Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Summary of Best Evidence for the Management and Recurrence Prevention of Febrile Seizures in Children
Authors Tang R ![]() , Wang M, He X, He Q, Chen L, Liu D
, Wang M, He X, He Q, Chen L, Liu D
Received 3 November 2025
Accepted for publication 24 February 2026
Published 4 March 2026 Volume 2026:19 578796
DOI https://doi.org/10.2147/JMDH.S578796
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tilakavati Karupaiah
Rongzhu Tang,1 Min Wang,2 Xue He,1 Qi He,1 Lan Chen,1 Dingxiang Liu1
1Department of Pediatrics, Suining Central Hospital, Suining, Sichuan, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, Suining Central Hospital, Suining, Sichuan, People’s Republic of China
Correspondence: Dingxiang Liu, Department of Pediatrics, Suining Central Hospital, Suining, Sichuan, People’s Republic of China, Tel +86-0825-2292441, Email [email protected]
Objective: This study aims to systematically search, screen, evaluate, and summarize the best evidence related to the prevention and management of febrile seizures in children, with the goal of providing evidence-based guidance for clinical practice in this field.
Methods: A comprehensive search was conducted across multiple databases, including UpToDate, Joanna Briggs Institute (JBI), Guidelines International Network, Agency for Healthcare Research and Quality, Scottish Intercollegiate Guidelines Network, National Institute for Health and Care Excellence, Registered Nurses Association of Ontario, the Cochrane Library, Embase, PubMed, Web of Science, China National Knowledge Internet (CNKI), SinoMed, and WanFang database. The search deadline was from database establishment to July, 2025. Two researchers independently evaluated the quality of the included literature and extracted and summarized the evidence.
Results: Twenty literature sources were included, comprising 3 clinical decision, 7 guidelines, 4 expert consensus, 1 best practice, and 5 systematic reviews. Through integration of these sources, 29 best evidence statements were ultimately developed, covering 6 major themes: Clinical assessment and diagnosis, Indications of hospitalization, risk assessment, non-pharmacological treatment, pharmacological treatment, as well as caregiver support and follow-up.
Conclusion: This study summarizes the best evidence for the prevention and management of febrile seizures in children. In clinical application, healthcare professionals should make professional judgment and select evidence based on clinical circumstances and the preferences of the child, thereby providing a more scientifically grounded basis for clinical nursing practice.
Trial and Protocol Registration: This study was based on the evidence summary reporting specifications of the Fudan University Center for the Evidence-based Nursing, the register name is “Evidence summary for prevention and management of febrile seizures in children”, the registration number is “ES20246803”.
Keywords: children, febrile seizures, evidence-based nursing, prevention, management
Introduction
Febrile seizures (FS) are the most common neurological disorder in children, with a prevalence of 3%–5%, most frequently occurring between 6 months and 5 years of age.1 They are defined as convulsive episodes occurring during fever (axillary temperature ≥38°C or rectal temperature ≥38.5°C), excluding seizures caused by central nervous system infections or other etiologies, and with no prior history of afebrile seizures.2 Based on clinical characteristics, FS are classified as simple febrile seizures (SFS) and complex febrile seizures (CFS).3
While the majority of FS are self-limiting with a favorable prognosis and no neurological sequelae,4 early recurrence during the same febrile illness poses significant challenges for clinicians and families. Statistics indicate that approximately 14% to 24% of children with febrile seizures may experience recurrence within 24 hours.5 If FS recur or progress to status epilepticus, prompt and effective medical intervention is essential. Failure to do so may lead to cerebral hypoxia, causing irreversible neuronal damage and long-term neurological sequelae, which can impair the child’s quality of life.6,7 Studies have shown that most parents have insufficient knowledge of FS and are prone to improper handling in the first aid process, thereby increasing the risk of secondary injury.8 Furthermore, the sudden onset and prominent symptoms of FS cause significant psychological distress to families, often triggering high levels of panic and anxiety.9 This can lead to heightened expectations for hospitalization, potentially increasing the risk of medical disputes.10 Therefore, implementing scientifically sound and effective prevention and management strategies for FS is crucial for improving patient outcomes and the quality of life for affected families.
Currently, the field of prevention and management of childhood fever presents various challenges, including fragmented evidence (eg, caregiver support), partially conflicting conclusions (eg, use of antipyretics, necessity of laboratory testing), lack of clear guidance on key clinical aspects (eg, medication use at different disease stages, absence of long-term follow-up recommendations), and significant variations in international and regional practices. These issues not only reduce consistency in clinical decision-making and adherence to home management but also impact the effectiveness and standardization of diagnostic and therapeutic practices. Therefore, this study aims to systematically synthesize high-quality evidence in this field, clarify existing controversies, and fill gaps in evidence for critical aspects. This will provide evidence-based guidance for clinical practice and home care, with the goal of improving patient outcomes and reducing unnecessary healthcare resource consumption.
Materials and Methods
There is a lack of reporting standards for evidence summarization, but the Evidence-based Nursing Center of Fudan University developed reporting standards according to the Joanna Briggs Institute evidence summary principles.11 This reporting standard involves six areas: problem establishment, literature search, literature screening, literature evaluation, evidence summarization and classification, and forming practice recommendations.
Problem Establishment
The first step in the standard of evidence summary report of Fudan University Evidence-Based Nursing Center is “problem establishment”,12 and this study constructed the following evidence-Based problems according to the PIPOST model: P (target population for evidence application): Children with FS; I (intervention): Interventions for prevention and management of FS in children, including risk assessment, prognostic factors, medication, health education, follow-up, etc; P (professionals applying the evidence): Medical staff in pediatrics; O (outcome): Incidence of febrile convulsions, degree of injury caused by febrile convulsions, social/psychological status, quality of life; S (place of applying the evidence): Medical institutions at all levels, communities, and families; T (type of evidence): clinical decision-making, best practice, guidelines, evidence summaries, expert consensus and systematic review.
Retrieval Strategy
According to the “6s” evidence pyramid model, we searched the following databases from the top down: UpToDate, Joanna Briggs Institute (JBI), Guidelines International Network, Agency for Healthcare Research and Quality, Scottish Intercollegiate Guidelines Network, National Institute for Health and Care Excellence, Registered Nurses Association of Ontario, China Medical Pulse Guide Network, the Cochrane Library, Embase, PubMed, Web of Science, CNKI, SinoMe, WanFang database. We searched using a combination of subject terms + free words, with the search terms being “seizures, febrile/febrile seizures/FS/febrile convulsion*/pyrexial seizure*/pyrexial convulsion*/fever Convulsion*/fever seizure*/seizure, febrile, complex/seizure, febrile, simple” “pediatrics/child/infant/neonatology/pediatric emergency medicine/child*/newborn/neonate/kids/adolescents” “clinical decision-making/guidelines as topic/practice guidelines as topic/guideline [Publication Type]/practice guideline [Publication Type]/evidence-basedpractice/guideline*/consensus/systematic review [Publication Type]/systematic reviews as topic/review [Publication Type]/review literature as topic/systematic review/review/meta-analysis [Publication Type]/meta-analysis as topic/network meta-analysis/meta-analysis/best practices/evidence summary”. The search deadline was from database establishment to July, 2025. An example of the PubMed search strategy is provided in Table 1.
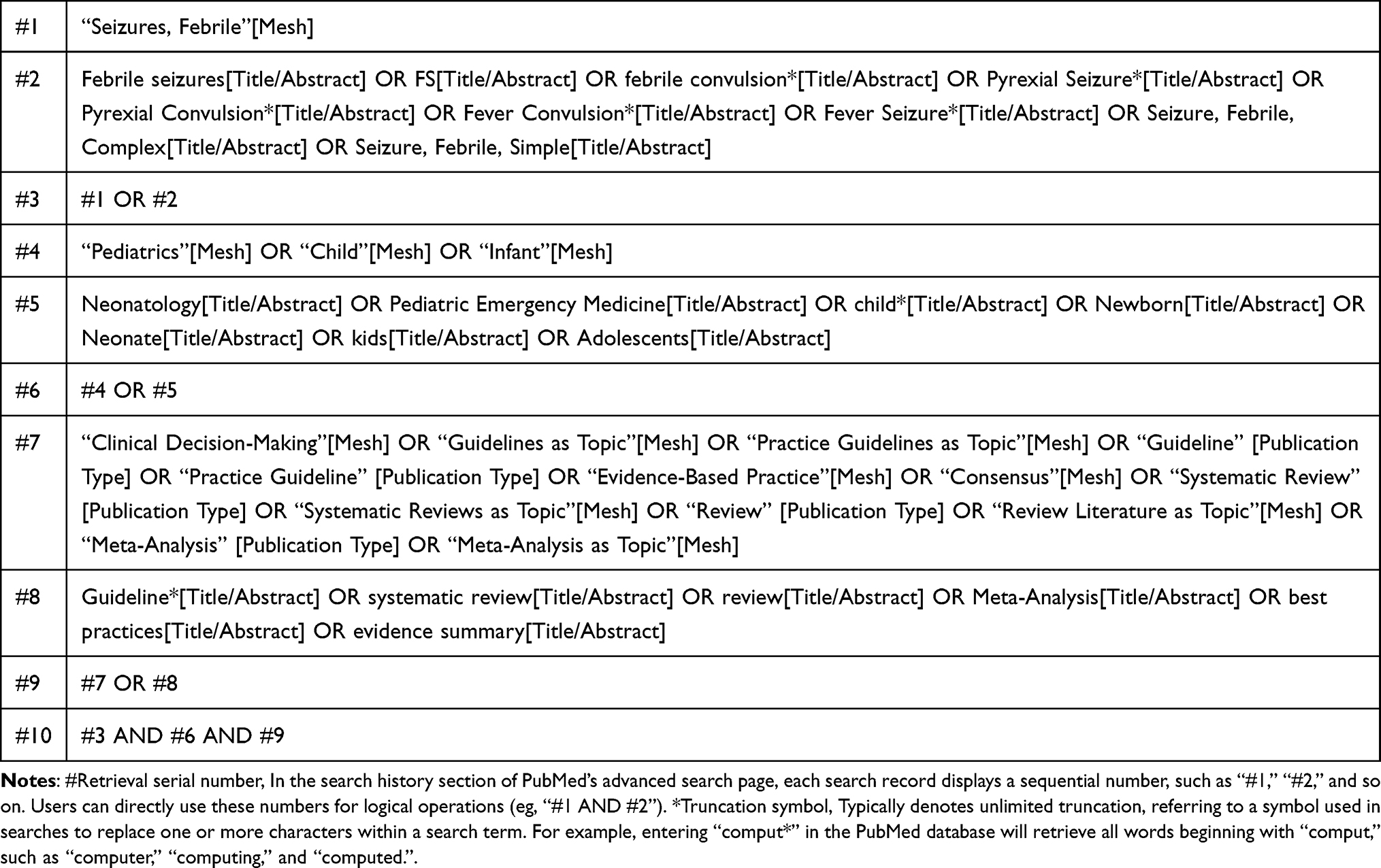 |
Table 1 Literature Search Strategy of PubMed |
Inclusion and Exclusion Criteria of Evidences
Inclusion criteria for this study were (1) study subjects were children with FS; (2) research topics were the prevention and management of interventions for children with FS, including risk assessment, prognostic factors, medication, health education, follow-up, etc; (3) evidences were applied in medical institutions at all levels, communities, and families; (4) literature types were clinical decision-making, best practice, guidelines, evidence summaries, expert consensus and systematic review, etc; (5) The languages of research were English and Chinese literatures.
Exclusion criteria were (1) unable to obtain full-text literature, literature with duplicate publications or incomplete information; (2) original research, translated versions of foreign guidelines, interpretation of guidelines, and drafts; (3) abstracts, conference papers and literature in the research proposal; (4) existing updated versions of literature; (5) papers that did not meet the criteria for quality evaluation.
Quality Evaluation of the Literature
The quality of the guidelines was evaluated using the Appraisal of Guidelines for Research and Evaluation II (AGREE II).13 The quality evaluation of the guidelines was independently conducted by four researchers who had undergone systematic learning of evidence-based methodology. Perform consistency testing on the evaluation results using intra group correlation coefficients. The evaluation criteria consist of 6 fields, 23 items, and 2 guidelines for overall evaluation. Each item is rated at 1–7 points, with 1 point indicating complete non-compliance and 7 points indicating complete compliance. The standardized score for each field is the percentage of the highest possible score in that field, and the higher the score, the higher the quality of the guidelines. Standardized scores in each field = [(actual score evaluated − lowest possible score)/(highest possible score − lowest possible score)] × 100%. The guidelines recommend division of the standardization score into three grades: if 6 items score ≥60%, it is recommended as a grade A; if ≥3 items score ≥30% with some items with scores <60%, it is recommended as a grade B after modification and improvement; and ≥3 areas with scores <30% are excluded as grade C.
The systematic review was evaluated using the systematic review tool by the Australian JBI Centre for Evidence-Based Health Care,14 which consists of 11 evaluation items, each of which contains four options, “Yes”, “No”, “Unclear”, and “Not Applicable”. The expert consensus and best practice were evaluated using the Expert Consensus Evaluation Tool by the JBI Centre for Evidence-Based Health Care in Australia,14 with six evaluation items, each with four options, “Yes”, “No”, “Unclear”, and “Not Applicable”.
UpToDate from authoritative databases was directly considered high-quality evidence. The quality evaluation of the guidelines was completed independently by four researchers, and the quality evaluation of the remaining literature was completed independently by two researchers. When there were different opinions, the third researcher was asked to assist in the evaluation. The intra-group correlation coefficient (ICC) was used to determine the inter-rater consistency. When evidence conclusions conflicted, the highest quality and recently published evidence from authoritative journals was selected.
Method for Forming Evidence Level and Recommendation Level
The JBI Evidence Pre Grading and Evidence Recommendation Level System (2014 Edition)15 was used to classify the level of evidence. According to the different types of research designs, the level of evidence was divided into levels 1a to 5c. The more rigorous the research design was, the higher the level of evidence was, with level 1a being the highest and decreasing in sequence. The guide traced the evidence level of the original literature it referred to. Based on the FAME structure of evidence, which includes its feasibility, suitability, clinical significance and effectiveness,15 recommendation levels were divided into A-level recommendation (strong recommendation) and B-level recommendation (weak recommendation).
Results
Literature Search Results
This study retrieved 7163 articles, of which 7161 were obtained through systematic search, and 2 was obtained through retrospective reference. After import to EndNote 20 and removal of duplicates, 4280 articles remained. After initial screening, 111 articles were selected for full-text review, and 20 articles were ultimately included: 3 clinical decision,4,16,17 7 guidelines,2,18–23 4 expert consensus,24–27 1 best practice,28 and 5 systematic reviews.29–33 The literature screening process is illustrated in Figure 1, and the general characteristics of the included literature are presented in Table 2.
 |
Table 2 Characteristic of Included Literature (n = 20) |
 |
Figure 1 Flowchart of Literature Screening. Abbreviations: JBI, Joanna Briggs Institute; GIN, Guidelines International Network; AHRQ, Agency for Healthcare Research and Quality; SIGN, Scottish Intercollegiate Guidelines Network; NICE, National Institute for Health and Care Excellence; RNAO, Registered Nurses Association of Ontario; CNKI, China National Knowledge Internet. |
Quality Evaluation of Included Literature
Quality Evaluation of Clinical Decision-Making Outcomes
Clinical decisions were directly incorporated as high-quality evidence from authoritative databases.
Quality Evaluation Results of Guidelines
The quality assessment results for the guidelines are presented in Table 3. The ICC of the four researchers for quality assessment ranged from 0.911 to 0.991, indicating a high level of consistency.
 |
Table 3 Quality Evaluation Results of Guidelines (n = 7) |
Quality Evaluation Results of Expert Consensus and Best Practice
The quality assessment results for expert consensus and best practice are presented in Table 4
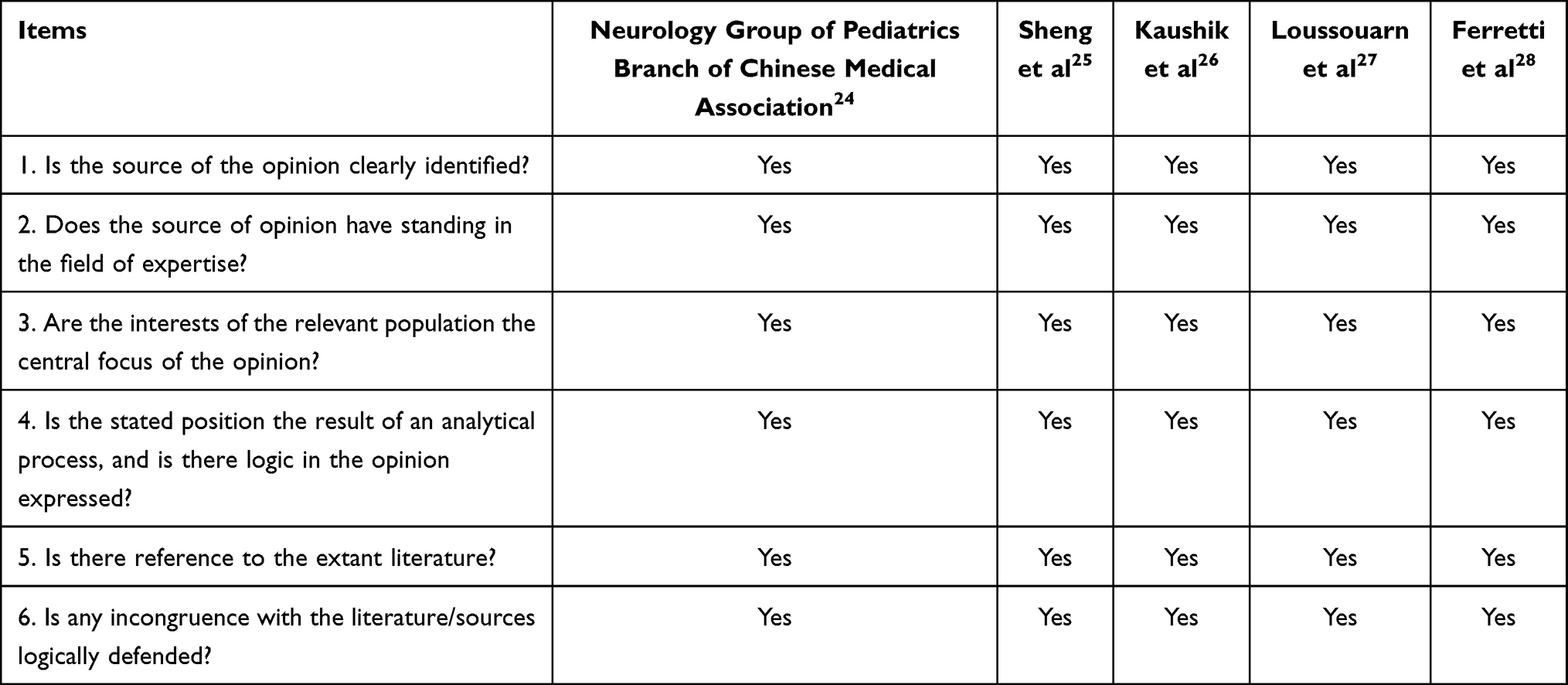 |
Table 4 Quality Evaluation Results of Expert Consensus and Best Practice (n = 5) |
Quality Evaluation Results of Systematic Reviews
The quality assessment results for the systematic reviews are presented in Table 5
 |
Table 5 Quality Evaluation Results of Systematic Reviews (n = 5) |
Evidence Synthesis
This study provides a comprehensive overview of the evidence for the prevention and management of children with FS. It encompasses clinical assessment and diagnosis, indications of hospitalization, risk assessment, non-pharmacological treatment, pharmacological treatment, as well as caregiver support and follow-up. In total, 29 pieces of evidence are presented in Table 6
 |
Table 6 Evidence Summary for the Prevention and Management of Children with Febrile Seizures |
Discussion
Comprehensive Clinical Evaluation and Diagnosis are the Basis for the Management of FS
Febrile seizures (FS) are clinically classified as a diagnosis of exclusion, requiring differentiation from other conditions that can cause seizures, such as central nervous system infections, epilepsy, toxic encephalopathy, metabolic disorders, acute poisoning, and inherited metabolic diseases.24 Failure to conduct a comprehensive and systematic clinical evaluation and differential diagnosis may lead to misdiagnosis or missed diagnosis, delaying treatment and potentially endangering the child’s life.34 When collecting the medical history of children with FS, the following details should be clarified: the specific manifestations of the seizure, its duration, the presence of focal features (such as convulsions in one limb or a localized area of the body), relevant medication history, personal or family history of seizures, and whether there are any neurological abnormalities or developmental delays.17,19,20,28 Whenever possible, interview witnesses to obtain detailed information. However, witnesses are often in a state of tension or fear during the seizure and may struggle to accurately describe details. The information they provide may be biased, necessitating careful assessment of its reliability. During general physical and neurological examinations of children with FS, focus should be placed on assessing vital signs, level of consciousness, presence of meningeal irritation signs, tension or bulging of the fontanelle, and any focal abnormalities in muscle tone, muscle strength, or voluntary movement.17,19,28 If any of the above positive findings are detected during examination, be highly vigilant for the possibility of other underlying causes, such as central nervous system infection or severe systemic infection.
To avoid overtreatment and reduce the financial burden on families, pediatricians should strictly adhere to the indications for ancillary tests. For children with typical SFS who are in generally good condition and show no focal neurological signs, routine diagnostic tests are generally unnecessary.17,34 Complete blood count, serum electrolytes, blood glucose, serum calcium, and blood urea nitrogen tests are recommended only when specific clinical indications exist, such as a history of vomiting, diarrhea, or abnormal fluid intake, or when physical examination reveals signs of dehydration or edema.2,17,19,20,22–24,26 Lumbar puncture is also an unconventional test but should be considered or recommended in the following situations: when the child exhibits meningeal irritation signs or other clinical manifestations suggestive of central nervous system infection; when the child is aged 6–12 months and has not received scheduled influenza or pneumococcal vaccinations, or has an unclear vaccination history; when the child has already received antibiotic treatment, as the medication may mask typical symptoms of meningitis or encephalitis. If lumbar puncture is performed, concurrent blood cultures and blood glucose testing are recommended to aid differential diagnosis and comprehensive assessment of the patient’s condition.2,17,19–24,26,28
Electroencephalography (EEG) is not a routine test for children with FS.17 However, when seizures persist for an extended duration or exhibit focal characteristics, EEG monitoring and close neurological follow-up are warranted due to the elevated risk of subsequent epilepsy.2,4,17,19–24,26,28 While there is no established consensus on the optimal timing for EEG testing, research suggests that performing the test within 72 hours after febrile status epilepticus may hold value for prognostic assessment.35 In neuroimaging, children with simple FS do not require CT or MRI scans. However, if a child exhibits abnormal head circumference, abnormal neurological examination findings, focal neurological signs, or increased intracranial pressure, an urgent contrast-enhanced CT or MRI scan is necessary to rule out structural lesions.2,17,19,20,22–24,26 Genetic testing is generally not recommended for most children with FS, even in the presence of a positive family history.17 However, in specific clinical situations, such as when children aged 12 to 18 months experiences recurrent prolonged focal FS accompanied by other seizure types, genetic testing is recommended to aid diagnosis when considering hereditary epilepsies such as Dravet syndrome.36 Currently, there is no unified standardized process for the clinical assessment and diagnosis of FS. Future efforts should focus on promoting multidisciplinary collaboration to comprehensively enhance diagnostic and treatment capabilities.
Clear Hospitalization Criteria and Comprehensive Risk Assessment are the Primary Steps in Managing FS
Establishing clear indications for hospitalization is crucial for achieving precision medicine and optimizing healthcare resource allocation. For children experiencing their first febrile seizure, the core purpose of inpatient observation is to rule out or promptly treat acute infections potentially affecting the central nervous system, while closely monitoring clinical changes to identify early risks of seizure recurrence or secondary epilepsy. A Glasgow Coma Scale score less than 15 more than an hour after the seizure indicates neurological abnormalities, warranting hospitalization to determine the cause.28 Children experiencing their first seizure before 18 months of age, especially those who have received empirical antibiotic treatment, present with atypical clinical manifestations and a relatively higher risk of intracranial infection, thus requiring hospitalization.19–24,28 Hospitalization is also recommended when the infectious cause of FS is unclear or the infection is severe.19–24,28 Studies by Kavanagh et al indicate that 25% of children with prolonged FS ≥30 min and 67% of children requiring ≥2 intravenous anticonvulsants to stop seizures subsequently developed viral encephalitis.37 For children with CFS or febrile status epilepticus, hospital admission is recommended for the management of potential CNS infections.19–24,28 For children without a clear family history of FS, hospitalization for observation is recommended to determine the cause.24 When caregivers exhibit severe anxiety or are assessed as unlikely to manage recurrent seizures effectively, hospitalization for observation is recommended to provide education and support.19 The majority of children can be safely discharged after a period of observation if they have returned to their neurological baseline.
Identifying risk factors for recurrent FS and secondary epilepsy facilitates proactive monitoring of high-risk children, promotes early recognition and intervention for FS, and thereby improves long-term prognosis.38 Simultaneously, accurate risk assessment provides families with clear information about FS recurrence and secondary epilepsy risks, alleviating anxiety and panic stemming from uncertainty and fostering rational coping strategies.39 A retrospective observational study indicates that seizure duration, number of recurrent seizures, family history, body temperature, time from fever onset to seizure, time from seizure onset to arrival at the emergency department, hyponatraemia, osmotic pressure and low haemoglobin level, are risk factors for recurrent FS.40 Additionally, a meta-analysis indicates that iron deficiency anemia is also a risk factor for recurrent FS.31 Iron metabolism status is closely linked to children’s nutrition, neurodevelopment, and immune function.41 Iron deficiency can lower the seizure threshold and increase the risk of brain damage.31 Notably, the recurrence rate of FS is high within the first 8 hours of onset (approximately 82–86%), while it significantly decreases to 4.2% after 8 hours following the initial episode.37 Therefore, for children with high-risk factors for recurrence, it is recommended to conduct an 8-hour observation and anticipatory management in the hospital setting. This allows for timely intervention and completion of relevant examinations, thereby avoiding repeated hospital visits due to subsequent seizures.
FS may cause long-term enhancement of hippocampal neuronal excitability, subsequently inducing hippocampal sclerosis, damage, and atrophy, ultimately increasing the risk of epileptic seizures.33 Research indicates that preterm birth, history of perinatal asphyxia, age at the first seizure <12 months, peak temperature <39°C, onset of fever to seizure <1h, CFS, duration of the seizure >15 min, Multiple seizures (≥2/episode) in one attack, focal seizures, recurrent FS (≥2), neurodevelopmental abnormality, developmental delay, family history of epilepsy, family history of FS, electroencephalogram abnormal, Brain imaging abnormalities are risk factors for FS to develop into epilepsy.16,18,24,28,33 During infancy and early childhood, the brain and cortical structures are not yet fully developed.42 Minor injuries such as asphyxia or intracranial inflammation are more likely to cause neuronal damage and developmental disorders.42 Secondly, CFS tend to occur multiple times and last for a long time, and metabolism, oxygen consumption, and blood flow of nerve cells change during the seizure, resulting in central nervous system lesions and secondary epilepsy.43 At the same time, Children with a family history of epilepsy exhibit a significantly elevated risk of developing epilepsy later in life. This suggests that genetic susceptibility and associated gene mutations may trigger abnormal activity in specific brain regions following FS, ultimately leading to epilepsy.44 Therefore, early identification of risk factors for seizure recurrence or secondary epilepsy in children with FS, development of effective prevention and management strategies targeting modifiable risk factors, and implementation of continuous long-term follow-up for high-risk children hold significant clinical importance.
Prioritize Non-Pharmacological Treatment of FS to Ensure Patient Safety
FS are common acute neurological disorders in infants and young children. Most episodes are transient and self-limiting, lasting 1 to 3 minutes and generally not requiring immediate drug intervention. During an episode, healthcare providers should promptly perform ABC (Airway, Breathing, Circulation) assessment and support.16,22–24,28 Maintaining airway patency is the primary measure, requiring timely clearance of oral and nasal secretions to prevent asphyxia or aspiration pneumonia.24 If the child SpO2 <90% or signs of inadequate ventilation, oxygen therapy should be administered promptly to mitigate cerebral hypoxia.22–24 Regarding nutritional support, children with FS generally do not require routine supplementation of micronutrients such as iron, zinc, or vitamin D.26,29 However, recent studies suggest certain nutritional statuses may be associated with seizure risk.31 Therefore, targeted supplementation under medical supervision is recommended only when specific nutrient deficiencies are confirmed through clinical assessment or laboratory testing, or when the child belongs to a high-risk group. It is important to emphasize that breastfeeding has been confirmed by multiple studies as a protective factor against FS.30 Prospective cohort studies indicate that infants receiving mixed feeding or exclusive breastfeeding exhibit a significantly reduced risk of FS before 2.5 years of age compared to those exclusively formula-fed.45 The protective mechanism may be related to the immune-active components and neuroprotective factors present in breast milk.30,45 Therefore, breastfeeding is recommended during infancy and early childhood to mitigate this risk.
Pharmacological Treatment is the Core Means to Reduce the Risk of Recurrence in High-Risk Patients
Pharmacological management should follow a tiered approach, with medication selection based on seizure duration, availability of intravenous access, and the child’s individual characteristics. When FS lasts longer than 5 minutes, immediate drug intervention is required to prevent brain damage or progression to status epilepticus.29 Intravenous diazepam is the drug of choice, with a recommended dose of 0.3–0.5 mg/kg (maximum single dose ≤ 10 mg).16,19,20,22–24,28,29 The infusion rate must be strictly controlled at 1–2 mg/min.24 If the seizure ceases during administration, injection should be stopped immediately.16,19,20,22–24,28,29 Note that excessive infusion rates may cause adverse reactions such as respiratory depression, bradycardia, and hypotension.24 If intravenous access cannot be established, alternative options include intramuscular injection of midazolam at 0.3 mg/kg (≤10 mg per dose), rectal administration of diazepam, or enema with 10% chloral hydrate solution at 0.5 mL/kg, all of which can achieve anticonvulsant effects.19,20,22–24,28,29 If seizures persist 5 minutes after the initial diazepam dose or recur shortly after control, repeat administration is permissible.16,24,28 If seizures persist for over 30 minutes, they progress to status epilepticus.24 It is recommended to administer 15 mg/kg of valproic acid intravenously over at least 5 minutes, followed by a maintenance infusion at a rate of 1–2 mg/kg/h.22,24,29 However, valproate carries a risk of hepatotoxicity and should be used with caution in children under 2 years of age.46 Liver function should be assessed and potential metabolic disorders ruled out prior to administration. For children experiencing frequent seizures within a short period (≥3 episodes within 6 months or ≥4 episodes within 1 year) or those with FS with complications, intermittent prophylactic treatment may be considered.24 Administering diazepam 0.3 mg/kg orally at the onset of fever, repeated every 8 hours and not exceeding 3 doses within 24 hours, can effectively reduce the risk of seizure recurrence.18–20,24,29 Additionally, levetiracetam, as a newer antiepileptic drug, has been shown in studies to prevent recurrence when used intermittently (15–30 mg/kg/day, divided into two oral doses) with fewer adverse reactions.24,29
For long-term prophylactic treatment, the prognosis for SFS is favorable, with a risk of secondary epilepsy ranging from 1% to 1.5%.22 The risk of adverse reactions from long-term antiepileptic drug therapy may outweigh its potential benefits.29 Therefore, long-term antiepileptic drug therapy is not recommended for children with SFS.16–19,23,24,26,29 For CFS, particularly in children experiencing status epilepticus or possessing other high-risk factors for secondary epilepsy, long-term antiepileptic therapy may be considered.24,28,29 However, thorough communication with the child’s guardians is essential prior to initiating medication, along with a comprehensive assessment of its efficacy versus potential risks.29 Regarding antipyretic medications, it is crucial to recognize their limited scope of action. Antipyretics such as ibuprofen and acetaminophen effectively reduce fever, improve patient comfort, and alleviate parental anxiety.32 However, current evidence indicates that antipyretics do not effectively prevent the initial occurrence of FS or reduce their recurrence risk.4,16,18–22,24,26,28,29,32 Therefore, routine or preemptive use of antipyretics for the purpose of preventing FS is not recommended.
Regarding vaccination, FS are not generally considered a contraindication for vaccination.25 Certain vaccines, such as the trivalent inactivated influenza vaccine, pneumococcal vaccine, DTaP vaccine, and MMR vaccine, may induce fever reactions post-vaccination, potentially triggering FS.17,25 Analysis indicates that this is primarily associated with underlying genetic abnormalities in children, rather than the immunization causes epilepsy.47 Research has confirmed that vaccine-induced FS show no significant differences in seizure frequency, severity, recurrence risk, or long-term prognosis compared to FS triggered by other febrile illnesses.48 They also do not increase the risk of neurological sequelae or developmental disorders.48 As children with epilepsy are at a higher risk of complications from vaccine-preventable diseases, vaccination in children with epilepsy should be optimized, especially early in life, as these children may not be able to rely on herd protection.49 Therefore, for children with SFS or infrequent episodes (<3 episodes within 6 months and <4 episodes within 1 year) and no history of status epilepticus, all vaccines may be administered according to the immunization schedule after recovery from the current febrile illness, with one dose recommended per vaccination.17,20,21,25 However, for children with CFS or frequent seizures within a short period (≥3 episodes within 6 months or ≥4 episodes within 1 year), vaccination should be deferred and the child referred to a specialist clinic for further evaluation.21,25 Additionally, routine use of antipyretics before or after vaccination for prophylactic purposes is not recommended, as it may interfere with the body’s immune response to vaccine antigens.28
Caregiver Support and Follow-Up is the Fundamental Guarantee for Effective Family Care
Although FS typically follow a benign clinical course, their first occurrence often represents a profoundly traumatic event for parents.28 Research indicates that when a child experiences their first febrile seizure, only 46% of mothers correctly identify it as a seizure, while a significant 39% believe their child is near death.50 This widespread lack of awareness coupled with heightened anxiety may lead parents to take inappropriate actions during seizures, such as stimulating the child or rushing them to the hospital while neglecting on-site management, thereby increasing the risk of secondary injury.8 To effectively address this challenge, healthcare providers should enhance education for parents or caregivers.16,39 First, emphasize the benign prognosis of FS, the recurrence risk, and the low probability of future epilepsy development.4,21,23,24,26,27 This alleviates caregivers’ anxiety and panic, helping them respond rationally. Secondly, it is essential to clearly instruct parents on the correct management of acute seizures. Parents should remain calm, place the child in a supine position with the head turned to one side or in a lateral recumbent position, and promptly clear secretions from the mouth and nose to prevent choking.4,21,23,24,27 Harmful actions such as pinching the philtrum, prying open the jaw, pressing down on the child, or shaking them must be strictly prohibited.4,21,23,24,27 More importantly, healthcare providers should teach parents or caregivers to accurately record the type and duration of FS, and clearly identify indications requiring emergency medical attention (eg, seizures lasting >5 minutes or delayed recovery of consciousness).16,21,23,24 For high-risk children with a history of recurrent or prolonged seizures, consider training parents to administer at-home interventions such as diazepam rectal gel (0.5 mg/kg), midazolam nasal spray, or buccal mucosal solution for early intervention.4,16,19,21,22,26,27 Additionally, healthcare providers should recognize that the first occurrence of FS may constitute psychological trauma for parents.28 It is recommended to offer professional psychological counseling support within 2–3 weeks after the event to prevent the development of acute stress disorder or post-traumatic stress disorder.28 Finally, for children with CFS, it is advisable for specialists to conduct long-term follow-up, dynamically monitor their neurological development, and assess the long-term risk of epilepsy.17,20,24
Limitations
This study comprehensively summarizes the evidence for the prevention and management of FS recurrence in children, but there are also certain limitations. First, differences in geographic regions, ethnicities, and cultural backgrounds may affect the applicability of the study conclusions. Second, to maintain the integrity of the evidence and address gaps in the field, this review included some classic guidelines published over five years ago. These documents may carry risks of relatively outdated methodologies or obsolete conclusions. Furthermore, the literature search was limited to Chinese and English databases, failing to include studies in other languages, which may introduce language bias. Future research should continuously update evidence in this field while comprehensively evaluating the feasibility, applicability, effectiveness, and integration with clinical practice of such evidence. This approach will facilitate the translation of evidence into practice, ultimately enhancing healthcare quality.
Conclusion
Through a systematic scientific evidence-based approach, this study summarized 29 pieces of best evidence in 6 dimensions, including clinical assessment and diagnosis, indications of hospitalization, risk assessment, non-pharmacological treatment, pharmacological treatment, as well as caregiver support and follow-up, providing a reference for medical personnel in the prevention and management of FS in children. This evidence supports the development of standardized, tiered clinical management pathways to improve patient outcomes and enhance overall quality of care. By clarifying diagnostic criteria and hospitalization indications, high-risk children can be accurately identified, avoiding overtreatment of low-risk cases. Implementing individualized acute-phase management and prevention strategies based on risk stratification helps reduce febrile seizure recurrence rates. Concurrently, systematic caregiver education and follow-up support enhance family coping abilities, alleviate caregiving anxiety, and ensure continuous monitoring of children’s neurodevelopment. Ultimately, this evidence-based practice model will optimize the allocation of healthcare resources and reduce the risk of complications, thereby improving the physical and mental health outcomes and quality of life for pediatric patients and their families. It should be noted that since evidence originates from different countries, the actual circumstances of the local region should be thoroughly evaluated prior to clinical application. Reasonable adjustments should be made based on departmental conditions, patient preferences, and consent.
Date Sharing Statement
Data is available on request from the corresponding author.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hauser WA. The prevalence and incidence of convulsive disorders in children. Epilepsia. 1994;35(2):S1–19. doi:10.1111/j.1528-1157.1994.tb05932.x
2. Subcommittee on Febrile Seizures; American Academy of Pediatrics. Neurodiagnostic evaluation of the child with a simple febrile seizure. Pediatrics. 2011;127(2):389–394. doi:10.1542/peds.2010-3318
3. Biltz S, Speltz L. Febrile Seizures. Pediatr Ann. 2023;52(10):e388–e393. doi:10.3928/19382359-20230829-03
4. Millichap JJ. Treatment and prognosis of febrileseizures. Available from: https://www.uptodate.cn/contents/zh-Hans/treatment-and-prognosis-of-febrile-seizures.
5. Jiang W, Cheng A, Wang J, et al. Early recurrence of febrile seizures during acute illness: risk factors and lack of association with long-term epilepsy in a pediatric cohort. Front Neurol. 2026;16:1733941. doi:10.3389/fneur.2025.1733941
6. Jongruk P, Wiwattanadittakul N, Katanyuwong K, et al. Risk factors of epilepsy in children with complex febrile seizures: a retrospective cohort study. Pediatr Int. 2022;64(1):e14926. doi:10.1111/ped.14926
7. Marangoni MB, Corsello A, Cozzi L, et al. The non-clinical burden of febrile seizures: a systematic review. Front Pediatr. 2024;12:1377939. doi:10.3389/fped.2024.1377939
8. Rice SA, Müller RM, Jeschke S, et al. Febrile seizures: perceptions and knowledge of parents of affected and unaffected children. Eur J Pediatr. 2022;181(4):1487–1495. doi:10.1007/s00431-021-04335-1
9. Othman A, Razak SA, Nasir A, et al. Depressive, anxiety, and stress symptoms in parents of children being admitted for febrile seizures in a tertiary hospital in the east coast of Malaysia. Eur J Investig Health Psychol Educ. 2023;13(6):1015–1025. doi:10.3390/ejihpe13060077
10. Hakizimana O, Kalimba E, Arnold L, et al. The assessment of parents’ knowledge, attitudes and concerns about febrile seizures in children at tertiary hospitals in Rwanda-a descriptive study. J Trop Pediatr. 2021;67(1):fmab003. doi:10.1093/tropej/fmab003
11. Munn Z, Lockwood C, Moola S. The development and use of evidence summaries for point of care information systems: a streamlined rapid review approach. Worldviews Evid Based Nurs. 2015;12(3):131–138. doi:10.1111/wvn.12094
12. Zhu Z, Hu Y, Xing W, et al. Composition of the different types of evidence-based problems. J Nurs Train. 2017;32(21):1991–1994. doi:10.16821/j.cnki.hsjx.2017.21.025
13. Brouwers MC, Kho ME, Browman GP, et al. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010;182(18):E839–E842. doi:10.1503/cmaj.090449
14. Aromataris E, Lockwood C, Porritt K, et al. JBI manual for evidence synthesis. JBI; 2024. Available from: https://synthesismanual.jbi.global.
15. Wang C, Hu Y. JBI evidence pre-classification and evidence recommendation level system (2014 edition). J Nurs Train. 2015;30(11):964–967. doi:10.16821/j.cnki.hsjx
16. Millichap JJ. Patient education: febrile seizures. Available from: https://www.uptodate.cn/contents/febrile-seizures-beyond-the-basics.
17. Millichap JJ. Clinical features and evaluation of febrile seizures. Available from: https://www.uptodate.com/contents/clinical-features-and-evaluation-of-febrile-seizures.
18. Steering Committee on Quality Improvement and Management, Subcommittee on Febrile Seizures American Academy of Pediatrics. Febrile seizures: clinical practice guideline for the long-term management of the child with simple febrile seizures. Pediatrics. 2008;121(6):1281–1286. doi:10.1542/peds.2008-0939
19. British Columbia Medical Services Commission Guidelines and Protocols Advisory Committee. Febrile seizures. British Columbia Medl Assoc. 2010;41(1):215–222.
20. Natsume J, Hamano SI, Iyoda K, et al. New guidelines for management of febrile seizures in Japan. Brain Dev. 2017;39(1):2–9. doi:10.1016/j.braindev.2016.06.003
21. Guidelines for the Management of Convulsions with Fever. Joint working group of the research unit of the Royal College of Physicians and the British Paediatric Association. BMJ. 1991;303(6803):634–636. doi:10.1136/bmj.303.6803.634
22. Capovilla G, Mastrangelo M, Romeo A, et al. Recommendations for the management of “febrile seizures”: ad Hoc Task Force of LICE guidelines commission. Epilepsia. 2009;50(1):2–6. doi:10.1111/j.1528-1167.2008.01963.x
23. Aguirre-Velázquez CG, Huerta Hurtado AM, Ceja-Moreno H, et al. Clinical guideline: febrile seizures, diagnosis, and treatment. Revista Mexicana de Neurociencia. 2019;20(2):97–103. doi:10.24875/rmn.m19000029
24. Neurology Group of Pediatrics Branch of Chinese Medical Association. Expert consensus on the diagnosis, treatment and management of febrile seizures (2017 edition). Chin J Appl Clin Pediatr. 2017;32(18):1379–1382. doi:10.3760/cma.j.issn.2095-428X.2017.18.005
25. Sheng Y. Expert consensus on vaccination for children with special health status ——febrile seizures and vaccination. Chin J Pract Pediat. 2019;34(02):81–82. doi:10.19538/j.ek2019020601
26. Kaushik JS, Sondhi V, Yoganathan S, et al. Association of Child Neurology (AOCN) consensus statement on the diagnosis and management of febrile seizures. Indian Pediatr. 2022;59(4):300–306. doi:10.1007/s13312-022-2497-2
27. Loussouarn A, Devlin A, Bast T, et al. Consensus statements on the information to deliver after a febrile seizure. Eur J Pediatr. 2021;180(9):2993–2999. doi:10.1007/s00431-021-04067-2
28. Ferretti A, Riva A, Fabrizio A, et al. Best practices for the management of febrile seizures in children. Ital J Pediatr. 2024;50(1):95. doi:10.1186/s13052-024-01666-1
29. Offringa M, Newton R, Nevitt SJ, et al. Prophylactic drug management for febrile seizures in children. Cochrane Database Syst Rev. 2021;6(6):CD003031. doi:10.1002/14651858.CD003031
30. Muniz MCR, Lima RV, Maia VQCC, et al. The protective effect of breast feeding on febrile seizures: a systematic review with meta-analysis. Eur J Pediatr. 2024;183(5):2049–2058. doi:10.1007/s00431-024-05501-x
31. Sulviani R, Kamarullah W, Dermawan S, et al. Anemia and poor iron indices are associated with susceptibility to febrile seizures in children: a systematic review and meta-analysis. J Child Neurol. 2023;38(3–4):186–197. doi:10.1177/08830738231170333
32. Hashimoto R, Suto M, Tsuji M, et al. Use of antipyretics for preventing febrile seizure recurrence in children: a systematic review and meta-analysis. Eur J Pediatr. 2021;180(4):987–997. doi:10.1007/s00431-020-03845-8
33. Zhang J, Jing Q, Li S, et al. Risk factors for secondary epilepsy following febrile seizures in children: a meta-analysis. Epilepsy Behav. 2024;161:110051. doi:10.1016/j.yebeh.2024.110051
34. Corsello A, Marangoni MB, Macchi M, et al. Febrile seizures: a systematic review of different guidelines. Pediatr Neurol. 2024;155:141–148. doi:10.1016/j.pediatrneurol.2024.03.024
35. Shah PB, James S, Elayaraja S. EEG for children with complex febrile seizures. Cochrane Database Syst Rev. 2020;4(4):CD009196. doi:10.1002/14651858.CD009196.pub5
36. Wirrell EC, Hood V, Knupp KG, et al. International consensus on diagnosis and management of Dravet syndrome. Epilepsia. 2022;63(7):1761–1777. doi:10.1111/epi.17274
37. Kajiwara K, Koga H. Risk factors for acute encephalitis and early seizure recurrence in complex febrile seizures. Eur J Pediatr. 2022;181(8):3103–3110. doi:10.1007/s00431-022-04529-1
38. Leung JS. Febrile seizures: an updated narrative review for pediatric ambulatory care providers. Curr Pediatr Rev. 2024;20(1):43–58. doi:10.2174/1573396318666220829121946
39. Eiseman M. Febrile seizures: a clinical review and focus on caregiver education. JAAPA. 2024;37(9):37–41. doi:10.1097/01.JAA.0000000000000052
40. Yücel G, Arslan AK, Özgör B, et al. Prediction of recurrent febrile seizures risk during the same febrile illness in children at a single tertiary centre in Turkiye. BMJ Paediatr Open. 2025;9(1):e002908. doi:10.1136/bmjpo-2024-002908
41. Chaber R, Helwich E, Lauterbach R, et al. Diagnosis and treatment of iron deficiency and iron deficiency anemia in children and adolescents: recommendations of the polish pediatric society, the polish society of pediatric oncology and hematology, the polish society of neonatology, and the polish society of family medicine. Nutrients. 2024;16(21):3623. doi:10.3390/nu16213623
42. Dimitrova R, Pietsch M, Ciarrusta J, et al. Preterm birth alters the development of cortical microstructure and morphology at term-equivalent age. Neuroimage. 2021;243:118488. doi:10.1016/j.neuroimage.2021.118488
43. Duan M, Liao Y, Guo H, et al. Risk factors for secondary epilepsy in children with complex febrile seizures and their effect on growth and development-a retrospective cohort study. Transl Pediatr. 2023;12(5):918–926. doi:10.21037/tp-23-203
44. Ghiasian M, Daneshyar S, Khanlarzadeh E, et al. Investigating the relationship of positive family history pattern and the incidence and prognosis of idiopathic epilepsy in epilepsy patients. Caspian J Intern Med. 2020;11(2):219–222. doi:10.22088/cjim.11.2.219
45. Na JY, Cha JH, Moon JH, et al. Protective effect of breastfeeding against febrile seizure: a nationwide study in Korea. Pediatr Neurol. 2023;138:52–57. doi:10.1016/j.pediatrneurol.2022.10.005
46. Kadam R, Palkar M, Pingili RB. Mechanisms involved in the valproic acid-induced hepatotoxicity: a comprehensive review. Toxicol Mech Methods. 2025;35(6):565–580. doi:10.1080/15376516.2025.2459176
47. Scott RC, Moshé SL, Holmes GL. Do vaccines cause epilepsy? Review of cases in the national vaccine injury compensation program. Epilepsia. 2024;65(2):293–321. doi:10.1111/epi.17794
48. Deng L, Wood N, Macartney K, et al. Developmental outcomes following vaccine-proximate febrile seizures in children. Neurology. 2020;95(3):e226–e238. doi:10.1212/WNL.0000000000009876
49. Righolt CH, Pabla G, Donelle J, et al. Vaccine coverage among children with epilepsy in two Canadian provinces: a Canadian immunization research network study. Vaccine. 2021;39(15):2117–2123. doi:10.1016/j.vaccine.2021.03.009
50. Kolahi AA, Tahmooreszadeh S. First febrile convulsions: inquiry about the knowledge, attitudes and concerns of the patients’ mothers. Eur J Pediatr. 2009;168(2):167–171. doi:10.1007/s00431-008-0724-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Short-Term Management Outcomes of Supracondylar Fractures of the Humerus and Their Associated Factors in Children Managed at Mulago National Referral Hospital
Sheikdon AA, Mulepo P, Waiswa G, Bugeza S, Sereke SG, Mfaume B, Patrick S, Jada SA, Emusugut M
Orthopedic Research and Reviews 2022, 14:235-245
Published Date: 15 July 2022
Demographic, Clinical Profile and Management Outcomes of Ocular Chemical Injuries in Saudi Children

Al-Ghadeer H, Al Amry M, Aldihan KA, Alobaidan OS, AlQahtani GMS, Khandekar R
Clinical Ophthalmology 2022, 16:3247-3255
Published Date: 1 October 2022
Incidence, Pathophysiology, Complications, and Management of Positive Vitreous Pressure During Penetrating Keratoplasty: A Literature Review
Alkharashi M, AlAbdulhadi HA, Otaif W, Alahmadi AS, Alanazi B, Al Habash A, Aldayel A, Aljindan M, Almulhim A, Bin Helayel H
Clinical Ophthalmology 2023, 17:583-590
Published Date: 14 February 2023
Analysis of the Current Status of Nurses’ Knowledge of Pressure Injuries and Factors Influencing It in Shaanxi Province, China: A Cross-Sectional Study
Luo L, Wen X, Wang J, Xiao Q, Su L, Zhou M
Risk Management and Healthcare Policy 2024, 17:1451-1462
Published Date: 31 May 2024
Evidence Based Strategies for Preventing Falls in Community-Dwelling Older Adults
An X, Pan Y, He C, Liang Y
Journal of Multidisciplinary Healthcare 2025, 18:4033-4044
Published Date: 16 July 2025