")
Back to Journals » Orthopedic Research and Reviews » Volume 14
Surgical Approaches for Managing Femoral Head Fractures (FHFs); What and How to Choose from the Different Options?
Authors Khalifa AA , Ahmed EM, Farouk OA
Received 11 December 2021
Accepted for publication 2 April 2022
Published 23 April 2022 Volume 2022:14 Pages 133—145
DOI https://doi.org/10.2147/ORR.S353582
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Ahmed A Khalifa,1 Esraa M Ahmed,2 Osama A Farouk3
1Orthopedic Department, Qena Faculty of Medicine and University Hospital, South Valley University, Qena, Egypt; 2Qena Faculty of Medicine, South Valley University, Qena, Egypt; 3Orthopedic and Traumatology department, Assiut University Hospital, Assiut, Egypt
Correspondence: Ahmed A Khalifa, Orthopedic Department, Qena Faculty of Medicine and University Hospital, South Valley University, Kilo 6 Qena-Safaga Highway, Qena, 83523, Egypt, Tel +20 965337573, Fax +20 965337571, Email [email protected]
Abstract: Femoral head fractures (FHFs) are considered a relatively uncommon injury; however, they carry a challenge to the trauma surgeon. Choosing the appropriate management option, either conservatively or surgically, if the latter was chosen, should it be open reduction and internal fixation or simple excision of the fragment, or acute total hip arthroplasty. Furthermore, selecting the best surgical approach through which surgical management could be performed depends on the fracture classification, the familiarity of the surgeon, and the presence of associated injuries. All approaches to the hip, including hip arthroscopy, had been proposed for the management of FHFs; however, the difference among approaches is related to the complexity of the approach, the need for special training or equipment, the effect of the approach on the functional outcomes as well as the rate of postoperative complications. This review discussed the possible surgical approaches used to manage FHFs, advantages, and disadvantages for each, and offered a guideline for selecting the most appropriate surgical approach.
Keywords: femoral head fracture, Pipkin, approaches, Kocher-Langenbeck, Smith-Peterson, surgical hip dislocation
Introduction
Femoral head fractures (FHFs) pose a challenge to the trauma surgeon; after being diagnosed and classified, the surgeon has to decide the best way of management; the controversy starts from the moment the patient is seen if the hip is dislocated, should it be reduced by closed maneuver or open surgery.1,2 After successful reduction, will the fracture be treated surgically or conservatively, if the surgery was chosen, should the surgeon excise the fractured fragment or will it be fixed or an acute total hip replacement will be the option,3 and through which approach the surgery will be performed?.4
Several classification systems had been proposed upon which the management will be chosen, commonly and after which the fracture was named is the Pipkin classification5 (Figure 1), other classifications included the Chiron’s classification system,6 AO classification,7 Brumback’s classification,8 and Yoon.9
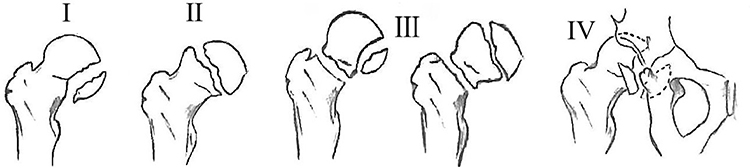 |
Figure 1 Pipkin classification of femoral head fractures. Type I: Fracture below fovea, Type II: Fracture above fovea, Type III: Type I or II with an associated femoral neck fracture, and Type IV: Type I or II with associated acetabular fracture. |
Most of the approaches to the hip joint, including hip arthroscopy (Figure 2A–D), were suggested for surgical management of FHFs (either excision or open reduction and internal fixation (ORIF), or acute total hip arthroplasty (THA)); however, there is no golden approach that fits all injuries.10,11 Instead, these approaches could be classified according to the direction the hip joint would be approached into anterior, posterior, lateral, and medial-based approaches.10–12 In addition, it could be classified as conventional approaches or minimally invasive (such as arthroscopy).13,14
 |
Figure 2 Demonstration of the suggested approaches for the management. (A) Medial approach to the hip. (B) Anterior, anterolateral, lateral, and posterior approaches. (C) Hip arthroscopy. (D) Surgical hip dislocation (SHD). |
In the systematic review by Giannoudis et al, the data regarding the surgical approaches used were retrieved from 14 articles forming 177 surgical cases; the approaches were distributed as follows: the posterior was the most commonly used in 72 (40.68%) cases, followed by the anterior in 44 (24.86%) cases, in the third place was the surgical hip dislocation (SHD) in 36 (20.34%) patients, other approaches were reported in fewer numbers (lateral in ten (5.65%), anterolateral in five (2.82%), and medial in six (3.36%)), they reported the use of dual approaches (anterior and posterior) in four (2.26%) cases.10
Proper selection of the surgical approach is paramount for the preservation of soft tissues and better visualization, which ultimately should result in optimum functional and radiographic outcomes with the least possible complication rates, so the current review aimed to describe the possible surgical approaches suitable for managing different types of FHFs based on Pipkin classification types, reporting the potential advantages and disadvantages of each approach, and providing guidelines and an algorithm for how to select the best surgical approach.
Possible Approaches for FHFs Surgical Management
Before choosing the approach to perform the surgery, the surgeon should be familiar with the anatomical structures and landmarks of the hip region; some approaches like the SHD need special training and practice without rushing to adopt such an approach in daily practice.12,15
From a technical point of view, the surgery starts by preoperative planning (including choosing the approach), then in the operative theater, proper positioning of the patient and proper draping (taking into account the possibility of approach extension or the need for a graft), optimum placement of the skin incision, gentle handling of the soft tissues, working and dissecting through normal cleavage lines and taking care of important structures (neurovascular bundle).16,17
For the sake of simplicity, we will discuss different approaches based on the direction of entry to the hip joint:
Anterior-Based Approaches
Carl Hueter, a German surgeon, in 1881, was the first to describe a direct anterior approach to the hip,18 which was then popularized by Marius N. Smith-Petersen, and the approach was known by his name since then as the Smith‑Petersen (S-P) approach.19
Approach details: the incision starts from the middle of the iliac crest to the anterior superior iliac spine (ASIS) along an imaginary line extending distally to the fibular head; the incision is carried as a straight line centered over the tensor fascia latae (TFL) and could be extended distally for about ten cm. It could be minimized to what is called the “mini‑incision anterior approach.” Superficially, the interval is between the TFL (superior gluteal nerve), and the Sartorius muscle (femoral nerve), the lateral femoral cutaneous nerve piercing the deep fascia close to the intramuscular interval is saved, the lateral femoral circumflex artery (LFCA) ascending branch should be identified, and if possible clamped, while it crosses this interval. Further, deep dissection is carried through the interval between the rectus femoris (femoral nerve) detached from its origin and retracted medially, and the gluteus medius (superior gluteal nerve) retracted laterally; this will expose the hip joint capsule. Capsulotomy will expose the femoral head and enables the surgeon to identify, and then excise or fix the fractured fragments.
Advantages
1. It is proposed to be safer regarding hip vascularity than the posterior approaches.20
2. In isolated FHF (Pipkin I and II) cases, the main fragment is mostly located in the anteromedial part of the head, making the S-P approach suitable for reaching this fragment and fixation without the need for fully dislocating the hip.21
3. The dissection is carried through true internervous and intermuscular planes (superficially and deep).
4. It avoids disruption and detachment of the abductor muscles with less incidence of postoperative limping.
5. Using the S-P approach, we showed a reduction in the operative time, blood loss, and incidence of femoral head avascular necrosis (AVN) in some studies.22,23
Disadvantages
1. A reported increased risk of heterotopic ossification (HO) formation with the anterior approaches, reaching up to 40%.20,22
2. The possibility of interrupting the remaining blood supply (LFCA ascending branch) to the head as the blood supply may be already jeopardized after the incident of the posterior dislocation.1
3. It will not allow for a wide free inspection of the acetabulum unless an extensive release of the TFL and gluteus medius is performed.24
4. Persistent anterolateral thigh numbness in up to 9% of patients managed through the S-P approach.25
5. Concomitant posterior injury could not be handled using this approach as Pipkin type IV.
Posterior-Based Approaches
This section will mainly describe the two main posterior approaches reported to manage FHFs: the classic posterior approaches to the hip (mainly Kocher-Langenbeck approach) and the Ganz surgical hip dislocation.
Classic Posterior Approaches to the Hip
It was first described by Bernhard von Langenbeck in 1874 and modified by Kocher, and since then, it has been known as “Kocher-Langenbeck (K-L) approach”.26 This approach does not disrupt the abductor mechanism, and many variations were described depending on the placement of the skin incision and the level at which the gluteus maximus muscle is dissected.27–29
Approach details: Skin incision started about ten cm distal to the posterior superior iliac spine extending laterally and directed distally toward the greater trochanter about 15 cm coincident with the femoral shaft. After dividing the gluteal fascia in line with the skin incision, the gluteus maximus fibers are bluntly dissected into proximal and distal halves (this is a true internervous plane as the superior gluteal vessels and nerves supply the proximal half of the muscle, while the inferior gluteal vessels and nerves supply the distal half). The sciatic nerve is then identified and protected, and to expose the hip joint capsule, the short external rotators are dissected and detached from the femoral insertion (usually the piriformis tendon was tagged and released, but the Gemelli and obturator internus were preserved) and retracted medially as a sleeve, which aids in the protection of the sciatic nerve. Damage to the obturator externus muscle indicates the severity of the injury as this muscle is closely related to the medial femoral circumflex artery.
Advantages
1. In cases where the hip was posteriorly dislocated and irreducible, this approach is suitable for open reduction.30
2. Suitable for managing associated acetabulum fracture as in Pipkin IV injuries.
Disadvantages
1. A higher possibility of vascular supply injury with an increased risk of AVN.
2. If the fracture was oriented more anteriorly and medially, which was suggested to be the most commonplace for the injury from an anatomical and biomechanical point of view,31 direct screw fixation is difficult.32
3. Risk of iatrogenic sciatic nerve injury.
Surgical Hip Dislocation (SHD)
The original description of this approach was popularized by Ganz et al.33
Approach details: the same skin incision as in the K-L approach; however, the Gibson interval27 is used, dissecting between the gluteus medius anteriorly and the gluteus maximus posteriorly, following identification of the greater trochanter and the short external rotators, the interval between the piriformis tendon and the posterior border of the gluteus minimus was identified, then the trochanteric flip osteotomy (TFO) about 1.5 cm thick is initiated from the posterosuperior border of the greater trochanter and extended to the border of the vastus lateralis, which is then retracted anteriorly, the gluteus minimus is dissected sharply from the capsule followed by hip flexion to relax the anterior structures. Finally, the capsulotomy was carried out in a Z-shaped fashion; the femoral head is delivered by progressive hip flexion and external rotation, which a hook around the femoral neck could facilitate after cutting the ligamentum teres.
Advantages
1. All external rotator muscles are not interrupted and protect the medial femoral circumflex artery (MFCA), which is the main vascular supply to the femoral head, with a lower incidence of AVN.34
2. It provides 360 degrees of visualization of the femoral head and the acetabulum, with the ability to fully assess the femoral head and acetabulum to detect any associated injuries like labrum avulsion or impaction injuries even if not diagnosed in the preoperative imaging studies.35
3. The Z-shaped capsulotomy will allow elevation of a retinacular flap, which further protects the blood supply.33
4. The ability to check the vascularity intraoperatively can be performed through a small perforation in the head and a bleeding sign positively correlated with the viability of the femoral head.33,35 Some authors described using intraoperative laser Doppler flowmetry as proposed by Nötzli et al.36
Disadvantages
SHD carried some unique complications such as:
1. TFO non-union, which had been reported in some studies.33,37
2. The surgeon should be trained and familiar with the approach, as some authors reported an inability to use this approach due to unfamiliarity.38
3. The screws used to fix the TFO could cause trochanteric bursitis with persistent lateral thigh pain necessitating its removal.39,40
4. The higher incidence of HO formation reached up to 37% of the cases.33
5. The possibility of increased operative time for the extra steps needed for fixing the TFO.
Lateral-Based Approaches
These approaches were suggested as the best approach for managing Pipkin III fractures, as it enables addressing the head fracture element and the neck fracture element through one approach.21
Anterolateral Approach
This first description of the approach was by Sayer in 1876, and then it was popularized by Watson-Jones (W-J) in 1936, and the approach is known by this name.41 Some authors introduced modifications, such as Charnley,42 Harris,43 and Muller.44
Approach details: The skin incision is centered laterally over the mid-portion of the greater trochanter and could be extended superiorly to a point about three cm posterior to the ASIS and could be extended distally about 10 to 15 cm along the axis of the femoral shaft. After incising the fascia lata in line with the skin incision, the intermuscular plane between the TFL and gluteus medius is developed by blunt dissection.45,46 The superior aspect of the hip joint capsule and the femoral neck is exposed by retracting the gluteus medius and the gluteus minimus proximally and laterally.
Lateral Approaches
The lateral approaches can be subclassified according to the detaching of the abductor mechanism either into a direct lateral (going through the musculotendinous portion) or trans‑trochanteric techniques; however, in both techniques, the surgeon goes through the hip abductor mechanism.
1. The direct lateral technique: was first described by McFarland and Osborne in 1954,47 and further modifications were introduced, such as the one done by Hardinge in 1982.48 The main idea behind this approach is that the gluteus medius and vastus lateralis are considered a direct functional unit that continues through the thick tendinous periosteum over the greater trochanter.47,49
Approach details: A straight skin incision as in the anterolateral approach, the fascia lata and iliotibial band are divided in line with the skin incision, the difference between the different approaches lies in the deep dissection as follows: McFarland and Osborne described retracting the gluteus maximus posteriorly and the TFL anteriorly, after identification of the gluteus medius, incising the posterior border of the muscles down to the bone, and the tendon of the gluteus medius, the periosteum, and origin of vastus lateralis is dissected and retracted anteriorly as one flap followed by dividing retracting gluteus minimus proximally to expose the joint capsule. In contrast, Hardinge described his modification by going trans‑gluteal by incising the gluteus medius tendon at the greater trochanter and dividing the muscle into an intact posterior half still attached to the trochanter dissecting the anterior half to expose the gluteus minimus and the joint capsule.
2. Trans‑trochanteric technique: In this technique, the abductor mechanism and the vastus laterals attachment to the greater trochanter are osteotomized and mobilized as one flap as described by Charnley and Ferreiraade.50 Harris technique is the most popularly used; after dividing the iliotibial band in line with the skin incision, the osteotomized greater trochanter with the attached gluteus medius is reflected proximally, while the origin of the vastus lateralis is retracted distally; this will expose the short external rotators, which are divided from its femoral origin to expose the hip joint capsule.51 Glassman et al introduced a modification by creating an osteotomy in the sagittal plane, which preserves the gluteus medius and vastus lateralis as one unit, which is then retracted anteriorly.52
Advantages
1. The anterolateral approach offers a true intermuscular approach.
2. It provides optimum exposure to the femoral neck in cases with Pipkin III injuries.
3. It carries a lower risk of femoral head AVN, as the LFCA ascending branch could require ligation as it passes deep into TFL and gluteus medius; however, the superior retinacular vessels are not interrupted in this approach, which preserves the vascularity of the femoral head.
Disadvantages
1. It offers limited exposure to the acetabulum and posterior injuries.
2. If the dissection is taken proximally, injuring the superior gluteal vessel and nerve is a risk.
3. Postoperative limping secondary to abductor weakness could occur with the lateral approach.
Medial-Based Approach
This section will describe two main approaches: the classic direct medial approach described by Ludloff (including its modifications), and the anterior medial approach described recently by some authors as a minimally invasive approach for managing FHFs.53
Direct Medial Approaches
It was first described by Ludloff in 1908 to be utilized in developmental hip dysplasia surgeries,54,55 then in 1973, Ferguson modified and popularized the approach.56 Ludloff, in his original description, did not define the exact intervals; however, the approach was defined as being through the plane between the adductor longus and sartorius superficially and between the iliopsoas and pectineus deeply. Ferguson’s modified the approach to go more posteriorly between the gracilis and adductor longus superficially and the interval between the adductor brevis and adductor Magnus deeply.56 Chiron et al reported using a novel “medial hip approach” to manage anterior-inferior FHFs; they used a more anterior interval that passes between the adductor muscles bellies (longus, brevis, and pectineus) posteriorly and their aponeuroses anteriorly.6,57
Approach details: While the patient is supine, the hip is flexed, abducted, and externally rotated, making the lesser trochanter and medial joint capsule closer to the skin. A longitudinal skin incision about three cm distal to the pubic tubercle and coincident with the adductor longus: bluntly, develop the superficial plane between the adductor longus and gracilis (the obturator nerve supplies both), then the deep plane between the adductor brevis and adductor Magnus (the obturator nerve supplies both) is developed. The adductor longus and brevis are retracted anteriorly, while the gracilis and adductor Magnus are retracted posteriorly. To expose the hip joint capsule, dissect and transect the iliopsoas tendon to expose the lesser trochanter deep in the approach.
Advantages
1. Minimum dissection and blood loss.
2. This approach allows direct exposure of the fracture site, mainly in Pipkin type I and II, with the ability to expose other structures, mainly the base of the femoral neck, the lesser trochanter, and the anterosuperior, anterior, and anteroinferior parts of the acetabular wall with the labrum.57,58
Disadvantages
1. Technically difficult for unfamiliar surgeons.
2. Risk of damage to the MFCA with increased risk of femoral head AVN.
3. Specific drawbacks of using the approach described by Chiron et al are the proximity to the femoral vascular bundle anteriorly and the limited access to the femoral head posterior aspect.
Anterior Medial Fenestration Approach
This approach was described by Wang et al for in situ fixation of Pipkin I and II injuries.53
Approach details: After hip flexion, abduction, and external rotation, while the patient is in a supine position, an incision about 6–9 cm is carried medially to the femoral artery. After incising the deep fascia, the authors described feeling the femoral artery pulsation, and at its medial border, the adductor longus and pectineus were exposed, taking care to protect the superficial great saphenous vein and its branches on the lateral side.
The adductor longus and the pectineus will be retracted medially (medial boundary), the femoral artery and vein were retracted laterally (lateral boundary), this will expose the lesser trochanter, then the iliopsoas muscle was dissected and retracted proximally (upper boundary); this will expose the deep femoral artery and the transverse branch of the MFCA at the inferior portion of the approach (inferior boundary), where they should be identified and protected before retracting them inferiorly. The fenestration is essentially formed between these four boundaries where the hip capsule could be deeply exposed and opened to reveal the lower part of the femoral head.
Advantages
The authors reported this approach as being minimally invasive, preserving the vascularity of the femoral head, being medial to the femoral sheath guard against injury of the femoral nerve, enabling in situ reduction and fixation with a limited opening of the hip joint capsule, and the ligamentum teres need not be cut.
Disadvantages
The authors mentioned one major disadvantage (although it did not happen to them) is the possibility of infection spread to the femoral artery and vein; due to their proximity to the approach, which could be fatal, they recommended keeping the femoral sheath intact. However, the authors did not mention regarding the amount of retraction needed and whether this will increase deep venous thrombosis (DVT) development risk.
5-Hip Arthroscopy
Hip arthroscopy was introduced to manage various situations of hip traumatic conditions and could be used in cases with FHFs either for excision of the fractured fragment or ORIF, especially in pipkin type I.11,13,59
Advantages
1. Hip arthroscopy offers conservative arthrotomy, particularly when fragment excision is decided due to too small or fragmented pieces not amenable for fixation.
2. Less blood loss, a shorter operating time,
3. Better cosmetic appearance.
4. It enables the management of associated intraarticular injuries, such as labral tears.14
Disadvantages
1. Associated acetabular fractures could not be managed.
2. Peripheral neurological injury caused by traction or by the surgical instruments (pudendal nerve, lateral cutaneous nerve of the thigh, sciatic nerve, and the femoral nerve).
3. The need for special training and equipment.
4. Bleeding from the portals, abdominal compartment syndrome in case of fluid leakage through the acetabulum, chondral damage.60,61
5. Some precautions were reported as mentioned by Park et al14 (after their experience of managing three cases of Pipkin type I by ORIF through hip arthroscopy); the authors eluded to some critical points the surgeon should be aware of before attempting ORIF of the FHFs through arthroscopy rather than excising the fragment, full knowledge of the safe portals, incorporating capsulotomy as performed during femoroacetabular impingement surgery, ability to use a 70-degree arthroscope, and carefully managing the fluid intraarticularly to avoid the risk of fluid extravasation into the intraabdominal and retroperitoneal spaces.14,62
Factors Affecting Approach Selection
This is a tough question to answer, choosing the appropriate approach depends on many factors; some of them are related to the injury (such as fracture classification and the presence of any associated injuries), the surgeon (such as experience and familiarity with the approaches), and the presence of special equipment (such as the hip arthroscopy preparations).10,11 To refer to an approach as being “ideal,” it should be safe, simple, anatomic (follows internervous and intermuscular planes), reproducible, versatile, with minor soft tissue damage, and it should provide adequate exposure to the injured area or to the area, which will be operated upon.16,17 Some of the crucial factors when selecting an approach are as follows:
Femoral Head Vascularity Preservation
Avascular necrosis (AVN) of the femoral head is one of the major complications after FHFs; however, this complication could occur due to damage to the main nutrient artery at the time of trauma or by surgical intervention, the incidence reported in the literature ranges from 7% to 24% independent of the approach.63,64
Supporters of posterior-based approaches based their argument on the possibility that the anterior-based approaches (mainly S-P) would damage any residual blood supply to the posteriorly displaced FHF;24 however, studies showed that the MFCA deep branch, which is the main supply to the femoral head was preserved after traumatic posterior dislocation;65 however, it could be injured during the posterior approach as shown in cadaveric studies.66,67 After dissecting 24 hips, Gautier et al found that the tenomyotomy of the external rotators is mandatory for hip dislocation during the posterior-based approaches; this will endanger the anastomosis between the MFCA deep branch and the inferior gluteal artery.66 At the same time, the contribution of LFCA to the femoral head vascularity was less (which is disrupted during anterior-based approaches).66 After introducing the SHD proposed by Ganz, this conflict was solved, where he showed definite protection of the MFCA deep branch while performing this approach.33
Visualization
For proper anatomical reduction and fracture fixation with an interfragmentary compression, the chosen approach should provide adequate visualization of the fracture surface; if visualization was not achieved, this might lead to changing the decision from fixation to excising the fragment as reported in the study by Swiontkowski et al.22 Another point is the ability of the approach to provide adequate exposure of the acetabulum for inspecting any associated injuries, the exposure of the femoral neck for appropriate fixation as in Pipkin III fractures, and the visualization of associated acetabulum injury as in Pipkin IV fractures.
Safety and Outcomes
Safety of the approach is measured by the incidence of its related complications (which in FHFs are represented into three major entities: HO formation, AVN, posttraumatic arthritis) and their effect on the functional outcomes of these patients.68
Giannoudis et al studied the relation between the functional outcomes and the utilized approach in 119 cases reported in 9 studies, excellent and good results according to the Thompson–Epstein criteria was reported in 83.4% (20 out of 24) of patients treated through SHD, to 65.4% (17 out of 26) with S-P approach, 49% (27 out of 53) with K-L approaches, and in 88.9% (eight out of nine) with lateral approach.10
For reporting the major late complications in relation to the surgical approach (after a mean follow-up of 59.7 months), 153 cases from 11 studies were reported upon, AVN was reported in 8.3% (three out of 36) patients treated through SHD, 5.3% (two out of 38) treated through the S-P approach, 16.9% (11 out of 65) treated through K-L approach, 0% (0 out of five) with W-J approach, and 11.1% (one out of nine) with the lateral approach. In addition, the authors reported that the chance of a patient to develop AVN when treated through a posterior approach was 3.67 and 2.24 times higher than an anterior or SHD approach, respectively (p > 0.05).10
Posttraumatic OA was not reported in any case in patients treated through SHD or lateral approach, while it was reported in 21%, 29.2%, and 20% in patients treated through the S-P, K-L, and W-J approaches, respectively. Post-traumatic arthritis was estimated to have a 20.3 (p = 0.04) and 30.6 (p = 0.018) times higher incidence when an anterior or posterior approach was used, respectively, versus SHD.10
For the HO development incidence, no cases were reported with the lateral approach; 47.2% of the patients managed through SHD, 44.7% with the S-P approach, 32.3% with the K-L approach, and 40% with the W-J approach.10
In a recent study by Abdelazeem et al evaluating their results of managing FHFs through the medial approach, the authors reported on 21 patients all Pipkin type I; however, the authors subdivided these according to the location of the fracture fragment into inferior anterior (IA) 14 (67.7%) and inferior posterior (IP) 7 (33.3%), after a mean follow-up of 24.3 months, all fractures healed by eight weeks, at the last follow-up, five cases (23.8%) showed posttraumatic OA, functional outcome according to Harris hip score at the last follow-up had a mean score of 82.3 (range: 14.6–95.8) and graded as good; however, the authors reported decreased range of hip external rotation in all patients.69
Wang et al reported using an anterior medial fenestration approach for in situ reductions and fixation of FHFs, claiming that this will be more conservative for the soft tissues, for management of Pipkin 1 and 2 type fractures (Pipkin type I (8 cases) and II (4 cases)), 12 cases were included, in situ fixation was performed through this approach, excellent and good rate of 83.33% according to Thomson–Epstein evaluation.53
Recently, Aparato et al compared hip arthroscopy and SHD for managing Pipkin type I fractures, they included five patients where FHFs were fixed through hip arthroscopy compared to eight managed through SHD, they achieved anatomic reduction in four patients in the arthroscopy group compared to five in the SHD group, the functional outcomes were significantly better in the arthroscopy group according to modified Harris hip score (94 points vs 88 points, P = 0.03), no major complications were reported from the arthroscopy group, the authors concluded that arthroscopic reduction and fixation of Pipkin type I fracture gave results equal and even better than SHD with a lower rate of complications.70
Approach Recommendations (Figure 3)
Based on the patient age, preinjury hip condition, and the Pipkin fracture classification, the approach for surgical management (excision, ORIF, or acute THA) could be selected as follows:
 |
Figure 3 Example flow chart showing how to select the most appropriate approach for femoral head fractures (FHFs) surgical management as per Pipkin classification (Type I: Fracture below fovea, Type II: Fracture above fovea, Type III: Type I or II with an associated femoral neck fracture, and Type IV: Type I or II with associated acetabular fracture). * The mentioned approaches could be used for either fragment fixation or excision, ** better to avoid a posterior approach to preserve the blood supply. Abbreviations: ORIF, open reduction and internal fixation; THA, total hip arthroplasty. |
1. For young patients (with a preinjury normal hip joint):
A-Pipkin types I and II fractures, if the hip joint is congruent after reduction and the fragment is anterior or anterolateral, anterior-based approaches (S-P or Hueter) or the W-J approach are advised for excision or ORIF. If the surgeon is familiar with the medial approach or hip arthroscopy, it could be utilized. If the fragment is posteriorly oriented or associated with an irreducible posterior hip dislocation, a posterior-based approach (K-L or SHD) is recommended.
B-Pipkin type III fractures, if successful reduction of the hip was achieved, percutaneous fixation of the femoral neck fracture through a lateral stab incision should be performed first, followed by exposure and fixing FHF, then the same approaches described with Pipkin types I and II could be utilized. Some authors advise against using the K-L with this specific fracture type as it carries a higher risk of femoral head vascular damage.10,11
Tosounidis et al reported having a very low threshold for managing patients presented with Pipkin Type-III through acute THA; however, they will offer ORIF only if there is no evidence of dislocation or a comminuted horizontal femoral neck fracture, they advised performing it as early as possible through SHD then checking the status of posterosuperior retinaculum, which, if it was disrupted, they would convert to THA intraoperatively.3
C-Pipkin type IV fractures, the associated acetabulum fracture, and the possibility of associated intraarticular injury (such as labrum injury) will dictate the approach to be used:
1. If the head fragment is posterior or associated with posterior-oriented acetabulum fracture, or if an impaction injury of the femoral head was suspected preoperatively, a posterior-based approach (K-L or SHD) is preferable.
2. If the major acetabulum involvement was anterior, a dual approach could be used, one approach described previously for fixation of the FHF and another approach such as the anterior ilioinguinal approach or modified Stoppa approach for acetabular fracture fixation.
2. For old age, the decision will depend on the pre-injury status of the hip; if it was healthy with no signs of arthritis, the previous algorithm for the young patient could be applied. If the hip appeared diseased or in type II and III fractures (according to some authors3,11), an acute THA should be performed, and the approach will be according to the surgeon’s preference (Anterior or lateral, or posterior).
Conclusion
Most of the approaches to the hip could be utilized for femoral head fracture management; however, the surgeon should base his choice of the most appropriate approach according to fracture classification and the presence of associated injuries, though the familiarity of the surgeon with a particular approach could not be overlooked.
Abbreviations
FHFs, femoral head fractures; ORIF, open reduction and internal fixation; THA, total hip arthroplasty; SHD, surgical hip dislocation; S-P, Smith‑Petersen; ASIS, anterior superior iliac spine; TFL, tensor fascia latae; LFCA, lateral femoral circumflex artery; AVN, avascular necrosis; HO, heterotopic ossification; K-L, Kocher-Langenbeck; TFO, trochanteric flip osteotomy; MFCA, medial femoral circumflex artery; W-J, Watson-Jones; DVT, deep venous thrombosis; IA, inferior anterior; IP, inferior posterior.
Consent for Publication
The authors declare that the images are entirely unidentifiable and there are no details on the individuals reported in the published version.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval for the version to be published, agreed to the submitted journal, and agreed to be accountable for all aspects of the work.
Funding
No funding was received for this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Epstein HC, Wiss DA, Cozen L. Posterior fracture dislocation of the hip with fractures of the femoral head. Clin Orthop Relat Res. 1985;201:9–17.
2. Henle P, Kloen P, Siebenrock KA. Femoral head injuries: which treatment strategy can be recommended? Injury. 2007;38(4):478–488. doi:10.1016/j.injury.2007.01.023
3. Tosounidis T, Aderinto J, Giannoudis PV. Pipkin Type-III fractures of the femoral head: fix it or replace it? Injury. 2017;48(11):2375–2378. doi:10.1016/j.injury.2017.10.002
4. Johal H, Axelrod D, Bhandari M. Femoral Head Fractures. In: Giannoudis PV, editor. Fracture Reduction and Fixation Techniques. Springer International Publishing; 2020:183–191.
5. Pipkin G. Treatment of grade IV fracture-dislocation of the hip. J Bone Joint Surg Am. 1957;39-A(5):1027–42 passim. doi:10.2106/00004623-195739050-00004
6. Chiron P, Lafontan V, Reina N. Fracture-dislocations of the femoral head. Orthop Traumatol Surg Res. 2013;99(1 Suppl):S53–66. doi:10.1016/j.otsr.2012.11.007
7. Muller ME, Nazarian S. [Classification of fractures of the femur and its use in the A.O. index (author’s transl)]. Classification et documentation AO des fractures du femur. Rev Chir Orthop Reparatrice Appar Mot. 1981;67(3):297–309.
8. Brumback RJ, Kenzora JE, Levitt LE, Burgess AR, Poka A. Fractures of the femoral head. Hip. 1987;15:181–206.
9. Yoon PW, Jeong HS, Yoo JJ, Koo KH, Yoon KS, Kim HJ. Femoral head fracture without dislocation by low-energy trauma in a young adult. Clin Orthop Surg. 2011;3(4):336–341. doi:10.4055/cios.2011.3.4.336
10. Giannoudis PV, Kontakis G, Christoforakis Z, Akula M, Tosounidis T, Koutras C. Management, complications and clinical results of femoral head fractures. Injury. 2009;40(12):1245–1251. doi:10.1016/j.injury.2009.10.024
11. Giordano V, Giordano M, Gloria RC, et al. General principles for treatment of femoral head fractures. J Clin Orthop Trauma. 2019;10(1):155–160. doi:10.1016/j.jcot.2017.07.013
12. Hoppenfeld S, DeBoer P, Buckley R. Surgical Exposures in Orthopaedics: The Anatomic Approach. Lippincott Williams & Wilkins; 2012.
13. Lansford T, Munns SW. Arthroscopic treatment of Pipkin type I femoral head fractures: a report of 2 cases. J Orthop Trauma. 2012;26(7):e94–6. doi:10.1097/BOT.0b013e3182323f4f
14. Park MS, Yoon SJ, Choi SM. Arthroscopic reduction and internal fixation of femoral head fractures. J Orthop Trauma. 2014;28(7):e164–8. doi:10.1097/BOT.0000000000000048
15. Harty M, Joyce JJ. Surgical approaches to the hip and femur. JBJS. 1963;45(1):175–190. doi:10.2106/00004623-196345010-00019
16. Rathi RA, Khan T. Surgical approaches to the hip joint. Orthop Trauma. 2015;29(6):374–383. doi:10.1016/j.mporth.2015.10.005
17. Onyemaechi N, Anyanwu E, Obikili E, Ekezie J. Anatomical basis for surgical approaches to the hip. Ann Med Health Sci Res. 2014;4(4):487–494. doi:10.4103/2141-9248.139278
18. Hueter C. Fünfte abtheilung: die verletzung und krankheiten des hüftgelenkes, neunundzwanzigstes capitel [Fifth section: the injury and diseases of the hip joint, twenty-ninth chapter]. In: Grundriss der chirurgie [Outline of surgery]. Vol. 2, 1883:129–200. German.
19. Smith-Petersen MN. Approach to and exposure of the hip joint for mold arthroplasty. J Bone Joint Surg Am. 1949;31A(1):40–46. doi:10.2106/00004623-194931010-00003
20. Scolaro JA, Marecek G, Firoozabadi R, Krieg JC, Routt MLC. Management and radiographic outcomes of femoral head fractures. J Orthop Traumatol. 2017;18(3):235–241. doi:10.1007/s10195-017-0445-z
21. Braun BJ, Holstein JH, Pohlemann T. Pipkin Fractures. In: Fractures of the Hip. Springer; 2019:123–137.
22. Swiontkowski MF, Thorpe M, Seiler JG, Hansen ST. Operative management of displaced femoral head fractures: case-matched comparison of anterior versus posterior approaches for Pipkin I and Pipkin II fractures. J Orthop Trauma. 1992;6(4):437–442. doi:10.1097/00005131-199212000-00008
23. Stannard JP, Harris HW, Volgas DA, Alonso JE. Functional outcome of patients with femoral head fractures associated with hip dislocations. Clin Orthop Relat Res. 2000;377:44–56. doi:10.1097/00003086-200008000-00008
24. Wang J, Cai L, Xie L, Chen H, Guo X, Yu K. 3D printing-based Ganz approach for treatment of femoral head fractures: a prospective analysis. J Orthop Surg Res. 2019;14(1):338. doi:10.1186/s13018-019-1383-7
25. Del Core MA, Gross B, Ahn J, Wallace SB, Starr A. Clinical and radiographic outcomes of femoral head fractures associated with traumatic hip dislocations. Strategies Trauma Limb Reconstr. 2019;14(1):6–10. doi:10.5005/jp-journals-10080-1416
26. Dawson J, Fitzpatrick R, Murray D, Carr A. Comparison of measures to assess outcomes in total hip replacement surgery. Qual Health Care. 1996;5(2):81–88. doi:10.1136/qshc.5.2.81
27. Gibson A. Posterior exposure of the hip joint. J Bone Joint Surg Br. 1950;32-B(2):183–186. doi:10.1302/0301-620X.32B2.183
28. Marcy GH, Fletcher RS. Modification of the posterolateral approach to the hip for insertion of femoral-head prosthesis. J Bone Joint Surg Am. 1954;36-A(1):142–143. doi:10.2106/00004623-195436010-00021
29. Osborne R. The approach to the hip‐joint: a critical review and a suggested new route. Br J Surg. 1930;18(69):49–52. doi:10.1002/bjs.1800186907
30. Rana R, Verma D
31. Kelley LL, Petersen C. Sectional Anatomy for Imaging Professionals-E-Book. Elsevier Health Sciences; 2018.
32. Roeder LF
33. Ganz R, Gill TJ, Gautier E, Ganz K, Krugel N, Berlemann U. Surgical dislocation of the adult hip a technique with full access to the femoral head and acetabulum without the risk of avascular necrosis. J Bone Joint Surg Br. 2001;83(8):1119–1124. doi:10.1302/0301-620x.83b8.11964
34. Khalifa AA, Haridy MA, Fergany A. Safety and efficacy of surgical hip dislocation in managing femoral head fractures: a systematic review and meta-analysis. World J Orthop. 2021;12(8):604–619. doi:10.5312/wjo.v12.i8.604
35. Keel M, Eid K, Isler B, Trentz O, Ertel W. The role of surgical hip dislocation in the treatment of acetabular and femoral head fractures. Eur J Trauma. 2005;31(2):138–147. doi:10.1007/s00068-005-1403-7
36. Notzli HP, Siebenrock KA, Hempfing A, Ramseier LE, Ganz R. Perfusion of the femoral head during surgical dislocation of the hip. Monitoring by laser Doppler flowmetry. J Bone Joint Surg Br. 2002;84(2):300–304. doi:10.1302/0301-620x.84b2.12146
37. Mostafa MF, El-Adl W, El-Sayed MA. Operative treatment of displaced Pipkin type I and II femoral head fractures. Arch Orthop Trauma Surg. 2014;134(5):637–644. doi:10.1007/s00402-014-1960-5
38. Peng SH, Wu CC, Yu YH, Lee PC, Chou YC, Yeh WL. Surgical treatment of femoral head fractures. Biomed J. 2020;43(5):451–457. doi:10.1016/j.bj.2019.08.004
39. Ross JR, Schoenecker PL, Clohisy JC. Surgical dislocation of the hip: evolving indications. HSS J. 2013;9(1):60–69. doi:10.1007/s11420-012-9323-7
40. Sink EL, Beaule PE, Sucato D, et al. Multicenter study of complications following surgical dislocation of the hip. J Bone Joint Surg Am. 2011;93(12):1132–1136. doi:10.2106/JBJS.J.00794
41. Watson‐Jones R. Fractures of the neck of the femur. Br J Surg. 1936;23(92):787–808. doi:10.1002/bjs.1800239213
42. Charnley J. Low Friction Arthroplasty of the Hip: Theory and Practice. Springer Science & Business Media; 2012.
43. Harris WH. A new lateral approach to the hip joint. J Bone Joint Surg Am. 1967;49(5):891–898. doi:10.2106/00004623-196749050-00005
44. Muller M. Total Hip Replacement Without Trochanteric Osteotomy. Harris W, ed. St Louis: CV Mosby; 1974:231–237.
45. Muller M, Tohtz S, Dewey M, Springer I, Perka C. Evidence of reduced muscle trauma through a minimally invasive anterolateral approach by means of MRI. Clin Orthop Relat Res. 2010;468(12):3192–3200. doi:10.1007/s11999-010-1378-5
46. Skoldenberg O, Ekman A, Salemyr M, Boden H. Reduced dislocation rate after hip arthroplasty for femoral neck fractures when changing from posterolateral to anterolateral approach. Acta Orthop. 2010;81(5):583–587. doi:10.3109/17453674.2010.519170
47. McFarland B, Osborne G. Approach to the hip: a suggested improvement on Kocher’s method. J Bone Joint Surg Br. 1954;36(3):364–367. doi:10.1302/0301-620X.36B3.364
48. Hardinge K. The direct lateral approach to the hip. J Bone Joint Surg Br. 1982;64(1):17–19. doi:10.1302/0301-620X.64B1.7068713
49. Alecci V, Valente M, Crucil M, Minerva M, Pellegrino CM, Sabbadini DD. Comparison of primary total hip replacements performed with a direct anterior approach versus the standard lateral approach: perioperative findings. J Orthop Traumatol. 2011;12(3):123–129. doi:10.1007/s10195-011-0144-0
50. Charnley J, Ferreiraade S. Transplantation of the greater trochanter in arthroplasty of the hip. J Bone Joint Surg Br. 1964;46(2):191–197. doi:10.1302/0301-620X.46B2.191
51. Harris WH. Extensive exposure of the hip joint. Clin Orthop Relat Res. 1973;91:58–62. doi:10.1097/00003086-197303000-00010
52. Glassman AH, Engh CA, Bobyn JD. A technique of extensile exposure for total hip arthroplasty. J Arthroplasty. 1987;2(1):11–21. doi:10.1016/S0883-5403(87)80026-8
53. Wang ZH, Li KN, Zhao P, Chen ED, Zheng J. In situ reduction and fixation of the anterior medial fenestration approach for femoral head fracture. Orthop Surg. 2019;11(6):1163–1172. doi:10.1111/os.12578
54. Koizumi W, Moriya H, Tsuchiya K, Takeuchi T, Kamegaya M, Akita T. Ludloff’s medial approach for open reduction of congenital dislocation of the hip. A 20-year follow-up. J Bone Joint Surg Br. 1996;78(6):924–929. doi:10.1302/0301-620x78b6.6885
55. Ludloff K. The open reduction of the congenital hip dislocation by an anterior incision. JBJS. 1913;2(3):438–454.
56. Ferguson AB
57. Chiron P, Murgier J, Cavaignac E, Pailhe R, Reina N. Minimally invasive medial hip approach. Orthop Traumatol Surg Res. 2014;100(6):687–689. doi:10.1016/j.otsr.2014.06.009
58. Cavaignac E, Laumond G, Regis P, Murgier J, Reina N, Chiron P. Fixation of a fractured femoral head through a medial hip approach: an original approach to the femoral head. Hip Int. 2015;25(5):488–491. doi:10.5301/hipint.5000248
59. Aprato A, Bertolo F, Bistolfi A, Sabatini L, Massè A. The use of hip arthroscopy in trauma of the hip. In: Fractures of the Hip. Springer; 2019:189–196.
60. Mullis BH, Dahners LE. Hip arthroscopy to remove loose bodies after traumatic dislocation. J Orthop Trauma. 2006;20(1):22–26. doi:10.1097/01.bot.0000188038.66582.ed
61. Niroopan G, de Sa D, MacDonald A, Burrow S, Larson CM, Ayeni OR. Hip arthroscopy in trauma: a systematic review of indications, efficacy, and complications. Arthroscopy. 2016;32(4):692–703 e1. doi:10.1016/j.arthro.2015.12.029
62. Newman JT, Saroki AJ, Philippon MJ. Hip arthroscopy for the management of trauma: a literature review. J Hip Preserv Surg. 2015;2(3):242–248. doi:10.1093/jhps/hnv047
63. Stirma GA, Uliana CS, Valenza WR, Abagge M. Surgical treatment of femoral head fractures through previously controlled hip luxation: four case series and literature review. Rev Bras Ortop. 2018;53(3):337–341. doi:10.1016/j.rboe.2018.03.013
64. Khalifa AA, Refai O, Farouk O, Abdelnasser MK. Management of femoral head fractures through surgical hip dislocation (SHD): a demanding but safe technique. Arch Orthop Trauma Surg. 2021;141(10):1701–1710. doi:10.1007/s00402-020-03666-2
65. Zlotorowicz M, Czubak J, Caban A, Kozinski P, Boguslawska-Walecka R. The blood supply to the femoral head after posterior fracture/dislocation of the hip, assessed by CT angiography. Bone Joint J. 2013;95-B(11):1453–1457. doi:10.1302/0301-620X.95B11.32383
66. Gautier E, Ganz K, Krugel N, Gill T, Ganz R. Anatomy of the medial femoral circumflex artery and its surgical implications. J Bone Joint Surg Br. 2000;82(5):679–683. doi:10.1302/0301-620x.82b5.10426
67. Rego P, Mascarenhas V, Collado D, Coelho A, Barbosa L, Ganz R. Arterial topographic anatomy near the femoral head-neck perforation with surgical relevance. J Bone Joint Surg Am. 2017;99(14):1213–1221. doi:10.2106/JBJS.16.01386
68. Henriques R, Ramalho D, Soares Do Brito J, Rocha P, Spranger A, Almeida P. Management of pipkin fractures using a safe surgical hip dislocation. Case Rep Orthop. 2019;2019:3526018. doi:10.1155/2019/3526018
69. Abdelazeem A, Fahmy M, Abdelazeem H. Modified Ludloff’s medial approach for management of Pipkin’s type I femoral head fracture. Int Orthop. 2021;45(6):1591–1598. doi:10.1007/s00264-020-04667-x
70. Aprato A, Buzzone M, Di Benedetto P, Massè A. Surgical hip dislocation vs arthroscopy for fixation of subfoveal femoral head fractures: a new technique for Pipkin type 1 fractures. Acta Biomed. 2021;92(S3):e2021016. doi:10.23750/abm.v92iS3.11724
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.