Back to Journals » Patient Preference and Adherence » Volume 18
Real-World Maintenance Phase Persistence on Ustekinumab and Adalimumab in Ulcerative Colitis
Authors Zhdanava M, Kachroo S, Shah A, Ding Z, Lefebvre P, Zhao R, Kerner C, Pilon D
Received 21 November 2023
Accepted for publication 9 March 2024
Published 10 April 2024 Volume 2024:18 Pages 809—820
DOI https://doi.org/10.2147/PPA.S446861
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Maryia Zhdanava,1 Sumesh Kachroo,2 Aditi Shah,1 Zhijie Ding,2 Patrick Lefebvre,1 Ruizhi Zhao,2 Caroline Kerner,2 Dominic Pilon1
1Analysis Group, Inc, Montréal, QC, Canada; 2Janssen Scientific Affairs, LLC, Horsham, PA, USA
Correspondence: Maryia Zhdanava, Analysis Group, Inc, 1190 avenue des Canadiens-de-Montréal, Suite 1500, Montréal, QC, H3B 0G7, Canada, Tel +1-514-394-4469, Fax +1-514-394-4461, Email [email protected]
Purpose: To describe real-world persistence in bio-naïve and bio-experienced adults with ulcerative colitis (UC) treated with ustekinumab, a recently approved anti-interleukin 12/23 antibody, or adalimumab, an anti-TNF biologic.
Methods: This is a descriptive, retrospective cohort study. Patients initiating ustekinumab or adalimumab (index date, between 10/21/2019 and 08/13/2021) were selected from the Komodo Health comprehensive dataset and stratified into bio-naïve and bio-experienced subgroups based on biologic use 12 months pre-index date. Endpoints evaluated at 12-months after maintenance phase start using Kaplan–Meier analysis included 1) persistence; 2) persistence while being corticosteroid-free (< 14 consecutive days of corticosteroid supply after day 90 post-index); and, 3) persistence while on monotherapy (no immunomodulators/non-index biologics/advanced therapies).
Results: Ustekinumab cohort included 778 patients (236 bio-naïve, 542 bio-experienced) and adalimumab cohort included 1693 patients (1517 bio-naive, 176 bio-experienced). At 12 months after maintenance phase start, 75.5% and 50.5% of bio-naïve patients persisted on ustekinumab and adalimumab and 72.3% and 56.9% of bio-experienced patients persisted on ustekinumab and adalimumab, respectively. Further, 55.1% and 38.2% of bio-naïve patients were persistent and corticosteroid-free with ustekinumab and adalimumab; 43.7% and 33.4% of bio-experienced patients were persistent and corticosteroid-free with ustekinumab and adalimumab, respectively. Moreover, 68.1% and 44.5% of bio-naïve patients were persistent and on monotherapy with ustekinumab and adalimumab; 61.6% and 47.9% of bio-experienced patients were persistent and on monotherapy with ustekinumab and adalimumab, respectively.
Conclusion: At 12 months after maintenance phase start, patients with UC treated with ustekinumab had numerically higher persistence, including persistence while corticosteroid-free and persistence while on monotherapy, than patients treated with adalimumab.
Keywords: biologics, inflammatory bowel disease, outcomes research
Introduction
Ulcerative colitis (UC) and Crohn’s disease are the two major types of inflammatory bowel disease. Specifically, UC is characterized by chronic autoimmune-mediated inflammation of the colon and rectum.1 In 2016, the prevalence of UC among adults in the United States (US) was estimated to be nearly 500,000 and is steadily increasing.2,3
Although there is no known pharmacological cure for UC, current pharmacological treatments aim to achieve mucosal healing, induce and maintain corticosteroid-free remission, and prevent hospitalization and surgery.4 First-line treatments for moderate-to-severe UC recommended by the American College of Gastroenterology (ACG) and the American Gastroenterological Association (AGA) guidelines include glucocorticoids and biologic agents (with or without immunomodulators).4,5 Once remission is achieved, guidelines recommend maintaining remission with a biologic/advanced therapy agent, while tapering off corticosteroids if used in the initial phase of treatment.4–6
Anti-TNF agents, including adalimumab (approved by the US Food and Drug Administration [FDA] for UC in September 2012), have revolutionized the management of UC in recent decades. The ACG clinical guidelines recommend treatment with anti-TNF agents to induce and maintain remission in patients with moderate-to-severe UC.4 Despite the integral role of anti-TNF agents, 50% of patients with UC do not respond to anti-TNF treatment or lose response over time,7 highlighting the need for alternative therapies to manage UC. The anti-interleukin 12/23 antibody ustekinumab was approved by the FDA in October 2019 based on evidence from the UNIFI clinical trial demonstrating that ustekinumab was more effective than placebo for inducing and maintaining remission in patients with moderate-to-severe UC who had failed conventional or biologic therapy.8,9 In this trial, clinical remission was induced in 18.8% of patients within 16 weeks; among patients achieving remission, 43.8% sustained clinical remission at week 44 while receiving ustekinumab once every 8 weeks.9 Ustekinumab has also been shown to be effective in inducing clinical remission among real-world patients with inflammatory bowel disease, including UC.10,11
In view of the expanding treatment options for UC and lack of head-to-head trials, leveraging real-world data may help to inform optimal positioning of biologics for treatment selection. Further, given the short time interval since FDA approval of ustekinumab, information on treatment patterns among patients with UC in the ustekinumab era is limited. Treatment persistence in the real world is an important measure that reflects the effectiveness and safety of a biologic.12–14 This study describes real-world persistence in both bio-naïve and bio-experienced patients with UC, initiated and reaching maintenance on ustekinumab, the newest approved biologic for UC at the time of this study conduct, or adalimumab, one of the first approved and commonly used biologics for moderate-to-severe UC, which as an anti-TNF agent, is also recommended as first-line treatment by the ACG.
Methods
Data Source
Closed claims data were obtained from the Komodo Health comprehensive dataset (10/01/2015–02/13/2022), a de-identified database containing over 320 million US patients across Medicaid, Commercial and Medicare insurers. Closed claims have the advantage of capturing all medical events and filled prescriptions that occurred during a patient’s health plan enrollment period. The data included patient health plan enrollment information, medical and pharmacy claims (cost information was not available in claims). The Komodo Health database complies with patient confidentiality requirements of the Health Insurance Portability and Accountability Act. Therefore, no institutional review board approval was necessary.
Study Design
A retrospective cohort design with an intent-to-treat approach was used (Figure 1). Patients initiated on ustekinumab or adalimumab between 10/21/2019 and 08/13/2021 (intake period) were classified into the ustekinumab or adalimumab cohort. The intake period aligned with the period in which both treatment options were available on the US market and ensured that patients in both cohorts had an equal amount of time (6 months) to discontinue the index therapy before the end of data availability. The index date was the date of the first observed claim for ustekinumab or adalimumab in the intake period. The two cohorts were not mutually exclusive, ie, patients who initiated ustekinumab or adalimumab on different dates during the intake period could be included in both cohorts.
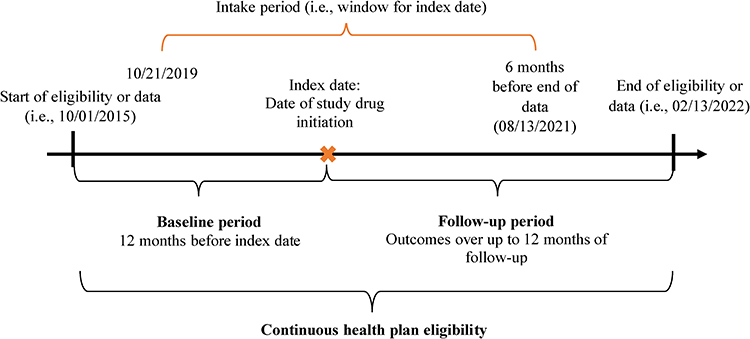 |
Figure 1 Study design scheme. |
The baseline period was the 12-month period with continuous health plan eligibility prior to the index date. The start of maintenance phase was the date of the first subcutaneous claim for ustekinumab and the date of the first claim following a cumulative dose of 240 mg for adalimumab. The follow-up period spanned from the start of maintenance phase to the earliest of 12 months, end of insurance eligibility, or end of data availability.
Study Sample
Patients meeting the following criteria were included in the study sample: (1) first observed claim for ustekinumab or adalimumab (index therapy) during the intake period; (2) ≥12 months of continuous insurance eligibility before the index date; (3) ≥1 medical claim with a diagnosis for UC [International Classification of Diseases, Tenth Revision, Clinical Modification codes [ICD-10-CM]: K51.x] in the baseline period or on the index date; (4) ≥18 years of age on the index date; (5) persistent on index therapy (defined as no gaps in days of supply >120 days for ustekinumab or >60 days for adalimumab) between the index date and maintenance phase start. Patients were excluded from the study if they met any of the following criteria: (1) ≥1 medical or pharmacy claim for the index biologic before the index date during the period of continuous eligibility; (2) ≥1 medical or pharmacy claim for a biologic other than the index biologic on the index date; (3) any medical claim for ankylosing spondylitis, hidradenitis suppurativa, juvenile idiopathic arthritis, plaque psoriasis, psoriatic arthritis, relapsing polychondritis, rheumatoid arthritis, or uveitis during the baseline period; (4) a diagnosis of Crohn’s disease before or after the index date.
Within each cohort, patients were further classified into bio-naïve and bio-experienced subgroups based on the absence or presence of pharmacy/medical claims for UC-indicated biologics or advanced therapy agents (ie, adalimumab, golimumab, infliximab and biosimilars, ozanimod, tofacitinib, upadacitinib, ustekinumab, vedolizumab) during the baseline period.
Outcomes Measures
Per label, ustekinumab has one induction dose as an intravenous infusion (2–4 vials; 260–520 mg depending on weight); the maintenance dose is a subcutaneous dose (90 mg) taken every 8 weeks after induction.15 Adalimumab is administered as subcutaneous injection and has 2 induction doses: 160 mg in one day or two consecutive days and 80 mg in 2 weeks; the maintenance dose of 40 mg starts at week 4 and is administered bi-weekly.16
The primary outcome was persistence on index therapy at 12 months after the start of the maintenance phase. For the ustekinumab cohort, persistence was defined as no gaps in days of supply >120 days, based on twice the duration of the maintenance cycle of 8 weeks (~60 days).8 For the adalimumab cohort, persistence was defined as no gaps in days of supply >60 days, based on twice the mode of days of adalimumab supply in the data (28 days). Although adalimumab has a per-label maintenance cycle of two weeks (~15 days),16 each dispensing of adalimumab typically contains two doses, so each claim is considered to supply the patient for approximately 30 days.
Two composite outcomes of persistence were also examined: (1) persistence while being corticosteroid-free; and (2) persistence while on monotherapy.
Being corticosteroid-free was defined as <14 consecutive days of corticosteroid supply after day 90 post-index. Patients who, based on this definition, were not corticosteroid-free at the start of the maintenance phase were excluded from the analysis of this outcome. The grace period of 90 days post-index was implemented to allow patients to taper off corticosteroids after initiating index therapy (ie, if a patient used corticosteroids between the index date and 90 days, the corticosteroid use was ignored).
Being on monotherapy was defined as no use of immunomodulators, non-index biologics, or advanced therapy agents. Patients who were not on monotherapy between the index date and the start of the maintenance phase were excluded from the analysis of this outcome.
Persistence was measured from the start of the maintenance phase until the discontinuation date (ie, date of the last refill before the exposure gap plus the days of supply of the last refill of the index agent). For composite outcomes, persistence was measured from the start of maintenance phase to the earliest of the discontinuation date, the day before the first of ≥14 consecutive days of corticosteroid supply, or the day before the use of immunomodulators, non-index biologics, or advanced therapy agents. Patients for whom discontinuation, use of corticosteroids with ≥14 days of supply, or use of immunomodulators, non-index biologics, or advanced therapy agents were not observed during the follow-up period were censored on the last day of index therapy supply preceding the end of the follow-up period.
In claims data, persistence is measured based on days of supply for medications, which could be inconsistent with the frequency of administration per label or missing (eg, for medical claims of intravenous ustekinumab). This motivates the need for the imputation of days of supply. The mode of days of supply observed in the data, the mode of time between claims, and the US label frequency of administration were used to derive the rules for the days of supply imputation. For the ustekinumab cohort, starting at the first claim, claims with missing days of supply and pharmacy claims with days of supply <34 days were imputed as 28 days if the gap until the next claim was <38 days, 42 days if the gap was 38 to 46 days, 56 days if the gap was >46 days; if there was no next claim, days of supply of the previous claim were carried forward, or the per label number of days of supply (56 days) was imputed if the original value was missing. For adalimumab, claims with missing days of supply were imputed as 28 days.
Statistical Analysis
Patient baseline characteristics, including demographics, comorbidities, use of UC-related treatments, and healthcare resource use were described with means, medians, and standard deviations (SDs) for continuous variables, and frequencies and proportions for categorical variables.
Kaplan–Meier (KM) survival analysis was used to describe the three persistence outcomes. Rates of persistence were reported at 3, 6, 9 and 12 months after the maintenance phase start and if reached, median persistence time (ie, time by which 50% of patients persist on their index therapy) was also reported.
All analyses were performed in bio-naïve and bio-experienced subgroups of ustekinumab and adalimumab cohorts.
Results
Baseline Characteristics
A total of 2471 patients met inclusion criteria, of which 778 were in the ustekinumab cohort and 1693 in the adalimumab cohort. In the ustekinumab cohort, 30.3% were bio-naïve and 69.7% were bio-experienced, while 89.6% and 10.4% were bio-naïve and bio-experienced in the adalimumab cohort, respectively (Figure 2). During the baseline period, among bio-experienced ustekinumab and adalimumab subgroups, 57.6% and 63.6% used an anti-TNF agent, 44.8% and 31.3% used vedolizumab, and 17.2% and 6.8% used tofacitinib, respectively; additionally, 6.8% of adalimumab patients used ustekinumab (Table 1).
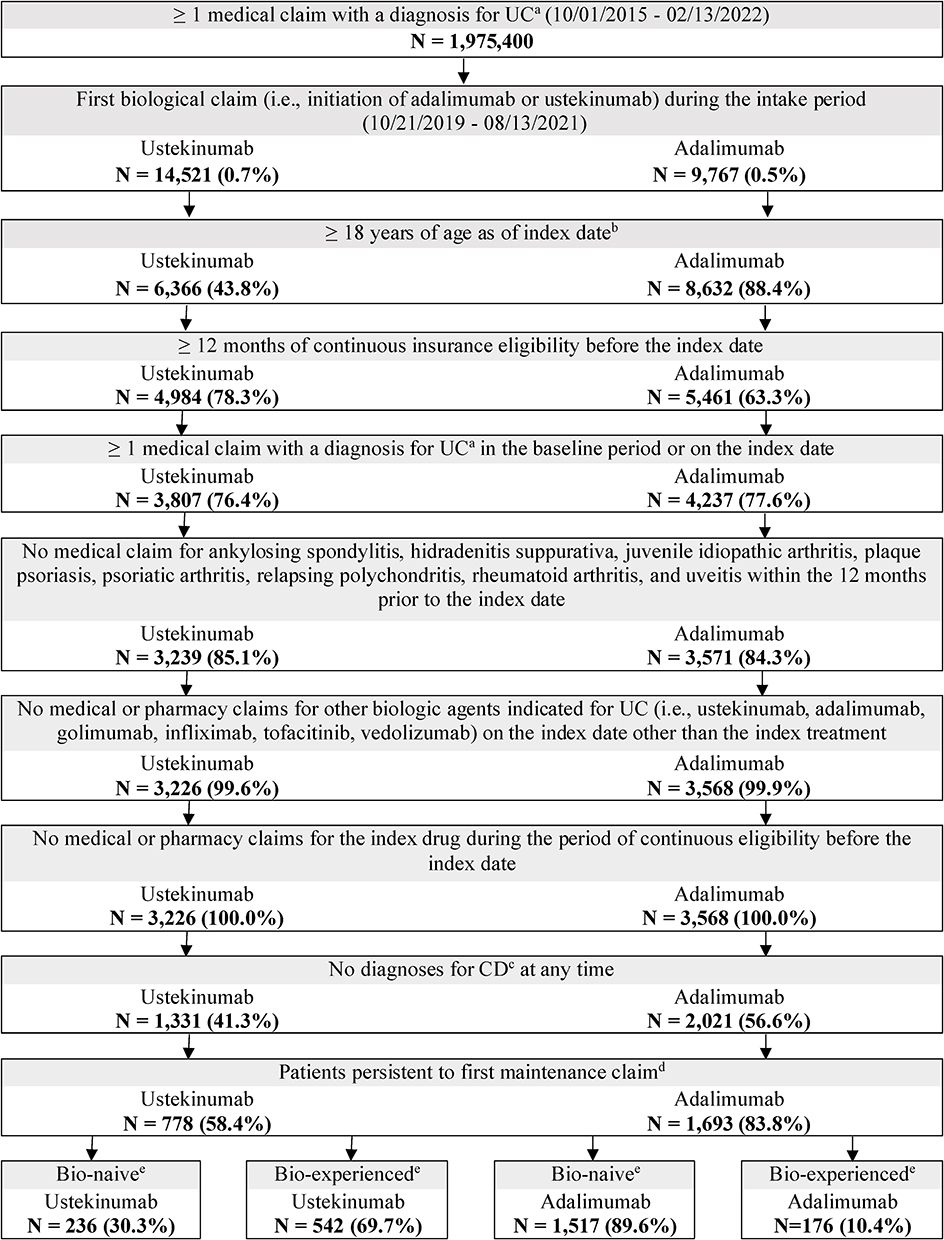 |
Figure 2 Patient flow chart. Abbreviations: CD, Crohn’s disease; ICD-10-CM, International Classification of Disease, 10th revision, Clinical Modification; UC, ulcerative colitis. Notes: a. Diagnosis of UC was ICD-10-CM: K51.x. b. The index date was the date of the first claim for ustekinumab or adalimumab during the intake period between 10/21/2019 and 08/13/2021. c. Diagnosis of CD was ICD-10-CM: K50.x. d. The first maintenance claim was identified as the date of the first subcutaneous claim for ustekinumab and the date of the first claim following a cumulative dose of 240 mg for adalimumab. e. Bio-naïve and bio-experienced subgroups were based on the absence or presence of pharmacy or medical claims for UC-indicated biologics or advanced therapy agents (ie, adalimumab, golimumab, infliximab and biosimilars, ozanimod, tofacitinib, upadacitinib, ustekinumab, vedolizumab) during the baseline period. |
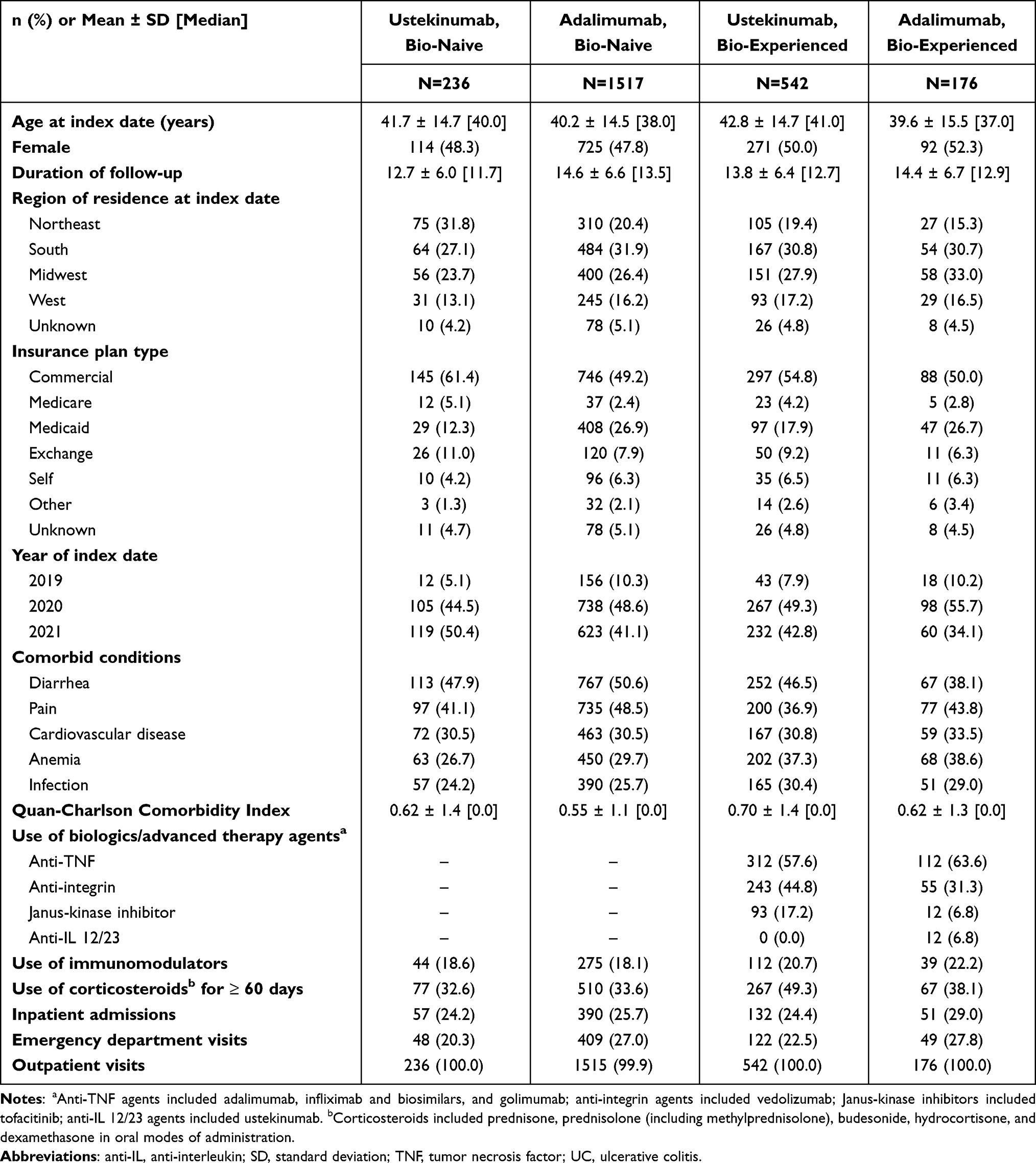 |
Table 1 Patient Baseline Characteristics Among UC Patients Who Persist to Their First Maintenance Claim |
Overall Persistence
Mean [median] duration of follow-up (in months) was 12.7 [11.7] and 14.6 [13.5] in the bio-naive ustekinumab and adalimumab subgroups, respectively, and 13.8 [12.7] and 14.4 [12.9] in the bio-experienced subgroups.
At 12 months after maintenance phase start, 75.5% and 50.5% were persistent in the bio-naïve ustekinumab and adalimumab subgroups, respectively (Figure 3A). Among bio-experienced subgroups, 72.3% were persistent with ustekinumab and 56.9% with adalimumab at 12 months (Figure 3B). For both the bio-naïve and bio-experienced subgroups, persistence probability at 3, 6, and 9 months was numerically higher for patients initiated on ustekinumab than adalimumab, and median persistent time was not reached within 12 months for either cohort.
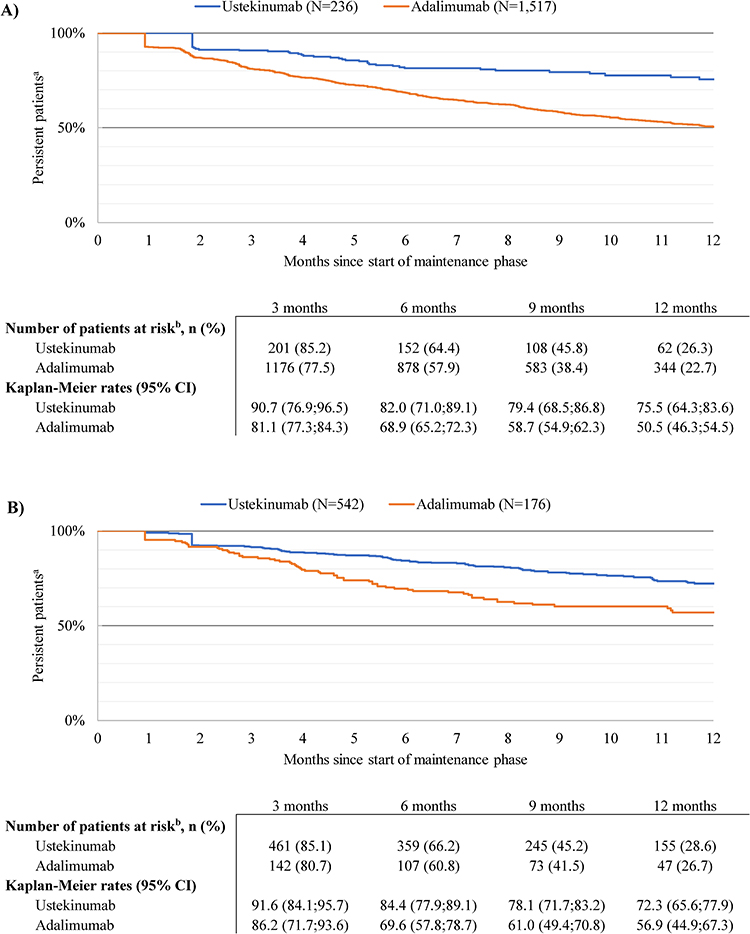 |
Figure 3 Persistence during the maintenance phase in the ustekinumab and adalimumab cohorts. (A) Among bio-naïve patients with UC. (B) Among bio-experienced patients with UC. Abbreviations: CI, confidence interval; UC, ulcerative colitis. Notes: a. Persistent time was measured from the maintenance phase start until the discontinuation date. Patients without discontinuation were censored on the last day of index therapy supply. b. Patients at risk of having the event were patients who had not had the event and had not been lost to follow-up at that point in time. |
Corticosteroid-Free Persistence
In bio-naïve subgroups, 233 patients initiated on ustekinumab and 1502 patients initiated on adalimumab were corticosteroid-free at maintenance phase start. The probability of being persistent and corticosteroid-free at 12 months after maintenance phase start was 55.1% with ustekinumab and 38.2% with adalimumab (Figure 4A). The median corticosteroid-free persistent time was 7.2 months for the bio-naïve adalimumab subgroup and was not reached within 12 months for the bio-naïve ustekinumab subgroup.
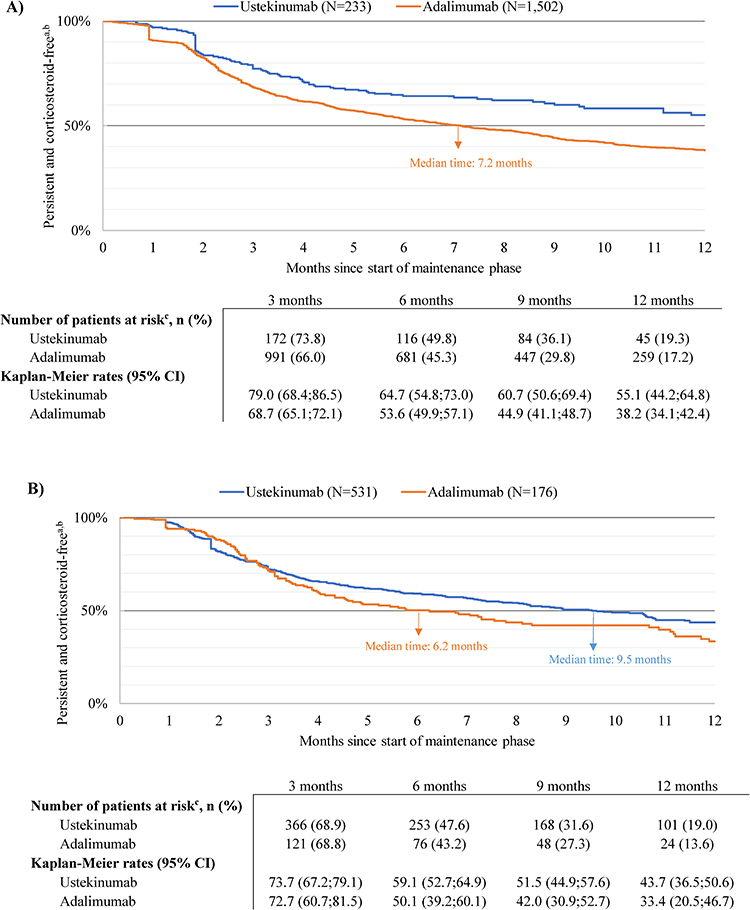 |
Figure 4 Corticosteroid-free persistence during the maintenance phase in the ustekinumab and adalimumab cohorts. (A) Among bio-naïve patients with UC. (B) Among bio-experienced patients with UC. Abbreviations: CI, confidence interval; UC, ulcerative colitis. Notes: a. Persistent time was measured from the maintenance phase start until the earliest among the discontinuation date or corticosteroid use date. Patients without discontinuation or corticosteroid use were censored on the last day of index therapy supply. b. A patient was defined as corticosteroid-free if they had less than 14 consecutive days of supply of corticosteroids after 90 days post-index. c. Patients at risk of having the event were patients who had not had the event and had not been lost to follow-up at that point in time. |
In bio-experienced subgroups, 531 patients initiated on ustekinumab and 176 initiated on adalimumab were corticosteroid-free at maintenance phase start. The probability of being persistent and corticosteroid-free at 12 months was 43.7% with ustekinumab and 33.4% with adalimumab (Figure 4B). The median corticosteroid-free persistent time was 9.5 months for the bio-experienced ustekinumab subgroup and 6.2 months for the bio-experienced adalimumab subgroup.
At 3, 6, and 9 months after maintenance phase start, the proportion of patients that were persistent and corticosteroid-free was numerically higher in the ustekinumab cohort relative to the adalimumab cohort, for both subgroups (Figure 4A and B).
Persistence on Monotherapy
In bio-naïve subgroups, 222 patients initiated on ustekinumab and 1390 patients initiated on adalimumab were on monotherapy at maintenance phase start. The probability of being persistent and on monotherapy at 12 months after maintenance phase start was 68.1% with ustekinumab and 44.5% with adalimumab (Figure 5A). The median persistent time on monotherapy was 9.9 months for the bio-naïve adalimumab subgroup and was not reached within 12 months for the bio-naïve ustekinumab subgroup.
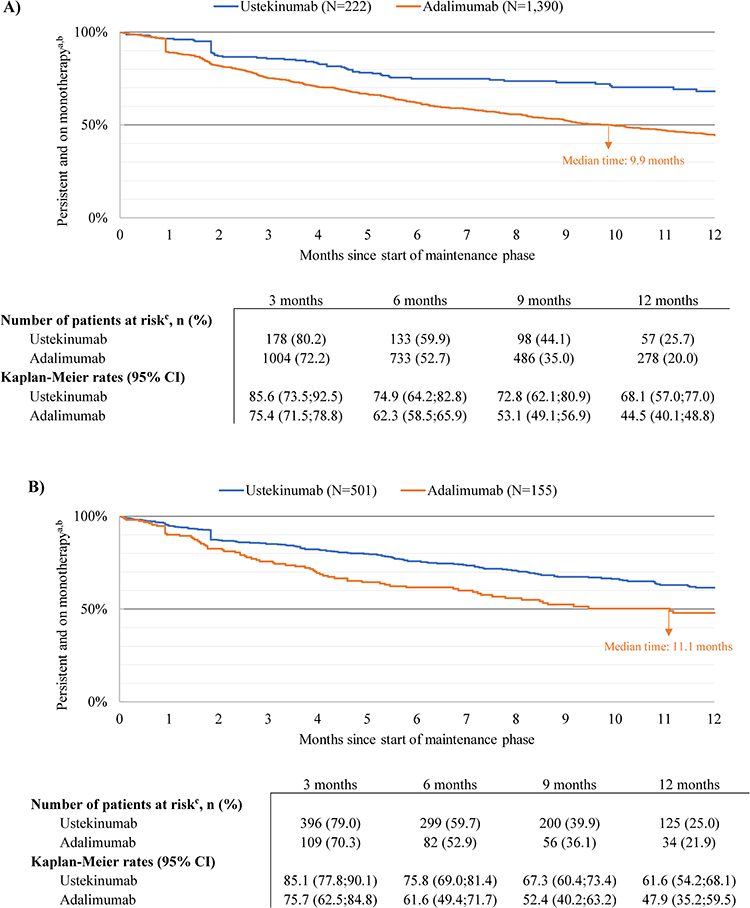 |
Figure 5 Persistence on monotherapy during the maintenance phase in the ustekinumab and adalimumab cohorts. (A) Among bio-naive patients with UC. (B) Among bio-experienced patients with UC. Abbreviations: CI, confidence interval; UC, ulcerative colitis. Notes: a. Persistent time was measured from the maintenance phase start until the earliest among the discontinuation date or immunomodulator/non-index biologic/advanced therapy agent use date. Patients without discontinuation or immunomodulator/non-index biologic/advanced therapy agent use were censored on the last day of index therapy supply. b. A patient was on monotherapy if they did not use any immunomodulators, non-index biologic or advanced therapy agent. c. Patients at risk of having the event were patients who had not had the event and had not been lost to follow-up at that point in time. |
In bio-experienced subgroups, 501 patients initiated on ustekinumab and 155 patients initiated on adalimumab were on monotherapy at maintenance phase start. The probability of being persistent and on monotherapy at 12 months was 61.6% with ustekinumab and 47.9% with adalimumab (Figure 5B). The median persistent time on monotherapy was 11.1 months for the bio-experienced adalimumab subgroup and was not reached for the bio-experienced ustekinumab subgroup.
At 3, 6, and 9 months after maintenance phase start, the proportion of patients that were persistent and on monotherapy was numerically higher in the ustekinumab cohort relative to the adalimumab cohort, for both subgroups (Figure 5A and B).
Discussion
This retrospective cohort study using claims data described treatment persistence among patients with UC initiated on ustekinumab or adalimumab. Numerically higher persistence during the 12-month period following the start of maintenance phase was observed among patients initiated on ustekinumab compared to adalimumab, regardless of past biologic or advanced therapy agent experience. Results were similar for corticosteroid-free persistence and persistence on monotherapy.
The one-year persistence of >70% on ustekinumab observed in this study is comparable to recent findings from other observational studies. For example, in a registry-based study of 133 patients with UC in Sweden, 67% of bio-experienced patients with UC persisted on ustekinumab after a median follow-up of ~7 months.17 Similarly, in a study of 66 patients with UC initiated on ustekinumab in the US (the majority of which had prior biologic/advanced therapy experience), persistence at 12 months was 71%.18 In an Italian study of 68 patients with UC treated off-label with ustekinumab (97% had previous biologics/advanced therapy exposure), probability of treatment persistence at 12 months was 87%.19 Although we are not aware of any other published real-world studies comparing persistence between ustekinumab and adalimumab in UC, real-world studies of patients with Crohn’s disease have demonstrated higher persistence with ustekinumab than adalimumab.20–23 Taken together, this evidence demonstrates relatively high persistence on ustekinumab in a real-world setting.
Treatment options for patients with UC often include corticosteroids and/or immunomodulators (ie, thiopurines). The ACG recommends the use of systemic corticosteroids to induce remission in patients with UC in certain cases; however, corticosteroids have known side effects and are not recommended for remission maintenance.4 In patients with previous moderately-to-severely active UC who are in remission due to corticosteroid induction, the ACG conditionally recommends thiopurines for maintenance compared with no treatment or corticosteroid maintenance.4 Combination therapy with immunomodulators is sometimes used because immunomodulators may improve the therapeutic effect of biologics,5,6 but it may be associated with elevated risk of infections and malignancies.24,25 In addition to the potential adverse health effects associated with the use of corticosteroids and immunomodulators, medication and clinical management costs might be higher when treated with several therapy agents at the same time compared to monotherapy. The findings of this study demonstrating numerically higher corticosteroid-free persistence and persistence on monotherapy among ustekinumab users provide relevant information to help guide treatment selection.
Biologics that have been on the market for a relatively long period of time (eg, adalimumab) are frequently used as first-line biologic treatment, but many do not respond to initial therapy; for example, in a large claims-based study in the US, almost 70% of patients with UC initiated on biologic therapy received second-line therapy within 24 months.26 Newer biologics to treat UC (including ustekinumab) are often used in patients who have failed prior therapies. This pattern was reflected in this current study, where more bio-experienced patients received ustekinumab than adalimumab, by a 3-fold margin, while more bio-naïve patients received adalimumab over ustekinumab, by a 6.4-fold margin. Prior biologic experience has been associated with reduced response to subsequent lines of therapy,27 which could in turn influence treatment persistence, highlighting the importance of evaluating treatment persistence by subgroups of patients based on prior biologic experience. In this study, we observed consistent patterns of persistence favoring ustekinumab over adalimumab in both bio-naïve and bio-experienced subgroups, positioning ustekinumab as a good treatment option for UC patients regardless of prior biologic experience.
Data pertaining to reasons for discontinuation were not available in this study, so we were unable to evaluate why persistence on ustekinumab was numerically higher than adalimumab. However, differences in the dosing regimen of ustekinumab (administered subcutaneously in maintenance phase once every eight weeks) relative to adalimumab (administered subcutaneously in maintenance phase every other week) may have influenced persistence rates. In addition, the presence of side effects, loss of treatment effectiveness, patient preference, and out-of-pocket costs may also contribute to differences in persistence.28–31
Limitations
Although the data source for this claims-based study is comprehensive, the results may not be generalizable to those without health insurance. Analysis of administrative claims cannot account for prescription fills where the medication dispensed was not taken as prescribed. Use of claims data also assumes correct diagnosis, procedure, and drug codes, and instances of misclassification cannot be ruled out. Moreover, imputation of days of supply assumes that there is a single administration per claim for ustekinumab and double administration for adalimumab, and that the time to the next claim is a proxy for the intended time between doses. Finally, although persistence was numerically higher in the ustekinumab versus adalimumab cohort, analyses were descriptive, differences between cohorts during the baseline period were not adjusted for, and no statistical tests were performed. Future analyses may consider formally comparing persistence rates between cohorts while accounting for potential confounders.
Conclusions
In this claims-based analysis of bio-naïve and bio-experienced patients with UC initiated on ustekinumab and adalimumab, overall treatment persistence, corticosteroid-free persistence, and persistence while on monotherapy were numerically higher in the ustekinumab cohort than the adalimumab cohort. The real-world evidence presented in this study may position ustekinumab as a good treatment option for patients with UC regardless of prior biologic experience and contribute to clinical decision-making as treatment persistence is integral to managing chronic diseases.
Data Sharing Statement
The data that support the findings of this study were used under license from the Komodo Health. Any researchers interested in obtaining the data used in this study can access the database through Komodo Health, under a license agreement, including the payment of appropriate license fee.
Compliance with Ethics Guidelines
The open-source claims in the database are de-identified and comply with the patient requirements of the Health Insurance Portability and Accountability Act (HIPAA); therefore, institutional review board approval was not required.
Acknowledgments
Medical writing assistance was provided by Christopher Crotty, PhD, an employee of Analysis Group, Inc., a consulting company that has provided paid consulting services to Janssen Scientific Affairs, LLC, which funded the development and conduct of this study and manuscript. Chris Holiday, MA, a former employee of Analysis Group, Inc., contributed to the analysis.
This paper was presented at the Crohn’s & Colitis Congress – January 19-21, 2023, Denver, CO as a poster presentation with interim findings. The poster’s abstract was published in the American Gastroenterological Association’s Gastroenterology journal (DOI: https://doi.org/10.1053/j.gastro.2023.03.086) and in the Inflammatory Bowel Diseases journal (DOI: https://doi.org/10.1093/ibd/izac247.067).
Author Contributions
All authors have made substantial contributions to the conception or design of the study, or the acquisition, analysis, or interpretation of data, drafting the manuscript and revising it critically for important intellectual content, and have provided final approval of this version to be published and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by Janssen Scientific Affairs, LLC. The study sponsor was involved in the study design, interpretation of data, and writing of the manuscript.
Disclosure
Sumesh Kachroo, Zhijie Ding, Ruizhi Zhao, and Caroline Kerner are employees of Janssen Scientific Affairs, LLC. and hold stock in Johnson & Johnson. Maryia Zhdanava, Aditi Shah, Patrick Lefebvre, and Dominic Pilon are employees of Analysis Group, Inc., a consulting company that has provided paid consulting services to Janssen Scientific Affairs, LLC. The authors report no other conflicts of interest in this work.
References
1. Ungaro R, Mehandru S, Allen PB, Peyrin-Biroulet L, Colombel JF. Ulcerative colitis. Lancet. 2017;389(10080):1756–1770. doi:10.1016/S0140-6736(16)32126-2
2. Mak WY, Zhao M, Ng SC, Burisch J. The epidemiology of inflammatory bowel disease: east meets west. J Gastroenterol Hepatol. 2020;35(3):380–389. doi:10.1111/jgh.14872
3. Ye Y, Manne S, Treem WR, Bennett D. Prevalence of inflammatory bowel disease in pediatric and adult populations: recent estimates from large national databases in the United States, 2007–2016. Inflammatory Bowel Dis. 2019;26(4):619–625. doi:10.1093/ibd/izz182
4. Rubin DT, Ananthakrishnan AN, Siegel CA, Sauer BG, Long MD. ACG clinical guideline: ulcerative colitis in adults. Am J Gastroenterol. 2019;114(3):384–413. doi:10.14309/ajg.0000000000000152
5. Feuerstein JD, Isaacs KL, Schneider Y, et al. AGA clinical practice guidelines on the management of moderate to severe ulcerative colitis. Gastroenterology. 2020;158(5):1450–1461. doi:10.1053/j.gastro.2020.01.006
6. Sandborn WJ, Feagan BG, Hanauer SB, Lichtenstein GR. The guide to guidelines in ulcerative colitis: interpretation and appropriate use in clinical practice. Gastroenterol Hepatol. 2021;17(4 Suppl 4):567.
7. Farrell RJ. Biologics beyond anti-TNF agents for ulcerative colitis - efficacy, safety, and cost? N Engl J Med. 2019;381(13):1279–1281. doi:10.1056/NEJMe1910742
8. Augustin M, Costanzo A, Pink A, et al. Real-world treatment patterns and treatment benefits among adult patients with atopic dermatitis: results from the Atopic Dermatitis Patient Satisfaction and Unmet Need Survey. Acta Derm Venereol. 2022;102:adv00830. doi:10.2340/actadv.v102.3932
9. Sands BE, Sandborn WJ, Panaccione R, et al. Ustekinumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2019;381(13):1201–1214. doi:10.1056/NEJMoa1900750
10. Miranda A, Gravina AG, Cuomo A, et al. Efficacy of ustekinumab in the treatment of patients with Crohn’s disease with failure to previous conventional or biologic therapy: a prospective observational real-life study. J Physiol Pharmacol. 2021;72:567.
11. Uchida G, Nakamura M, Yamamura T, Tsuzuki T, Kawashima H. Real-world effectiveness of ustekinumab for patients with ulcerative colitis: a systematic review and meta-analysis. Nagoya J Med Sci. 2023;85(3):402–427. doi:10.18999/nagjms.85.3.402
12. Bressler B, Yarur A, Silverberg MS, et al. Vedolizumab and anti-tumour necrosis factor α real-world outcomes in biologic-naïve inflammatory bowel disease patients: results from the EVOLVE study. J Crohn’s Colitis. 2021;15(10):1694–1706. doi:10.1093/ecco-jcc/jjab058
13. Khan S, Rupniewska E, Neighbors M, Singer D, Chiarappa J, Obando C. Real-world evidence on adherence, persistence, switching and dose escalation with biologics in adult inflammatory bowel disease in the United States: a systematic review. J Clin Pharm Ther. 2019;44(4):495–507. doi:10.1111/jcpt.12830
14. Chen C, Hartzema AG, Xiao H, et al. Real-world pattern of biologic use in patients with inflammatory bowel disease: treatment persistence, switching, and importance of concurrent immunosuppressive therapy. Inflamm Bowel Dis. 2019;25(8):1417–1427. doi:10.1093/ibd/izz001
15. Janssen Biotech, Inc. STELARA® (Ustekinumab) Prescribing Information. Horsham, PA: Janssen Biotech, Inc; 2022.
16. AbbVie Inc. HUMIRA® (Adalimumab) Prescribing Information. North Chicago, IL: AbbVie Inc; 2021.
17. Thunberg J, Bjorkqvist O, Hedin CRH, et al. Ustekinumab treatment in ulcerative colitis: real-world data from the Swedish inflammatory bowel disease quality register. United Eur Gastroenterol J. 2022;10(7):631–639. doi:10.1002/ueg2.12275
18. Hong SJ, Krugliak Cleveland N, Akiyama S, et al. Real-world effectiveness and safety of ustekinumab for ulcerative colitis from 2 tertiary IBD centers in the United States. Crohn's Colitis. 2021;3(1):otab002. doi:10.1093/crocol/otab002
19. Chiappetta MF, Viola A, Mastronardi M, et al. One-year effectiveness and safety of ustekinumab in ulcerative colitis: a multicenter real-world study from Italy. Expert Opin Biol Ther. 2021;21(11):1483–1489. doi:10.1080/14712598.2021.1981855
20. Teeple A, Sah J, Mallampati R, Adams C, Waters D, Muser E. Persistence, dosing, and other treatment patterns among Crohn’s disease patients initiating biologics in United States. Crohn’s & Colitis. 2021;3(4):360. doi:10.1093/crocol/otab076
21. Silverberg JI, Toth D, Bieber T, et al. Tralokinumab plus topical corticosteroids for the treatment of moderate-to-severe atopic dermatitis: results from the double-blind, randomized, multicentre, placebo-controlled Phase III ECZTRA 3 trial. Br J Dermatol. 2021;184(3):450–463. doi:10.1111/bjd.19573
22. Zhdanava M, Ding Z, Manceur AM, et al. Treatment persistence among bio-naïve patients with Crohn’s disease initiated on ustekinumab or adalimumab. Curr Med Res Opin. 2023:1–11. doi:10.1080/03007995.2023.2178148
23. Chien TH, Puig A, Khuong T, Kouhkamari MH, Che S, Huang TH. An Australian real-world study of treatment persistence of ustekinumab in Crohn’s disease. Biologics. 2021;15:237–245. doi:10.2147/btt.S310076
24. Hashash JG, Fadel CGA, Rimmani HH, Sharara AI. Biologic monotherapy versus combination therapy with immunomodulators in the induction and maintenance of remission of Crohn’s disease and ulcerative colitis. Ann Gastroenterol. 2021;34(5):612–624. doi:10.20524/aog.2021.0645
25. Dulai PS, Siegel CA, Colombel J-F, Sandborn WJ, Peyrin-Biroulet L. Systematic review: monotherapy with antitumour necrosis factor α agents versus combination therapy with an immunosuppressive for IBD. Gut. 2014;63(12):1843–1853. doi:10.1136/gutjnl-2014-307126
26. Brady JE, Stott-Miller M, Mu G, Perera S. Treatment patterns and sequencing in patients with inflammatory bowel disease. Clin. Ther. 2018;40(9):1509–1521.e5. doi:10.1016/j.clinthera.2018.07.013
27. Privitera G, Pugliese D, Rapaccini GL, Gasbarrini A, Armuzzi A, Guidi L. Predictors and early markers of response to biological therapies in inflammatory bowel diseases. J Clin Med. 2021;10(4):853. doi:10.3390/jcm10040853
28. Biemans VBC, Sleutjes JAM, de Vries AC, et al. Tofacitinib for ulcerative colitis: results of the prospective Dutch Initiative on Crohn and Colitis (ICC) registry. Aliment Pharmacol Ther. 2020;51(9):880–888. doi:10.1111/apt.15689
29. Chaparro M, Garre A, Iborra M, et al. Effectiveness and safety of ustekinumab in ulcerative colitis: real-world evidence from the ENEIDA registry. J Crohn’s Colitis. 2021;15(11):1846–1851. doi:10.1093/ecco-jcc/jjab070
30. Luttropp K, Dalén J, Svedbom A, Dozier M, Black CM, Puenpatom A. Real-world patient experience of switching biologic treatment in inflammatory arthritis and ulcerative colitis – a systematic literature review. Patient Preference Adherence. 2020;14:309–320. doi:10.2147/PPA.S238843
31. Kane SV, Accortt NA, Macgowan S, Brixner D. Predictors of persistence with 5-aminosalicylic acid therapy for ulcerative colitis. Aliment Pharmacol Ther. 2009;29(8):855–862. doi:10.1111/j.1365-2036.2009.03941.x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Emerging Therapies for Ulcerative Colitis: Updates from Recent Clinical Trials
AlAmeel T, AlMutairdi A, Al-Bawardy B
Clinical and Experimental Gastroenterology 2023, 16:147-167
Published Date: 17 August 2023
Advanced Combination Therapy with Biologics and Upadacitinib in Refractory Inflammatory Bowel Disease: A Retrospective Study from Taiwan
Meng MJ, Kuo CJ, Lai MW, Chiu CT, Su MY, Chang ML, Le PH
Journal of Inflammation Research 2025, 18:2733-2742
Published Date: 26 February 2025
Surgeons Knowledge, Attitude, and Practice Toward Preoperative Inflammatory Bowel Disease Medications and Post-Operative Complications
Alhassan N, Alnwdel AN, Beyari MB, Aldeligan SH, Alhassan R, Abdulla MH, Bin Traiki T
Therapeutics and Clinical Risk Management 2025, 21:1149-1159
Published Date: 22 July 2025