")
Back to Journals » International Journal of General Medicine » Volume 16
Survey of Inpatient Consultations with General Internal Medicine Physicians in a Tertiary Hospital: A Retrospective Observational Study
Authors Kawamura R , Harada Y , Yokose M , Hanai S , Suzuki Y , Shimizu T
Received 15 February 2023
Accepted for publication 7 April 2023
Published 14 April 2023 Volume 2023:16 Pages 1295—1302
DOI https://doi.org/10.2147/IJGM.S408768
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Ren Kawamura, Yukinori Harada, Masashi Yokose, Shogo Hanai, Yudai Suzuki, Taro Shimizu
Department of Diagnostic and Generalist Medicine, Dokkyo Medical University Hospital, Mibu, Tochigi, Japan
Correspondence: Taro Shimizu, Department of Diagnostic and Generalist Medicine, Dokkyo Medical University Hospital, 880 Kitakobayashi, Shimotsuga, Mibu, Tochigi, 321-0293, Japan, Tel +8128286-1111, Email [email protected]
Purpose: The general internal medicine (GIM) department can be an effective diagnostic coordinator for undiagnosed outpatients. We investigated the contribution of GIM consultations to the diagnosis of patients admitted to specialty departments in hospitals in Japan that have not yet adopted a hospitalist system.
Patients and Methods: This single-center, retrospective observational study was conducted at a university hospital in Japan. GIM consultations from other departments on inpatients aged ≥ 20 years, from April 2016 to March 2021, were included. Data were extracted from electronic medical records, and consultation purposes were categorized into diagnosis, treatment, and diagnosis and treatment. The primary outcome was new diagnosis during hospitalization for patients with consultation purpose of diagnosis or diagnosis and treatment. The secondary outcomes were the purposes of consultation with the Diagnostic and Generalist Medicine department.
Results: In total, 342 patients were included in the analysis. The purpose of the consultations was diagnosis for 253 patients (74%), treatment for 60 (17.5%), and diagnosis and treatment for 29 patients (8.5%). In 282 consultations for diagnosis and diagnosis and treatment, 179 new diagnoses were established for 162 patients (57.5%, 95% confidence interval [CI], 51.5– 63.3).
Conclusion: The GIM department can function as a diagnostic consultant for inpatients with diagnostic problems admitted to other specialty departments in hospitals where hospitalist or other similar systems are not adopted.
Keywords: diagnosis, diagnostic excellence, consultation, consultative medicine, hospital admission
Introduction
Diagnostic accuracy is essential for hospitalized patients. A systematic review showed that harmful diagnostic adverse events occur in a minimum of 0.7% of hospitalized patients. In particular, a vast array of diseases, including many common ones, are missed.1 Diagnostic adverse events can occur not only in patients who are hospitalized with difficult-to-diagnose problems but also in patients with new problems during hospitalization. In hospitals that implement a hospitalist system, diagnostic workups can be coordinated well by hospitalists with effective specialist consultations. Meanwhile, in hospitals where each specialist department works independently, the diagnostic workup may be fragmented and disorganized for patients who have multisystem problems or problems outside the scope of the specialists in a said hospital. Indeed, when complex cases are examined by specialists, they tend to assign higher probabilities to diagnoses within their own domain than to those outside.2 This tendency may lead to an overestimation of symptoms and signs as precursors to serious diseases related to their specialty.3 Moreover, if specialists determine that patients’ problems are not within the scope of their specialty, they will refer them to other specialty departments that may be expected to be related. Consequently, specialists are more likely to refer patients to other specialties than generalists, including hospitalists, resulting in long hospital stays and increased resource use.4,5 Therefore, in hospitals where each specialist department independently cares for inpatients, the involvement of generalists as coordinators for patients with difficult-to-diagnose or complex multimorbidity is warranted.6,7
While hospitalists in the United States and acute care physicians in the United Kingdom are responsible for the acute care of hospitalized patients in many hospitals,8 only a few hospitals in Japan have implemented a system in which generalists widely cover hospitalized patients. Instead, in many hospitals in Japan, physicians in the general internal medicine (GIM) department play a role in coordinating the diagnostic processes. A previous study showed that the GIM department can serve as an effective diagnostic coordinator for undiagnosed outpatients in specialty departments of a large hospital.9 However, its effectiveness for inpatients is still unclear.10 Therefore, we conducted this study to clarify the contribution of the GIM department in the diagnosis of patients hospitalized in specialty departments.
Materials and Methods
Study Design
This was a single-center, retrospective, observational study that used data from Dokkyo Medical University Hospital (DMUH) in Japan. DMUH is a university hospital with 29 departments. Notably, there are no infectious disease departments in the hospital. Therefore, patients with difficult cases of infectious diseases tend to be referred to the Department of Diagnostic and Generalist Medicine (DGM).
Ethical Consideration
This study complied with the Declaration of Helsinki and was approved by the Research Ethics Committee of the Dokkyo Medical University Hospital (R-53-4J). All data were anonymous and aggregated; therefore, the requirement to obtain written informed consent from patients was waived by the Research Ethics Committee under the condition that we used an opt-out method. We informed patients by showing detailed information about the study in the GIM outpatient waiting area and the GIM inpatient ward.
Patient Population
We included DGM consultations from other departments within the DMUH for hospitalized patients aged 20 years and older between April 1, 2016, and March 31, 2021. Since the DGM was founded in April 2016, the 5 years between its foundation and the start of the study were set as the study period. Also, Japanese law assumes patients 20 years and older to be adults; therefore, patients 20 years and older were included to make it an adult-oriented study. DGM covers the role of GIM in DMUH. We excluded cases in which consultations were made during hospitalization, but the patient was examined in the outpatient setting after discharge; cases in which the DGM department was involved in the patient’s care in the outpatient clinic prior to admission; and cases in which consultations were established according to the consultation letter addressed to the DGM department for reasons other than admission.
Data Collection
We retrospectively reviewed patients’ medical records and extracted data regarding age, sex, admission date, consulting department, consultation date, consultation letter, and response letter. All cases were independently reviewed by two of the five reviewers (RK, YH, MY, SH, and YS).
The medical records were reviewed as follows: First, based on the consultation letter, the purpose of the consultation was categorized into diagnosis, treatment, and diagnosis and treatment. For consultations classified as being for the purpose of diagnosis, the main problems requiring a diagnosis were extracted from the consultation letter, and the reviewers judged if any new diagnoses related to the main problems were established during hospitalization. For cases with new diagnoses, the names of the new diagnoses were extracted, and the degree of validity of the new diagnoses (confirmed or suspected) and the presence or absence of treatment for the new diagnoses were evaluated. We defined confirmed diagnosis as a correct diagnosis with sufficient evidence or judged equal to well-founded between two reviewers and suspected diagnosis as a clinically correct diagnosis but with insufficient evidence. For consultations whose purpose was classified as treatment, the disease prompting the consultation was extracted from the consultation letter, and the presence or absence of new treatment during hospitalization for the disease was evaluated. For consultations whose purpose was classified as diagnosis and treatment, the diagnosis and treatment were evaluated in the same manner as described above. In case of disagreement between the two reviewers, conflicts were resolved through discussion or by a third reviewer. New diagnoses were categorized using ICD-10 codes by RK.
Outcomes
The primary outcome was the percentage of established new diagnosis during hospitalization for patients with consultation purposes of diagnosis or diagnosis and treatment. The secondary outcomes were the purposes of consultation with the DGM department.
Statistical Analysis
Continuous data were presented as medians with interquartile ranges. Categorical data were presented as counts and proportions (%). For the primary outcome, we calculated the incidence of newly established diagnoses in the cases for which consultation purposes were classified as diagnosis or diagnosis and treatment with 95% confidence intervals (CI). Cohen’s Kappa was calculated to examine agreement for the presence of new diagnoses between the two reviewers at the initial review. All statistical analyses were conducted using STATA statistical software, version 17.0 BE (StataCorp).
Results
A total of 357 consultations were conducted during the study period. After excluding 15 cases (13 cases in which consultation was made during hospitalization but the patients were examined in the outpatient setting after discharge, one case in which the DGM department was involved in the patient’s care in the outpatient clinic prior to admission, and one case in which the consultation was established according to the consultation letter addressed to the DGM department for reasons other than admission), data of 342 patients were analyzed for this study (Figure 1). The median age of patients was 69 (IQR, 53–77) years, and 202 (59.1%) patients were male. The purpose of the consultations was diagnosis for 253 patients (74.0%), treatment for 60 patients (17.5%), and diagnosis and treatment for 29 patients (8.5%). The top three consulting departments were cardiovascular medicine (18.4%), followed by cardiovascular surgery (12.9%), gastroenterology (7.9%), and orthopedics (7.9%) (Supplementary Figure 1).
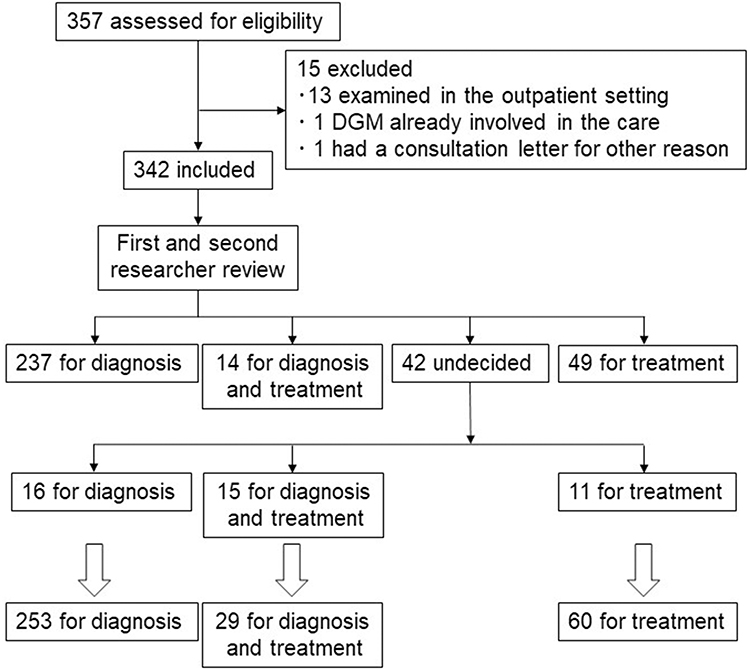 |
Figure 1 Flowchart of this study. |
In 282 consultations for diagnosis and diagnosis and treatment, we identified a total of 303 main problems. The top three problems were fever (48.2%), abnormal laboratory results (6.9%), and unknown causes of bacteremia (3.0%) (Table 1 and Supplementary Table 1). Seventeen consultations were conducted for the exclusion of other diagnoses, although the specialty department had already established the diagnosis. In total, 179 new diagnoses were established for 162/282 cases (57.5%; 95% CI, 51.5–63.3). Two diagnoses were established for 11 patients, and three patients had three new diagnoses. Of the 162 patients who received a new diagnosis, the degree of validity was assessed as confirmed for 94 patients (58.0%) and suspected for 68 patients (42.0%). The inter-researcher agreement on the presence of new diagnoses at the initial review was 75.9% (214/282; Cohen’s kappa=0.47). The top three ICD-10 categories of new diagnoses were the musculoskeletal system and connective tissue (16.8%), certain infectious and parasitic diseases (13.4%), and digestive system (10.1%) (Figure 2). Of the 146 consultations for diagnosis of the cause of fever, a total of 106 new diagnoses in 99 patients (67.8%) were established: infectious diseases in 64 (64.7%), non-infectious diseases in 33 (33.3%), and mixed infectious and non-infectious diseases in 2 patients (2.0%) (Table 2). A total of 95 diseases in 89 consultations were made for treatment: 86 for infectious diseases (90.5%) and nine for non-infectious diseases (9.5%).
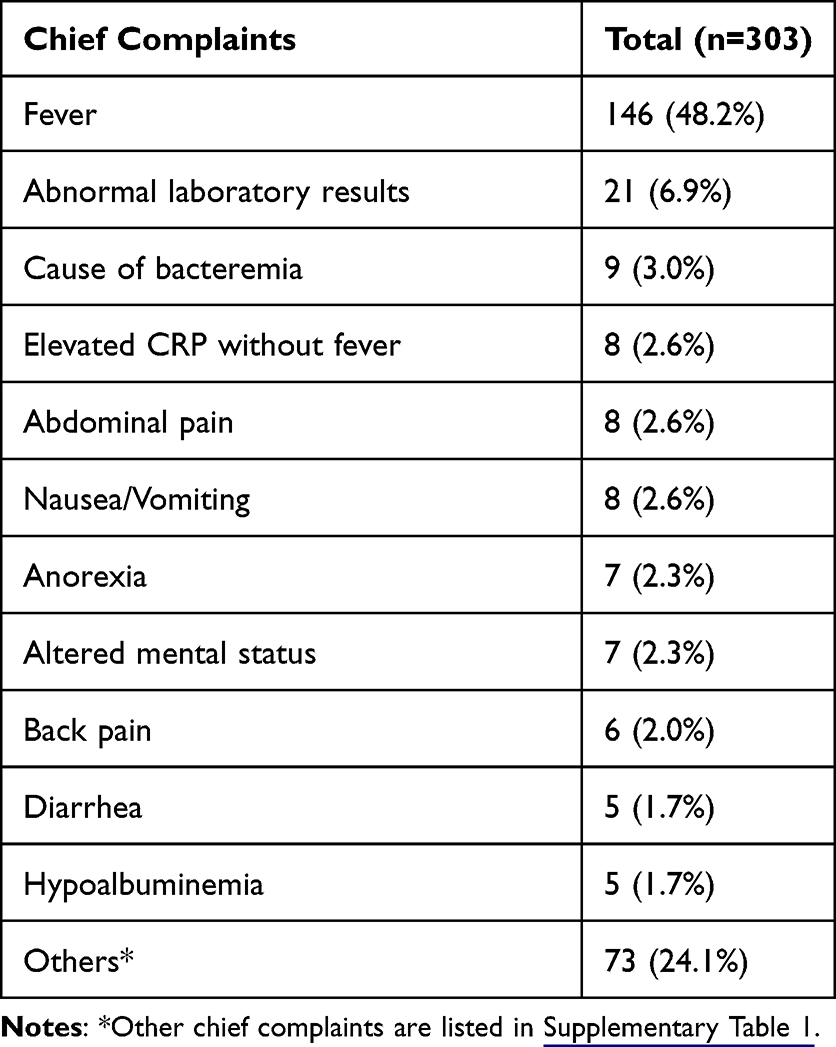 |
Table 1 Main Problems That Prompted Consultation for Diagnosis |
 |
Table 2 New Diagnoses After Consultation for Diagnosis for the Cause of Fever |
 |
Figure 2 International classification of diseases-10 categories of new diagnoses. |
Discussion
We found that 82.5% of in-hospital consultations from specialty departments to the DGM department had diagnostic purposes in the university hospital, where the DGM department functioned as a specialty department, not as hospitalist. New diagnoses were established for approximately 60% of the consultations. In cases where new diagnoses were established, musculoskeletal system and connective tissue diseases, infectious diseases, including parasitic diseases, and gastrointestinal diseases were the most common diagnoses.
This study showed that diagnostic consultation was the main purpose of inpatient GIM consultations from other specialty departments. The results were largely different from those of previous studies in that most consultations of hospitalized patients with specialty departments were requests for evaluation, testing, and treatment related to their specialty area.11–16 This difference indicates that GIM is expected to have specialty in diagnosis.7,17 Indeed, although a small portion, some consultations were for the purpose of checking for missed diagnoses in already diagnosed patients. Patients with atypical symptoms, clinical courses, and symptoms involving multiple organs are likely to be difficult to diagnose.18 To manage such patients, physicians must allow for diagnostic uncertainty and seek the best way to generate and rank hypotheses for differential diagnosis based on detailed history taking and physical examination.3,19,20 In addition, smooth communication with specialty departments is required.21 Because generalists are trained in the skills necessary for diagnosis, they are expected to be active in the diagnostic field. In addition, the wide range of main problems in diagnostic consultations and new diagnoses in this study indicate that the GIM can deal with widely heterogeneous diagnostic problems.22,23 Considering these results, it can be assumed that if these diagnostic problems had been tackled by specialists, unnecessary testing would have been repeatedly performed, since specialists tend to gravitate to toward their own specialties.2,3 These results suggest that the involvement of GIMs as diagnostic consultants for hospitalized patients may contribute to diagnostic excellence24 and streamline the diagnostic process. Furthermore, since GIMs are often in charge of educating young in-house physicians in Japan, by being involved in consultations, they may be able to train the in-house physicians to achieve high diagnostic accuracy at an early stage in their career and help prevent excessive consultations when they move on to specialty departments in their later career.25
The efficacy of diagnostic consultations for hospitalized patients from other departments to the GIM department, ie, the new diagnosis rate established during admission after the consultation, was 57.5% in this study. Several second opinion clinics have emerged outside Japan as specialized departments dedicated to clinical-based diagnosis. Of those, the Mayo clinic’s second opinion clinic reported that 21% of patients referred for diagnostic purposes had a change in diagnosis, and 66% had a clearer diagnosis, although the study was not limited to hospitalized patients.26 In addition, although again not limited to inpatients, the Stanford Consultative Medicine diagnostic second opinion service reported that 53% of patients referred for diagnostic purposes had a new single or multi-factorial diagnosis.27 Compared to these studies, the rate of new diagnoses in this study is comparable, indicating that consultation for DGM for diagnostic purposes is effective. Compared to our previous data on the rate of new diagnoses in outpatients’ consultations with the GIM department by other specialty departments (70.7%) using the same methods for evaluation, the rate of new diagnoses in this study was slightly low.9 This may be partly because the study did not include cases in which the diagnosis was made after hospital discharge.
In this study, fever, abnormal blood test results (including high CRP levels), and scrutiny of the cause of bacteremia were the top three reasons for diagnostic consultations. This result may have been influenced by the fact that our hospital does not have a department for infectious diseases. In Japan, in hospitals that do not have either a GIM or infectious disease department, one department tends to cover the area of the other department, especially for patients with unexplained fever, elevated inflammatory marker levels, or infectious diseases.28–30 In the previous studies conducted at hospitals in Japan that had infectious disease departments but not GIM departments (including inpatients and outpatients), infectious disease accounted for over 90% of the consultations from other departments to infectious disease departments for diagnosis of unexplained fever or elevated inflammatory marker levels.28,29 On the other hand, in this study conducted in a hospital that had a GIM department but not an infectious disease department, infectious causes accounted for 65% of the inpatient consultations from other departments for fever. Although this difference may be because this study exclusively surveyed inpatient consultation, it also suggests that more unclear cases are referred to the GIM department than to the infectious disease department, even in hospitals where either department covers both areas, and consultation with GIM may have occurred at an earlier stage of diagnostic evaluation.7 As the high proportion of neoplasms and connective tissue/autoinflammatory diseases in the consultations for fever was consistent with the results of previous studies of febrile patients admitted to the GIM department,31 GIM physicians should consider these diagnostic categories in cases consulted for unexplained fever even during hospitalization.
This study had several limitations. First, since this was a single-center, retrospective, observational study, the generalizability of the results may be low. In particular, our hospital does not have a department of infectious diseases, as is common in Japan,28,29,32,33 which has resulted in many consultations for diagnostic purposes related to fever and elevated inflammatory response as well as for the treatment of infectious diseases. Second, in this study, cases that led to a diagnosis after discharge from the hospital were counted as having no new diagnosis. Therefore, the actual rate of new diagnoses may have been higher. On the other hand, since suspected cases were also counted as a new diagnosis, it is possible that some patients may have received another new diagnosis during the clinical course.
Conclusion
GIM departments can serve as diagnostic consultants for inpatients with diagnostic problems admitted to other specialties. These tendencies may be prominent in hospitals where hospitalist systems are not implemented. Regardless of the differences in the medical context in different countries and regions, it is reasonable to expect GIM physicians, who treat patients across all disciplines, to be able to contribute to diagnostic quality leveraging their diagnostic expertise as a “specialty”.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
This study complied with the Declaration of Helsinki and was approved by the Research Ethics Committee of the Dokkyo Medical University Hospital (R-53-4J).
Patient Consent
All data were anonymous and aggregated; therefore, the requirement to obtain written informed consent from patients was waived by the Research Ethics Committee under the condition that we used an opt-out method. We informed patients by showing detailed information about the study in the GIM outpatient waiting area and the GIM inpatient ward.
Acknowledgments
We would like to thank Editage for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gunderson CG, Bilan VP, Holleck JL, et al. Prevalence of harmful diagnostic errors in hospitalised adults: a systematic review and meta-analysis. BMJ Qual Saf. 2020;29(12):1008–1018. doi:10.1136/bmjqs-2019-010822
2. Hashem A, Chi MTH, Friedman CP. Medical errors as a result of specialization. J Biomed Inform. 2003;36(1–2):61–69. doi:10.1016/S1532-0464(03)00057-1
3. Scott IA, Campbell DA. The gaps in specialists’ diagnoses. Med J Aust. 2018;208(5):196–197. doi:10.5694/mja17.00905
4. Parekh V, Saint S, Furney S, Kaufman S, McMahon L. What effect does inpatient physician specialty and experience have on clinical outcomes and resource utilization on a general medical service? J Gen Intern Med. 2004;19(5):395–401. doi:10.1111/j.1525-1497.2004.30298.x
5. Bernard AM, Shapiro LR, McMahon LF Jr. The influence of attending physician subspecialization on hospital length of stay. Med Care. 1990;28(2):170–174. doi:10.1097/00005650-199002000-00007
6. Koizumi S. Current status and prospects of hospital general practitioners. Byoin. 2011;70:94–100.
7. Heath I, Sweeney K. Medical generalists: connecting the map and the territory. BMJ. 2005;331(7530):1462–1464. doi:10.1136/bmj.331.7530.1462
8. Smith GR, Stein JM, Jones MC. Acute medicine in the United Kingdom: first-hand perspectives on a parallel evolution of inpatient medical care. J Hosp Med. 2012;7(3):254–257. doi:10.1002/jhm.1006
9. Yokose M, Harada Y, Hanai S, Tomiyama S, Shimizu T. Outcomes of general internal medicine consultations for diagnosis from specialists in a tertiary hospital: a retrospective observational study. Int J Gen Med. 2022;15:7209–7217. doi:10.2147/IJGM.S378146
10. Wang ES, Moreland C, Shoffeitt M, Leykum LK. Medicine consult/comanagement consortium. Who consults us and Why? An evaluation of medicine consult/comanagement services at academic medical centers. J Hosp Med. 2018;13(12):840–843. doi:10.12788/jhm.2996
11. Sullivan JF, Forde JC, Creagh TA, et al. A review of inpatient urology consultations in an Irish tertiary referral centre. Surgeon. 2013;11(6):300–303. doi:10.1016/j.surge.2013.06.003
12. England RW, Ho TC, Napoli DC, Quinn JM. Inpatient consultation of allergy/immunology in a tertiary care setting. Ann Allergy Asthma Immunol. 2003;90(4):393–397. doi:10.1016/S1081-1206(10)61822-4
13. Raymundo DU, Dalio MB, Ribeiro MS, Joviliano EE. Inpatient consultations with the vascular and endovascular surgery team at an academic tertiary hospital. J Vasc Bras. 2022;21:e20210159. doi:10.1590/1677-5449.20210159
14. Tajunisah I. Ophthalmology inpatient consultation: does it make a difference to inpatient management? Med J Malaysia. 2009;64:130–133.
15. Mancha D, Roda Â, Queirós C, Garrido P, Filipe P. Reasons for inpatient dermatological consultation requested by other specialities: a five-year data analysis of 1052 patients from a Portuguese tertiary teaching hospital. Eur J Dermatol. 2022;32:214–219.
16. Cai Q, Bruno CJ, Hagedorn CH, Desbiens NA. Temporal trends over ten years in formal inpatient gastroenterology consultations at an inner city hospital. J Clin Gastroenterol. 2003;36(1):34–38. doi:10.1097/00004836-200301000-00011
17. Lai AT, Keely E, McCutcheon T, Liddy C, Afkham A, Frost DW. A retrospective analysis of the use of electronic consultation in general internal medicine. Intern Med J. 2022. doi:10.1111/imj.15940
18. Geng LN, Verghese A, Tilburt JC, Malina D. Consultative medicine — an emerging specialty for patients with perplexing conditions. Malina D, ed. N Engl J Med. 2021;385(26):2478–2484. doi:10.1056/NEJMms2111017
19. Amano M, Harada Y, Shimizu T. Effectual diagnostic approach: a new strategy to achieve diagnostic excellence in high diagnostic uncertainty. Int J Gen Med. 2022;15:8327–8332. doi:10.2147/IJGM.S389691
20. Dahm MR, Crock C. Understanding and communicating uncertainty in achieving diagnostic excellence. JAMA. 2022;327(12):1127. doi:10.1001/jama.2022.2141
21. Adams TN, Bonsall J, Hunt D, et al. Hospitalist perspective of interactions with medicine subspecialty consult services. J Hosp Med. 2017. doi:10.12788/jhm.2882
22. Jordan MR, Conley J, Ghali WA. Consultation patterns and clinical correlates of consultation in a tertiary care setting. BMC Res Notes. 2008;1:96. doi:10.1186/1756-0500-1-96
23. Verma AA, Guo Y, Kwan JL, et al. Prevalence and costs of discharge diagnoses in inpatient general internal medicine: a multi-center cross-sectional study. J Gen Intern Med. 2018;33:1899–1904.
24. Yang D, Fineberg HV, Cosby K. Diagnostic excellence. JAMA. 2021;326:1905. doi:10.1001/jama.2021.19493
25. Shimizu T, Tsugawa Y, Tanoue Y, et al. The hospital educational environment and performance of residents in the general medicine in-training examination: a multicenter study in Japan. Int J Gen Med. 2013;6:637–640. doi:10.2147/IJGM.S45336
26. Van Such M, Lohr R, Beckman T, Naessens JM. Extent of diagnostic agreement among medical referrals. J Eval Clin Pract. 2017;23:870–874. doi:10.1111/jep.12747
27. Chao S, Lotfi J, Lin B, et al. Diagnostic journeys: characterization of patients and diagnostic outcomes from an academic second opinion clinic. Diagnosis. 2022;9:340–347. doi:10.1515/dx-2022-0029
28. Hadano Y, Matsumoto T. Infectious disease consultations in a Japanese tertiary care teaching hospital: a retrospective review of 508 cases. BMC Health Serv Res. 2018;18(1):983. doi:10.1186/s12913-018-3802-6
29. Itoh N, Hadano Y, Yamamoto Y, Terada N, Kurai H. Infectious disease specialist consultations in a Japanese cancer center: a retrospective review of 776 cases. BMC Health Serv Res. 2020;20(1):500. doi:10.1186/s12913-020-05380-6
30. Hadano Y, Kosaka S, Tomoda Y, Awaya Y, Kato R. Infectious diseases consultations from general internal medicine physicians in Japan: a descriptive single-center study. Medicine. 2022;101(47):e31896. doi:10.1097/MD.0000000000031896
31. Uchida S, Ishikawa S, Kumada M, Kuroki S, Kajii E. A retrospective study of 221 hospitalized patients with fever in the department of general practice at Jichi medical university hospital. Off J Jpn Prim Care Assoc. 2012;35:279–285.
32. Iwata K. Quantitative and qualitative problems of infectious diseases fellowship in Japan. Int J Infect Dis. 2013;17(12):e1098–e1099. doi:10.1016/j.ijid.2013.07.009
33. Kishida N, Nishiura H. Accelerating reductions in antimicrobial resistance: evaluating the effectiveness of an intervention program implemented by an infectious disease consultant. Int J Infect Dis. 2020;93:175–181. doi:10.1016/j.ijid.2020.01.051
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.