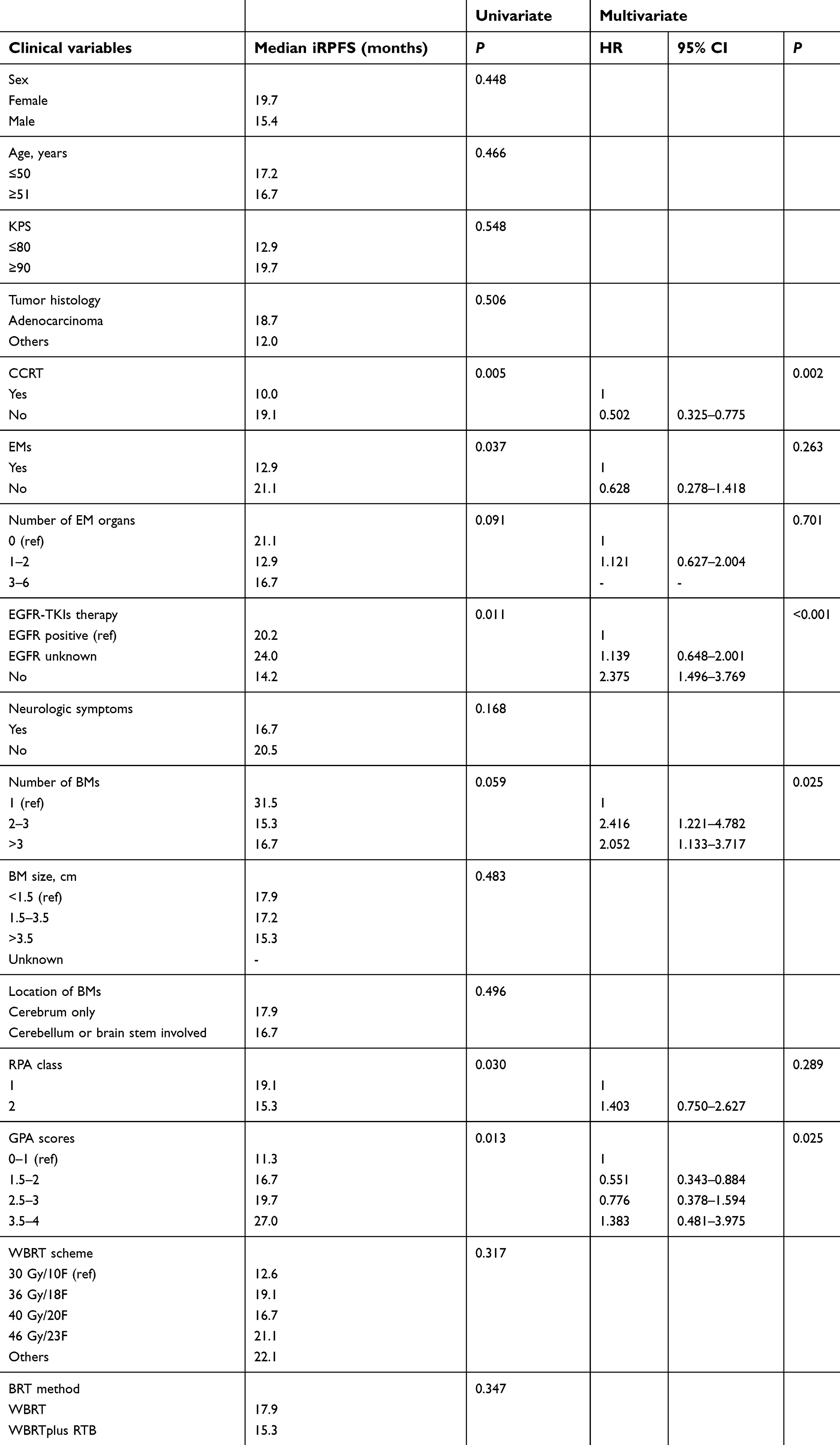 | Table 4 Univariate and multivariate analysis for iRPFS |
Subgroup analysis of patients treated with EGFR-TKI therapy
From the results of univariate and multivariate analyses, we concluded that treatment with EGFR-TKI therapy was an independent prognostic factor associated with OS, iLPFS, and iRPFS. Therefore, we further performed a subgroup analysis of patients treated with EGFR-TKI therapy to explore the survival and intracranial local control differences between the two treatment groups. In total, 104 patients (50.5%) received TKI therapy and 42 patients were excluded from the analysis because the EGFR status of them was unknown. The median age of the remaining 62 patients was 55 years (range, 28–72 years). 43 patients (69.4%) underwent WBRT alone and 19 patients were treated with WBRT plus RTB. Baseline characteristics between the WBRT group and the WBRT plus RTB group were well-balanced except for the number of brain lesions. There were more patients with more than 3 lesions in the WBRT-alone group compared with those in the WBRT plus RTB group (74.4% vs 31.6%, P=0.002, Table 5).
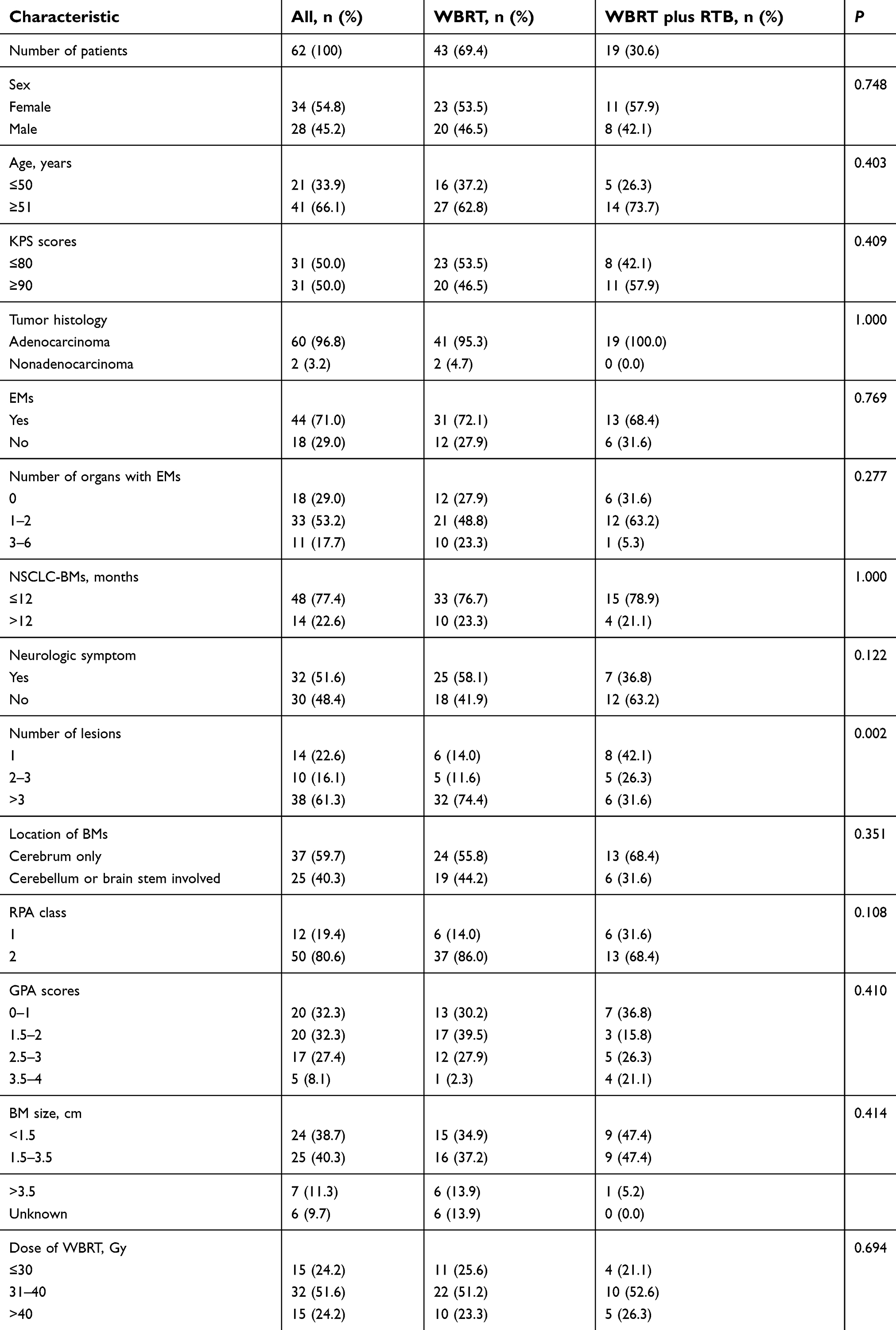 | Table 5 Baseline characteristics of patients with EGFR-TKI therapy |
The 62 patients had a surprising median OS of 58.3 months, and the median iLPFS and iRPFS were 24.7 months and 20.2 months, respectively. The median OS was 58.3 months in the WBRT-alone group and had not yet been reached in the WBRT plus RTB group by the last follow-up. There was no difference in median OS between the two treatment groups (P=0.190, Figure 3A). The median iLPFS was 24.7 months in the WBRT-alone group and had also been reached in the WBRT plus RTB group (P=0.334, Figure 3B). A significant difference in median iRPFS was also not found between the two groups (26.5 months in the WBRT-alone group and 12.9 months in the WBRT plus RTB group, P=0.338, Figure 3C).
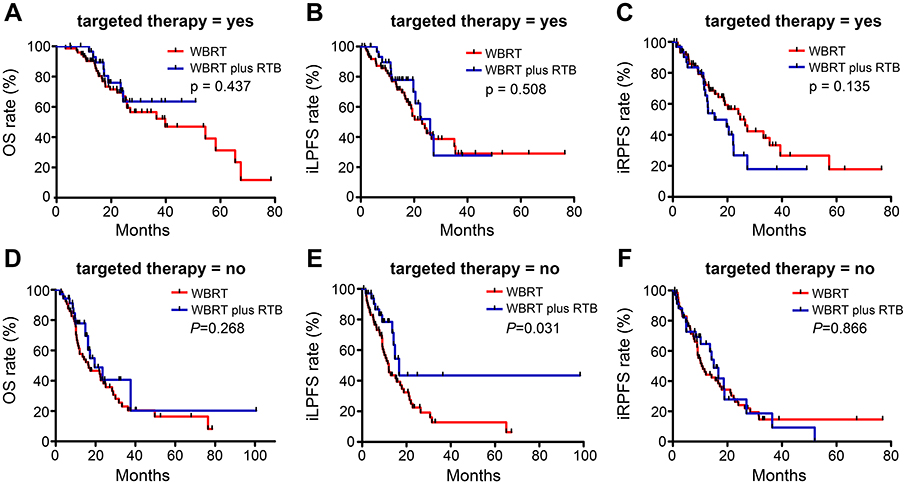 | Figure 3 Comparison of cumulative incidence of OS (A), iLPFS (B), iRPFS (C) between WBRT-alone group and WBRT plus RTB group for patients with EGFR-TKI therapy; comparison of cumulative incidence of OS (D), iLPFS (E), iRPFS (F) between WBRT-alone group and WBRT plus RTB group for patients without EGFR-TKI therapy. Abbreviations: mOS, median overall survival; iLPFS, intracranial local progression-free survival; iRPFS, intracranial regional progression-free survival; WBRT, whole-brain radiotherapy; RTB, radiotherapy boost; EGFR-TKIs, epidermal growth factor receptor-tyrosine kinase inhibitors. |
Subgroup analysis of patients treated without EGFR-TKI therapy
We also performed a subgroup analysis of patients treated without EGFR-TKI therapy. In the other 102 patients without TKI treatment, 65 patients (63.7%) were treated with WBRT alone. Patients with more than 3 brain lesions and EMs were common in the WBRT-alone group (Table 6).
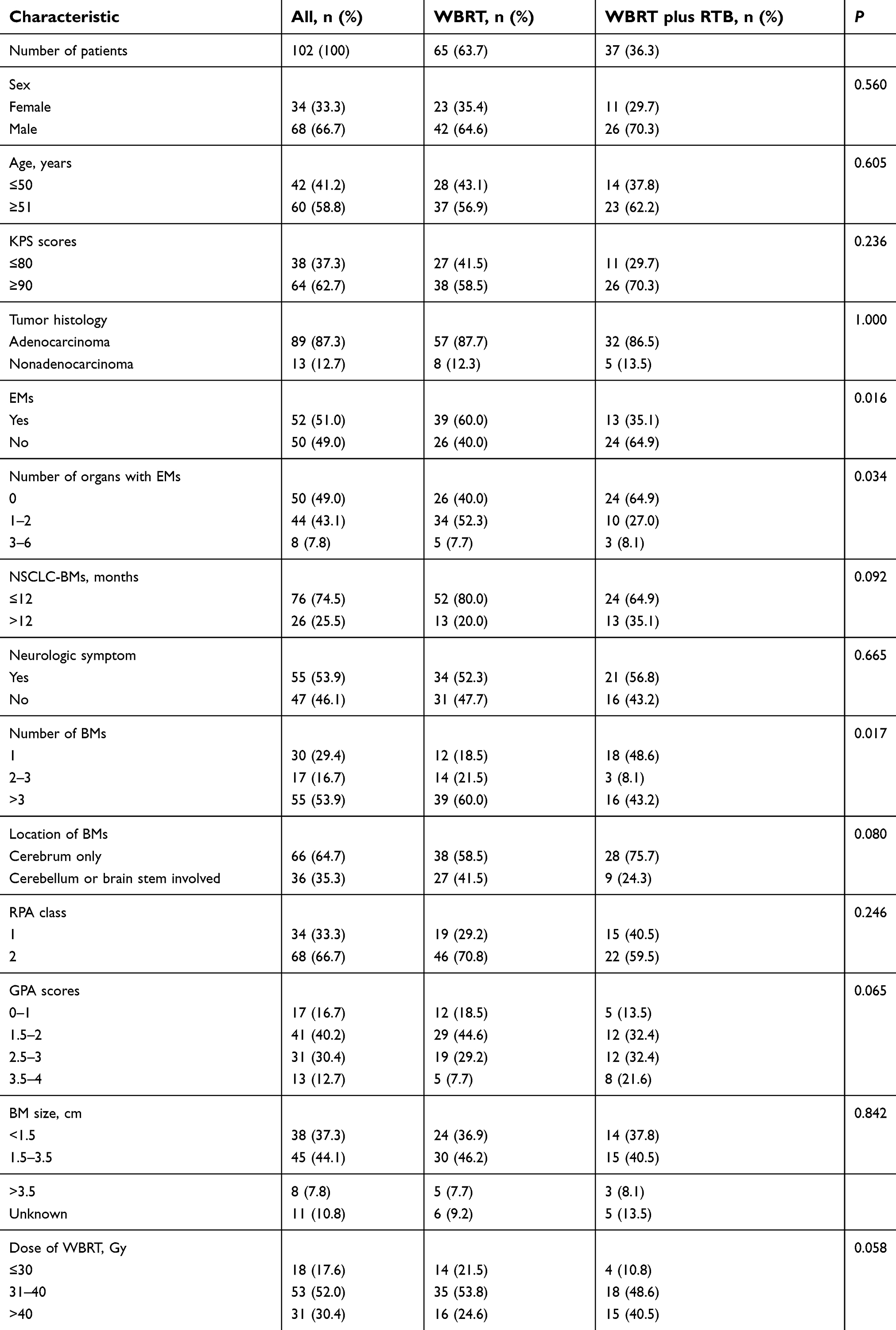 | Table 6 Baseline characteristics of patients without EGFR-TKI therapy |
Among the 102 patients, the median OS, iLPFS, and iRPFS were just 19.5 months, 14.8 months, and 14.2 months, respectively. There was no difference in median OS between the two treatment groups (16.5 months in the WBRT-alone group vs 23.5 months in the WBRT plus RTB group, P=0.182, Figure 3D). WBRT plus RTB was also not beneficial to median iRPFS compared with WBRT alone (16.7 vs 10.6 months, P=0.837; Figure 3F). However, the median iLPFS was significantly longer in the WBRT plus RTB group than in the WBRT-alone group (16.7 vs 12.0 months, P=0.032; Figure 3E).
Discussion
There are many options for the treatment of NSCLC patients with BMs, such as radiotherapy, targeted therapy, surgery, chemotherapy, and immunotherapy, but the most suitable treatment of BMs is controversial.18 As treatments for patients with BMs advance, the survival of patients is prolonged.
In this study, we retrospectively analyzed the clinical data of 206 NSCLC patients with BMs who were treated with brain radiotherapy at our institution. The median OS for all patients was 25.8 months, which was better than that in multiple previous reports. In a study that included 457,481 patients with NSCLC and aimed to investigate the prevalence of BMs, BMs were observed in 47,546 patients (10.4%), and the median OS of patients with BMs was just 6 months.3 However, information about the treatment of BMs was unknown in this study. The reason why our study achieved a good OS may be as follows: 1) most patients (88.8%) had a pathological type of adenocarcinoma and 2) more than half of the patients (51.5%) received targeted therapy. Previous research confirmed that adenocarcinoma histology was associated with better median survival compared with squamous histology (8.8 vs 5.4 months, P=0.01) in patients with BMs.27 In this research, among the patients with anaplastic lymphoma kinase (ALK) fusions and EGFR mutations, 79% (15/19) of patients received ALK inhibitor treatment and 72% (44/61) of patients received EGFR inhibitor treatment; the median survival was longest among patients with ALK fusions (49.2 months), followed by patients with EGFR mutations (20.3 months) and patients with wild-type adenocarcinomas (10.0 months, P=0.01).
We noticed that WBRT plus RTB had a significant clinical benefit on iLPFS compared with WBRT alone (22.3 months vs 17.9 months, P=0.041); however, there were no significant differences in OS and iRPFS between the two groups. Several studies compared the effectiveness between WBRT and WBRT plus a stereotactic boost for BMs. In the RTOG 9508 randomized trial that included patients with one to three newly diagnosed BMs, Andrews et al10 compared 167 patients treated with WBRT plus stereotactic radiosurgery (SRS) and 164 patients treated with WBRT alone. This study included 105 (64%) lung cancer patients in the WBRT plus SRS group and 106 (63%) lung cancer patients in the other group. All patients received a WBRT dose of 37.5 Gy/15f (2.5 Gy/f, 5 f/w), and patients in the WBRT plus the boost group received an additional SRS boost dose of 15–24 Gy depending on the broadest diameter of the BMs. The mean survival time was not significantly different between the two groups (6.5 months for WBRT alone vs 5.7 months for WBRT plus SRS, P=0.1356). However, the SRS boost had good local control rates (P=0.0132) and a significant benefit to survival in patients with a single BM (6.5 months vs 4.9 months, P=0.0390). The result of this study, that WBRT plus the boost received better local control but no difference in OS compared with WBRT alone, was similar to the results of our study. In another matched-pair analysis comparing WBRT with and without a stereotactic boost, the results also showed that WBRT plus a stereotactic boost significantly improved IC but not OS.9 The recent Cochrane database of systematic reviews included two studies and a meta-analysis with a total of 358 participants also found no difference in OS between WBRT plus SRS and WBRT alone (HR =0.82; 95% CI, 0.65 to 1.02), but local control was significantly better in the SRS boost group.28 Another retrospective analysis showed that RTB was associated with an improved survival in patients with performance status (PS) ≤2 and no more than three BMs, and the median OS was 8.9 months in patients receiving RTB versus 4.0 months in patients with no RTB (P=0.0024).29 However, this study included not only lung cancer patients with BMs but also breast cancer and melanoma patients.
The multivariate analysis showed that treatment with EGFR-TKIs was an independent favorable prognostic factor for OS, iLPFS, and iRPFS, and patients treated with TKIs had a significantly better OS and ICR. At present, a large number of studies have focused on targeted therapy for NSCLC patients with BMs. Sung et al17 investigated the efficacy of TKIs with and without radiotherapy, and all patients in the study had histologically confirmed EGFR-mutant adenocarcinoma. The median time interval to intracranial progression (ICP) was 36.8 months in the TKIs plus RT group and 12.2 months in the TKI-alone group. The 2-year cumulative incidence of ICP was significantly lower in the TKIs plus RT group than in the TKI-alone group (36.5% vs 62.2%, P=0.006). However, no significant differences were observed in the 2-year OS rate (P=0.267). An updated meta-analysis including 1,552 NSCLC patients with BMs suggested that radiotherapy plus EGFR-TKIs achieved a superior response rate and disease control rate and prolonged the time to central nervous system progression and OS.30 All of these studies concluded that targeted therapy combined with radiotherapy could achieve good ICR and survival.
In our study, we further performed subgroup analyses of patients treated with or without EGFR-TKI therapy to explore the survival and IC differences between the two treatment groups. These analyses suggested that the median OS, iLPFS, and iRPFS of patients with EGFR-TKI therapy were not significantly different between the WBRT and WBRT plus RTB groups. Among patients without TKI therapy, there were also no significant differences in OS and iRPFS between the two treatment groups, but WBRT plus RTB effectively prolonged the iLPFS (P=0.032). To the best of our knowledge, this is the first report showing that WBRT plus RTB has no survival and IC benefits in patients treated with TKI therapy. In a survey about diversity of BMs screening and management in NSCLC in Europe, Levy et al31 investigated the responses of 462 European physician in 394 institutions to the screening and treatment of BMs in NSCLC patients, and they found that patients with a driver mutation were more likely to receive more aggressive local treatment such as SRS compared with nondriver mutation patients (27% vs 21%; P<0.01) even in patients with more than four brain lesions. However, there was no consensus on the local treatment of BM patients with a driver mutation, and clinical studies were needed to be carried out to determine a more appropriate local treatment for these patients.
The multivariate analysis also showed that RPA class 1 was significantly associated with better OS and iLPFS, and good GPA scores were significantly associated with better OS, iLPFS, and iRPFS. These results indicate that GPA scores and RPA classes could accurately estimate the prognosis of patients with BMs and were similar to previously reported results.19–22 Recently, an updated GPA score using molecular markers (Lung-molGPA) has been used to evaluate the survival of NSCLC patients with BMs. Significant prognostic factors included the original 4 factors used in the GPA index plus 2 new factors: EGFR and ALK alterations in patients with adenocarcinoma. Several studies found that patients with adenocarcinoma lung cancer and Lung-molGPA scores of 3.5 to 4.0 had a median survival of nearly 4 years and that the Lung-molGPA index was useful for estimating OS and appeared to provide the most accurate predictions.32–34 These results were attributed to the effect of targeted therapy. In our study, we also found that patients treated with TKIs had better survival and intracranial local control than patients without TKI treatment. Therefore, in the era of targeted therapy, more accurate prognostic indicators need to further consider the gene status.
Our study had many limitations, such as its retrospective nature with a number of confounding factors, the small sample size, missing data on the EGFR status of some patients treated with TKI therapy, no record of treatment toxicity, the variable dose of radiotherapy, and complex targeted therapy drugs. Additionally, evidence to support the use of SRS alone in patients with BMs continues to increase. A multi-institutional prospective study demonstrated that SRS without WBRT in patients with 5 to 10 BMs was noninferior and safe to that in patients with 2 to 4 BMs.35,36 At present, with the advances in research on treatments of BMs, the proportion of patients treated with WBRT or RTB has become increasingly less. However, SRS is not yet available in some institutions, and the results of research are valuable to these institutions. But we cannot ignore the heterogeneity in our results due to differences in baseline characteristics between the two study groups. Therefore, the results of this study should be interpreted with caution. Further studies are warranted to confirm these findings and to increase the study power.
Conclusion
In conclusion, WBRT plus RTB significantly improved iLPFS compared with WBRT alone, especially in patients without EGFR-TKI treatment. However, there were no significant differences in iRPFS and OS between the two groups. EGFR-TKI therapy was an independent favorable prognostic factor for OS, iLPFS, and iRPFS. NSCLC patients with BMs who have been treated with TKI therapy may not benefit from WBRT plus RTB in terms of survival and intracranial local control. Further prospective studies are needed to confirm these discoveries.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (Nos.81660504, 81560488, 81860536), Yunnan Provincial Training Special Funds for High-level Health Technical Personnel (No.H-201624), Yunnan Health Science Foundation (Nos.2017NS191, 2018NS0065, 2018NS0064).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics. CA Cancer J Clin. 2018;68(1):7–30. doi:10.3322/caac.21442
2. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.21338
3. Waqar SN, Samson PP, Robinson CG, et al. Non-small-cell lung cancer with brain metastasis at presentation. Clin Lung Cancer. 2018;19(4):e373-e379.
4. Mulvenna P, Nankivell M, Barton R, et al. Dexamethasone and supportive care with or without whole brain radiotherapy in treating patients with non-small cell lung cancer with brain metastases unsuitable for resection or stereotactic radiotherapy (QUARTZ): results from a phase 3, non-inferiority, randomised trial. Lancet. 2016;388(10055):2004–2014.
5. Wang W, Song Z, Zhang Y. Efficacy of brain radiotherapy plus EGFR-TKI for EGFR-mutated non-small cell lung cancer patients who develop brain metastasis. Arch med sci. 2018;14(6):1298–1307. doi:10.5114/aoms.2018.78939
6. Sperduto PW, Kased N, Roberge D, et al. Summary report on the graded prognostic assessment: an accurate and facile diagnosis-specific tool to estimate survival for patients with brain metastases. J Clin Oncol. 2012;30(4):419–425. doi:10.1200/JCO.2011.38.0527
7. Khuntia D, Brown P, Li J, Mehta MP. Whole-brain radiotherapy in the management of brain metastasis. J Clin Oncol. 2006;24(8):1295–1304. doi:10.1200/JCO.2005.04.6185
8. Patla A, Walasek T, Jakubowicz J, et al. Methods and results of locoregional treatment of brain metastases in patients with non-small cell lung cancer. Contemp Oncol (Pozn). 2016;20(5):358–364. doi:10.5114/wo.2015.51825
9. Rades D, Janssen S, Bajrovic A, Khoa MT, Veninga T, Schild SE. A matched-pair analysis comparing whole-brain radiotherapy with and without a stereotactic boost for intracerebral control and overall survival in patients with one to three cerebral metastases. Radiat Oncol. 2017;12(1):69.
10. Andrews DW, Scott CB, Sperduto PW, et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: phase III results of the RTOG 9508 randomised trial. Lancet. 2004;363(9422):1665–1672. doi:10.1016/S0140-6736(04)16250-8
11. Zhou L, Liu J, Xue J, et al. Whole brain radiotherapy plus simultaneous in-field boost with image guided intensity-modulated radiotherapy for brain metastases of non-small cell lung cancer. Radiat Oncol. 2014;9:117. doi:10.1186/1748-717X-9-117
12. Dobi A, Fodor E, Maraz A, et al. Boost irradiation integrated to whole brain radiotherapy in the management of brain metastases. Pathol Oncol Res. Epub 2018 Jan 17.
13. Wu YL, Zhou C, Cheng Y, et al. Erlotinib as second-line treatment in patients with advanced non-small-cell lung cancer and asymptomatic brain metastases: a phase II study (CTONG-0803). Ann Oncol. 2013;24(4):993–999. doi:10.1093/annonc/mds529
14. Iuchi T, Shingyoji M, Sakaida T, et al. Phase II trial of gefitinib alone without radiation therapy for Japanese patients with brain metastases from EGFR-mutant lung adenocarcinoma. Lung Cancer. 2013;82(2):282–287. doi:10.1016/j.lungcan.2013.08.016
15. Park SJ, Kim HT, Lee DH, et al. Efficacy of epidermal growth factor receptor tyrosine kinase inhibitors for brain metastasis in non-small cell lung cancer patients harboring either exon 19 or 21 mutation. Lung Cancer. 2012;77(3):556–560. doi:10.1016/j.lungcan.2012.05.092
16. Welsh JW, Komaki R, Amini A, et al. Phase II trial of erlotinib plus concurrent whole-brain radiation therapy for patients with brain metastases from non-small-cell lung cancer. J Clin Oncol. 2013;31(7):895–902. doi:10.1200/JCO.2011.40.1174
17. Sung S, Lee SW, Kwak YK, Kang JH, Hong SH, Kim YS. Intracranial control and survival outcome of tyrosine kinase inhibitor (TKI) alone versus TKI plus radiotherapy for brain metastasis of epidermal growth factor receptor-mutant non-small cell lung cancer. J Neurooncol. 2018;139(1):205–213. doi:10.1007/s11060-018-2861-1
18. Preusser M, Winkler F, Valiente M, et al. Recent advances in the biology and treatment of brain metastases of non-small cell lung cancer: summary of a multidisciplinary roundtable discussion. ESMO Open. 2018;3(1):e000262. doi:10.1136/esmoopen-2017-000262
19. Gaspar L, Scott C, Rotman M, et al. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int J Radiat Oncol Biol Phys. 1997;37(4):745–751.
20. Gaspar LE, Scott C, Murray K, Curran W. Validation of the RTOG recursive partitioning analysis (RPA) classification for brain metastases. Int J Radiat Oncol Biol Phys. 2000;47(4):1001–1006.
21. Sperduto PW, Berkey B, Gaspar LE, Mehta M, Curran W. A new prognostic index and comparison to three other indices for patients with brain metastases: an analysis of 1,960 patients in the RTOG database. Int J Radiat Oncol Biol Phys. 2008;70(2):510–514. doi:10.1016/j.ijrobp.2007.06.074
22. Woody NM, Greer MD, Reddy CA, et al. Validation of the disease-specific GPA for patients with 1 to 3 synchronous brain metastases in newly diagnosed NSCLC. Clin Lung Cancer. 2018;19(1):e141-e147.
23. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
24. Leighl NB, Rekhtman N, Biermann WA, et al. Molecular testing for selection of patients with lung cancer for epidermal growth factor receptor and anaplastic lymphoma kinase tyrosine kinase inhibitors: American Society of Clinical Oncology endorsement of the College of American Pathologists/International Association for the study of lung cancer/association for molecular pathology guideline. J Clin Oncol. 2014;32(32):3673–3679. doi:10.1200/JCO.2014.57.3055
25. Kim E, Feldman R, Wistuba II. Update on EGFR mutational testing and the potential of noninvasive liquid biopsy in non-small-cell lung cancer. Clin Lung Cancer. 2018;19(2):105–114. doi:10.1016/j.cllc.2017.08.001
26. Kalemkerian GP, Narula N, Kennedy EB, et al. Molecular testing guideline for the selection of patients with lung cancer for treatment with targeted tyrosine kinase inhibitors: American Society of Clinical Oncology Endorsement of the College of American Pathologists/International Association for the study of lung cancer/association for molecular pathology clinical practice guideline update. J Clin Oncol. 2018;36(9):911–919. doi:10.1200/JCO.2017.76.7293
27. Miller JA, Kotecha R, Ahluwalia MS, et al. The impact of tumor biology on survival and response to radiation therapy among patients with non-small cell lung cancer brain metastases. Pract Radiat Oncol. 2017;7(4):e263-e273.
28. Patil CG, Pricola K, Sarmiento JM, Garg SK, Bryant A, Black KL. Whole brain radiation therapy (WBRT) alone versus WBRT and radiosurgery for the treatment of brain metastases. Cochrane Database Syst Rev. 2017;9:CD006121.
29. Assouline A, Levy A, Chargari C, Lamproglou I, Mazeron JJ, Krzisch C. Whole brain radiotherapy: prognostic factors and results of a radiation boost delivered through a conventional linear accelerator. Radiother Oncol. 2011;99(2):214–217. doi:10.1016/j.radonc.2011.05.006
30. Jiang T, Min W, Li Y, Yue Z, Wu C, Zhou C. Radiotherapy plus EGFR TKIs in non-small cell lung cancer patients with brain metastases: an update meta-analysis. Cancer Med. 2016;5(6):1055–1065. doi:10.1002/cam4.673
31. Levy A, Faivre-Finn C, Hasan B, et al. Diversity of brain metastases screening and management in non-small cell lung cancer in Europe: results of the European Organisation for Research and Treatment of Cancer Lung Cancer Group survey. Eur J Cancer. 2018;93:37–46. doi:10.1016/j.ejca.2018.01.067
32. Sperduto PW, Yang TJ, Beal K, et al. The effect of gene alterations and tyrosine kinase inhibition on survival and cause of death in patients with adenocarcinoma of the lung and brain metastases. Int J Radiat Oncol Biol Phys. 2016;96(2):406–413. doi:10.1016/j.ijrobp.2016.06.006
33. Sperduto PW, Yang TJ, Beal K, et al. Estimating survival in patients with lung cancer and brain metastases. JAMA Oncol. 2017;3(6):827. doi:10.1001/jamaoncol.2016.3834
34. Li H, Lian J, Han S, et al. Applicability of graded prognostic assessment of lung cancer using molecular markers to lung adenocarcinoma patients with brain metastases. Oncotarget. 2017;8(41):70727–70735. doi:10.18632/oncotarget.19980
35. Yamamoto M, Serizawa T, Shuto T, et al. Stereotactic radiosurgery for patients with multiple brain metastases (JLGK0901): a multi-institutional prospective observational study. Lancet Oncol. 2014;15(4):387–395. doi:10.1016/S1470-2045(14)70061-0
36. Yamamoto M, Serizawa T, Higuchi Y, et al. A Multi-institutional prospective observational study of stereotactic radiosurgery for patients with multiple brain metastases (JLGK0901 study update): irradiation-related complications and long-term maintenance of mini-mental state examination scores. Int J Radiat Oncol Biol Phys. 2017;99(1):31–40. doi:10.1016/j.ijrobp.2017.04.037
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.