Back to Journals » Journal of Pain Research » Volume 15
Sublingual Sufentanil versus Standard-of-Care (Patient-Controlled Analgesia with Epidural Ropivacaine/Sufentanil or Intravenous Morphine) for Postoperative Pain Following Pancreatoduodenectomy: A Randomized Trial
Authors Groen JV ![]() , Boon SC, Minderhoud MW, Bonsing BA, Martini CH, Putter H, Vahrmeijer AL, van Velzen M
, Boon SC, Minderhoud MW, Bonsing BA, Martini CH, Putter H, Vahrmeijer AL, van Velzen M ![]() , Vuijk J, Mieog JSD, Dahan A
, Vuijk J, Mieog JSD, Dahan A ![]()
Received 22 February 2022
Accepted for publication 17 June 2022
Published 22 June 2022 Volume 2022:15 Pages 1775—1786
DOI https://doi.org/10.2147/JPR.S363545
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jinlei Li
Jesse Vincent Groen,1 SC Boon,2 MW Minderhoud,2 Bert A Bonsing,1 CH Martini,2 H Putter,3 AL Vahrmeijer,1 Monique van Velzen,2 J Vuijk,2 JSD Mieog,1,* A Dahan2,*
1Department of Surgery, Leiden University Medical Center, Leiden, The Netherlands; 2Department of Anesthesiology, Leiden University Medical Center, Leiden, The Netherlands; 3Department of Medical Statistics, Leiden University Medical Center, Leiden, The Netherlands
*These authors contributed equally to this work
Correspondence: A Dahan, Department of Anesthesiology, Leiden University Medical Center, Albinusdreef 2, Leiden, 2300 RC, The Netherlands, Tel +31 71 526 2301, Email [email protected]
Background: The optimal treatment strategy for postoperative pain following pancreatoduodenectomy remains unknown. The aim of this study was to investigate whether sublingual sufentanil tablet (SST) is a non-inferior analgesic compared to our standard-of-care (patient-controlled epidural analgesia [PCEA] or PCA morphine) in the treatment of pain following pancreatoduodenectomy.
Methods: This was a pragmatic, strategy, open-label, non-inferiority, parallel group, randomized (1:1) trial. The primary outcome was an overall mean pain score (Numerical Rating Scale: 0– 10) on postoperative days 1 to 3 combined. The non-inferiority margin was − 1.5 since this difference was considered clinically relevant.
Results: Between October 2018 and July 2021, 190 patients were assessed for eligibility and 36 patients were included in the final analysis: 17 patients were randomized to SST and 19 patients to standard-of-care. Early treatment failure in the SST group occurred in 2 patients (12%) due to inability to operate the SST system and in 2 patients (12%) due to severe nausea despite antiemetics. Early treatment failure in the standard-of-care group occurred in 2 patients (11%) due to preoperative PCEA placement failure and in 1 patient (5%) due to hemodynamic instability caused by PCEA. The mean difference in pain score on postoperative day 1 to 3 was − 0.10 (95% CI − 0.72– 0.52), and therefore the non-inferiority of SST compared to standard-of-care was demonstrated. The mean pain score, number of patients reporting unacceptable pain (pain score > 4), Overall Benefit of Analgesia Score, and patient satisfaction per postoperative day, perioperative hemodynamics and postoperative outcomes did not differ significantly between groups.
Conclusion: This first randomized study investigating the use of SST in 36 patients following pancreatoduodenectomy showed that SST is non-inferior compared to our standard-of-care in the treatment of pain on postoperative days 1 to 3. Future research is needed to confirm that these findings are applicable to other settings.
Keywords: postoperative pain, pancreatoduodenectomy, sufentanil, epidural analgesia, morphine
Introduction
Epidural analgesia (EA) is the gold standard for perioperative analgesic management in most major open abdominal surgeries.1 Recently, we performed a systematic review of the various analgesic treatment strategies after pancreatoduodenectomy in our own center2 and in the current literature.3 The reported use of EA in patients undergoing pancreatoduodenectomy varies from 9% to 85%.3 The potential benefits of EA are lower pain scores in the first postoperative days and fewer postoperative (pulmonary) complications.2,3 The disadvantages of EA are the invasive nature, early failure rates, hemodynamic instability and notorious, albeit uncommon, complications (eg spinal hematoma and epidural infections).2–6 The most used alternative to EA is intravenous (iv) morphine.1–3,7_ENREF_3 The advantages of iv morphine are that most patients are eligible (eg patients with coagulation disorders or spine anatomy alterations) and that it is a less invasive method compared to EA. The disadvantages of iv morphine are the suboptimal pain control and a higher consumption of opioids compared to EA with associated side effects.2,3,8 The anesthesia and surgical teams at our center recently concluded that our standard-of-care treatment strategies following pancreatoduodenectomy were currently not comprehensive, and hence alternatives are explored.
Among the available alternatives for EA and iv morphine is sublingual sufentanil tablets (SST). _ENREF_9 SST consists of a patient-controlled non-invasive hand-held device that delivers 15 µg sufentanil micro-tablets with a 20 min lockout time. The advantages of SST are as follows: (1) it is a non-invasive method of analgesia; (2) sufentanil is highly lipophilic and is rapidly absorbed after which it passes the blood–brain barrier within minutes (t½ ke0 or blood-effect-site equilibration half-life about 6 min); (3) Due to the sublingual formulation peak concentrations are relatively low and consequently, concentration dependent side effects – such as acute respiratory depression – do not occur; and (4) Due to its rapid onset of action, there is little delay in pain relief between the moment of administration and the onset of pain reduction. The disadvantages of SST are the inability to set a background infusion and the ability to operate the SST system.9 SST showed adequate pain control in earlier randomized studies in abdominal and orthopedic surgery, and in a recent retrospective cohort analysis of nearly 300 of our patients after laparoscopic abdominal and orthopedic surgery, we observed low average pain scores (75% of patients with a pain score ≤4 on the first postoperative day).10–13_ENREF_10 Nevertheless, no studies are available which investigated the use of SST in patients undergoing pancreatoduodenectomy.3
The PROSPECT group states that there might be shortcomings when using general analgesic guidelines for choosing the optimal treatment strategy for postoperative pain following a specific surgical procedure.14 Therefore, this study compares treatment strategies (rather than medication per se) and investigates whether SST is a non-inferior analgesic compared to our standard-of-care strategy (patient controlled analgesia with EA (PCEA) or patient controlled analgesia with iv morphine (PCA morphine)) in the treatment of postoperative pain following pancreatoduodenectomy.
Methods
Study Design and Participants
This was a pragmatic, strategy, open-label, non-inferiority, parallel group, randomized trial in a single center according to the CONSORT guidelines.15 Inclusion criteria were as follows: American Society of Anesthesiologists scores 1 to 3; age ≥18 years; elective pancreatoduodenectomy (eg open or robot-assisted procedures). Exclusion criteria were: unable to give written informed consent; contra-indication for SST, PCEA or PCA morphine such as allergies or coagulopathies; presumed inability to operate the SST or standard-of-care; opioid use >12 weeks; complex chronic pain disorders; liver failure (Child Pugh class C). Patients received information regarding the study preoperatively at the outpatient clinic or by phone. All included patients signed an informed consent form prior to study-related activities. The original protocol and two amendments (also including robot-assisted procedures and changing the non-inferiority margin) were approved by the Medical Ethical Committee (P18.061) and the Board of Directors of the Leiden University Medical Center. The Data Monitoring Committee was deemed unnecessary. The full study protocol was registered at the Netherlands Trial Register (NTR7318; www.trialregister.nl) and is available in Supplementary Files.
Randomization and Blinding
Patients were randomized (1:1) within the electronic data capture system CASTOR (www.castoredc.com), stratified by procedure type (open or robot-assisted; to ensure equal distribution in both groups of the study) and with varying block sizes (4, 6, 8). Patients randomized to standard-of-care received PCEA or PCA morphine at discretion of the attending anesthesiologist and were mainly dependent on procedural type: PCEA for open, PCA morphine for robot-assisted procedures. Blinding between study participants and investigators was not done since the treatment strategies were evidently different.
Treatment Strategies
Sst
Patients randomized to SST received iv sufentanil during surgery and long-acting iv opioids, such as morphine, 45–60 min prior to the end of surgery. In the Post Anesthesia Care Unit (PACU), pain scores were assessed using an 11-point Numerical Rating Scale (NRS; from 0, no pain to 10, most extreme pain imaginable). If needed, patients received 2 mg iv morphine bolus doses to reduce pain scores ≤4, only when pain scores were ≤4 and patients were able to operate the SST system, the SST system was started. The SST system consists of a patient-controlled non-invasive hand-held device that delivers 15 µg sufentanil micro-tablets for sublingual use at a 20 min interval (lockout). A unique adhesive tag on the patients’ thumb can activate the device by radio-frequency. The device is fixed to the patients’ bed and contains a cartridge with 40 micro-tablets. The Acute Pain Service can manage the SST system with a specific card (remove/replace cartridges, link the thumb tag to the device, etc.).
Standard-of-Care
Patients in the PCEA group received patient-controlled epidural analgesia. The PCEA catheter was inserted preoperatively at level Th6-Th10. Following induction of anesthesia, a 6–12 mL bolus containing ropivacaine 0.75% was administered epidurally, followed by a continuous infusion of a mixture of ropivacaine 0.2% and sufentanil 0.75 µg/mL, at 6–10 mL/h; with the possibility of giving an additional bolus. During surgery, patients received additional iv sufentanil if deemed necessary by the attending anesthesiologist. At the PACU, pain scores were assessed at regular intervals and the level of the epidural blockade was tested with an ice pack. In case of pain score >4, 2 mL boluses at a 20 min interval (lockout) from the PCEA system were permitted. In case of failure to place the epidural catheter preoperatively, patients received PCA morphine according to the PCA morphine protocol.
Patients with PCA morphine received patient-controlled iv morphine. These patients received 0.1–0.2 mg/kg iv morphine 45–60 min prior to the end of surgery. During surgery, patients received iv sufentanil if deemed necessary by the attending anesthesiologist. At the PACU, pain scores were assessed at regular intervals. If needed, initially, patients received 2 mg iv morphine bolus doses to reduce pain scores ≤4; thereafter, the PCA morphine device was started. A background infusion of 0.5 mg morphine per h was administered. Patient could additionally administer a 1 mg bolus at a 5-min interval (lockout) with a maximum dosage of 28 mg per 4 hours.
Perioperative Care
The full study protocol describes the pre, peri and postoperative care in detail and is available in the Supplementary Files. All patients received paracetamol 1000 mg 4 times daily and if needed metamizole 1000 mg 3 times daily. In case of insufficient pain treatment (persistent pain scores >4) during the course of treatment, patients could receive rescue pain medication at discretion of the attending anesthesiologist, ie such as conversion to another of the mentioned techniques. If this did not help, iv ketamine could be added (up to 10 mg/h). On postoperative day 3, both the SST system and the standard-of-care were terminated and replaced by paracetamol and oral or subcutaneous (sc) opioids, although both the SST system and the standard-of-care could be prolonged until maximum postoperative day 6 at the discretion of the attending anesthesiologist.
Outcomes and Comparisons
There was a single primary outcome, which was the overall mean pain score on postoperative days 1 to 3 combined. The non-inferiority margin was set at −1.5 since a difference greater than −1.5 points was considered to be clinically relevant.16 Secondary outcomes included mean pain score and patients reporting unacceptable pain per postoperative day, Overall Benefit of Analgesia Score (OBAS)17 and patient satisfaction score on postoperative day 1 to 3 combined and per postoperative day. Additional secondary outcomes were early treatment failure, perioperative hemodynamics (occurrence of hypotension, use and dosage of vasopressors, postoperative fluid balances) and several additional postoperative outcomes (complications related to analgesia, day of resumption of oral diet intake and day of urinary catheter removal, Clavien-Dindo classification,18 mortality within 30 days, length of hospital stay, readmission).
Outcomes were compared by intention-to-treat analysis (SST versus standard-of-care). Predefined subgroup analyses of pain scores were performed using the intended procedure type (open and robot-assisted procedure) and the protocol version (original and amended protocol). To investigate if older patients had the ability to operate the SST system and achieve adequate pain control, post-hoc subgroup analyses of pain scores were performed by age subgroups of ≤65 and >65 years.
Data Collection and Definitions
Pain scores were assessed on an 11-point NRS ranging from 0 (no pain) to 10 (most extreme pain imaginable). Pain scores were assessed by the Acute Pain Service (a dedicated and specialized team of nurses and anesthesiologists who visit the patient twice daily and who are responsible for [early] postoperative pain treatment) or nursing staff at least 3 times daily according to local and national protocol.19,20 Several training sessions were organized before and during the trial to ensure standardized assessment of pain scores. The OBAS was measured by the Acute Pain Service on the morning on postoperative days 1 to 3. The OBAS is a composite score of pain scores, side-effects, and patient satisfaction, ranging from 0 to 28, in which a lower score is superior to higher scores.17 Patient satisfaction scores were recorded by the patients themselves at the end of each hospital day (11-point NRS ranging from 0 [not satisfied at all]) to 10 [fully satisfied]). Additional data were collected from the electronic medical records. The day of surgery was considered as postoperative day 0. Perioperative hypotension was defined as a mean arterial pressure <55 mmHg. Unacceptable pain was defined as a reported pain score >4. Early treatment failure was defined as ending the use of the SST system or termination of standard-of-care before postoperative day 3 due to problems, such as preoperative placement failure, inadequate pain control, hemodynamic instability, or side effects impeding further treatment. The Clavien-Dindo classification was used to score overall postoperative complications.18
Sample Size and Statistical Analysis
Based on a non-inferiority margin of −1.5 for the primary outcome (overall mean pain score for postoperative day 1 to 3 combined), 36 patients were required to be 90% certain that the lower limit of the 95% confidence interval was above the non-inferiority limit (PASS Software version 15.0.4). The primary outcome was tested at the p-value <0.05 level for significance. Mean differences were reported with 95% confidence intervals. In case the confidence interval was included in the inferiority limit, non-inferiority was considered demonstrated. Further analysis compared groups using independent samples t-test or Mann–Whitney test, depending on their distribution, for continuous variables. Chi-square test and Fisher’s exact tests were used for categorical variables. Statistical analyses were performed using the SPSS statistical software package version 26.
Results
Baseline Characteristics
Between October 2018 and July 2021, 190 patients were assessed for eligibility of which 38 patients were included (Figure 1). The main reasons for exclusion were temporary stop of study activities in our institution during the peak of the COVID pandemic (n = 40) and logistics (n = 38). Randomization allocated 19 patients in the SST group and 19 patients in the standard-of-care group. Two patients in the SST group were excluded (exclusion criterium found after randomization [n = 1] and no resection being performed [n = 1]) and therefore 36 patients were included in the final analyses.
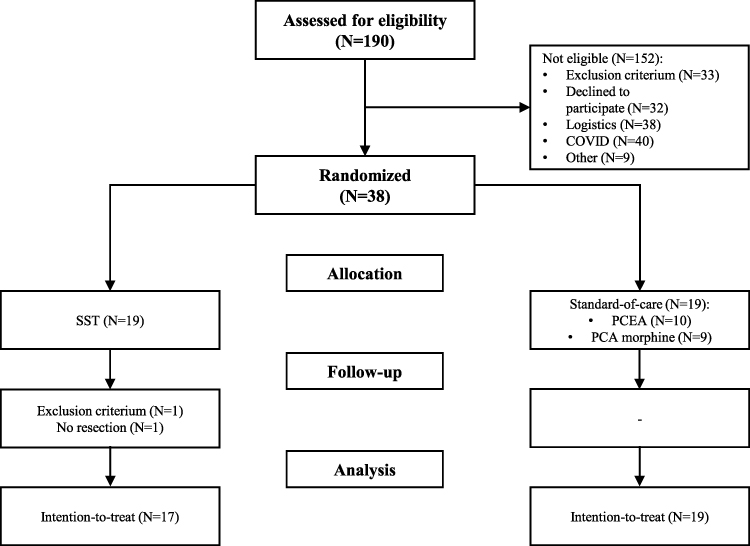 |
Figure 1 Flow chart of inclusion. |
Baseline characteristics did not differ between the two groups (Table 1). In the SST group, 10 patients (59%) underwent an open procedure, 5 patients (30%) underwent a robot-assisted procedure and 2 (12%) underwent a robot-assisted procedure converted to an open procedure, compared to 11 (58%), 7 (37%) and 1 patients (5%) in the standard-of-care group, respectively (p = 0.739).
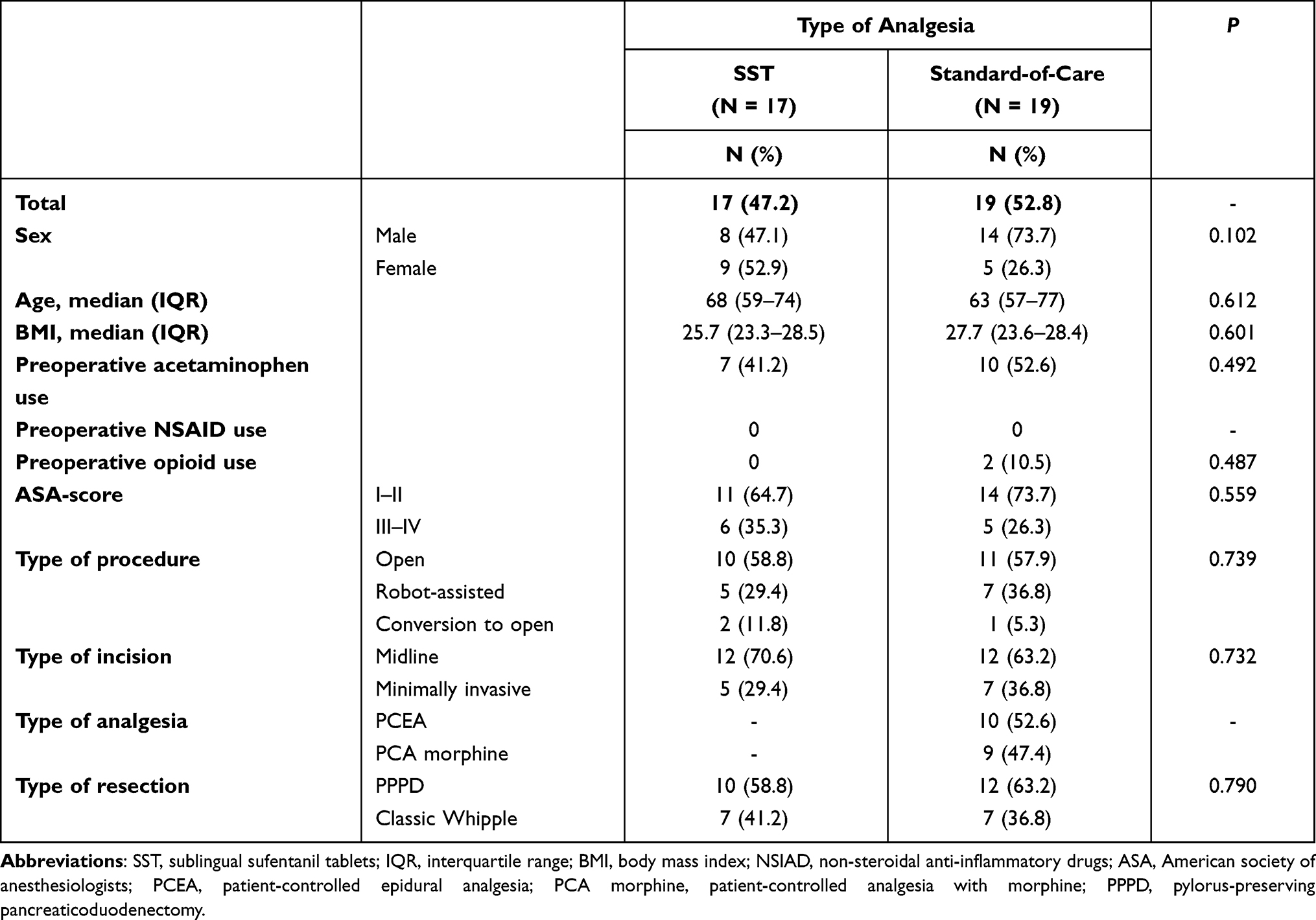 |
Table 1 Baseline Characteristics |
In the SST group, early treatment failure occurred in 2 patients (12%) due to the inability to operate the SST system and in 2 other patients (12%) due to severe nausea despite antiemetic treatment (Figure 2). In the standard-of-care group, 10 patients were intended for PCEA and 9 patients were intended for PCA morphine. Early treatment failure occurred in 2 patients (11%) due to preoperative placement failure of PCEA and in 1 patient (5%) due to hemodynamic instability caused by the PCEA. The rate of early treatment failure did not differ between the groups (p = 0.558).
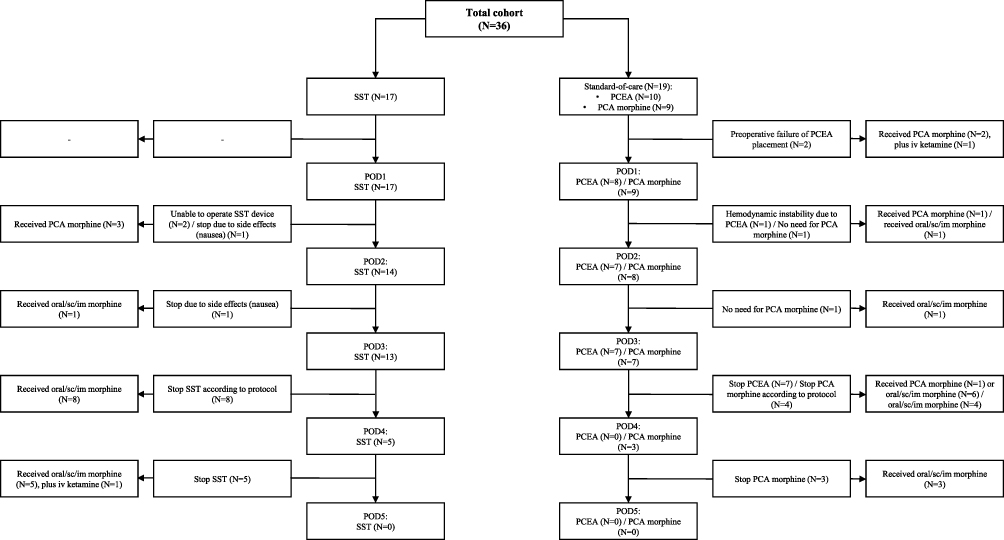 |
Figure 2 Flow chart of the use of SST and standard-of-care per postoperative day. |
Primary Outcome
The mean (SD) pain score on postoperative days 1 to 3 was 2.24 (1.00) in the SST group and 2.24 (0.77) in the standard-of-care group. The mean difference was −0.10 (95% CI −0.72–0.52) (Table 2). The lower limit of the 95% CI was higher than the predefined limit for non-inferiority (−1.5), and therefore the non-inferiority of SST compared to standard-of-care was demonstrated.
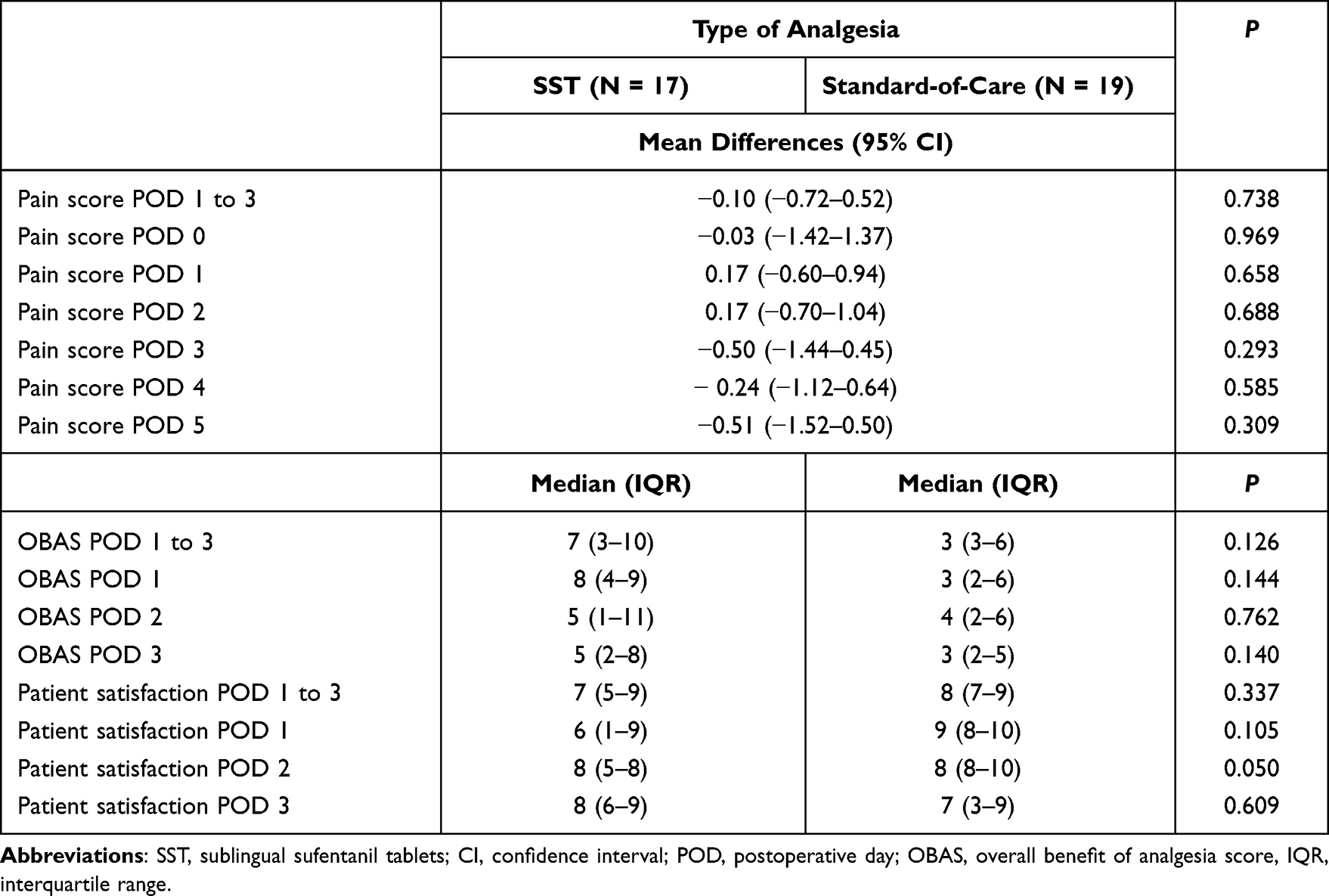 |
Table 2 Mean Difference in Pain Scores, Overall Benefit of Analgesia Score (OBAS) and Patient Satisfaction Scores per Postoperative Day |
Secondary Outcomes
Pain Scores
The mean pain score and patients reporting unacceptable pain (pain score >4) per postoperative day did not differ between groups (Table 2; Figure 3). In both groups, an increase was observed in patients reporting unacceptable pain on postoperative day 3 compared to day 2.
 |
Figure 3 Mean (SD) pain score per postoperative day (left), and percentage of patients reporting a pain score >4 per postoperative day (right). |
Overall Benefit of Analgesia Scores (OBAS)
The median (IQR) OBAS on postoperative days 1 to 3 was 7 (3–10) in the SST group and 3 (3–6) in the standard-of-care group (p = 0.126) (Table 2). Also, the median (IQR) OBAS per postoperative day did not differ between groups.
Patient Satisfaction Scores
The median (IQR) patient satisfaction score on postoperative day 1 to 3 was 7 (5–9) in the SST group and 8 (7–9) in the standard-of-care group (p = 0.337) (Table 2). Median (IQR) patient satisfaction scores per postoperative day did not differ between groups.
Perioperative Hemodynamics
Perioperative characteristics did not differ between groups (Table 3). The use and total dosage of vasopressors did not differ between groups. In the SST group, 7 patients (41%) experienced perioperative hypotension compared to 5 patients (26%) in the standard-of-care group (P = 0.345). Fluid balances on postoperative days 0 to 5 did not differ between groups.
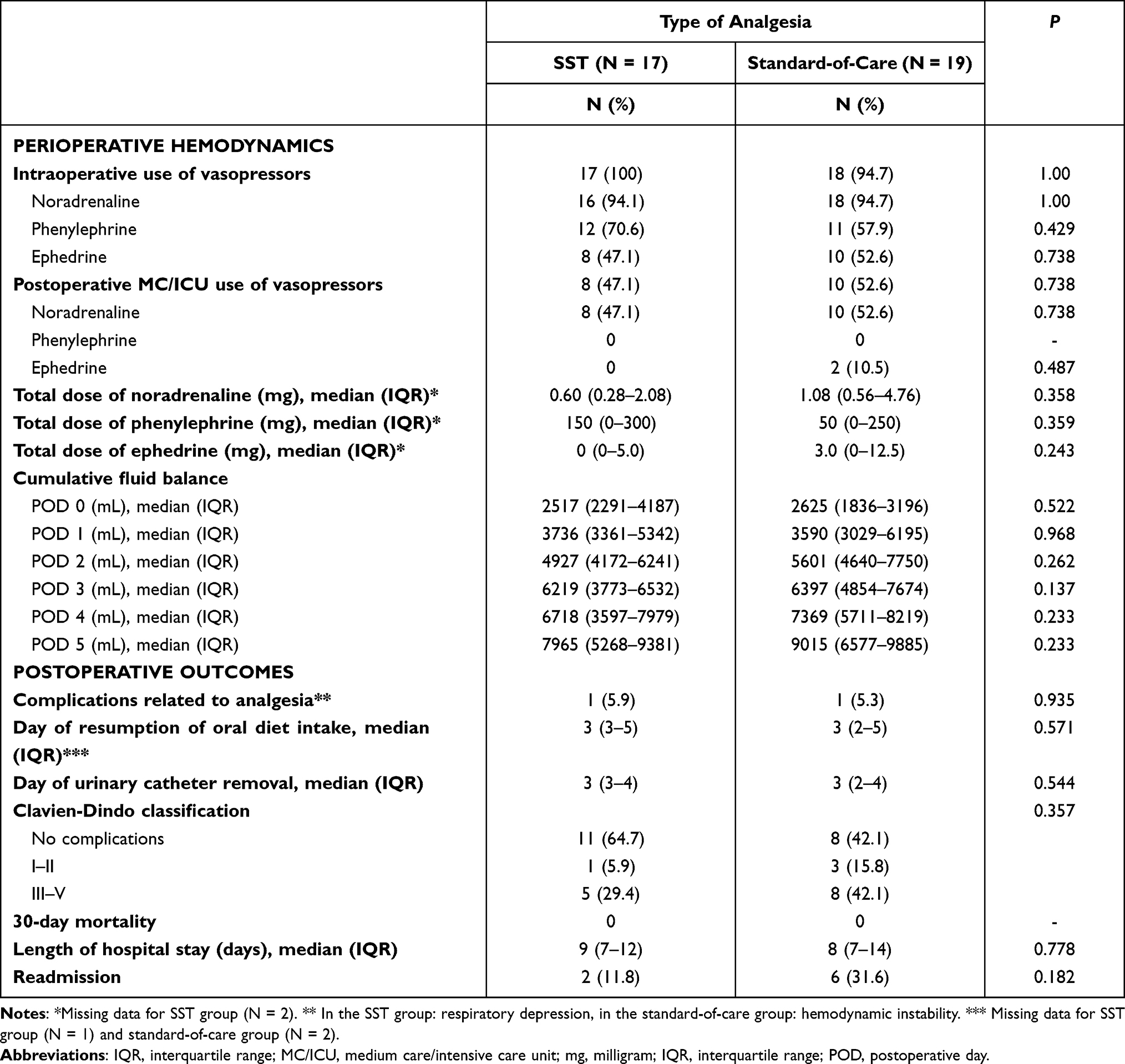 |
Table 3 Perioperative Hemodynamics and Postoperative Outcomes |
Additional Postoperative Outcomes
Postoperative characteristics did not differ between groups (Table 3). In both groups, 1 patient (SST group: 6%, standard-of-care group: 5%) experienced a complication related to analgesia (SST group: respiratory depression with good effect of naloxone treatment, standard-of-care group: hemodynamic instability with good effect of stopping PCEA).
Subgroup Analysis
Predefined Subgroup Analysis by Intended Type of Procedure
Patients undergoing an intended open procedure (SST [n = 10] versus standard-of-care: PCEA [n = 10] and PCA morphine [n = 1]) showed similar results for mean pain score on postoperative days 1 to 3 (mean difference −0.23 [95% CI −1.22–0.75]). The mean (SD) pain score on postoperative day 3 was significantly lower in the SST group compared to the standard-of-care group (1.19 [0.97] versus 2.75 [1.84]; p = 0.03). Other pain scores per postoperative day did not differ between these groups. Patients undergoing an intended robot-assisted procedure (SST [n = 7] versus standard-of-care: PCA morphine [n = 8]) showed similar results for mean pain score on postoperative days 1 to 3 (mean difference 0.02 [95% CI −0.58–0.62]). The mean (SD) pain score on postoperative day 1 was significantly lower in the SST group compared to the PCA morphine group (2.42 [0.83] versus 3.22 [0.44]; p = 0.033). Other pain scores per postoperative day did not differ between these groups.
Predefined Subgroup Analysis by Original and Amended Protocol
Patients during the original protocol (SST [n = 3] versus standard-of-care [n = 5]) showed similar results for mean pain score on postoperative days 1 to 3 (mean difference 0.98 [95% CI −2.23–2.56]). The mean (SD) pain scores on postoperative days 0 and 1 were significantly higher in the SST group compared to the standard-of-care group (3.67 [1.1] versus 1.62 [1.17]; p = 0.05 and 3.83 [1.74] versus 1.28 [0.82]; p = 0.027). Other pain scores per postoperative day did not differ between these groups. Patients during the amended protocol (SST [n = 14] versus standard-of-care [n = 14]) showed similar results for mean pain score on postoperative day 1 to 3 (mean difference −0.17 [95% CI −0.80–0.47]). Pain scores per postoperative day did not differ between these groups.
Post-Hoc Subgroup Analysis by Age
Patients ≤65 years (SST [n = 8] versus standard-of-care [n = 10]) and >65 years (SST [n = 9] versus standard-of-care [n = 9]) showed similar results for mean pain score on postoperative days 1 to 3 and mean pain score per postoperative day (data not shown).
Discussion
This first randomized study investigating the use of SST in 36 patients following pancreatoduodenectomy showed that the SST treatment strategy, as part of a multimodal approach, is a non-inferior analgesic compared to our standard-of-care (PCEA or PCA morphine) in the treatment of pain on postoperative days 1 to 3. Early treatment failure occurred in 24% of patients in the SST group and in 16% of patients in the standard-of-care group. Additional outcomes such as pain scores, OBAS and patient satisfaction scores did not differ between the two groups. Also, perioperative hemodynamics and postoperative outcomes did not differ between the two groups.
The mean difference in pain score on postoperative day 1 to 3 was −0.10 (95% CI −0.72–0.52), and therefore, non-inferiority of SST was demonstrated. No previous randomized data were available that reported mean postoperative pain scores with SST. An observational study of our first clinical experience with SST did show comparable postoperative pain scores in laparoscopic abdominal and orthopedic surgery.10 Previous randomized trials with (PC)EA and PCA or iv morphine showed similar pain scores during the first postoperative days.21–24 This suggests that our results regarding pain scores might be applicable to other settings. It should be noted that this study investigated multimodal treatment strategies, including standard use of paracetamol and if needed metamizole and ketamine besides SST, PCEA or PCA morphine, and therefore no conclusions can be drawn on the effectiveness of the individual components of the treatment strategy. An increase was observed in patients reporting unacceptable pain on postoperative day 3 compared to day 2 in both groups. This may have been caused by the termination of SST and standard-of-care and (painful) transition to paracetamol and oral or sc opioids.2 Evidently, more efforts are needed to improve this transition and prevent an upsurge in pain scores when the primary treatment strategy is ended.
The OBAS did not differ significantly between groups. The reported OBAS of the SST group was somewhat higher (a lower score is better) than the standard-of-care group and also higher than reported in a study comparing continuous wound infiltration plus PCA morphine to (PC)EA in patients undergoing open hepato-pancreato-biliary surgery.24 Since we did not separately analyze side effects (mainly nausea and dizziness), we can only hypothesize that OBAS of the SST group was somewhat higher due to more frequently experienced side effects of the SST and not due to higher pain scores. This possibly also explains why patient satisfaction scores were slightly lower in the SST group. A more proactive administration of antiemetics and communication with the patient could be a solution. We did not assess the level of sedation prior to pain scoring or OBAS. Sedation may have affected scores, but it is our experience that residual sedation is minimal in our patient population following total intravenous anesthesia and preemptive morphine dosing.
Early treatment failure occurred in 24% of patients in the SST group and in 16% of patients in the standard-of-care group (all in the PCEA group; 30%). In a previous randomized trial with SST in open abdominal and orthopedic surgery, the early failure rate was 18%.12 A disadvantage of SST is that patients need a good cognition, vision and hand-to-mouth coordination in order to operate the system, and careful patient selection (eg low risk for post-operative delirium) is therefore warranted. A meta-analysis performed by us showed similar data of early treatment failure in patients with EA (29%).3 We did not formally check the position of the PCEA catheter with, eg radiography, as this is not part of our standard clinical practice. Patients were analyzed using an intention-to-treat approach to avoid potential bias due to exclusion of patients and resemble standard clinical care as much as possible.
EA has been associated with significant vasoactive medication, fluid administration and even impaired anastomotic healing.25,26 Perioperative hemodynamics did not differ between the groups in this study, yet the sample size could have been too small to detect relevant and significant differences. This also applies to the other postoperative outcomes. The use of SST has a benefit over PCEA and PCA morphine as no epidural catheter or iv line is needed which can hinder the patient from early ambulation and early urinary catheter removal. Unfortunately, no difference was observed regarding urinary catheter removal in the current study.
Several subgroup analyses were performed to confirm the robustness of the results. In intended open procedures, pain scores on postoperative day 3 were lower in the SST group compared to the standard-of-care (PCEA) group. As already mentioned, this might be the result of the (painful) transition to paracetamol and oral or sc opioids.2 During the original protocol, pain scores on postoperative days 0 and 1 were higher in the SST group compared to the standard-of-care (PCEA) group. We speculate that this may be caused by a short learning curve in the use of SST in clinical practice following pancreatoduodenectomy. The subgroup analysis of >65 years showed similar results between SST and standard-of-care, though we would have expected higher pain scores in the SST group since the SST system is more difficult to operate compared to standard-of-care. A possible explanation may be that also for the standard-of-care group patients require a good understanding of the systems as these are also patient controlled methods. There is no one-size-fits-all type of analgesic treatment strategy and for choosing the most appropriate treatment strategy, in the process of shared decision-making, the clinician together with the patients should weigh all relevant factors including patient characteristics and the potential advantages and disadvantages of each different treatment strategy. Careful patient selection, a multimodal treatment strategy and a dedicated and specialized team, including the Acute Pain Service,19 are pivotal for a successful postoperative pain treatment.
This study has several limitations. First, the sample size was small, although large enough to demonstrate non-inferiority of the primary outcome. Due to the small sample size, it is possible that some relevant and significant differences were not found for the secondary outcomes (Type II or β error). Second, postoperative day 0 (day of surgery) was not included in the primary outcome since, in our experience, this day is used to establish an adequate level of pain control as modifications of treatment and repetitive instruction of the patient are often needed.2 Another reason was that the antinociceptive treatment during surgery may have differed among patients with differences in their residual analgesic effects in the first postoperative hours. To investigate possible variations in pain scores during each postoperative day which were not reflected within the mean pain score, we also analyzed the proportion of patients that reported unacceptable pain and observed no significant difference. Third, the open-label design (no blinding) introduces a risk of performance bias. Blinding was not done since the treatment strategies were evidently different, and blinding of study participants and investigators is not pragmatic and does not resemble standard clinical care. Fourth, two relevant amendments were made to the protocol during the study (allow inclusion of robot-assisted procedures and changing the non-inferiority margin) which might have affected the outcomes. These amendments were reviewed and approved by an independent ethics committee (including a statistical review). Enlarging the inclusion criteria was done as the number of open pancreatoduodenectomies declined rapidly over the last two years in our center, partly related to the COVID-19 pandemic and to the wishes of surgeons and patients to perform a minimal invasive procedure. Minimally invasive pancreatoduodenectomy has been suggested to cause less pain and a faster recovery in non-randomized studies.27 Stratification of procedure type was used to ensure equal distribution of open and robot-assisted procedures in both groups. The treatment strategies in the standard-of-care group changed due to the inclusion of robot-assisted procedures (from only PCEA to PCEA or PCA morphine). This amendment to the protocol was not in conflict with our goal, which was to demonstrate that the SST treatment strategy is a non-inferior alternative to our standard-of-care following pancreatoduodenectomy. The change was regarded as statistically acceptable since our own retrospective data showed that patients with PCEA and PCA morphine following pancreatoduodenectomy reported similar overall mean pain scores on postoperative days 1 to 3 combined. Due to slow accrual, we changed the non-inferiority margin from −1.0 to −1.5 in order to decrease the required sample size. It should be noted that −1.5 is still somewhat strict, as other studies used a margin of −2.0.21,28 Multiple subgroup analysis (eg by intended procedure type and protocol version) was performed to check the robustness of the outcomes. And lastly, we chose not to include secondary outcomes investigating the pharmaco-economics. This should be included in future trials.
In conclusion, this study demonstrated that the SST treatment strategy is a non-inferior analgesic compared to our standard-of-care (PCEA or PCA morphine) in the treatment of pain following pancreatoduodenectomy. In our institution, SST can definitely be added to the pallet of postoperative pain treatment strategies following pancreatoduodenectomy. Future research is needed to confirm that these findings are applicable to other settings, preferably by studies with larger sample sizes and multicenter study designs.
Data Sharing Statement
The datasets used during this study are available on reasonable requests from the corresponding authors.
Ethics Approval and Consent to Participate
The Medical Ethics Committee of the Leiden University Medical Center approved the study (P18.061) and all participants provided a signed informed consent form. This study adhered to the tenets of the Declaration of Helsinki.
Trial Registration
Netherlands Trial Register: NTR7318 (www.trialregister.nl)
Study Protocol
The full study protocol can be found in the Supplementary Files.
Sources of Support
The primary sponsor of the study was the Department of Anesthesiology, Leiden University Medical Center (address: Albinusdreef 2, 2333 ZA, Leiden). JSDM received funding from the Bas Mulder Award (grant UL2015-7665) from the Alpe d’HuZes foundation/Dutch Cancer Society. AD received an educational grant and speaker fees from Grunenthal BV (the Netherlands). The sponsors/funders had no role in the study design, collection, analyses, or interpretation of the data, drafting of the manuscript or the decision to publish.
Acknowledgments
We would like to thank patients for their participation in this study. We also appreciate the efforts of all health-care providers, especially the Acute Pain Service and the nursing staff. We also thank E.M.C. van der Stroom and N.A. Poublon (Department of Anesthesiology, Leiden University Medical Center, Leiden, The Netherlands) for their help with patient recruitment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
AD received an educational grant and speaker fees from Grunenthal BV (the Netherlands); grants from MSD, personal fees from Grunenthal, grants from Medasense, grants, personal fees from Enalare, grants from Takeda, grants from AMO Pharma, grants from ZonMW, grants from FDA, grants from LTS Lohmann, grants from Bedrocan, outside the submitted work. Dr Monique van Velzen reports grants from Grunenthal, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Werawatganon T, Charuluxanun S. Patient controlled intravenous opioid analgesia versus continuous epidural analgesia for pain after intra-abdominal surgery. Cochrane Database Syst Rev. 2005;1(1):CD004088.
2. Groen JV, Slotboom DEF, Vuyk J, et al. Epidural and Non-epidural analgesia in patients undergoing open pancreatectomy: a retrospective cohort study. J Gastrointest Surg. 2019;23(12):2439–2448. doi:10.1007/s11605-019-04136-w
3. Groen JV, Khawar AAJ, Bauer PA, et al. Meta-analysis of epidural analgesia in patients undergoing pancreatoduodenectomy. BJS Open. 2019;3(5):559–571. doi:10.1002/bjs5.50171
4. Axelrod TM, Mendez BM, Abood GJ, Sinacore JM, Aranha GV, Shoup M. Peri-operative epidural may not be the preferred form of analgesia in select patients undergoing pancreaticoduodenectomy. J Surg Oncol. 2015;111(3):306–310. doi:10.1002/jso.23815
5. Low J, Johnston N, Morris C. Epidural analgesia: first do no harm. Anaesthesia. 2008;63(1):1–3. doi:10.1111/j.1365-2044.2007.05407.x
6. Pratt WB, Steinbrook RA, Maithel SK, Vanounou T, Callery MP, Vollmer CM. Epidural analgesia for pancreatoduodenectomy: a critical appraisal. J Gastrointest Surg. 2008;12(7):1207–1220. doi:10.1007/s11605-008-0467-1
7. Groen JV, Henrar RB, Hanna Sawires RG, et al. Pain management, fluid therapy and thromboprophylaxis after pancreatoduodenectomy: a worldwide survey among surgeons. HPB (Oxford). 2021;1:5487.
8. Aloia TA, Kim BJ, Segraves-Chun YS, et al. Trial of postoperative thoracic epidural analgesia versus intravenous patient-controlled analgesia after major hepatopancreatobiliary surgery. Ann Surg. 2017;266(3):545–554. doi:10.1097/SLA.0000000000002386
9. van de Donk T, Ward S, Langford R, Dahan A. Pharmacokinetics and pharmacodynamics of sublingual sufentanil for postoperative pain management. Anaesthesia. 2018;73(2):231–237. doi:10.1111/anae.14132
10. Meijer F, Cornelissen P, Sie C, et al. Sublingual sufentanil for postoperative pain relief: first clinical experiences. J Pain Res. 2018;11:987–992. doi:10.2147/JPR.S160091
11. Jove M, Griffin DW, Minkowitz HS, Ben-David B, Evashenk MA, Palmer PP. Sufentanil Sublingual Tablet System for the Management of Postoperative Pain after Knee or Hip Arthroplasty: a Randomized, Placebo-controlled Study. Anesthesiology. 2015;123(2):434–443. doi:10.1097/ALN.0000000000000746
12. Melson TI, Boyer DL, Minkowitz HS, et al. Sufentanil sublingual tablet system vs. intravenous patient-controlled analgesia with morphine for postoperative pain control: a randomized, active-comparator trial. Pain Practice. 2014;14(8):679–688. doi:10.1111/papr.12238
13. Ringold FG, Minkowitz HS, Gan TJ, et al. Sufentanil sublingual tablet system for the management of postoperative pain following open abdominal surgery: a randomized, placebo-controlled study. Reg Anesth Pain Med. 2015;40(1):22–30. doi:10.1097/AAP.0000000000000152
14. Kehlet H, Wilkinson RC, Fischer HB, Camu F, Prospect Working G. PROSPECT: evidence-based, procedure-specific postoperative pain management. Best Pract Res Clin Anaesthesiol. 2007;21(1):149–159. doi:10.1016/j.bpa.2006.12.001
15. Blom JW, Muth C, Glasziou P, et al. Describing deprescribing trials better: an elaboration of the CONSORT statement. J Clin Epidemiol. 2020;127:87–95. doi:10.1016/j.jclinepi.2020.07.011
16. Cepeda MS, Africano JM, Polo R, Alcala R, Carr DB. What decline in pain intensity is meaningful to patients with acute pain? Pain. 2003;105(1–2):151–157. doi:10.1016/S0304-3959(03)00176-3
17. Lehmann N, Joshi GP, Dirkmann D, et al. Development and longitudinal validation of the overall benefit of analgesia score: a simple multi-dimensional quality assessment instrument. Br J Anaesth. 2010;105(4):511–518. doi:10.1093/bja/aeq186
18. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213. doi:10.1097/01.sla.0000133083.54934.ae
19. Rawal N, Berggren L. Organization of acute pain services: a low-cost model. Pain. 1994;57(1):117–123. doi:10.1016/0304-3959(94)90115-5
20. VMS-Veiligheidsprogramma. Vroege herkenning en behandeling van pijn; 2009. Available from: https://wwwvmszorgnl/wp-content/uploads/2017/11/web_20090109_praktijkgids_pijnpdf.
21. Hutchins JL, Grandelis AJ, Kaizer AM, Jensen EH. Thoracic paravertebral block versus thoracic epidural analgesia for post-operative pain control in open pancreatic surgery: a randomized controlled trial. J Clin Anesth. 2018;48:41–45. doi:10.1016/j.jclinane.2018.04.013
22. Klotz R, Larmann J, Klose C, et al. Gastrointestinal Complications After Pancreatoduodenectomy With Epidural vs Patient-Controlled Intravenous Analgesia: a Randomized Clinical Trial. JAMA Surg. 2020;155(7):e200794. doi:10.1001/jamasurg.2020.0794
23. Marandola M, Cilli T, Alessandri F, et al. Perioperative management in patients undergoing pancreatic surgery: the anesthesiologist’s point of view. Transplant Proc. 2008;40(4):1195–1199. doi:10.1016/j.transproceed.2008.03.114
24. Mungroop TH, Bond MJ, Lirk P, et al. Preperitoneal or Subcutaneous Wound Catheters as Alternative for Epidural Analgesia in Abdominal Surgery: a Systematic Review and Meta-analysis. Ann Surg. 2018;1:47.
25. Kulemann B, Fritz M, Glatz T, et al. Complications after pancreaticoduodenectomy are associated with higher amounts of intra- and postoperative fluid therapy: a single center retrospective cohort study. Ann Med Surg. 2017;16:23–29. doi:10.1016/j.amsu.2017.02.042
26. Wright GP, Koehler TJ, Davis AT, Chung MH. The drowning whipple: perioperative fluid balance and outcomes following pancreaticoduodenectomy. J Surg Oncol. 2014;110(4):407–411. doi:10.1002/jso.23662
27. Chen K, Pan Y, Liu XL, et al. Minimally invasive pancreaticoduodenectomy for periampullary disease: a comprehensive review of literature and meta-analysis of outcomes compared with open surgery. BMC gastroenterology. 2017;17(1):120. doi:10.1186/s12876-017-0691-9
28. Liu SS, Richman JM, Thirlby RC, Wu CL. Efficacy of continuous wound catheters delivering local anesthetic for postoperative analgesia: a quantitative and qualitative systematic review of randomized controlled trials. J Am Coll Surg. 2006;203(6):914–932. doi:10.1016/j.jamcollsurg.2006.08.007
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sufentanil-Dezocine Combination in Patient-Controlled Intravenous Analgesia for Postoperative Pain After Pancreatic Cancer Surgery: A Retrospective Propensity Score-Matched Study
Huang Z, Li J, Xia Y, Li Q, Song X, Xu X, Luo Y
Journal of Pain Research 2025, 18:5523-5531
Published Date: 21 October 2025
Determination of the ED90 for Epidural Hydromorphone and Morphine for Postoperative Pain Using a Biased-Coin Up-and-Down Sequential Design After Elective Cesarean Delivery
Tang X, Liang Y, Hu Y, Li P, Wang J, Wang Y, Xie M
Drug Design, Development and Therapy 2026, 20:588767
Published Date: 9 June 2026