Back to Journals » Patient Preference and Adherence » Volume 16
Support Life Club: A New Model Based on Social Media Group Chats and Social Activities That Can Improve Adherence and Clinical Outcomes in Patients Receiving Cardiac Rehabilitation
Authors Zhang S, Zuo H, Meng X, Hu D
Received 7 April 2022
Accepted for publication 28 July 2022
Published 3 August 2022 Volume 2022:16 Pages 1907—1917
DOI https://doi.org/10.2147/PPA.S368615
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Sisi Zhang,1 Houjuan Zuo,1 Xiaoping Meng,2 Dayi Hu1,3
1Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Affiliated Hospital of Changchun Traditional Chinese Medicine, Changchun, People’s Republic of China; 3People’s Hospital of Peking University, Beijing, People’s Republic of China
Correspondence: Xiaoping Meng, Affiliated Hospital of Changchun Traditional Chinese Medicine, Gongnong Avenue No. 1478, Chaoyang District, Changchun, 130000, People’s Republic of China, Tel +86-13180889540, Email [email protected] Dayi Hu, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Jiefang Avenue No. 1095, Qiaokou District, Wuhan, 430000, People’s Republic of China, Tel +86-13901389171, Email [email protected]
Aim: To describe a new model, the Support Life Club (SLC), for participants of Phase II cardiac rehabilitation (CR) programs and to evaluate this model for adherence, completion rates, and clinical outcomes.
Methods: This retrospective study involved 391 consecutive patients who participated in an outpatient CR program between September 2016 and May 2020. The intervention group (SLC) was comprised of 198 patients who participated in education, WeChat-based group activity as well as outdoor activities, while the control group (non-intervention) was comprised of 193 cases. All patients attended a 12-week supervised outpatient CR program (three sessions per week, each lasting 40min). The intervention and control groups were compared for completion rates, Cardiopulmonary Exercise Test (CPET) results, Six-minute Walk Test (6MWT) distances, and Patient Health Questionnaire-9 (PHQ-9) scores.
Results: Patients in the intervention group attended at least 75% of the exercise training sessions more often than those in the control group (72.5% vs 40.41%, adjusted odds ratio (OR): 27.385; 95% CI: 10.2 to 73.6; P = 0.0000). Analysis of variance (2 × 2 ANOVA) revealed a significant group-by-time interaction in PHQ9 and 6MWT test results (p = 0.000).
Conclusion: The addition of SLC to a cardiac rehabilitation program resulted in better outcomes for PHQ9 and 6MWT tests and may be a useful strategy to improve exercise adherence.
Keywords: cardiac rehabilitation, support life club, adherence, completion rate, WeChat platform
Introduction
Major advances have been made in the diagnosis and treatment of cardiovascular disease (CVD). Nevertheless, it remains the leading cause of mortality worldwide, accounting for 40% of deaths in China.1–3 Effective preventive measures for reducing morbidity and mortality and for improving the quality of life and prognosis of this disease are essential. In this regard, cardiac rehabilitation (CR) is a multidisciplinary program consisting of exercise training, nutritional assessment, psychological intervention, risk factor modification, patient education, and counseling.4–8 It has been confirmed that CR is an effective intervention that reduces hospital readmission and mortality, while also improving the quality of life for patients with coronary artery disease. International guidelines recommend CR as a Class I for patients with coronary artery disease (CAD).9,10 Nevertheless, the utilization of CR remains suboptimal. Many eligible patients are not referred for CR programs, while many who do participate drop out.11 Data collected from the United States, Canada, Netherlands, and the United Kingdom indicate that less than 30% of eligible patients participate in CR.12–15 Of these, only 40–50% complete the full program, with 30–60% continuing to exercise for a further 6–12 months.16,17 In China, CR programs are still developing and have received scant attention to date. Of the 11.4 million coronary heart disease (CHD) patients in mainland China, only one-third receive education about CR and less than 10% receive an individualized prescription.18 Barriers to CR include gender, age, Medicare coverage, travel distance, financial status, multiple comorbidities, psychological barriers, low education level, living alone, patient motivation, and blocks in the referral system. Previous studies have reported several key strategies aimed at increasing the uptake of CR programs.19–22 The American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR), the American Heart Association (AHA), and the American College of Cardiology (ACC) have stated that home-based CR is an option for eligible patients.23,24 The Million Hearts Cardiac Rehabilitation Collaborative has developed a road map aimed at improving the CR participation rate from 20% to more than 70%.25 Systematic referral for CR after hospitalization and the use of web- or telephone-based CR programs have also been proposed in order to increase uptake.26 However, little consideration has been given to the effect of regional, cultural, economic, and educational diversity on the rate of CR uptake. In China, the medical system, healthcare providers, medical insurance policies, lack of facilities, and insufficient health awareness all contribute to low rates of CR participation and adherence. Hence, a new and more effective model is urgently needed to improve the uptake of traditional CR therapy in China.27
In many countries, community-based cardiac rehabilitation (CBCR) is an important component of the intervention.28 In this program, close cooperation between cardiologists, physical therapists, participants, and their families can improve the rates of referral and compliance. However, there is little evidence to support the success of this program in China. Alternatively, the Support Life Club (SLC) consists of doctors, nurses, rehabilitation therapists, patients, and their spouses. Medical practitioners establish connections with patients by forming a WeChat Group. Professional teams provide individualized instructions, high-level clinical care, and counseling in relation to prevention, prognosis, and rehabilitation. This enhances the patients’ self-management and consciousness while increasing their overall confidence, adherence, and completion rate. However, these benefits are based on theoretical models and we could not find any published evidence confirming the positive effects of SLC on CR adherence and completion rates. Therefore, in the present study, we hypothesized that the addition of SLC to CR would increase adherence. We studied SLC in a cohort of patients undergoing outpatient CR to examine its impacts on adherence and completion in a phase II CR program.
Method
This single-center retrospective study was conducted on 391 consecutive patients who were referred as outpatients to a phase II CR program between September 2016 and May 2020. Patients aged more than 18 years old who had previously been diagnosed with CVD were eligible for the study. All eligible patients who enrolled in the outpatient CR program at our center were included. Patients were excluded if they were unable to perform cardiopulmonary exercise testing (CPET) or phase II CR for any reason.
Patients self-selected into one of two groups: the SLC group, in which patients participated in SLC as an adjunct to the standard CR program; the control group, in which patients only participated in the outpatient CR program. The SLC details are described below. Data including demographics, etiologies, clinical factors, complications and outcomes were extracted from databases and hospital records in the CR center and cardiology unit. The requirement for informed consent was waived.
All patients undertook the six-minute walking test (6MWT) and the standard CPET at baseline and at the end of the outpatient CR program. Results were compared between the SLC and control groups.
Outpatient CR Program
Exercise training was supervised by trained physical therapists in the outpatient unit according to evidence-based clinical algorithms for the exercise prescription.29 The specific details were as follows: (a) Exercise method: patients exercise on a treadmill or cycle ergometer. (b) Exercise duration: each session lasts for 40 min, comprising 5 min of warm-up, 30 min of aerobic exercise, and 5 min of cool-down. (c) Exercise frequency: three times per week for 12 consecutive weeks. (d) Exercise intensity: all participants received individualized exercise prescriptions aimed at achieving 60% to 80% of the maximal heart rate measured in the CPET evaluation. (e) Monitoring: Electrocardiographs and blood pressure were recorded during exercise and monitored by cardiologists.
Support Life Club
This club is based on humanistic care and cooperation, with strong involvement by the participants. SLC consists of three components: an education program to increase participant awareness of the benefits and necessity of CR and how to cope with chronic heart disease; establishment of the WeChat-based group providing personalized supervision and instruction; and psychological intervention and therapy.30
Patient Education (PE)
The education program was held twice a month by one of the senior cardiologists and was approximately 90 to 120 minutes duration. It consisted of four modules: basic knowledge of CR; self-management of blood cholesterol, blood pressure (BP), blood glucose, and other risk factors; healthy lifestyle and healthy eating habits, smoking cessation, weight control, limitation of alcohol consumption; and physical activity. The main educator was usually an experienced cardiologist who started with a brief introduction of CR and emphasized the benefits to the patient. Each module focused on patient concerns about their disease, rather than monotonous presentations. Previous patients were also encouraged to share their successful experiences in the form of small-group discussions, thus strengthening participant motivation and confidence.
WeChat-Based Group Intervention
WeChat is one of the most popular social media applications and currently has more than 1 billion monthly active users worldwide.31,32
The WeChat group “Support Life Club” was established by a senior administrator in our team who was also responsible for quality control, technical support and access to the group. A total of 35 physicians, nurses, health care professionals and others were added to the group. Once the patient agreed to participate, a supervisor would include them in the group and provide the patient and their family with assistance on how to use the platform.
The four WeChat-based group services were as follows:
- Timely reminders: Staff in the group were responsible for reminding patients to take their medications on schedule and to consume more lean meat, fish, eggs, fruits, vegetables, roots and nuts, while limiting their dietary intake of grains, dairy products, processed foods, sugar and salts. Reminder messages about adhering to the CR program were also provided by phone.
- Multimedia Education: Text messages, voice mail and videos were used to deliver personalized prescriptions including pharmacological therapies, moderate exercise programs, smoking cessation, healthy diet, and psychological assessment by health care professionals, dietitians and cardiac nurses. Other materials related to the CR program were also released to the group in the form of electronic documents, pictures, videos, and web links.
- WeChat-based communication and consulting: All participants could communicate with doctors or physicians whenever required by using the group chat function in WeChat. The cardiologists or trained nurses would reply as soon as possible with comforting, interpretative, and encouraging words. Patients were also encouraged to discuss their disease, share their feelings, and express any concerns and worries about their prognosis and recovery within this group. Through this WeChat group platform, patients with similar symptoms could further discuss with each other and share their personal experiences.
- Convenient access to hospital: When patients experienced discomfort such as chest pain, or showed abnormal ECG or laboratory results, they could immediately consult or upload images to the WeChat group. The cardiologists in the group would read new entries as quickly as possible and then guide the patient on how to deal with their situation. In case of an emergency cardiac event such as ST-segment elevation myocardial infarction (STEMI), the medical staff on duty would organize for the patient to transfer to our percutaneous coronary intervention (PCI) center. The intervention personnel in the catheter room would be contacted via telephone or via the WeChat group. Following PCI treatment, the patient would be admitted to the cardiac care unit (CCU) for dynamic observation. No patient information or data was allowed to be shared on the WeChat platform. The supervisor would delete all images using the remote wiping function in the WeChat app. For other emergencies, the SLC also provides easy access to medical care instead of traditional consultation with a physician. The SLC group saves patient time by avoiding queuing for medical treatment and provides them with more convenient medical services.
Outdoor Activities
The SLC offers participants various outdoor and entertainment activities, including group singing, group dancing, theatrical performances, and nature hiking. The group singing was usually facilitated by the health teacher and supported by one or two experienced music leaders who provided music accompaniment (keyboard or accordion). The medical staff also engaged in this activity, and patients with limited singing ability were encouraged to participate. The main form of singing was a choir in the style of traditional Chinese stage art such as Chinese opera. In addition, nature hikes were held regularly in wetland parks and in national forest parks on important dates such as World Heart Day, World Tobacco Day, and National Hypertension Day. The clinicians participated as hike leaders and wore uniform clothing, provided health care, and handled any physical emergencies that arose in patients with heart disease. Small prizes were also awarded to patients in order to encourage participation in these activities. Outdoor activities were conducted once every three months on average and for up to two hours duration. Each session involved a person-centered approach intended to promote self-confidence and a sense of support and motivation amongst participants. Patient caregivers were also invited to join in the outdoor activities program.
Measures
Baseline variables that were recorded included age, gender, reason for referral, cardiovascular risk factors, and pharmacological history. Clinical parameters obtained from the electronic medical record included BP, total cholesterol (TC), low-density lipoprotein (LDL-C), high-density lipoprotein (HDL-C), triglycerides (TG), and hemoglobin.
The primary outcomes were exercise adherence and the total number of exercise sessions attended in the CR program. The secondary outcomes included exercise capacity and depression.
Adherence to CR was defined as the number of participants completing at least 75% of the assigned sessions. The cut-off value used was obtained from the European position statement recommendations.33 The completion rate refers to the total number of exercise sessions attended. The data was collected from patient medical records and exercise diaries.
A secondary outcome was exercise capacity as estimated by the distance travelled during the six-minute walking test (6MWT) and performed according to The American Thoracic Society guidelines.34
The peak exercise oxygen uptake (peak VO2, mL/kg/min), metabolic equivalent, and VO2 at the anaerobic threshold (AT) were measured by cardiopulmonary exercise testing (CPET) performed on an electromagnetically braked cycle ergometer (CARDIOVIT AT-104, Schiller, Switzerland). The protocol for CPET includes 3 min of warm-up, followed by incremental resistance of 10w per min until volitional exhaustion. Depression was assessed using the Patient Health Questionnaire-9 (PHQ-9), which is a validated 9-item self-report of major depression.35,36 Each item ranges from 0 (not at all) to 3 (nearly every day), with the total score ranging between 0 and 27.37
Statistical Analysis
Data were analyzed using SPSS software, version 25. Variables were compared between the intervention (SLC) and control groups. Continuous variables were reported as the mean ± SD and compared with independent samples or the Mann–Whitney U-test according to the data distribution. Categorical variables were described as frequencies or percentages and were compared using the chi-square test. Logistic regression analysis, which adjusts for selection bias and baseline parameters, was used to obtain the odds ratio (OR) and 95% confidence interval (CI) for adherence in the intervention group. P values of < 0.05 were considered statistically significant. A 2×2 analysis of variance (ANOVAs), with time (pre-intervention, post-intervention) as a within-subject variable and group (intervention, control) as a between-subject variable, was performed to assess the effects of SLC intervention on primary outcomes (PHQ9, 6MWT, peak VO2, peak Mets, and VO2@AT). Partial eta-squared (η2p) was expressed as the effect size, with higher values representing higher proportions of variance explained by the independent variable. The alpha level was set to 0.05.
Results
This study involved 393 patients, of which 200 were in the SLC intervention group and 193 were in the control group. The baseline characteristics of the two groups are shown in Table 1.
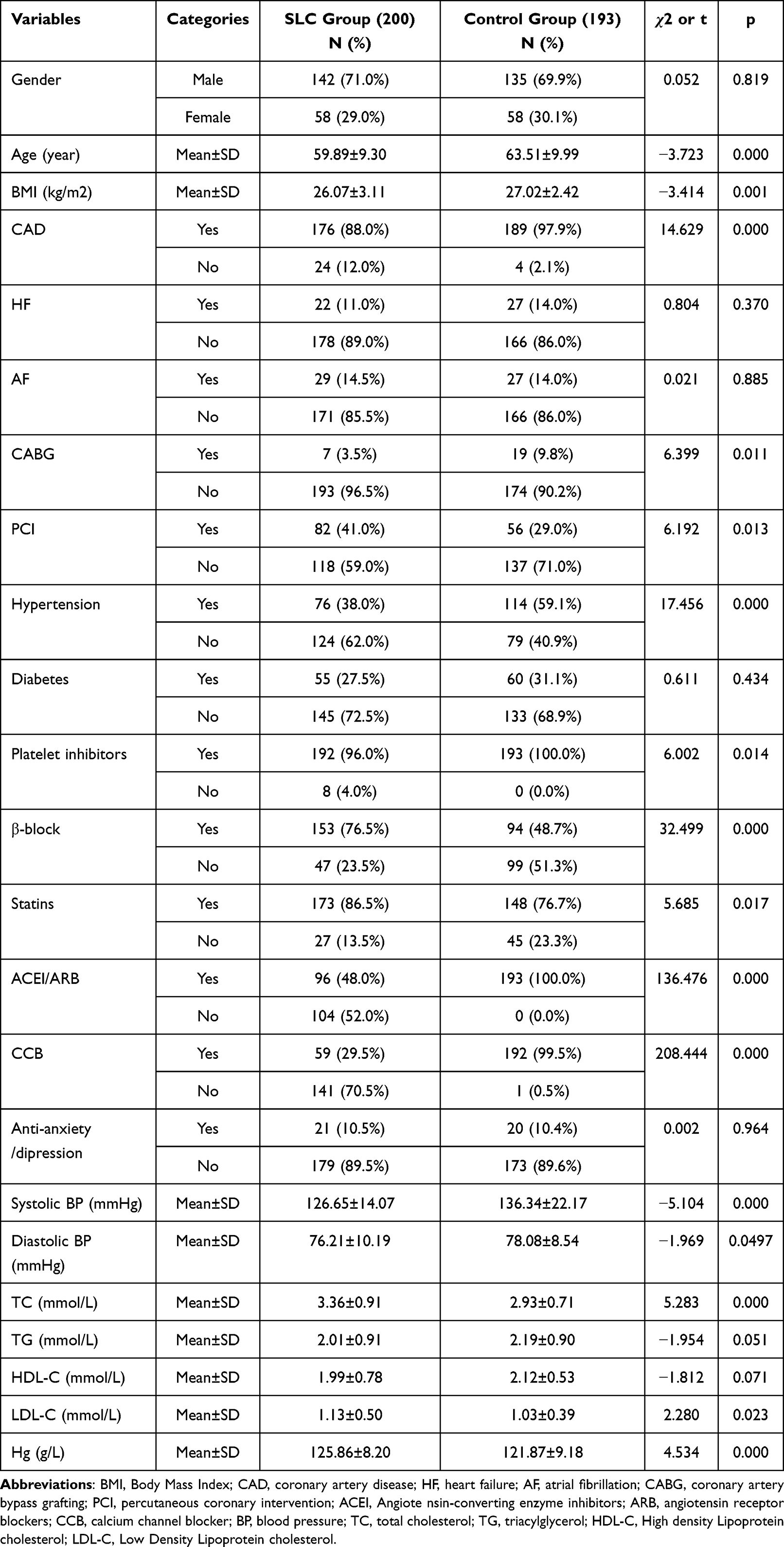 |
Table 1 Baseline Characteristics of Patients in Participation and Non-Participation Groups |
Patients in the SLC group showed a 55% decrease in their PHQ9 score (pre: 5.16 ± 5.53 vs post: 2.32 ± 2.87), while those in the control group showed a 39% decrease (pre: 2.61 ± 2.98 vs post: 1.59 ± 2.06). Repeated-measures ANOVA showed significant main effects of group and time (F = 23.09, P = 0.000, ηp2 = 0.049; and F = 168.03, P = 0.000, ηp2 = 0.067, respectively), and group-by-time interaction (F = 37.62, P = 0.000, ηp2 = 0.016).
An improvement of 6.6% in the 6MWT was observed in the SLC intervention group (pre: 650.48 ± 74.70 m vs post: 693.69 ± 81.78 m), while the control group improved by 1.4% (pre: 495.61 ± 72.76 m vs post: 502.57 ± 86.73 m). ANOVA revealed significant main effects of group and time (F = 514.032, P = 0.000, ηp2 = 0.545; and F = 98.456, P = 0.000, ηp2 = 0.025, respectively), and group-by-time interaction (F = 51.438, P = 0.000, ηp2 = 0.013).
Analysis of the results also found that both SLC and control groups showed significantly improved peak VO2 (P = 0.000, ηp2 = 0.013), peak Mets (P = 0.000, ηp2 = 0.0.01), and VO2@AT (p = 0.000, η2p = 0.25). However, no significant differences were found between the two groups.
In the SLC intervention group, 72.5% of patients adhered to at least 75% of the exercise-based CR sessions, compared to 40.41% in the control group (p = 0.000). The mean completion rate for exercise sessions in the intervention group was 28.95 ± 5.30 compared to 20.38 ± 8.31 in the control group (p = 0.000) (Table 2). Logistic regression analysis showed the SLC group had significantly better adherence compared with the control group (OR 27.385, 95% CI [10.2–73.6]; p = 0.000).
 |
Table 2 Adherence and Completion Rate Between Groups |
Discussion
This study found that the addition of SLC to a standard CR program improves exercise adherence and the number of patients who complete CR compared to a control group. Both the SLC and control groups showed statistically significant improvements in PHQ9 and exercise capacity at the end of CR. To our knowledge, this is the first study to investigate the effects of a novel intervention model on adherence and completion rates for CR in China. Several studies have reported different strategies for promoting adherence during CR, including self-monitoring, action planning, stress management, PE, telephone communication, small group interaction, early access to a cardiac clinic, and nurse practitioner-led CR.12 However, the risk of bias in these studies was relatively high. In the present study, 72.5% of patients in the SLC group attended more than 75% of the CR sessions. This rate was higher than that reported in recent studies. Furthermore, the completion rate was 80.4% for the SLC participants compared to previously reported completion rates of 13% to 39%.38,39 Moreover, patients who attend more than 25 sessions of the CR program are 19% less likely to die after five years compared to those who attend fewer sessions.40 The median completion rate of 80.4% observed in the present study with SLC patients was therefore an encouraging result.41
The results from this study show that both the SLC and control groups experienced clinical improvements in all of the outcome measures. These findings confirm the positive effects of exercise-based CR in helping patients to improve their cardiopulmonary fitness and psychological state. However, the completion rates were still not optimal, meaning that adherence to CR programs remains a critical challenge for enhancing exercise capacity in future interventions. In our study, patients who received the combination of SLC and CR showed a greater improvement in PHQ9 and 6MWT compared to those who participated only in the CR program (Table 3). Participants in the SLC program had significantly fewer symptoms and better exercise capacity post-program, confirming the importance of offering SLC as part of CR. These outcomes are consistent with a previous randomized controlled trial in which an exercise-focused smartphone app was effective at improving fitness levels (measured by Peak VO2) at a one-year follow-up.42 A Cochrane review also demonstrated the efficacy and safety of Web-based interventions, emphasizing the importance of factors such as multi-disciplinary team cooperation and educational visits.43 Lack of motivation, older age, living alone, low socioeconomic status, and lower educational level are known factors for low participation and high dropout rates in CR programs.12,38,39 Effective PE is associated with better psychological, physiological, and social health. Patients’ increased knowledge and awareness of CR can strengthen their motivation to participate, thus contributing to improved adherence. In the novel SLC model, PE is an important component that ensures the effectiveness and adherence of phase II CR.
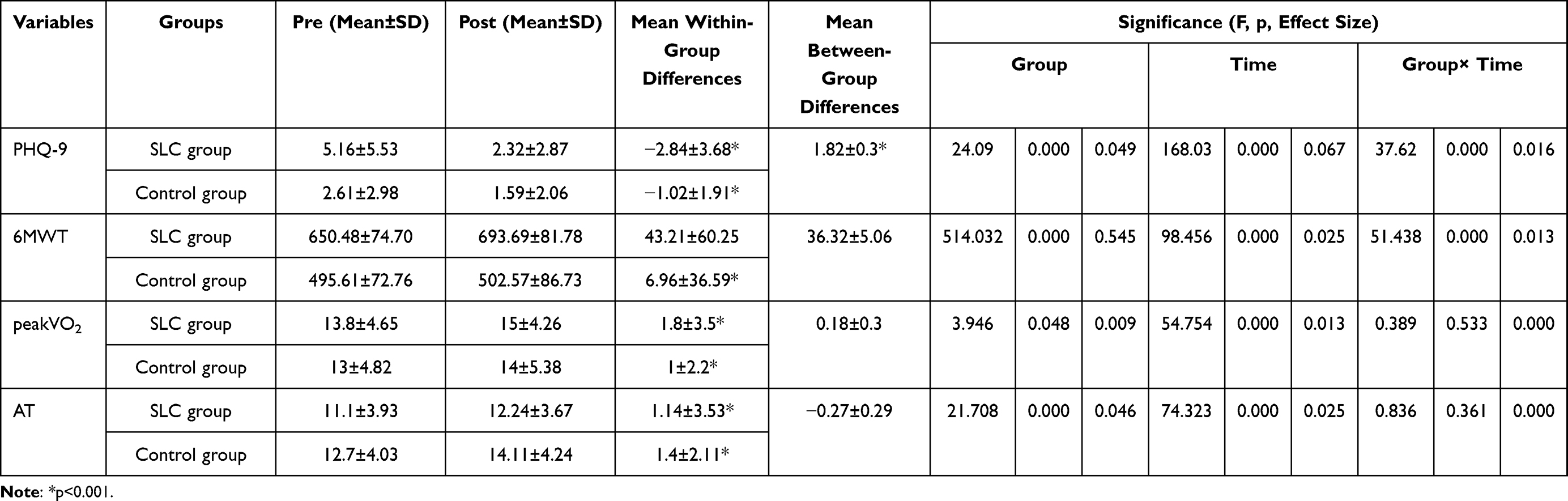 |
Table 3 Within-Group Change and Comparison of Between-Group Differences for the Two Groups |
In China, most patients have a strong desire to share their medical information with their health care provider. However, due to the lack of an interconnected working system and remote consultation platform, doctors cannot offer specialized consultation. Frequent and continuous reminders and communication play an important role in increasing patient adherence. It may be possible to strengthen the relationship between the patient and professional staff by adding telephone contact during the CR program. With this approach, patients would submit their daily food consumption, medicine intake, and exercise data and then receive a reminder phone call from select nurses who record any issues and problem-solve adherence. Previous studies have reported the effect of regular reminders on patient adherence to various preventive and management strategies.44 De Leon et al also described the positive results on behavioral changes over a short-term period.45 The WeChat app allows easy dissemination of information and is widely accepted by the public, especially the elderly population. A recent clinical trial found that the WeChat app could improve quality of life and lung function and contribute to better adherence.46 In the current study, SLC participants could share their health information, express their own experiences, encourage each other, and gain access to many medical and health care services.47 If these patients experience an emergency condition such as AMI or acute heart failure, convenient hospital access helps reduce their waiting time and guarantees timely treatment. Meanwhile, uploading the ECG or laboratory examination results and sharing medical records helps the medical staff make a rapid pre-hospital diagnosis. Consequently, the novel SLC model has significantly positive effects on clinical status and exercise adherence.
Patients with CHD usually have psychological issues such as stress, anxiety, helplessness, and feeling out of control.48 Uncertainty about their disease increases the fear of death in elderly CHD patients, primarily due to the lack of self-control.49 Access to multimedia education can improve the self-control felt by elderly people. The SLC group’s interactive model provides the guidance and freedom to satisfy patient needs in this regard.
Most eligible patients tend to become sedentary by one year after discharge. The reasons for this include insufficient educational resources, traffic difficulties, and psychological issues.50 Inadequate physical activity contributes to the prevalence of heart disease, stroke, diabetes, hypertension, depression, and cognitive decline, accounting for 1.9 million deaths worldwide each year.51 Walking is a common, accessible, low-risk, and easily accepted form of exercise by older adults. It has been shown to prevent chronic health conditions, improve physical and mental health, and reduce stress and negative emotions.52,53 Group walks allow participants to enjoy this activity even more, to engage in it more frequently, and to benefit from the social interaction that it affords in outdoor locations.54 The medical practitioners played a pivotal role in the successful delivery of this activity, providing both support and encouragement through interpretation and accompaniment.
Another core component of SLC is entertainment activities. Theatrical performances involving live interactions between patients and health providers provide a humanized and comfortable environment. This contrasts with the passive receiving of treatment and may lead to increased adherence. Moreover, different modalities of artistic performance can bring a range of psychological and health-related benefits. For example, choral singing may provide mental and emotional benefits, while listening to music can bring a sense of relaxation and wellbeing.55,56 Furthermore, the participation of health providers, including professors, doctors, nurses, and therapists, can increase social contact, reduce social isolation, and strengthen the confidence of participants.
The binary logistic regression analysis found that participation in SLC was significantly associated with good adherence to the CR program. The results of this study indicate that SLC has advantages in education, behavior, and psychological domains that may generally be applicable to increase adherence and completion rates in CR. The positive results obtained here provide more evidence of the benefits of SLC intervention and confirm the feasibility of this model in the CR program.
Limitation
As this was a retrospective study, some confounding factors were difficult to avoid. Moreover, we were unable to obtain some clinically important covariates with the database available for this research. Secondly, the sample size was limited and further prospective randomized studies are needed to confirm the utility of this novel model in routine clinical practice.
Conclusion
This Chinese study shows that SLC results in better adherence and completion rates in the phase II CR program. In turn, this could improve the exercise capacity and psychological state of patients.
Funding
There is no funding to report.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Deloukas P, Kanoni S, Willenborg C, et al. Large-scale association analysis identifies new risk loci for coronary artery disease. Nat Genet. 2013;45:25–33. doi:10.1038/ng.2480
2. Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392:1736–1788.
3. Zhao D, Liu J, Wang M, Zhang X, Zhou M. Epidemiology of cardiovascular disease in China: current features and implications. Nat Rev Cardiol. 2019;16:203–212. doi:10.1038/s41569-018-0119-4
4. Ambrosetti M, Abreu A, Corrà U, et al. Secondary prevention through comprehensive cardiovascular rehabilitation: from knowledge to implementation. 2020 update. A position paper from the secondary prevention and rehabilitation section of the European association of preventive cardiology. Eur J Prev Cardiol. 2021;28:460–495. doi:10.1177/2047487320913379
5. Wilhelm M, Abreu A, Adami PE, et al. EAPC core curriculum for preventive cardiology. Eur J Prev Cardiol. 2022;29(1):251–274. doi:10.1093/eurjpc/zwab017
6. Cho C, Lee C, Kim M, Kohzuki M. Effects of cardiac rehabilitation on health-related quality of life in patients with cardiovascular disease: a systematic review. Asian J Hum Serv. 2016;11:111–123. doi:10.14391/ajhs.11.111
7. Shepherd CW, While A. Cardiac rehabilitation and quality of life: a systematic review. Int J Nurs Stud. 2012;49:755–771. doi:10.1016/j.ijnurstu.2011.11.019
8. Salzwedel A, Jensen K, Rauch B, et al. Effectiveness of comprehensive cardiac rehabilitation in coronary artery disease patients treated according to contemporary evidence based medicine: update of the Cardiac Rehabilitation Outcome Study (CROS-II). Eur J Prev Cardiol. 2020;27(16):1756–1774. doi:10.1177/2047487320905719
9. Smith SC Jr, Allen J, Blair SN, et al. AHA/ACC guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease: 2006 update: endorsed by the national heart, lung, and blood institute. Circulation. 2006;113:2363–2372. doi:10.1161/CIRCULATIONAHA.106.174516
10. Piepoli MF, Hoes AW, Agewall S, et al. European Guidelines on cardiovascular disease prevention in clinical practice. Rev Esp Cardiol. 2016;2016(69):939.
11. Oosenbrug E, Marinho RP, Zhang J, et al. Sex differences in cardiac rehabilitation adherence: a meta-analysis. Can J Cardiol. 2016;32:1316–1324. doi:10.1016/j.cjca.2016.01.036
12. Jackson L, Leclerc J, Erskine Y, Linden W. Getting the most out of cardiac rehabilitation: a review of referral and adherence predictors. Heart. 2005;91:10–14. doi:10.1136/hrt.2004.045559
13. Van Engen-Verheul M, de Vries H, Kemps H, Kraaijenhagen R, de Keizer N, Peek N. Cardiac rehabilitation uptake and its determinants in the Netherlands. Eur J Prev Cardiol. 2013;20:349–356. doi:10.1177/2047487312439497
14. Candido E, Richards JA, Oh P, et al. The relationship between need and capacity for multidisciplinary cardiovascular risk-reduction programs in Ontario. Can J Cardiol. 2011;27:200–207. doi:10.1016/j.cjca.2011.01.008
15. Taylor RS, Brown A, Ebrahim S, et al. Exercise-based rehabilitation for patients with coronary heart disease: systematic review and meta-analysis of randomized controlled trials. Am J Med. 2004;116:682–692. doi:10.1016/j.amjmed.2004.01.009
16. Sanderson BK, Phillips MM, Gerald L, DiLillo V, Bittner V. Factors associated with the failure of patients to complete cardiac rehabilitation for medical and nonmedical reasons. J Cardiopulm Rehabil. 2003;23:281–289. doi:10.1097/00008483-200307000-00005
17. Bock BC, Carmona-Barros RE, Esler JL, Tilkemeier PL. Program participation and physical activity maintenance after cardiac rehabilitation. Behav Modif. 2003;27(1):37–53. doi:10.1177/0145445502238692
18. Cao X. Investigation and analysis on the status of stage I cardiac rehabilitation in 25 hospitals in Guangdong Province. J Nurs. 2012;6(19):28–30.
19. Bittner V, Sanderson B, Breland J, Green D. Referral patterns to a University-based cardiac rehabilitation program. Am J Cardiol. 1999;83:252–A5. doi:10.1016/S0002-9149(98)00830-3
20. Resurrección DM, Moreno-Peral P, Gómez-Herranz M, et al. Factors associated with non-participation in and dropout from cardiac rehabilitation programmes: a systematic review of prospective cohort studies. Eur J Cardiovasc Nurs. 2019;18:38–47. doi:10.1177/1474515118783157
21. Pardaens S, Willems AM, Clays E, et al. The impact of drop-out in cardiac rehabilitation on outcome among coronary artery disease patients. Eur J Prev Cardiol. 2017;24:1490–1497. doi:10.1177/2047487317724574
22. Sunamura M, Ter Hoeve N, Geleijnse ML, et al. Cardiac rehabilitation in patients who underwent primary percutaneous coronary intervention for acute myocardial infarction: determinants of program participation and completion. Neth Heart J. 2017;25:618–628. doi:10.1007/s12471-017-1039-3
23. Sun EY, Jadotte YT, Halperin W. Disparities in cardiac rehabilitation participation in the United States: a SYSTEMATIC REVIEW AND META-ANALYSIS. J Cardiopulm Rehabil Prev. 2017;37:2–10. doi:10.1097/HCR.0000000000000203
24. Evenson KR, Fleury J. Barriers to outpatient cardiac rehabilitation participation and adherence. J Cardiopulm Rehabil. 2000;20:241–246. doi:10.1097/00008483-200007000-00005
25. Ades PA, Keteyian SJ, Wright JS, et al. Increasing cardiac rehabilitation participation from 20% to 70%: a road map from the million hearts cardiac rehabilitation collaborative. Mayo Clin Proc. 2017;92:234–242. doi:10.1016/j.mayocp.2016.10.014
26. McLachlan A, Sutton T, Ding P, Kerr A, Nurse Practitioner A. Clinic: a novel approach to supporting patients following heart valve surgery. Heart Lung Circ. 2015;24:1126–1133. doi:10.1016/j.hlc.2015.04.064
27. Ragupathi L, Stribling J, Yakunina Y, Fuster V, Mclaughlin MA, Vedanthan R. Availability, use, and barriers to cardiac rehabilitation in LMIC. Glob Heart. 2016;12(4):323–334. doi:10.1016/j.gheart.2016.09.004
28. Perk J, Graham I. European guidelines on cardiovascular disease prevention in clinical practice (version 2012): the fifth joint task force of the European society of cardiology and other societies on cardiovascular disease prevention in clinical practice. Eur J Prev Cardiol. 2012;19:585–667.
29. Achttien RJ, Vromen T, Staal JB, et al. Development of evidence-based clinical algorithms for prescription of exercise-based cardiac rehabilitation. Neth Heart J. 2015;23(12):563–575. doi:10.1007/s12471-015-0761-y
30. Lynggaard V, May O, Beauchamp A, Nielsen CV, Wittrup I. LC-REHAB: randomised trial assessing the effect of a new patient education method–learning and coping strategies–in cardiac rehabilitation. BMC Cardiovasc Disord. 2014;14:186. doi:10.1186/1471-2261-14-186
31. Hui L, Cao Y. Examining WeChat users’ motivations, trust, attitudes, and positive word-of-mouth: evidence from China. Comput Hum Behav. 2014;41:104–111.
32. Hong YA, Zhou Z, Fang Y, Shi L. The digital divide and health disparities in China: evidence from a national survey and policy implications. J Med Internet Res. 2017;19:e317. doi:10.2196/jmir.7786
33. Abreu A, Frederix I, Dendale P, et al. Standardization and quality improvement of secondary prevention through cardiovascular rehabilitation programs in Europe: the avenue towards EAPC accreditation program: a position statement of the secondary prevention and rehabilitation section of the European Association of Preventive Cardiology (EAPC). Eur J Prev Cardiol. 2020: 2047487320924912. doi:10.1177/2047487320924912
34. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test [published correction appears in Am J Respir Crit Care Med. 2016 May 15;193(10):1185]. Am J Respir Crit Care Med. 2002;166:111–117. doi:10.1164/ajrccm.166.1.at1102
35. Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. primary care evaluation of mental disorders. patient health questionnaire. JAMA. 1999;282:1737–1744. doi:10.1001/jama.282.18.1737
36. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–613. doi:10.1046/j.1525-1497.2001.016009606.x
37. Wittkampf KA, Naeije L, Schene AH, Huyser J, van Weert HC. Diagnostic accuracy of the mood module of the patient health questionnaire: a systematic review. Gen Hosp Psychiatry. 2007;29:388–395. doi:10.1016/j.genhosppsych.2007.06.004
38. Ruano-Ravina A, Pena-Gil C, Abu-Assi E, et al. Participation and adherence to cardiac rehabilitation programs. A systematic review. Int J Cardiol. 2016;223:436–443. doi:10.1016/j.ijcard.2016.08.120
39. Kerins M, McKee G, Bennett K. Contributing factors to patient non-attendance at and non-completion of Phase III cardiac rehabilitation. Eur J Cardiovasc Nurs. 2011;10:31–36. doi:10.1016/j.ejcnurse.2010.03.006
40. Corones K, Coyer M, Theobald A. Exploring the information needs of patients who have undergone PCI. Br J Cardiac Nurs. 2009;4:123–130.
41. Aazami S, Jaafarpour M, Mozafari M. Exploring expectations and needs of patients undergoing angioplasty. J Vasc Nurs. 2016;34:93–99. doi:10.1016/j.jvn.2016.04.003
42. Lunde P, Bye A, Bergland A, Grimsmo J, Jarstad E, Nilsson BB. Long-term follow-up with a smartphone application improves exercise capacity post cardiac rehabilitation: a randomized controlled trial. Eur J Prev Cardiol. 2020;27(16):1782–1792. doi:10.1177/2047487320905717
43. Ivers N, Jamtvedt G, Flottorp S, et al. Audit and feedback: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2012;6:CD000259.
44. Cole-Lewis H, Kershaw T. Text messaging as a tool for behavior change in disease prevention and management. Epidemiol Rev. 2010;32(1):56–69. doi:10.1093/epirev/mxq004
45. De Leon E, Fuentes LW, Cohen JE. Characterizing periodic messaging interventions across health behaviors and media: systematic review. J Med Internet Res. 2014;16(3):e93. doi:10.2196/jmir.2837
46. Bi J, Yang W, Hao P, et al. WeChat as a platform for baduanjin intervention in patients with stable chronic obstructive pulmonary disease in China: retrospective randomized controlled trial. JMIR Mhealth Uhealth. 2021;9(2):e23548. doi:10.2196/23548
47. Xu J. Application of WeChat public platform in the health education of the hospital. J Health Educ China. 2015;31:86–87.
48. Pelle AJ, Denollet J, Zwisler AD, Pedersen SS. Overlap and distinctiveness of psychological risk factors in patients with ischemic heart disease and chronic heart failure: are we there yet? J Affect Disord. 2009;113:150–156. doi:10.1016/j.jad.2008.05.017
49. Qin L, Cui C, Huo Y, Yang X, Zhao Y. Clinical efficacy of physical factors combined with early psychological intervention in treatment of patients with chronic limb pain. Iran J Public Health. 2019;48:858–863.
50. Guiraud T, Granger R, Gremeaux V, et al. Accelerometer as a tool to assess sedentarity and adherence to physical activity recommendations after the cardiac rehabilitation program. Ann Phys Rehabil Med. 2012;55:312–321. doi:10.1016/j.rehab.2012.05.002
51. Norum KR. World Health Organization’s global strategy on diet, physical activity, and health: the process behind the scenes. Food Nutr Res. 2005;49(2):83–88. doi:10.1080/11026480510037147
52. Marselle MR, Irvine KN, Warber SL. Walking for well-being: are group walks in certain types of natural environments better for well-being than group walks in urban environments? Int J Environ Res Public Health. 2013;10:5603–5628. doi:10.3390/ijerph10115603
53. Roe J, Aspinall P. The restorative benefits of walking in urban and rural settings in adults with good and poor mental health. Health Place. 2011;17:103–113. doi:10.1016/j.healthplace.2010.09.003
54. Maas J, van Dillen SME, Verheij RA, Groenewegen PP. Social contacts as a possible mechanism behind the relation between green space and health. Health Place. 2009;15:586–595. doi:10.1016/j.healthplace.2008.09.006
55. Yung PM, Chui-Kam S, French P, Chan TM. A controlled trial of music and pre-operative anxiety in Chinese men undergoing transurethral resection of the prostate. J Adv Nurs. 2002;39:352–359. doi:10.1046/j.1365-2648.2002.02296.x
56. Dingle GA, Brander C, Ballantyne J, Baker FA. ‘To be heard’: the social and mental health benefits of choir singing for disadvantaged adults. Psychol Music. 2013;41:405–421. doi:10.1177/0305735611430081
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Conceptual Model of Home-Based Cardiac Rehabilitation Exercise Adherence in Patients with Chronic Heart Failure: A Constructivist Grounded Theory Study
Yang Z, Sun L, Sun Y, Dong Y, Wang A
Patient Preference and Adherence 2023, 17:851-860
Published Date: 24 March 2023
Adherence to Cardiac Rehabilitation in Patients with Acute Myocardial Infarction After PCI: A Scoping Review
Li P, Zhang W, Wu B
Journal of Multidisciplinary Healthcare 2024, 17:4165-4176
Published Date: 28 August 2024