Back to Journals » Infection and Drug Resistance » Volume 13
Successful Incidences of Controlling Multidrug-Resistant, Extensively Drug-Resistant, and Nosocomial Infection Acinetobacter baumannii Using Antibiotic Stewardship, Infection Control Programs, and Environmental Cleaning at a Chinese University Hospital
Received 29 April 2020
Accepted for publication 5 July 2020
Published 27 July 2020 Volume 2020:13 Pages 2557—2570
DOI https://doi.org/10.2147/IDR.S260525
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Lei Liu,1,2 Bin Liu,3 Wei Li1
1Heilongjiang Key Laboratory for Zoonosis, College of Veterinary Medicine, Northeast Agricultural University, Harbin, People’s Republic of China; 2Department of Respiratory Medicine, The Fourth Affiliated Hospital of Harbin Medical University, Harbin, People’s Republic of China; 3Department of Respiratory Medicine, The First Affiliated Hospital of Harbin Medical University, Harbin, People’s Republic of China
Correspondence: Wei Li Email [email protected]
Objective: We estimated the efficacy of antimicrobial stewardship (AMS), infection control programs (ICP), and environmental cleaning (ENC) for controlling the resistance of Acinetobacter baumannii (AB) and controlling the incidence of multidrug-resistant AB (MDRAB), extensively drug-resistant AB (XDRAB), and nosocomial infection AB in the ICU (NIAB-ICU) at a university hospital.
Methods: The intervention included 4-year AMS+ICP and 3-year AMS+ICP+ENC between January 2012 and December 2019.
Results: A total of 2636 AB isolates were collected totally, and 64.98% of AB isolates were MDR and 29.97% were XDR. Preintervention and postintervention incidences of MDRAB, XDRAB, and NIAB-ICU by AMS+ICP measures ranged from 84.96% to 71.98%, 41.96% to 33.13%, and 45.6% to 38%, respectively. However, all of them were not statistically changed (P=0.085, 0.072, 0.061, separately). The preintervention and postintervention incidences of MDRAB, XDRAB, and NIAB-ICU by AMS+ICP+ENC measures ranged from 71.98% to 36.55%, 33.13% to 19.88%, and 38% to 22.5%, respectively. Statistically significant declines were observed (P=0.016, 0.041, 0.032, separately). The defined daily doses (DDD) per 1000 patient-days (PD) decreased from 45± 3.3 to 30.81± 1.5 per 1000 PD across from 2012 to 2019, and a statistical decline was seen (P=0.01). Concurrently, the alcohol-based hand gel (ABHG) consumption per 1000 PD increased from 0.6± 0.05 L to 12.5± 2.3 L per 1000 PD, and a statistical increase was observed (P=0.0001). A statistically positive correlation was revealed between the DDD and incidence of MDRAB, XDRAB, and NIAB-ICU (r=0.905 and p=0.002; r=0.939 and p=0.001; r=0.956 and p=0.0002; respectively). Simultaneously, a statistically negative correlation was showed between the ABHG and incidence of MDRAB, XDRAB, and NIAB-ICU (r=− 0.858 and p=0.006; r=− 0.888 and p=0.003; r=− 0.882 and p=0.004, separately).
Conclusion: The AMS, ICP, and ENC may be one of the most effective and best measures to address the increasing incidence of MDRAB, XDRAB, and NIAB-ICU currently.
Keywords: Acinetobacter baumannii, antibiotic resistance, antibiotic stewardship, infection control programs, environmental cleaning
Introduction
Multidrug-resistant (MDR) and extensively drug-resistant (XDR) Acinetobacter baumannii (AB) is one of the most important nosocomial opportunistic pathogens; it has a unique ability for manifesting antimicrobial resistance.1 The reported incidence of MDRAB and XDRAB infections has substantially increased over the past decades.2 A rising incidence of carbapenem-resistant AB (CRAB), intrahospital and interhospital spread of CRAB, and a colistin-resistant AB complex has appeared in intensive care units (ICUs).3,4 It must be noted that a high mortality rate has been associated with infections caused by CRAB strains.5 The rapid spread of MDRAB and XDRAB in clinical settings has made choosing an appropriate antibiotic to treat these infections and executing contact precautions difficult for clinicians; indeed, institutional outbreaks caused by MDRAB and XDRAB are a tremendous public health problem.3,5 Although controlling the transmission of MDRAB and XDRAB is a high priority for hospitals, there is little information and data about MDRAB and XDRAB control.1 The limited or even no effective treatment options make the clinical management of MDRAB and XDRAB infections particularly challenging.6
Despite several recommendations over the years, infection control programs (ICPs) and antimicrobial stewardship (AMS) have been implemented in several hospitals to promote the appropriate use of antimicrobials and prevent MDRAB. The interventions vary widely by region and effect.7 A few studies have revealed how education for ICPs, hand hygiene campaigns, and the judicious use of carbapenem may decrease the nosocomial incidence of CRAB and MDRAB.8–10 However, more and more studies have shown that the drug resistance of AB has generally increased; the prevalence of CRAB has increased worldwide, and numerous hospital outbreaks in ICUs have been reported.11–14 Some studies have even suggested enhanced stewardship programs are urgently needed and have been developed to avoid the spread and potential outbreaks by MDRAB, especially in high-resistance endemic settings.15,16
Consequently, the relative efficacy of ICP and AMS is still inconclusive and controversial when it comes to controlling MDRAB and XDRAB.11,12
Environmental cleaning (ENC) is an important component of a comprehensive strategy to control healthcare-associated infections, especially in wards such as the ICU, where patients are compromised.17,18 One study showed that comprehensive measures with environmental cleaning in a NICU environment were effective and significantly reduced the incidence rate of methicillin-resistant Staphylococcus aureus.19
A systematic review showed some strategies were differential for certain bacteria in ICUs, and when ENC was added to standard care + AMS, there was a significant reduction in the acquisition of MDR-AB. Hence, it is necessary to deeply evaluate the most effective prevention strategies.11
Therefore, the purpose of our study is to estimate the efficacy of AMS, ICP, and ENC for controlling the resistance trend of AB and controlling the incidence of MDRAB, XDRAB, and nosocomial infection of AB in ICU (NIAB-ICU). The study was conducted from January 2012 to December 2019 at a tertiary hospital center.
Methods
The 4th Affiliated Hospital of Harbin Medical University, a 2600-bed teaching hospital located in northeastern China, has a 30-bed medical ICU and a 20-bed surgical ICU. Because of an increased incidence of MDRAB, XDRAB, and NIAB-ICU, ICP and AMS have been executed at this hospital since 2013. Active and exhaustive ENC has been implemented strictly since 2016. Therefore, we retrospectively estimated the efficacy of the intervention measures, including ICP, AMS, and ENC, between January 2012 and December 2019.
Bacterial Isolates
AB, which was included in our study, was confirmed infection from the patient’s clinical case and clinician. Clinical isolates from samples including blood, respiratory tract, urinary tract, wound surface, and other sources were obtained for every year. Isolate identification and antimicrobial susceptibility testing of AB were performed using VITEK II (bioMerieux, Marcy L’Etoile, France). Hand cultures from health care workers were also estimated for those working in the ICU. Environmental cultures were conducted for a diverse group of sites, including surrounding curtains, bedrails, bedside tables, respiratory equipment ventilator tubes, blood pressure cuffs, infusion pumps, stethoscopes, suctioning equipment, washbasins, computer keyboards, and monitors. The environmental and hand cultures were sampled using a sterile premoistened cotton swab, which was inoculated onto MacConkey agar plates. Isolates were transferred to the coordinating laboratory, subcultured on suitable media, and reserved in skim milk at −80°C until the minimum inhibitory concentration (MIC) was determined.
Antimicrobial Sensitivity and Resistance
The in vitro activity of regularly utilized antimicrobial agents was determined by broth microdilution in line with the guidelines of the Clinical and Laboratory Standards Institute (CLSI).20,21 The interpretive standards for the MIC of the antibiotics were determined based on the CLSI breakpoints.21 Classification of the AB isolates as a MDR or XDR was based on the EUCAST Expert Rules.22 Nosocomial infection with AB in the ICU was defined using the Centers for Disease Control and Prevention’s definitions of nosocomial infections.20,23 The seven types of antibiotic agents tested in the current study were extended-spectrum cephalosporins (ceftazidime), carbapenems (imipenem and meropenem), quinolones (ciprofloxacin), b-lactam/b-lactamase inhibitor combinations (piperacillin/tazobactam and cefoperazone/sulbactam), aminoglycosides (gentamicin and amikacin), glycopeptides (colistin), and tetracyclines (tigecycline). Colistin was examined in line with the recommendations of the CLSI–European Committee on Antimicrobial Susceptibility Testing (EUCAST).23
Environmental Cleaning
According to the literature,20 an exhaustive environmental cleaning program was established since 2016 at the 4th Affiliated Hospital of Harbin Medical University. The disinfectants used were hypochlorite-based disinfectants; a wipe disinfectant containing benzalkonium chloride and propane-1,2-diol was used for the handling of nondisposable medical products in which this disinfectant was not appropriate. Disposable medical products were discarded once the patient did not need them anymore, here by following the Centers for Disease Control’s recommendations,20 and nondisposable products were disinfected following the procedures previously illustrated. Two detailed checklists were established to verify the environmental decontamination sequence: one for the medical equipment sterilization and the other for the general environmental cleaning. These checklists had to be signed by the cleaning staff after executing any sterilization procedure, and the frequency was twice a day; the qualification rate was analyzed weekly. The infection control specialist met with the cleaning staff several times a week for feedback of the monitoring results and educational aims. Each ICU ward was closed in sequence periodically for a terminal sterilization at least three times every year. In addition, the bedside and room of a patient with MDRAB or XDRAB infection underwent terminal cleaning after discharge.
Infection Control Projects
According to the literature,21 a comprehensive ICP has been implemented since 2013 at the 4th Affiliated Hospital of Harbin Medical University, as follows:
- Illustrations for hand hygiene were provided via an education plan. An alcohol-based hand gel (ABHG) was available at all bedsides in the ICUs. Dispensers for ABHGs were fixed in every room and aisle to sustain and promote fundamental hygiene. Education of the hospital staff and campaigns to increase hand hygiene adherence were also conducted.
- Hand hygiene adherence was continuously monitored by blinded nurses who were working in each ICU. Cultures from the hands of the medical staff who had cared for the infected patients and the environment were analyzed at three time points during their ICU stay to investigate cross-infection and the spread of infection to the staff. Monthly, the individual results were reported to the health care workers and the administration staff.
- Illustrations for contact with and the seclusion of patients infected with MDRAB and XDRAB were provided. A list of infected patients for seclusion and cautionary contact was also created. The list was kept secret. Furthermore, the list also applied to the next hospital stay until colonization was removed.
- Active surveillance for MDRAB and XDRAB colonization was conducted. All patients admitted to adult ICUs were screened weekly. Surveillance cultures were obtained by rectal and pharyngeal swabs. Positive monitoring was performed in all the patients who were admitted to the ICU for more than 2 days during an ongoing transmission.
- Environmental cleaning for wards that infected patients might have touched was implemented according to the guidelines of the Centers for Disease Control and Prevention.24 Environmental cleaning and disinfectants for any equipment were applied for an adequate period to achieve sterilization, based on the manufacturer’s guidelines.
- Regular meetings for the healthcare workers of affected areas were held every 2 to 4 weeks during the first year of intervention and every 2 to 3 months afterwards; these were compulsory for ICU staff. In addition, all staff members were periodically informed about the evolution of rates as part of the educational program (monthly in ICUs, quarterly in other units).
Antimicrobial Stewardship
Based on the literature,21 antibiotic usage was strictly restricted through AMS since 2013 at the 4th Affiliated Hospital of Harbin Medical University, antibiotic use classification management included the following system:
- Special usage classification of antibiotics: Limited clinical data are available on the efficacy or safety of new antibiotics or their superiority. These drugs are expensive, and hence, their use must be strictly controlled. The prescription of special usage classification antimicrobial agents requires approval from a respiratory medicine or infectious diseases physician. Doctors qualified at the sub senior level or above were granted special usage of such antibiotics and could prescribe them after examination.
- Restricted usage classification of antibiotics: There are limitations based on the safety, cost, efficacy, and so forth of the drug for antibiotics that have a significant influence on pathogen resistance. A prescription for the restricted usage classification of antimicrobial agents requires approval from an respiratory medicine or infectious diseases physician. Doctors at an intermediate level or above were granted restricted usage of the antibiotics and could prescribe them after examination.
- Unrestricted usage classification of antibiotics: This is applicable in the case of antibiotics that have been proven to be inexpensive, effective, and safe in clinical practice for a long time; they also have little influence on bacterial resistance. The doctors were granted unrestricted usage of the antibiotics and could prescribe them after examination.
On a hospital-wide basis, the prescription of restricted antimicrobial agents requires approval from a respiratory medicine or infectious diseases physician. An online antimicrobial control system has been deployed since 2013. Through the hospital information system, the respiratory medicine or infectious diseases physician can review the reports of cultures, the clinical and laboratory presentation, and the images of each patient to whom special use of antimicrobial agents and the restricted antibiotics have been prescribed. Should a denial be made, the antimicrobial is discontinued by the hospital information system and notified immediately to modify the prescription.
Data Collection
The incidence density rate of hospital-onset MDRAB or XDRAB was defined as the per-patient number of first MDRAB or XDRAB isolates from clinical specimens and active surveillance testing at ≥3 calendar days after admission to the ICU; this was done after excluding patients with a history of colonization or infection.25 Multiple positive isolates from one patient were considered as a single sample. Isolates were defined as susceptible, resistant, or intermediate to an antibiotic for statistical analysis. The ABHG consumption was calculated as the number of liters per 1000 patient-days (PD) and utilized as a marker for adherence to ICP rules. Antibiotic consumption was calculated as the defined daily dose (DDD) per 1000 PD, which is in line with the suggestions from the World Health Organization.26 Data on antibiotic consumption were obtained from the hospital pharmacy service.
Statistical Analysis
Analyses were performed using SPSS v.17 (IBM, Armonk, NY). The chi-square test was utilized to compare the incidence density rate of susceptibility and resistance to AB, MDRAB, XDRAB, and NIAB-ICU during the study period. A t test was used to compare the variations of ABHG consumption and antibiotic consumption. A Pearson correlation coefficient was applied to confirm the correlation between the incidence rate of MDRAB, NIAB-ICU, and XDRAB and the ABHG consumption and the DDD. All examinations were two-tailed, and P<0.05 was considered to indicate statistical significance.
Results
In total, between January 2012 and December 2019, 2636 AB clinical isolates were collected. Overall, 64.98% (1713) of the AB clinical isolates assessed were MDRAB, and 29.97% (790) were XDRAB. The number of AB clinical isolates obtained annually varied between 286 and 402.
Table 1 reveals that the AB clinical isolates were mainly isolated from the patient’s respiratory tract sample, ICU ward, and patients over 65 years old, accounting for 79.5% (2096), 68% (1794), and 65% (1713), respectively.
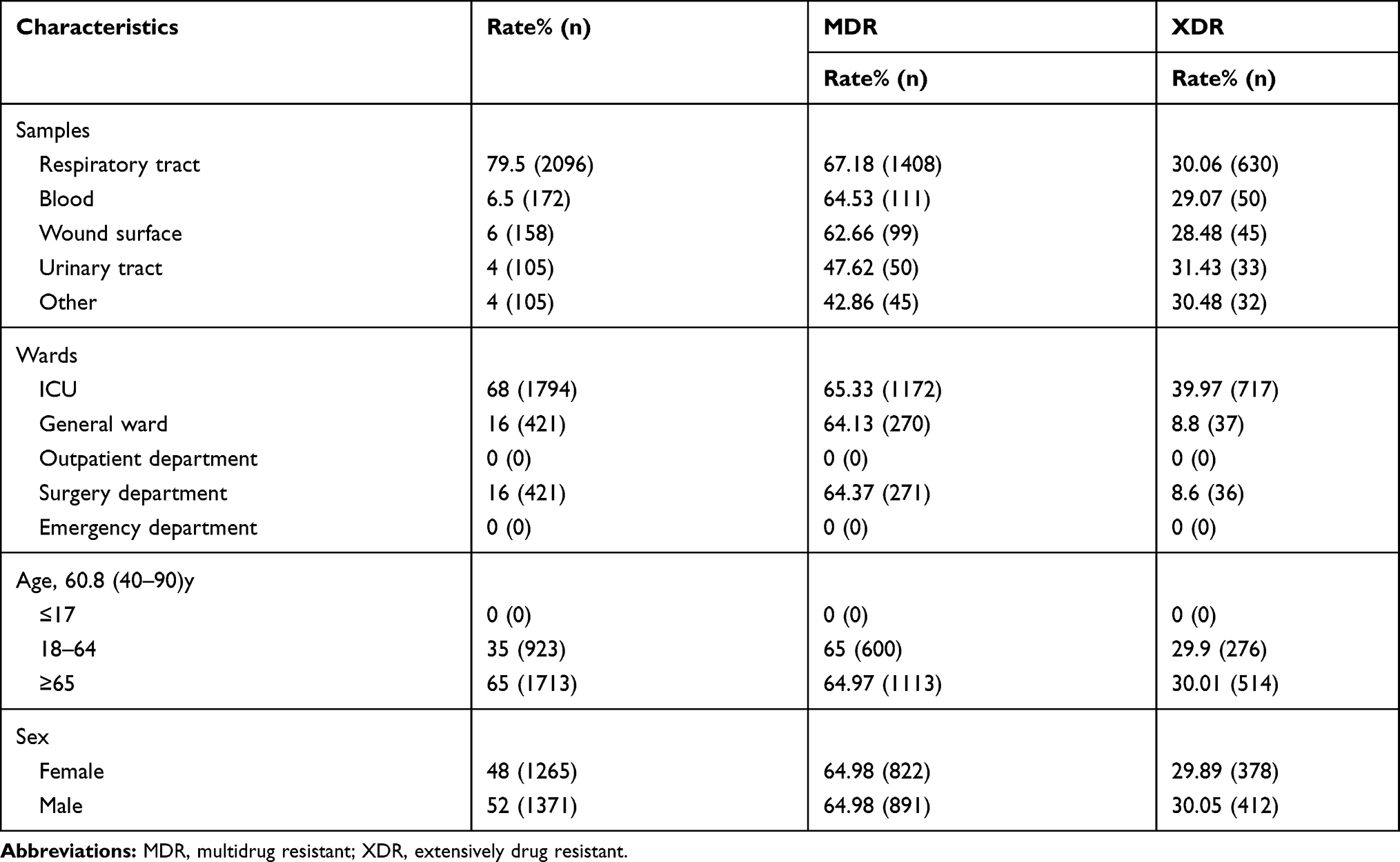 |
Table 1 Patients Characteristics of 2636 AB Clinical Isolates from 2012 to 2019 |
Table 2 presents the data related to antibiotic susceptibility and resistance of the AB clinical isolates. Colistin and tigecycline were the most effective antibiotics assessed: 99.6% and 98.83% of the AB isolates showed in vitro susceptibility to colistin and tigecycline, respectively, and 0.4% and 1.17% of the AB isolates showed resistance to colistin and tigecycline, respectively. In contrast, ciprofloxacin and piperacillin/tazobactam were the least effective antibiotics evaluated: only 10.9% of the AB clinical isolates were susceptible, and 79% were resistant to ciprofloxacin; in addition, 13.82% were susceptible and 81.07% were resistant to piperacillin/tazobactam. Colistin and tigecycline remained the most effective antibiotics assessed, with 98.5% and 95% of the MDRAB clinical isolates showing in vitro susceptibility to colistin and tigecycline, separately. Furthermore, colistin and tigecycline were the most effective antibiotics assessed for XDRAB, with 91.4% and 82% of the XDRAB clinical isolates showing in vitro susceptibility to colistin and tigecycline, respectively.
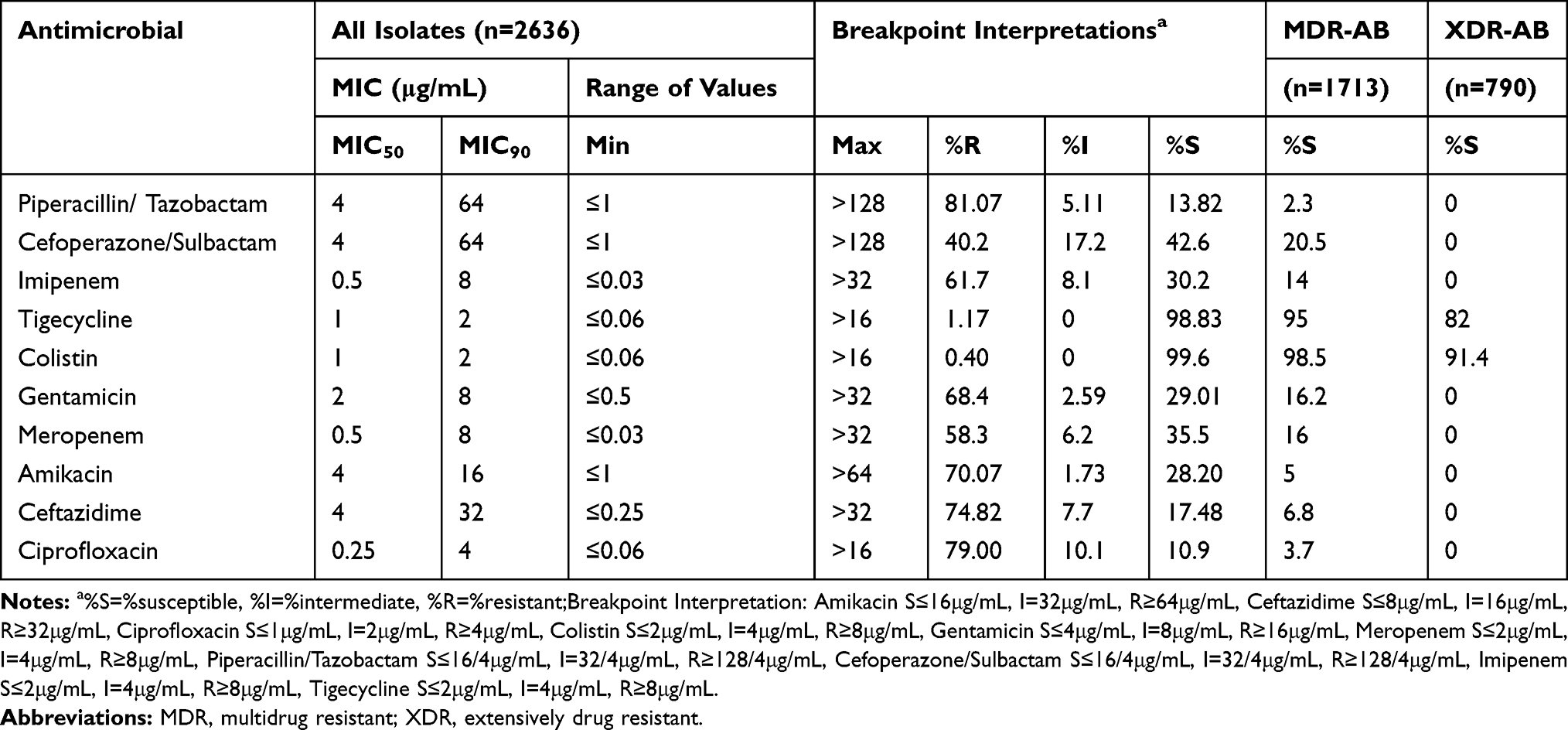 |
Table 2 Antimicrobial Susceptibility of AB Clinical Isolates Obtained from Patients at a Hospital Center in China,2012–2019 |
The resistance of the AB clinical isolates, stratified by study year, is presented in Table 3 and Figure 1. Over the 8-year study period, colistin and tigecycline were found to be stable and to have the lowest resistance among the antimicrobial agents. After the AMS and ICP interventions were implemented in 2013 and the ENC intervention was executed in 2016, the resistance of other antimicrobial agents to the AB clinical isolates, except for colistin and tigecycline, obviously decreased.
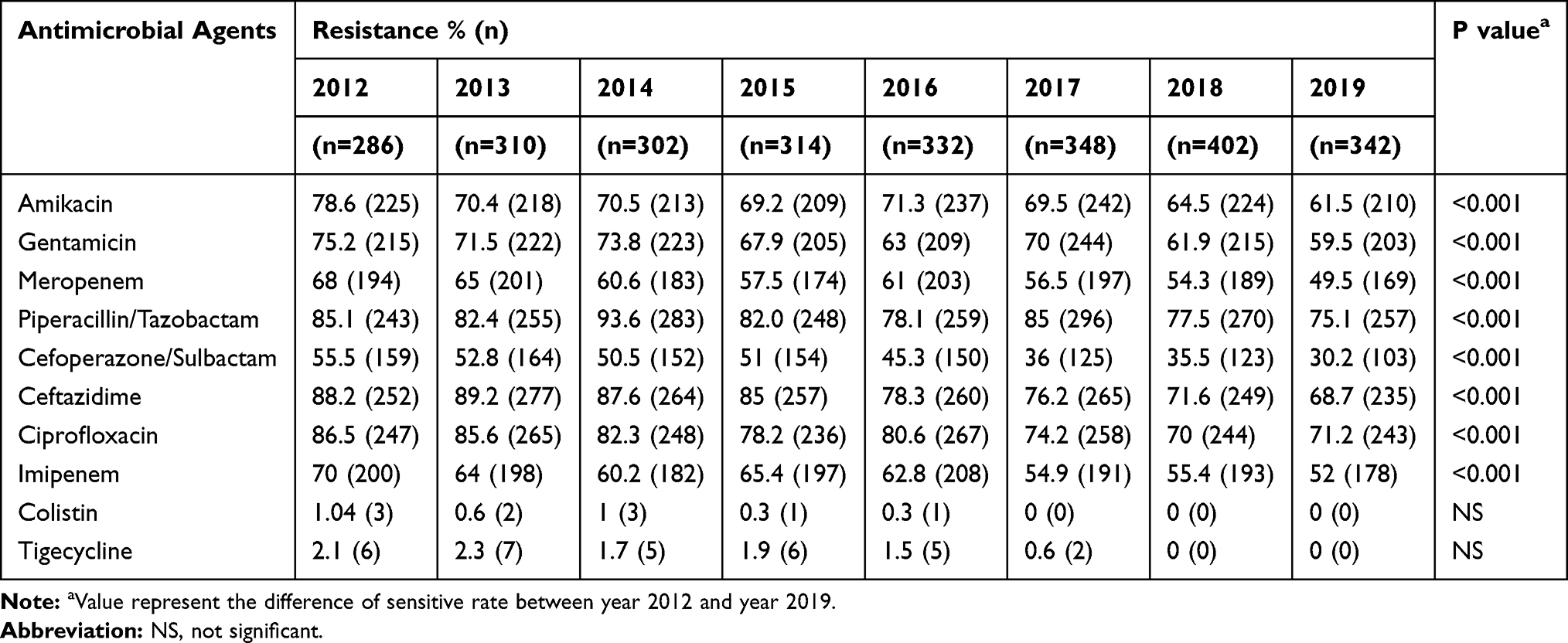 |
Table 3 Antimicrobial Resistance of AB Clinical Isolates |
 |
Figure 1 Antimicrobial resistance of AB clinical isolates obtained from patients at a hospital center in China, 2012–2019. |
The sensitivity of the AB clinical isolates, stratified by study year, is presented in Table 4 and Figure 2. Over the 8-year study period, colistin and tigecycline were found to be stable and to have the highest susceptibility among the antimicrobial agents. After the AMS and ICP interventions were implemented in 2013 and the ENC intervention was executed in 2016, the susceptibility of the other antimicrobial agents to the AB clinical isolates, except for colistin and tigecycline, significantly improved.
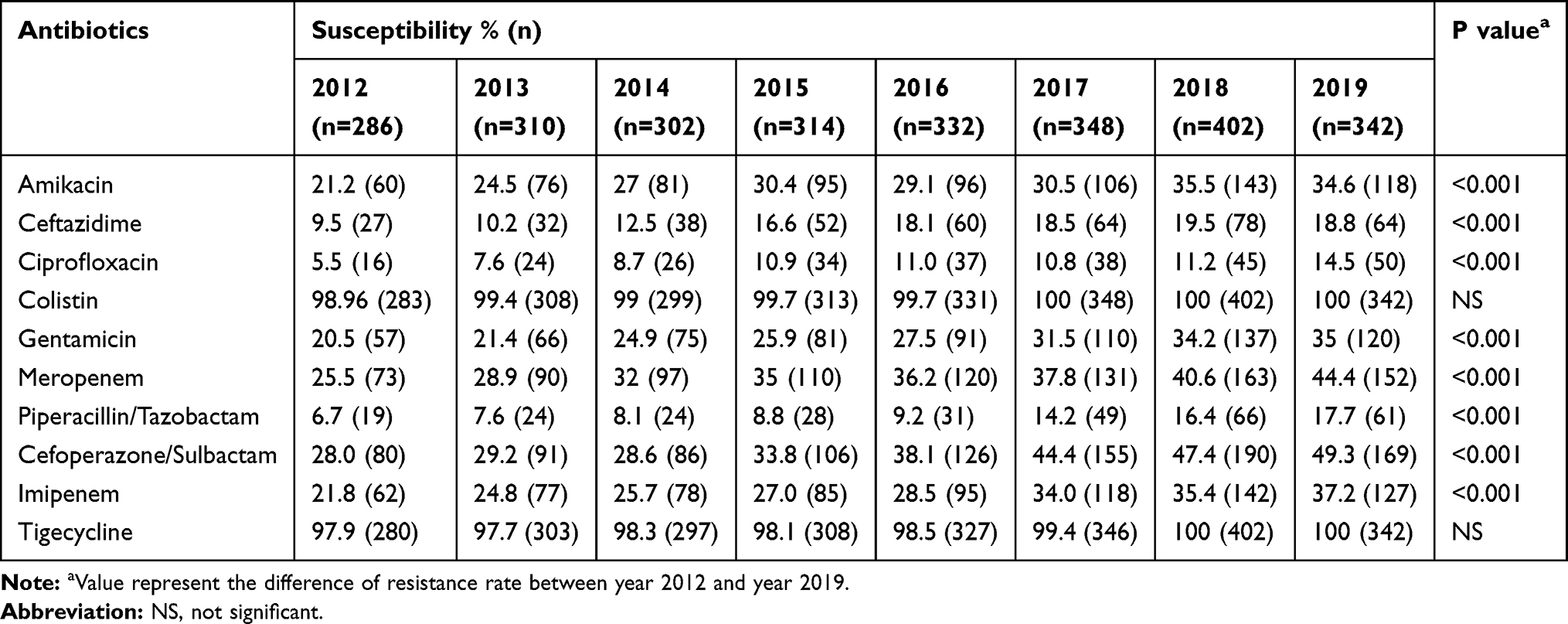 |
Table 4 Antimicrobial Susceptibility of AB Clinical Isolates |
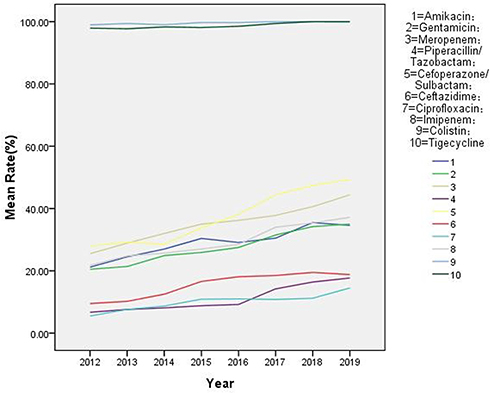 |
Figure 2 Antimicrobial susceptibility of AB clinical isolates obtained from patients at a hospital center in China, 2012–2019. |
As shown in Table 5 and Figure 3, after the AMS+ICP interventions were implemented in 2013, the percentage of MDRAB clinical isolates ranged between 84.96% and 71.98% from 2012 to 2016; this was not a statistically significant change (P=0.085). However, after the AMS+ICP+ENC interventions were strictly executed in 2016, the percentage of MDRAB clinical isolates ranged between 71.98% and 36.55% from 2016 to 2019, and a statistically significant decline was observed (P=0.016). In the same way, the percentage of XDRAB clinical isolates ranged between 41.96% and 33.13% from 2012 to 2016, but this was not a statistically significant difference (P=0.072). However, after the AMS+ICP+ENC interventions were strictly executed in 2016, the percentage of XDRAB clinical isolates ranged between 33.13% and 19.88% from 2016 to 2019, which was a statistically significant decline (P=0.041). In the same light, the rate of NIAB-ICU ranged between 45.6% and 38% from 2012 to 2016, and this was not a statistically significant change (P=0.061); however, after the AMS+ICP+ENC interventions were strictly executed in 2016, the rate of NIAB-ICU ranged between 38% and 22.5% from 2016 to 2019, which was a statistically significant reduction (P=0.032).
 |
Table 5 DDD, ABHG and the Rate of MDR-AB,XDR-AB and NIAB-ICU from 2012 to 2019 |
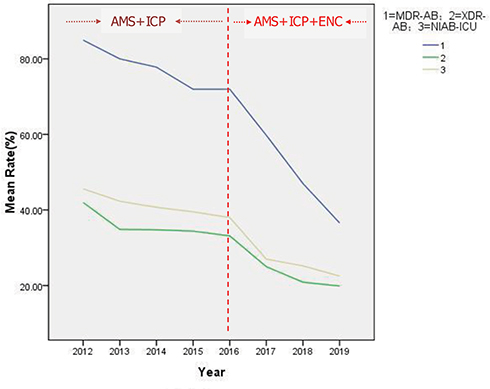 |
Figure 3 The trends of MDR-AB rate, XDR-AB rate and NIAB-ICU rate from 2012 to 2019. Abbreviations: AMS, antimicrobial stewardship; ICP, infection control programs; ENC, environmental cleaning; NIAB-ICU, nosocomial infection of acinetobacter baumannii in ICU. |
The consumption of antimicrobial agents is shown in Table 5. After the AMS and ICP interventions were strictly executed in 2013 and the ENC intervention was implemented in 2016, the DDD per 1000 PD of total antimicrobial agents decreased gradually from 45±3.3 to 30.81±1.5 between 2012 and 2019, meaning a statistically significant decline was observed (P=0.01). In the same way, the ABHG consumption per 1000 PD increased obviously from 0.6±0.05 L to 12.5±2.3 L between 2012 and 2019, and a statistically significant increase was observed (P=0.0001).
The Pearson correlation coefficient is shown in Tables 6–8, and Figure 4. Over the 8-year study period, a statistically significant positive correlation was found between the DDD and the incidence rate of MDRAB, XDRAB, and NIAB-ICU (r=0.905, p=0.002; r=0.939, p=0.001; r=0.956, p=0.0002; respectively). A statistically significant negative correlation was found between the ABHG and the incidence rate of MDRAB, XDRAB, and NIAB-ICU (r=−0.858, p=0.006; r=−0.888, p=0.003; r=−0.882, p=0.004; separately).
 |
Table 6 The Correlation of Isolation Rates of MDR-AB with Consumption of Antimicrobial Agents and ABHG |
 |
Table 7 The Correlation of Isolation Rates of XDR-AB with Consumption of Antimicrobial Agents and ABHG |
 |
Table 8 The Correlation of Rates of NIAB-ICU with Consumption of Antimicrobial Agents and ABHG |
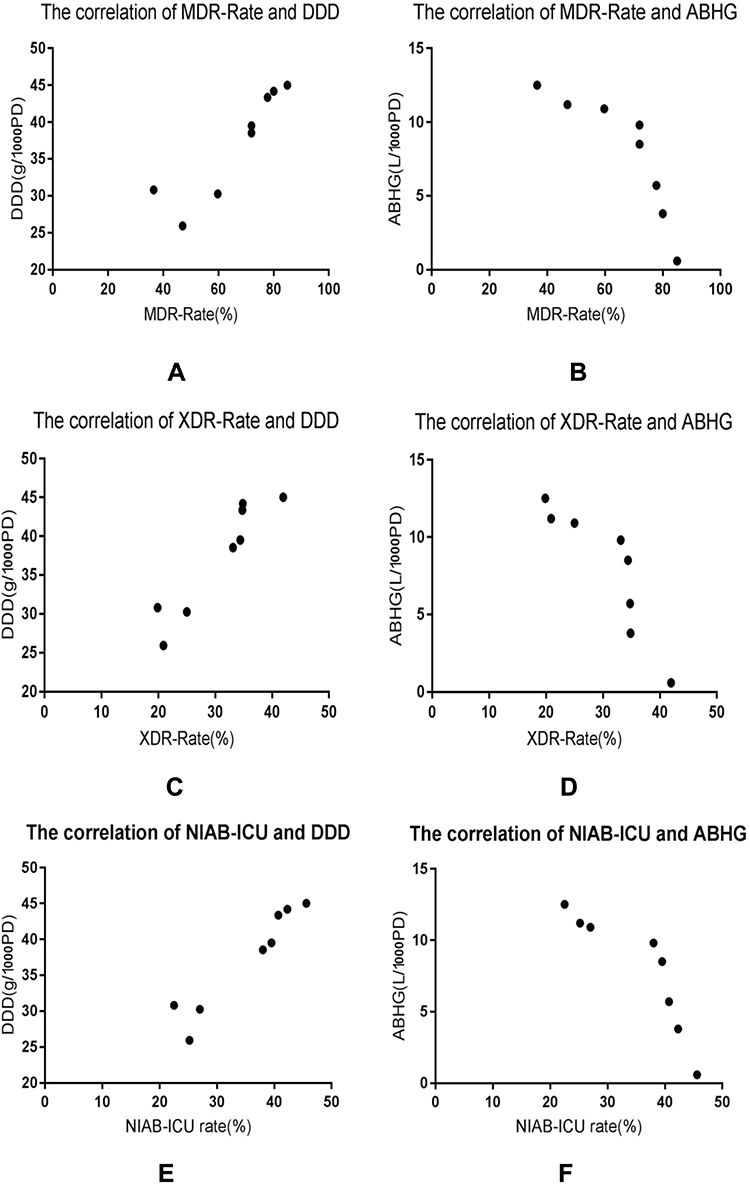 |
Figure 4 The correlations of isolation rates of MDR-AB, XDR-AB and NIAB-ICU with DDD and ABHG. |
Discussion
Acinetobacter baumannii is one of the most important nosocomial infection pathogens.27 The emergence of MDRAB and XDRAB strains is becoming a major public health concern.28 There is a high morbidity rate from AB infections in hospitals, especially in the ICU, and sputum is the most common sample type;29 this is consistent with our research results. Our results further revealed that old age is a high risk group of AB nosocomial infection. A sex bias for AB nosocomial infection was reported,30 but it was not shown in our study; this difference may be explained as regional and endemic.
Antibiotic exposure increases the acquisition of highly resistant AB. Thus, appropriate antibiotic use is imperative.31 Based on the local database of antibiotic resistance from the Taiwan Nosocomial Infection Surveillance System during the period 2003~2012, because of the overuse of carbapenems, the proportion of AB isolates that are resistant to imipenem or meropenem increased from 17.2% to 72.8%.32 Indeed, the proportion of AB clinical isolates resistant to imipenem or meropenem is similar to our research results. Cutting down on the unreasonable usage of antibiotics has been shown to improve patient prognosis and contain the adverse effects of antibiotic consumption.33 Antibiotic application should be based on drug sensitivity and the prevalence of local resistant AB.34 In our study, colistin and tigecycline were found to be the most effective antibiotics assessed, yet some drug sensitivity results are inconsistent with individual reports,35,36 which could be explained by differences in the habit, frequency, and region of antibiotic use. Antibiotic resistance is complex and driven by many interrelated factors, including expectations, time constraints, economic incentives, knowledge, attitudes, perceptions, cultural factors, health system characteristics, and regulations.37,38 Therefore, changing antibiotic prescription behavior is a complex initiative that requires a strategic intervention.37
AMS has also been a cornerstone of controlling resistance AB. Many studies have found it crucial.39 Australia’s first National Antimicrobial Resistance policy for 2015~2019 mentions the demand for resources to sustain the implementation of AMS in all hospitals.40 One study revealed that the incidence of MDRAB was addressed by controlling the inappropriate duration of antimicrobial treatments and the misuse of carbapenems.41 However, the values of DDD in our study are clearly higher than those reported in Australia and the Netherlands.21,42 This may be related to the insufficient of administration of antibiotic application.
MDRAB and XDRAB have a high potential to spread among ill patients in the wards, especially in the ICU.43 Clonal dissemination provides evidence for the prevalence of multidrug-resistant AB among clinical isolates.29 During nosocomial outbreaks, the colonization in the hospital environment was very important for the transmission of MDRAB, and environmental cultures revealed that numerous sites in ICUs were contaminated with MDRAB.44 These reports suggested that the high incidence of MDRAB, XDRAB, and NIAB-ICU should be solved immediately, and the medical specialty must undertake most duties.45
Early recognition and timely implementation of appropriate ICP were crucial in preventing outbreaks.43 Our results suggest monitoring cultures are needed to obviously reduce the incidence of MDRAB, XDRAB and NIAB-ICU. One study showed that providing education about ICP may decrease the nosocomial incidence of CRAB.8 Another study showed that improved monitoring of hospital-acquired infections and effective ICP may be the best way to solve this problem.46 A few studies also have shown that better hand hygiene, isolation of infected patients, environmental disinfection, and targeted surveillance can improve the success rate of controlling MDRAB infection.47,48
Although ICP and AMS were essential for the control of MDRAB infections,1 MDRAB and XDRAB are some of the most difficult multidrug-resistant pathogens to achieve sufficient control. There are still many outbreaks of AB nosocomial infections reported, especially in ICUs,3,16,35,49-52 which indicated that it cannot achieve successful control only through AMS and ICP. This is consistent with what we observed in 2012~2016.
The comprehensive measures of a neonatal ICU with improved ENC practice have been shown to be effective and significantly in reducing the incidence of nosocomial infections.53 Particular attention should be paid to effective ENC.54 Disinfectants should be applied for an adequate period of time to achieve sterilization. The disinfection of potentially contaminated medical equipment should be done meticulously.55 Special attention is required for the sterilization of mechanical ventilators. The ENC and ICP methods that were employed in the current study were based on the accepted tenets of unit closure, intense environmental cleaning, environmental cultures, and improved ICP by the staff.16 Hand hygiene compliance should be improved.54 Testing of the cleaning processes caused the discovery of several leaks, and the environmental cultures provided important feedback for the ICU and cleaning staff. The leaks were addressed with education and checklists.
Curbing the development of resistance in AB is important in hospitals, but there are limited reports on MDRAB, XDRAB, and NIAB-ICU control measures. Although AMS, ICP, and ENC are coordinated strategies designed to promote the appropriate use of antimicrobials and avoid drug resistance of pathogens, their effectiveness have not been fully evaluated. Hence, the current systematic review was performed to evaluate the relative efficacy of strategies for the prevention of MDR gram-negative bacteria in the ICU. When ENC was added to standard care + AMS, there was a significant reduction in the acquisition of MDRAB.11 Because some strategies were differential for certain bacteria, the current study highlights the need for further evaluation of the efficacy of ASM+ICP+ENC.
We assessed the effectiveness of ASM+ICP and ASM+ICP+ENC measures in our study, respectively. Despite the downward trend, the incidences of MDRAB, XDRAB, and NIAB-ICU were not significantly controlled by ASM+ICP intervention measures. The results of our study are counter to those that have been reported in the literature;1 the reason for this may be related to the different level of environmental disinfection. However, after the AMS+ICP+ENC intervention measures were strictly executed, a statistically significant decline in the percentage of MDRAB, XDRAB, and NIAB-ICU was observed. This is showed what we observed in 2016~2019. Our study results further suggest that a statistically significant positive correlation can be found between the DDD and the incidence rate of MDRAB, XDRAB, and NIAB-ICU. Simultaneously, a statistically significant negative correlation was found between the ABHG and the incidence rate of MDRAB, XDRAB, and NIAB-ICU. Nowadays, new antibiotics with resistance to AB are not being developed quickly enough. The control of drugs resistance to AB is imperative. Gajdács M pointed out the main foci of our scientific advancements should be to preserve the drugs that we currently have (through the development of rapid and sensitive diagnostic tools to ensure their prudent use, and antibiotic stewardship practices).56 Hence, our study results have revealed that the trends in the resistance of AB to antibiotics can be affected by AMS, ICP, and ENC. Our study findings suggest that controlling the increasing incidences of MDRAB, XDRAB, and NIAB-ICU by only combining AMS and ICP is far from enough. However, when ENC was added to AMS and ICP, there was a statistically significant decline in the incidence of MDRAB, XDRAB, and NIAB-ICU. Therefore, AMS, ICP, and ENC may be one of the most effective and best measures to address the increasing incidence of MDRAB, XDRAB, and NIAB-ICU.
The main advantages of our study are the time series analysis and the prospective data collection, which permits the exact analysis in the ICP, AMS, and ENC intervention studies. In addition, obtaining a more effective solution for better controlling the incidence of MDRAB, XDRAB, and NIAB-ICU in hospitals needs a multidisciplinary and transversal team. However, our research has a few limitations. First, the design of the current study stops us from realizing if adding any other methods would have led to removing MDRAB, XDRAB, and NIAB-ICU. Simultaneously, the period for observation may not be enough to demonstrate how long the effectiveness of these interventions is maintained after the interventions. Afterwards, despite our study reporting data from the hospital, the application of these methods to other kinds of hospitals and units may need a modification to the local epidemic situation and hospital environment characteristics. Ultimately, testing the susceptibility and resistance to AB clinical isolates was not done for all the antimicrobial agents; therefore, the treatment of MDRAB and XDRAB was based on the local sensitiveness to the main antimicrobial agents and the local epidemiology.
Conclusion
In total, 2636 AB clinical isolates were collected, and 64.98% of the AB clinical isolates assessed were MDRAB, and 29.97% were XDRAB. AB clinical isolates were mainly isolated from the patient’s respiratory tract sample, the ICU ward, and patients over 65 years of age. Colistin and tigecycline were the most effective antibiotics assessed: 99.6% and 98.83% of the AB isolates showed in vitro susceptibility to colistin and tigecycline, respectively. Our study findings suggest that controlling the increasing incidences of MDRAB, XDRAB, and NIAB-ICU by only combining AMS and ICP is far from enough. However, in our study, when ENC was added to AMS and ICP, there was a statistically significant decline in the incidence of MDRAB, XDRAB, and NIAB-ICU. Our study results further suggest that a statistically significant positive correlation can be found between the DDD and the incidence rate of MDRAB, XDRAB, and NIAB-ICU. Simultaneously, a statistically significant negative correlation was found between the ABHG and the incidence rate of MDRAB, XDRAB, and NIAB-ICU. Therefore, AMS, ICP, and ENC may be one of the most effective and best measures to address the increasing incidence of MDRAB, XDRAB, and NIAB-ICU.
Ethics and Consent Statement
This study has been reviewed and approved by the Research Ethics Committee of the Fourth Affiliated Hospital of Harbin Medical University (no. 2019-127). The patient had given his consent for publication of clinical details, and written informed consent was obtained. All authors have been personally and actively involved in substantive work leading to the report, and will hold themselves jointly and individually responsible for its content. All relevant ethical safeguards have been met in line with the Declaration of Helsinki.
Disclosure
The authors report no funding and no conflicts of interest for this work.
References
1. Chen CH, Lin LC, Chang YJ, Chen YM, Chang CY, Huang CC. Infection control programs and antibiotic control programs to limit transmission of multi-drug resistant acinetobacter baumannii infections: evolution of old problems and new challenges for institutes. Int J Environ Res Public Health. 2015;12(8):8871–8882. doi:10.3390/ijerph120808871
2. Gaynes R, Edwards JR; National Nosocomial Infections Surveillance System. Overview of nosocomial infections caused by gram-negative bacilli. Clin Infect Dis. 2005;41(6):848–854. doi:10.1086/432803
3. Nhu NTK, Lan NPH, Campbell JI, et al. Emergence of carbapenem-resistant Acinetobacter baumannii as the major cause of ventilator-associated pneumonia in intensive care unit patients at an infectious disease hospital in southern Vietnam. J Med Microbiol. 2014;63(Pt 10):1386–1394. doi:10.1099/jmm.0.076646-0
4. Qureshi ZA, Hittle LE, O’Hara JA, et al. Colistin-resistant Acinetobacter baumannii: beyond carbapenem resistance. Clin Infect Dis. 2015;60(9):1295–1303. doi:10.1093/cid/civ048
5. Vázquez-López R, Solano-Gálvez SG, Juárez Vignon-Whaley JJ, et al. Acinetobacter baumannii resistance: a real challenge for clinicians. Antibiotics (Basel). 2020;9(4):205. doi:10.3390/antibiotics9040205
6. Karaiskos I, Giamarellou H. Multidrug-resistant and extensively drug-resistant gram-negative pathogens: current and emerging therapeutic approaches. Expert Opin Pharmacother. 2014;15:1351–1370. doi:10.1517/14656566.2014.914172
7. Apisarnthanarak A, Khawcharoenporn T, Mundy LM. Practices to prevent multidrug-resistant Acinetobacter baumannii and methicillin-resistant Staphylococcus aureus in Thailand: a national survey. Am J Infect Control. 2013;41:416–421. doi:10.1016/j.ajic.2012.05.011
8. Cho OH, Bak MH, Baek EH, Park KH, Kim S, Bae IG. Successful control of carbapenem-resistant Acinetobacter baumannii in a Korean university hospital: a 6-year perspective. Am J Infect Control. 2014;42(9):976–979. doi:10.1016/j.ajic.2014.05.027
9. Rodríguez-Baño J, García L, Ramírez E, et al. Long-term control of hospital-wide, endemic multidrug-resistant Acinetobacter baumannii through a comprehensive “bundle” approach. Am J Infect Control. 2009;37(9):715–722. doi:10.1016/j.ajic.2009.01.008
10. Cheon S, Kim MJ, Yun SJ, Moon JY, Kim YS. Controlling endemic multidrug-resistant Acinetobacter baumannii in Intensive Care Units using antimicrobial stewardship and infection control. Korean J Intern Med. 2016;31(2):367–374. doi:10.3904/kjim.2015.178
11. Teerawattanapong N, Kengkla K, Dilokthornsakul P, Saokaew S, Apisarnthanarak A, Chaiyakunapruk N. Prevention and control of multidrug-resistant gram-negative bacteria in adult intensive care units: a systematic review and network meta-analysis. Clin Infect Dis. 2017;64(suppl_2):S51–S60. doi:10.1093/cid/cix112
12. Moodley P, Whitelaw A. The pros, cons, and unknowns of search and destroy for carbapenem-resistant enterobacteriaceae. Curr Infect Dis Rep. 2015;17(6):483. doi:10.1007/s11908-015-0483-8
13. He S, Li Z, Yang Q, Quan M, Zhao L, Hong Z. Resistance trends among 1294 nosocomial acinetobacter baumannii strains from a tertiary general Hospital in China, 2014–2017. Clin Lab. 2020;66(3). doi:10.7754/Clin.Lab.2019.190629
14. Romanin P, Palermo RL, Cavalini JF, et al. Multidrug- and extensively drug-resistant acinetobacter baumannii in a tertiary hospital from brazil: the importance of carbapenemase encoding genes and epidemic clonal complexes in a 10-year study. Microb Drug Resist. 2019;25(9):1365–1373. doi:10.1089/mdr.2019.0002
15. Molter G, Seifert H, Mandraka F, et al. Outbreak of carbapenem resistant Acinetobacter baumannii in the intensive care unit: a multi-level strategic management approach. J Hosp Infect. 2016;92(2):194–198. doi:10.1016/j.jhin.2015.11.007
16. Ayraud-Thevenot S, Huart C, Mimoz O, et al. Control of multi-drug-resistant Acinetobacter baumannii outbreaks in an intensive care unit: feasibility and economic impact of rapid unit closure. J Hosp Infect. 2012;82(4):290–292. doi:10.1016/j.jhin.2012.08.016
17. Wilson AP, Livermore DM, Otter JA, et al. Prevention and control of multi-drug-resistant Gram-negative bacteria: recommendations from a Joint Working Party. J Hosp Infect. 2016;92(Suppl 1):S1–S44. doi:10.1016/j.jhin.2015.08.007
18. Casini B, Righi A, De Feo N, et al. Improving cleaning and disinfection of high-touch surfaces in intensive care during carbapenem-resistant acinetobacter baumannii endemo-epidemic situations. Int J Environ Res Public Health. 2018;15(10):2305. doi:10.3390/ijerph15102305
19. Li QF, Xu H, Ni XP, et al. Impact of relocation and environmental cleaning on reducing the incidence of healthcare-associated infection in NICU. World J Pediatr. 2017;13(3):217–221. doi:10.1007/s12519-017-0001-1
20. Anudit C, Kooltheat N, Potup P, Pankla Sranujit R, Usuwanthim K. Nosocomial infection of multidrug-resistant Acinetobacter baumannii in Thailand. Am J Infect Control. 2016;44(10):1161–1163. doi:10.1016/j.ajic.2016.03.068
21. Liu L, Liu B, Li Y, Zhang W. Successful control of resistance in Pseudomonas aeruginosa using antibiotic stewardship and infection control programs at a Chinese university hospital: a 6-year prospective study. Infect Drug Resist. 2018;11:637–646. doi:10.2147/IDR.S163853
22. Leclercq R, Cantón R, Brown DF, et al. EUCAST expert rules in antimicrobial susceptibility testing. Clin Microbiol Infect. 2013;19(2):141–160. doi:10.1111/j.1469-0691.2011.03703.x
23. Chang YY, Chen HP, Lin CW, et al. Implementation and outcomes of an antimicrobial stewardship program: effectiveness of education. J Chin Med Assoc. 2017;80(6):353–359. doi:10.1016/j.jcma.2016.09.012
24. Goossens H, Ferech M, Vander Stichele R, Elseviers M; Group EP. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet. 2005;365(9459):579–587. doi:10.1016/S0140-6736(05)70799-6
25. Cohen AL, Calfee D, Fridkin SK, et al. Recommendations for metrics for multidrug-resistant organisms in healthcare settings: SHEA/HICPAC position paper. Infect Control Hosp Epidemiol. 2008;29:901–913. doi:10.1086/591741
26. Borg MA. National cultural dimensions as drivers of inappropriate ambulatory care consumption of antibiotics in Europe and their relevance to awareness campaigns. J Antimicrob Chemother. 2012;67:763–767. doi:10.1093/jac/dkr541
27. Froment P, Marchandin H, Vande Perre P, Lamy B. Automated versus manual sample inoculations in routine clinical microbiology: a performance evaluation of the fully automated InoqulA instrument. J Clin Microbiol. 2014;52(3):796–802. doi:10.1128/JCM.02341-13
28. Degli Atti MC, Bernaschi P, Carletti M, et al. An outbreak of extremely drug resistant Pseudomonas aeruginosa in a tertiary care pediatric hospital in Italy. BMC Infect Dis. 2014;14:494. doi:10.1186/1471-2334-14-494
29. Zhao SY, Jiang DY, Xu PC, et al. An investigation of drug-resistant acinetobacter baumannii infections in a comprehensive hospital of East China. Ann Clin Microbiol Antimicrob. 2015;14(7). doi:10.1186/s12941-015-0066-4
30. Yuan WL, Shen YJ, Deng DY. Sex bias of Acinetobacter baumannii nosocomial infection. Am J Infect Control. 2018;46(8):957–958. doi:10.1016/j.ajic.2018.04.231
31. Lim CLL, Chua AQ, Teo JQM, Cai Y, Lee W, Kwa AL. Importance of control groups when delineating antibiotic use as a risk factor for carbapenem resistance, extreme-drug resistance, and pan-drug resistance in Acinetobacter baumannii and Pseudomonas aeruginosa: A systematic review and meta-analysis. Int J Infect Dis. 2018;76:48–57. doi:10.1016/j.ijid.2018.05.017
32. Wang CH, Li JF, Huang LY, et al. Outbreak of imipenem-resistant Acinetobacter baumannii in different wards at a regional hospital related to untrained bedside caregivers. Am J Infect Control. 2017;45(10):1086–1090. doi:10.1016/j.ajic.2017.04.016
33. MacDougall C, Polk RE. Antimicrobial stewardship programs in health care systems. Clin Microbiol Rev. 2005;18(4):638–656. doi:10.1128/CMR.18.4.638-656.2005
34. Ni W, Han Y, Zhao J, et al. Tigecycline treatment experience against multidrug-resistant Acinetobacter baumannii infections: a systematic review and meta-analysis. Int J Antimicrob Agents. 2016;47(2):107–116. doi:10.1016/j.ijantimicag.2015.11.011
35. Warde E, Davies E, Ward A. Control of a multidrug-resistant Acinetobacter baumannii outbreak. Br J Nurs. 2019;28(4):242–248. doi:10.12968/bjon.2019.28.4.242
36. Muñoz-Price LS, Carling P, Clearly T, et al. Control of a two-decade endemic situation with carbapenem-resistant Acinetobacter baumannii: electronic dissemination of a bundle of interventions. Am J Infect Control. 2014;42:466–471. doi:https://doi.org/10.1016/j.ajic.2013.12.024
37. Stalsby Lundborg C, Tamhankar AJ. Understanding and changing human behaviour–antibiotic mainstreaming as an approach to facilitate modification of provider and consumer behaviour. Ups J Med Sci. 2014;119:125–133. doi:10.3109/03009734.2014.905664
38. Sahoo KC, Tamhankar AJ, Johansson E, et al. Antibiotic use, resistance development and environmental factors: a qualitative study among healthcare professionals in Orissa, India. BMC Public Health. 2010;10:629. doi:10.1186/1471-2458-10-629
39. Hong J, Jang OJ, Bak MH, et al. Management of carbapenem-resistant Acinetobacter baumannii epidemic in an intensive care unit using multifaceted intervention strategy. Korean J Intern Med. 2018;33(5):1000–1007. doi:10.3904/kjim.2016.323
40. Aljindan R, Bukharie H, Alomar A, Abdalhamid B. Prevalence of digestive tract colonization of carbapenem-resistant Acinetobacter baumannii in hospitals in Saudi Arabia. J Med Microbiol. 2015;64(Pt 4):400–406. doi:10.1099/jmm.0.000033
41. Biswas D, Tiwari M, Tiwari V. Comparative mechanism based study on disinfectants against multidrug-resistant Acinetobacter baumannii. J Cell Biochem. 2018;119(12):10314–10326. doi:10.1002/jcb.27373
42. Bianco A, Quirino A, Giordano M, et al. Control of carbapenem-resistant Acinetobacter baumannii outbreak in an intensive care unit of a teaching hospital in Southern Italy. BMC Infect Dis. 2016;16(1):747. doi:10.1186/s12879-016-2036-7
43. Doi Y, Murray GL, Peleg AY. Acinetobacter baumannii: evolution of antimicrobial resistance-treatment options. Semin Respir Crit Care Med. 2015;36(1):85–98. doi:10.1055/s-0034-1398388
44. Cartelle Gestal M, Zurita J, Gualpa G, Gonzalez C, Paz Y, Mino A. Early detection and control of an Acinetobacter baumannii multi-resistant outbreak in a hospital in Quito, Ecuador. J Infect Dev Ctries. 2016;10(12):1294–1298. doi:10.3855/jidc.7544
45. Carlet J, Collignon P, Goldmann D, et al. Society’s failure to protect a precious resource: antibiotics. Lancet. 2011;378(9788):369–371. doi:10.1016/S0140-6736(11)60401-7
46. Zhu X, Tong A, Wang D, Sun H, Chen L, Dong M. Antibiotic resistance patterns of Gram-negative and Gram-positive strains isolated from inpatients with nosocomial infections in a tertiary hospital in Beijing, China from 2011 to 2014. J Chemother. 2016;27:1–4.
47. Karageorgopoulos DE, Falagas ME. Current control and treatment of multidrug- resistant Acinetobacter baumannii infections. Lancet Infect Dis. 2008;8:751–762. doi:10.1016/S1473-3099(08)70279-2
48. Tacconelli E, Sifakis F, Harbarth S, et al. Surveillance for control of antimicrobial resistance. Lancet Infect Dis. 2018;18(3):e99–e106. doi:10.1016/S1473-3099(17)30485-1
49. Bassetti M, Righi E, Vena A, Graziano E, Russo A, Peghin M. Risk stratification and treatment of ICU-acquired pneumonia caused by multidrug- resistant/extensively drug-resistant/pandrug-resistant bacteria. Curr Opin Crit Care. 2018;24(5):385–393. doi:10.1097/MCC.0000000000000534
50. Ben-Chetrit E, Wiener-Well Y, Lesho E, et al. An intervention to control an ICU outbreak of carbapenem-resistant Acinetobacter baumannii: long-term impact for the ICU and hospital. Crit Care. 2018;22(1):319. doi:10.1186/s13054-018-2247-y
51. Shamsizadeh Z, Nikaeen M, Nasr Esfahani B, Mirhoseini SH, Hatamzadeh M, Hassanzadeh A. Detection of antibiotic resistant Acinetobacter baumannii in various hospital environments: potential sources for transmission of Acinetobacter infections. Environ Health Prev Med. 2017;22(1):44. doi:10.1186/s12199-017-0653-4
52. Cheng VCC, Wong SC, Chen JHK, et al. Control of multidrug-resistant Acinetobacter baumannii in Hong Kong: role of environmental surveillance in communal areas after a hospital outbreak. Am J Infect Control. 2018;46(1):60–66. doi:10.1016/j.ajic.2017.07.010
53. Apisarnthanarak A, Warren DK, Fraser VJ. Creating a cohort area to limit transmission of pandrug-resistant Acinetobacter baumannii in a Thai tertiary care center. Clin Infect Dis. 2009;48:1487–1488. doi:10.1086/598512
54. Siegel JD, Rhinehart E, Jackson M, et al.; Healthcare Infection Control Practices Advisory Committee. 2007 guidelines for isolation precautions: preventing transmission of infectious agents in healthcare settings. Am J Infect Control. 2007;35(10):6490–6497. doi:10.1016/j.ajic.2007.10.007.
55. Edwards J, Patel G, Wareham DW. Low concentrations of commercial alcohol hand rubs facilitate growth of and secretion of extracellular proteins by multidrug-resistant strains of Acinetobacter baumannii. J Med Microbiol. 2007;56:1595–1599. doi:10.1099/jmm.0.47442-0
56. Gajdács M. The concept of an ideal antibiotic: implications for drug design. Molecules. 2019;24(5):892. doi:10.3390/molecules24050892
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.