Back to Journals » Advances in Medical Education and Practice » Volume 14
Supporting Bystanders and Other Staff Exposed to Negative Workplace Behaviour: Developing and Testing the IMO Intervention Framework in the Clinical Workplace
Authors Gamble Blakey A ![]() , Anderson L, Smith-Han K
, Anderson L, Smith-Han K ![]() , Collins E, Berryman E, Wilkinson TJ
, Collins E, Berryman E, Wilkinson TJ ![]()
Received 22 June 2022
Accepted for publication 17 January 2023
Published 3 February 2023 Volume 2023:14 Pages 71—86
DOI https://doi.org/10.2147/AMEP.S379429
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Md Anwarul Azim Majumder
Althea Gamble Blakey,1 Lynley Anderson,2 Kelby Smith-Han,3 Emma Collins,4 Elizabeth Berryman,5 Tim J Wilkinson1
1Otago Medical School, University of Otago, Dunedin, New Zealand; 2Bioethics Centre, University of Otago, Dunedin, New Zealand; 3Medical Education Unit, University of Western Australia, Perth, Australia; 4Department of Women’s and Children’s Health, University of Otago, Dunedin, New Zealand; 5Chnnl Limited, Auckland, New Zealand
Correspondence: Althea Gamble Blakey, Otago Medical School, University of Otago, Sayers Building, Dunedin, New Zealand, Email [email protected]
Background: Medical student and health-care staff bullying remain international concerns. Our understanding about what might solve such problems is still developing. A common approach suggested for bystanders to bullying is that they challenge or “stand up” to the bully. At the same time, the considerable risks should they act (eg, verbal rebuke) are rarely acknowledged, and neither is the potential for considerable cognitive dissonance should they choose not to.
Methods: Drawing on a substantial literature review, we developed an interventional program, initially with medical student bullying in mind, that generally employed a discourse for values cultivation. We implemented and evaluated this program through 6 cycles of action research methodology in 6 different departments of one tertiary teaching hospital. Data include individual interviews, discussions with key participants plus freehand comments from wider staff’s workshop evaluations.
Results: Alongside others, an early serendipitous finding was the “IMO” [Indirect, focus on Me, focus on Outcome] framework, intended for bystanders to student bullying. From using this framework, participants reported developing confidence in tackling negative behaviours, that interactions had better outcomes and that the workplace atmosphere felt more relaxed. It’s use also significantly reduced cognitive dissonance. Encouragingly, participants went on to use IMO for staff–staff bullying incidents, and other common negative behaviours. We attribute IMO’s utility to its memorability, simplicity and for catering to the many possible causes of bullying, including values issues, without perpetuating or creating conflict.
Conclusion: The IMO framework is offered as a widely usable framework for all staff in a clinical environment – a useful addition to popular frameworks used in the clinical workplace, ideas from which might also help these be further refined. Further evaluation would establish whether IMO invites long-term change and its utility in other contexts.
Keywords: bullying, bystander, clinical environment, framework, IMO, intervention, medical student, onlooker, verbal
Plain Language Summary
Medical student and health-care staff bullying is a big problem and bystanders seldom know what to do about it. Those “standing up” to a bully risk being bullied themselves, and those who do not can experience stress around failing to help.
We designed and tested a program to help stop medical student bullying based on suggestions made in the literature. During the program, we identified a way of speaking to a potential bully which helps the bystander feel safer and more empowered to act. We taught this method to subsequent participants who reported it to be useful for bullying and other negative behaviours, with all staff and students. The “IMO” framework [Indirect, focus on Me, focus on Outcome] also seemed to improve workplace “atmosphere”.
We think IMO is useful because it is memorable and simple to use under stress, and caters for the many possible causes of bullying without creating further conflict.
We recommend IMO for use in the clinical workplace and to potentially offer a way to improve other common mnemonics. We would like to keep testing IMO with different kinds of workplaces, staff and students, to see if it changes work satisfaction, overall atmosphere and long-term bullying rates.
Background
In response to continuing worldwide and local concern about the prevalence of medical student bullying, and our own experiences in clinical practice, we undertook a research project aimed at creating a more positive learning environment. This is particularly because the effects of student and staff bullying may extend across a workforce to adversely affect physical and mental health, learning, teamwork, patient care, outcomes and efficiency.1 Among several useful findings, we identified the need for a verbal framework/tool to assist the bullying bystander. A verbal framework (the “IMO” framework: Indirect, focus on Me, focus on Outcome) was constructed from participant and researcher contributions, polished and tested, primarily for use by bystanders to staff-student bullying. Ultimately, we hoped to produce a method by which the bystander might also facilitate positive change in wider aspects of work.
However, during the research, the IMO framework was also found to be useful in other common, challenging situations, such as staff–staff conflict. Our research context and focus thus broadened to testing this framework with all participant staff members in our selected workplaces, and in relation to all workplace interactions.
We acknowledge that the effects of student and staff bullying may extend across a workforce to adversely affect physical and mental health, learning, teamwork, patient care, outcomes and efficiency.1 The nature of, and effects of such interactions are not the focus of this paper. Rather, this paper’s focus is the reasoning for the framework’s development and its testing and evaluation over six action research cycles, each in a different clinical area of one tertiary hospital.
Defining Terms
Currently, there is no widely accepted definition of what constitutes workplace bullying. We use a definition which specifically references the learner, an important stakeholder in our research context. Formal and informal learners represent a considerable proportion of staff in most clinical workplaces; thus, we continue to reference this definition despite our widened research focus. In summary, that intentional or unintentional bullying can happen where a person behaves in ways that are disrespectful of the dignity of others or, for learners in the workplace, that interfere with the processes of learning. Examples might include:
Sexual harassment; discrimination or harassment based on race, religion, ethnicity, gender, or sexual orientation; humiliation; psychological or physical punishment; and the use of grading and other forms of assessment in a punitive manner.2
The Bystander
The bystander, the focus of the intervention in this paper, can witness students or other staff being bullied/on the receiving end of other negative behaviours. Because a bystander’s actions can significantly influence the outcome of such acts,3 the bystander (“witness” or “onlooker”)4 is thus another important stakeholder in these events. At the same time, the bystander might risk many other adverse outcomes. The bystander might:
- Exacerbate a situation, eg, by drawing negative attention to the bully, whose behaviour then worsens;5
- Cause a distraction, further endangering patient safety;6
- Become an acute bullying target, eg, suffer verbal rebuke;7
- Become a longer-term target, eg, by marginalisation.8
Risks to the bystander can also be exacerbated where the alleged bully is their senior3,9,11 and where increased professional and social networks allow retributional acts to extend outside of the direct workplace context, eg, via stymied career progression.8,10 It has been said that at worst, an intervening bystander might suffer treatment comparable with that of the primary victim.12
Despite the potential risks of such actions, a portion of the literature advising the bystander suggests the bystander confront the apparent bully, eg, by challenging or “speaking out” to them in the moment.13 Similar advice is found in legislative documentation, professional practice guidelines10,14,15 and media-popular drives such as “Stand up and Speak out against bullying”16 and the ubiquitous “Pink Shirt Day” campaign (see www.pinkshirtday.org.nz). Such advice might sound positive, and assuage compunction to act against these difficult behaviours, but it also fails to acknowledge the presence of the myriad of potential concomitant risks when doing so. Because media around these kinds of “interventions” is often very visible to health-care staff, their overall influence on the bystander can be significant.
Cognitive Dissonance
One option for the bystander to bullying is to stay silent.16–18 However, even when doing this, the bystander may continue to suffer, as it is likely they experience cognitive dissonance as a result of their silence. This phenomenon – of strong, coexistent, contrasting emotion or desire about a central issue – can be distressing and compromise a person’s health and wellbeing in the short and long term.19 Where witnessing a bullying incident, cognitive dissonance might emanate from a bystander experiencing a strong compulsion to help the victim, but at the same time experiencing intense fear of the risks and dangers of doing so. Thus, we become mindful of implications of fault or blame directed at the bystander who does not act:
…doing nothing makes you part of the problem.20
The real problem is that those who observe deviations or infractions say nothing.21
Such statements may be made with positive intent and driven by a compulsion to act. However, we suggest that rather than representing a “call to arms”, such statements may instead contribute further to bystanders’ mental distress. This distress may result from an implicit implication of blame levied at the bystander, understood as a personal attack. As such, such an implication might be considered a bullying act in its own right. Such actions are unhelpful and damaging, but also fundamentally incompatible with our aim to cultivate positive workplace behaviour.
So, effectively and safely ameliorating apparent bullying incidents “in progress” might mean a bystander faces a tough, threefold remit: helping the victim acutely, minimising, eliminating or managing the many associated risks, plus resolving their cognitive dissonance. The IMO framework was developed with such situations in mind. We describe how this framework came about, evaluate its utility in the clinical workplace, discuss why it seems to work, and suggest its possible contributions to the field.
A Summary Understanding of IMO
It is important for the reader to gain a foundational understanding of the verbal framework discussed here. Rather than describing our overall intervention program, we discuss the development, testing and evaluation of a specific verbal framework for use “in the moment” by bystanders to negative behaviour.
IMO is a mnemonic, each letter representing a sentence portion and how it is formulated. Another way to understand IMO is three foci needing to be present in a sentence, while avoiding contrasting foci. Letters were chosen for function, humour and memorability – colloquially, “IMO” can mean “in my opinion”. The following Table 1 is a useful summary of IMO meaning:
 |
Table 1 IMO Meaning |
Worked Example
A doctor seems to be excluding one specific student from viewing a procedure, perhaps enacting racist values (or, alternatively, too busy to attend to a shy student, etc). A bystander using IMO might respond:
Hang on (I), if we (M) bring everyone around this side, we can all get a good view (O). Alternatively:
Let us check in (I) to see who has not (M) seen this procedure yet, come over if you need to see one (O).
These sentences are IMO sentences because the bystander approaches the situation indirectly, as a suggestion (I) rather than a way likely to incite conflict. Their focus is on the wider team and students, rather than the doctor (M) and on a positive aim, helping everyone learn, also avoiding drawing attention to the doctor’s apparent negative behaviour.
Method
Action research (AR) methodology is suitable for raising and addressing questions about practice and can also help raise research questions distinct from primary questions proposed at its outset.22 AR also allows the development, testing and evaluation of solutions in practical contexts and multiple opportunities to hone these over subsequent cycles.22–24 For this research, we undertook six formal cycles, named 1–6 in the text, one after the other, each in a different health-care setting in the same hospital. Research began in 2017, with one cycle every approx. 9 months and was called “The CAPLE Project” [Creating A Positive Learning Environment].25–29
Our initial research focus was to seek ways to best ameliorate student bullying in clinical workplaces. Based on the results of an extensive literature review,25 a skeleton “approach” and workshop program was developed, which employed adult learning methods: discussion-based, non-didactic, active learning strategies and participant responsive discussion around a selected topic. After cycles 1 and 2, IMO was introduced as part of these workshops, in relation to each central topic.
The initial general focus of our intervention was on preventative, positive development of long-term healthy behaviours within the teacher–learner interface, eg, how to offer effective feedback, together with a focus on effective values within this remit – such as how exactly to phrase this feedback for it to be valuable, and non-deleterious to student learning.
Selection of Clinical Workplace, Participant Criteria and Recruitment
Six different clinical workplaces in one tertiary teaching hospital were selected by simple virtue of allowing us access. We first obtained the relevant clinical leader’s verbal consent and then undertook formal research access policies. We also aimed to cover a range of hospital-based settings where medical students were placed. There was no requirement for an identified bullying problem in any workplace: preparatory work led us to understand that reported and unreported bullying was likely to be present in most settings. Criteria for key participants for each cycle were to be employed in the area in question and qualified healthcare or administration staff (who often have considerable student contact). We aimed to recruit 12 “key” participants from various denominations (medicine, nursing, administration having clinical contact, etc.) for each cycle, as well as surveying and workshopping wider staff.
Recruitment entailed asking clinical leaders to email information sheets to all staff, introducing the research. Potential “key” participants were invited to contact the interventionist-researcher (IR) to ask further questions, after which formal consent was sought in person. Staff attending workshops (between 8 and 20 staff at each) but not taking part as “key” participants were consented at the time, to allow us to access their paper evaluation of the workshop. An information sheet was provided to indicate that filling out the evaluation would be indicative of consent to use information as research data.
Specific Ethical and Methodological Considerations
Prior experience made us mindful of this topic’s sensitivity, which played out in our preparatory interactions with management and other staff. Specifically, that our approach should avoid a department, profession or staff group feeling “targeted.” Instead, we carefully framed the intervention as a gratis staff development and research opportunity.25,30
Another concern was about the close relationship between the IR and participants. While advantageous for gathering sensitive data, such a relationship might at the same time preclude participants from offering negative, but important feedback, particularly around the IRs facilitation skills or discussions about values. Thus, for cycles 3 and 4, a second IR (KSH) repeated participants’ final interviews to determine whether any such comments had been withheld – there were none.
We also felt concerned that research participants may recall, or reveal unanticipated, sensitive issues. To counter this, and as reassurance, the IR repeatedly raised issues of confidentiality, of participants’ ability to view and rescind any comment (eg, from an interview transcript) and, importantly, the availability of institutional counselling and support services.
Ethical Approval
The CAPLE Project was granted access to the healthcare institutions concerned via formal locality access processes as well as receiving ethical approval from the research institution.
Interventionist- Researcher (IR) Expertise and Research Positioning
The interventionist-researcher was the primary author, a tertiary clinical teacher with over 30 years’ experience in clinical practice, small group teaching, and research in medicine and allied health sciences. The IR also undertook the foundational literature review and program design, supported by the research team. The IR was also the primary author for the values discourse28 employed in this research, described later in this paper. This person was not an employee of the hospital in which research was undertaken.
As can be usual for action research, the interventionist-researcher contributed data additional to that gathered from participants.22 In this case, from the point of view of facilitating workshops, summing up discussions and in formal individual interviews. While we principally focus on participants’ experiences, we necessarily include IR comments where valuable or in the case that data would benefit fuller contextualisation.
Data Type and Collection
Data from key participants comprised:
- Individual entry/exit interviews (approx. 40 min, semi-structured, audio recorded, in a convenient and private workplace setting) about teaching and learning and related challenging workplace behaviours. As is usual with semi-structured interviews, the interviewer began with an open question, and developed subsequent questions reflexively, around the respondents’ reply. In this case, the research began by the IR asking an open question about how the participant found the workplace “atmosphere;”
- IR reflective journal about experiences teaching workshops, discussions with staff about workplace behaviour and field notes, eg, about what worked in workshops;
- IR email conversations with participants (casual).
- Hardcopy workshop evaluations (only freehand comments used for the current paper).
Data from other participants comprised only the latter source, of which only the workshop evaluation freehand comments were used for the current report (Q3: What did you get out of the workshop? Please explain).
The IMO framework was developed during, and after cycles 1 and 2 and purposefully included in each workshop in cycles 3–6. We thus report some data from cycles 1 and 2, but mostly drawn from cycles 3–6.
Data Analysis
Free-text comments and interview audio recordings (transcribed verbatim) were analysed with an iterative thematic method27 by the IR, reviewed by KSH & other research team members at monthly research meetings. Any theme or detail apparently unclear or open to misinterpretation were checked against hard copy, or if possible with the participant concerned.
As part of this analysis, data from workshop evaluations and interview transcripts were searched for words relevant to IMO, as this foundational “theme” developed after the deliberate introduction of IMO into the program.
Workshop Content, Teaching Methods and Structure
In each cycle, we offered a series of five 40-min active learning workshops, framed as upskilling in teaching and learning,24 including relevant values/behaviours.26 Content was tailored to common issues, determined by pre-intervention research26–30 and specific, perhaps values-related issues captured during participants’ individual interviews. For example, where we understood that staff/students were being offered feedback in verbally negative ways, in the “Effective Feedback” workshop we included a discussion about potential pitfalls with offering feedback, and the idea that empathy needs to be enacted within the process of doing so. Other topics included “Effective relationship for learning”, “Creating welcome in learning”, “Dealing with learner fear and anxiety” and “Developing thinking in learning”.
Workshops were held once a week in an in-house seminar room/ward space allowing staff to rapidly attend to clinical needs if required. We aimed for all staff to participate in all five workshops, but key participants rostered to attend as a priority. To cater to those unavailable/called away, workshops were offered again later in the day/week.
In all workshops, the IR also employed the specific discourse28 aiming to expedite reflection on and development of issues around values and related behaviour. This discourse was also employed in ongoing communication with key participants, on the understanding that values issues were likely to be raised and that participants effective engagement in such discussions, even casually, might be challenging.28
Each workshop began with a simple theoretical discussion (eg, what is feedback? What are its essential features? What are the pitfalls when offering feedback?). Staff were then introduced to the IMO framework and a worked example then asked to apply IMO to a workplace scenario in which bullying seemed evident. For example, how might IMO be used where witnessing a student verbally abused during a feedback session? Staff worked on scenarios in pairs, presented IMO sentences to the group and were invited to critique and explore each other’s offerings.
Results
In this section, we report on the evolution of IMO as part of cycles 1 and 2 and its testing and evaluation in the following cycles of the research. We report data relevant to IMO in three main themes, together with subthemes, summarized in this Table 2 for ease:
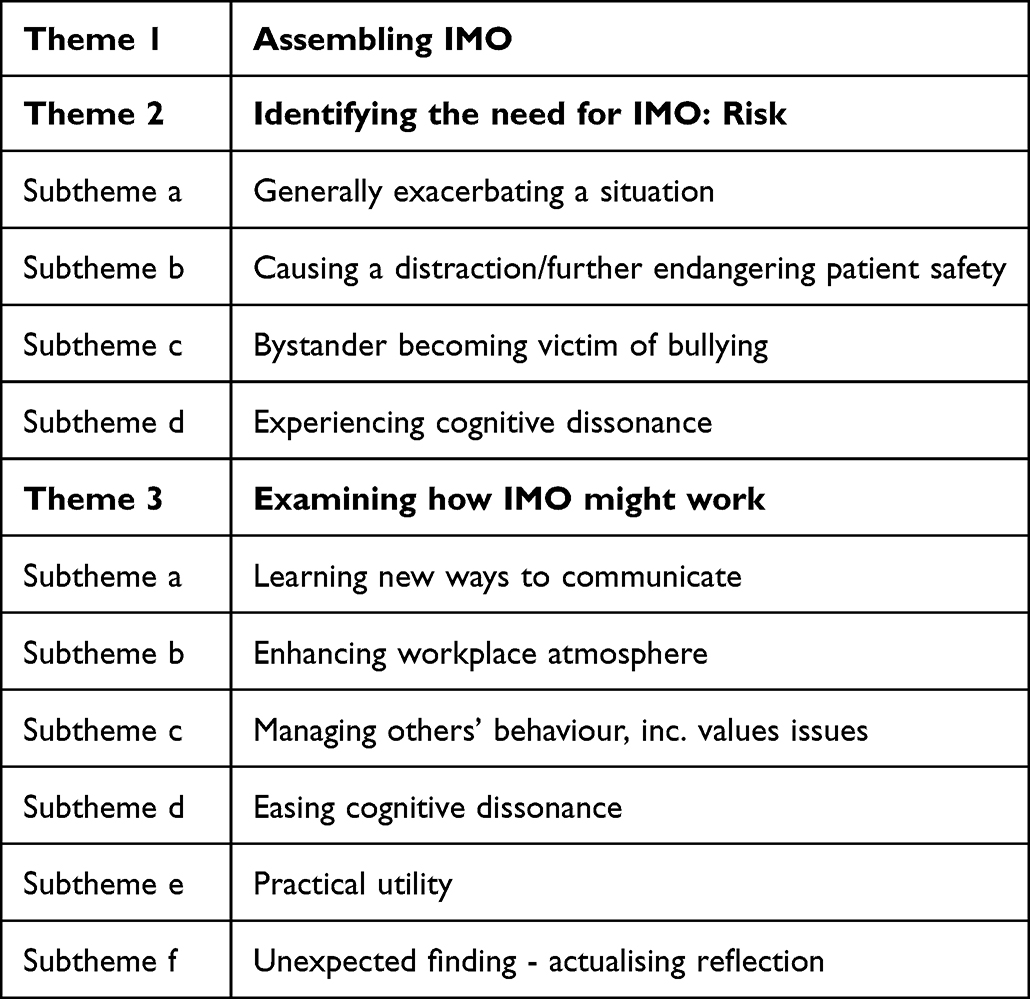 |
Table 2 Summary of Themes and Sub-Themes from Data |
We report empirical data using quotes or paraphrase, where representative or efficient to do so, identified by source: cycle (1–6), data collection method, participant (P1, 2…) or interventionist-researcher (IR).
Theme 1 Assembling IMO – Best Guess
During cycles 1 and 2, participants’ comments focused on what they thought of our general intervention approach and workshops. The idea for IMO developed from brief staff discussions and workshop comments in these cycles around wanting to help students (and more latterly other staff) apparently being bullied.
These brief comments were assembled into IMO by the IR in a “best guess”. These included words such as those found in column 1 in the following Table 3. Column 2 in the table shows the “letter” these became in the IMO framework itself: (Participant interviews, field notes and email discussions, cycles 1 and 2).
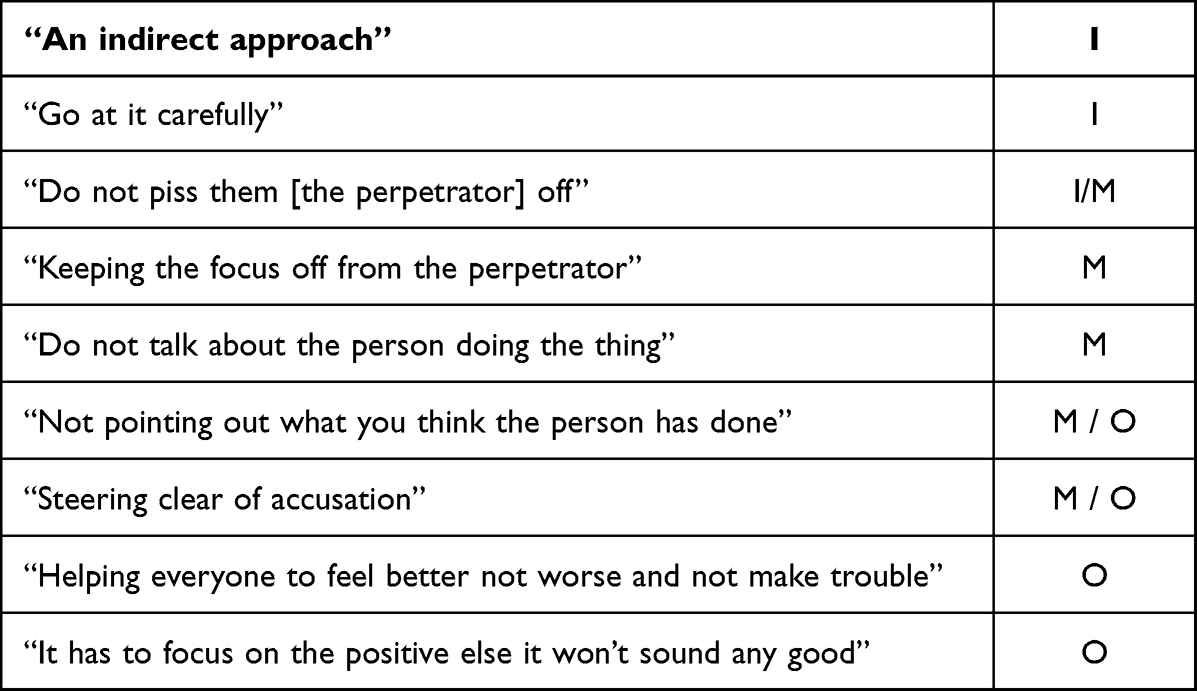 |
Table 3 Assembling IMO |
While many of these words might also be described under theme 3, examining how IMO might work, it is important to acknowledge the origins of IMO development from informal, and formal conversations during research periods. As can be seen, one or two IMO characteristics might be covered by the same phrase.
Following these discussions, the IR reflected on the judicious preparation that such a bystander framework might require:
It’s [IMO] going to have to approach things very, very carefully.
(IR, reflective journal, early CAPLE 2)
Theme 2: Why IMO Was Developed: Risk
All participant groups seemed to contain staff who had wanted to intervene in situations, but had not. Central to this reluctance was an apparent appreciation of the many potential risks in doing so, and the ensuing need for their words to cater to those. Specific risks reported were:
Subtheme a: Generally Exacerbating a Situation
P1 discussed how speaking out would need considerable thought, because bullying incidents can have unpredictable, negative outcomes:
P1:It’s [acting as a bystander] not something you have a go at lightly, I will say that. …You never know what might happen. All manner of things can go wrong.
(CAPLE 4 post workshop discussion)
Subtheme b: Causing a Distraction/Further Endangering Patient Safety
Participants also understood that any action taken to assist a “bullied” student or staff member in the moment should mindfully protect the patient, as a matter of professional responsibility:
P1:…the point is that you need to get past what it is they [the apparent bully] are banging on about [saying] and you need to help the person in their sights [their target] and get the clinical stuff done, out the door, and safely. That’s our job.
(P1 interview, post CAPLE 4)
Subtheme c: Bystander Becoming Victim of Bullying
Similarly, participants understood the potential for the apparent bully to seek retribution if intervention was done “wrong”, perhaps for the bystander to be bullied at a later date:
IR:Do not give them [the apparent bully] anything to “get you” with. It’s got to be respectful, to the point, and do not make a scene else you will “get it” [be bullied] next time. Or in your performance review.
P2:Hell yes. I have heard of that happening, it was someone I know. It did not end well.
(CAPLE 4, field notes)
Subtheme d: Experiencing Cognitive Dissonance
Participants also reported the risk that they experience cognitive dissonance when witnessing workplace bullying and how this had a deleterious effect on themselves and the workplace atmosphere. P3 described how learning about, and using IMO helped relieve this sensation and change the “feel” in the room. This report was among several which encouraged the research team to focus on interactions in the workplace outside that of staff-student:
P3:…bloody painful, that’s what it is and it’s in your head. We stand around while the atmosphere gets worse and worse and we do not know what to do.
(P3 interview, post CAPLE 4)
Theme 3: Examining How IMO Might Work
IMO’s popularity was identified in several data sources: workshop evaluation freehand comments, post workshop discussions and final participant interviews, which made sense, as at that time participants had had opportunity to learn, use, test and think about how IMO might work.
Over CAPLE 3–6 we gathered 71 positive comments about IMO from Question 3 “What did you get out of the workshop?” The few negative comments all centred around wanting more time to practice IMO, which we went on to address by repeating IMO for every workshop in the program and also practicing it with participants in one-on-one discussion about specific personal issues.
However, participant data revealed much thought around how IMO might work:
Subtheme a: Learning New Ways to Communicate
Essentially, IMO seemed to offer participants a “new” way to communicate. Many comments seemed enthusiastic about learning this “new way”, to include how they valued being able to listen to and critique the attempts of others as they learned IMO:
So glad to have a new way to talk to people in tough situations
I like working through the IMO statements so that here are particular phrases I can draw upon
[IMO] Opens my eyes (to) communication in its different forms, how it can affect others
It was great to hear of different ways that other people have dealt with/managed feedback in particular situations
It has been great listening to others who created great IMO questions (arrow up) - learnt from those!
Subtheme b: Enhancing Workplace Atmosphere
As they began to hear IMO being used by colleagues in more “ordinary” situations, participants also reported feeling an apparent positive change in workplace atmosphere. This finding pointed to the potential for IMO’s use in a wider range of situations than simply as bystanders to student bullying, our initial aim:
IR:Since CAPLE was here, have you seen anything specific being used, like, the things that we talked about in the groups, about how to approach people who were being yuck with feedback and that kind of thing?
P6:Just the way the people are not just going off and getting upset they are saying … what’s up with you today – in a nice way though…the way people are relating to each other …asking the person what’s up and trying to help the situation and have a way out for everyone.
Later in the conversation…
P6:Yes, I have, I have seen it particularly being used within the CAPLE team and how they discuss things with each other - now instead of having a conversation within themselves afterwards and bitching about someone in the team, saying something like she was a bit snippy wasn’t she, they will say to the actual person something … straight away … people are no longer going away and being unhappy…the way that people are relating to each other is changing…
(P6 post-interview CAPLE 4)
Subtheme c: Managing Others’ Behaviour, Inc. Values Issues
The words of P4 suggest an understanding that IMO works by way of managing others’ behaviour: “You’re essentially managing other people, are not you?” which suggests an operational, follow on, perhaps guiding element to IMO that would likely be missing from more confrontational approaches.
P4 goes on to describe their maiden attempt using IMO in practice:
P4:It [the IMO framework] gave me something to do, something to hang my words on, get started and be more sure that I would not make things worse [their emphases]. You are essentially managing other people, are not you? And sometimes ahead of time or just-in-case, but helping one of them [the victim], and that feels good.
(P4 interview, post CAPLE 4)
How exactly this “management” might happen seems to be two fold. First, that IMO is somewhat “circumspect” in its approach – it’s use avoids confrontation and thus does not imply that what is happening is intended to be negative – and at the same time also caters to the possibility that the perpetrator might be acting on negative values.
The IR summarises participants’ apparent understanding that a potential bully may be acting out values issues in their workplace behaviour. As such issues can be difficult to effectively address, any framework for use in such circumstances would need to tackle such issues – perhaps thinking of values issues as a “worst case scenario”:
IR:What everyone seems to be telling me about IMO is that it can be about values for the person doing the bullying. If this is true, and I guess it’s common enough, as well as those who are just inept, and then we have to be able to cater to both cases without knowing fully [whether the person is actually “a bully”]. So it’s about values dialogue, maybe, like a lot of the ways I teach in the workshops. Let us hope it is, we might be onto something.
(IR Reflective journal, post CAPLE 3)
P5:I think without something like that [IMO] you’d have fat chance of getting anyone to change their ways. It’s their belief system is not it and just telling them off or putting up posters will not help that kind of thing, but I reckon this has a chance, once we have learned it enough.
(P5 interview, post CAPLE 5)
Subtheme d: Easing Cognitive Dissonance
It’s good to have something up your sleeve, finally, to be able to say something that doesn’t make you feel worse.
(P6 interview, post CAPLE 4)
Subtheme e: Practical Utility
Participants also indicated that IMO framework worked because of its practicality. They elaborated on this, and remarked that IMO’s inherent simplicity, ease of learning (with a little practice) flexibility and general utility around their workplace context were key to its effective use. Here, IMO is described comparatively:
P7:I did the Crucial Conversations course and it was very complicated, drove me a bit mad. Did not seem to have much content that I could take and use tomorrow, if you see what I mean. It was more about board-room stuff, you know, management stuff, not the things we see around here, you know, bolshie [defiant/rude] doctors and such. This one [IMO] is the opposite. It covers loads of different things and it’s bloody useful.
(P7 interview, post CAPLE 5)
Subtheme f: Unexpected Finding - Participant Reflection
Data also suggest the process of learning and using IMO helped participants reflect on their own behaviour, especially its effect on others. For example, in a workshop discussion, P8 offered a worked example of an IMO phrase, their colleague then offering an opinion of how this might sound. In response, P8 reflected on the effect of their words, specifically on their reference to “me or us” (M) rather than the perpetrator:
P8:…does it really? Goodness, I’d never thought about that. Is it better to say “let’s try to get a good picture of what’s going on?” What do you think? Shall I change it? It is better because it’s about me, or us, really is not it [referring to the “M”]?
(Field notes, CAPLE 4)
Discussion
Principal Findings
To reiterate, IMO was a serendipitous finding allowed by our action research methodology. As we continued, the research question also became clear, in 3 parts: What are the requirements of a verbal framework for use in bystander situations to negative behaviours? What is the utility of IMO for bystander staff when responding to bullying and other negative behaviours in the clinical environment? How does IMO work?
Criteria to determine IMO’s utility are provided by the challenges experienced and perceived by our participants. Whilst often in the minority, these challenges have begun to be noted in the literature, although rarely in texts recommending a “Stand up” approach. Compiling these, the IMO framework needed to:
- Assist the apparent bully’s primary victim(s).
- Minimise/avoid risk (exacerbating a situation, causing a distraction and further endangering patient safety, bystander becoming a target).
- Ease the bystander’s cognitive dissonance.
- Allow for the many possible causes of bullying behaviour, esp. values issues.
By virtue of the clinical context, in which clinical staff had limited ability to attend staff development opportunities, and acknowledge the limitations of other frameworks aimed to assist with difficult workplace behaviours, IMO should also be judged against criteria to be:
- Teachable and learnable in the clinical workplace.
- Appropriate to practice situations.
We now examine how we thought IMO fulfilled these and compare it with other popular frameworks suggested for the clinical workplace.
On criterion 1, data specifically about bullying victims’ experiences of IMO are not available but we are encouraged by participants’ developing confidence, documented in final interviews and positive workshop evaluation comments.
Confidence might be understood as indicative of vicarious “success” on the part of the bullying victim, as staff would be unlikely to report improved confidence if IMO had not gone well. We are also encouraged by reports that participants had begun to employ IMO when they, themselves, experienced negative behaviour (eg, staff-staff conflict) and that a general improvement in atmosphere followed. On the basis of these promising results, we suggest gathering further detailed accounts from victims where colleagues have used IMO. For this sensitive task, we propose returning to clinical areas studied in CAPLE to build on pre-existing positive relationships.
Criterion 2 is catered for by participants’ reports that they understood bullying incidents broadly as a kind of conflict. This explains why a generally non-confrontational behaviour management approach seemed useful and how each element of the IMO framework could be understood to contribute to conflict reduction. Specifically, avoiding words that might incite conflict. For example, opening with “I” (indirect approach) avoids inciting self-protective “knee-jerk” counter-confrontation; M (focus on me/we/team) avoids acute and chronic conflict via public accusation; O (positive outcome) avoids shaming a potential bully publicly, another potential conflict situation. We received no reports of acute or medium term interpersonal “fallout” from using IMO, which is encouraging, and suggest gathering data about long term effects of using IMO to add confidence to this picture, eg, whether bystanders felt disadvantaged by having intervened, or whether error rates changed in areas where IMO is used.
Further to understanding IMO as a conflict resolution approach, we find other support in the literature. For example, that positive, outcome-based solutions (“O”) are upheld in the field of workplace conflict, acknowledged to reduce an intervening person’s long-term psychological burden31 - perhaps that we describe as Criterion 3, “cognitive dissonance”. “Positive” approaches to workplace difficulties are also recommended as a way to reduce overall stress levels, climate and enhance workplace efficiency,34,35 explaining perhaps IMO’s association with improved workplace atmosphere.
Criterion 4 is that IMO needs to cater to potential (and usually unknown) causes of bullying behaviour. In summary, from our literature review25 common causes are:
- Personal factors, eg, stress.
- Being bullied/feeling bullied oneself.
- Challenging work/environment.
- Personal values.
- Inherited behaviour.
- Lack of skill (eg, in communication, or teaching).
Examining these potential causes, we suggest IMO works thus: Point a: IMO avoids putting pressure on a person acting negatively due to personal factors, eg, stress, instead calmly inviting solution-focused conversation. Point c avoids distracting a person responding to a challenging work environment, but rather offers a positive, helpful fait accompli. A person bullying because of their own experiences of being bullied, or having “inherited” a behaviour (Points b and e) would not have past experiences compounded, but are instead modelled positive behaviours avoiding “calling them out” or causing embarrassment.35 A person bullying due to lack of teaching skill (Point f) is also offered and modelled a positive solution, rather than given a shameful experience.
Handling personal values-issues (Point d) is acknowledged by both IR and participants as the most demanding to effectively negotiate. Authors of work around values in clinical practice note these demands. Specifically, they acknowledge that “pointing out” flawed/negative values can be interpreted as criticising “who someone is”, and a source of further counter-conflict or reactionary negative behaviour. Instead, authors recommend the skilled use of language to encourage a person towards reflection and values cultivation,28,36 as deliberately done in CAPLE.
Examining IMO we find evidence of language similar to the discourse for values cultivation (DVC) instigated by the IR in the project more generally.28 Such a similarity seems to bode well for the efficacy of this discourse as an operational framework in bullying intervention and the use of IMO, and the DVC more generally, eg, around issues of professionalism. We were able to identify two pedagogic strategies from the DVC in the current project, which we demonstrate in the following Table 4:
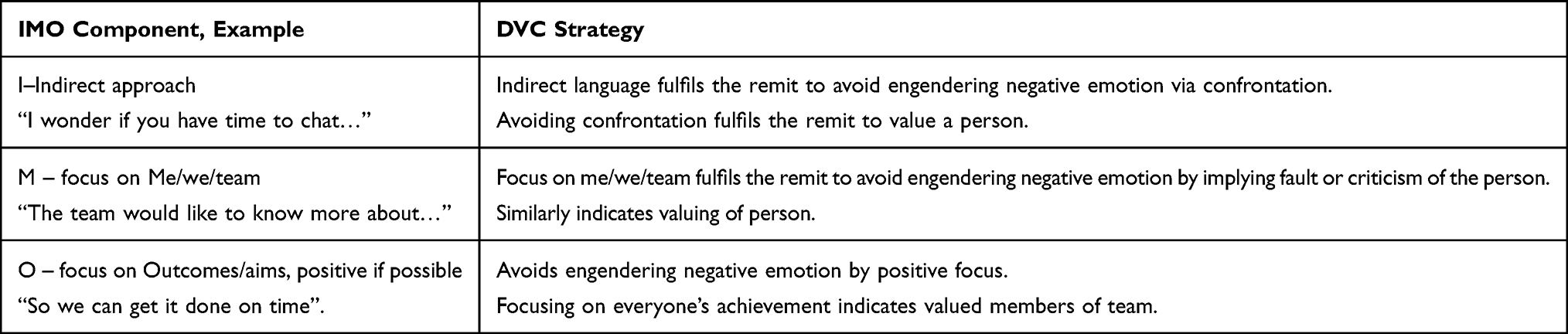 |
Table 4 IMO & the Discourse for Values Cultivation (Summarised from Interventionist-Researcher’s Notes During CAPLE 3 Workshops & Gamble Blakey & Pickering, 201828) |
Strategy 1: Framing language about values to avoid engendering negative emotion.
Strategy 2: Demonstrating the values of belief in a person and valuing them.
That IMO caters to values-issues is important. Participants described the difficulties in knowing why a potential bully acted as they did. Determining what to do would thus be challenging, but repercussions if values issues not tackled well could be extremely negative. Making a positive contribution to an apparent bullying situation might thus depend on using an IMO approach as a matter of course, a coverall in case the issue is about personal values. In summary: It’s also got to cater to anything, really…It might be a values- beliefs thing.
(P5, interview, post CAPLE 4).
Criteria 6 and 7 essentially involve the selection of a pedagogy congruent with teaching IMO, a practical skill requiring thought and critique to master, to the adult learner in a complex and busy environment. Before we undertook the intervention, we understood that much of our teaching would not be a matter of providing a written resource or a lecture; didactic and other more passive teaching methods frequently lack efficacy for many adult learners, especially those aiming to develop a practical skill or behaviour.37 As well as instigating an active learning pedagogy (discussion, critique, etc.) suitable for adult learners we carefully created a place for participants to safely and consistently practise that which is being learned. Cognitive “rehearsal” and learning to frame speech is especially important where a learner needs to gain confidence in using new skills before use in more “real” contexts.38 Arguably, this is especially important where barriers (eg, fear of retaliation) may preclude their use.10,39–41
Much of IMO’s pedagogic utility also seemed founded in its accessibility. Point-of-contact delivery in each clinical context allowed exposure to development training which can be logistically and financially hard to access.33 Negotiating the notorious logistical challenges of clinical practice (described by Vivar33) was indeed difficult and we note participants’ desire for more time to practice IMO. Nevertheless, we are encouraged by our findings, in that they were obtained under considerable constraints and we thus earmark extended, committed time for practicing IMO in future research. The training of the general workforce using such methods has been upheld by recent expert opinion.42 That the IMO framework seems to be easy to use under very common constraints adds further encouragement around its utility.
IMO adds an interesting point over and above these criteria – that its use encouraged participants’ reflective thinking. Specific data about this process are limited but we suggest this mechanism as another important foci for future research, possibly bringing together IMO with other ways to develop personal reflection, currently a popular aim in health professional training.43
Comparison with Other Verbal Frameworks
Literature about other mnemonics and aide memoirs seem to echo IMO’s general purpose, to provide an appropriate way to avoid knee jerk, conflict-inducing responses, instead offering a framework to assist staff towards positive outcomes, under pressure.
General Verbal Frameworks
Two popular verbal workplace frameworks are described under the umbrella term assertiveness - The DESC tool (Describe the unwanted behaviour, Express how the behaviour makes you feel, Specify the behaviour that must change, Consequences of the behaviour)44 and Stop! Reflect! Respond!45 One tool (DESC) also offers opportunity to consider how best to generally frame speech around a way forward. However, both authors warn that a situation might still require careful thought about what exactly to say. Such models may thus lack specific guidance around content demanded by some practitioners in clinical practice, especially for the beginner and those dealing with potentially complex or challenging situations. Both models still seem to lack ways to frame a positive way forward, as IMO does, suggesting a potential lack of utility in some situations, perhaps inciting shame and conflict as a result.
Verbal Frameworks for the Clinical Environment
Specific, popular verbal frameworks for use in the clinical workplace are the CUSS46 framework and ISBAR (developed from the original SBAR used in the US Navy).47 These frameworks focus on improving interpersonal communication and enhancing clinical practice. The former is growing in popularity as a way to frame speech raising potential concerns, and the latter now widely accepted as an essential framework for minimising patient handover error.47
Such frameworks are found useful for two main reasons. First, to provide a memorable mental “script” for a person to follow under pressure. Second, to encourage them to speak to others about perceived danger or error (CUSS), or important concerns (ISBAR). For example, CUSS (I am Concerned, I need to Understand, I think there is a Safety issue, I think we should Stop) encourages a person to formulate language around potential issues with the procedure at hand, eg, “I am Concerned that…”. ISBAR (Introduction/Situation, Background, Assessment, Recommendation) offers very specific guidance about what exactly to say under several vital categories. For example, S stands for Situation, and encourages a person to briefly explain what has happened so far to their patient “the situation is that this patient….” and ensure this information is given to those taking over the patients care. Testing such verbal frameworks over time has revealed a significant contribution to a workplace’s positive culture, and around specific events such as perioperative care44 and the transfer of patients between services.47
Recent experiences with IMO offer a perspective with which to critique these frameworks, especially CUSS, and suggest further refinements. We wonder if this more “loose” framework might risk inciting conflict with those “spoken to”. For example, CUSS might be used in a situation where a staff member is being overbearing and halting healthy discussion about the procedure at hand, resulting in a failure to use best practice. As we found, we need to be wary that such behaviour might be a values-issue, and as such warranting very careful handling. For example, the overbearing person might not value the input of other staff members. Attempting resolution using CUSS, say, might result in publicly shaming this person. Words like “I am Concerned that you are not following procedure”, while having a non-confrontational initial focus on “I”, might still incite conflict because of the use of “you” and a focus on the “thing done wrong”. This CUSS phrase may then be interpreted as a challenge and result in retaliatory negative behaviour.
We do not dismiss the need for staff to act quickly and speak firmly should danger be apparent, as one might with “stat” (Latin statim – immediately). However, we wonder if CUSS might be enhanced with circumspect, but clear language within its framework. For example, a person might respond to the above situation thus:
I am concerned about what we should do next. Can we take a break so I can check current procedure?
While this statement is more direct than some, this IMO phrase adheres to “M” and “O” components and as such might overall return a more positive reaction.
There is also a recent upsurge in the popularity of programs such as Crucial Conversations20 which incorporate several tools and frameworks to approach difficult interactions in the workplace. This program requires commitment, money and dedicated training which might not be readily available to the staff demographic we studied. Whilst the value of such programs is not in doubt, the utility of IMO at least in part fills the needs of staff on the shop floor who need to have “Crucial Conversations” but lack the resourcing required by such programs.
Strengths and Weaknesses of the Study
As discussed, we are not privy to the thinking of those on the receiving end of IMO but rely on participants’ comments, their considerable expertise plus our own, in order to gauge its impact and utility. We are offered confidence in this by the parallel nature of our participants’ and alleged perpetrators’ contexts: working in the same field and workplace, with similar situational experiences. While personal contexts would likely differ (eg, home life, past experience) we trust insights to offer a firm starting point for our developing understanding.
Implications for Staff and Policymakers
This finding points to a potential “gap” in staff development training around workplace skills and complaint proceedings such as those actioned by human resources staff. While many workplace programs aim to help staff “speak up” to bullies, we suggest redirecting these efforts to training in more practical, fruitful and safe methods.
Limitations to Generalisability of Findings
Findings are generalizable to many other clinical contexts and workplaces. However, we should be mindful that some may have bullying which occurs for a reason we have not considered here, eg, as a vendetta - The use of IMO in such cases is as yet untested. We also note that language and its use can vary, eg, culturally, as can boundaries around personal confrontation. As such, we cannot claim IMO will help, or should be used to help every kind of bullying without further thought or judgement.
Recommendations for Practice
If we wish to “stop making things worse”29 we need to:
- Stop asking bullying bystanders to challenge behaviour, especially without offering them skill development support;
- Safeguard all staff as potential primary victims and bystanders by training them in approaching situations more fruitfully, with frameworks like IMO;
- Gain purchase on ameliorating workplace bullying for bystander and victim by preserving active learning methods, accessible staff development and a focus on developing practical skill;
- Avoid the instigation of didactic “mass teaching” of potentially nuanced and sensitive issues, even where complex logistics are challenging;
- Consider the refinement of the CUSS framework, or find a way to merge it with a more positive, conflict reducing approach.
Recommendations for Further Research
Substantial ethical challenges notwithstanding, we recommend:
- Monitoring the applicability of IMO in more severe situations, to determine limits or specific modifications necessary;
- Similarly, around long-term implications for the bystander;
- Further examining the intersection of IMO with conflict resolution theory and practice, to potentially expand our understanding and IMOs remit;
- Capitalising on existing expertise to further develop and test the DVC around cultivating values in the workplace;
- Investigating the further utility of IMO in developing reflective thinking for practitioners both in itself and in relation to workplace behaviour.
Conclusions
With a little practice and peer support IMO seems a good step forward in skilfully tackling some important aspects of workplace bullying. Its aim, content, pedagogy and accessibility seem congruent with several important criteria in helping the victim to bullying, their bystander colleagues and the workplace more generally. This is especially the case given the current climate of significant resource constraint which means staff are often unable to access funding or time to undertake more comprehensive skill-based programs. This climate is also one in which strategies for effective conflict management are still developing.48,49
Abbreviations
CAPLE, Creating A Positive Learning Environment research project; IMO [In My Opinion], a verbal framework for use in situations around negative workplace behaviours; IR, Interventionist-Researcher; AR, Action Research; KSH, Kelby Smith-Han, researcher.
Ethics and Consent Statements
This project was granted ethics approval in its entirety from the University of Otago, Dunedin, NZ. Participants all granted their written consent prior to taking part in the research, to include consent for participation and publication of their anonymised responses gathered during the research. Data and other materials are unavailable for lodging in an accessible repository as ethical approval did not allow for this.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We acknowledge with gratitude funding received from the Division of Health Sciences, University of Otago, Dunedin, NZ. Study design was developed by a research team independent to the funding body.
Disclosure
The authors declare no competing interests around undertaking or reporting this research.
References
1. Fnais N, Soobiah C, Chen M, et al. Bullying and discrimination in medical training: a systematic review and meta-analysis. Acad Med. 2014;89(5):187–827.
2. Mavis B, Sousa A, Lipscomb W, Rappley M. Learning about medical student mistreatment from responses to the medical school graduation questionnaire. Acad Med. 2014;89(5):705–711. doi:10.1097/ACM.0000000000000199
3. Einarsen S, Hoel H, Zapf D, Cooper C, Eds. Bullying and Harassment in the Workplace: Theory, Res Pract. CRC Press; 2020.
4. Godkin L. An epidemicological approach to workplace bullying. J Leader Account Eth. 2015;12(3):76–91.
5. O’Daniel M, Rosenstein AH. Professional communication and team collaboration. In: Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Rockville: Agency Healthc Res Qual; 2008.
6. Cosby K, Croskerry P. Profiles in patient safety: authority gradients in medical error. Acad Emerg Med. 2004;11(12):1341–1345. doi:10.1197/j.aem.2004.07.005
7. Vessey J, Demarco R, Gaffney D, Budin W. Bullying of staff registered nurses in the workplace: a preliminary study for developing personal and organizational strategies for the transformation of hostile to healthy workplace environments. J Prof Nurs. 2009;25(5):299–306. doi:10.1016/j.profnurs.2009.01.022
8. Kohut M. The Complete Guide to Understanding, Controlling, and Stopping Bullies & Bullying at Work: A Complete Guide for Managers, Supervisors, and Co-Workers. Ocala: Atlantic Publishing Group; 2007.
9. Sayre M, McNeese-Smith D, Leach L, Phillips L. An educational intervention to increase “speaking-up” behaviours in nurses and improve patient safety. J Nurs Care Qual. 2012;27(2):154–160. doi:10.1097/NCQ.0b013e318241d9ff
10. RACS. Royal Australasian college of surgeons: surgeon’s stories. Available from: https://www.surgeons.org/about-respect/stories-and-news/surgeons’-stories.
11. Price S, Doucet S, Hall L. The historical social positioning of nursing and medicine: implications for career choice, early socialization and interprofessional collaboration. J Interprof Care. 2014;28(2):103–109. doi:10.3109/13561820.2013.867839
12. Cassidy T, McLaughlin M, McDowell E. Bullying and health at work: the mediating roles of psychological capital and social support. Work Stress. 2014;28(3):255–269. doi:10.1080/02678373.2014.927020
13. Leiper J. Nurse against nurse: how to stop horizontal violence. Nurs. 2020;35(3):44–45.
14. HSWA. Introduction to the Health and Safety at Work Act 2015. Wellington, NZ: Special Guide. Available from:. https://worksafe.govt.nz/managing-healthand-safety/getting-started/introduction-hswa-special-guide/.
15. National Workplace Bullying Coalition. Jesse Bluma at Pointe Viven. Available from: http://pointeviven.blogspot.com/2018/06/Stand-Up-Speak-Out-Against-Workplace-Bullying-Catherine-Mattice-Jesse-Bluma-Pointe-Viven-Civility-Partners-NWBC.html.
16. Milliken F, Morrison E, Hewlin P. An exploratory study of employee silence: issues that employees don’t communicate upward and why. J Manage Stud. 2003;40(6):1453–1476. doi:10.1111/1467-6486.00387
17. Morrison E, Milliken F. Speaking up, remaining silent: the dynamics of voice and silence in organizations. J Manage Stud. 2003;40(6):1353–1358. doi:10.1111/1467-6486.00383
18. Easteal P, Ballard A. Shutting-up or speaking-up: navigating the invisible line between voice and silence in workplace bullying. Alt Law J. 2017;42(1):47–54.
19. Festinger L. A Theory of Cognitive Dissonance. Vol. 2. California: Stanford University Press; 1957.
20. Hills L. What the medical practice employee needs to know about workplace bullying. J Med Prac Manage. 2012;27(5):295–300.
21. Patterson K, Grenny J, McMillan R, Switzler A. Crucial Conversations. New York: McGraw-Hill; 2012.
22. Herr K, Anderson G. Quality Criteria for Action Research: An Ongoing Conversation. Thousand Oaks: Sage; 2005.
23. Herr K, Anderson G. The Action Research Dissertation: A Guide to Faculty and Students. New York: Sage; 2015.
24. McNiff J. Writing Up Your Action Research Project. London: Routledge; 2016.
25. Gamble Blakey A, Smith-Han K, Anderson L, Collins E, Berryman E, Wilkinson T. Interventions addressing student bullying in the clinical workplace: a narrative review. BMC Med Educ. 2019;19(1):1–13. doi:10.1186/s12909-019-1578-y
26. Gamble Blakey A, Smith-Han K, Anderson L, Collins E, Berryman E, Wilkinson T. It’s ‘probably the teacher!’ A strategic framework for clinical staff engagement in clinical student bullying intervention. BMC Med Educ. 2019b;19(1):1–13. doi:10.1186/s12909-019-1552-8
27. Thomas DA. General inductive approach for analyzing qualitative evaluation data. Am J Eval. 2006;27(2):247–346. doi:10.1177/1098214005283748
28. Gamble Blakey A, Pickering N. Putting it on the table: towards better cultivating medical student values. Med Sci Educ. 2018;28(3):533–542. doi:10.1007/s40670-018-0584-8
29. Gamble Blakey A, Anderson L, Smith-Han K, Wilkinson T, Collins E, Berryman E. Time to stop making things worse: an imperative focus for healthcare student bullying. NZ Med J. 2018;131(1479):81–85.
30. Gamble Blakey A, Smith-Han K, Anderson L, Collins E, Berryman E, Wilkinson T. “They cared about us students:” learning from exemplar clinical teaching environments. BMC Med Educ. 2019;19(1):1–10. doi:10.1186/s12909-019-1551-9
31. Blakey A Cultivating thinking and values in medical education [Unpublished Doctoral Thesis]. Dunedin, NZ: University of Otago; 2016.
32. Ames D, Lee A, Wazlawek A. Interpersonal assertiveness: inside the balancing act. Soc Pers Psych Comp. 2017;11(6):e12317. doi:10.1111/spc3.12317
33. Vivar C. Putting conflict management into practice: a nursing case study. J Nurs Manage. 2006;14:201–206. doi:10.1111/j.1365-2934.2006.00554.x
34. Johansen M, Cadmus E. Conflict management style, supportive work environments and the experience of work stress in emergency nurses. J Nurs Manage. 2016;24(2):211–218. doi:10.1111/jonm.12302
35. Seibel L, Fehr F. ‘They can crush you:’ nursing students’ experiences of bullying and the role of faculty. J Nurs Educ Pract. 2018;8(6):66–76. doi:10.5430/jnep.v8n6p66
36. Harland T, Pickering N. Values in Higher Education Teaching. London: Routledge; 2010.
37. Biggs R, Tang C. Teaching for Quality Learning at University.
38. Northam S. Cognitive rehearsal. Nurs Educ. 2000;25(1):19–20. doi:10.1097/00006223-200001000-00013
39. Knops K, Lamba S. Clinical application of ASCEND: a pathway to higher ground for communication. J Pall Med. 2010;13(7):825–830. doi:10.1089/jpm.2010.0023
40. Okuyama A, Wagner C, Bijnen B. Speaking up for patient safety by hospital-based health care professionals: a literature review. BMC Heal Serv Res. 2014;14(1):1–8. doi:10.1186/1472-6963-14-61
41. Hogan R, Orr F, Fox D, Cummins A, Foureur M. Developing nursing and midwifery students’ capacity for coping with bullying and aggression in clinical settings: students’ evaluation of a learning resource. Nurs Educ Pract. 2018;29:89–94. doi:10.1016/j.nepr.2017.12.002
42. Lassiter BJ, Bostain NS, Lentz C. Best practices for early bystander intervention training on workplace intimate partner violence and workplace bullying. J Interpers Violence. 2021;36(11–12):5813–5837. doi:10.1177/0886260518807907
43. Cruess R, Cruess S, Boudreau J, Snell L, Steinert Y. Reframing medical education to support professional identity formation. Acad Med. 2014;89(11):1446–1451. doi:10.1097/ACM.0000000000000427
44. Bower S, Bower G. Asserting Yourself-Updated Edition: A Practical Guide for Positive Change. UK: Hachette; 2009.
45. Griffin M. Teaching cognitive rehearsal as a shield for lateral violence: an intervention for newly licensed nurses. J Cont Educ in Nurs. 2004;35(6):257–263. doi:10.3928/0022-0124-20041101-07
46. Gluyas H. Effective communication and teamwork promotes patient safety. Nurs Standard. 2014;5(29):49–50.
47. Haig K, Sutton S, Whittington J. SBAR: a shared mental model for improving communication between clinicians. Joint Commiss J Qual Pat Saf. 2006;32(3):167–175.
48. Kitney P, Tam R, Bennett P, Buttigieg D, Bramley D, Wang W. Handover between anaesthetists and post-anaesthetic care unit nursing staff using ISBAR principles: a quality improvement study. ACORN. J Periop Nurs Austral. 2016;29(1):30–35.
49. Almost J, Wolff A, Stewart‐Pyne A, McCormick L, Strachan D, D’Souza C. Managing and mitigating conflict in healthcare teams: an integrative review. J Adv Nurs. 2016;72(7):1490–1505. doi:10.1111/jan.12903
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.