Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Surgeons Knowledge, Attitude, and Practice Toward Preoperative Inflammatory Bowel Disease Medications and Post-Operative Complications
Authors Alhassan N, Alnwdel AN, Beyari MB ![]() , Aldeligan SH
, Aldeligan SH ![]() , Alhassan R, Abdulla MH, Bin Traiki T
, Alhassan R, Abdulla MH, Bin Traiki T
Received 18 March 2025
Accepted for publication 13 July 2025
Published 22 July 2025 Volume 2025:21 Pages 1149—1159
DOI https://doi.org/10.2147/TCRM.S527037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Noura Alhassan,1 Abdullah Nasser Alnwdel,2 Mohammed Basem Beyari,3 Saleh Husam Aldeligan,3 Reem Alhassan,4 Maha Hamadien Abdulla,1 Thamer Bin Traiki1
1Colorectal Research Chair, Department of Surgery, College of Medicine, King Khalid University Hospital, King Saud University, Riyadh, Saudi Arabia; 2Colorectal Surgery, Department of Surgery, King Fahad Specialist Hospital, Buraydah, Saudi Arabia; 3College of Medicine, King Saud University, Riyadh, Saudi Arabia; 4Pharmacy Department, Prince Sultan Military Medical City, Riyadh, Saudi Arabia
Correspondence: Mohammed Basem Beyari, Email [email protected]
Background: Biologics, particularly anti-TNF agents, have transformed the management of inflammatory bowel disease (IBD), but concerns about their perioperative safety persist.
Objective: This study evaluates the knowledge, attitudes, and practices of surgeons in Saudi Arabia regarding the preoperative management of IBD patients undergoing surgery while on biological treatments.
Methods: A cross-sectional survey was conducted among 115 surgeons. Participants included general and colorectal surgeons with extensive experience in IBD management. Data were analyzed to assess knowledge, attitudes, and practices related to the impact of biologics, corticosteroids, and immunomodulators on wound healing and postoperative complications.
Results: The response rate of 67.8% and Most surgeons (74.4%) believed biologics negatively affect wound healing, despite evidence suggesting their safety. Corticosteroids were unanimously recognized for their adverse effects, while immunomodulators were widely perceived as safe. A majority preferred tapering biologics and corticosteroids 4 weeks preoperatively but continued immunomodulators. Differences between specialties were observed, with colorectal surgeons demonstrating greater adherence to evidence-based guidelines compared to general surgeons, who expressed more concerns about biologics’ risks.
Conclusion: This study identifies a persistent gap between evidence and practice in the perioperative management of IBD patients on biologics among Saudi surgeons, with general surgeons often stopping biologics due to safety concerns despite evidence of their safety, while colorectal surgeons are more likely to follow current guidelines. Unnecessary cessation may increase disease flare risk, highlighting the need for targeted education and multidisciplinary collaboration to optimize surgical outcomes.
Keywords: inflammatory bowel disease, biologics, corticosteroids, immunomodulators, surgical outcomes
Introduction
Inflammatory bowel disease (IBD), encompassing Crohn’s disease (CD) and ulcerative colitis (UC), is a chronic and debilitating condition with an increasing global incidence.1 The global surge in IBD is closely linked to the spread of Westernized lifestyles, urbanization, environmental exposures, and microbiome changes, with industrializing regions now experiencing the same trends previously seen in Western countries.2,3 Approximately 10% of UC patients still require colectomy within five years of diagnosis despite advancements in medical management.4 The therapeutic approach for UC patients requiring colectomy should be individualized based on disease severity, patient characteristics, and surgical urgency. Key success factors include appropriate timing of surgery, preoperative optimization, utilization of minimally invasive techniques when feasible, staged surgical approaches for high-risk patients, and comprehensive multidisciplinary care. The combination of these approaches, particularly when enhanced recovery protocols are implemented, provides the best outcomes for UC patients requiring surgical intervention.5–7 The introduction of anti-TNF-α biologics like infliximab has revolutionized IBD treatment by targeting tumor necrosis factor-alpha (TNF-α), a key proinflammatory cytokine.8 Infliximab, a monoclonal antibody and cornerstone of biologic therapy, binds both soluble and transmembrane TNF-α, inducing apoptosis in inflammatory cells through caspase-dependent mechanisms. It has demonstrated efficacy in both induction and maintenance of remission for Crohn’s disease (CD) and ulcerative colitis (UC), with clinical responses observed within 8–9 days for CD and weeks for UC, Remission rates reach 39% in UC and 45% in CD by week 30 in some studies.9 Despite these benefits, a significant proportion of IBD patients still require surgical intervention, initially raising concerns about perioperative safety of biologics.10 Anti-TNF biologics do not universally eliminate surgery particularly in UC, where colectomy rates remain elevated despite treatment, and some studies associate anti-TNF use with higher colectomy risk compared to no treatment.11 Perioperative use of biologics has not been consistently shown to increase postoperative complications in most studies, though guidelines vary and some data suggest caution with certain procedures.12 Infliximab provides long term disease control for most IBD patients but necessitates proactive monitoring of drug levels, immunogenicity, and infections. Tailored strategies like combination therapy and therapeutic drug monitoring optimize outcomes while mitigating risks.13 Infliximab works by binding to and neutralizing TNF-α, a key inflammatory cytokine in IBD, which leads to reduced inflammation, induction of immune cell apoptosis, and restoration of immune balance both systemically and in the gut mucosa. This results in decreased immune cell infiltration, improved mucosal healing, and overall suppression of the abnormal immune response in IBD patients. Predictive biomarkers for infliximab response include serum 90K/Mac-2 BP, neutrophil-to-albumin ratio (NAR), C-reactive protein (CRP), and certain genetic markers. Monitoring infliximab trough levels and anti-drug antibodies can also help predict and optimize treatment response.14,15 Corticosteroids, widely used in IBD management, alter the body’s natural metabolism and are linked to poor wound healing and increased infection risk, raising concerns about their impact on surgical outcomes.16–18 Long term corticosteroid use in IBD patients disrupts the body’s natural metabolism by increasing muscle breakdown, reducing bone density (leading to osteoporosis), raising blood sugar and cholesterol levels, and suppressing the immune system, which increases infection risk and delays wound healing. Steroids also heighten the risk of blood clots and cardiovascular problems. Because of these significant side effects, guidelines recommend minimizing long-term steroid use in favor of safer, steroid-sparing therapies whenever possible.19–21 Similarly, immunomodulators such as azathioprine are used as adjunct therapies in IBD but carry potential risks, including bone marrow suppression and increased cancer risk.22 When combined with biologic drugs like infliximab, azathioprine reduces the formation of anti-drug antibodies and increases drug availability, leading to higher remission rates.23 Researches have shown that combination therapy with infliximab and thiopurines enhances remission rates by reducing immunogenicity and improving drug availability.24,[25 This study aims to evaluate the knowledge, attitudes, and practices of surgeons in Saudi Arabia regarding the management of IBD patients undergoing surgery while on biologic, corticosteroid, or immunomodulator therapy, particularly in light of the absence of prior studies in the literature on this topic. By identifying gaps in understanding and adherence to best practice evidence, the study seeks to provide insights for optimizing preoperative management strategies.
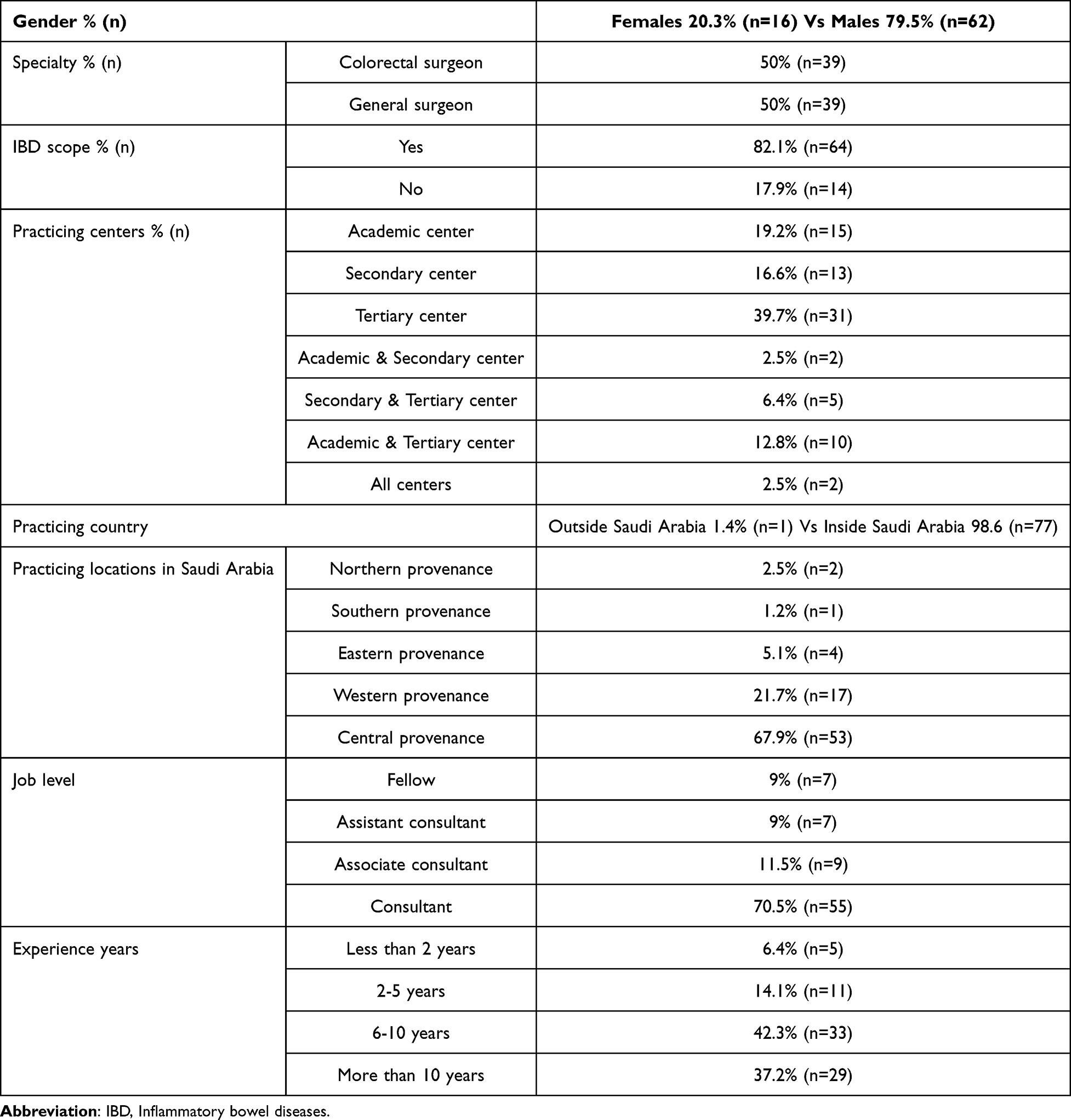 |
Table 1 Population Demographics and years of Experience |
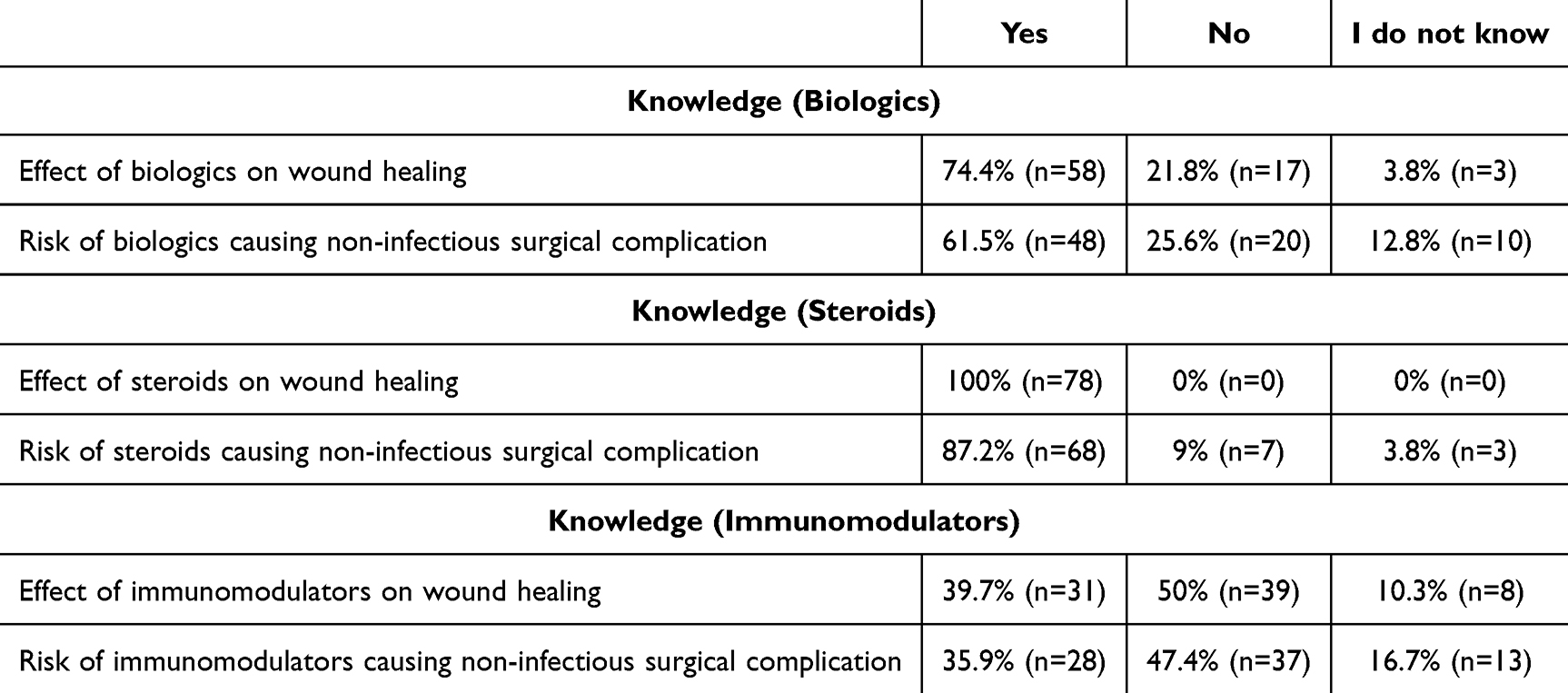 |
Table 2 Knowledge Assessment for Steroids, Biologics and Immunomodulators Usage in IBD Patients by Surgeons |
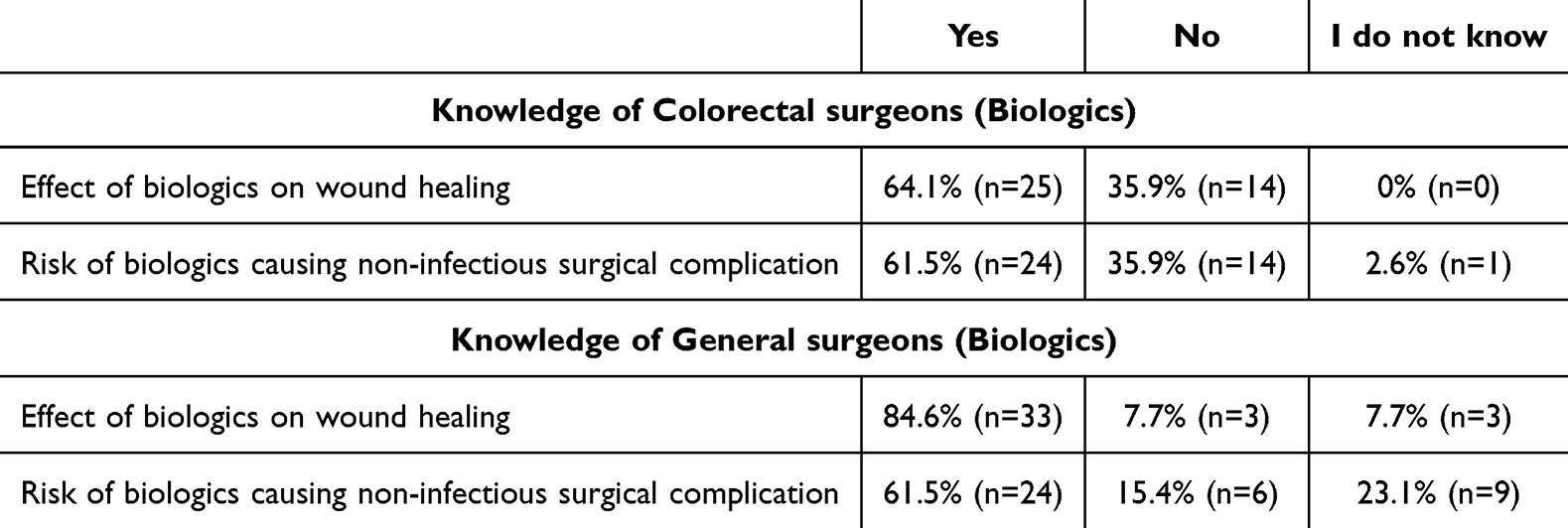 |
Table 3 Knowledge Assessment for Steroids, Biologics and Immunomodulators Usage in IBD Patients in Comparison Between Colorectal Surgeons and General Surgeons |
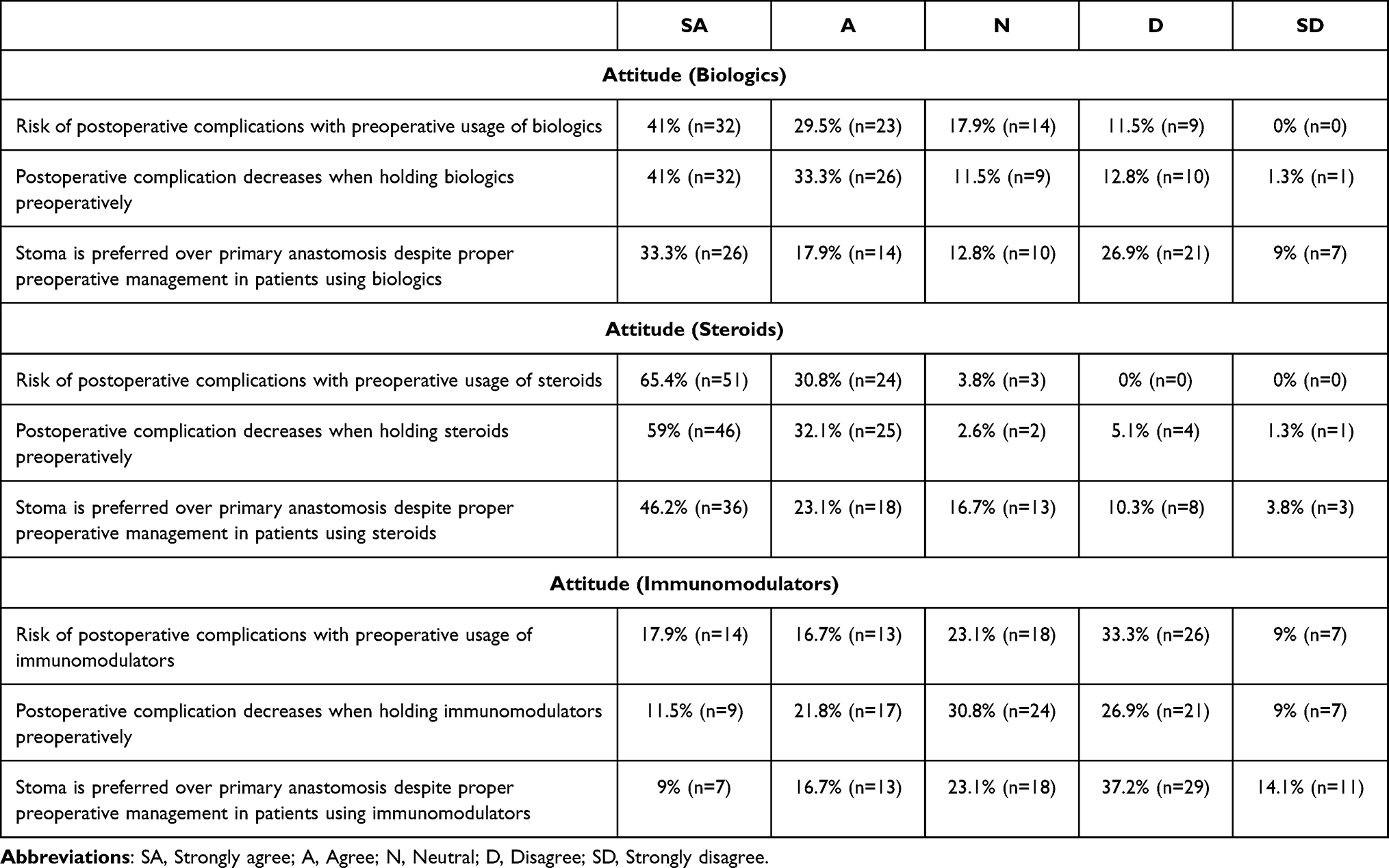 |
Table 4 Attitudes Assessment for Steroids, Biologics and Immunomodulators Usage in IBD Patients by Surgeons |
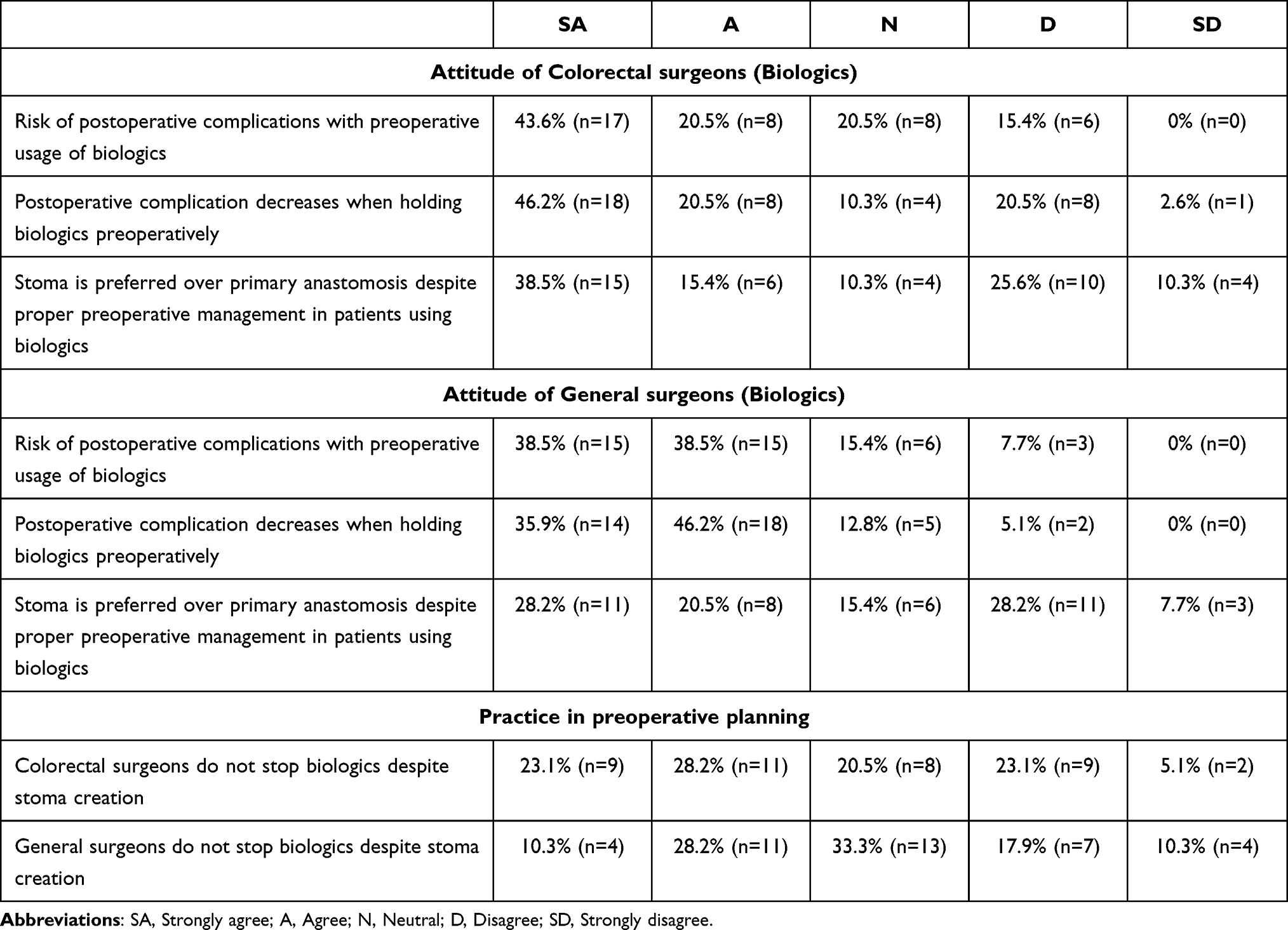 |
Table 5 Attitudes Assessment for Steroids, Biologics and Immunomodulators Usage in IBD Patients in Comparison Between Colorectal Surgeons and General Surgeons |
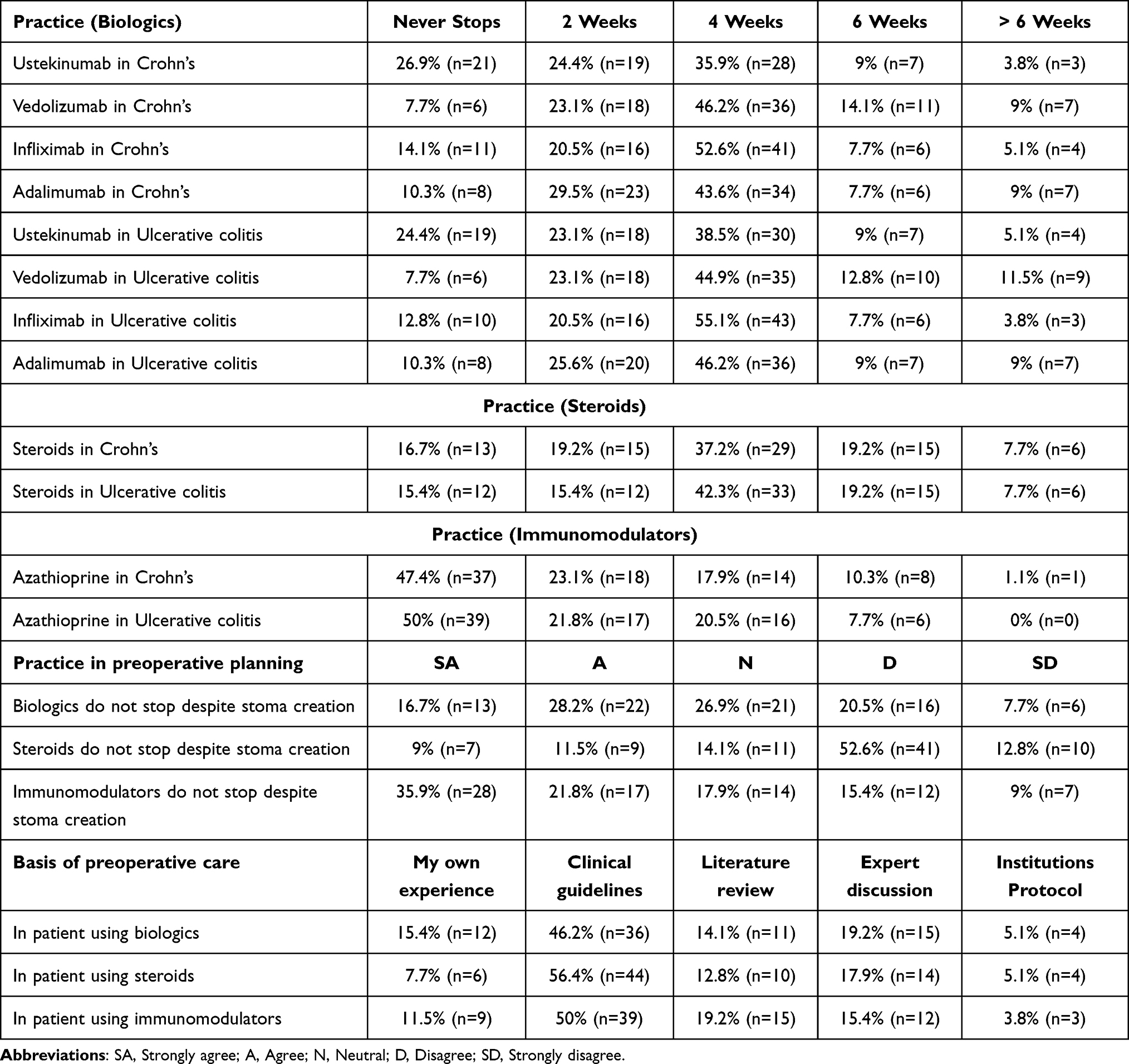 |
Table 6 Practices Assessment for Steroids, Biologics and Immunomodulators Usage in IBD Patients by Surgeons |
Methodology
This is a cross-sectional study assessed the knowledge, attitudes, and practices of both general and colorectal surgeons in Saudi Arabia regarding the management of IBD patients undergoing surgical intervention while on biological treatments, immunomodulators, or steroids, using a questionnaire developed with input from three academic colorectal consultants at King Saud University Medical City, Riyadh, and distributed from January to September 2024. The survey, which included four sections sociodemographic information (such as gender, specialty, hospital type, job title, years of experience, and scope of practice), knowledge about the use of biologics, immunomodulators, and steroids in conjunction with surgery, attitudes toward preoperative cessation of these medications, and practices regarding their cessation prior to surgery was administered via a snowballing technique, with consultants sharing the questionnaire among their professional networks and participants providing informed consent after Institutional Review Board (IRB) approval (Ref. No. E-24-9285); those who declined did not complete the questionnaire, and data were analyzed using JASP software (Version 0.19.0) with descriptive statistics. The study revealed that surgeons face several challenges, including uncertainty about the true perioperative risks of biologics due to conflicting evidence, lack of consensus on when to stop biologics before surgery, and the need for close coordination with gastroenterologists, as well as increased risks for patients on both steroids and biologics, higher complication rates in Crohn’s disease, and the necessity to adapt surgical approaches based on case complexity. Additionally, findings showed that surgeons’ knowledge, attitudes, and behaviors vary by specialty and hospital setting, with colorectal surgeons and those in academic centers generally being more knowledgeable, up-to-date, and likely to continue biologics perioperatively while routinely collaborating with gastroenterologists, whereas general surgeons and those in community hospitals are more cautious, often stopping biologics before surgery due to outdated risk perceptions and less access to multidisciplinary teams or current guidelines.8,26 These differences underscore the importance of targeted education and standardized protocols to optimize the safe and effective use of biologics across all surgical settings.
Results
The survey was sent to 115 participants, and 78 completed the questionnaire, yielding a 67.8% response rate. Among the participants, 79.5% (n=62) were male, with an equal distribution of specialties: 50% (n=39) were general surgeons, and 50% (n=39) were specialized colorectal surgeons. A majority (82.1%, n=64) reported that their main surgical scope included IBD, with colorectal surgeons comprising 59.4% (n=38) of this group. Regarding workplace settings, 39.7% (n=31) worked in tertiary centers, 19.2% (n=15) in academic centers, 16.6% (n=13) in secondary centers. Geographically, 67.9% (n=53) of participants were from the central region, 21.7% (n=17) from the western region, and less than 5% from other regions. In terms of job titles, 70.5% (n=55) were consultants, with 75.0% (n=48) of these having IBD within their scope of practice. Participants had varying years of experience, with 42.3% (n=33) having 6–10 years and 37.2% (n=29) more than 10 years of experience (Table 1).
In the knowledge assessment, 74.4% (n=58) of participants agreed that biologics negatively affect wound healing, while 100% (n=78) believed that corticosteroids have adverse effects on wound healing. Opinions on immunomodulators were divided, with 50% (n=39) disagreeing that they negatively affect wound healing. A statistically significant difference (p=0.0037) was found between colorectal and general surgeons, with general surgeons more likely to agree that biologics negatively affect wound healing. Regarding postoperative complications, 61.5% (n=48) agreed that biologics increase the risk of non-infectious complications, while 87.2% (n=68) reported the same for corticosteroids. A significant difference (p=0.0082) was observed between colorectal and general surgeons on the knowledge of postoperative risks associated with biologics, with more general surgeons expressing unawareness of the correct answer. Responses about immunomodulators showed that 35.9% (n=28) believed they do not pose such risks, and 16.7% (n=13) were uncertain (Tables 2 and 3).
Participants’ attitudes and practices toward preoperative management varied across biologics, corticosteroids, and immunomodulators. Regarding biologics, 41% (n=32) strongly agreed and 29.5% (n=23) agreed that their preoperative use increases the risk of complications. In practice, 52.6% (n=41) of participants reported ceasing biologics four weeks prior to surgery, irrespective of the type of IBD or biologic used. For corticosteroids, 65.4% (n=51) strongly agreed and 30.8% (n=24) agreed that their preoperative use increases the risk of complications, with 42.3% (n=33) of participants ceasing corticosteroids four weeks before surgery. In contrast, attitudes toward immunomodulators were more divided, with 33.3% (n=26) disagreeing and 21.6% (n=16) expressing neutral opinions about their preoperative risks. Reflecting this uncertainty, 47.4% (n=37) of participants continued immunomodulators without cessation. Preferences for stoma creation versus primary anastomosis also varied. For biologics, 41% (n=32) strongly agreed and 33.3% (n=26) agreed that stoma creation is preferable to primary anastomosis, with similar attitudes observed for corticosteroids (46.2%, n=36 strongly agreed and 23.1%, n=18 agreed). Conversely, 37.2% (n=29) of participants disagreed with stoma preference in patients on immunomodulators (Tables 4 and 5).
Across all practices, most participants (46.2%, n=36) indicated that their preoperative planning was guided primarily by clinical guidelines. Subgroup analysis comparing colorectal and general surgeons revealed that 35.9% (n=14) of colorectal surgeons disagreed that biologics negatively affect wound healing, compared to 7.7% (n=3) of general surgeons. When asked about the increased risk of non-infectious complications with biologics, 61.5% (n=24) of both groups agreed, but 23.1% (n=9) of general surgeons expressed uncertainty. Additionally, 51.3% (n=20) of colorectal surgeons reported continuing biologics preoperatively compared to 38.5% (n=15) of general surgeons (Table 6).
Discussion
Biologics, particularly anti-TNF agents like infliximab, have transformed the management of IBD by effectively inducing and maintaining remission in patients with Crohn’s disease (CD) and ulcerative colitis (UC).27,28 Despite robust evidence supporting their safety in the preoperative setting, significant concerns persist among surgeons regarding their impact on postoperative outcomes, including anastomotic leaks, delayed wound healing, and non-infectious complications.29,[30 Furthermore, for elective low-risk surgeries, biologics can typically be continued without interruption. For high-risk or major surgeries, some protocols suggest stopping biologics 1–2 weeks before surgery. After surgery, biologics are usually restarted once good wound healing is confirmed, typically around 10–14 days postoperatively.31 Furthermore, the differences in opinions between general and colorectal surgeons about biologics significantly affect IBD treatment choices and patient outcomes. General surgeons are more likely to stop biologics before surgery due to concerns about infection and healing, leading to higher rates of disease flare, increased steroid use, which itself raises complication risks, and more frequent stoma creation. In contrast, colorectal surgeons, who are more familiar with current evidence, tend to continue biologics perioperatively, use minimally invasive techniques, and collaborate closely with gastroenterologists resulting in fewer complications, better disease control, and improved quality of life for patients.32–34, Our findings highlight a disconnect between emerging evidence and current surgical practices. Most participants in our study believed that biologics negatively affect surgical outcomes, even though recent research demonstrates that preoperative biologic use does not increase the risk of postoperative complications.35,36 This discrepancy underscores the need for targeted education to address misconceptions and promote adherence to updated clinical evidence. The main causes of the gap between evidence and practice in the surgical use of biologics for IBD include outdated perceptions from early studies suggesting increased surgical risks, slow adoption of new evidence, and variability in guideline adherence among clinicians. Many surgeons continue to pause biologics before surgery due to concerns about infections and complications, even though large, recent studies and real world data including the PUCCINI trial and multi institutional analyses show that continuing biologics does not increase postoperative infection or complication rates Additional factors include differences in training, lack of multidisciplinary coordination, and practical concerns like drug costs or insurance restrictions, which can further delay the adoption of evidence-based protocols, addressing these issues through updated education, simplified guidelines, and collaborative care models is necessary to align surgical practice with current research and improve patient outcomes.37–39 When assessing attitudes toward biologics, a majority of participants expressed concerns about increased postoperative risks, with many favoring stoma creations over primary anastomosis in patients on biologics. This preference appears rooted in a cautious approach to mitigate perceived risks of anastomotic leaks, despite studies showing no significant difference in postoperative complication rates between patients who continued biologics and those who did not.40,41 Most surgeons follow that practice of tapering biologics 4 to 6 weeks before surgery, although there is growing evidence that such tapering may not be necessary in all cases.42 Differences between general and colorectal surgeons further emphasize the gap in knowledge and application of evidence. General surgeons were more likely to believe that biologics negatively impact surgical outcomes, with 84.6% (n=33) agreeing on their adverse effects on wound healing compared to 64.1% (n=25) of colorectal surgeons. Colorectal surgeons, who frequently manage complex IBD cases, demonstrated greater familiarity with current evidence and were more likely to continue biologics preoperatively in their practices. This difference likely reflects the specialized exposure and training of colorectal surgeons, enabling them to make evidence-based decisions when managing biologic therapies.43 While immunomodulators were included in the study, their use and associated risks were less of a focal point compared to biologics. Unlike biologics, immunomodulators are widely considered safe in the preoperative setting, with minimal controversy surrounding their impact on surgical outcomes. In contrast, biologics continue to provoke debate, largely due to historical concerns that have not been fully addressed through education and dissemination of updated evidence.44 Both options are considered safe for perioperative use in IBD patients, as neither significantly increases the risk of postoperative infections or surgical complications when used alone. However, biologics are more effective at inducing and maintaining remission, achieving mucosal healing, and preventing disease progression, especially in moderate-to-severe cases. Immunomodulators are valuable for reducing the formation of anti-drug antibodies when combined with biologics, but carry risks of bone marrow suppression and a slightly increased risk of lymphoma. Combination therapy biologic plus immunomodulator is superior to monotherapy for achieving deep remission and maintaining long-term disease control. Overall, both classes are safe preoperatively, but biologics offer greater effectiveness for disease control, while immunomodulators require careful monitoring for hematologic and cancer risks.45–49 The study findings reinforce the importance of clinical guidelines in shaping preoperative management decisions. Most participants cited guidelines as their primary source for planning surgical interventions in patients on biologics. However, the lingering reluctance to use biologics preoperatively suggests that efforts to close the evidence-practice gap requires updated surgical training, robust interdisciplinary communication, and standardized protocols. By fostering collaboration and continuous education, healthcare systems can ensure biologics are managed perioperatively based on current evidence, improving outcomes for IBD patients.50 Future initiatives should focus on providing targeted education and multidisciplinary collaborations to ensure that surgical teams are well-informed about the safety of biologics in the preoperative setting.
Limitations
This study has several limitations. The relatively small sample size of 78 participants may not fully capture the diverse practices and opinions of surgeons across Saudi Arabia, potentially limiting the generalizability of the findings. The reliance on self-reported data introduces the possibility of response bias, as participants may have provided socially desirable answers rather than accurately reflecting their true practices or beliefs. Additionally, the geographic concentration of participants in central regions may not represent practices in less populated or rural areas. The survey’s narrow focus on knowledge and attitudes toward specific medications (biologics, immunomodulators, and corticosteroids) may have overlooked other critical factors influencing surgical decisions, such as patient-specific variables or institutional protocols. Collectively, these limitations affect the study’s ability to present a comprehensive and nationally representative picture of surgeons’ approaches to preoperative IBD medication management and their understanding of postoperative complications.
Conclusion
This study highlights a significant disconnect between current evidence and clinical practices among surgeons in Saudi Arabia regarding the preoperative management of IBD patients on biologic therapies. Our findings demonstrate that, despite robust evidence supporting the perioperative safety of biologics, many surgeons, especially general surgeons remain cautious and often choose to stop biologics prior to surgery due to persistent concerns about wound healing and postoperative complications. In contrast, colorectal surgeons show greater alignment with current guidelines and are more likely to continue biologics perioperatively, reflecting stronger familiarity with evolving evidence and more frequent collaboration with multidisciplinary teams. The widespread practice of tapering biologics and corticosteroids before surgery, while influenced by clinical guidelines, may not always be necessary and could inadvertently increase the risk of disease flare. These results underscore the urgent need for targeted educational initiatives and updated guideline dissemination to address misconceptions and bridge the evidence-practice gap across all surgical specialties. Ultimately, optimizing preoperative strategies through enhanced education and multidisciplinary collaboration will improve surgical outcomes and ensure that IBD patients benefit from the most current and effective perioperative care.
Data Sharing Statement
The data sets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board at the College of Medicine, King Saud University, Ref. No. (E-24-9285). This study was conducted in accordance with the declaration of Helsinki. All participants provided written informed consent prior to the commencement of the study.
Acknowledgment
This work was supported by the ongoing Research Funding program (ORF-2025-344), King Saud University, Riyadh, Saudi Arabia.
Funding
This work was supported by the ongoing Research Funding program (ORF-2025-344), King Saud University, Riyadh, Saudi Arabia.
Disclosure
The authors declare that they have no competing interest in this work.
References
1. Muzammil MA, Fariha F, Patel T, et al. Advancements in inflammatory bowel disease: a narrative review of diagnostics, management, epidemiology, prevalence, patient outcomes, quality of life, and clinical presentation. Cureus. 2023;15(6):e41120. PMID: 37519622; PMCID: PMC10382792. doi:10.7759/cureus.41120
2. Hracs L, Windsor JW, Gorospe J, et al. Global evolution of inflammatory bowel disease across epidemiologic stages. Nature. 2025;642(8067):458–466. doi:10.1038/s41586-025-08940-0
3. Carreras-Torres R, Ibáñez-Sanz G, Obón-Santacana M, et al. Identifying environmental risk factors for inflammatory bowel diseases: a Mendelian randomization study. Sci Rep. 2020;10(1):19273. doi:10.1038/s41598-020-76361-2
4. Zhang YZ, Li YY. Inflammatory bowel disease: pathogenesis. World J Gastroenterol. 2014;20(1):91–99. PMID: 24415861; PMCID: PMC3886036. doi:10.3748/wjg.v20.i1.91
5. Kuehn F, Hodin RA. Impact of modern drug therapy on surgery: ulcerative colitis. Visc Med. 2018;34(6):426–431. Epub 2018 Oct 31. PMID: 30675487; PMCID: PMC6341373. doi:10.1159/000493492
6. Stoner PL, Kamel A, Ayoub F, et al. Perioperative care of patients with inflammatory bowel disease: focus on nutritional support. Gastroenterol Res Pract. 2018;2018:7890161. PMID: 30344603; PMCID: PMC6174741. doi:10.1155/2018/7890161
7. Kotze PG. The essential role of a multidisciplinary approach in inflammatory bowel diseases. Clin Colon Rectal Surg. 2022;35(1):3–4. PMID: 35069024; PMCID: PMC8763457. doi:10.1055/s-0041-1740034
8. Schnitzler F, Tillack-Schreiber C, Szokodi D, et al. Safety of perioperative treatment with biologics in patients with inflammatory bowel disease undergoing bowel surgery: experience from a large urban center. PLoS One. 2024;19(1):e0290887. PMID: 38236926; PMCID: PMC10796016. doi:10.1371/journal.pone.0290887
9. Mohagheghi Darehranj S, Alatab S, Vahedi H, et al. Efficacy of anti-TNF therapy for the treatment of patients with moderate-to-severe inflammatory bowel disease; a first Iranian report. Middle East J Dig Dis. 2020;12(1):12–18. PMID: 32082516; PMCID: PMC7023648. doi:10.15171/mejdd.2020.158
10. Chinyu S, Salzberg BA, Lewis JD, et al. Efficacy of anti-tumor necrosis factor therapy in patients with ulcerative colitis. Am J Gastroenterol. 2002;97(10,2002):2577–2584,ISSN0002–9270. doi:10.1016/S0002-9270(02)04384-8
11. Lima CCG, Queiroz NSF, Sobrado CW, Silva GLR, Nahas SC. Recent advances in the management of inflammatory bowel disease: the role of anti-TNF agents in the era of new biologics. Arquivos de Gastroenterologia. 2020;57(3):323–334. doi:10.1590/S0004-2803.202000000-59
12. Kulaylat AS, Kulaylat AN, Schaefer EW, et al. Association of preoperative anti-tumor necrosis factor therapy with adverse postoperative outcomes in patients undergoing abdominal surgery for ulcerative colitis. JAMA Surg. 2017;152(8):e171538. Epub 2017 Aug 16. PMID: 28614561; PMCID: PMC5831468. doi:10.1001/jamasurg.2017.1538
13. Schnitzler F, Fidder H, Ferrante M, et al. Long-term outcome of treatment with infliximab in 614 patients with Crohn’s disease: results from a single-centre cohort. Gut. 2009;58:492–500. doi:10.1136/gut.2008.155812
14. Fidder H, Schnitzler F, Ferrante M, et al. Long-term safety of infliximab for the treatment of inflammatory bowel disease: a single-centre cohort study. Gut. 2009;58(4):501–508. Epub 2008 Oct 2. PMID: 18832524. doi:10.1136/gut.2008.163642
15. Kaddoura R, Ghelani H, Alqutami F, Altaher H, Hachim M, Jan RK. Identification of specific biomarkers and pathways in the treatment response of infliximab for inflammatory bowel disease: in-silico analysis. Life. 2023;13(3):680. PMID: 36983834; PMCID: PMC10057676. doi:10.3390/life13030680
16. Lichtenstein GR, Hanauer SB, Sandborn WJ. Preoperative steroid use and risk of postoperative complications in patients with inflammatory bowel disease undergoing abdominal surgery. Am J Gastroenterol. 2008;103(6):1394–1401. doi:10.1111/j.1572-0241.2008.01942.x
17. Nunes T, Acosta MB-D, Marin-Jiménez I, Nos P, Sans M. Oral locally active steroids in inflammatory bowel disease. J Crohn’s Colitis. 2013;7(3):183–191. doi:10.1016/j.crohns.2012.06.010
18. Nguyen GC, Elnahas A, Jackson TD. the impact of preoperative steroid use on short-term outcomes following surgery for inflammatory bowel disease. J Crohn’s Colitis. 2014;8(12):1661–1667. doi:10.1016/j.crohns.2014.07.007
19. Bradford Rice J, White AG, Scarpati LM, Wan G, Nelson WW et al . Long-term Systemic Corticosteroid Exposure: A Systematic Literature Review. Clinical therapeutics. 2017;39(11):2216–2229. doi:10.1016/j.clinthera.2017.09.011
20. Barrett K, Saxena S, Pollok R. Using corticosteroids appropriately in inflammatory bowel disease: a guide for primary care. Br J Gen Pract. 8;68(675):497–498. doi:10.3399/bjgp18X699341
21. European Crohn’s and Colitis Organisation (ECCO) Guidelines; 2024.
22. Dubinsky MC. Azathioprine, 6-mercaptopurine in inflammatory bowel disease: pharmacology, efficacy, and safety. Clin Gastroenterol Hepatol. 2004;2(9):731–743. PMID: 15354273. doi:10.1016/s1542-3565(04)00344-1
23. Qu YT, Ding JY, Pan W, Liu FR, Dong AL. Perspectives in clinical research on Azathioprine for steroid-dependent ulcerative colitis. Front Med. 2025;12:1551906. PMID: 40201324; PMCID: PMC11975918. doi:10.3389/fmed.2025.1551906
24. Pasternak B, Svanström H, Schmiegelow K, Jess T, Hviid A. Use of azathioprine and the risk of cancer in inflammatory bowel disease. American Journal of Epidemiology. 2013;177(11):1296–1305. doi:10.1093/aje/kws375
25. Privitera G, Pugliese D, Onali S, et al. Combination therapy in inflammatory bowel disease - from traditional immunosuppressors towards the new paradigm of dual targeted therapy. Autoimmun Rev. 2021;20(6):102832. Epub 2021 Apr 15. PMID: 33866066. doi:10.1016/j.autrev.2021.102832
26. Nones RB, Fleshner PR, Queiroz NSF, et al. Therapeutic drug monitoring of biologics in IBD: essentials for the surgical patient. J Clin Med. 2021;10(23):5642. PMID: 34884344; PMCI. doi:10.3390/jcm10235642
27. Vyas KS, Vasconez HC. Wound healing: biologics, skin substitutes, biomembranes and scaffolds. Healthcare. 2014;2(3):356–400. PMID: 27429283; PMCID: PMC4934597. doi:10.3390/healthcare2030356
28. Ardizzone S, Cassinotti A, Manes G, Porro GB. Immunomodulators for all patients with inflammatory bowel disease? Therap Adv Gastroenterol. 2010;3(1):31–42. PMID: 21180588; PMCID: PMC3002564. doi:10.1177/1756283X09354136
29. Jeganathan NNA, Koltun WA. Special considerations of anastomotic leaks in crohn’s disease. Clin Colon Rectal Surg. 2021;34(6):412–416. PMID: 34853563; PMCID: PMC8610635. doi:10.1055/s-0041-1735273
30. Rumer KK, Dehghan MS, Sceats LA, Trickey AW, Morris AM, Kin C. Use of biological medications does not increase postoperative complications among patients with ulcerative colitis undergoing colectomy: a retrospective cohort analysis of privately insured patients. Dis Colon Rectum. 2020;63(11):1524–1533. PMID: 33044293; PMCID: PMC8034550. doi:10.1097/DCR.0000000000001684
31. Lightner AL, Vogel JD, Carmichael JC, et al. The American Society of Colon and Rectal Surgeons clinical practice guidelines for the surgical management of crohn’s disease. Dis Colon Rectum. 2020;63(8):1028–1052. PMID: 32692069. doi:10.1097/DCR.0000000000001716
32. Loftus EV
33. Qayed E, Wei B-Z, Wang Y-F, et al. Perioperative management of biologics in IBD: a review. World J Gastrointest Surg. 2024;16(2):196–210. [PMC10796016]. doi:10.4240/wjgs.v16.i1.196
34. Cohen BL, Fleshne P, Kane SV, et al. Prospective cohort study to investigate the safety of preoperative tumor necrosis factor inhibitor exposure in patients with inflammatory bowel disease undergoing intra-abdominal surgery. Gastroenterology. 2022;163(1):204–221. doi:10.1053/j.gastro.2022.03.057
35. Lamb CA, Kennedy NA, Raine T, et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut. 2019;68:s1–s106. doi:10.1136/gutjnl-2019-318484
36. Gasparetto M, Angriman I, Guariso G. The multidisciplinary health care team in the management of stenosis in Crohn’s disease. J Multidiscip Healthc. 2015;8:167–179. PMID: 25878504; PMCID: PMC4388000. doi:10.2147/JMDH.S38729
37. Scott FI, Singh S. Bridging gaps in evidence-based clinical practice in inflammatory bowel diseases: observational comparative effectiveness research for the win. Clin Gastroenterol Hepatol. 2019;17(9):1726–1728. Epub 2019 Jan 7. PMID: 30630101; PMCID: PMC6612465. doi:10.1016/j.cgh.2018.12.047
38. Goss Sawhney T, Dobes A, O’Charoen S. Real-world persistency for inflammatory bowel disease biologics using patient registry data. Crohns Colitis. 2023;3(4):otad051. PMID: 37941597; PMCID: PMC10629214. doi:10.1093/crocol/otad051.
39. Kapizioni C, Desoki R, Lam D, et al. Biologic therapy for inflammatory bowel disease: real-world comparative effectiveness and impact of drug sequencing in 13 222 Patients within the UK IBD BioResource. J Crohn’s Colitis. 2024;18(6):790–800. doi:10.1093/ecco-jcc/jjad203
40. Meeralam YK, Al Zanabgi A, Mosli M, et al. A regional survey of awareness of inflammatory bowel disease among the Saudi population. Inflamm Intest Dis. 2023;7(3–4):139–146. PMID: 37064540; PMCID: PMC10091000. doi:10.1159/000529318
41. Ismael H, Horst M, Farooq M, Jordon J, Patton JH, Rubinfeld IS. Adverse effects of preoperative steroid use on surgical outcomes. Am J Surg. 2011;201(3):305–8;discussion308–9. PMID: 21367368. doi:10.1016/j.amjsurg.2010.09.018
42. Manrai M, Jha AA, Dawra S, Pachisia AVB. Small molecules and more in inflammatory bowel disease: the present and the future. Future Pharmacol. 2024;4:279–316. doi:10.3390/futurepharmacol4010017
43. Nakase H, Uchino M, Shinzaki S, et al. Evidence-based clinical practice guidelines for inflammatory bowel disease 2020. J Gastroenterol. 2021;56(6):489–526. Epub 2021 Apr 22. PMID: 33885977; PMCID: PMC8137635. doi:10.1007/s00535-021-01784-1
44. Sun Z, Song T, Guo Z, Cao L, Zhu W, Li Y. Biologic use is not associated with postoperative complications in patients with Crohn’s disease undergoing stoma reversion. ANZ J Surg. 2023;93(12):2921–2927. Epub 2023 Dec 1. PMID: 38041216. doi:10.1111/ans.18790
45. Ferrari L, Krane MK, Fichera A. Inflammatory bowel disease surgery in the biologic era. World J Gastrointestinal Surg. 2016;8(5):363–370. doi:10.4240/wjgs.v8.i5.363
46. Hodges P, Adeniyi O, Devani S, et al. Emerging patterns of inflammatory bowel disease in Sub-Saharan Africa: 175 cases from an inflammatory bowel disease network. J Crohn’s Colitis. 2025;19. doi:10.1093/ecco-jcc/jjae126
47. Shehab M, Alfadhli A, Abdullah I, Alostad W, Marei A, Alrashed F. Effectiveness of biologic therapies in achieving treatment targets in inflammatory bowel disease; realworld data from the Middle East (ENROLL study). Front Pharmacol. 2024;15:1388043. doi:10.3389/fphar.2024.1388043
48. Hashash JG, Abou Fadel CG, Rimmani HH, Sharara AI, Mehta JL. Biologic monotherapy versus combination therapy with immunomodulators in the induction and maintenance of remission of Crohn’s disease and ulcerative colitis. Annals Gastroenterol. 2021;34(1):1–13. doi:10.20524/aog.2021.0645
49. Nguyen NH, Singh S, Sandborn WJ, Loftus EV. Positioning therapies in the management of Crohn’s disease. J Gastroenterol Hepatol. 2020;35(1):23–31. doi:10.1111/jgh.14648
50. PMC8007245 (MIS training) | PMC8763454 (MDT coordination) | ECCO 2023 Guidelines | NSQIP Collaborative. (PMC10796016).
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Emerging Therapies for Ulcerative Colitis: Updates from Recent Clinical Trials
AlAmeel T, AlMutairdi A, Al-Bawardy B
Clinical and Experimental Gastroenterology 2023, 16:147-167
Published Date: 17 August 2023
Real-World Maintenance Phase Persistence on Ustekinumab and Adalimumab in Ulcerative Colitis
Zhdanava M, Kachroo S, Shah A, Ding Z, Lefebvre P, Zhao R, Kerner C, Pilon D
Patient Preference and Adherence 2024, 18:809-820
Published Date: 10 April 2024
Advanced Combination Therapy with Biologics and Upadacitinib in Refractory Inflammatory Bowel Disease: A Retrospective Study from Taiwan
Meng MJ, Kuo CJ, Lai MW, Chiu CT, Su MY, Chang ML, Le PH
Journal of Inflammation Research 2025, 18:2733-2742
Published Date: 26 February 2025