Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Suicidal Ideation and Its Associated Factors Among Patients with Major Depressive Disorder at Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia
Authors Basha EA ![]() , Mengistu BT, Engidaw NA, Wubetu AD
, Mengistu BT, Engidaw NA, Wubetu AD ![]() , Haile AB
, Haile AB ![]()
Received 17 March 2021
Accepted for publication 4 May 2021
Published 21 May 2021 Volume 2021:17 Pages 1571—1577
DOI https://doi.org/10.2147/NDT.S311514
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Elyas Adamsu Basha,1 Bethelehem Taye Mengistu,1 Nigus Alemnew Engidaw,1 Abate Dargie Wubetu,1 Assalif Beyene Haile2
1Department of Nursing, College of Health Science, Debre Berhan University, Debre Berhan, Ethiopia; 2Department of Midwifery, College of Health Science, Debre Berhan University, Debre Berhan, Ethiopia
Correspondence: Elyas Adamsu Basha Tel +251 911057308
Email [email protected]
Background: Suicidal ideation is thinking about suicide/serving as the agent of one’s own death. Patients with a major depressive disorder are the highest group which are affected by suicidal ideation. It is a pre-condition for suicide attempts and to commit suicide among major depressive patients. Suicidal behavior and major depressive disorder have been becoming the main attention in recent years. In Ethiopia, there is limited knowledge of suicidal ideation among major depressive disorder patients and the factors of suicidal ideation are also limited.
Objective: This study assessed the prevalence of suicidal ideation and its associated factors among major depressive disorder patients at Amanuel Mental Specialized Hospital, Ethiopia.
Methods: A cross-sectional study was conducted from March 1– 30, 2019. A total of 337 major depressive disorder patients were successfully interviewed using structured and pre-tested questionnaires. A systematic random sampling technique was applied. Logistic regression was applied to identify factors of suicidal ideation. Statistical significance was considered at P-value < 0.05.
Results: In this study, the prevalence of suicidal ideation among major depressive disorder patients was 48.4%. Being female (AOR 2.4, 95% CI=1.40, 4.25), family history of suicide (AOR 3.2, 95% CI=1.26, 8.11), and having poor social support (AOR 4.2, 95% CI=2.29, 7.59) were significantly associated with suicidal ideation among patients with major depressive disorder.
Conclusion: The prevalence of suicidal ideation among major depressive disorder patients was relatively high. Hence, due attention should be given to the screening of suicidal ideation for all patients with major depressive disorder to initiate timely interventions.
Keywords: major depressive disorder, suicidal ideation, Amanuel Mental Hospital, Ethiopia
Introduction
Suicide is a deadly act of ending one’s own life.1 It has different stages such as suicidal ideation, plan, attempt, and commit. Suicide is the result of a whole coordinated suicidal process.2 In the beginning, there are intermittent suicidal ideas that could lead to the establishment of a suicidal plan.3 Some people may plan even for yours to commit suicide while others end their own life impulsively.4 Suicide is a huge but largely preventable health problem causing almost half of all violent deaths.5,6 It is a major risk among patients with major depressive disorder (MDD) and a significant proportion of patients with major mood disorders die by suicide.5–9
The occurrence of suicide among individuals with MDD is substantial, and it is one of the most disturbing outcomes of depression. Suicide is obviously the end consequence of a person’s feeling of hopelessness, worthlessness, and incapacity.10
Suicidal ideation is thinking about suicide/serving the agent of one’s own death.11 It is an important phase in the suicidal process preceding attempted suicide and it is common in the general population.12 Suicidal ideation is considered a dangerous step leading to subsequent suicidal behaviors. Furthermore, suicidal ideation or suicidal thoughts are a major risk factor for suicide attempts.13,14 Even though suicidal ideation is highly prevalent among patients with MDD, it may be present outside of depression, and is now being recognized as a trans diagnostic phenomenon.11
Suicidal ideation arises as a symptom of depression, especially if there are reasons for a person to feel hopeless concerning the future.11 Patients with MDD are the highest group which are affected by suicidal ideation.9 Suicidal ideation appears to be a pre-condition for suicide attempts and is a strong risk factor for completed suicide among patients with MDD.12,15 According to previous studies there is significant association between suicidal ideation among patients with MDD.10 MDD causes feelings of sadness, loss of interest in activities once enjoyed.16
The prevalence of suicidal ideation has been reported since the 1970s. In recent years, the prevalence of suicidal ideation is increasing.3 Depending on the setting of each particular study, the 12-month prevalence has varied from 2.3% to 58%%.6,11 Prior studies also suggest a variety of risk factors for suicidal ideation. Low social support, substance use disorder,14 previous suicide attempts,17 hopelessness and sleep disturbances,18 elevated inflammation19 have been found to be associated with suicidal ideation. The studies we have cited above have also investigated suicidal ideation among patients with MDD. The association between suicidal behavior and MDD has been becoming the main attention in recent years. In Ethiopia, there are currently very limited studies about the prevalence of suicidal ideation and its associated factors among patients with MDD. Therefore, this study assessed the prevalence of suicidal ideation and its associated factors among patients with MDD at Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia. Early detection of suicidal ideation may enable the health care providers to identify patients at relatively high risk for eventual suicide and to initiate timely interventions.
Materials and Methods
Study Area and Period
The study was conducted from March 1–30, 2019 at Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia. The hospital is one of the oldest and the only mental care hospital in Ethiopia. The hospital provides services for people with psychiatric, neurological, substance use, and psychosocial problems in both outpatient and inpatient cares. It serves on average for 682 major depressive disorder patients monthly and provides outpatient and inpatient service (unpublished Amanuel Mental Specialized Hospital report 2019).
Study Design
A cross-sectional study design was carried out to achieve the aim of this study.
Source and Study Population
All patients with MDD who had a follow-up at the outpatient department of Amanuel Mental Specialized Hospital were the source population. Those who came for the follow-up during the data collection period were considered as the study population.
Inclusion and Exclusion Criteria
Clients with a confirmed clinical diagnosis of MDD and age above or equal to 18 years during the data collection period were considered as eligible candidates for participation, whereas those who had other known psychiatric disorder (other than MDD) and those who are unable to speak or hear were excluded from the study.
Study Variables
The dependent variable was suicidal ideation. The independent variables included sociodemographic factors (age, sex, ethnicity, religion, living condition, marital status, educational status, occupational status) and psychosocial factors (social support).
Operational Definitions
Suicidal Ideation
It is defined as thinking about suicide/serving the agent of one’s own death. It was measured by asking the participants: “Have you ever seriously thought about committing suicide?” If the respondent answered “Yes” for the question, the patient had suicide ideation.
Social Support
It was measured with Oslo’s 3 social support scale. Oslo’s social support scale is a 14-item multiple-choice tool for measuring the perceived social support of patients with MDD. The value of each answer is scored as poor, moderate, and strong social support. Oslo social support scale is scored by summing across all scale items. Respondents who answered “3–8ʹ, “9–11” and “12–14” of Oslo’s social support scale questions correctly were classified as poor social support, moderate social support, and strong social support, respectively.20
Ever Substance Use
It is defined as consuming any substance at least once in his/her lifetime. It was measured by asking the participants: “Have you ever used any substance in your lifetime?” If the respondent answered “Yes” for the question, the participants had ever used the substance.
Current Substance Use
It is defined as taking of any one of the substances at least once with in the last one month.
Sample Size and Sampling Technique
The sample size was determined by using a single population proportion formula with the following assumptions. The proportion of suicidal ideation p= 15.2% taken from the previous study conducted in Saint Paul General Hospital,21 with a 95% confidence interval (CI) to be 1.96, and margin of error to be 4%. With the above assumptions and adding a non-respondent rate of 10%, the total sample size was 337.
The study participants were selected by using systematic random sampling technique. The sampling interval was determined by dividing the total study population (major depressive disorder patients) who had monthly follow-up during the study period by the total sample size (682/337). The first study participant was selected by the lottery method from their order to follow up registration, and every other patient at the exit of the hospital was included in the study.
Data Collection
The structured and pre-tested questionnaire was prepared first in English from peer-reviewed articles21,22 and then translated into Amharic (national languages) by expertise. A necessary correction was done after the pretest. The included questionnaire comprised four sections; socio-demographic characteristics, social support questions, suicidal ideation measuring tool, and ever substance used history. Data collectors were trained by principal investigators on how to use the questionnaire and the ethical principles of confidentiality before the actual data collection. The principal investigators control the overall events of the data collection.
Suicidal ideation was assessed using the suicidality module of the World Mental Health survey initiative version of the World Health Organization Composite International Diagnostic Interview tool which was validated in Ethiopia.23 Social support was measured by the Oslo social support scale which is validated for measuring social functioning.20
Data Analysis
Data were checked for completeness and inconsistencies. Epi-data version 3.1 was used for data entry and data were exported into SPSS version 21 for further analysis. Descriptive statistics were computed. Logistic regression analyses were done to identify the relationship between suicidal ideation and independent variables. Independent variables that had a significant association in the bivariate analysis were entered into the multivariable analysis. A significant association was declared at a p < 0.05. The results were presented in text and tables with adjusted odds ratio (AOR) and the corresponding 95% confidence interval.
Ethical Considerations
Helsinki declaration for medical research involving human subjects was followed. Ethical approval was obtained from the research and an ethical review committee of Debre Berhan University. Written informed consent was obtained from each study participant. All the information obtained from the study participants were kept confidential throughout the process of study, and the name of the participant was replaced by code. Withdrawal from the study at any point if they wished was assured.
Results
Socio-Demographic Characteristics
A total of 337 patients with MDD were successfully interviewed. The mean age of the participants was 31.82 (±10.14) years. Fifty-five percent (55.5%) of respondents were female. Half (50.4%) of the study participants were Orthodox Christians and 27.6% were Muslim. The largest proportions, (84%) of the participants were living alone and more than half of the respondents were single (52.2%). Concerning the occupation of the respondents, 20.5% of the respondents were daily laborers. Twenty-eight percent (28.5%) of respondents were had completed secondary education whereas 27.7% of study participants could not read and write. From the total of the study participants, 221 (65.6%) of them reported that poor social support (Table 1).
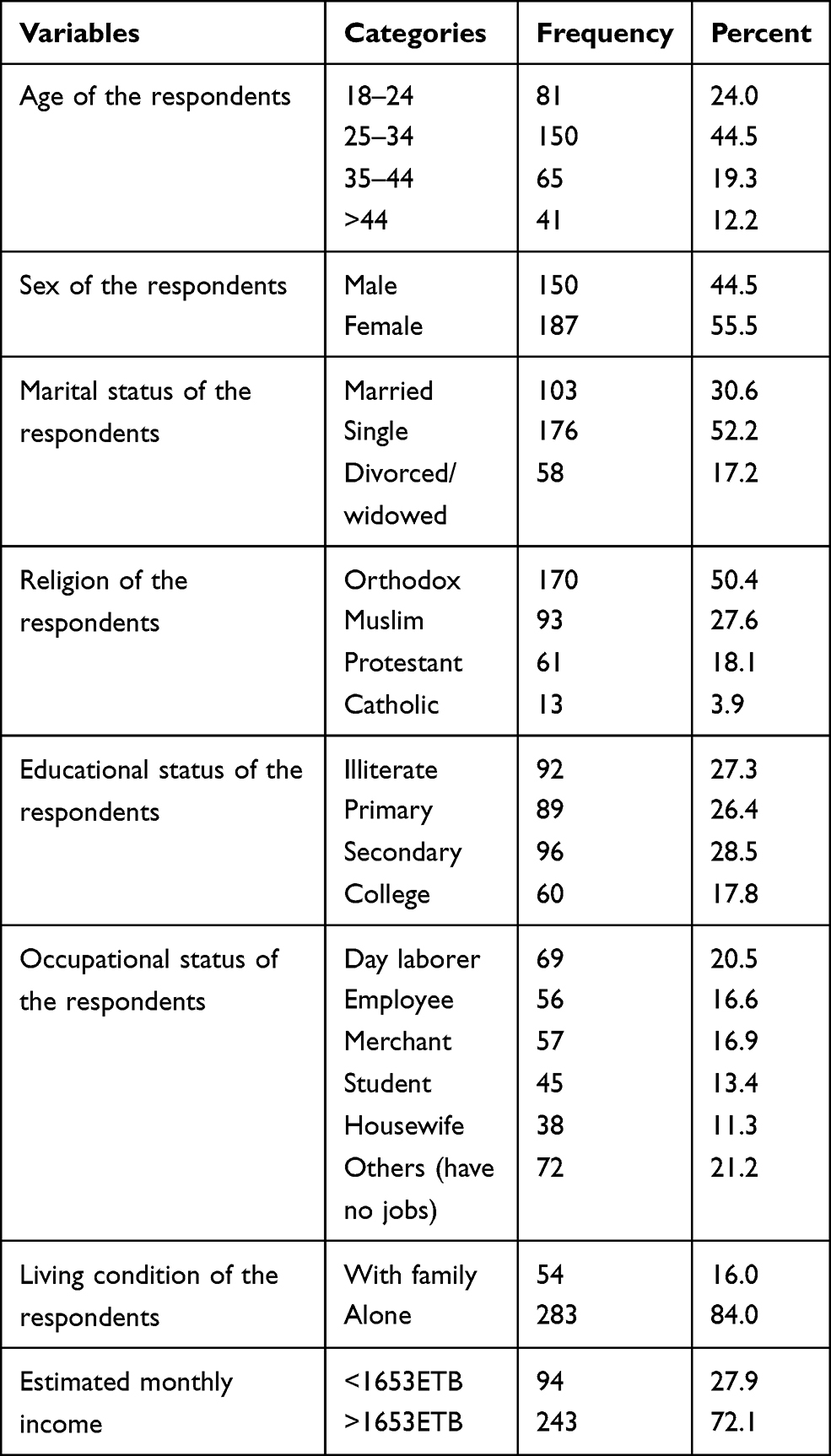 |
Table 1 Socio-Demographic Characteristics of Major Depressive Disorder Patients at Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia, 2019 |
Clinical Characteristics and Substance Use
Among the respondents majority of them were first episodes 178 (52.8%) and 192 (57.0%) were one up to 12 month since diagnosed. Among the respondents 37 (11.0%) have known physical illness. One hundred twenty nine (38.3%) study participants have ever use of substance and 115 (34.1%) have current use of substance use.
Prevalence and Factors Associated with Suicidal Ideation
Alarmingly, the overall prevalence of suicidal ideation among patients with MDD were 163 (48.4%); of whom 120 (35.6%) of them reported suicidal ideation in the last 12 months. In addition, 133 (39.5%) of the respondents had ever planned to commit suicide. For fourteen percent of the study participants, the presence of family conflict was the reason for suicidal ideation (Table 2).
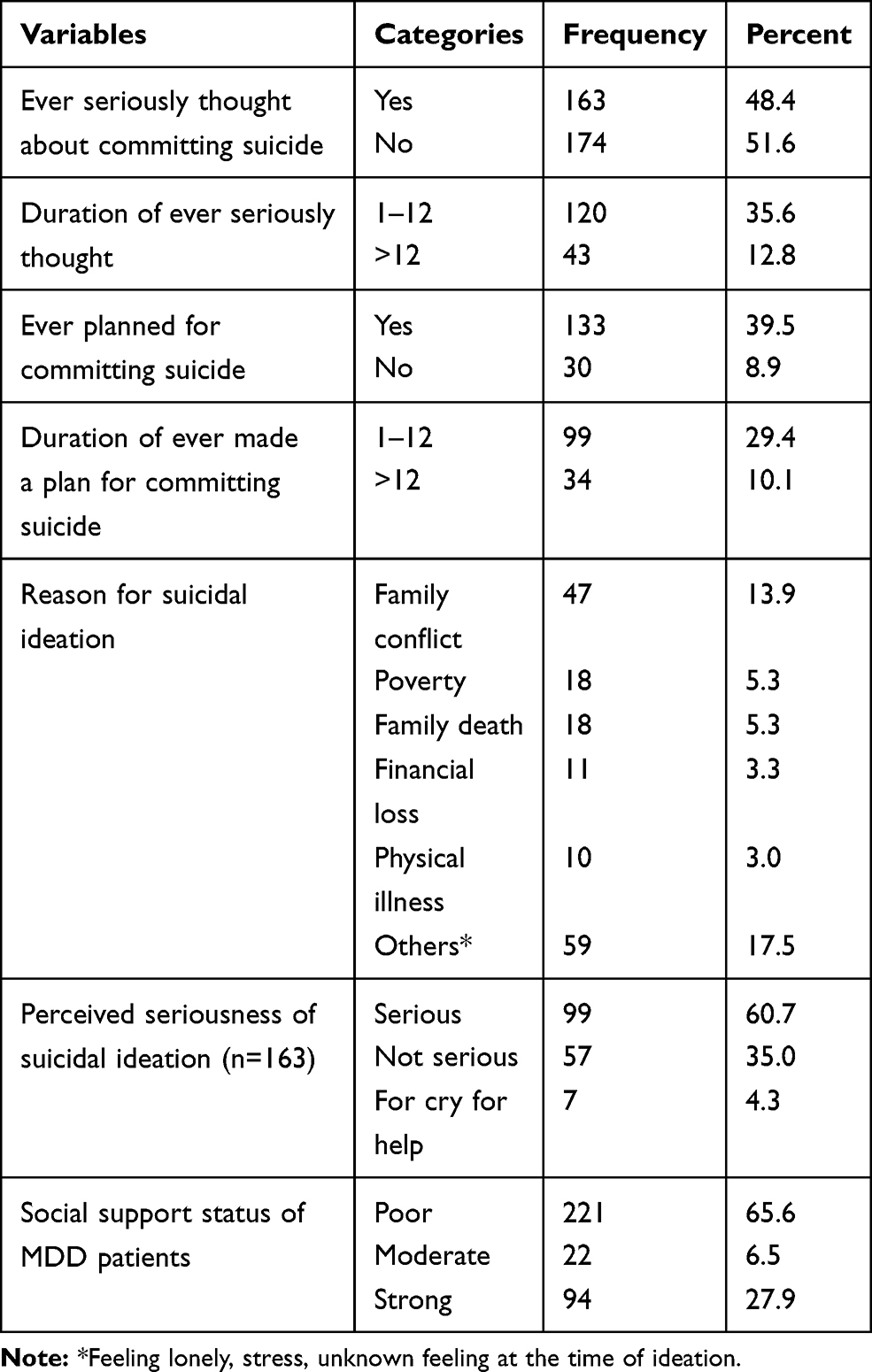 |
Table 2 The Status of Suicidal Ideation Among MDD Patients at Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia, 2019 |
In the multivariable analysis, being a female, previous family history of suicide, and having poor social support were associated with suicidal ideation among patients with MDD. It was observed that females were 2 times more likely to have suicidal ideation than males (AOR 2.4, 95% CI=1.40–4.25). In addition, the odds of suicidal ideation were higher among MDD patients who had a previous family history of suicide (AOR 3.2, 95% CI=1.26, 8.11). On the other hand, suicidal ideation was higher among patients with MDD who had poor social support than those who had strong social support (AOR=4.2, 95% CI=2.29, 7.59) (Table 3).
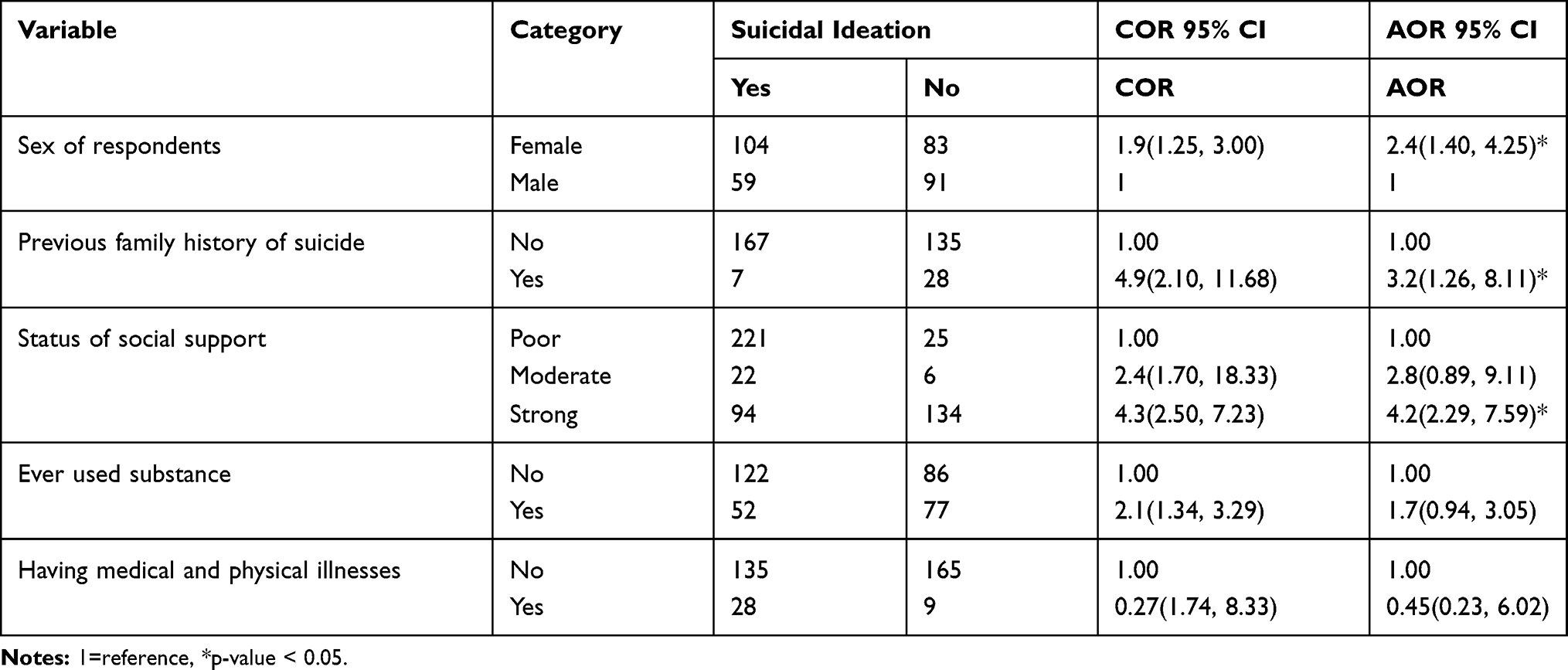 |
Table 3 Factors Associated with Suicidal Ideation Among MDD Patients at Amanuel Mental Specialized Hospital, Addis Ababa, Ethiopia, 2019 |
Discussions
This is one of the few studies that shed light on the prevalence of suicidal ideation and its associated factors among patients with MDD in Ethiopia, thereby helping health professionals and health services to tailor suitable treatment and prevention programs in this context. Alarmingly, the overall prevalence of suicidal ideation among patients with MDD was 48.4%. This figure was higher than the study conducted in Tanzania (26.9%),3 and Singapore (43.6%).24 On the other hand, it was also lower than a study done in Finland (58%).11 This variation could be due to socioeconomic and time variation, the difference in the geographical area, and social support practices for MDD patients. Strong social support could reduce suicidal ideation by hiding feelings of sadness and prevent loss of interest in activities once enjoyed.25
In this analysis, associated factors of suicidal ideation among major depressive disorder patients were identified. Our study found that females were 2 times more likely to have suicidal ideation than males. This is supported by previous studies.3,26 The possible reason might be cyclical hormonal fluctuation that intensifies their stress response. Women are greater vulnerability to other psychosocial stressors.27 There is also evidence that women’s traditional family roles may lead to higher female suicide ideation.28 A family history of suicide was one of the predicting variables for suicidal ideation. The odds of suicidal ideation were higher among MDD patients who had a previous family history of suicide. In agreement with our results, a family history of suicide has been reported as a factor for thinking of suicide in a study conducted in Hungary.29,30 Family relations and connections could contribute to suicidal ideation, also feeling of hopelessness lead to a feeling of worthlessness and a dark future which might be the cause for suicidal ideation.
Another important finding of our study concerns about perceived social support of patients with major depressive disorder. Suicidal ideation was higher among patients with MDD who have poor social support than those who have strong social support. The previous study done in Ethiopia, in line with our result, revealed that poor social support was associated with suicidal ideation.31 World Health Organization also reported that weak social ties and low support from friends or relatives have been significantly associated with suicidal ideation.32 The reason might be poor social ties leads to the perceived stigma which again may result in suicidal thinking.
Conclusions
In this study, the prevalence of suicidal ideation among major depressive disorder patients was relatively high. Being female, previous family history of suicide, and having poor perceived social support were associated with suicidal ideation among major depressive disorder patients. Hence, due attention should be given to the screening of suicidal ideation for all major depressive disorder patients for early diagnosis and treatment.
Data Sharing Statement
The data used to support the findings of this study are included in this manuscript.
Ethics Approval and Consent to Participate
Declaration of Helsinki for medical research involving human subjects was followed. Ethical clearance was obtained from the Ethical Review Committee of Debre Berhan University, College of Health Science. Permission was obtained from Amanuel Specialized Mental Hospital. Confidentiality and privacy of the information were assured and maintained by preventing disclosure of the information to other third parties.
Consent for Publication
Not applicable
Acknowledgments
We would like to thank Debre Berhan University for allowing us an opportunity to work on identified title and financial grants. We are also grateful to our study participants, data collectors, head/directors of Amanuel Mental Specialized Hospital for their great contribution and support. We also express our gratitude to Mr. Alemayehu Gonie (Assistant professor at Debre Berhan University, Ethiopia) for editing the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by research and community service of College of Health Science, Debre Berhan University (protocol No: RCSC/150/2018) in Ethiopia. The funding university does not have any role in the design of the study, data collection, analysis and interpretation of data, and in writing the manuscript.
Disclosure
The authors declare that they have no any competing interests.
References
1. Kaplan BJ. Kaplan and sadock’s synopsis of psychiatry. Behavioral sciences/clinical psychiatry. Tijdschr Psychiatr. 2016;58(1):78–79.
2. Al-Maani MA. Suicidal Ideation among Patients Suffering Depression. Middle East J Psychiatry Alzheimers. 2015;84(1696):1–3.
3. Guedria-Tekari A, Missaoui S, Kalai W, Gaddour N, Gaha L. Suicidal ideation and suicide attempts among Tunisian adolescents: prevalence and associated factors. Pan Afr Med J. 2019;34. doi:10.11604/pamj.2019.34.105.19920
4. Lee J-I, Lee M-B, Liao S-C, et al. Prevalence of suicidal ideation and associated risk factors in the general population. J Formosan Med Assoc. 2010;109(2):138–147. doi:10.1016/S0929-6646(10)60034-4
5. Mekonnen D, Kebede Y. The prevalence of suicidal ideation and attempts among individuals attending an adult psychiatry out-patient clinic in Gondar, Ethiopia. Afr Health Sci. 2011;11(1):103–107.
6. Bulloch AG, Williams JV, Lavorato DH, Patten SB. The relationship between major depression and marital disruption is bidirectional. Depress Anxiety. 2009;26(12):1172–1177. doi:10.1002/da.20618
7. Vuorilehto M, Valtonen H, Melartin T, Sokero P, Suominen K, Isometsä E. Method of assessment determines prevalence of suicidal ideation among patients with depression. European Psychiatry. 2014;29(6):338–344. doi:10.1016/j.eurpsy.2013.08.005
8. Nordentoft M, Mortensen PB, Pedersen CB. Absolute risk of suicide after first hospital contact in mental disorder. Arch Gen Psychiatry. 2011;68(10):1058–1064. doi:10.1001/archgenpsychiatry.2011.113
9. Trivedi MH, Morris DW, Wisniewski SR, et al. Clinical and sociodemographic characteristics associated with suicidal ideation in depressed outpatients. Canadian J Psychiatry. 2013;58(2):113–122. doi:10.1177/070674371305800209
10. Bhattacharjee A, Deb S. Suicidal tendencies among depressive patients. J Indian Acad Appl Psychology. 2007;33(2):213–218.
11. Sokero P. Suicidal ideation and attempt among psychiatric patients with major depressive disorder. 2006. Available from: https://www.julkari.fi/bitstream/handle/10024/78764/2006a13.pdf;sequence=1.
12. Dunlop BW, Polychroniou PE, Rakofsky JJ, Nemeroff CB, Craighead WE, Mayberg HS. Suicidal ideation and other persisting symptoms after CBT or antidepressant medication treatment for major depressive disorder. Psychol Med. 2019;49(11):1869–1878. doi:10.1017/S0033291718002568
13. Ben-Zeev D, Young MA, Depp CA. Real-time predictors of suicidal ideation: mobile assessment of hospitalized depressed patients. Psychiatry Res. 2012;197(1–2):55–59. doi:10.1016/j.psychres.2011.11.025
14. Gensichen J, Teising A, König J, Gerlach FM, Petersen JJ. Predictors of suicidal ideation in depressive primary care patients. J Affect Disord. 2010;125(1–3):124–127. doi:10.1016/j.jad.2009.12.008
15. Banwari GH, Vankar GK, Parikh MN. Comparison of suicide attempts in schizophrenia and major depressive disorder: an exploratory study. Asia-Pacific Psychiatry. 2013;5(4):309–315. doi:10.1111/j.1758-5872.2012.00188.x
16. Holma KM, Haukka J, Suominen K, et al. Differences in incidence of suicide attempts between bipolar I and II disorders and major depressive disorder. Bipolar Disord. 2014;16(6):652–661. doi:10.1111/bdi.12195
17. Xin L-M, Chen L, Su Y-A, et al. Risk factors for recent suicide attempts in major depressive disorder patients in China: results from a National Study. Front Psychiatry. 2018;9:300. doi:10.3389/fpsyt.2018.00300
18. Chellappa SL, Araújo JF. Sleep disorders and suicidal ideation in patients with depressive disorder. Psychiatry Res. 2007;153(2):131–136. doi:10.1016/j.psychres.2006.05.007
19. O’Donovan A, Rush G, Hoatam G, et al. Suicidal ideation is associated with elevated inflammation in patients with major depressive disorder. Depress Anxiety. 2013;30(4):307–314. doi:10.1002/da.22087
20. Abiola T, Udofia O, Zakari M. Psychometric properties of the 3-item oslo social support scale among clinical students of Bayero University Kano, Nigeria. Malaysian J Psychiatry. 2013;22(2):32–41.
21. Whittier AB, Gelaye B, Deyessa N, et al. Major depressive disorder and suicidal behavior among urban dwelling Ethiopian adult outpatients at a general hospital. J Affect Disord. 2016;197:58–65. doi:10.1016/j.jad.2016.02.052
22. Wonde M, Mulat H, Birhanu A, Biru A, Kassew T, Shumet S. The magnitude of suicidal ideation, attempts and associated factors of HIV positive youth attending ART follow ups at St. Paul’s hospital Millennium Medical College and St. Peter’s specialized hospital, Addis Ababa, Ethiopia, 2018. PLoS One. 2019;14(11):e0224371. doi:10.1371/journal.pone.0224371
23. Kessler RC, Üstün TB. The world mental health (WMH) survey initiative version of the world health organization (WHO) composite international diagnostic interview (CIDI). Int J Methods Psychiatr Res. 2004;13(2):93–121. doi:10.1002/mpr.168
24. Subramaniam M, Abdin E, Seow E, Picco L, Vaingankar JA, Chong SA. Suicidal ideation, suicidal plan and suicidal attempts among those with major depressive disorder. Ann Acad Med Singapore. 2014;43(8):412–421.
25. Nock MK, Borges G, Bromet EJ, et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br j Psychiatry. 2008;192(2):98–105. doi:10.1192/bjp.bp.107.040113
26. Beyene A, Taddese M, Getachew Y, Kumara P, Birkie M. Suicidal Attempt and Associated Factors among Patients with Depressive Disorder Visiting Psychiatric Unit. IOSR Journal of Nursing and Health Science (IOSR-JNHS).7(1):62-66. doi:10.9790/1959-0701106266
27. Molla A, Mengesha A, Derajew H, Kerebih H. Suicidal ideation, attempt, and associated factors among patients with tuberculosis in Ethiopia: a cross-sectional study. Psychiatry j. 2019;2019:1–10. doi:10.1155/2019/4149806
28. Organization WH. Scaling up mental health care: a framework for action. World Health Organization. Regional Office for the Eastern Mediterranean; 2015.
29. Tóth MD, Ádám S, Zonda T, Birkás E, Purebl G. Risk factors for multiple suicide attempts among Roma in Hungary. Transcult Psychiatry. 2018;55(1):55–72. doi:10.1177/1363461517731703
30. Guintivano J, Brown T, Newcomer A, et al. Identification and replication of a combined epigenetic and genetic biomarker predicting suicide and suicidal behaviors. Am j Psychiatry. 2014;171(12):1287–1296. doi:10.1176/appi.ajp.2014.14010008
31. Hussien Z, Solomon H, Yohannis Z, Ahmed A. Prevalence and associated factors of suicidal ideation and attempt among people with schizophrenia at amanuel mental specialized hospital Addis Ababa, Ethiopia. J Psychiatry. 2015;18(1):184. doi:10.4172/Psychiatry.1000184
32. McKinnon B, Gariépy G, Sentenac M, Elgar FJ. Adolescent suicidal behaviours in 32 low-and middle-income countries. Bull World Health Organ. 2016;94(5):340. doi:10.2471/BLT.15.163295
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.