")
Back to Journals » Infection and Drug Resistance » Volume 16
Surface Disinfection Practice in Public Hospitals in the Era of COVID-19: Assessment of Disinfectant Solution Preparation and Use in Addis Ababa, Ethiopia
Authors Selam MN , Tegegne AM , Ababu A , Matsabisa M , Birhanu G
Received 9 March 2023
Accepted for publication 18 May 2023
Published 23 May 2023 Volume 2023:16 Pages 3213—3224
DOI https://doi.org/10.2147/IDR.S411835
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Suresh Antony
Muluken Nigatu Selam,1 Aychew Mekuriaw Tegegne,2 Andualem Ababu,3 Motlalepula Matsabisa,4 Gebremariam Birhanu1,4
1Department of Pharmaceutics and Social Pharmacy, School of Pharmacy, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 2Department of Pharmacy, College of Health Sciences, Debre Berhan University, Debre Berhan, Ethiopia; 3Pharmaceutical and Medical Equipment Lead Executive Office, Ministry of Health, Addis Ababa, Ethiopia; 4Department of Pharmacology, Faculty of Health Sciences, University of the Free State, Bloemfontein, 9300, South Africa
Correspondence: Muluken Nigatu Selam, Department of Pharmaceutics and Social Pharmacy, School of Pharmacy, Addis Ababa University, P.O. Box 1176, Addis Ababa, Ethiopia, Tel +251912159807, Email [email protected]
Background: Surface disinfection of healthcare facilities with appropriate disinfectants is among the infection control strategies against the spread of coronavirus disease 2019 (COVID-19). As sodium hypochlorite solution (SHS) is a commonly used surface disinfectant, its preparation and proper use should be given a due attention. The current study aimed at assessing the practice of Addis Ababa public hospitals in the preparation and use of SHS.
Methods: A cross-sectional observational study was employed to assess the adequacy of disinfectant solution preparation and use. Checklists were used for data collection. Descriptive statistics were used for data analyses, and categorical variables were described by frequencies and percentages.
Results: Out of the twelve public hospitals included in the study; only three hospitals checked the potency of the working SHS. Majority of the hospitals (8 hospitals) stored the concentrated SHS products in cool, dry, and direct sunlight protected places. It was only in one hospital where appropriate personal protective equipment was used during the preparation and quality control activities. Surfaces were not cleaned in all hospitals before disinfection; and the rooms were ventilated only in 2 hospitals during the application of the disinfectant solution.
Conclusion: The study revealed that the preparations of SHS in the public hospitals did not comply with most of the requirements of good compounding practice. Moreover, standard practices were not maintained in majority hospitals during the use of SHS for surface disinfection. As a control strategy in the spread of COVID-19 and other infections, appropriate corrective actions shall be implemented in the studied hospitals to mitigate the limitations observed in the preparation and use of SHS.
Keywords: compounding, COVID-19, disinfectants, proper use, public hospitals, sodium hypochlorite solution
Introduction
The emergence of the COVID-19 (Coronavirus Disease-2019) pandemic has become a significant global public health concern. The prevention and control measures for the spread of coronavirus include hand hygiene, disinfection of surfaces, avoidance of touching one’s face, and use of face masks and they are effective when combined.1,2
Contaminated surfaces are an important potential source for transmission of coronavirus and many other healthcare-associated pathogens.3,4 Severe acute respiratory syndrome, coronavirus 2 (SARS-CoV-2), the virus for COVID-19, can remain on surfaces viable for between eight hours and several days, depending on the type of surface.5–7 Surfaces become contaminated when virus-containing droplets land on them, or when someone with contaminated hands touches the surfaces. Decontamination of the healthcare environment is therefore vital because it can efficiently disrupt the lipid envelope of coronavirus.7,8 The term disinfection describes a process that eliminates many or all pathogenic microorganisms, except bacterial spores, on inanimate objects.9
Effective infection prevention and control programs help in the reduction of healthcare-associated infections (HCAIs) and prevent morbidity and mortality and also reduce healthcare costs.10 The World Health Organization (WHO) recommends implementation of appropriate environmental cleaning and disinfection procedures in hospitals using disinfectants such as sodium hypochlorite solution.11
In hospitals, compounding practice is practiced when the market failed to provide medicines and disinfectants in the required dosage form and strength.12 Supply and stability issues of disinfectants in the market call attention for its preparation at the point of care. During the preparation, principle of good compounding practice (GCP) shall be implemented to assure the products’ quality and protect compounders and the environment from chemical exposure. The requirements of GCP include use of appropriate ingredients, equipment, and premises for compounding and storage; maintaining sanitation and hygiene during preparation; applying quality control activities; involvement of qualified personnel; and documentation.13
Environmental surfaces in healthcare settings include furniture and other fixed items inside and outside of patient rooms and bathrooms, such as tables, chairs, walls, light switches, etc. These surfaces are likely to be contaminated with the COVID-19 virus and must be properly cleaned and disinfected to prevent further transmission.7,14,15 Several studies indicated the effectiveness of surface disinfection to prevent the secondary transmission of SARS-CoV-2.5,16–18 Various disinfectants have been recognized and used against SARS-CoV-2 in different environments. These include chlorine-containing disinfectants, alcohol, hydrogen peroxide, and others.19,20 Hypochlorites are widely used in healthcare facilities in a variety of settings. For disinfection of noncritical surfaces and equipment, a 1:10 to 1:100 dilution of 5.25% to 6.15% sodium hypochlorite (ie, household bleach) has been recommended for decontamination.21
Organic matter can impede direct contact of a disinfectant to a surface and inactivate several disinfectants’ germicidal properties or modes of action. The disinfectant concentration which is directly affected by dilution accuracy22 and contact time are also critical for effective surface disinfection. Target microorganisms; application surfaces; compatibility, toxicity, stability and ease of use are among the criteria for selection of disinfectants. For the prevention of COVID-19 transmission, standard disinfectant preparation and surface disinfection procedures should be followed.7,23
During the COVID-19 pandemic, the cleaning and disinfection of environmental surfaces shall take place on a regular basis. It should follow detailed standard operating procedures (SOPs) with a clear delineation of responsibilities (eg, housekeeping or clinical staff) regarding the type of surfaces and frequency of disinfection of surfaces.7,23 Since effective cleaning and disinfection remain the cornerstone of environmental control programs, strategies should be devised to monitor cleaning and ensuring the adequacy of the disinfection practices.9 In general, the use of the chosen disinfectant, at the appropriate concentration and for the appropriate time, should kill pathogenic microorganisms including SARS-CoV-2, rendering an object and environment safe for use.
Some studies have demonstrated contamination of surfaces after completion of a cleaning and disinfection process. Such contamination has been attributed primarily to poor quality products and suboptimal application of disinfectants, a common problem in healthcare facilities.4,24,25 Moreover, the pandemic has created a shortage of supplies such as disinfectants, compounding and quality control equipment, and personal protective equipment (PPE) that make the preparation of the disinfectants at the hospital level and their proper use challenging. Lack of necessary information, including correct methods of preparation and application of disinfectants, use of PPE during the application of disinfectants, and safe storage of disinfectants were also reported somewhere else20,26 as gaps in preparation and use of disinfectants in healthcare settings.
Most African countries had been struggling to contain the rapidly spreading pandemic due to weak healthcare system and limited resources, and Ethiopia is not an exception. As of 13 October 2022, Ethiopia has reported 493,723 confirmed cases of COVID-19 with 7572 deaths.27 Following the COVID-19 outbreak, various healthcare facilities in Ethiopia have started compounding of different disinfectant solutions, mainly sodium hypochlorite solutions (SHS), at the facility level. The effectiveness of disinfectant products is dependent on their quality and rational use. These compounded products are required to meet minimum regulatory requirements and quality standards. Moreover, standard practices need to be followed during the application of the disinfectant on surfaces in the healthcare settings; which if violated may result in health risks for patients, healthcare providers, compounders, cleaning staff, and the environment. Hence, the present study focused on the evaluation of the adequacy of SHS preparation and utilization practice for surface disinfection in the era of COVID-19 in public hospitals found in Addis Ababa, Ethiopia.
Methods
Study Design and Settings
An observation-based cross-sectional study design was employed to assess the disinfectant solution preparation and the disinfection practice in the study hospitals. The current assessment was conducted in all of the 12 public hospitals found in Addis Ababa, Ethiopia. The hospitals are referral and provide all types of clinical services. They serve large number of people coming from different parts of the country (during a period of July 2021–June 2022, a total of 1,930,675 outpatient visits were recorded in the hospitals). The list of hospitals included in this study is indicated in Table 1. The study was conducted between May and June 2022.
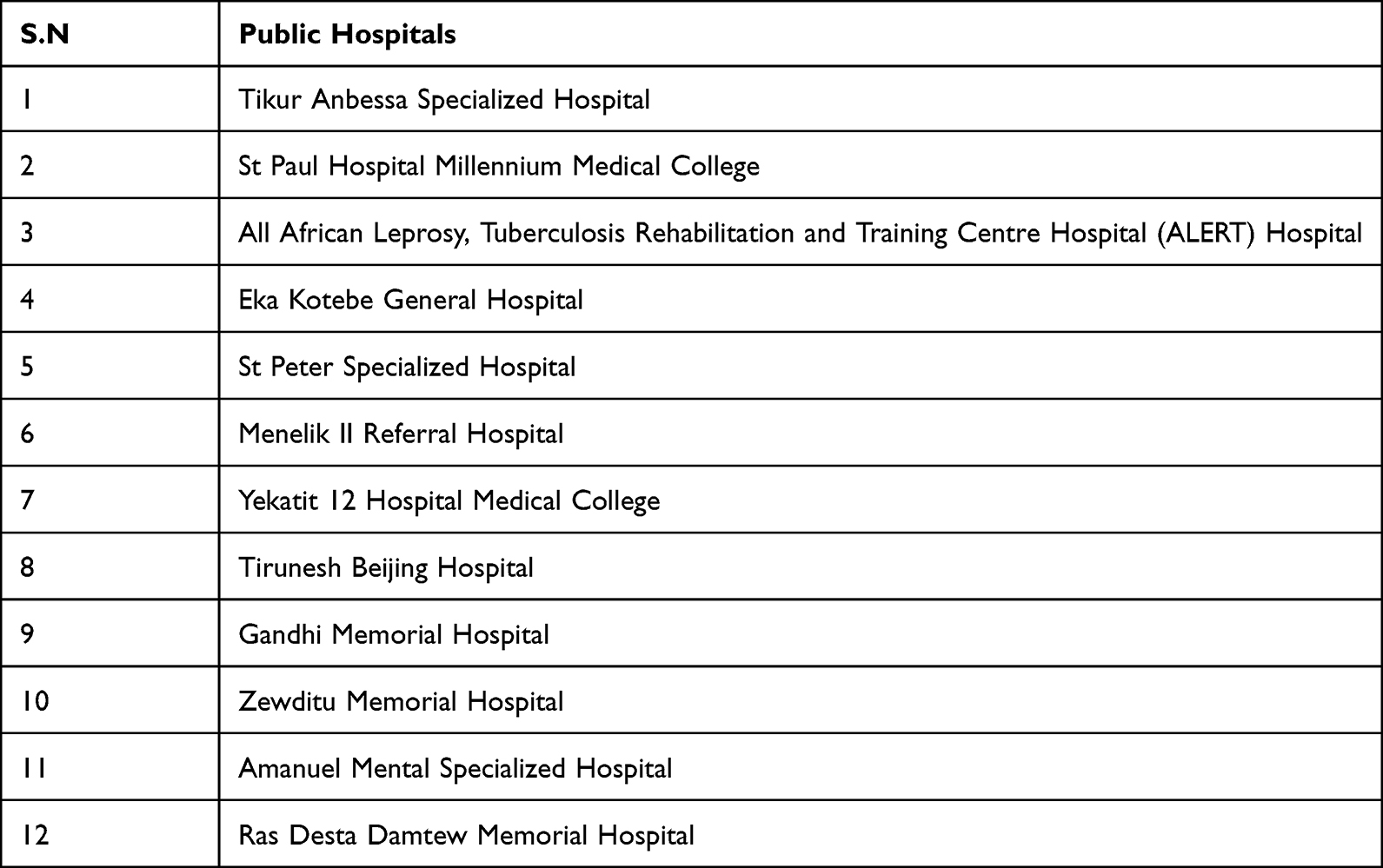 |
Table 1 List of Public Hospitals Included in the Study in Addis Ababa, Ethiopia, 2022 |
Sample Size and Sampling Technique
A purposive sampling technique was used for the current study. All public hospitals having disinfectant solution preparation units and those using their disinfectant solutions for surface disinfection purposes were included in the study. Therefore, a total of 12 hospitals from Addis Ababa were purposively selected and included in the study.
Eligibility Criteria
Public hospitals with functional disinfectant solution preparation unit and implementing surface disinfection in their compound during the study period were included in the study.
Data Collection Procedure
The data for the study were collected at disinfectant solution preparation units and at places where surface disinfections were taking place in the study hospitals. Data collection was done using checklists that were prepared by adopting standard documents of WHO, Federal Ministry of Health-Ethiopia, and USP.23,28–30 The preparation units and surface disinfection places were observed in addition to the compounders and cleaning staff to assess the compliance with the practice to requirements for disinfectant solution preparation and use. The observation checklists were comprised of closed-ended items on the preparation of disinfectant solutions and quality control activities; adequacy of premises; the adequacy of storage practices; hygiene, sanitation, and personnel protection; recording and documentation; and availability of trained personnel. Additionally, the surface disinfection processes in the hospitals were investigated for their rationality. Data collectors were trained for two days on the study’s purpose, details of the data collection checklist, ensuring the participants’ confidentiality, and COVID-19 prevention methods. Follow-up and supervisions were done by the principal investigators throughout the data collection period. The supervision focus includes on complying of data collectors to the COVID-19 prevention measures, their visit to the compounding and disinfection areas, their involvement in checking the presence of working documents, etc.
Data Quality Assurance
The data collection tools were reviewed by the experts from Addis Ababa University and Ethiopian Food and Drug Authority. Revision of the data collection tools according to the existent situation was done before the real data collection. Data consistency and correctness were ensured throughout the data collection, data entry, and analysis by cross-checking the hard copy of the checklists containing the data with the database.
Data Analysis
The data were entered and analyzed using Statistical Package for IBM Social Sciences (SPSS) version 25. Descriptive statistics were used for analyses of data. Categorical variables were described by frequencies and percentages.
Ethical Approval and Consent to Participate
Ethical approval was obtained from the Ethical Review Board of School of Pharmacy, Addis Ababa University (ERB/SOP/422/14/2022). An informed consent to participate in the study was obtained from each participant of the study hospitals. Participation was voluntary, and participants (pharmacy professionals and cleaners) were aware of their rights to withdraw from the study at any time. The data obtained from the observation were kept confidential.
Results
All the 12 public hospitals were observed for the assessment of their compliance with the practice at the time of compounding of SHS and surface disinfection.
Compounding of SHS
The Premise for the Compounding and Quality Control Activities
Of the 12 hospitals included in the study, only 5 (41.7%) and 1 (8.3%) hospitals had a dedicated room for compounding and quality control (QC) activities, respectively. It was only in 3 (25%) hospitals where the preparation of SHS was carried out in well-ventilated areas (Table 2).
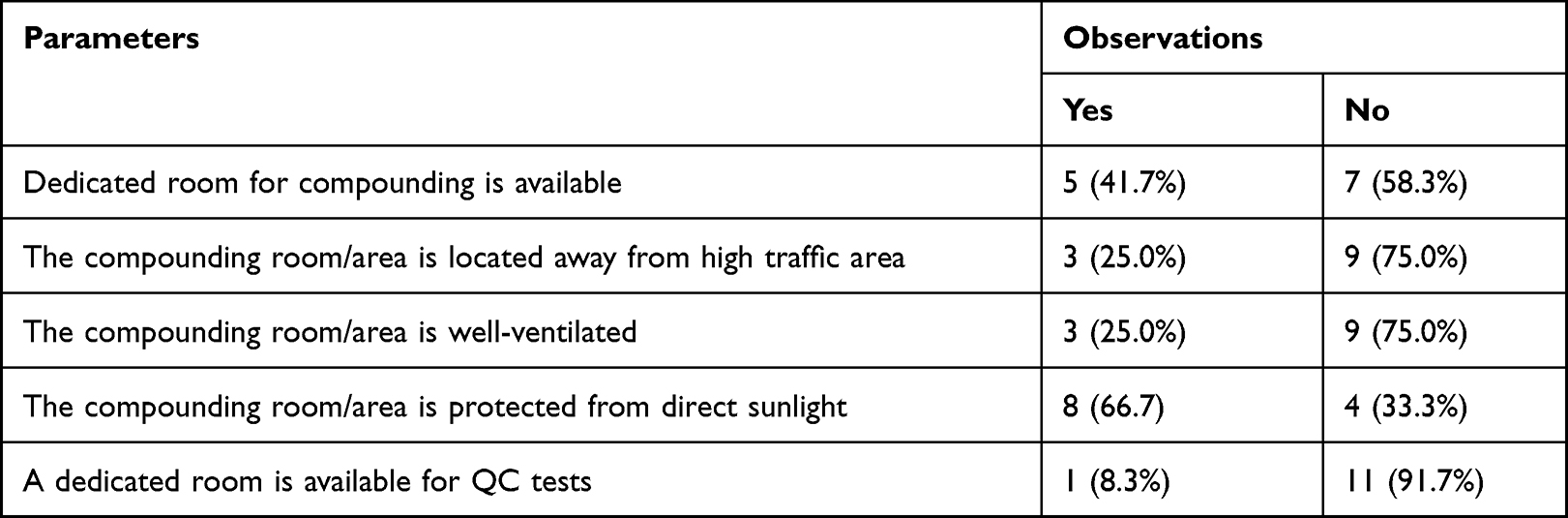 |
Table 2 Adequacy of Premises for the Preparation and QC of SHS in Public Hospitals, Addis Ababa, Ethiopia |
Compounding and QC Activities
Among the study hospitals, it was only in one hospital where the preparation of SHS was made in a dedicated compounding room. All of the hospitals failed to follow SOP during the preparation of the disinfectant. Only one hospital verified the strength of the undiluted SHS before operation (Table 3).
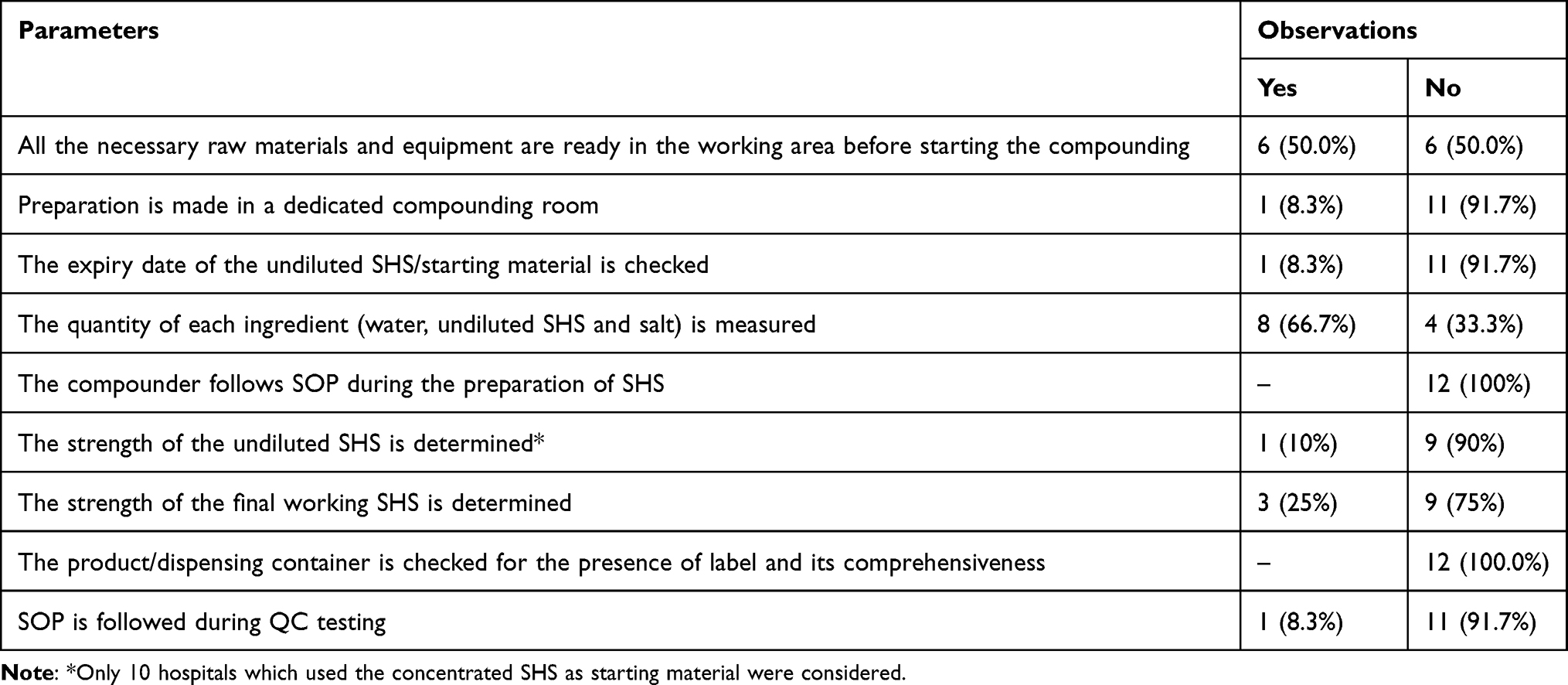 |
Table 3 Compounding and QC Activities for Sodium Hypochlorite Working Solution in Public Hospitals, Addis Ababa, Ethiopia |
Storage Premise and Condition
All 12 hospitals consumed the final diluted SHS within 24 hours. More than half of the hospitals (80%) stored the concentrated SHS in sunlight-protected places (Table 4).
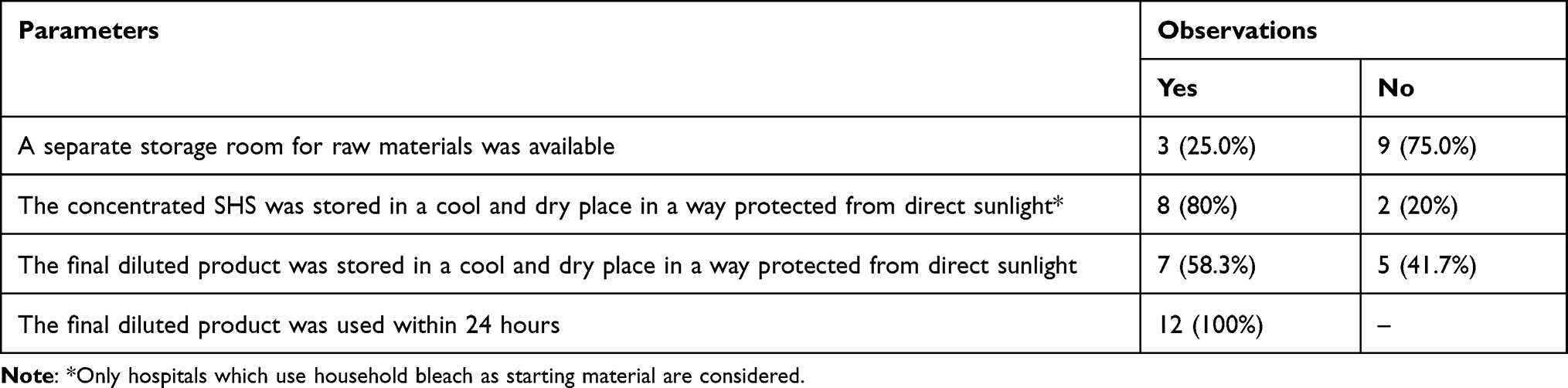 |
Table 4 Storage Premise and Condition for the SHS at the Public Hospitals in Addis Ababa, Ethiopia |
Hygiene, Sanitation and Personnel Protection
In all of the hospitals, the operator/s did not wash their hands before starting the compounding process. Appropriate PPE was not used by most of the hospitals (91.7%) during the preparation of the SHS (Table 5). The preparation areas were not cleaned both before and after the activity in all hospitals.
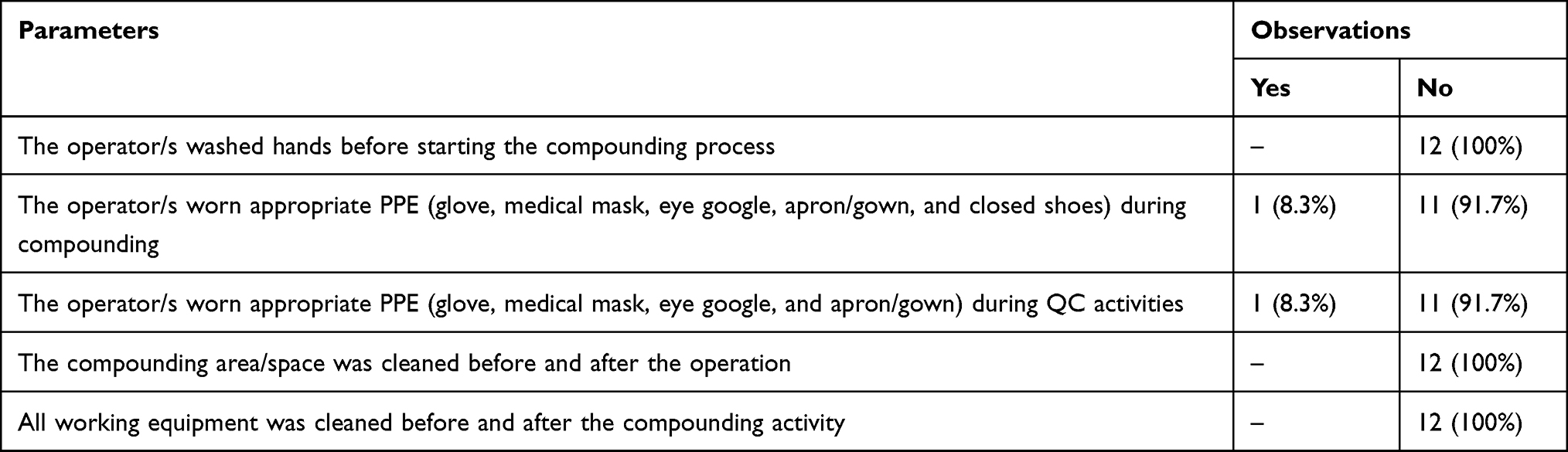 |
Table 5 Hygiene, Sanitation, and Personal Protection During the Preparation and QC of SHS in Public Hospitals, Addis Ababa, Ethiopia |
Documentation and Recording
The SOP for the production and QC operation of the SHS were found to be available only in 2 and 1 hospitals, respectively. Only a quarter of the hospitals had distribution records for the prepared SHS. Majority of the hospitals (66.7%) had reference documents for the preparation of SHS (Table 6).
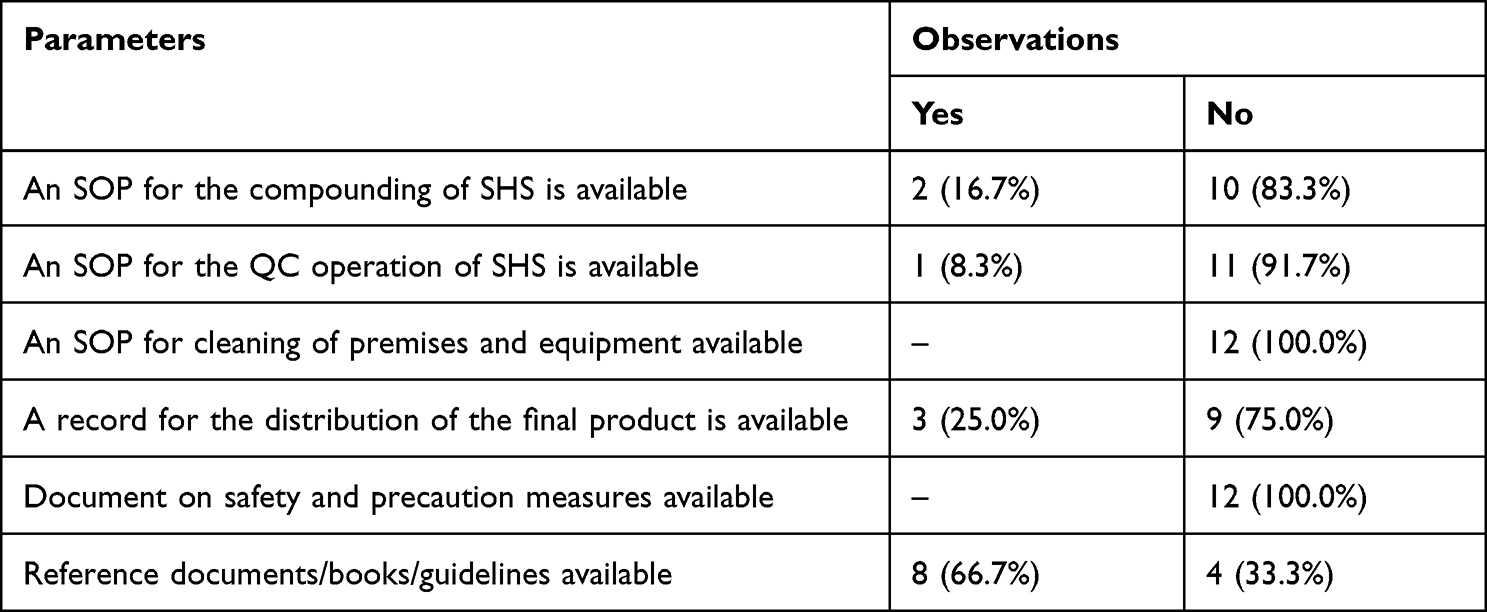 |
Table 6 Availability of Documents and Records for the Preparation and QC Activities of SHS in Public Hospitals, Addis Ababa, Ethiopia |
Compounding Personnel
All the studied hospitals had dedicated teams for the preparation of SHS. It was only in a single hospital that the compounding was performed by pharmacy professionals. Compounders in more than half of the hospitals (58.3%) did not take training on disinfectant preparation.
Use of Disinfectants for Surface Disinfection
Disinfection Process
Out of the 12 hospitals, only 3 hospitals applied the SHS only on non-metallic surfaces. Half of the hospitals included in this study gave sufficient contact time for the SHS with the surfaces in which the solution was applied. None of the hospitals cleaned the surfaces before disinfection and the majority (83.3%) did not wear the appropriate PPE during disinfection (Table 7).
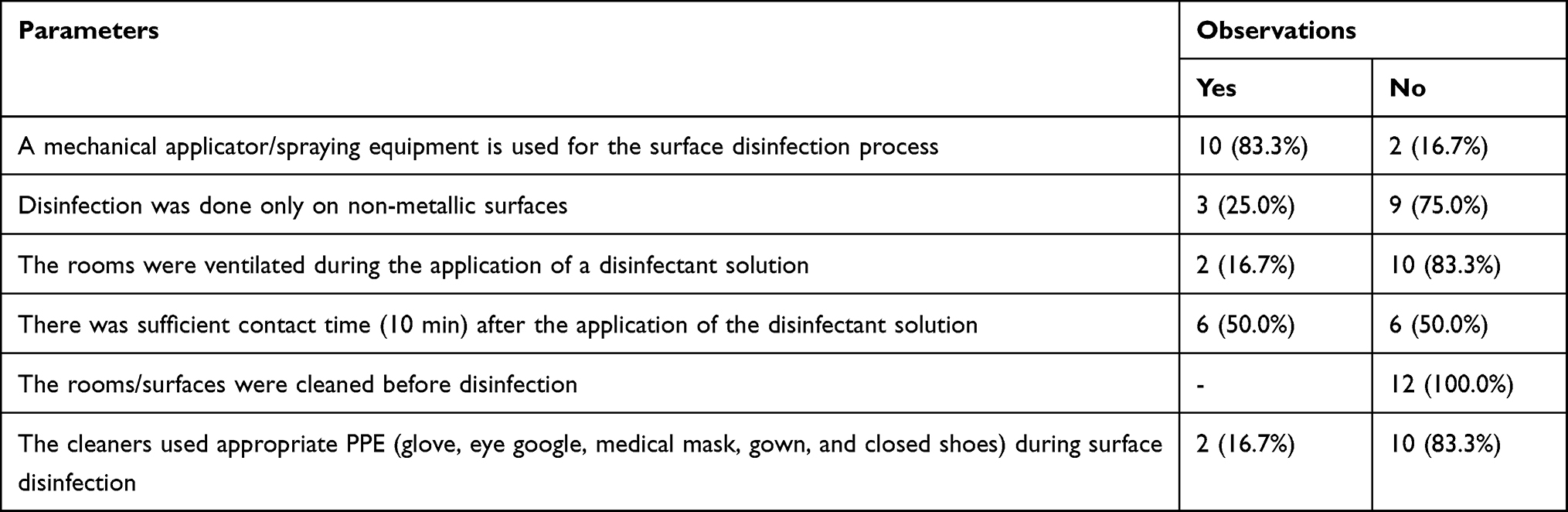 |
Table 7 Disinfection of Surfaces Using SHS in Public Hospitals, Addis Ababa, Ethiopia |
Documentation and Cleaning Personnel
Relevant documents for the effective use of SHS such as SOP for proper use, safety and precaution guideline, and records of the disinfection process were not available in all hospitals. It was also reported that only persons in 4 of the hospitals (33.3%) took formal training on the surface disinfection process using SHS.
Discussion
COVID-19 has confirmed the central role that infection prevention and control play in the prevention and containment of outbreaks in healthcare facilities and in the community.31 There is increasing evidence that rigorous disinfection is needed to prevent surface transmission of coronavirus 232 as the virus can remain viable on surfaces for days. Potentially contaminated surfaces must be frequently cleaned and disinfected to prevent further spread of the virus. The selected disinfectant products should be recognized as being effective in killing the COVID-19 virus.
Most healthcare facilities in Ethiopia and other developing countries are commonly using SHS as a surface disinfectant mainly due to its low cost and relatively simple preparation technique (ie, dilution) in comparison with other disinfectants. The use of this product for surface disinfection in healthcare facilities and other environmental places is increasing amid COVID-19.
Although new cases, hospitalizations, and deaths due to COVID-19 are down in Ethiopia, the implementation of various infection control strategies need to continue until the pandemic is under control worldwide. Surface disinfection in healthcare facilities is among the measures exercised in hospitals to control the spread of SARS-CoV-2 and other pathogens responsible for HCAIs. Sodium hypochlorite solution, at a concentration of 0.1 to 0.5% is a commonly used hospital-level disinfectant that is applied on environmental surfaces in Ethiopian healthcare facilities.33
The current study evaluated the practice of sodium hypochlorite working solution preparation and its use for surface disinfection in public hospitals during the time of COVID-19 crisis. At the time of observation, most of the hospitals (75%) prepared less than 50 liters of SHS at once. Ten of the studied hospitals used commercial household bleaches as starting materials which are to be diluted and the rest two hospitals prepared the working SHS using on-site chlorine generator machines. In all the hospitals, where concentrated household bleach was available, a manual dilution method was followed for the preparation of the working SHS of the required strength (ie, 0.5%).
The present study showed the availability of compounding rooms in 5 of the 12 hospitals. However, except in one hospital where SHS was prepared in the dedicated compounding room, the preparations of the disinfectant solution in the rest of the hospitals were carried out in other rooms, corridors, and, in some cases, in toilets which were not convenient and difficult to adhere with the standard compounding practice. It was only in 3 hospitals where the preparation areas were properly ventilated which is necessary during handling of such chemicals.
During the preparation of the SHS in the studied hospitals, gaps were identified in that none of them did the dilution process by following the working document (ie, SOP), 91.7% did not check the starting household bleach for its usable shelf life, the strength of the undiluted and the working solutions, and none of them checked the dispensing container for the labeling information. This indicates the insufficiency of the disinfectant preparation to the standard practice. Generally, disinfectants must be used in the dilution specified by the manufacturer or reference documents for optimal decontamination and hence attention must be given to quality control activities as the germicidal activity of SHS depends on its concentration. Commercially available household bleaches with claimed potency of 3–5% are the main sources of concentrated SHS for the healthcare facilities in the country in which the strength of the disinfectant shall be verified with appropriate tests before dilution. Failing to verify the potency of the starting SHS may lead to an incorrect dilution that will affect the strength of the final working solution and its effectiveness. In addition, the working SHS of higher strength resulting from incorrect dilution may expose compounders and cleaners to this hazardous chemical during preparation and disinfection, respectively, if handled inappropriately. Three hospitals used to check the potency of the working SHS with chemical titration technique (1 hospital) and test strips (2 hospitals), but the majority did not conduct the test which could be due to the absence of a test strip in the domestic market which is a relatively simple testing method for checking the potency.
Moreover, the disinfectant containers should be labeled with the relevant information such as product name, strength, warnings, and expiry date to ensure that the right product is selected for the intended use. Labels should also show directions for users, which can be read clearly, to reduce improper use and prevent unnecessary chemical exposures.34 None of the hospitals read the labels for the information from the containers collected from the compounding unit. Lack of some of the malpractices observed in the preparation and QC activities by the public hospitals may be due to the use of the working solution at or around the preparation area immediately or within a short period after the preparation is over.
The SHS is generally unstable and the available chlorine concentration deteriorates with time if exposed to light and heat.35,36 Therefore, the SHS should be stored properly and used in the recommended usable time. The current study revealed that most of the hospitals (80%) complied with the storage requirements for the concentrated SHS products in that they were stored in cool, dry places, and protected from sunlight. Ideal SHS should be prepared fresh every day which otherwise needs to be tested for potency if used for days.37 With this aspect, all the public hospitals prepared and used the fresh SHS within a day for surface disinfection.
Another huge gap was also observed from the hospitals with regard to PPE use both in the preparation and disinfection time. When disinfecting a healthcare setting, WHO recommended to use, at minimum, rubber gloves, waterproof aprons, eye protection, medical masks, and closed shoes to protect against chemicals.38 Only one and two hospitals were found to wear the minimum PPE during the disinfectant preparation and use, respectively. Such inadequate implementation of good practice leads to the exposure of workers to chemicals and occupational risks. The domestic household bleach at its concentration (ie, 3–5%) may produce ocular irritation or oropharyngeal, esophageal, and gastric burns if handled inappropriately.33,39 A study done in the United States to characterize knowledge and practices of disinfection during the COVID-19 pandemic identified knowledge gaps in the safe preparation of disinfectant solutions, use of recommended PPE, and safe storage of disinfectants.26 When using chlorine-based disinfectants, the proper barrier protection should be used.40 The poor practice of wearing appropriate PPE in the investigated hospitals may be due to the shortage of PPE materials, lack of awareness of their potential benefits, or the health workers’ negligence. Insufficient PPE supplies for the workers in developing countries’ healthcare facilities were also reported elsewhere during the COVID-19 pandemic.40 WHO also reported that in response to COVID-19, countries allocated more budgets for the procurement of PPE, hand hygiene, and cleaning supplies.31
It is clearly indicated that GCP encompasses good documentation as standard of practice29 as it gives clear directions on the safe and precise practice of compounding and QC and other operations and minimizes the risk of errors. Appropriate documents should be maintained in a hospital compounding unit so that preparations can be replicated consistently and the safety of compounders is ensured.41 Majority of the hospitals in the current study had poor documentation, and it is only in very few hospitals that SOP for SHS preparation and QC activities were obtained. Caution must be exercised to avoid hazards with handling or using disinfectants. With respect to the availability of precautionary documents, none of the hospitals had such document for the safe handling, processing and use of SHS. This type of document usually contains information about health hazards associated with specific disinfectants and suggestions on how individuals can protect themselves against those health hazards while handling the products.42
Although the presence of a dedicated team in all hospitals for the preparation of SHS is a good start, the assignment of personnel with appropriate knowledge, skill, and experience for the practice is lacking and this personnel issue should not be overlooked. Though the preparation of SHS for surface disinfection purpose is simple and involves the dilution of the concentrated solution, basic knowledge and skill in compounding are essential to prepare quality products and protect oneself and the environment from unwanted chemical exposure. In this regard, the engagement of pharmacy professionals in the compounding service is an essential step towards strengthening the practice at the hospital level. It is only in one hospital that the SHS preparation was run by pharmacy professionals which may be due to the absence of compounding practice in most of the hospitals, as evidenced by the lack of compounding premises, where pharmacy professionals are mostly involved. Compounders in more than half of the study hospitals (58.3%) engaged in the preparation of SHS without taking training on GCP which might contribute to the substandard practices observed during the product preparations.
Even if the commonly used disinfectants meet the safety standards, if the instructions for their use are not followed correctly, they may be harmful to the health of workers. Therefore, before use, it is necessary to properly understand the method of use, precautions, and first-aid measures recommended for the disinfectant product.40 The disinfectant concentration and contact time are the two key variables determining the efficiency of disinfection using SHS.35 Items and surfaces must be exposed to the germicide for the appropriate minimum contact time using the correct potency of disinfectants. It is recommended to expose the items and surfaces to the SHS disinfectant for a minimum of 10 minutes to get the desired germicide effect28,40 though the contact time varies depending on the concentration of disinfectant and the nature of surfaces or items to be decontaminated. In half of the facilities (6 hospitals), the applied surfaces were wiped and back into business before the indicated contact time has passed.
Hypochlorites are known to have some disadvantages including corrosiveness to metals, inactivation by organic matter, discoloring or “bleaching” of fabrics, and release of toxic chlorine gas when mixed with ammonia or acid.35,39 Hence, to perform disinfecting operations effectively, it is necessary to understand both the chemical properties of sodium hypochlorite and the mechanisms by which microbes are killed.35 The interference of germicidal activity of SHS in the presence of organic matter emphasizes the importance of meticulous cleaning (with detergent or soap and water) as a pretreatment step to perform disinfection efficiently. All hospitals in the current study did not clean the environmental surfaces before applying the SHS which could have helped in reducing the microbial load on the contaminated surfaces. Moreover, it was only in 3 hospitals where disinfections were carried on non-metallic surfaces/items, but the disinfectant solution was applied on both metallic surfaces (like door handles and beds) and non-metallic surfaces in the rest of the hospitals. When applied on metallic surfaces repeatedly, the SHS may have negative results on the life of buildings and equipment. It is reported that some damages were observed on the hospital furniture, surgery tools, and equipment due to disinfection treatment by various chemicals.43 Hence, the selection of disinfectant type and its concentration should consider its damaging effects on the surfaces.
Moreover, while disinfection of the surfaces was undergone, rooms of 10 hospitals (83.3%) under the study were not well-ventilated. Disinfectant solutions should always be prepared and used in well-ventilated areas. When applying the SHS, the doors or windows should be left open, and fans can be used, if possible, to protect the operator from the chemical risk.28,38,44 Exposures to chemicals associated with increased use of disinfectants have also been reported in a literature due to improper use, not wearing protective gear, and applying in poorly ventilated areas.34
It is dangerous to use SHS inappropriately because the effectiveness of its performance can be overestimated. The chemicals should only be used after providing training to the workers to familiarize them with the required information.40 It is recommended that hospitals should provide training for cleaners and other staff in order to fully comply with the standard of practice required to disinfect SARS-CoV-2 on surfaces.35 The training has to be audited, and feedback should be obtained.
Regular disinfection of surfaces in hospitals is among the simple strategies to control the spread of COVID-19 and other HCAIs. In spite of the introduction of new disinfectants, due to the numerous advantages, the wide use of SHS is likely to continue in hospitals and other healthcare settings. Hence, considerable attention should be given to the preparation of this product and its appropriate use to maximize the benefits. Despite the challenges, the Ethiopian hospitals are facing during the COVID-19 pandemic, there is an urgent need to bridge the gaps identified in the preparation and use of disinfectants to ensure the quality of care and health workers’ safety.
Limitations of the Study
A single-time observation at the study settings may not reflect the real practice of the hospitals which makes the generalization of the findings difficult.
Conclusion
The preparation of SHS in the public hospitals did not comply with most of the requirements of GCP. Only one hospital verified the potency of concentrated SHS and 33.3% of the studied hospitals did not store this starting material in a proper place. It was only in one hospital that appropriate PPE was used properly, indicating that the operators in majority of the hospitals are at risk of exposure to hazardous chemicals. Moreover, majority of the hospitals lack the documents that are relevant for compounding operations, QC activities, and precautionary measures.
Similar negligence of standard practice was observed during the use of SHS for the surface disinfection in most of the studied hospitals. Only 3 hospitals applied the SHS only on non-metallic surfaces and none of the hospitals cleaned the surfaces before disinfection which could lower the germicidal effect of the product. In the majority hospitals (83.3%), the rooms were not well-ventilated during the application of SHS on surfaces. Cleaners in only 4 of the hospitals (33.3%) took formal training about the surface disinfection process.
In general, much has to be done in standardizing the compounding practice and use of SHS for surface disinfection in public hospitals to control the spread of COVID-19 and other HCAIs.
Recommendations
The health workers handling disinfectants should be informed about the potential work hazards and trained on associated safety practices, procedures, and protective measures.
The Ministry of Health-Ethiopia shall continuously assess the health facilities for the proper use of SHS for surface disinfection and provide feedback for the improvement of the practice. The Ethiopian Food and Drug Authority shall regularly inspect the hospitals’ compounding premises and their activities and provide guidance for compliance with regulatory standards.
Effective on-job training programs should be implemented for hospitals’ workers involving in the disinfectant solution preparation and surface disinfection to ensure the adherence to rational practices, especially during the COVID-19 pandemic. Additionally, to promote best practices, hospitals that showed good compounding and disinfection practices shall share their experiences to the other hospitals.
Data Sharing Statement
The datasets used for this publication can be obtained from the corresponding author on reasonable request.
Acknowledgments
We, the authors, would like to thank Addis Ababa University for funding this adaptive research. Our acknowledgment also goes to the Ministry of Health-Ethiopia for facilitation of this study. Finally, we are also grateful to all public hospitals in Addis Ababa for their permission and participation in the study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Funding
The financial support for the study was granted by the Research and Technology Transfer Office of Addis Ababa University from the competitive adaptive and problem-solving research grant.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Shimabukuro PMS, Duarte ML, Imoto AM, et al. Environmental cleaning to prevent COVID-19 infection. A rapid systematic review. Sao Paulo Med J. 2020;138:505–514.
2. To KK, Tsang OT, Yip CC, et al. Consistent detection of 2019 novel coronavirus in saliva. Clin Infect Dis. 2020;71:841–843. doi:10.1093/cid/ciaa149
3. Donskey CJ. Does improving surface cleaning and disinfection reduce health care-associated infections? Am J Infect Control. 2013;41(5 Suppl):S12–S19. doi:10.1016/j.ajic.2012.12.010
4. Hota B. Contamination, disinfection, and cross-colonization: are hospital surfaces reservoirs for nosocomial infection? Clin Infect Dis. 2004;39:1182–1189. doi:10.1086/424667
5. Mondelli MU, Colaneri M, Seminari EM, et al. Low risk of SARS-CoV-2 transmission by fomites in real-life conditions. Lancet Infect Dis. 2021;21(5):e112. doi:10.1016/S1473-3099(20)30678-2
6. Van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med. 2020;382(16):1564–1567. doi:10.1056/NEJMc2004973
7. Liu XY, Zhang Y, Tu HX, et al. Cleaning and disinfection in health care settings during the COVID-19 outbreak. Community Eye Health. 2020;33:36–37.
8. Abramowicz JS, Basseal JM. World federation for ultrasound in medicine and biology position statement: how to perform a safe ultrasound examination and clean equipment in the context of COVID-19. Ultrasound Med Biol. 2020;46:1821–1826. doi:10.1016/j.ultrasmedbio.2020.03.033
9. Rutala WA, Weber DJ. Guideline for disinfection and sterilization in healthcare facilities; 2008. Available from: https://www.cdc.gov/infectioncontrol/guidelines/disinfection/index.html.
10. World Health Organization. Improving infection prevention and control at the health facility: interim practical manual supporting implementation of the WHO guidelines on core components of infection prevention and control programmes; 2018. Available From: https://apps.who.int/iris/handle/10665/279788.
11. World Health Organization. Infection prevention and control during health care when novel coronavirus (nCoV) infection is suspected. Interim Guidance. 2020 Available From: https://www.who.int/publications/i/item/10665-331495.
12. Giam JA, McLachlan AJ, Krass I. Characterizing specialized compounding in community pharmacies. Res Social Adm Pharm. 2012;8:240–252. doi:10.1016/j.sapharm.2011.05.003
13. Masupye EM, Suleman F, Govender T. Investigating extemporaneous compounding practices in the Polokwane tertiary hospital pharmacies in South Africa - a pilot study. Afr J Pharmacy Pharmacol. 2015;9:1099–1105. doi:10.5897/AJPP2015.4282
14. Ong SWX, Tan YK, Chia PY, et al. Air, surface environmental, and personal protective equipment contamination by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA. 2020;323:1610–1612. doi:10.1001/jama.2020.3227
15. Ye G, Lin H, Chen S, et al. Environmental contamination of SARS-CoV-2 in healthcare premises. J Infect. 2020;81:e1–e5. 9. doi:10.1016/j.jinf.2020.04.034
16. Moore G, Rickard H, Stevenson D, et al. Detection of SARS-CoV-2 within the healthcare environment: a multi-centre study conducted during the first wave of the COVID-19 outbreak in England. J Hosp Infect. 2021;108:189–196. doi:10.1016/j.jhin.2020.11.024
17. Martins CPV, Xavier CSF, Cobrado L. Disinfection methods against SARS-CoV-2: a systematic review. J Hosp Infect. 2022;119:84–117. doi:10.1016/j.jhin.2021.07.014
18. Wang Y, Tian H, Zhang L, et al. Reduction of secondary transmission of SARS-CoV-2 in households by face mask use, disinfection and social distancing: a cohort study in Beijing, China. BMJ Glob Health. 2020;5(5):e002794. doi:10.1136/bmjgh-2020-002794
19. He M, Xiong J, Huang S, et al. Airborne precautions recommended in Wuhan, China for bedside fiberoptic bronchoscopy examination of patients with COVID-19. J Infect. 2020;81:e75–e77. doi:10.1016/j.jinf.2020.03.055
20. Sharafi SM, Ebrahimpour K, Nafez A. Environmental disinfection against COVID-19 in different areas of health care facilities: a review. Rev Environ Health. 2020;36:193–198. doi:10.1515/reveh-2020-0075
21. Rutala WA, Weber DJ. Selection and use of disinfectants in healthcare; 2004. Available from: https://basicmedicalkey.com/selection-and-use-of-disinfectants-in-healthcare/.
22. Mazzola PG, Jozala AF, Novaes LCDL, et al. Minimal inhibitory concentration (MIC) determination of disinfectant and/or sterilizing agents. Braz J Pharma Sci. 2009;45:241–248. doi:10.1590/S1984-82502009000200008
23. World Health Organization. Cleaning and disinfection of environmental surfaces in the context of COVID-19; 2020. Available From: https://www.who.int/publications/i/item/cleaning-and-disinfection-of-environmental-surfaces-inthe-context-of-covid-19.
24. Mitchell BG, Dancer SJ, Anderson M, et al. Risk of organism acquisition from prior room occupants: a systematic review and meta-analysis. J Hosp Infect. 2015;91:211–217. doi:10.1016/j.jhin.2015.08.005
25. Sitzlar B, Deshpande A, Fertelli D, et al. An environmental disinfection odyssey: evaluation of sequential interventions to improve disinfection of clostridium difficile isolation rooms. Infect Control Hosp Epidemiol. 2013;34:459–465. doi:10.1086/670217
26. Gharpure R, Hunter CM, Schnall AH, et al. Knowledge and practices regarding safe household cleaning and disinfection for COVID-19 prevention — United States, May 2020. Morb Mortality Wkly Report. 2020;69:705–709. doi:10.15585/mmwr.mm6923e2
27. World Health Organization Coronavirus (COVID-19) Dashboard. Available from: https://covid19.who.int/region/afro/country/et.
28. Ministry of Health - Ethiopia. Standard operating procedures for preparation of commonly used disinfectants against coronavirus (COVID-19): guidance for healthcare and non-healthcare facilities; 2020. Available From: https://e-library.moh.gov.et/library/wp-content/uploads/2021/07/Standard-Operating-Procedures-for-Preparation-of-Commonly-used-Disinfectants-and-Fumigants-against-Coronavirus-SARS-CoV-2.pdf.
29. Ministry of Health - Ethiopia. National Guideline for Compounding of Dermatological Preparations.
30. USP. (795). Pharmaceutical compounding - non sterile preparations; 2019. Available From: https://www.uspnf.com/sites/default/files/usp_pdf/EN/USPNF/revisions/gc795.pdf.
31. World Health Organization. Strategic preparedness, readiness and response plan to end the global COVID-19 emergency in 2022; 2022. Available from: https://www.who.int/publications/i/item/WHO-WHE-SPP-2022.1.
32. Tyan K, Levin A, Avalos-Pacheco A, et al. Considerations for the selection and use of disinfectants against SARS-CoV-2 in a health care setting. Open Forum Infect Dis. 2020;7:ofaa396. doi:10.1093/ofid/ofaa396
33. Federal Ministry of Health - Ethiopia. National Comprehensive Covid19 Management Handbook.
34. Chang A, Schnall AH, Law R, et al. Cleaning and disinfectant chemical exposures and temporal associations with COVID-19 - national poison data system, United States. MMWR Morb Mortality Wkly Rep. 2020;69:496–498. doi:10.15585/mmwr.mm6916e1
35. Fukuzaki S. Mechanisms of actions of sodium hypochlorite in cleaning and disinfection processes. Biocontrol Sci. 2006;11:147–157. doi:10.4265/bio.11.147
36. Clarkson RM, Moule AJ, Podlich HM. The shelf-life of sodium hypochlorite irrigating solutions. Aust Den J. 2001;46:269–276. doi:10.1111/j.1834-7819.2001.tb00291.x
37. Ghafoor D, Khan Z, Khan A, et al. Excessive use of disinfectants against COVID-19 posing a potential threat to living beings. Curr Res Toxicol. 2021;2:159–168. doi:10.1016/j.crtox.2021.02.008
38. World Health Organization. Coronavirus disease (COVID-19): cleaning and disinfecting surfaces in non-health care settings; 2022. Available from: https://www.who.int/news-room/questions-and-answers/item/coronavirus-disease-covid-19-cleaning-and-disinfecting-surfaces-in-non-health-care-settings.
39. Rutala WA, Weber DJ. Disinfection, sterilization, and control of hospital waste; 2015. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7099662/.
40. Rim KT. COVID‑19 pandemic and the protection of workers’ health from disinfectant chemicals. Toxicol Environ Health Sci. 2021;13:1–7. doi:10.1007/s13530-020-00077-z
41. McElhiney LF. Records and record-keeping for the hospital compounding pharmacist. Int J Pharm Compd. 2007;11:136–141.
42. Centers for Disease Control and Prevention. The National Institute for Occupational Safety and Health (NIOSH). Hazard communication for disinfectants used against viruses. Health Hazards and Protective Measures. Available from: file:///D:/AAU/Adaptive%20research%203/2014/REPORT/Disinfectants%20references/Hazard%20Communication%20for%20Disinfectants%20Used%20Against%20Viruses%20NIOSH%20CDC.html.
43. Mireles LK, Dayan J, Massicotte R, et al. Interactions of active compounds of disinfectants on metallic and polymeric hospital surfaces. Clin Med Invest. 2016;1:39–47.
44. Cleaning and disinfection. The Northern Ireland regional infection prevention and control manual. Available from: https://www.niinfectioncontrolmanual.net/cleaning-disinfection.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.