Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Substance Use, Sexual Activity Prevalence, and Knowledge Gaps in Young Adults with Type 1 Diabetes in a Pediatric Clinic
Authors Waterman LA ![]() , Polsky S, Akturk HK
, Polsky S, Akturk HK ![]() , Stewart B, Karami AJ, Taylor K, Cobry EC
, Stewart B, Karami AJ, Taylor K, Cobry EC
Received 6 January 2026
Accepted for publication 11 February 2026
Published 20 February 2026 Volume 2026:19 590267
DOI https://doi.org/10.2147/DMSO.S590267
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mark D. DeBoer
Lauren A Waterman, Sarit Polsky, Halis K Akturk, Bennett Stewart, Angela J Karami, Kasserine Taylor, Erin C Cobry
Barbara Davis Center for Diabetes, University of Colorado Anschutz Medical Campus, Aurora, CO, USA
Correspondence: Lauren A Waterman, University of Colorado Anschutz Medical Campus, 1775 Aurora Court, Aurora, CO, 80045, USA, Tel +13037242323, Email [email protected]
Purpose: Substance use and sexual activity can impact the glycemic management and health of people living with type 1 diabetes (T1D), but data in pediatric populations are sparse. We set out to explore patient engagement and knowledge of the impacts on glycemia from substance use and sexual activity in a pediatric type 1 diabetes center.
Patients and methods: Surveys assessing rates and frequency of cannabis use, alcohol use, sexual activity, and participants’ knowledge of their glycemic impacts were administered to participants ≥ 18 years old with type 1 diabetes between July 2024 and May 2025 at the Barbara Davis Center for Diabetes pediatric clinic. Respondents were classified by substance use (alcohol and/or cannabis) and sexual activity. Demographic and glycemic data were obtained from electronic medical records. Student’s t-tests and chi-square tests were performed to compare between groups. Linear regression models were fit to compare HbA1c by cannabis use, adjusting for age, diabetes duration, non-Hispanic White race and ethnicity, and automated insulin delivery use.
Results: Of the 103 participants, 50 (48.5%) and 56 (54.4%) reported cannabis and alcohol use, respectively. Sexual activity was reported by 63 (61.2%) individuals. Cannabis users had a 0.8% higher HbA1c compared to non-users, even when controlling for confounders, and were less knowledgeable about its impact on glucose levels. Alcohol users were more knowledgeable about alcohol’s impacts compared to non-users, especially concerning delayed hypoglycemia. Knowledge of goal HbA1c during pregnancy was low.
Conclusion: Substance use and sexual activity are common among emerging adults with T1D, though their knowledge around the impact on diabetes is limited. Consistent and comprehensive education on these topics should begin early as part of routine diabetes care in pediatric populations. Further research into the effect of cannabis on glucose levels and diabetes care is necessary.
Keywords: cannabis, alcohol, sexual activity, emerging adults, type 1 diabetes
Introduction
Adolescence and emerging adulthood can be significantly challenging,1 especially for those living with type 1 diabetes (T1D). These periods of life include increased self-sufficiency and importance of independent diabetes management. During this time period, insulin resistance is at the highest due to pubertal hormones, yet attention to diabetes self-care is often not prioritized.2 Emerging adults with T1D also experience higher rates of mental health challenges, compared to their peers.2 These factors result in a multi-year period of higher average glucose levels, which can lead to acute and chronic complications, despite the fact that glycemic control generally improves later in adulthood. These risks are heightened for those engaging in substance use and sexual activity; both of which can have significant impacts on blood glucose and overall health.3,4
Alcohol is one of the most frequently used substances for people living with and without diabetes.5 The initial impact on glucose levels is dependent on the carbohydrate content of the alcoholic drink. However, the most significant risk of alcohol intake with diabetes is delayed hypoglycemia that can occur 4–6 hours after a person starts drinking and can last over 8 hours, depending on the amount of alcohol consumed.6 This is in part due to the liver’s focus on metabolizing ethanol into a non-toxic form, which subsequently deters its ability to perform counterregulatory mechanisms to prevent hypoglycemia. Moreover, the reduction of nicotinamide adenine dinucleotide (NAD) to NADH during alcohol metabolism results in inhibition of gluconeogenesis, which increases the risk of hypoglycemia. This can also reduce the effectiveness of emergency medications, like glucagon, to treat hypoglycemia. While the risk of significant hypoglycemia is better recognized, higher rates of alcohol consumption may also lead to increased ketosis.7 The reasons for this increased ketosis are multifactorial but include reduced diabetes self-care and increased insulin resistance.7
In addition to the high use of alcohol in the United States, a larger number of people are now using cannabis, sometimes on a daily or near daily basis.8,9 Almost half of the states, plus the District of Columbia, allow for recreational use of cannabis over the age of 21 years, with 40 states allowing medicinal cannabis for those ≥18 years old. Expanding legalization has led to a large increase in cannabis users, including in people with T1D.10 The primary modes of cannabis consumption are vaporization of cannabis concentrates, inhalation from smoking flower, and edibles. The specific effects can vary dramatically depending on the formulation, strain (indica or sativa blends), and amount consumed.11
The impact of cannabis use on diabetes is less clear, as much of the research comes from retrospective studies. Unlike alcohol where the physiological mechanisms are well-characterized, the mechanisms by which cannabis affects glycemia remain poorly understood. Much of the literature to date has described trends of hyperglycemia and increased hospitalizations in those that use cannabis. Hyperglycemia may arise from decreased diabetes self-management behaviors, particularly dosing with insufficient amounts of insulin around “the munchies” if carbohydrate snacks are consumed.4 Users may develop cannabinoid hyperemesis syndrome that can mimic symptoms of diabetic gastroparesis12,13 and can lead to emergency room visits related to hyperglycemic ketosis or retractable emesis.14 There has also been an associated increased risk of diabetic ketoacidosis (DKA) in adults with T1D with cannabis use.9 While many experience hyperglycemia with cannabis use, users may also experience hypoglycemia through increased insulin sensitivity.15–17 In addition to true hypoglycemia, the physiologic and mental effects of certain strains of cannabis can mimic perception of low symptoms, like increased heart rate, leading to inappropriate treatment.
People living with T1D engage in similar rates of sexual activity as the general population.18 However, those living with T1D face unique challenges when sexually active, particularly around glucose fluctuations related to intercourse.18 These include hyperglycemia due to adrenaline surges and hypoglycemia due to physical exertion.19 An additional challenge is that intercourse may lead to an unintended, unplanned pregnancy, which can result in a higher risk of complications to the mother and fetus when the HbA1c level is above the goal for pregnant people with T1D.20–22
Prior studies show that adolescents and young adults with T1D are engaging in risky behaviors, primarily alcohol consumption prior to the legal age and high-risk sexual intercourse.8,10 Despite the growing legality of cannabis, there has not been extensive study on the frequency and amount of use in youth and young adults with T1D. Additionally, there is a paucity of data on the knowledge base of this population around the impact of substance use and pregnancy on diabetes. These issues are not often addressed during adolescence by pediatric providers, as many people have their first sexual experience prior to counseling.19 Therefore, the objective of this study was to obtain a cross-sectional assessment of substance use, sexual activity, and knowledge surrounding these behaviors in young adults (ages 18 to 26) with T1D who receive care at a pediatric diabetes clinic.
Methods
Young adults were recruited from the Barbara Davis Center for Diabetes (BDC) pediatric clinic in Aurora, Colorado, United States, during clinic encounters between June 2024 and May 2025. Inclusion criteria were ages 18–26 years and a clinical diagnosis of T1D. The lower limit of 18 years was chosen to avoid the need for parental consent in order to increase the likelihood for truthful responses from participants, as well as being the age of legal medicinal cannabis use in Colorado. The Colorado Multiple Institutional Review Board (Aurora, Colorado) approved this study (24–0461). This study complies with the Declaration of Helsinki.
Eligible participants were approached by research staff during their routine clinical appointment. If interested, written informed consent was obtained from each participant. Less than 10% of those approached declined participation. The sample size was derived from a convenience sampling approach.
Demographics, including race/ethnicity, diabetes duration, age of participant, insurance status, most recent HbA1c, and time-in-range (70–180 mg/dL; TIR) from the most recent two weeks of continuous glucose monitoring (CGM) data, if available, were obtained from the medical record at the time of enrollment.
A substance use and sexual activity survey was administered to all participants. Questions from a previously published questionnaire on cannabis use in adults with T1D were used to assess for cannabis use.9,23 For those reporting cannabis use within the past 6 months (current cannabis use), the validated Cannabis Use Disorder Identification Test-Revised (CUDIT-R);24 was used to identify hazardous cannabis use and cannabis use disorder. In addition, current cannabis users completed questions related to the duration and frequency of use, and form of cannabis (vaporization, edible, or smoke). Questions on alcohol and sexual activity were developed following a literature review, with additional topics included after feedback from BDC endocrinologists. The survey was available in English and Spanish.
Participants were classified by substance use and sexual activity experience. Cannabis users were defined as those with current or past cannabis use of any frequency. Alcohol users were defined as those reporting current alcohol use (within the last 6 months). Those with any past or current (within the last 6 months) sexual activity were defined as sexually active. To assess topic knowledge, participants were asked to select which statements from a list of four (cannabis) and six (alcohol) were true. Topic knowledge scores were calculated by the number of true statements selected and false statements correctly left unselected. Participants also selected from multiple choice responses on what they thought the goal HbA1c was during pregnancy.
Student’s t-tests were performed to compare continuous variables (age, diabetes duration, HbA1c, and TIR) by lifetime substance use and sexual activity. Chi-square tests were performed to compare categorical variables (race/ethnicity, insurance status, sex) by lifetime substance use and sexual activity. Knowledge questions were compared using chi-square (comparisons of individual questions) and t-tests (for overall knowledge scores). Linear regression models were fit to compare HbA1c by lifetime cannabis use, adjusting for age, diabetes duration, non-Hispanic White race and ethnicity, and automated insulin delivery use.
Results
A total of 103 individuals consented to participate. Full demographics are shown in Tables 1 and 2. Participants had a mean age of 20.8 ± 1.8 years, mean diabetes duration of 10.5 ± 4.7 years, mean HbA1c 8.1% ± 1.8%, and mean TIR 57.8% ± 18.9% (N=84 with CGM data). Most participants (74.8%) were non-Hispanic White, 61.8% were assigned female at birth (AFAB), and 29.1% were on public insurance.
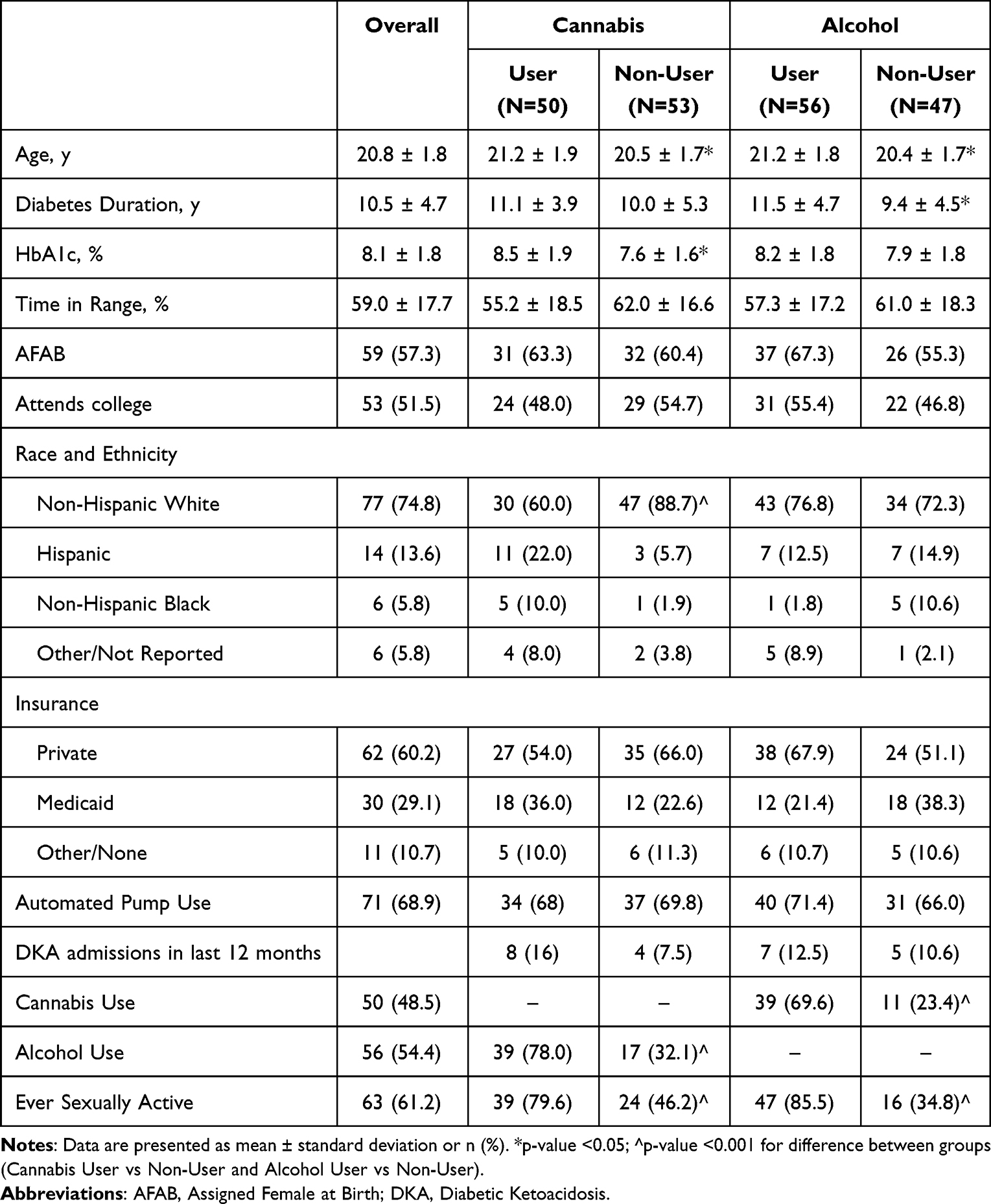 |
Table 1 Demographics Overall Sample and By Substance Use |
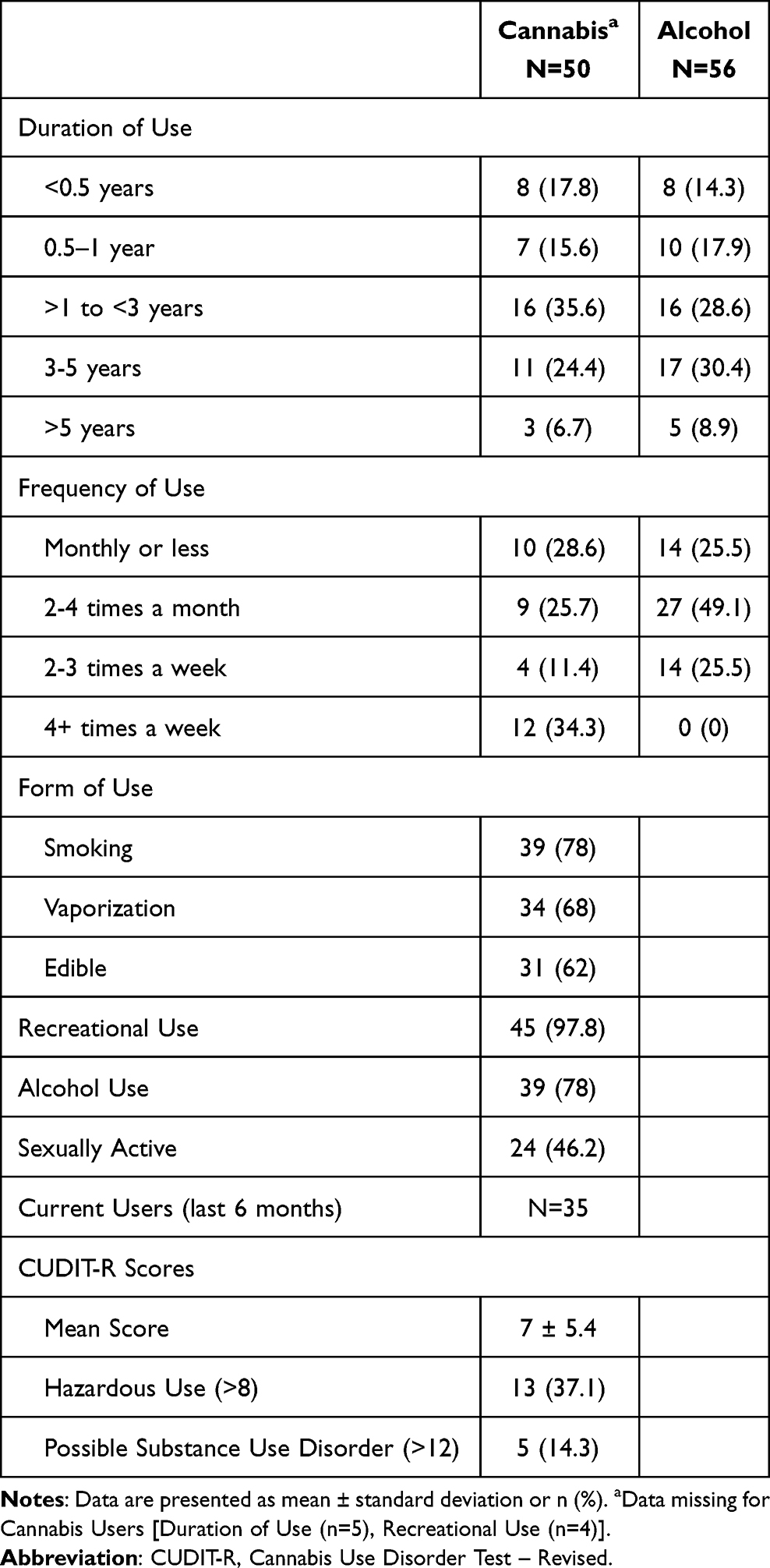 |
Table 2 Characteristics of Substance Users |
Cannabis Use
Of the 103 participants, 50 (48.5%) reported at least one instance of prior cannabis use (Table 1). Cannabis users were older compared to non-users (21.2 ± 1.9 vs 20.5 ± 1.7 years, p=0.0481), though there was no statistically significant difference in diabetes duration. Cannabis users were less likely to be non-Hispanic White (60.0% vs 88.7%, p=0.0006). Cannabis use was associated with alcohol use and sexual activity (p<0.0001 and p=0.0004, respectively), though there were no other statistically significant demographic differences.
Cannabis users had a statistically significant higher HbA1c compared to non-users (8.5% ± 1.9% vs 7.6% ± 1.6% respectively, p=0.0145) and a trend for a lower TIR (55.2% ±18.5% vs 62.0% ± 16.6%, p=0.0877). When controlling for age, diabetes duration, AID use, and being non-Hispanic white, any use of cannabis was associated with a 0.8% higher HbA1c (p=0.0210). However, there was no statistically significant difference in rates of DKA.
Characteristics of cannabis users are shown in Table 2. For the 50 individuals reporting cannabis use in the past, over 66% have been using cannabis for over 1 year, with almost half using at least weekly. Nearly all (97.8%) reported using cannabis recreationally rather than medicinally. The mean CUDIT-R score for the 35 individuals currently using cannabis was 7 ± 5.4. Thirteen (37.1%) participants met criteria for hazardous use and 5 (14.3%) met criteria for possible substance use disorders (scores ≥8 and 12, respectively).
Cannabis users had worse general cannabis knowledge compared to non-users (2.6 ± 0.9 vs 3.0 ± 1.0, p=0.0348) (Supplemental Table 1). Cannabis users were less likely to recognize the increased risk of DKA with cannabis use compared to non-users (20.0% vs 54.7%, p=0.0002), though cannabis users were more aware of the increase in blood sugars with uncovered carbohydrates during “the munchies” compared to non-users (88.0% vs 71.7%, p=−.0373) (Figure 1). Cannabis users had a trend of less recognition of the decreased blood sugar awareness with cannabis use compared to non-users (60.0% vs 77.4%, p=0.0562). See Figure 1 for further details.
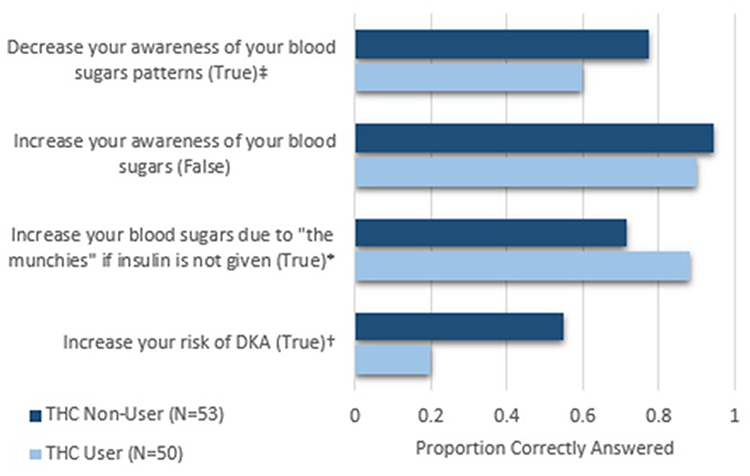 |
Figure 1 Cannabis Knowledge Questions Answered Correctly by Cannabis Use Status. *p-value <0.05; † p-value <0.001; ‡ p-value=0.0562 for difference between substance use groups. |
Cannabis users had better general alcohol knowledge compared to non-users (4.5 ± 1.2 vs 3.9 ± 1.4, p=0.0267). They were more likely to recognize the risk of delayed hypoglycemia than non-cannabis users (72.0% vs 52.8%, p=0.0439). There was no statistically significant difference in knowledge of pregnancy goal by cannabis use. See Supplemental Table 1 for additional details.
Alcohol Use
Of the 103 participants, 56 (54.4%) reported alcohol use (Table 1). Alcohol users were older than non-users (21.2 ± 1.8 vs 20.4 ± 1.7 years respectively, p=0.0381) with a longer diabetes duration (11.5 ± 4.7 vs 9.4 ± 4.5 years, respectively, p=0.0261). There were no other significant demographic differences between alcohol users and non-users, though there was a trend towards more non-users on Medicaid (28.3% vs 21.4%, p=0.0605). Alcohol use was associated with cannabis use (p<0.0001) and sexual activity (p=0.040). There were no statistically significant differences in HbA1c or TIR based on alcohol use.
Among the users of alcohol, over 67% have been using alcohol for over 1 year (Table 2). Over a quarter were using at least weekly, though no one reported using alcohol 4 or more days a week. Most were drinking 2–3 drinks per session.
Alcohol users had better general alcohol knowledge scores compared to non-users (4.6 ± 1.3 vs 3.8 ± 1.3, p=0.003) (Figure 2 and Supplemental Table 1). Alcohol users were more likely to recognize the potential for delayed hypoglycemia compared to non-users (73.2% vs 48.9%, p=0.0112). They were also more likely to recognize the decreased awareness of hypoglycemia compared to non-users (85.7% vs 68.1%, p=0.032). There was a trend toward greater recognition of the tendency of alcohol to immediately raise a person’s blood glucose level (58.9% vs 40.4%, p=0.0606).
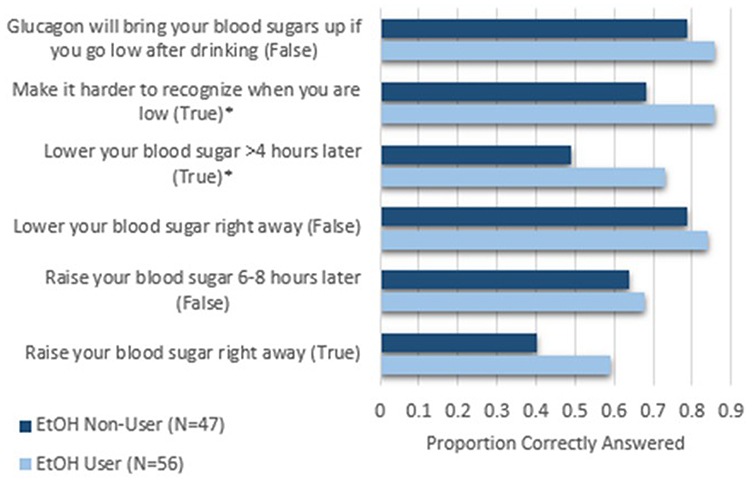 |
Figure 2 Alcohol Knowledge Questions Answered Correctly by Alcohol Use Status. *p-value <0.05 for difference between substance use groups. |
There was no significant difference in general cannabis knowledge between alcohol users and non-users. Alcohol users were more likely to recognize the goal HbA1c during pregnancy (30.4% vs 8.5%, p=0.0045) (Supplemental Table 1).
Sexual Activity
Of the 103 participants, 63 (61.2%) individuals reported at least one instance of prior sexual activity (sexually active), with 49 (47.6%) reporting sexual activity within the last 6 months (Table 3). Sexually active individuals were older than those not sexually active (21.1 ± 1.7 vs 20.3 ± 1.9 years, p=0.040). There was no significant difference in diabetes duration. A larger portion of those sexually active were assigned female at birth (AFAB) (71.0% vs 47.4%, p=0.0186). Those sexually active were more likely to report cannabis and alcohol use than those who were not (61.9% vs 26.3%, p=0.0004 and 74.6% vs 21.1%, p<0.001, respectively).
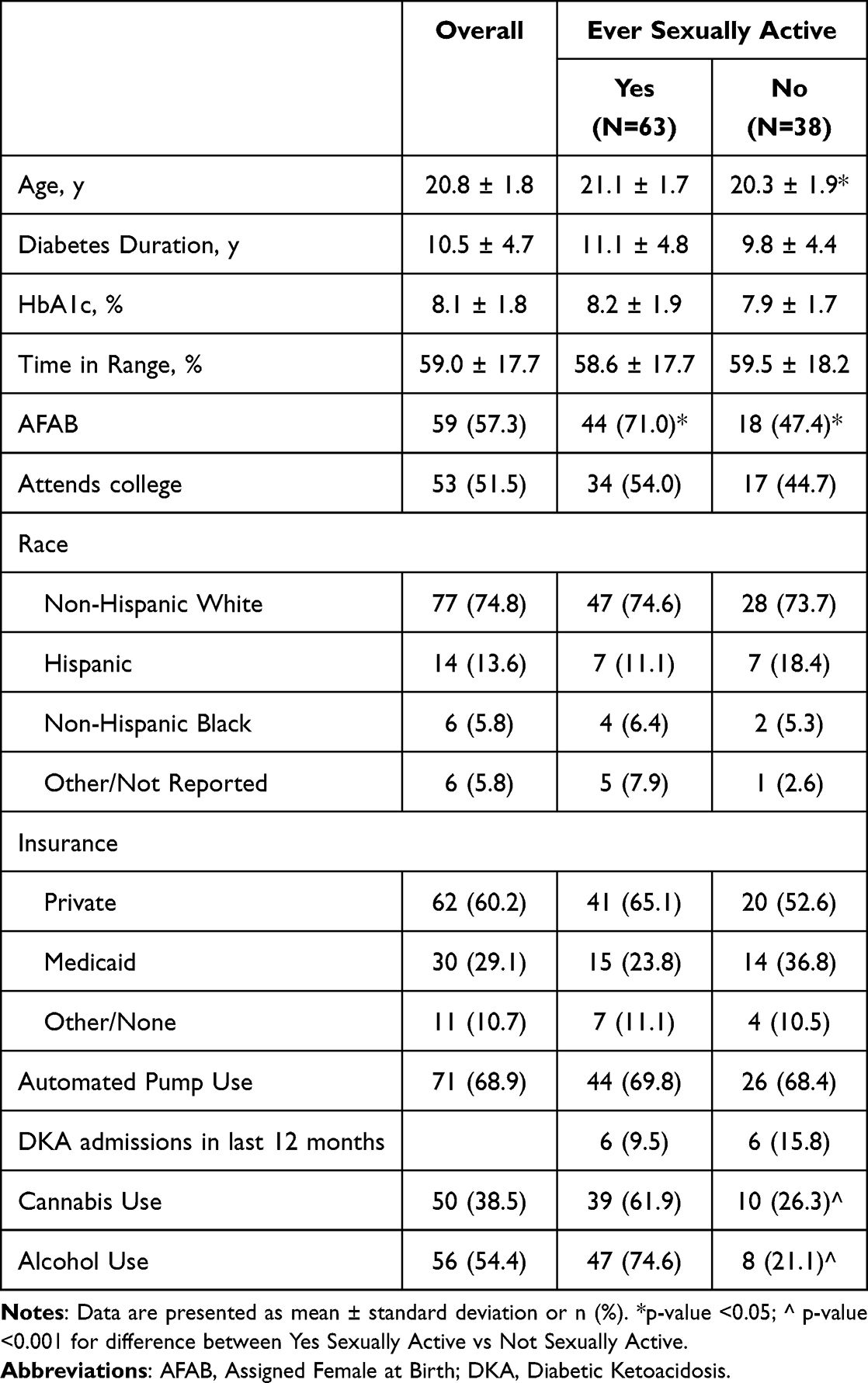 |
Table 3 Demographics by Sexual Activity |
For the 63 sexually active individuals, 69.8% began prior to the age of 18 years of age, with the majority beginning between 14–18 years old (Table 4). The majority of sexually active individuals had between 1–3 lifetime partners. Contraception was used by 79.4% of sexually active individuals or their partners, with the majority using condoms. Around a third of AFAB reported using an intrauterine device (IUD) or implant.
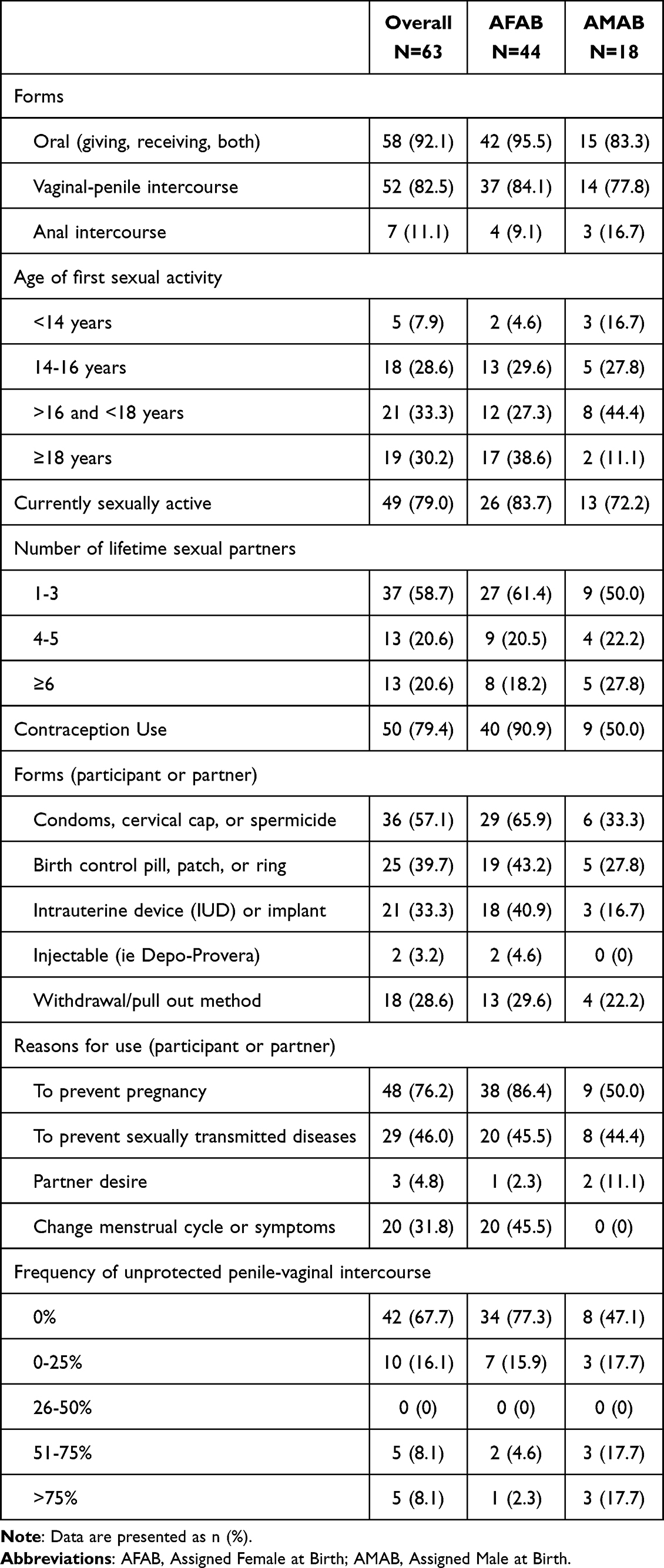 |
Table 4 Sexual Activity and Contraception Use by Gender Assigned at Birth |
There was no statistically significant difference on knowledge of goal HbA1c during pregnancy by sexual activity. However, there was a difference based on the sex assigned at birth with AFAB individuals more likely to recognize goal HbA1c compared to those assigned male at birth (30.2% vs 0.5%, p=0.001). However, across the general population, the majority selected “Don’t Know”. Those engaged in sexual activity had better general alcohol knowledge compared to those not sexually active (4.5 ± 1.2 vs 3.7 ± 1.4, p=0.0018). There was not significant difference in cannabis knowledge scores. See Supplemental Table 1 for additional details.
Discussion
Substance use and sexual activity are common in emerging adults with T1D receiving care at a pediatric diabetes clinic. The majority of participants reported alcohol use and sexual activity, with almost half reporting past or current cannabis use. Cannabis users had higher HbA1c levels compared to non-users, even when controlling for possible confounders, and a trend toward lower TIR. However, it is unclear whether this relationship is primarily mediated by impaired self-management behaviors or if physiological interactions may contribute. While alcohol use was common in this population, there were no differences in glycemic outcomes when comparing those using alcohol and those not using alcohol.
There were significant substance use knowledge gaps. In particular, cannabis users were less aware of the increased risk of diabetic ketoacidosis and the decreased glycemic awareness that can occur with cannabis use compared to non-users. However, users of any substance were more knowledgeable about alcohol’s impact, particularly the risk of delayed hypoglycemia. The differences in knowledge gaps between substances are likely due to the differences in the severity and frequency of the risks of alcohol and cannabis use, as well as the large overlap between cannabis and alcohol users. As delayed hypoglycemia can frequently occur with even moderate alcohol use, users are more likely to encounter this phenomenon once they start consuming alcohol regularly, though they may not understand the reason. In contrast, the increased risk of DKA with cannabis use is not as well established and may not be as noticeable at an individual level. In this study, there was a trend towards more DKA admissions in the cannabis group that was not statistically significant, although the sample size of DKA admissions decreased the power to detect differences between groups.
Across the entire sample, there was a lack of knowledge related to the goal HbA1c during pregnancy. While those capable of becoming pregnant were more likely to answer correctly, over half answered “Don’t Know” to the question. As many have been sexually active for years, this dearth of knowledge could have significant impacts on the health of the person and fetus if they were to become pregnant with an elevated HbA1c. More consistent education around pregnancy and T1D, as well as discussions around effective contraception options, are necessary. It is imperative that this is addressed starting within the pediatric clinic and not waiting until after transitioning to an adult provider. Sexual activity is commonly occurring during adolescence and young adulthood, when many patients are still receiving their diabetes care in pediatric practices.
Limitations
Although this study provides a look at substance use and sexual activity in emerging adults with T1D, there are some limitations. Substance use and sexual activity data were obtained through self-report, which may introduce bias, especially for those that were not comfortable reporting substance use and sexual activity. Participants were limited to those ≥18 years old to avoid the need for parental consent, thus data for younger adolescents were not obtained. As alcohol and cannabis use are still illegal for those <21 years old, there may have been some underestimation of substance use in individuals 18–20 years old. Despite the possibility of underreporting, this study still found a large percentage of patients willing to acknowledge their use. Additionally, while the CUDIT-R is a validated survey, the majority of information was not obtained through a validated questionnaire.
Certain metrics, like TIR, did not reach the level of statistical significance, though they may be clinically significant. This lack of statistical significance may be due to insufficient sample size. Additionally, further evaluation by substance use subgroup may provide additional insight when trying to isolate the effect of each substance. While the sample size of this study did not allow for this analysis, this may be a future area of research.
Additionally, as this occurred at a clinic located in Colorado, this study’s findings may not be applicable to clinics in states that have not legalized cannabis use. However, many participants in this sample began cannabis use before the age of 21 years old, which is the legal age of recreational use in Colorado and other states. This indicates that most were obtaining it through illegal channels. Several active cannabis users were also attending universities in states without legal recreational use.
Conclusion
Substance use and sexual activity are common among emerging adults with T1D, though their accurate knowledge around the impact on diabetes is limited. As many begin experimenting as adolescents, consistent and comprehensive education on these topics should begin in early high school as part of routine diabetes care in pediatric diabetes clinics. Additionally, those using cannabis have higher HbA1c levels compared to those that do not, though the etiology of this is unclear at this time. Further research into the effect of cannabis use on glucose levels and diabetes care, as well as identification of optimal timing of early educational interventions, is necessary.
Prior Presentation
Material from this study was presented at the American Diabetes Association Scientific Sessions in Chicago, Illinois in June 2025 and International Society of Pediatric and Adolescent Diabetes Annual Conference in November 2025.
Data Sharing Statement
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research supporting data is not available.
Author Contributions
Lauren A. Waterman: Conceptualization, methodology, investigation, supervision, data curation, formal analysis, writing – original draft. Erin C. Cobry: Conceptualization, methodology, supervision, writing – review and editing. Halis K. Akturk: Conceptualization, methodology, writing – review and editing. Sarit Polsky: Conceptualization, methodology, writing – review and editing. Angela J. Karami: Investigation, writing – review and editing. Kasserine Taylor: Investigation, writing – review and editing. Bennett Stewart: Investigation, writing – review and editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. L.A.W. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
This work was funded by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases (grant no. 5T32DK063687).
Disclosure
E.C.C. conducts research through the University of Colorado with Abbott Diabetes, Beta Bionics, Dexcom, Eli Lilly, Insulet, Luna Health, Medtronic MinMed, Sequel Med Tech, and Tandem Diabetes Care; has been a speaker and on an advisory board for Dexcom. S.P. was a contributing writer for diaTribe; was on an advisory board for Medtronic; has received research funding and/or support from Dexcom, Breakthrough T1D, Eli Lilly, JDRF, the Leona & Harry Helmsley Charitable Trust, the National Institute for Diabetes and Digestive and Kidney Diseases, Diasome Pharmaceuticals, Medtronic MiniMed, and Sanofi US Services; has received honoraria from the Children’s Diabetes Foundation, the American Diabetes Association, AACE and Keck School of Medicine; has received conference fees from American Diabetes Association, AACE, Keck School of Medicine, American College of Diabetology and Insulet; and was a Professional Practice Committee member for the American Diabetes Association Standards of Care 2024 and 2025. The authors report no other conflicts of interest.
References
1. Arnett JJ. Emerging adulthood. A theory of development from the late teens through the twenties. Am Psychol. 2000;55(5):469–12. doi:10.1037/0003-066X.55.5.469
2. McCoy RG, Kidney RSM, Holznagel D, Peters T, Madzura V. Challenges for younger adults with diabetes. Minn Med. 2019;102(2):34–36. doi:10.2337/dc19-S002
3. Pastor A, O’Brien CL, Teng J, et al. Experiences of young adults with type 1 diabetes while using alcohol and recreational drugs: an interpretative phenomenological analysis (IPA) of semi-structured interviews. Diabet Res Clin Pract. 2018;141:47–55. doi:10.1016/j.diabres.2018.04.029
4. Pastor A, Conn J, Teng J, et al. Alcohol and recreational drug use in young adults with type 1 diabetes. Diabet Res Clin Pract. 2017;130:186–195. doi:10.1016/j.diabres.2017.05.026
5. Potter K, Luca P, Pacaud D, et al. Prevalence of alcohol, tobacco, cannabis and other illicit substance use in a population of Canadian adolescents with type 1 diabetes compared to a general adolescent population. Paediatr Child Health. 2018;23(3):185–190. doi:10.1093/pch/pxx157
6. Sergel-Stringer OT, Al-Sallami HS, Styles SE, Boucsein A, de Bock MI, Wheeler BJ. Knowledge, safety, and impact of alcohol consumption in young adults with type 1 diabetes mellitus: a qualitative study. BMC Endocr Disord. 2023;23(1):229. doi:10.1186/s12902-023-01471-7
7. White ND. Alcohol use in young adults with type 1 diabetes mellitus. Am J Lifestyle Med. 2017;11(6):433–435. doi:10.1177/1559827617722137
8. Caulkins JP. Changes in self-reported cannabis use in the United States from 1979 to 2022. Addiction. 2024;119(9):1648–1652. doi:10.1111/add.16519
9. Kinney GL, Akturk HK, Taylor DD, Foster NC, Shah VN. Cannabis use is associated with increased risk for diabetic ketoacidosis in adults with type 1 diabetes: findings from the T1D exchange clinic registry. Diabetes Care. 2020;43(1):247–249. doi:10.2337/dc19-0365
10. Sannegowda R, Villalba K, Suk R, Gurnurkar S, Wasserman RM. Recent rates of substance use among adolescents and young adults with type 1 diabetes in the USA. Curr Diab Rep. 2023;23(1):1–17. doi:10.1007/s11892-022-01496-7
11. Pancer J, Dasgupta K. Effects of cannabis use in youth and young adults with type 1 diabetes: the highs, the lows, the don’t knows. Can J Diabetes. 2020;44(2):121–127. doi:10.1016/j.jcjd.2019.05.001
12. Akturk HK, Mason E, Snell-Bergeon J, Shah VN, Karakus KE. Differentiating diabetic gastroparesis and cannabis hyperemesis syndrome in people with type 1 diabetes. Clin Diabetes. 2025;43(3):416–419. doi:10.2337/cd24-0096
13. Karakus KE, Akturk HK. Cannabis hyperemesis syndrome can mimic diabetic gastroparesis in cannabis users with type 1 diabetes. Can J Diabetes. 2025;49(3):218–219. doi:10.1016/j.jcjd.2025.02.004
14. Akturk HK, Snell-Bergeon J, Kinney GL, Champakanath A, Monte A, Shah VN. Differentiating diabetic ketoacidosis and hyperglycemic ketosis due to cannabis hyperemesis syndrome in adults with type 1 diabetes. Diabetes Care. 2022;45(2):481–483. doi:10.2337/dc21-1730
15. Ghasemi-Gojani E, Kovalchuk I, Kovalchuk O. Cannabinoids and terpenes for diabetes mellitus and its complications: from mechanisms to new therapies. Trends Endocrinol Metab. 2022;33(12):828–849. doi:10.1016/j.tem.2022.08.003
16. VanderVeen BN, Cardaci TD, Unger CA, et al. Cannabis improves metabolic dysfunction and macrophage signatures in obese mice. Am J Physiol Cell Physiol. 2025;329(4):C1316–C1331. doi:10.1152/ajpcell.00503.2025
17. Penner EA, Buettner H, Mittleman MA. The impact of marijuana use on glucose, insulin, and insulin resistance among US adults. Am J Med. 2013;126(7):583–589. doi:10.1016/j.amjmed.2013.03.002
18. Charron-Prochownik D, Sereika SM, Falsetti D, et al. Knowledge, attitudes and behaviors related to sexuality and family planning in adolescent women with and without diabetes. Pediatr Diabetes. 2006;7(5):267–273. doi:10.1111/j.1399-5448.2006.00197.x
19. Pinhas-Hamiel O, Tisch E, Levek N, et al. Sexual lifestyle among young adults with type 1 diabetes. Diabetes Metab Res Rev. 2017;33(2). doi:10.1002/dmrr.2837
20. McCance DR, Casey C. Type 1 diabetes in pregnancy. Endocrinol Metab Clin North Am. 2019;48(3):495–509. doi:10.1016/j.ecl.2019.05.008
21. Bamehrez M. Hypoglycemia and associated comorbidities among newborns of mothers with diabetes in an academic tertiary care center. Front Pediatr. 2023;11:1267248. doi:10.3389/fped.2023.1267248
22. Gabbay-Benziv R, Reece EA, Wang F, Yang P. Birth defects in pregestational diabetes: defect range, glycemic threshold and pathogenesis. World J Diabetes. 2015;6(3):481–488. doi:10.4239/wjd.v6.i3.481
23. Akturk HK, Taylor DD, Camsari UM, Rewers A, Kinney GL, Shah VN. Association between cannabis use and risk for diabetic ketoacidosis in adults with type 1 diabetes. JAMA Intern Med. 2019;179(1):115–118. doi:10.1001/jamainternmed.2018.5142
24. Mezquita L, Bravo AJ, Pilatti A, Ortet G, Ibanez MI; Cross-Cultural Addictions Study T. Quantifying cannabis problems among college students from English and Spanish speaking countries: cross-cultural validation of the cannabis use disorders identification test-revised (CUDIT-R). Addict Behav. 2022;127:107209. doi:10.1016/j.addbeh.2021.107209
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence and Treatment of Substance Misuse in Older Adults: Beyond Early Adulthood
Hu J, Kulkarni N, Maliha P, Grossberg G
Substance Abuse and Rehabilitation 2024, 15:87-98
Published Date: 12 July 2024