")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Survey of Health Literacy Among Japanese Outpatients with Mental Illness
Authors Sato Y, Sugawara N , Kawamata Y , Shimoda K , Yasui-Furukori N
Received 23 February 2023
Accepted for publication 26 May 2023
Published 2 June 2023 Volume 2023:19 Pages 1369—1378
DOI https://doi.org/10.2147/NDT.S409882
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Taro Kishi
Yoshiteru Sato,1 Norio Sugawara,1 Yasushi Kawamata,1 Kazutaka Shimoda,1 Norio Yasui-Furukori1,2
1Department of Psychiatry, Dokkyo Medical University School of Medicine, Mibu, Japan; 2Department of Neuropsychiatry, Hirosaki Medical University, Graduate School of Medicine, Hirosaki, Japan
Correspondence: Norio Yasui-Furukori, Department of Psychiatry, Dokkyo Medical University School of Medicine, 880 Kitakobayashi, Mibu, Tochigi, 321-0293, Japan, Tel +81-28-287-2153, Fax +81-28-286-5187, Email [email protected]
Purpose: Low health literacy has been associated with adverse outcomes in health maintenance and the course of chronic physical illness. In particular, anxiety disorders can also affect one’s physical health, causing issues including cardiovascular, respiratory, gastrointestinal and immune system disorders. However, there are no reports on physical health literacy among Japanese patients with mental illness.
Patients and Methods: A patient background questionnaire, the Japanese version of the Ten-Item Personality Inventory, and the Japanese version of the Health Literacy Scale (HLS-EU-Q47; European Health Literacy Survey Questionnaire) were distributed face to face to 1000 psychiatric outpatients. A total of 785 valid responses including 211 patients with schizophrenia, 261 patients with mood disorders, and 234 patients with anxiety disorders were obtained by mail.
Results: Health literacy was “limited” in 52% of patients with schizophrenia, 51% of those with mood disorders, and 38% of those with anxiety disorders. Among patients with mood disorders, there were no differences between those with major depressive disorder and those with bipolar disorder. Anxiety disorders were associated with higher health literacy than schizophrenia and mood disorders (odds ratio (OR) 1.85, 95% confidence interval (95% CI) 1.07, 3.34), and in terms of personality, neuroticism (OR 0.85, 95% CI 0.75, 0.97) and openness (OR 0.85, 95% CI 0.74, 0.98) were associated with limited health literacy, while agreeableness (OR 1.36, 95% CI 1.18, 1.57) and extraversion OR 1.34, 95% CI 1.17, 1.52) were associated with higher health literacy.
Conclusion: The results of this study indicate limited health literacy in patients with mental illness, in particular, limited health literacy in outpatients with schizophrenia and mood disorders. In addition, gender and some personality traits were associated with physical health literacy. Based on these results, physical health education should be individualized.
Keywords: health literacy, mental illness, anxiety disorders, personality traits
Introduction
It is known that people experiencing severe mental illness have a life expectancy that is 10 to 15 years shorter than that of the general population.1 This is due to the high prevalence of abnormalities in glycolipid metabolism, so-called metabolic syndrome,2,3 among patients with psychiatric disorders. Difficulties in self-care in these patients are considered to promote this condition.4 In particular, anxiety disorders can also affect physical health, leading to issues including cardiovascular,5 respiratory,6 gastrointestinal7 and immune system disorders.8 Chronic stress and anxiety can contribute to high blood pressure, atherosclerosis, and other health problems affecting the heart and blood vessels.5 People with anxiety may experience shortness of breath or hyperventilation, which can worsen respiratory conditions, such as asthma or chronic obstructive pulmonary disease (COPD).6 Anxiety can cause or exacerbate digestive issues by affecting the way the digestive system functions.7 Chronic stress and anxiety can weaken the immune system, making individuals more susceptible to infections and illnesses, including cancer.8
Health literacy is the degree of an individual’s ability to research, obtain, understand, and effectively use basic health information and services needed to make appropriate health decisions.9 Health literacy is influenced by the ability to read and write medical information as well as by the ability to take action.10 In recent years, health literacy has become a significant factor influencing health decision making in an environment inundated with a large amount of information due to the introduction of information and communication technology (ICT), and the association of health literacy with health behaviors has been reported. Increased physical health literacy may promote engagement in self-management behaviors and have long-term effects on health status.11 Factors that enhance these health behaviors are related to self-efficacy, coping with stress, and effort, which are deeply influenced by personality.12
Two studies have examined the relationship between personality and physical health literacy: Iwasa & Yoshida13 reported that some personality traits (eg, extraversion, openness, and conscientiousness) may influence physical health literacy among healthy older adults living in Japan. In addition, a study by Mai et al14 found that in two-parent families, education, extraversion, agreeableness, conscientiousness, neuroticism, and openness were significantly associated with physical health literacy in Chinese subjects. In contrast, monthly income, agreeableness, and openness were factors influencing health literacy in single-parent families. However, to date, no studies have examined the relationship between personality and health literacy in people living with mental illness.
There are reports on physical health literacy in patients with physical illness11,15 and mental health literacy in the general population.16 However, there are very few reports on health literacy among patients with mental illnesses worldwide, and only one report17 showed that schizophrenia patients had better health literacy than healthy individuals. Therefore, we conducted a survey to quantitatively clarify physical health literacy among Japanese patients with major mental illnesses, such as schizophrenia, mood disorders, and anxiety disorders. To the best of our knowledge, no study has examined the relationship between personality and health literacy in mental illness subjects. We also identified factors such as personality traits that are associated with physical health literacy.
Method
Subjects
This study was a multicenter cross-sectional study. Data were collected at 5 sites: three were general hospitals, including a university hospital; two were psychiatric hospitals; and one was a mental health clinic. Four sites were in Aomori Prefecture and one was in Akita Prefecture; these are in the rural north-eastern region. The study was approved by the Ethics Committee of Hirosaki University Hospital and the affiliated hospitals where it was conducted. Outpatients at each hospital were given a written and oral explanation of the purpose and content of the study. A total of 1000 patients attending outpatient clinics for psychiatric disorders who were at least 20 years old at the time consent was obtained were included in the study.
Patients who agreed to participate were given a patient background questionnaire, the Japanese version18 of the Ten Item Personality Inventory19 (TIPI-J), and a health literacy scale (HLS-EU-Q47; European Health Literacy Survey Questionnaire).20
Personality Inventory
The TIPI-J, which consisted of ten items and which was developed by Gosling et al19 measures five important personality traits including openness, conscientiousness, extraversion, agreeableness, and emotional stability. Each sub-item in this seven-point Likert scale was rated from 1 (Strongly disagree) to 7 (Strongly agree) and consisted of two items.
Health Literacy Inventory
The Japanese version of the HLS-EU-Q4720 was distributed according to the method of Nakayama et al.21 The HLS-EU-Q47 consists of 47 items measuring health literacy. The difficulty of each item is rated on a 4-point Likert scale (1 = very difficult, 2 = difficult, 3 = easy, 4 = very easy), with the lowest mean score being 1 and the highest score being 4. Thus, the mean score varies from 1 to 4, with a range of 4–1=3. The HLS-EU-Q47 is based on a conceptual model of health literacy and measures four abilities for handling health-related information (access/obtain, understand, evaluate/judge/assess, and apply/use) in three domains listed below, including health care. The Health Literacy Index was constructed as the General Health Literacy Index (GEN-HL) consisting of all items. This system provides an overall index and three domains: the Health Care Health Literacy Index (HC-HL), the Disease Prevention Health Literacy Index (DP-HL), and the Health Promotion Health Literacy Index (HP-HL). The health literacy index is standardized as a unified index ranging from 0 to 50 with the following formula.

Here, Index is the specific index calculated, and the mean is the average of all items answered by each individual; 1 is the minimum value of the mean, 3 is the range of the mean, and 50 is the maximum value chosen for the new index. This is the maximum value of the new indicator. Thus, the following indicator values were obtained, where 0 represents the lowest health literacy and 50 represents the highest health literacy. Less than 33 points was classified as “limited” based on previous literature.21
Statistical Analyses
This study dealt only with data on schizophrenia, mood disorders, and anxiety disorders for which sufficient sample sizes were available. ANOVA, the χ-square test, and logistic regression analysis were used for statistical analysis, with P< 0.05 indicating statistical significance. In logistic regression analyses, the dependent variable was literacy status (Sufficient or above=1, limited=0), with personality, age, sex, marital status, alcohol and smoking status assigned as independent variables. Dummy variables were used for sex (male = 1, female = 0), alcohol (yes = 1, no = 0) and smoking (yes = 1, no = 0) respectively. Dummy variables were used for each marital status and each diagnosis name without categorical data. For example, a combination of dummy variables was assigned to married people (1, 0, 0, 0) and to unmarried people (0, 1, 0, 0). A combination of dummy variables was assigned to patients with schizophrenia (1, 0, 0) and mood disorders (0, 1, 0). Real numbers and TIPI scores were used for age, education and personality, respectively. This statistical method does not determine the relationship between independent variables. IBM SPSS Statistics Ver 28 was used for data analysis.
Results
Table 1 shows the characteristics of the participants. After face-to-face distribution of the questionnaires, a total of 785 valid responses were received by mail. Five-hundred seventy responses were received from general hospitals, 100 from psychiatric hospitals and 115 from mental clinics. The median age was 46.3 years for 211 patients with schizophrenia, 54.0 years for patients with 261 mood disorders, 48.1 years for 234 patients with anxiety disorders, 37.6 years for 79 patients with other disorders, including F5 psychosomatic disorders (n=10), F6 personality disorders (n=25), F7 intellectual disorder (n=11), F8 autism spectrum disorder (ASD) (n=24), and F9 attention-deficit/hyperactivity disorder (ADHD) (n=5). The proportion of women was 59% for patients with schizophrenia, 66% for patients with mood disorders, and 72% for patients with anxiety disorders.
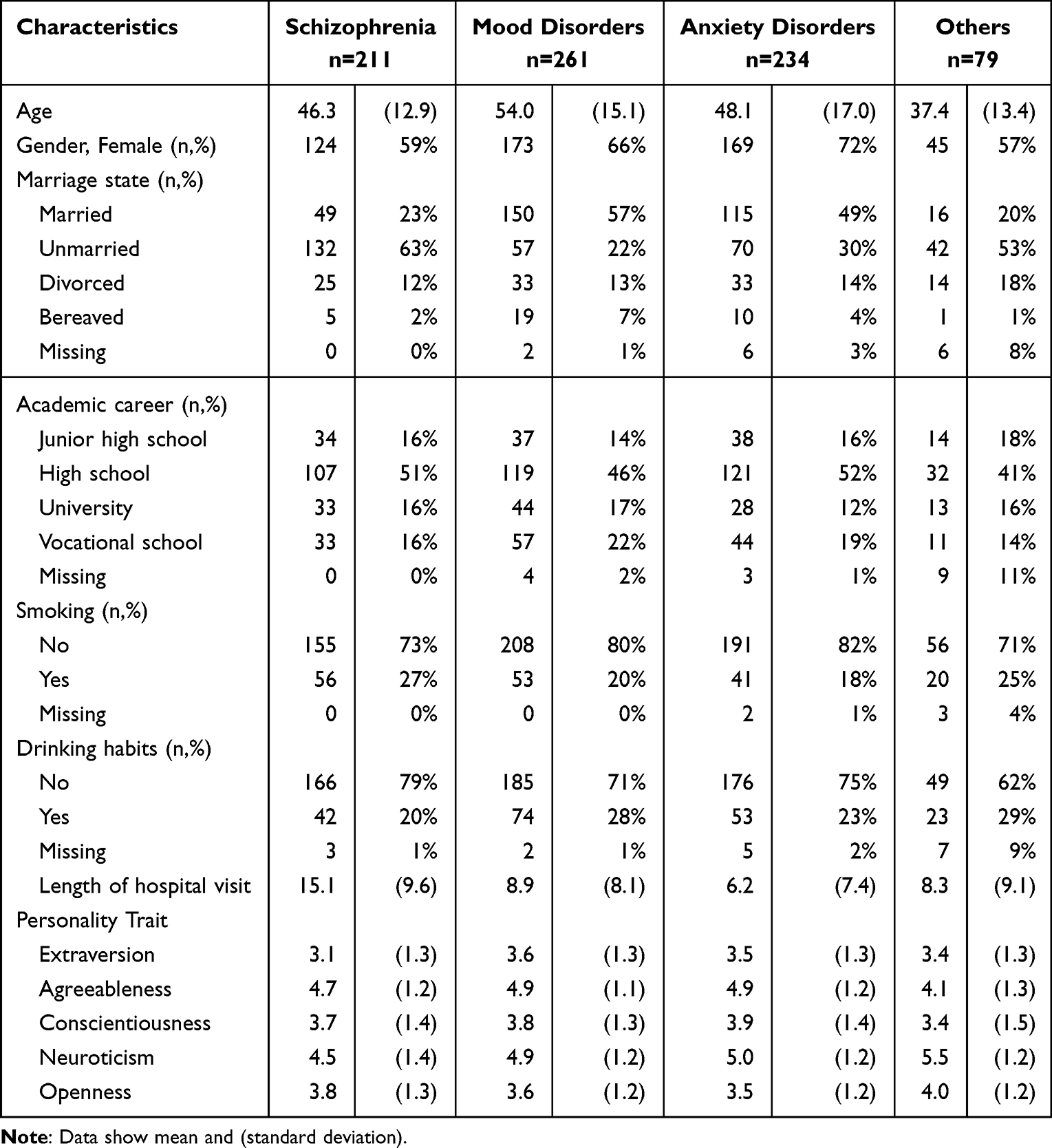 |
Table 1 Characteristics of Subjects with Mental Illness |
Health Literacy Scores Among Patients with the Major Psychiatric Diseases
Table 2 shows the health literacy scores among the three groups (patients with schizophrenia, mood disorders, and anxiety disorders). Fifty-two percent of patients with schizophrenia, 51% of patients with mood disorders, and 38% of patients with anxiety disorders were classified as having “limited” (0–33 points) health literacy according to the GEN-HL; 49% of patients with schizophrenia, 50% of patients with mood disorders, and 40% of patients with anxiety disorders were classified as having “limited” health literacy according to the HC-HL. According to the DP-HL, 46% of patients with schizophrenia, 43% of patients with mood disorder, and 34% of patients with anxiety disorder had ‘limited’ health literacy. Finally, according to the HP-HL, 44% of patients with schizophrenia, 44% of patients with mood disorder, and 35% of patients with anxiety disorder had ‘limited’ health literacy.
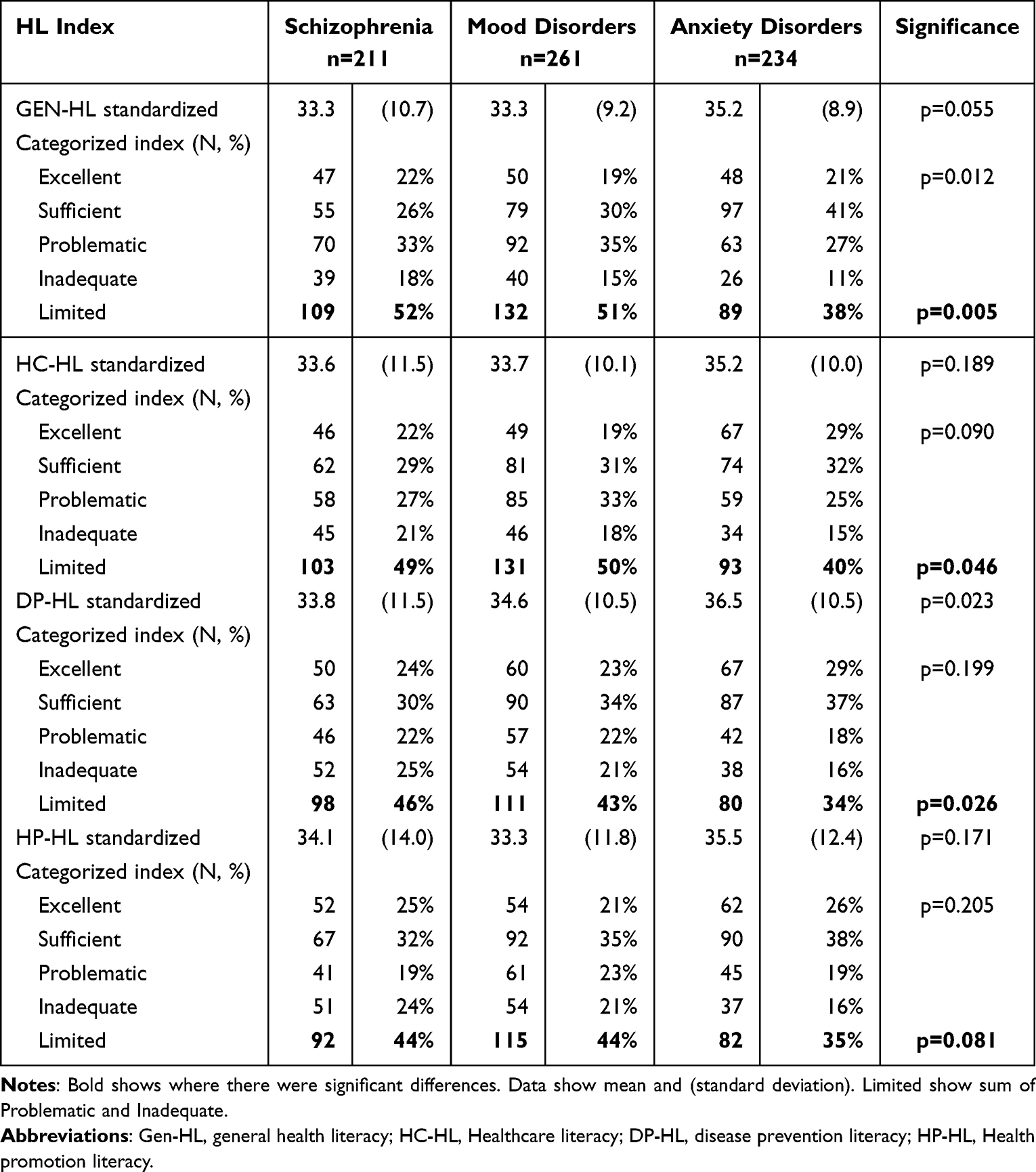 |
Table 2 Results of the Health Literacy Indices Among Three Metal Illness |
Health Literacy Scores Between Patients with Different Mood Disorders (Major Depressive Disorder and Bipolar Disorder)
Table 3 shows the health literacy scores for patients with major depressive disorder and those with bipolar disorder. Among patients with bipolar disorder and major depressive disorder, 51% and 50% were classified as having “limited” health literacy according to the GEN-HL, 49% and 50% according to the HC-HL, 37% and 44% according to the DP-HL, and 42% and 45% according to the HP-HL, respectively.
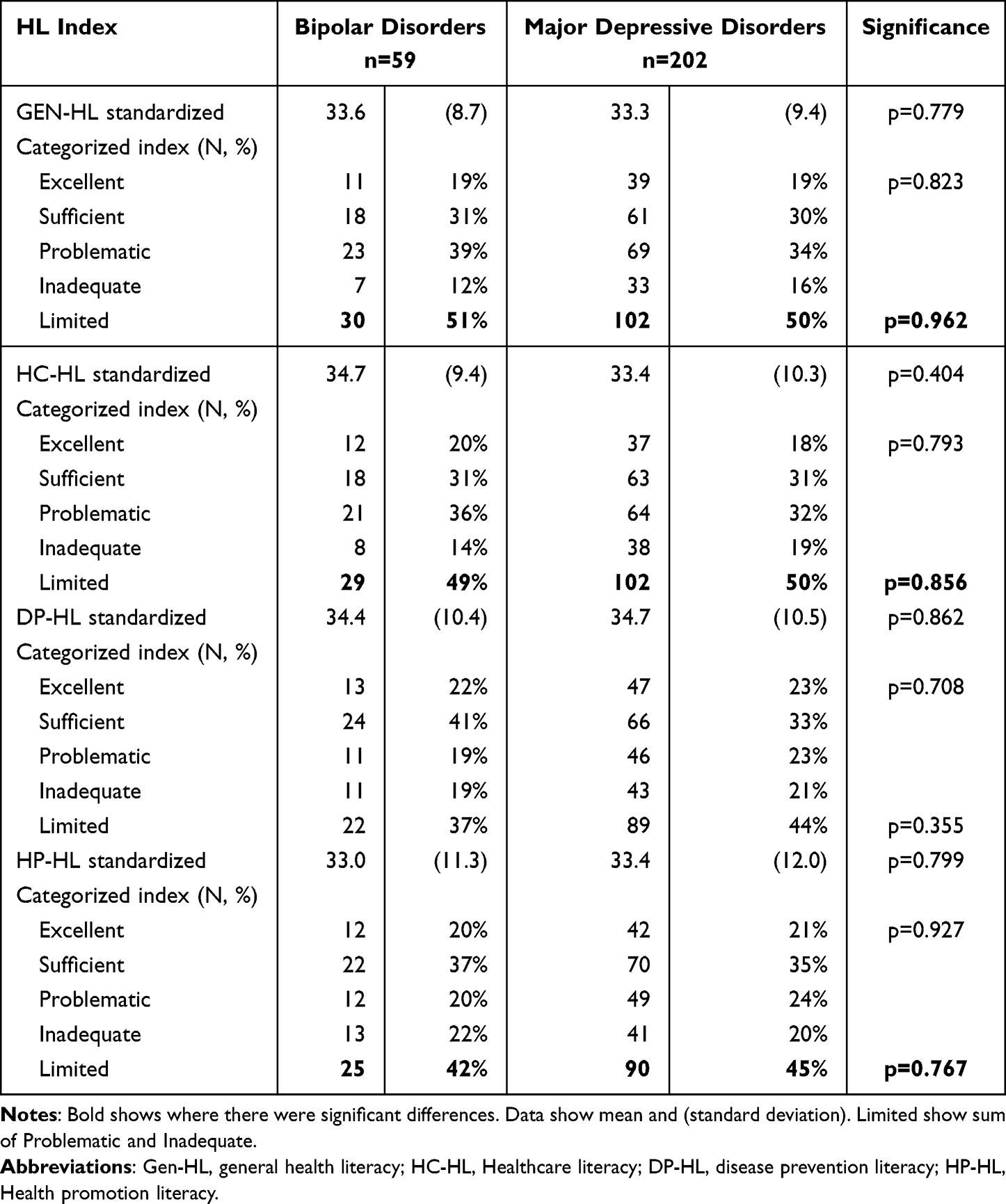 |
Table 3 Results of the Health Literacy Indices Between Bipolar Disorders and Major Depressive Disorders |
Factors Associated with Health Literacy
Logistic regression analysis was conducted to identify the determinants of general health literacy (Table 4 and Table 5). Female gender and four of the five personality factors, namely, extraversion, agreeableness, neuroticism, and openness, were identified as determinants of health literacy. Extraversion and agreeableness were associated with health literacy that was sufficient or above, while neuroticism and openness were associated with limited health literacy. In addition, anxiety disorders were associated with health literacy that was sufficient or above.
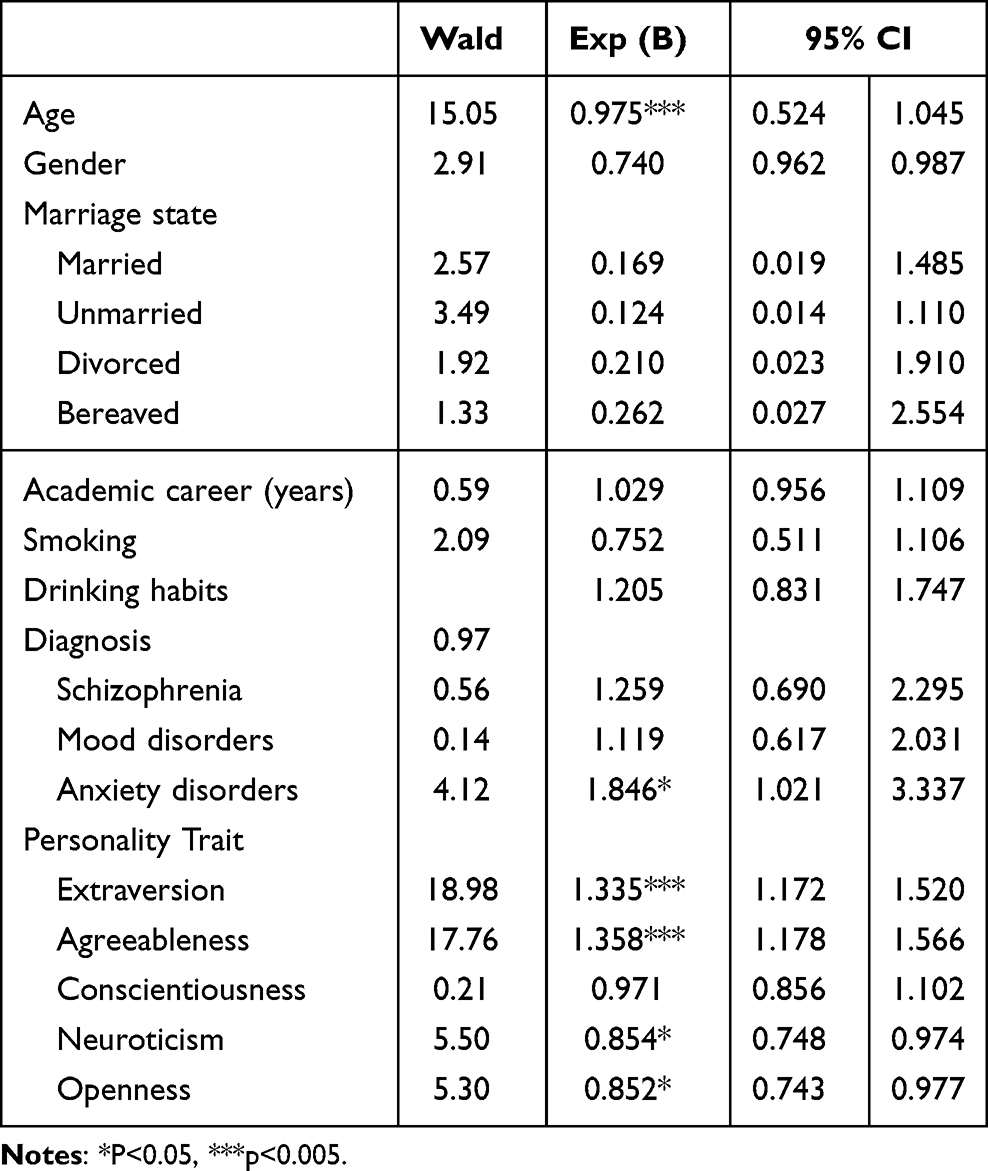 |
Table 4 Odds Ratio for General Health Literacy by Patient Characteristics in Logistic Regression Analysis |
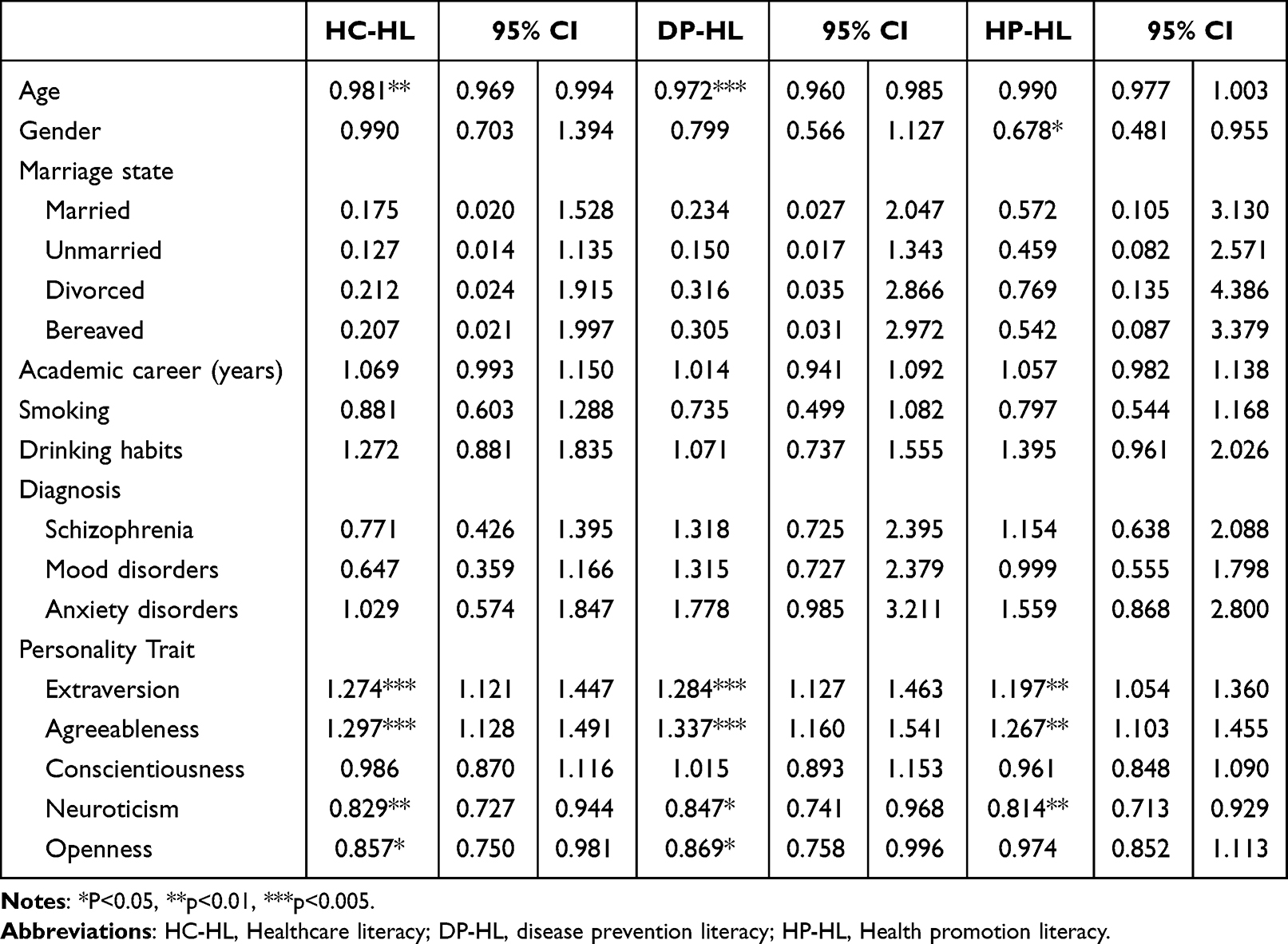 |
Table 5 Odds Ratio for Subitems of Health Literacy by Patient Characteristics in Logistic Regression Analyses |
Discussion
The results of this study showed that health literacy was sufficient or above in the anxiety disorder group than in the schizophrenia and mood disorder groups among patients with psychiatric disorders. This is the first study to determine whether there are differences in health literacy by illness. Higher health literacy in anxiety disorders than those in mood disorders or schizophrenia may be because anxiety disorders are less likely to be associated with cognitive dysfunction than mood disorders or schizophrenia22 and cognitive function is directly related to health literacy skills. Hence, more careful physical health instruction is needed for patients with mood disorders and schizophrenia. One-way service providers may be able to address this gap is by providing more careful health instruction for patients with mood disorders and schizophrenia.
In this study, extraversion and agreeableness were associated with high health literacy, while neuroticism and openness were associated with limited health literacy. Although the results for extraversion and neuroticism are reasonable because the vectors are always reversed, the association between openness and limited health literacy differs from the findings of previous studies of healthy subjects. Previous studies have found an association between increased openness scores and higher utilization of alternative medicine23 and use of complementary/alternative medicine,24 while an association between increased openness scores and increased use of medical services was reported.25 Openness is also referred to as the “ability to challenge” and is considered a measure of broadening of mental associations, diffuse thinking, and artistic sensitivity.26
While health literacy is important in the treatment of physical illnesses,9 and psychiatry is more concerned with the patient’s awareness of his or her illness and holistic care. Increasing health literacy for people with mental illness supports their active involvement in managing their own health and exercising their right to self-determination. The following are health literacy recommendations for people with mental illness. 1) Patients and their families need to be provided with accurate and understandable information about mental illness. It is also important to provide patients with education to help them develop self-management skills. 2) Improved communication with healthcare professionals can help patients become active participants in the healthcare process. It is important that healthcare professionals work with patients to set treatment goals and support them in the decision-making process. 3) Regular support is needed to help patients understand information and exercise self-determination. This support may take many forms and may come from different sources, including from healthcare professionals, family members and support groups. 4) To ensure that patients can achieve health literacy, the accessibility of information and services needs to be improved. This includes providing information in appropriate languages and formats, providing a barrier-free environment and providing online resources. 5) Patients can perform self-assessments to gain a better understanding of their health status and the care they need. It is important for healthcare professionals to provide patients with tools for self-assessment and to support them in managing their own health conditions.
This study has limitations. First, this was a single cross-sectional study in a single region, so causality could not be addressed. In addition, the study may have been strongly influenced by the local health care system. The areas from which participants were recruited are rural and lack adequate access to healthcare resources. Different results may be obtained in urban areas. Second, as the questionnaire was self-administered, it is not known whether the respondents answered the questions objectively and correctly. It is possible that the participants were influenced by social desirability bias, which confuses facts and wishes with statements. It is also possible that participants were strongly influenced by their own medical conditions. In other words, depression may have led to a negative portrayal of health literacy due to low self-esteem and the belief that it is a bad condition.
Conclusion
The results of this study showed that the health literacy of patients with psychiatric disorders was higher in the anxiety disorder group than in the schizophrenia and mood disorder groups. There was no difference between patients with bipolar disorder and patients with depression. Gender and four of the five factors in the personality model (extraversion, agreeableness, neuroticism, and openness) were associated with health literacy. In the future, it will be necessary to examine factors such as employment, economics, and education, as well as the relationship between health literacy and final outcomes of health and quality of life, including mortality, among persons with mental illness.
Abbreviations
ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; DP-HL, the Disease Prevention Health Literacy Index; GEN-HL, the General Health Literacy Index; HC-HL, the Health Care Health Literacy Index; HLS-EU-Q47, European Health Literacy Survey Questionnaire; HP-HL, the Health Promotion Health Literacy Index; TIPI-J, the Japanese version of the Ten Item Personality Inventory.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study protocol conformed with the Declaration of Helsinki and was approved by the Ethics Committee of Hirosaki University Hospital and the affiliated hospitals where it was conducted. Written informed consent was obtained from each patient to participate in the study.
Consent for Publication
Written informed consent was obtained from each patient for the publication.
Acknowledgments
We gratefully acknowledge Dr. Hanako Furukori, Dr. Taku Nakagami, Dr. Akira Fujii, Dr. Kazuyoshi Kubo, and Dr. Yasushi Sato for their kind support.
Funding
This study was funded by a Grant-in-Aid for Scientific Research (KAKENHI) from the Japan Society for the Promotion of Research JSPS, 21K07486 (Principal Investigator Norio Yasui-Furukori) and Dokkyo International Medical Education and Research Foundation Award (Yoshiteru Sato and Norio Yasui-Furukori). The funders had no role in the study design, the data collection and analysis, the decision to publish, or the preparation of the manuscript.
Disclosure
Dr Norio Yasui-Furukori reports grants from Mochida Pharmaceutical, Yoshitomi Yakuhin, grants from Tsumura, Mitsubishi-Sumitomo Pharmaceutical, Otsuka Pharmaceutical, Viatris Pharmaceutical and from Takeda Pharmaceutical, outside the submitted work. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Chang CK, Hayes RD, Perera G, et al. Life expectancy at birth for people with serious mental illness and other major disorders from a secondary mental health care case register in London. PLoS One. 2011;6(5):e19590. doi:10.1371/journal.pone.0019590
2. Sugawara N, Yasui-Furukori N, Sato Y, et al. Prevalence of metabolic syndrome among patients with schizophrenia in Japan. Schizophr Res. 2010;123(2–3):244–250. doi:10.1016/j.schres.2010.08.030
3. Sugawara N, Yasui-Furukori N, Sato Y, et al. Comparison of prevalence of metabolic syndrome in hospital and community-based Japanese patients with schizophrenia. Ann Gen Psychiatry. 2011;10:21. doi:10.1186/1744-859X-10-21
4. Gonzalez JS, Peyrot M, McCarl LA, et al. Depression and diabetes treatment nonadherence: a meta-analysis. Diabetes Care. 2008;31(12):2398–2403. doi:10.2337/dc08-1341
5. Frydensberg VS, Johansen JB, Moller S, et al. Anxiety and depression symptoms in Danish patients with an implantable cardioverter-defibrillator: prevalence and association with indication and sex up to 2 years of follow-up (data from the national DEFIB-WOMEN study). Europace. 2020;22(12):1830–1840. doi:10.1093/europace/euaa176
6. Calverley PMA, Walker PP. Contemporary concise review 2022: chronic obstructive pulmonary disease. Respirology. 2023;28(5):428–436. doi:10.1111/resp.14489
7. Peters JE, Basnayake C, Hebbard GS, Salzberg MR, Kamm MA. Prevalence of disordered eating in adults with gastrointestinal disorders: a systematic review. Neurogastroenterol Motil. 2022;34(8):e14278. doi:10.1111/nmo.14278
8. Nakhlband A, Farahzadi R, Saeedi N, Barzegar H, Montazersaheb S, Soofiyani SR. Bidirectional relations between anxiety, depression, and cancer: a review. Curr Drug Targets. 2023;24(2):118–130. doi:10.2174/1389450123666220922094403
9. Visscher BB, Steunenberg B, Heijmans M, et al. Evidence on the effectiveness of health literacy interventions in the EU: a systematic review. BMC Public Health. 2018;18(1):1414. doi:10.1186/s12889-018-6331-7
10. Parnell TA, Stichler JF, Barton AJ, Loan LA, Boyle DK, Allen PE. A concept analysis of health literacy. Nurs Forum. 2019;54(3):315–327. doi:10.1111/nuf.12331
11. Mahmud AJ, Olander E, Eriksén S, Haglund BJ. Health communication in primary health care -a case study of ICT development for health promotion. BMC Med Inform Decis Mak. 2013;13:17. doi:10.1186/1472-6947-13-17
12. Zielińska-Więczkowska H. Relationships between health behaviors, self-efficacy, and health locus of control of students at the universities of the third age. Med Sci Monit. 2016;22:508–515. doi:10.12659/MSM.894997
13. Iwasa H, Yoshida Y. Personality and health literacy among community-dwelling older adults living in Japan. Psychogeriatrics. 2020;20(6):824–832. doi:10.1111/psyg.12600
14. Mai J, Yibo W, Ling Z, Lina L, Xinying S. Health literacy and personality traits in two types of family structure-a cross-sectional study in China. Front Psychol. 2022;13:835909. doi:10.3389/fpsyg.2022.835909
15. Caruso R, Magon A, Baroni I, et al. Health literacy in type 2 diabetes patients: a systematic review of systematic reviews. Acta Diabetol. 2018;55(1):1–12. doi:10.1007/s00592-017-1071-1
16. Koyama T, Tachimori H, Sawamura K, et al. Mental health literacy of autism spectrum disorders in the Japanese general population. Soc Psychiatry Psychiatr Epidemiol. 2009;44(8):651–657. doi:10.1007/s00127-008-0485-z
17. Kim SW, Park WY, Jhon M, et al. Physical health literacy and health-related behaviors in patients with psychosis. Clin Psychopharmacol Neurosci. 2019;17(2):279–287. doi:10.9758/cpn.2019.17.2.279
18. Oshio A, Abe S, Cutrone P. Development, reliability, and validity of the Japanese version of Ten Item Personality Inventory (TIPI-J). Jpn J Pers. 2012;21:40–52.
19. Gosling SD, Rentfrow PJ, Swann WB Jr. A very brief measure of the Big-Five personality domains. J Res Pers. 2003;37:504–528. doi:10.1016/S0092-6566(03)00046-1
20. Sørensen K, Pelikan JM, Röthlin F, et al. Health literacy in Europe: comparative results of the European health literacy survey (HLS-EU). Eur J Public Health. 2015;25(6):1053–1058. doi:10.1093/eurpub/ckv043
21. Nakayama K, Osaka W, Togari T, et al. Comprehensive health literacy in Japan is lower than in Europe: a validated Japanese-language assessment of health literacy. BMC Public Health. 2015;15:505. doi:10.1186/s12889-015-1835-x
22. Yilmaz G, Yildirim EA, Tabakcı AS. Comparison of social-evaluative anxiety and theory of mind functions in social anxiety disorder, schizophrenia, and healthy controls. Psychopathology. 2023;14:1–13. doi:10.1159/000529880
23. Honda K, Jacobson JS. Use of complementary and alternative medicine among United States adults: the influences of personality, coping strategies, and social support. Prev Med. 2005;40(1):46–53. doi:10.1016/j.ypmed.2004.05.001
24. Gok Metin Z, Karadas C, Ozdemir L. Usage and attitudes related to complementary and alternative medicine among Turkish academicians on the basis of the five-factor model of personality: a multi-centered study. Complement Ther Med. 2019;44:151–156. doi:10.1016/j.ctim.2019.04.012
25. den Boeft M, Twisk JW, Terluin B, et al. The association between medically unexplained physical symptoms and health care use over two years and the influence of depressive and anxiety disorders and personality traits: a longitudinal study. BMC Health Serv Res. 2016;16:100. doi:10.1186/s12913-016-1332-7
26. O’Brien TB, DeLongis A. The interactional context of problem-, emotion-, and relationship-focused coping: the role of the big five personality factors. J Pers. 1996;64(4):775–813. doi:10.1111/j.1467-6494.1996.tb00944.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.