Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Supporting Behavior Change After AECOPD – Development of a Hospital-Initiated Intervention Using the Behavior Change Wheel
Authors Schmid-Mohler G ![]() , Hübsch C
, Hübsch C ![]() , Steurer-Stey C
, Steurer-Stey C ![]() , Greco N
, Greco N ![]() , Schuurmans MM
, Schuurmans MM ![]() , Beckmann S
, Beckmann S ![]() , Chadwick P
, Chadwick P ![]() , Clarenbach C
, Clarenbach C ![]()
Received 24 January 2022
Accepted for publication 30 April 2022
Published 26 July 2022 Volume 2022:17 Pages 1651—1669
DOI https://doi.org/10.2147/COPD.S358426
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Gabriela Schmid-Mohler,1,2 Christine Hübsch,1,2 Claudia Steurer-Stey,3,4 Nico Greco,5 Macé M Schuurmans,2,6 Sonja Beckmann,1 Paul Chadwick7 *, Christian Clarenbach2,6 *
1Centre of Clinical Nursing Science, University Hospital Zurich, Zurich, Switzerland; 2Division of Pulmonology, University Hospital Zurich, Zurich, Switzerland; 3Epidemiology, Biostatistics and Prevention Institute, University Zurich, Zurich, Switzerland; 4mediX Group Practice Zurich, Zurich, Switzerland; 5Physiotherapy Occupational Therapy, University Hospital Zurich, Zurich, Switzerland; 6Faculty of Medicine, University of Zurich, Zurich, Switzerland; 7Centre for Behavior Change, University College London, London, UK
*These authors contributed equally to this work
Correspondence: Gabriela Schmid-Mohler, Centre of Clinical Nursing Science, University Hospital Zurich, Ramistrasse 100, Zurich, CH-8091, Switzerland, Tel +41 44 255 20 03, Email [email protected]
Abstract: After hospitalization due to acute COPD exacerbations, patient-manageable behaviors influence rehospitalization frequency. This study’s aim was to develop a hospital-ward-initiated Behaviour-Change-Wheel (BCW)-based intervention targeting patients’ key health behaviors, with the aim to increase quality of life and reduce rehospitalization frequency. Intervention development was performed by University Hospital Zurich working groups and followed the three BCW stages for each of the three key literature-identified problems: insufficient exacerbation management, lack of physical activity and ongoing smoking. In stage one, by analyzing published evidence – including but not limited to patients’ perspective – and health professionals’ perspectives regarding these problems, we identified six target behaviors. In stage two, we identified six corresponding intervention functions. As our policy category, we chose developing guidelines and service provision. For stage three, we defined eighteen basic intervention packages using 46 Behaviour Change Techniques in our basic intervention. The delivery modes will be face-to-face and telephone contact. In the inpatient setting, this behavioral intervention will be delivered by a multi-professional team. For at least 3 months following discharge, an advanced nursing practice team will continue and coordinate the necessary care package via telephone. The intervention is embedded in a broader self-management intervention complemented by integrated care components. The BCW is a promising foundation upon which to develop our COPD intervention. In future, the interaction between the therapeutic care team-patient relationships and the delivery of the behavioral intervention will also be evaluated.
Keywords: AECOPD, complex intervention, behavior, behavior change, intervention development
Plain Language Summary
People suffering from a chronic respiratory disease can often influence the course of their disease with their health behavior. Therefore, it is important to implement interventions that support behavior change in the health care system. However, there are some challenges associated with this: The interventions must fit into the context, include the current state of knowledge and be transparent about their content. This is a prerequisite for the intervention to be effective and also enables research into its effectiveness. The Behaviour Change Wheel is a guide for developing interventions to meet these requirements. Considering that, to our knowledge, no intervention yet exists for people suffering from severe COPD lung attacks (exacerbations) following the Behaviour Change Wheel, we believed that developing such an intervention would have the potential to improve patients’ quality of life and reduce their rehospitalization frequency. This article describes our step-by-step processes of developing and then embedding that behavioral intervention in a broader self-management intervention in clinical care. Our overall aim is to make this rather complex method accessible to clinically active researchers and clinicians.
Introduction
Severe acute exacerbations of COPD (AECOPDs) that require hospitalization present heavy physical and emotional burdens for patients.1 They also constitute a substantial part of all COPD-related health care costs.2 The very high three-month rehospitalization rate—43%, of which over half (23% overall) are directly COPD-related—contributes significantly to these costs.3 Among stable patients, respiratory-related hospitalizations have been successfully reduced by models of care that tackle problem health behaviors via coordinated multi-professional processes. The most beneficial behaviors are early recognition and management of exacerbation, smoking cessation, physical activity, a healthy diet, medication adherence, and management of dyspnea and related burdensome emotions.4–8 Whilst the evidence base for stable patients is quite broad, the evidence for those suffering exacerbations is limited regarding effective interventions for lowering rehospitalization rates and improving quality of life. The main reasons are the limited number of available studies and the heterogeneity of interventions studied.9,10 If analysts focus sharply on exacerbated patient rehabilitation programs that include physical activity components, they can distinguish positive impacts on quality of life and exercise capacity; but reductions of hospitalization rates remain inconsistent.11
The Behavior Change Wheel (BCW) is a pragmatic guide for designing behavior change interventions based on a contextual understanding of behavior.12 Used alongside the Behaviour Change Technique (BCT) taxonomy, the BCW allows researchers first to understand the influences on specific behaviors using the COM-B model (Capability-Opportunity-Motivation-Behaviour) and the Theoretical Domains Framework (TDF),13 and then to describe the content of interventions to change these in a common language.13 The use of the BCT to specify the content of an intervention allows researchers to evaluate the impact of the intervention’s component parts. Since publication, the BCW framework has been used to develop behavior change interventions in chronic diseases including type 1 diabetes.14 The BCW, the BCT taxonomy and the TDF have also been used in research on COPD. The TDF was used to analyze self-management programs and to explore the determinants of sedentary and smoking behavior in qualitative studies,15–17 the BCW to develop interventions to increase physical activity,18 respectively providing an example,19 and the BCT taxonomy to describe the content of digital technology interventions.20
To our knowledge, no AECOPD-focused intervention has yet been developed using the BCW. This paper describes 1) the relevant behavioral problems based on their clinical risk of negatively influencing respiratory-related outcomes, 2) the development of a complex hospital-initiated behavioral intervention package using the BCW framework to stabilize respiratory-related outcomes, and 3) the planned intervention. Based on a recent analysis of the setting,21 the intervention will be delivered by a multidisciplinary team including a physician, a physiotherapist, and an advanced nursing practice nurse team (ANPT) during the participants’ hospital stay; following discharge and continued by the ANPT for at least 3 months.
Methods
Study Design
The three stages of the BCW approach were used to develop the intervention to address selected behavioral problems.
Selection of Health-Behavioral Problems
Health-behavior problems were selected based on a scoping review. To inform our intervention strategy, we sought out high-quality systematic reviews/meta-analyses and guidelines that addressed the impacts of health behaviors on our target respiratory-related outcomes. The PICOs-framework we applied included the following: ● Population: Adult patients with COPD exacerbation.● Intervention: Interventions to address health behavior. The chosen intervention addressed either a broad range of behaviors related to self-management, integrated care and/or rehabilitation; or it could be focused on individual behaviors such as smoking cessation, medication taking, physical activity, healthy eating, or others.● Control: Usual care.● Outcomes of Interest: Respiratory-related outcomes, operationalized as respiratory-related rehospitalization, number of exacerbations, lung function and health-related QoL.● Study, Article Type: Guidelines, Systematic Reviews, Meta-Analyses
Two searches were performed in June 2020:
Search A. For guidelines focused on interventions addressing health behaviors with the aim of improving respiratory-related outcomes, we searched PUBMED/MEDLINE. We used the search terms “COPD OR chronic obstructive pulmonary disease” Filters: Guideline, Practice Guideline. Guidelines were appraised with the AGREE II Reporting Checklist for clinical practice guidelines.22
Search B. Systematic reviews/meta-analyses reporting the effectiveness of health behavior interventions on respiratory-related outcomes. We searched “The Cochrane Database for Systematic Reviews” using the search term “COPD”. The quality of the included studies was appraised via the CASP Systematic Review Checklist.23
We applied four inclusion criteria: guidelines or systematic reviews/meta-analyses; published in the past 10 years (back to June 2010); including patients with COPD; and focusing on patients’ health behavior. We applied five exclusion criteria: a focus on a pharmacological or medical treatment’s efficacy (without involving any patient health behaviors); a primary focus on a special form of rehabilitation; inclusion of patients with other diseases than COPD; a focus on a subgroup with a particular comorbidity or symptom (cluster); local adaption of a guideline; or text language other than English or German.
As the development of an intervention using the BCW approach is time-intensive and the timeline of the project was limited to one year, we chose to focus on no more than three behavioral problems. If we identified relevant behaviors, we decided in advance that these should also be addressed in the program, but not subjected to the BCW development approach.
Based on narrative synthesis of the evidence (described in detail below), we chose three primary behavioral problems: insufficient exacerbation symptom management; lack of physical activity; and continued smoking.
According to Swiss law, no ethical approval was necessary for this study as no patients were involved.
Project Team
The intervention was developed at the University Hospital Zurich. A dedicated working group tackled each of the three main behavioral problems. All three included the same project leader (GSM (first author)), scientific collaborator (CH (author)), and pulmonologist (CC (author)). This common core was complemented as appropriate by clinical experts who were physiotherapists, physicians, nurses and nurse specialists. Each working group was also accompanied by one or two consultant(s) with internationally acknowledged expertise relevant to that group’s target behavior (physical activity: AF + TR (acknowledgement); exacerbation self- management: CSS (author); smoking cessation: MMS (author)). To ensure correct application of BCW methodology to the field of symptom management, the intervention’s development was supervised by PC and SB (authors).
Stage 1: Understanding Each Problem Behavior in Context
To understand each problem adequately, we performed a literature review and assessed health professionals’ perspectives: The health professional perspective was elicited via focus group (described elsewhere),21 and working group discussions. These were protocolled and checked for accuracy by the relevant working group members. The relevant literature included reviews and meta-analyses which have already been used to select the relevant behavioral problems (Table 1), and qualitative studies describing patients’ experiences. To identify the patient perspective for each behavioral problem, qualitative studies in PUBMED/MEDLINE were searched in June 2020 with the following search terms: (interview* OR experience* OR qualitative) AND Pulmonary Disease, Chronic Obstructive AND ((exacerbation*) OR (smoking cessation) OR (physical activity OR rehabilitation)).
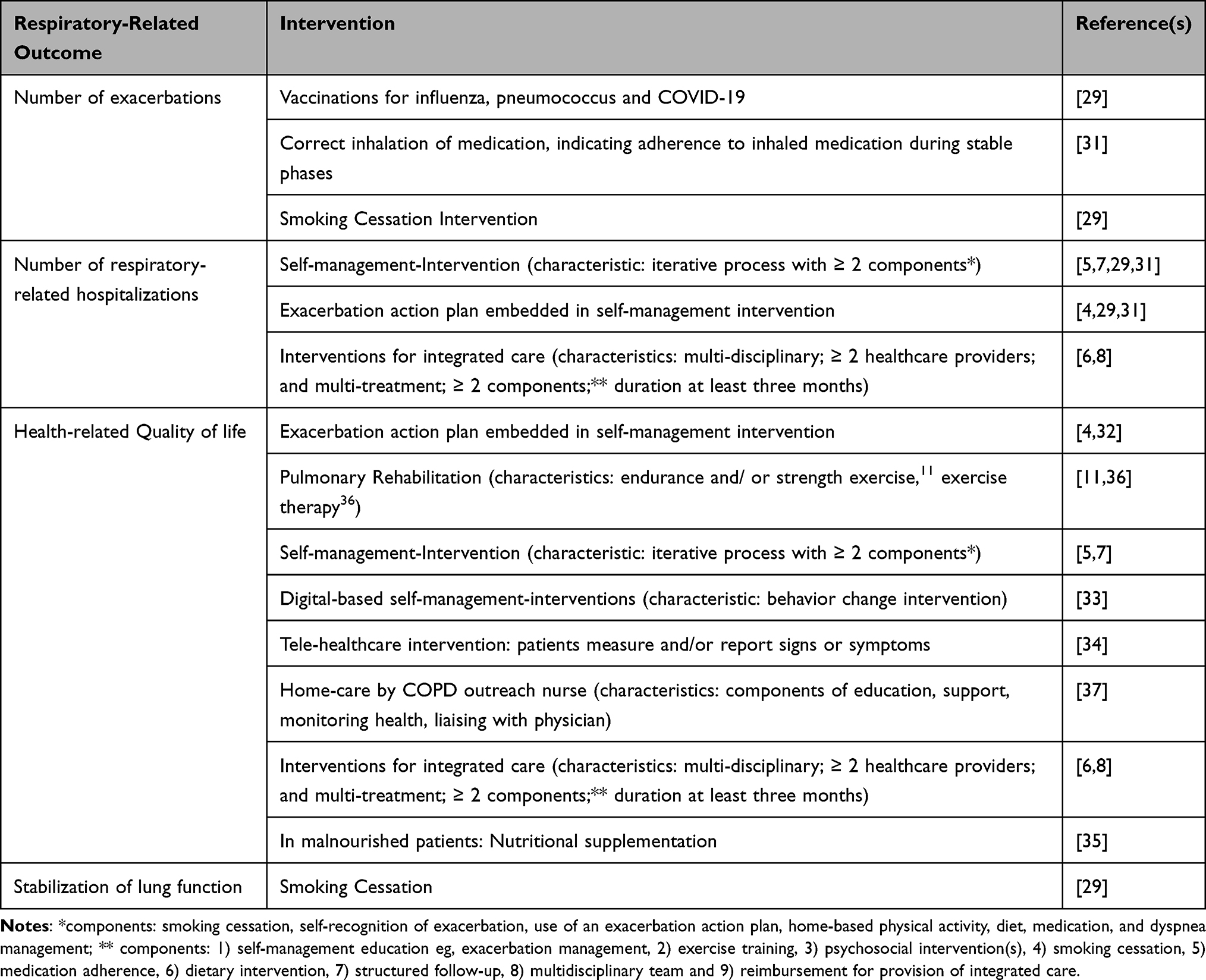 |
Table 1 Scoping Review of Articles on the Impact of Health Behavior Interventions on the Chosen Respiratory-Related Outcomes |
Next, target behaviors were formulated and specified to address each problem. As appropriate, these were reviewed and refined by the working groups and expert consultants.
Influences on each target behavior were identified by analyzing evidence both from the literature – including patient perspective - and from health professionals, then deductively coding the resulting data using the COM-B model of behavior and the TDF.24 Coding was done by one person (GSM) and reviewed by another (CH). Transcript passages that could correspond to two or more domains were discussed by the team, who reached consensus by applying the appropriate COM-B and TDF definitions.
Stage 2: Identify Intervention Options
Based on the results of Stage 1ʹs behavioral analyses, we consulted the BCW’s behavior change functions to determine which kind of intervention would apply to our target behaviors. This process yielded nine intervention functions:12 increase knowledge (“education”), use communication to induce feelings (“persuasion”), impart skills (“training”), augment the patient’s means or reduce barriers, increase capability or capitalize on opportunities (“enablement”), provide an example (“modelling”), and/ or change the context (“environmental restructuring”), create an expectation either of reward (“incentivization”) or of punishment (“coercion”), and use rules to narrow the range of opportunities to engage in the problem behavior (“restriction”). Useful intervention functions were selected by the project leader and scientific collaborator via a list of linkages between COM-B, TDF and intervention functions with the aim to generate ideas for the intervention.13 The project leader and scientific collaborator then appraised each intervention function according to affordability, practicability, effectiveness and cost-effectiveness, acceptability, side-effects and safety, and equity, ie, the APEASE criteria.13 The final selection was made via discussion within each working group.
As the following step, we followed the BCW’s suggestion to choose a “policy category”, which would determine how each category should be delivered. Ie, policy categories offer superordinate ways of implementing an intervention. The BCW describes seven policy categories:12 delivering a new service (“service provision”), creating documents that describe changes to existing services (“guidelines”), using media (“marketing”), designing and/or controlling the environment (“planning”), making or changing laws (“legislation”), using a tax system to change cost (“fiscal measures”), and establishing rules (“regulation”). The policy categories were selected on basis of the APEASE Criteria.
Stage 3: Identify Content and Implementation Options
In the third and final stage, the intervention’s content was refined and the delivery modes defined. The intervention was formulated from small individual ingredients drawn from a pool of 93 Behavior Change Techniques.13 Each BCT was selected first by considering the barriers identified either by the literature or by our health professionals in stage 1, then by using the linkage list between intervention functions13 and BCTs, and finally by appraising each candidate BCT according to the APEASE criteria. After selecting modes of delivery from the 13 offered possibilities, we formulated all BCTs in detail based on the current body of evidence. We based our BCT specifications on the recommendations of the international “Better living with COPD” program,25,26 the Global Strategy for Prevention, Diagnosis and Management of Chronic Obstructive Lung Disease, the “GOLD 2022” guidelines, and other guidelines,27–29 as well as information disseminated by Switzerland’s national Stop Smoking Program.30
Results
Selection of Health-Behavioral Problems
Search A. This search yielded 136 guidelines, of which nine met our selection criteria. Of those, seven fulfilled the quality criteria assessed via the AGREE tool. One high-quality guideline, which covered all topics addressed in the other six, was used predominantly to select behavioral problems.31 For the current report, we used this guideline’s updated version.29
Search B. Of 85 identified reviews, ten met our selection criteria.4–6,11,32–37 Two more met most of the criteria, but did not focus on any respiratory-related outcomes.27,38 While those could not be used to select health behaviors, they proved useful for the intervention development in stages 1–3. All reviews were of high quality. For the current publication, we used the updated versions of two reviews.7,8
An overview of the literature findings regarding COPD-relevant behaviors and their affects on respiratory-related outcomes is provided in Table 1. As smoking cessation slows the decline in lung function and decreases the number of exacerbations, it is seen as essential part of COPD care models.29 Those that focus on exacerbation management, including the noting of symptoms and/or correct use of written action plans, decrease respiratory-related hospitalizations and increase health-related quality of life; therefore, they are also recommended.4–8,29,31,32,34 And as those that foster regular physical activity, including supervised training in rehabilitation programs, decrease respiratory-related hospitalizations and increase health-related quality of life, they are also recommended for inclusion.5–8,11,29,31,33,36 Further, adherence to inhaled medications and vaccinations decreases the number of exacerbations: it is advised for COPD care according to local recommendations.29 As nutritional supplementation increases quality of life in malnourished patients, it is another essential component.29,35 Two other behaviors that do not have a direct impact on our defined respiratory-related outcomes have been identified as relevant for a COPD care model. Those are medical oxygen use and advance care planning. Although long-term administration of oxygen (>15 hours per day) does not affect respiratory-related outcomes, it has an effect on survival.29 And although fostering advance care planning does not affect respiratory-related outcomes, it may reduce burdensome emotions.29
Based on our literature review results, the following three behavioral problems were selected to be developed via the BCW framework: insufficient exacerbation symptom management; lack of physical activity; and continued smoking. While the associated intervention was not developed using the BCW framework, six of its targeted behavioral problems were judged relevant and included in the final care model. Those were non-adherence to vaccination recommendations, non-adherence to the prescribed inhalation regimen, non-adherence to long-term oxygen (in a patient subgroup), poor nutrition leading to underweight, inadequate management of dyspnea/related burdensome emotions, and insufficient end-of-life advance care planning.
Stage 1: Understanding the Behavior in the Context
The focus group interview results and our synthesis of the qualitative studies describing the patients’ perceptions of exacerbation management are reported elsewhere.21 Eight qualitative studies describing patient experiences have been identified: five for smoking cessation challenges,39–43 three for physical activity.44–46 The results of the literature review and the assessment of the health professionals’ perspective are described in Supplemental Table 1. The key results are presented in the following paragraphs:
Description of the Three Main Problems in Behavioral Terms
Problem 1 – Poor exacerbation management. Guidelines recommend drafting exacerbation action plans and education of patients regarding their correct and safe use.47 However, as was evident in our focus groups, many health professionals (HPs) were either unaware of the guidelines, or lack the time to implement them; therefore, few patients with COPD ever see a written action plan. A number of the HPs we interviewed also doubted such plans’ efficacy and safety. In those cases, their doubts may originate from a number of standalone studies that reported detrimental effects of self-medication in subgroups such as terminally ill patients.4 Evidence from qualitative studies indicate that patients with COPD have trouble differentiating day-to-day variations from exacerbation. Consequently, many do not start therapy or seek help until their exacerbation are more advanced and demand more complex treatment.48–50 Still, the patient’s relationship with his/her HPs is critical.48,49,51 With recent increases in the use of digital telehealth interventions, documentation of symptoms and recommended actions commonly reflects and improves exacerbation management;20 but, even in these cases, few patients keep daily logs of their symptoms and actions. Regarding the problem of poor exacerbation management, participating HPs recognized the value of pre-formulated action plans to support their patients in reacting to new symptoms. They also agreed that no patients should be expected to self-manage medication with oral corticosteroids and antibiotics unless assessments indicated that they possessed adequate competencies. A further discussion point was that, before patients can follow an action plan, they must be able to identify relevant changes in symptoms. Thus, interviewed HPs commonly saw consciously noting symptoms as a further key behavioral goal. While no COPD studies could be identified that investigated the effect of daily symptom reporting on rehospitalization, research on asthma interventions indicates that a combination of symptom self-monitoring, action plan adherence and regular GP review correlates with improved health outcomes.52
Problem 2 – Lack of daily physical activity. For COPD, the medical guidelines for physical activity recommend two supervised training sessions per week and the usual 30 minutes per day, mixing endurance and resistance training. This reflects the type of exercise regimen commonly embedded in a comprehensive pulmonary rehabilitation program.11,53 However, patients with COPD commonly experience barriers to adherence.45,54,55 During their in-patient stay, for example, their HPs may not provide them with information on the importance of regular physical activity, participation in a pulmonary rehabilitation program or how to overcome potential barriers to participation in such programs. Unfortunately, even patients who participate in pulmonary rehabilitation programs tend not to develop a habit of daily exercise. Instead, after having completed the program, they most commonly reduce their exercise levels.47,54
Problem 3 – Ongoing smoking. The GOLD 2022 guidelines highlight the importance of stopping any exposure to smoke particles, strongly recommending that smokers quit smoking, and that ex-smokers stay smoke-free.27,47 And while some patients with life-long smoking habits are convinced that they cannot stop,40,56 most reduce or even stop smoking during their inpatient stay. Among those who quit smoking while hospitalized for AECOPD, relapses are common.57 Those who experience AECOPD often become ambivalent about smoking, ie, they become more open to the possibility of smoking cessation. However, our focus group’s HPs often allow this effect to pass without comment.43,58 And finally, our participating HPs commonly reported that they were reluctant to address smoking cessation because they knew that addressing this topic could cause resistance and burden their physician-patient relationship.
Target Behaviors
The following three target behavioral problems and 6 goals were selected according to the BCW’s predefined criteria (see Supplemental Table 2 for further details):
Problem 1 “Poor exacerbation management”. 1) The patient keeps track of possible AE symptoms (coughing, sputum, breathlessness) daily. 2) The patient reacts to possible signs of AE according to a written exacerbation action plan (A: with self-medication; B: without self-medication). 3) The patient documents any possible AE symptoms and actions in a symptom journal.
Problem 2 “Lack of daily physical activity”. 4) The patient exercises 30 minutes daily. 5) The patient exercises regularly under in-person supervision of a physiotherapist and/or APNT. The frequency of sessions is defined individually for each patient.
Problem 3 “Ongoing smoking”. 6) A: In Smokers: Refrain from smoking at all times. B: In non- or ex-smokers: Keep up the non-smoking status at all times.
Need for Change
Based on the barriers and facilitators extracted from the literature, observation in practice and stakeholder interviews, the need for change at the patient level was defined for each of the six target behaviors:
Regarding “capability”, to influence the course of COPD, patients with COPD need to gain knowledge not only about their illness, but also about the relevance of behavioral problems and goals (TDF: “knowledge”). This will help them acquire the skills necessary to perform the desired behaviors—including muscle strengthening exercises—and adapt them to fit day-to-day variations of symptoms (TDFs: “physical skills” and “cognitive and interpersonal skills”). All patients need to establish a habit of starting new beneficial behaviors, for example, noting changes in symptoms and reacting according to an action plan.
Some behaviors, such as being physically active require daily repetition. Patients may also need to replace problematic behaviors with beneficial ones, eg, react to a written plan instead of reacting intuitively when experiencing symptoms, or resist the urge to light a cigarette when emotionally distressed (TDFs: “behavioral regulation” and “memory, attention and decision processes”).
Regarding “opportunity”, patients need to plan a series of actions to change their environment and activate resources to enable the performance of their desired behaviors, eg, placing their symptom journal in a prominent place, having an alternative plan for physical activity when the weather is bad or the fitness center is closed because of lockdown regulations due to COVID-19, or creating a smoke-free environment and reducing cues to smoke (TDF: “environmental context and resources”). And for the substantial number of patients with COPD who live alone, it is recommended to find one or several persons who support, foster or motivate their desired behaviors (TDF: “social influences”).
For “motivation”, patients need to cultivate a dualistic attitude: While aware of having a serious chronic condition (TDF: “identity”), they have to gain and act in the belief both that they are capable of making beneficial behavioral changes (TDF: “belief about capability”) and that those changes may improve the course of their disease, reducing their dyspnea and impacting their daily lives positively (TDF: “belief about consequences”). They also need to maintain their new behaviors as their long-term goal (TDF: “goal”), link them to positive emotions and remain aware that the risk for relapse is especially high during emotionally burdensome situations (TDF: “emotions”).
Behavior change is a particularly complex undertaking for patients with COPD, whose health situations are commonly aggravated by limited financial and social resources, high symptom burdens and low levels of energy. Still, change is possible, and some strategies and techniques are more successful than others. Therefore, HPs who support these patients should consider using interventions that have proved useful.
For more details on this stage, a description of the barriers to behavior change and an overview of the COM-B components that need change are presented respectively in Supplemental Tables 3 and 4.
Stage 2: Identify Intervention Options
Intervention Functions
The “education”, “persuasion”, “training”, “restructuring”, “modelling” and “enablement” intervention functions met the APEASE criteria largely or fully for all six behaviors. “Incentivisation” met the criteria only partly, as financial rewards are unacceptable in the given health-care system and culture; however social rewards are possible. Also, in the given health-care system the “coercion” and “restriction” intervention functions would be neither acceptable nor practicable.
The table describing the linkage between the COM-B model and the intervention functions for each behavior can be found in the supplementary material (see Supplemental Table 5).
Policy Categories
For the selected intervention functions, following policy categories met the APEASE criteria largely or fully: “service provision”, “guidelines”, “communication” and “environmental/social planning”.
The table describing the linkage between the intervention functions and the policy categories can be found in the supplementary material (see Supplemental Table 6).
Stage 3: Identify Content and Implementation Options
Behavior Change Techniques
BCTs were defined for both the basic and the follow-up intervention.
Basic Intervention
For each of the six target behaviors, BCTs were defined for delivery by each professional designation (ANPT, physiotherapist, physician) (Tables 2 and 3). For two target behaviors, the set of BCTs differed depending on the results of an initial assessment. As a result, the “reacting according to an action plan” package had two variations, while the “smoking cessation” package for ANPTs had seven variations. For the remaining four target behaviors, nine packages with no variation were defined. Consequently, each patient receives nine packages plus one variation of the “reacting according to an action plan” and one variation of the “smoking cessation” package. This resulted in the definition of eleven intervention packages for the basic intervention. Across the eighteen packages, 46 of the 93 available BCTs were used at least once. Some were used repetitively - for example, when the HP provided instruction (BCT 4.1) or information (BCT 4.2) about the intervention’s content. Details of the selected BCTs are shown in Supplemental Table 7.
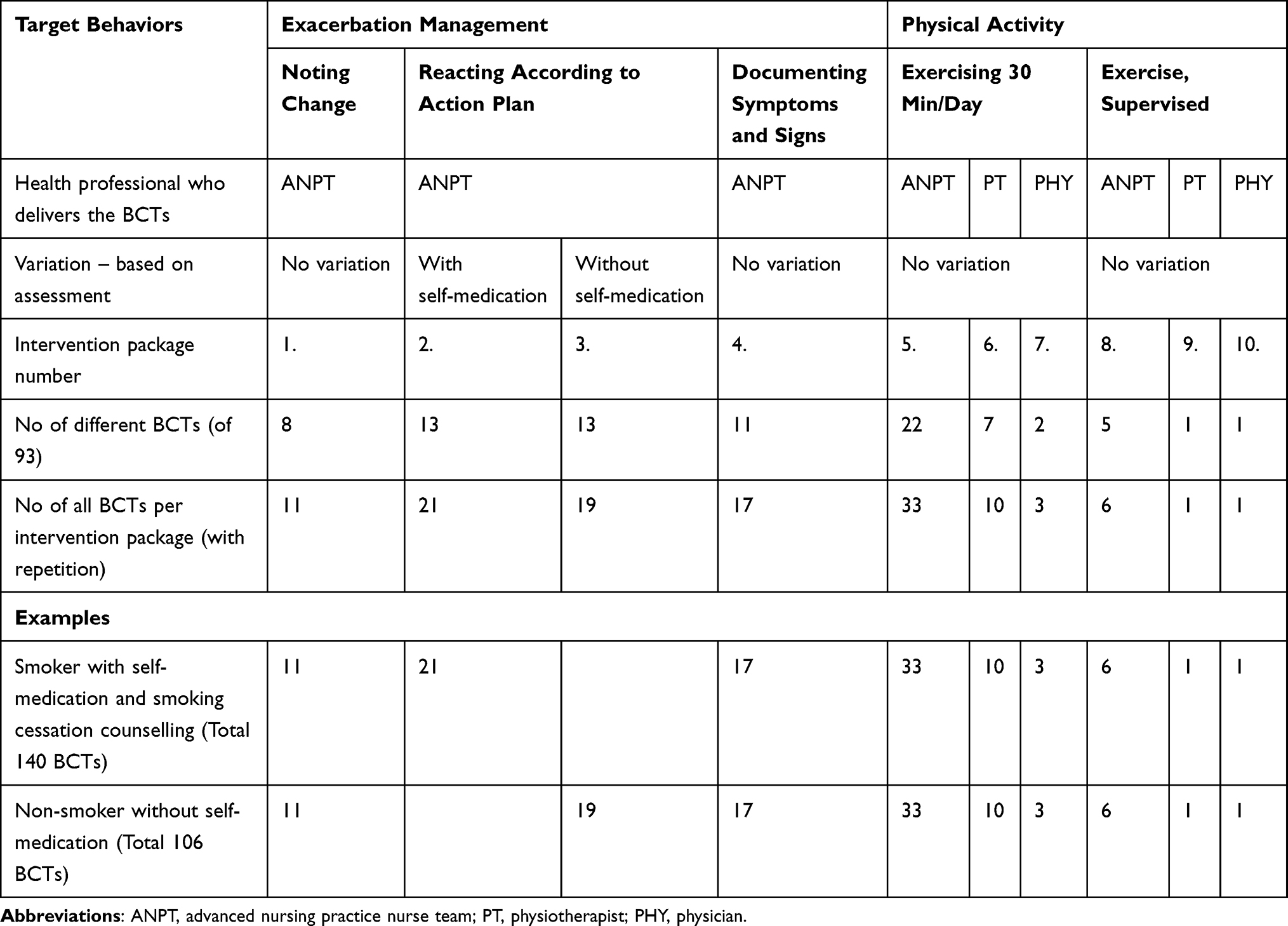 |
Table 2 Overview of Intervention Packages and Behaviour Change Techniques (BCTs) - Exacerbation Management and Physical Activity |
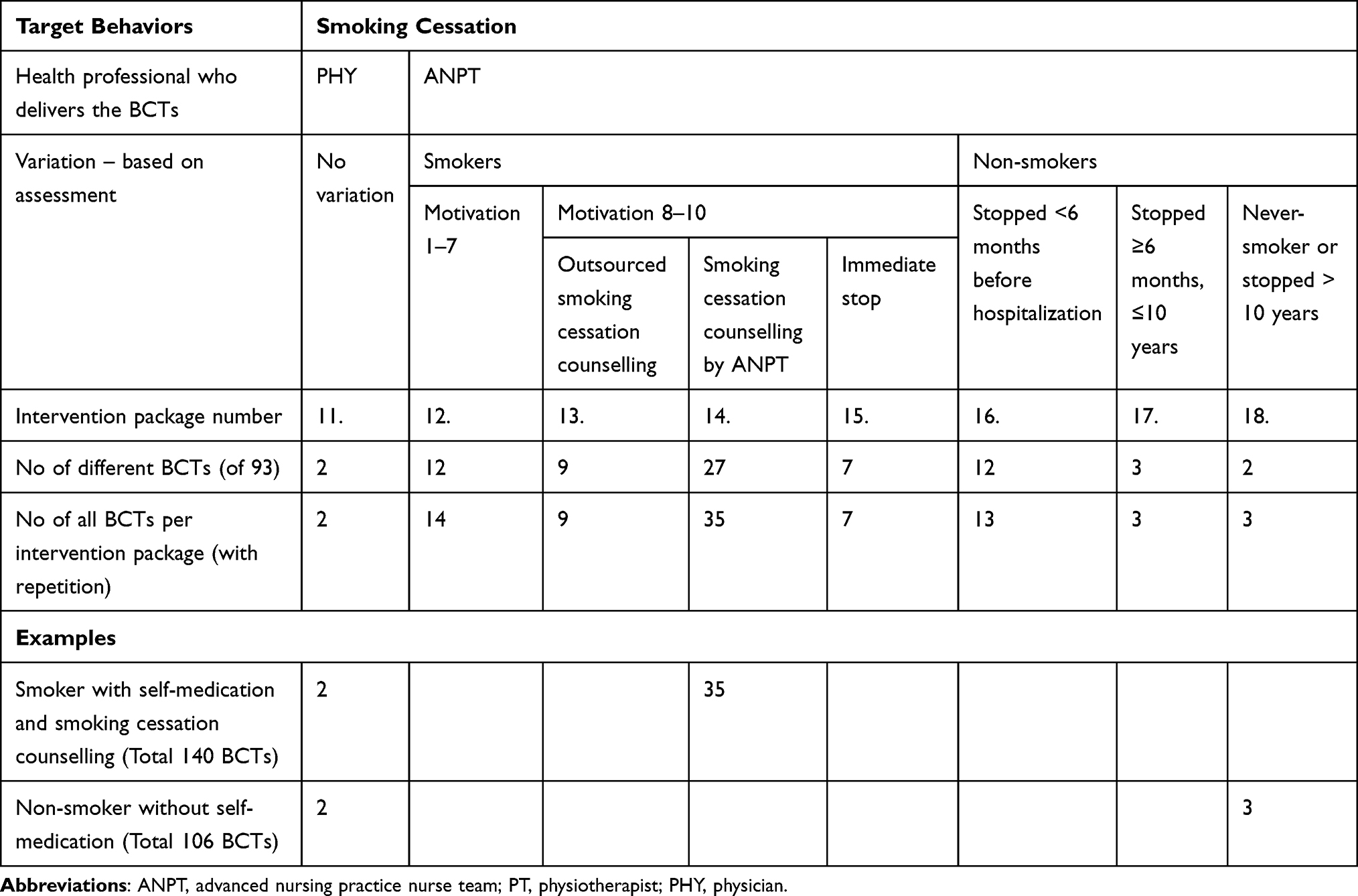 |
Table 3 Overview of Intervention Packages and Behaviour Change Techniques (BCTs) - Smoking Cessation |
As an example, depending on each patient’s initial assessment, each of the eleven intervention packages assembled for delivery within the basic intervention contained between 106 and 140 BCTs. While a non-smoking patient with an action plan including no self-medication received 106 BCTs, a smoker whose action plan included self-medication received 140.
Follow-Up Intervention
For the follow-up intervention, a different set of BCTs will be delivered for each behavior, depending on whether patients were successful in achieving the commonly agreed behavioral goals (Table 4).
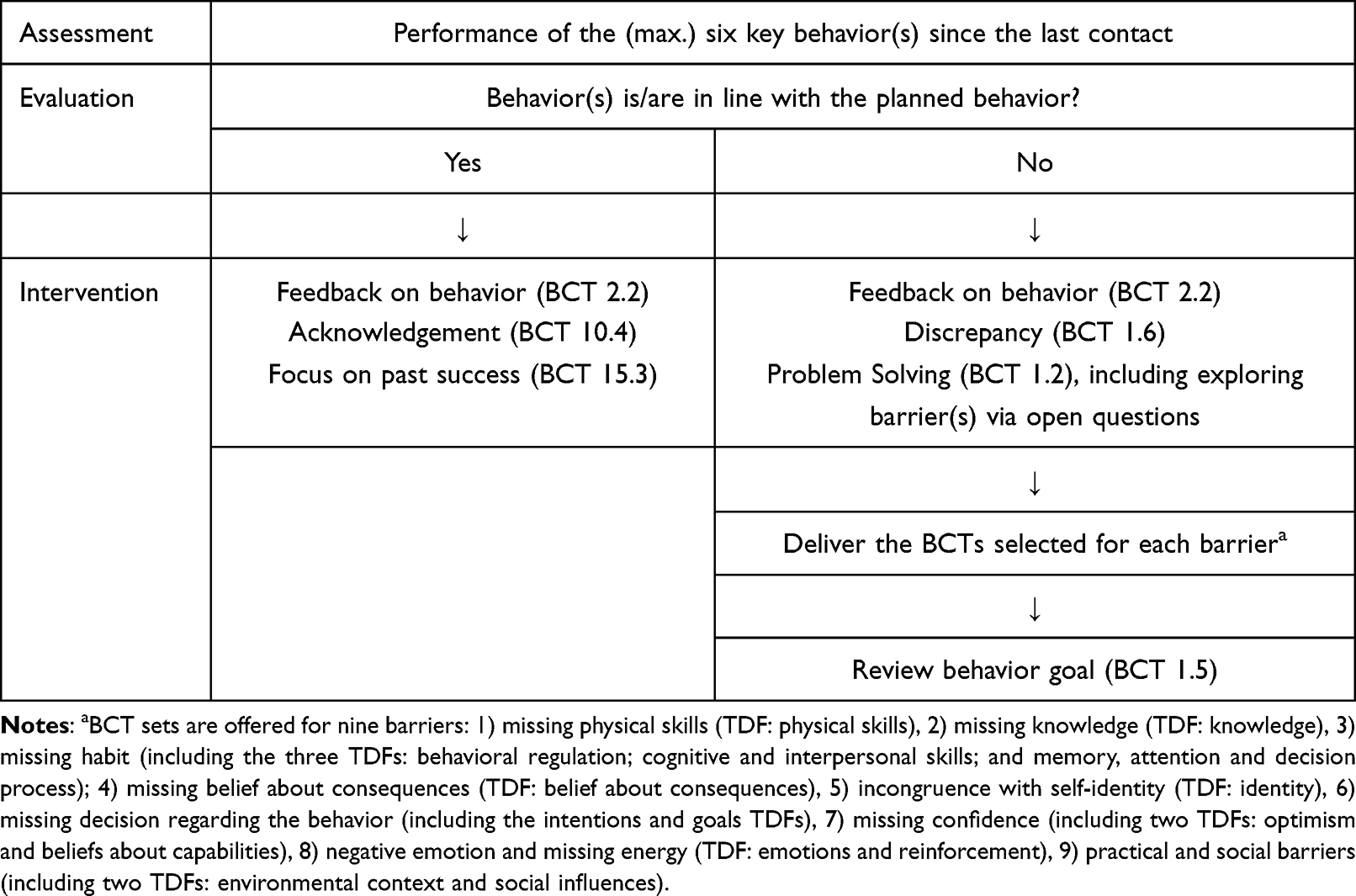 |
Table 4 Algorithm for Follow-Up Interventions |
Policy Categories
For the policy category “guidelines”, each BCT was specified based on current evidence and formulated in the intervention manual as a script to be read aloud by the ANPT member delivering it. An example of a fully-scripted intervention is provided in Table 5.
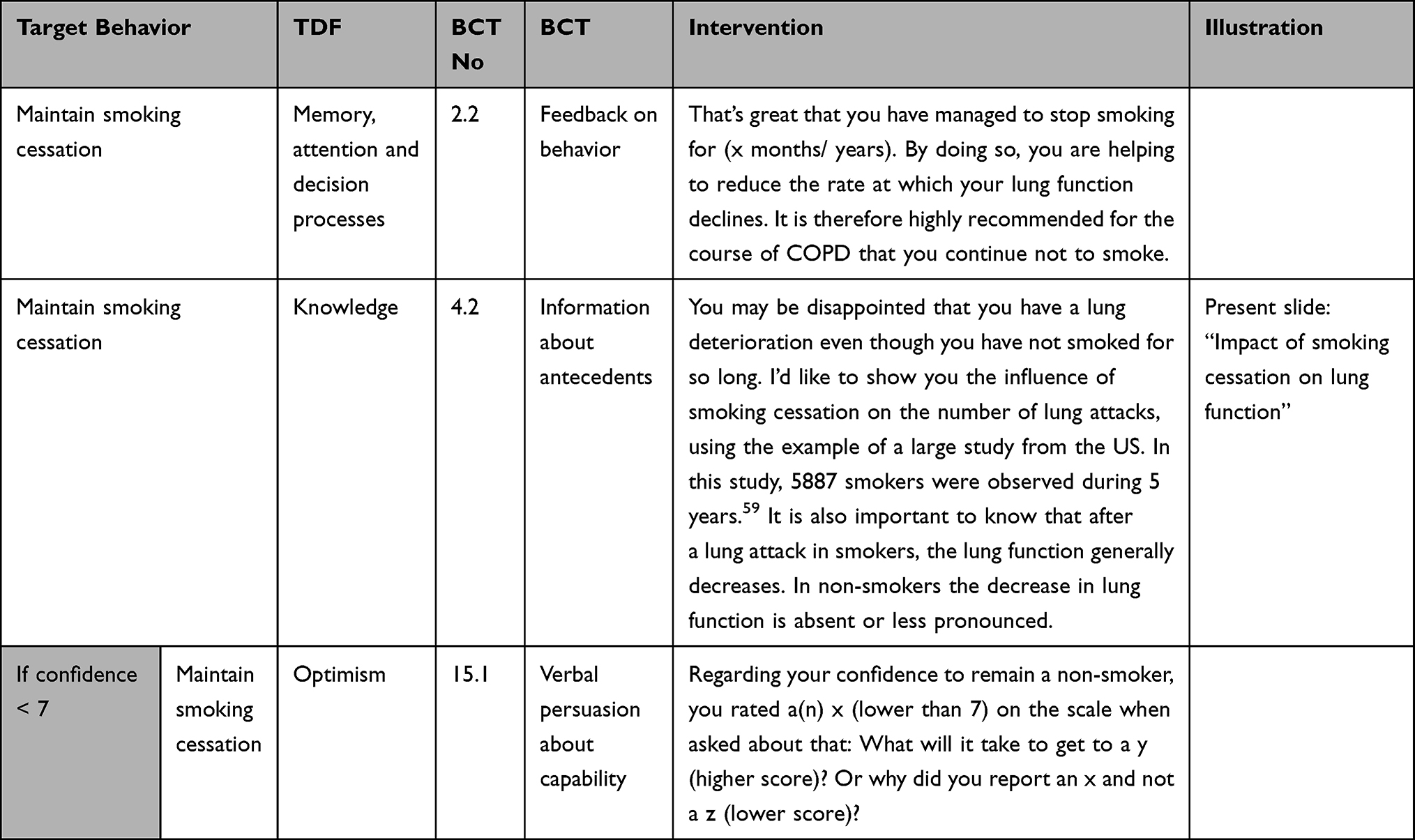 |
Table 5 Example of a Specified Intervention - Smoking Intervention for Ex-Smokers > 6 Months |
Regarding the policy category “communication”, patients received a folder including the following written materials: prints of slides presenting the key information for the target behaviors (as support for BCTs 4.1, 5.1, 5.2, 6.1, 9.1), a written action plan with or without self-medication, a symptom journal, ANPT contact information, a group photo including all team members, and a copy of the “Better living with COPD” brochure.
Mode of Delivery
If appropriate considering the patient’s condition and length of stay, the basic intervention (except “Exercising 30 min/day – ANPT”) will be delivered via face-to-face contact during his/her hospital stay. The basic intervention’s “Exercising 30 min/ day – ANPT” module and follow-up interventions are designed to be performed by telephone.
In-person visits—either at home or in hospital—were considered for all follow-up interventions, but did not meet the APEASE criteria. Ie, home visits are time-intensive and are not covered by the Swiss reimbursement system when performed by hospital staff/nurses; and in-hospital patient visits were assessed as burdensome for patients and travel costs as expensive.
The Nurse-Led Integrated Care COPD (NICCO) Intervention
Overview
The NICCO Intervention starts during the hospital stay and continues for twelve weeks after discharge. The previously presented BCTs are embedded in this Self-Management-Intervention, which consists of two broad components: firstly, 1–2 face-to-face meetings with the multi-professional team during the patient’s hospital stay; secondly, post-discharge telephone follow-up support for three months by the ANPT. For the first four weeks after discharge, the patient is contacted weekly by telephone (4 calls); for the remaining eight weeks, the ANPT shifts to a fourteen-day call schedule (4 calls). The frequency of follow-up calls is increased (to every 3–7 days) if patients experience AECOPD symptoms (“orange” or “red” days), then returned to the original schedule after the symptoms improve. After 12 weeks, patients are asked if they want to continue the follow-up calls at four-week intervals on a voluntary basis.
Alongside the three main behavioral goals, the intervention includes six complementary behaviors: adherence to vaccination recommendations; adherence to inhalation; adherence to long-term oxygen (in a subgroup of patients); adherence to nutrition to prevent or manage underweight; management of dyspnea and related emotional distress; and writing an advance care plan for end-of-life-care. However, as these modules were not developed following BCW methodology they are not reported in detail here.
For each behavioral goal, BCTs are selected and delivered based on a patient (re)assessment and embedded in a communication style that uses the attitude and techniques of Motivational Interviewing.60 In addition to the Self-Management-Intervention, the NICCO Intervention includes a comprehensive Integrated Care Intervention. The philosophy of the overall NICCO-intervention is “caring.” This is mirrored in the ANPT’s efforts to build a relationship of trust and a sense of being cared for.61 An overview of the intervention is provided in Table 6.
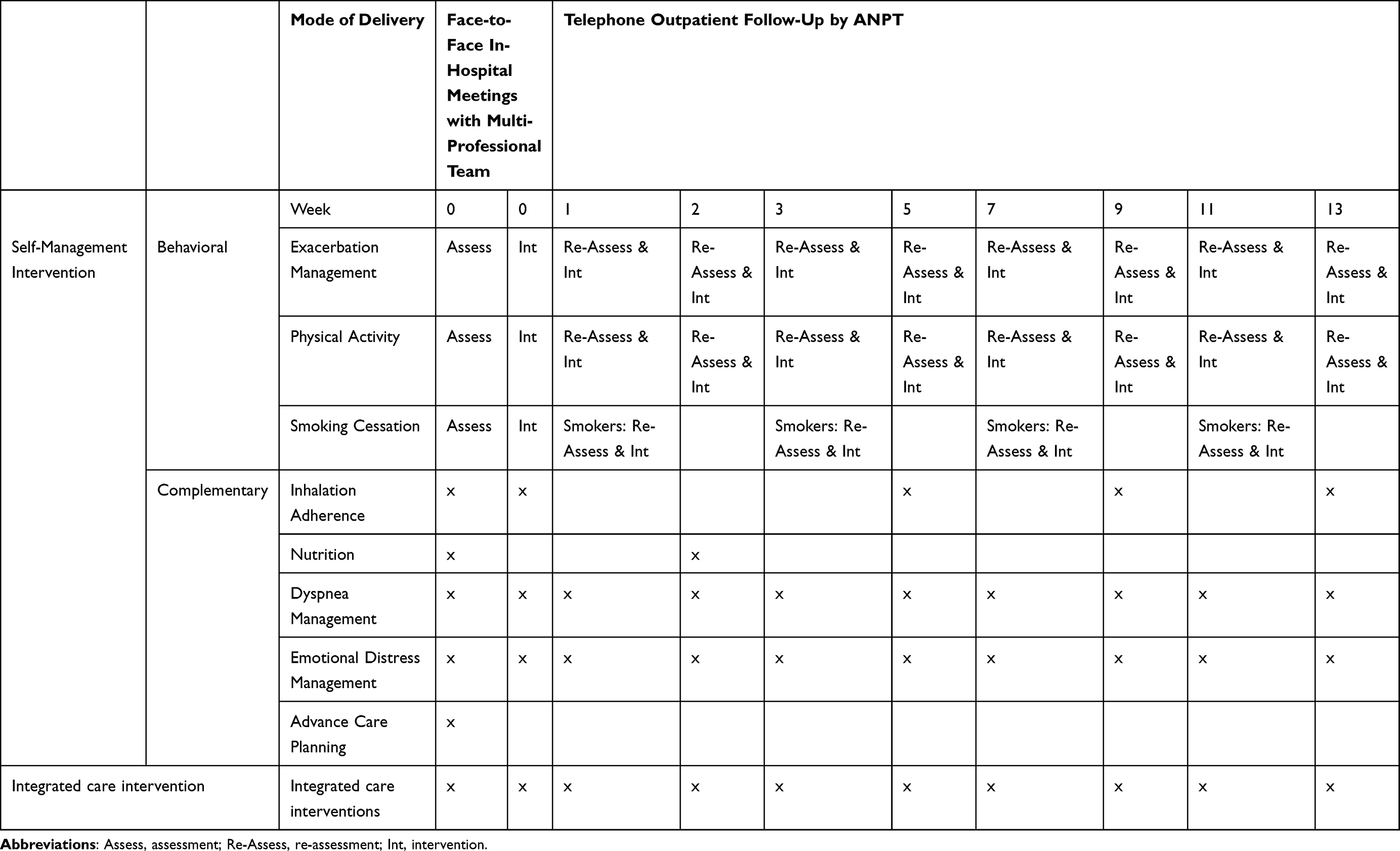 |
Table 6 Overview of the Nurse-Led Integrated Care COPD (NICCO) Intervention |
Assessment
First Assessment
For the basic intervention, the following interview-based assessment is conducted with the patient:
- Exacerbation Management: Checks for existence of a written exacerbation action plan and documentation system, history of exacerbations, patient’s exacerbation management, GPs’ attitudes toward self-medication.
- Physical Activity and Pulmonary Rehabilitation: Asks about minutes of physical activity per day, intensity (assessed by rating of perceived exertion on Borg Scale), muscle strength exercises (type, length and number of sessions per week), most recent pulmonary rehabilitation (including its time), and motivation for participating in future pulmonary rehabilitation.
- Smoking: Smoking status and history of smoking. Smokers self-rate motivation to stop smoking or self-confidence to keep up non-smoking status – both on a ten-point numeric scale (range: 1–10).
The first assessment is complemented by a set of predefined criteria which the ANPT answers based on his or her impression of the patient (Table 7). These were developed based on the literature and refined via discussion within the working group. This assessment guides the decision of whether the patient’s action plan should include self-medication.
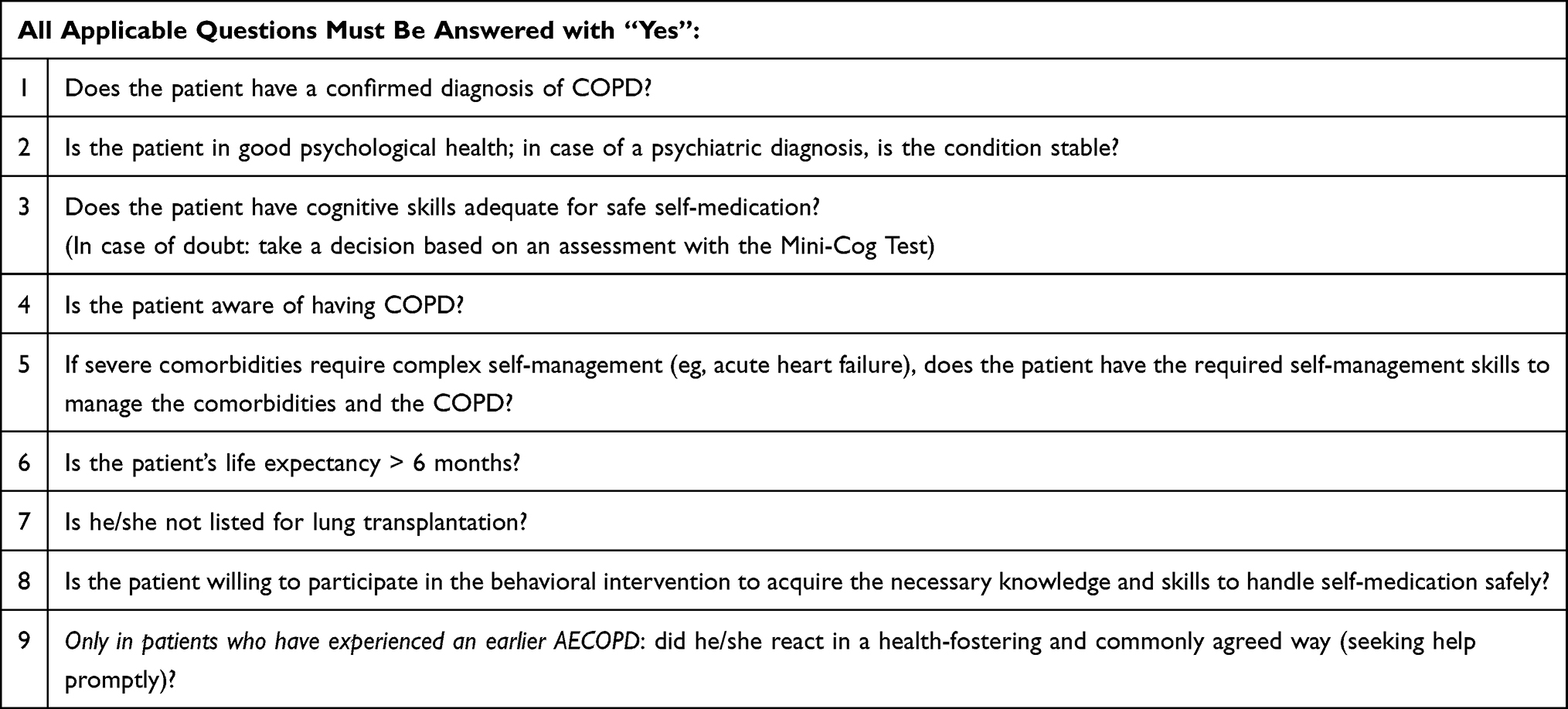 |
Table 7 Patient Criteria for Action Plan with Self-Medication |
Re-Assessment
During the follow-up calls, re-assessment is performed via a patient interview covering the following topics:
- Exacerbation Management: current state of health, numbers and times of “orange” and “red” days, actions taken on such days (explained in the next paragraph).
- Physical Activity and Pulmonary Rehabilitation: minutes of physical activity per day and intensity (assessed by the Borg Scale); frequency, type and length of muscle strength exercises per week, whether activities were supervised or non-supervised.
- Smoking: only in smokers: current smoking status and motivation to stop smoking. For those who have stopped smoking, self-confidence to keep up non-smoking status is also rated. Both ratings use a 10-point numeric scale (range: 1–10).
Behavioral Intervention
Exacerbation Management
Based on the patient’s first assessment, the ANPT delivers the corresponding BCTs. These vary depending on whether or not the patient’s action plan includes the option of self-medication. In either case, criteria for green, orange and red days are presented. Green indicates that the symptoms (cough, sputum, breathlessness and range of physical activity) fall within the normal day-to-day range; correspondingly, actions taken belong to the normal therapeutic regimen. Orange indicates that the symptoms (or symptom clusters) are somewhat more severe, frequent or otherwise worse than usual. In this case, patients are encouraged to take specific actions, but do not need to contact a health provider first. If the patient fulfills the criteria for self-medication, this part contains the prescription for a corticosteroid and if appropriate, an antibiotic regimen. In case of starting a corticosteroid and/or antibiotic regimen, patients are requested to inform their GPs. The ANPT drafts the action plan based on the current exacerbation treatment and a commonly agreed checklist. The physician checks the draft, prescribes the medication and carries the final responsibility for the prescription. For the final prescription to be added to the action plan, it must be double-checked and signed by two members of the ANPT.
Red indicates either that the symptoms or symptom clusters are much more severe, frequent or otherwise worse than usual or that they do not improve after 48 hours despite actions taken. Symptoms in the red area require that the patient immediately contact a physician. For the follow-up interventions, adherence to the three target behaviors is assessed; depending on the result, a new set of BCTs may be necessary.
Physical Activity
All patients receive BCTs for physical activity from all three involved professions. During the hospital stay, the PT delivers this intervention component, which is adjusted according to the PT’s risk assessment regarding potential falls and the patient’s capacity level. This includes but is not restricted to self-measurement of oxygen saturation and heart rate. After the patient returns home, the “Exercising 30 min/day – ANPT” intervention is delivered by the ANPT during the first two telephone calls. This intervention component builds on that already delivered by the PT during the hospital stay. For the follow-up calls, the BCTs chosen depend on the patient’s adherence to the relevant target behavior.
Smoking Cessation
The BCTs patients receive for this component is based on the results of the earlier assessment of smoking/non-smoking status and related points (Table 8) following the 5A method—ask, advice, assess, assist, arrange.29 The physician urges those who still smoke to stop, prescribing nicotine replacement products as a standard procedure.30 Depending on the assessment, smoking cessation counselling may be offered. Such counselling is mandatory for patients who request additional smoking cessation medication. Reassessment is ideally conducted once monthly, but the actual scheduling depends on discussion and agreement with the patient.
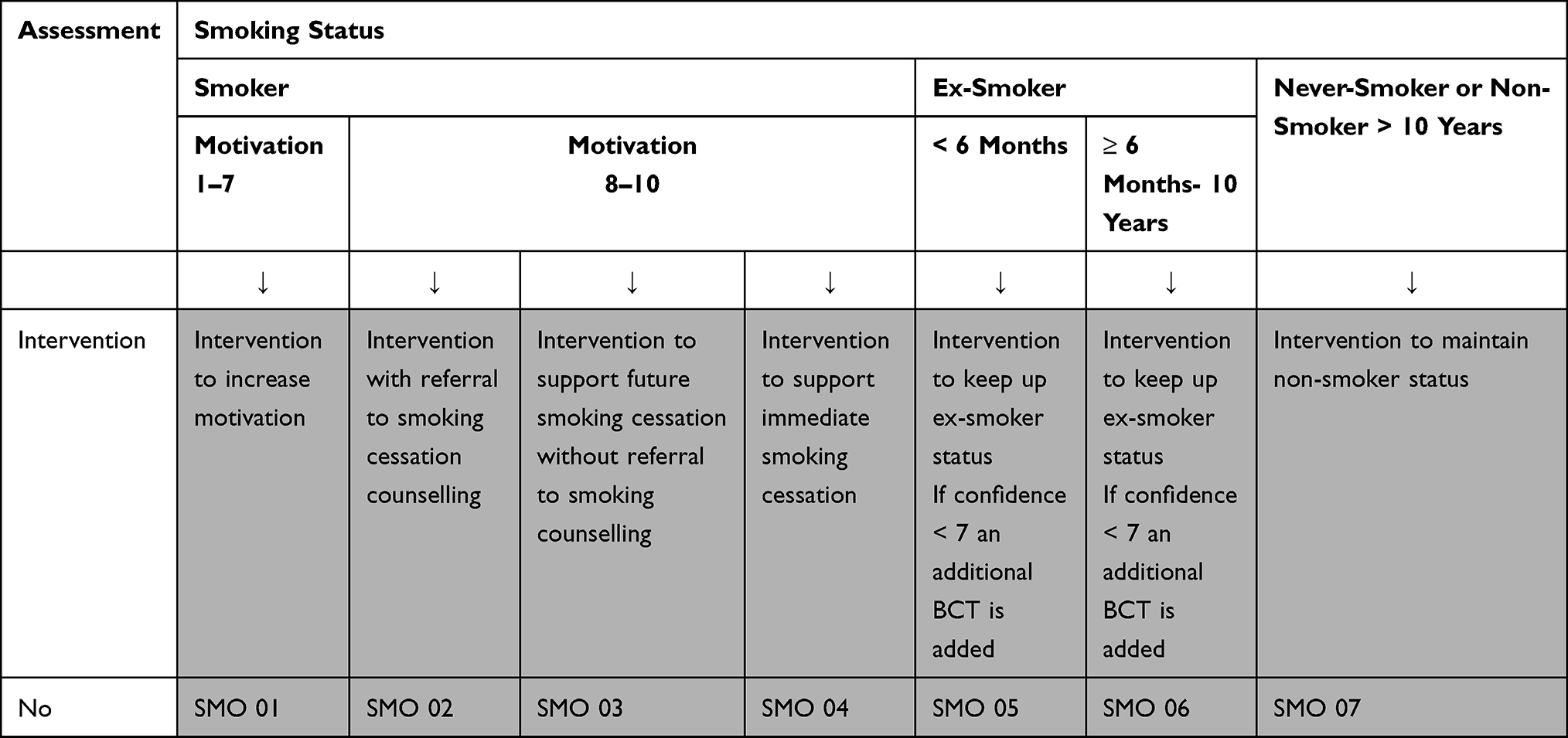 |
Table 8 Intervention Packages for Different Patient Smoking Situations After AECOPD |
Discussion
This paper describes the development of a hospital-initiated intervention to support patient behavior change during and after AECOPD. The intervention’s primary aim is to reduce the risk for respiratory-related rehospitalization and improve patients’ QoL. For this, the behavior change wheel provided a systematic framework to guide the intervention’s development. To handle the heterogeneity of the patient situations and meet the demand for standardization, we used assessment-guided delivery. Each patient’s assessment determines which sets of BCTs are delivered by the physiotherapist, the ANPT and the physician. This procedure has the advantage of tailoring the intervention to the most relevant patient characteristics while keeping it standardized to a large extent. One disadvantage is that delivery of the intervention is rather complex for the involved health professionals, especially the ANPT. Therefore, feasibility, appropriateness and acceptance from health professionals must be carefully evaluated in a future step.
Compelling evidence supports pairing self-management training with action plans that include self-medication. By improving patients’ recognition and responses to early signs of AECOPD, such plans lead first to improved self-efficacy regarding exacerbation management, then to reduced hospitalizations and rehospitalizations.4,26,32 As our study’s HPs were hesitant to trust all patients with the responsibility of self-medication, we developed and included a set of commonly agreed criteria for self-management competency as part of the intervention. Still, the appropriateness of self-medication is a valid concern: regular assessments will be essential to ensure patient safety.
In addition, there is also an ongoing need to reduce exacerbations by closing the gap between empirical knowledge and standard clinical practice. This may require not only training HP’s but also creating environments that enhance their self-management support skills. For one broadly implemented care bundle in the UK, perks including drop-in education on the intervention ward, process refinement via weekly projects, rewards for nurses’ fidelity to the intervention, opportunities to attend pulmonary rehabilitation sessions, and patient participation in producing the pulmonary rehabilitation leaflet led to increased patient enrolment and high intervention fidelity in nurses. This indicates that, as participative implementation strategies can be surprisingly effective, they should be considered for any further implementation.62 Future steps could include the development of an intervention to support HPs’ intervention delivery behavior.
Although physical activity’s health benefits are broadly documented and it is an important part of COPD non-pharmacological treatment,63 its integration in daily life is challenging for patients. One commonly recommended intervention in chronically ill populations is to use objective measurement devices such as pedometers or accelerometers to increase self-efficacy.64 However, pedometers are also reported by patients with COPD to cause a feeling of being controlled and under stress.65 Therefore, we decided to recommend their use only in a subsample that experiences low self-efficacy as a barrier to physical activity. This approach will be carefully evaluated in the ongoing project.
Although high fidelity was reported in the UK study’s nurses to the delivery of the care bundle,62 only 33% of patients were available for a follow-up intervention. One reason for this steep drop-off may be that members of the target patient population typically live with multiple comorbidities, leaving them heavily burdened. Regarding our intervention, the focus on behavior may decrease patients’ acceptance of the behavior change intervention. Especially those who have experienced little past success in behavior change are at risk for quitting the intervention. This intervention may also be challenging for patients who do not wish to reflect deeply on their COPD. One successful strategy to increase patients’ acceptance of our offered intervention was to deliver it through a 1:1 allocated advanced practice nurse who patients experienced as competent and trustworthy. Also, patients with COPD typically appreciate personal face-to-face encounters that include psychological and social support.66 Therefore, the embedding of the behavioral intervention within a broader care programme that addresses psychosocial aspects, burdensome emotions and dyspnea management may enhance acceptability. The element of personal contact at the hospital may also have a positive impact: a recent study showed that personal contact positively influenced the uptake of pulmonary rehabilitation.67 However, it may be a challenge for the ANPT to lay the foundation for a trustful relationship within the time-frame of just two face-to-face meetings. Further, regarding the nurse-patient relationship, the BCW guidelines’ suggestion that each nurse adapt his or her behavior to meet patients’ expectations requires nurses with particularly strong interpersonal skills.61 This intervention was developed for ward admissions but could be adapted for use with emergency department discharges as well. In that case, the adaption should include the possibility to build a trustful relationship, very likely supplemented with home visits.
Future evaluations will involve the investigation of implementation and effectiveness outcomes.68 Regarding implementation outcomes, we intend to gauge the current intervention’s feasibility and investigate potential barriers and facilitators of its delivery. The intervention’s impacts on QoL and rehospitalization rate will be investigated in a pilot study.
Conclusions
With this report, we have presented the development process of a complex hospital-initiated intervention that addresses patient health behaviors known to affect respiratory-related outcomes. The BCW provided an extremely useful framework for the development of this study’s COPD intervention, which will be delivered by a multi-professional core team. To satisfy the competing needs for standardization and patient-tailored adaption, we used an assessment-guided delivery system. As the strong focus on behavior change may threaten many patients’ motivation to participate, we tried to increase acceptability by embedding the behavioral intervention in a comprehensive care model that also addresses psychosocial needs. A next step will be to assess the intervention’s feasibility, acceptability, appropriateness and fidelity. Depending on those findings, the development of a behavioral intervention for the HPs delivering the interventions may also be useful. In addition, further specific research will be necessary to evaluate the intervention’s effectiveness on respiratory-related outcomes.
Abbreviations
AECOPD, acute exacerbations of COPD; BCW, Behavior Change Wheel; BCT, Behaviour Change Technique; COM-B, Capability-Opportunity-Motivation-Behaviour; TDF, Theoretical Domains Framework; ANPT, advanced nursing practice nurse team; HPs, health professionals; GOLD, Guidelines of the Global Initiative for Chronic Obstructive Lung Disease; PA, physical activity; PR, pulmonary rehabilitation; GP, general practitioner; PT, physiotherapist; PHY, physician.
Acknowledgments
We thank our colleagues of the University Hospital Zurich for their valuable collaboration in the development of the intervention: Matthias Peterer, Dr. Dario Kohlbrenner, and Céline Aregger in the “physical activity” working group; Corinne Steinbrüchel, Adina Wehrle, and Dr. Fiorenza Gautschi in the “exacerbation management” working group; Susanne Nicca and Christina Gassmann in the “healthy diet” working group; Severine Bruhin and Michael Klute in the “social issues” working group; Markus Feuz in the “advance care planning” working group; Ralf Schiemer and Eva Horvath in the “inhalation adherence” working group; Dr. Daniela Jordan and Mirella Palamar in the “emotional distress” working group; and Elena Hoffmann and Nicole Wassmer in the “dyspnea management” working group. We also thank this project’s external stakeholders for assessing the final intervention for relevance and transferability to other settings: Maya Spallinger, who lives with COPD, Florian Fehlmann from LUNGE ZUERICH, PD Dr. Marc Spielmanns from RehaKlinik Wald, Deborah Janz from Spitex Sihl and Rachel Jenkins from Spitex Zürich Limmat. Further thanks go to Dr. Anja Frei and Dr. Thomas Radtke of University Zurich’s Epidemiology, Biostatistics and Prevention Institute for their expert opinions on the physical activity intervention. Likewise, we are grateful to Prof. Dr. Stefan Büchi, Privatklinik Hohenegg for his expert input regarding the emotional distress intervention, and to Prof. Dr. Milo Puhan, also of University Zurich’s Epidemiology, Biostatistics and Prevention Institute, for his methodological advice regarding the development of the overall intervention. From UH Zurich we also owe many thanks to Annina Baltes-Wieser, Head of Nursing in the Heart-Vascular-Thorax Department, to Heidi Petry (PhD, RN), Head of the Centre of Clinical Nursing Science, to Malcolm Kohler (MD), Head of the Heart-Vascular-Thorax Department and Pulmonology Division, to Gabi Brenner, Director of Nursing, and to Christine Meier, Head of Physiotherapy Occupational Therapy, Monika Anderegg, Head of Pulmonology Ward, for their consistent, ongoing and energetic support of this project. We thank Chris Shultis for editing support. Finally, we thank LUNGE ZUERICH Switzerland for their generous financial support.
Funding
This work was supported by unrestricted research grant by LUNGE ZUERICH, Switzerland.
Disclosure
Claudia Steurer-Stey: reports receiving grants from AstraZeneca Schweiz, GSK Schweiz, consulting fees as an advisory board member and speaker honoraria from AstraZeneca Schweiz, GSK Schweiz and Novartis Schweiz. Paul Chadwick: received speakers honoraria for talks delivered to Roche. Christian Clarenbach: received advisory fees from Roche, Novartis, Boehringer, GSK, Astra Zeneca, Sanofi, Vifor, OM Pharma, Grifols, Daiichi Sankyo and Mundipharma. The authors report no other conflicts of interest in this work. Paul Chadwick and Christian Clarenbach share the senior authorship.
References
1. Giacomini M, DeJean D, Simeonov D, Smith A. Experiences of living and dying with COPD: a systematic review and synthesis of the qualitative empirical literature. Ont Health Technol Assess Ser. 2012;12(13):1–47.
2. Gutierrez Villegas C, Paz-Zulueta M, Herrero-Montes M, Paras-Bravo P, Madrazo Perez M. Cost analysis of chronic obstructive pulmonary disease (COPD): a systematic review. Health Econ Rev. 2021;11(1):31. doi:10.1186/s13561-021-00329-9
3. The Lancet. Complexities of care in COPD. Lancet. 2017;389(10069):574. doi:10.1016/s0140-6736(17)30327-6
4. Lenferink A, Brusse-Keizer M, van der Valk PD, et al. Self-management interventions including action plans for exacerbations versus usual care in patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017;8:Cd011682. doi:10.1002/14651858.CD011682.pub2
5. Zwerink M, Brusse-Keizer M, van der Valk PD, et al. Self management for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014;(3):Cd002990. doi:10.1002/14651858.CD002990.pub3
6. Kruis AL, Smidt N, Assendelft WJ, et al. Integrated disease management interventions for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2013;(10):CD009437. doi:10.1002/14651858.CD009437.pub2
7. Schrijver J, Lenferink A, Brusse-Keizer M, et al. Self-management interventions for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2022;1:CD002990. doi:10.1002/14651858.CD002990.pub4
8. Poot CC, Meijer E, Kruis AL, Smidt N, Chavannes NH, Honkoop PJ. Integrated disease management interventions for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2021;9:CD009437. doi:10.1002/14651858.CD009437.pub3
9. Harrison SL, Janaudis-Ferreira T, Brooks D, Desveaux L, Goldstein RS. Self-management following an acute exacerbation of COPD: a systematic review. Chest. 2015;147(3):646–661. doi:10.1378/chest.14-1658
10. Majothi S, Jolly K, Heneghan NR, et al. Supported self-management for patients with COPD who have recently been discharged from hospital: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2015;10:853–867. doi:10.2147/COPD.S74162
11. Puhan MA, Gimeno-Santos E, Cates CJ, Troosters T. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2016;12:CD005305. doi:10.1002/14651858.CD005305.pub4
12. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
13. Michie S, Atkins L, West R. The Behaviour Change Wheel - a Guide to Designing Interventions. Silverback Publishing; 2014.
14. Stanton-Fay SH, Hamilton K, Chadwick PM, et al. The DAFNEplus programme for sustained type 1 diabetes self management: intervention development using the behaviour change wheel. Diabet Med. 2021;38(5):e14548. doi:10.1111/dme.14548
15. Smalley KR, Aufegger L, Flott K, Mayer EK, Darzi A. Can self-management programmes change healthcare utilisation in COPD?: a systematic review and framework analysis. Patient Educ Couns. 2021;104(1):50–63. doi:10.1016/j.pec.2020.08.015
16. Wshah A, Selzler AM, Hill K, Brooks D, Goldstein R. Determinants of sedentary behaviour in individuals with COPD: a qualitative exploration guided by the theoretical domains framework. COPD. 2020;17(1):65–73. doi:10.1080/15412555.2019.1708883
17. Vuong K, Hermiz O, Razee H, Richmond R, Zwar N. The experiences of smoking cessation among patients with chronic obstructive pulmonary disease in Australian general practice: a qualitative descriptive study. Fam Pract. 2016;33(6):715–720. doi:10.1093/fampra/cmw083
18. Cheng SWM, Alison J, Dennis S, et al. A behaviour change intervention to reduce sedentary time in people with chronic obstructive pulmonary disease: protocol for a randomised controlled trial. J Physiother. 2017;63(3):182. doi:10.1016/j.jphys.2017.04.001
19. Cavalheri V, Straker L, Gucciardi DF, Gardiner PA, Hill K. Changing physical activity and sedentary behaviour in people with COPD. Respirology. 2016;21(3):419–426. doi:10.1111/resp.12680
20. Janjua S, Banchoff E, Threapleton CJ, Prigmore S, Fletcher J, Disler RT. Digital interventions for the management of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2021;4:CD013246. doi:10.1002/14651858.CD013246.pub2
21. Schmid-Mohler G, Clarenbach C, Brenner G, et al. Advanced nursing practice in COPD exacerbations: the solution for a gap in Switzerland? ERJ Open Res. 2020;6(2):00354–2019. doi:10.1183/23120541.00354-2019
22. Brouwers MC, Kho ME, Browman GP, et al. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010;182(18):E839–42. doi:10.1503/cmaj.090449
23. Critical Appraisal Skills Programme. CASP systematic review checklist. Available from: https://casp-uk.net/casp-tools-checklists/.
24. Atkins L, Francis J, Islam R, et al. A guide to using the theoretical domains framework of behaviour change to investigate implementation problems. Implement Sci. 2017;12(1):77. doi:10.1186/s13012-017-0605-9
25. COPD Lww. Living well with COPD. Available from: www.livingwellwithcopd.com.
26. Steurer-Stey C, Dalla Lana K, Braun J, Ter Riet G, Puhan MA. Effects of the “living well with COPD” intervention in primary care: a comparative study. Eur Respir J. 2018;51(1):1701375. doi:10.1183/13993003.01375-2017
27. Van Eerd EA, Van der Meer RM, Van Schayck OC, Kotz D. Smoking cessation for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2016;8:CD010744. doi:10.1002/14651858.CD010744.pub2
28. Stolz D, Barandun J, Borer H, et al. Diagnosis, prevention and treatment of stable COPD and acute exacerbations of COPD: the Swiss recommendations 2018. Respiration. 2018;96(4):382–398. doi:10.1159/000490551
29. Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease: 2022 Report; 2021.
30. Cornuz J, Jacot Sadowski I, Humair J-P. Ärztliche Rauchstoppberatung: Die Dokumentation für die Praxis. Vol. 3. Projekt FREI VON TABAK, Nationales Rauchstopp-Programm; 2015.
31. Global Initiative for Chronic Obstructive Lung Disease. Pocket guide to COPD diagnosis, management and prevention - a guide for health care professionals. J COPD Found. 2017;4(3):177.
32. Howcroft M, Walters EH, Wood-Baker R, Walters JA. Action plans with brief patient education for exacerbations in chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2016;12:CD005074. doi:10.1002/14651858.CD005074.pub4
33. McCabe C, McCann M, Brady AM. Computer and mobile technology interventions for self-management in chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017;5:CD011425. doi:10.1002/14651858.CD011425.pub2
34. McLean S, Nurmatov U, Liu JLY, Pagliari C, Car J, Sheikh A. Telehealthcare for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2011;2012(7). doi:10.1002/14651858.CD007718.pub2
35. Ferreira IM, Brooks D, White J, Goldstein R. Nutritional supplementation for stable chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;(12). doi:10.1002/14651858.CD000998.pub3
36. McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;(2). doi:10.1002/14651858.CD003793.pub3
37. Wong CX, Carson KV, Smith BJ. Home care by outreach nursing for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2012;(4):CD000994. doi:10.1002/14651858.CD000994.pub3
38. Burge AT, Cox NS, Abramson MJ, Holland AE. Interventions for promoting physical activity in people with chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2020;4(4). doi:10.1002/14651858.CD012626.pub2
39. Aumann I, Tedja L, von der Schulenburg JMG. Experiences of COPD patients with existing smoking cessation programs and their preferences for improvement - A qualitative analysis. Tob Induc Dis. 2016;14(1):31. doi:10.1186/s12971-016-0097-4
40. Chang YY, Dai YT, Chien NH, Chan HY. The lived experiences of people with chronic obstructive pulmonary disease: a phenomenological study. J Nurs Scholarsh. 2016;48(5):466–471. doi:10.1111/jnu.12230
41. Schroedl CJ, Yount SE, Szmuilowicz E, Hutchison PJ, Rosenberg SR, Kalhan R. A qualitative study of unmet healthcare needs in chronic obstructive pulmonary disease. A potential role for specialist palliative care? Ann Am Thorac Soc. 2014;11(9):1433–1438. doi:10.1513/AnnalsATS.201404-155BC
42. Andersen IC, Thomsen TG, Bruun P, Bodtger U, Hounsgaard L. The experience of being a participant in one’s own care at discharge and at home, following a severe acute exacerbation in chronic obstructive pulmonary disease: a longitudinal study. Int J Qual Stud Health Well-Being. 2017;12(1):1371994. doi:10.1080/17482631.2017.1371994
43. Torheim H, Kvangarsnes M. How do patients with exacerbated chronic obstructive pulmonary disease experience care in the intensive care unit? Scand J Caring Sci. 2014;28(4):741–748. doi:10.1111/scs.12106
44. Thorpe O, Johnston K, Kumar S. Barriers and enablers to physical activity participation in patients with COPD: a systematic review. J Cardiopulm Rehabil Prev. 2012;32(6):359–369. doi:10.1097/HCR.0b013e318262d7df
45. Kosteli MC, Heneghan NR, Roskell C, et al. Barriers and enablers of physical activity engagement for patients with COPD in primary care. Int J Chron Obstruct Pulmon Dis. 2017;12:1019–1031. doi:10.2147/copd.s119806
46. Mathar H, Fastholm P, Hansen IR, Larsen NS. Why do patients with COPD decline rehabilitation. Scand J Caring Sci. 2016;30(3):432–441. doi:10.1111/scs.12268
47. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2021 report; 2020:164. Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
48. Korpershoek Y, Vervoort S, Nijssen L, Trappenburg J, Schuurmans MJ. Factors influencing exacerbation-related self-management in patients with COPD: a qualitative study. Int J Chron Obstruct Pulmon Dis. 2016;11:2977–2990. doi:10.2147/copd.s116196
49. Williams V, Hardinge M, Ryan S, Farmer A. Patients’ experience of identifying and managing exacerbations in COPD: a qualitative study. NPJ Prim Care Respir Med. 2014;24:14062. doi:10.1038/npjpcrm.2014.62
50. Brandt CL. Study of older adults’ use of self-regulation for COPD self-management informs an evidence-based patient teaching plan. Rehabil Nurs. 2013;38(1):11–23. doi:10.1002/rnj.56
51. Laue J, Melbye H, Risor MB. Self-treatment of acute exacerbations of chronic obstructive pulmonary disease requires more than symptom recognition - A qualitative study of COPD patients’ perspectives on self-treatment. BMC Fam Pract. 2017;18(1):8. doi:10.1186/s12875-017-0582-8
52. Gibson PG, Powell H, Coughlan J, et al. Self-management education and regular practitioner review for adults with asthma. Cochrane Database Syst Rev. 2003;(1):CD001117. doi:10.1002/14651858.CD001117
53. Langer D, Hendriks E, Burtin C, et al. A clinical practice guideline for physiotherapists treating patients with chronic obstructive pulmonary disease based on a systematic review of available evidence. Clin Rehabil. 2009;23(5):445–462. doi:10.1177/0269215509103507
54. Thorpe O, Kumar S, Johnston K. Barriers to and enablers of physical activity in patients with COPD following a hospital admission: a qualitative study. Int J Chron Obstruct Pulmon Dis. 2014;9:115–128. doi:10.2147/copd.s54457
55. Mathar H, Fastholm P, Lange P, Larsen NS. Why do patients decline participation in offered pulmonary rehabilitation? A qualitative study. Clin Rehabil. 2017;31(12):1674–1683. doi:10.1177/0269215517708821
56. Bartlett YK, Sheeran P, Hawley MS. Effective behaviour change techniques in smoking cessation interventions for people with chronic obstructive pulmonary disease: a meta-analysis. Br J Health Psychol. 2014;19(1):181–203. doi:10.1111/bjhp.12071
57. Andersen IC, Thomsen TG, Bruun P, Bødtger U, Hounsgaard L. The experience of being a participant in one’s own care at discharge and at home, following a severe acute exacerbation in chronic obstructive pulmonary disease: a longitudinal study. Int J Qual Stud Health Well-Being. 2017;12(1). doi:10.1080/17482631.2017.1371994
58. Hilberink SR, Jacobs JE, Schlösser M, Grol RP, Vries H. Characteristics of patients with COPD in three motivational stages related to smoking cessation. Patient Educ Couns. 2006;61(3):449–457. doi:10.1016/j.pec.2005.05.012
59. Kanner RE, Anthonisen NR, Connett JE. Lower respiratory illnesses promote FEV(1) decline in current smokers but not ex-smokers with mild chronic obstructive pulmonary disease: results from the lung health study. Am J Respir Crit Care Med. 2001;164(3):358–364. doi:10.1164/ajrccm.164.3.2010017
60. Miller WR, Rollnick S. Motivational Interviewing: Helping People Change.
61. Wiechula R, Conroy T, Kitson AL, Marshall RJ, Whitaker N, Rasmussen P. Umbrella review of the evidence: what factors influence the caring relationship between a nurse and patient? J Adv Nurs. 2016;72(4):723–734. doi:10.1111/jan.12862
62. Hopkinson NS, Englebretsen C, Cooley N, et al. Designing and implementing a COPD discharge care bundle. Thorax. 2012;67(1):90–92. doi:10.1136/thoraxjnl-2011-200233
63. Lee IM, Shiroma EJ, Lobelo F, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380(9838):219–229. doi:10.1016/S0140-6736(12)61031-9
64. Bravata DM, Smith-Spangler C, Sundaram V, et al. Using pedometers to increase physical activity and improve health: a systematic review. JAMA. 2007;298(19):2296–2304. doi:10.1001/jama.298.19.2296
65. Marklund S, Tistad M, Lundell S, et al. Experiences and factors affecting usage of an eHealth tool for self-management among people with chronic obstructive pulmonary disease: qualitative study. J Med Internet Res. 2021;23(4):e25672. doi:10.2196/25672
66. Baker E, Fatoye F. Patient perceived impact of nurse-led self-management interventions for COPD: a systematic review of qualitative research. Int J Nurs Stud. 2019;91:22–34. doi:10.1016/j.ijnurstu.2018.12.004
67. Barker RE, Kon SS, Clarke SF, et al. COPD discharge bundle and pulmonary rehabilitation referral and uptake following hospitalisation for acute exacerbation of COPD. Thorax. 2021;76:829–831. doi:10.1136/thoraxjnl-2020-215464
68. Proctor E, Silmere H, Raghavan R, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health. 2011;38(2):65–76. doi:10.1007/s10488-010-0319-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.