Back to Journals » Journal of Pain Research » Volume 14
Subcutaneous Methylnaltrexone for Treatment of Opioid-Induced Constipation in Cancer versus Noncancer Patients: An Analysis of Efficacy and Safety Variables from Two Studies
Authors Chamberlain BH, Rhiner M, Slatkin NE ![]() , Stambler N
, Stambler N ![]() , Israel RJ
, Israel RJ
Received 27 March 2021
Accepted for publication 27 July 2021
Published 1 September 2021 Volume 2021:14 Pages 2687—2697
DOI https://doi.org/10.2147/JPR.S312731
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Bruce H Chamberlain,1 Michelle Rhiner,2 Neal E Slatkin,3,4 Nancy Stambler,5 Robert J Israel6
1Genesis Healthcare, Davenport, IA, USA; 2Loma Linda University Health, Department of Family Medicine, Loma Linda, CA, USA; 3University of California Riverside, School of Medicine, Riverside, CA, USA; 4Salix Pharmaceuticals, Medical Affairs, Bridgewater, NJ, USA; 5Progenics Pharmaceuticals, Inc., a subsidiary of Lantheus Holdings Inc., Clinical Research, New York, NY, USA; 6Bausch Health US, LLC, Clinical and Medical Affairs, Bridgewater, NJ, USA
Correspondence: Robert J Israel
Bausch Health US, LLC, Clinical and Medical Affairs, 400 Somerset Corporate Boulevard, Room 6-1001, Bridgewater, NJ, 08807, USA
Tel +1 908 541-2288
Fax +1 585 338-0668
Email [email protected]
Purpose: Methylnaltrexone inhibits opioid-induced constipation (OIC) by binding to peripheral μ-opioid receptors without impacting central opioid receptor mediated analgesia. This analysis compared methylnaltrexone efficacy and safety among advanced illness patients with and without active cancer and OIC.
Patients and Methods: This post hoc analysis included two multicenter, randomized, double-blind, placebo-controlled studies in adults with advanced illness and OIC who received subcutaneous methylnaltrexone. Efficacy endpoints included the proportion of patients achieving rescue-free laxation (RFL), time to RFL, weekly laxations within 24 hours after dosing, rescue laxative use, and pain scores. Adverse events were monitored for safety.
Results: After pooling, 178 patients received methylnaltrexone (n = 116 with cancer) and 185 received placebo (n = 114 with cancer). Median baseline daily opioid morphine equivalents (mg/d) were higher in cancer (methylnaltrexone: 180; placebo: 188) versus noncancer patients (methylnaltrexone: 120; placebo: 80). The proportions of patients achieving RFL within 4 hours after ≥ 2 of the first 4 doses were significantly greater with methylnaltrexone (cancer: 56.9%; noncancer: 58.1%) versus placebo (cancer: 5.3%; noncancer: 11.3%; P < 0.0001). The median time to laxation within 24 hours after the first methylnaltrexone dose was significantly shorter in cancer and noncancer patients versus placebo (cancer: 0.96 vs 22.53 hours, P < 0.0001; noncancer: 1.25 vs > 24 hours, P = 0.0002). The mean number of weekly laxations within 24 hours after dosing by week 2 was significantly higher in methylnaltrexone- vs placebo-treated cancer and noncancer patients (cancer: 7.9 vs 4.9, P < 0.0001; noncancer: 8.4 vs 5.0, P < 0.0001). Methylnaltrexone reduced rescue laxative use without impacting pain scores. Consistent with previous data, methylnaltrexone was well tolerated in cancer and noncancer patients, and the AE profile did not suggest symptoms of opioid withdrawal.
Conclusion: Methylnaltrexone reduced RFL time in advanced-illness patients with and without active cancer, while maintaining pain control with opioid treatment despite higher baseline opioid use among cancer patients.
Keywords: methylnaltrexone, opioid-induced constipation, μ-opioid receptor antagonist, cancer, chronic pain
Introduction
Moderate to severe pain occurs in patients with cancer and, despite their inherent risks, management often includes opioid analgesics.1,2 Opioid-induced constipation (OIC) is a common adverse effect of opioid analgesics, affecting up to 60% of patients being managed for cancer-related pain with opioids.3 When daily opioid therapy is prolonged in cancer patients, the likelihood of OIC increases.4–6 The development of OIC may limit opioid use, thereby compromising effective analgesia in patients with chronic pain.5,7 OIC also impacts quality of life in patients with cancer. In a trial of Japanese patients, quality of life measured 2 weeks after initiation of a strong opioid was significantly reduced among cancer patients with OIC compared with those without OIC.8
The use of traditional laxatives often fails to adequately manage symptoms associated with OIC because the underlying opioid receptor-mediated mechanism remains untargeted.2,9–11 OIC occurs as a result of an opioid binding to peripheral μ-opioid receptors in the gastrointestinal tract, leading to abnormal modulation of gastrointestinal secretion and absorption.9,12–14 These considerations have led to the development of the peripherally acting µ-opioid receptor antagonist (PAMORA) class of agents to specifically address OIC.15 However, constipation in patients with cancer is often multifactorial and may arise from several sources in addition to opioid use. For instance, constipation may be a consequence of cancer-related physiologic dysfunction (eg, gastrointestinal obstruction, tumors, autonomic dysfunction), concomitant medications (eg, anticholinergics, antiemetics, chemotherapy), dehydration, immobility, diet, or metabolic causes (eg, hypercalcemia, hypokalemia), among other factors.11 Hence, the response of constipated opioid-treated cancer patients to a PAMORA may differ from that of other opioid-treated patients having serious and advanced noncancer illnesses.
A number of reports have indicated that opioids and activation of u-opioid receptors (MOR) may be an overall risk factor for survival in patients with advanced cancer.16–19 In addition to the negative impact of OIC on the symptoms and healthcare resource utilization in cancer patients,20 the presence of constipation has itself emerged as a potential survival risk factor for such patients.21–23 As such, the control of opioid-mediated constipation takes on even greater significance. Indeed, in a retrospective analysis of the treatment of advanced illness patients with OIC, Janku et al found that peripheral µ-opioid inhibition played a role in enhancing cancer survival, an effect potentially directly related to improved gut function.24 These findings also complement preclinical studies showing that activation of the tumor based MOR has been directly implicated as a risk factor in cancer progression through a variety of mechanisms including MOR-related angiogenesis;18,25 an effect shown in several studies to be inhibited by a peripheral u-opioid antagonist.17,26,27
To the extent that OIC may not only be a distressing symptom in cancer patients, but a factor contributing to decreased survival, it is important to establish the efficacy of peripheral opioid antagonism in treating this symptom. Methylnaltrexone (Relistor®, Salix Pharmaceuticals, a division of Bausch Health US, LLC, Bridgewater, NJ, USA) is a selective, peripherally acting μ-opioid receptor antagonist (PAMORA) that improves gastrointestinal transit in opioid-treated patients.28 Since methylnaltrexone has restricted ability to cross an intact blood–brain barrier due to high polarity and low lipid solubility, it is able to act on opioid receptors in the gastrointestinal tract without affecting the analgesic effects of the opioid.14,28–32 Methylnaltrexone tablets and subcutaneous (SC) injection are approved for the treatment of OIC in adults with chronic pain related to prior cancer or its treatment who do not require frequent (eg, weekly) opioid dosage escalation.28 Methylnaltrexone SC injection is the only PAMORA approved for the treatment of OIC in adults with advanced illness or pain caused by active cancer who require opioid dosage escalation for palliative care.28
In two previously completed primary studies in patients with advanced illnesses including cancer, SC methylnaltrexone demonstrated robust efficacy and was well tolerated in treating OIC without affecting central analgesia or precipitating opioid withdrawal.29,31 To our knowledge, though, no prospective studies have assessed the efficacy and safety of PAMORAs or laxatives for the treatment of OIC in patients with cancer in the United States, and there are no published studies that compare SC methylnaltrexone use among patients with and without cancer. This post hoc analysis evaluated data from two similarly designed multidose studies and characterized the baseline demographics and efficacy and safety endpoints of patients with and without cancer, receiving opioids, and treated with methylnaltrexone or placebo. Results may provide a basis for future studies to assess additional clinical benefits of methylnaltrexone in cancer patients.
Methods
Study Design
Two multicenter, double-blind, randomized, placebo-controlled studies (302 [NCT00402038] and 4000 [NCT00672477]) were conducted in adult patients with advanced illness and OIC. Each individual study has been previously published.29,31 In study 302, a 5-day screening period was followed by 1:1 randomization of patients to receive SC injections of methylnaltrexone 0.15 mg/kg or placebo every other day for 2 weeks. Patients who had <3 bowel movements not associated with rescue medication or intervention (eg, enema) by day 8 were eligible for dose escalation to 0.30 mg/kg starting on day 9 at the discretion of the investigator. In study 4000, patients were randomized (1:1) to receive SC injections of methylnaltrexone on the basis of body weight: 0.4 mL of methylnaltrexone (8 mg) or equal volume of placebo for patients weighing 38 kg to <62 kg and 0.6 mL of methylnaltrexone (12 mg) or equal volume of placebo for those weighing ≥62 kg every other day for a maximum of 7 doses for 14 days. All patients who completed the studies were eligible to enroll in open-label extension studies (study 302, NCT01367613; study 4000, NCT00672139). Patients who did not continue in the extension studies were contacted 30 days after the last dose (study 302) or had a follow-up visit 15 to 21 days after the last dose (study 4000).
During the studies, treatment with rescue laxatives and enemas was not permitted within 4 hours before or after administration of study drug but was otherwise allowed. Patients could receive rescue doses of opioids as necessary.
Patients
Patients aged ≥18 years with a diagnosis of advanced illness, including terminal illnesses such as incurable cancer and end-stage acquired immune deficiency syndrome, with a life expectancy ≥1 month were eligible for enrollment in the studies. Patients were required to be receiving opioids routinely for discomfort or pain management for ≥2 weeks before the first dose of the study drug, and to be taking a stable regimen (defined as no reduction in dose of ≥50%; increases in dose were permitted) for ≥3 days before the first dose. Patients were required to have OIC, defined as (1) <3 bowel movements during the previous week and no clinically significant laxation in the 24 hours before the first dose of study drug or (2) no clinically significant laxation within 48 hours before the first dose of study drug. For patients taking laxatives, including stool softeners (eg, docusate sodium), stimulants (eg, senna and bisacodyl) and osmotic agents (eg, milk of magnesia, polyethylene glycol, lactulose, and sorbitol), the regimen was to be stable for ≥3 days prior to the first dose of study drug, and patients were permitted to continue these laxatives throughout the study.
Patients were excluded if they had a history of methylnaltrexone treatment, any disease process suggestive of mechanical bowel obstruction, evidence of fecal impaction, active diverticular disease, fecal ostomy, and any potential nonopioid cause of bowel dysfunction, which in the opinion of the investigator might have been primarily responsible for constipation. Additionally, patients with surgically acute abdomens were not eligible for study 302, and patients who received vinca alkaloids (eg, vincristine, vinblastine, or vinorelbine) during the 4 months before screening were not eligible for study 4000.
Assessments
Patients were stratified by those with active cancer and those without cancer. In order to show that methylnaltrexone worked quickly and to determine the temporal relationship between drug administration and response, the following efficacy endpoints were chosen: (1) the proportion of patients with RFL within 4 hours after ≥2 of the first 4 doses; (2) the proportion of patients with RFL within 4 hours after the first dose; (3) the time to first RFL assessed at 4 hours and 24 hours; (4) the number of laxations within 24 hours after dosing by week 2; (5) the proportion of patients with ≥3 rescue-free bowel movements per week in both weeks 1 and 2; (6) the proportion of patients using rescue laxatives; and (7) pain scores. The weekly number of laxations was set to missing for the week where bowel movement assessment was missing for more than 3 days. Current and worst levels of pain were evaluated after the first dose of study medication and on day 7 and graded on a scale of 0 (none) to 10 (worst possible pain).
Safety was evaluated in all patients who received a dose of study drug and included the incidence, severity, and type of adverse events (AEs). All AEs were coded according to the Medical Dictionary for Drug Regulatory Affairs version 6.0 (study 302) or 14.0 (study 4000). Treatment-emergent AEs (TEAEs), serious TEAEs, and TEAEs leading to premature study discontinuation were summarized overall and according to their relationship to study medication.
Statistical Analyses
Data were pooled from both studies and patients were stratified by those with active cancer and those without cancer. Efficacy analyses were performed on the intent-to-treat (ITT) analysis set, which was defined as patients who received ≥1 dose of study drug. Data were analyzed using chi-square tests for RFL response and use of rescue laxatives; log-rank tests for time to first RFL response censored at 48 hours or the time of the next dose of study medication; and Wilcoxon rank-sum tests for weekly number of laxations. Kaplan–Meier survival curves were used to compare the time to laxation onset between treatments for cancer and noncancer patients. The nominal level of significance was 0.05, with no adjustment for multiplicity.
Ethical Considerations
Both studies were designed and conducted in compliance with the principles of Good Clinical Practice and the Declaration of Helsinki. Written informed consent was obtained from each patient prior to their participation in the trial. Study protocols and informed consent forms received institutional review board approval from respective investigational sites before the study began (Supplementary Information).
Results
Patients
In the pooled population, a total of 178 patients received methylnaltrexone and 185 patients received placebo; 65.2% (n=116) of patients in the methylnaltrexone group and 61.6% (n=114) of patients in the placebo group had cancer. Demographics and baseline characteristics are shown in Table 1. Patients with cancer were taking higher median daily doses of opioid morphine equivalents (methylnaltrexone: 180 mg/d; placebo: 188 mg/d) at baseline compared with those without cancer (methylnaltrexone: 120 mg/d; placebo: 80 mg/d). Almost all (98.6%) patients were using laxatives at baseline, with similar laxative use between groups. There were no notable differences in current and worst pain scores between study populations at baseline.
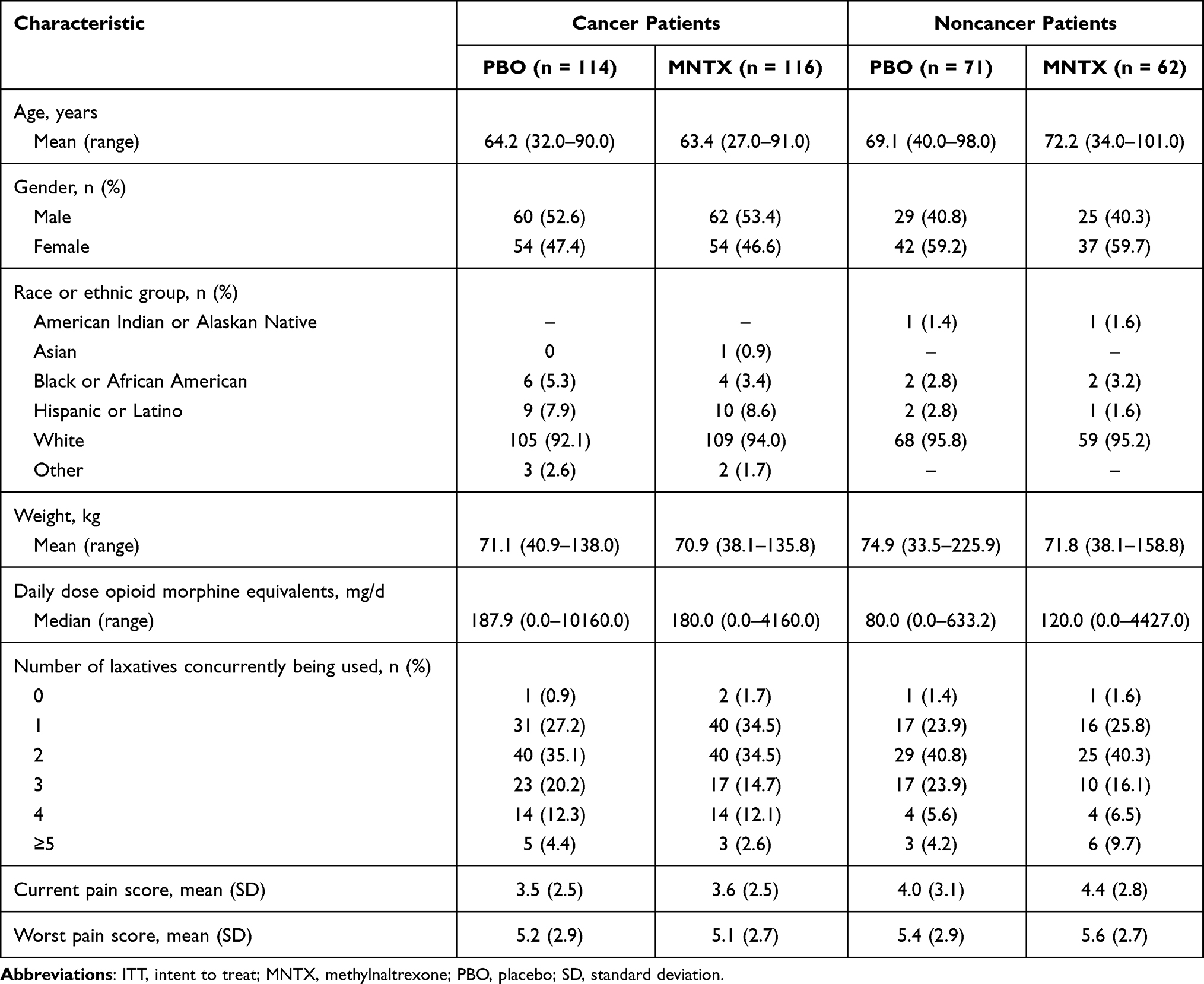 |
Table 1 Demographics and Baseline Characteristics of Patients Stratified by Cancer Status (Pooled ITT Population) |
Effect on Laxation
In patients with and without cancer, methylnaltrexone induced a significantly greater RFL response within 4 hours after the first dose of treatment compared with placebo (P < 0.0001; Figure 1). Significant differences in RFL after ≥2 of the first 4 doses of study drug were also observed (Figure 1B). The probability of having an RFL within 4 and 24 hours after the first dose of study medication was significantly greater following methylnaltrexone treatment in both cancer and noncancer patients compared with placebo (Figure 2). The median times to laxation within 24 hours after the first dose of study medication were 0.96 hours and 22.53 hours in cancer patients who received methylnaltrexone and placebo, respectively (P < 0.0001), and 1.25 hours and >24 hours in noncancer patients who received methylnaltrexone and placebo, respectively (P=0.0002). These data indicate that most cancer and noncancer patients who received methylnaltrexone and responded to treatment did so within the first hour after the first dose of study drug. The mean weekly number of laxations within 24 hours after dosing were similar in methylnaltrexone-treated patients with and without cancer by week 2 of the study and were higher in both cancer and noncancer patients who received methylnaltrexone versus placebo (Figure 3). Among cancer and noncancer groups, significantly higher proportions of patients receiving methylnaltrexone versus placebo achieved ≥3 RFL per week in both weeks 1 and 2 on study (Figure 4).
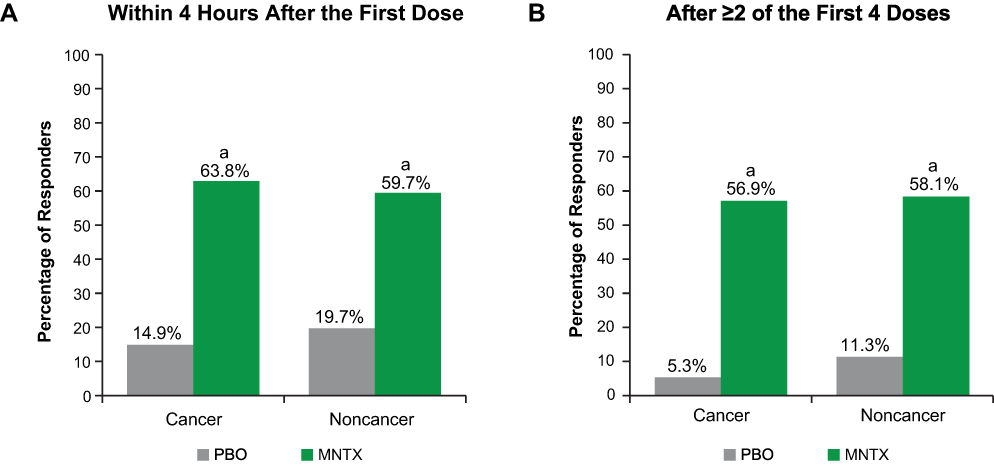 |
Figure 1 Responders with laxation (A) within 4 hours after the first dose and (B) after ≥2 of the first 4 doses (pooled ITT population). Abbreviations: ITT, intent to treat; MNTX, methylnaltrexone; PBO, placebo. Notes: Among patients with cancer, n = 114 for PBO; n = 116 for MNTX. Among patients without cancer, n = 71 for PBO; n = 62 for MNTX. aP < 0.0001 vs PBO. |
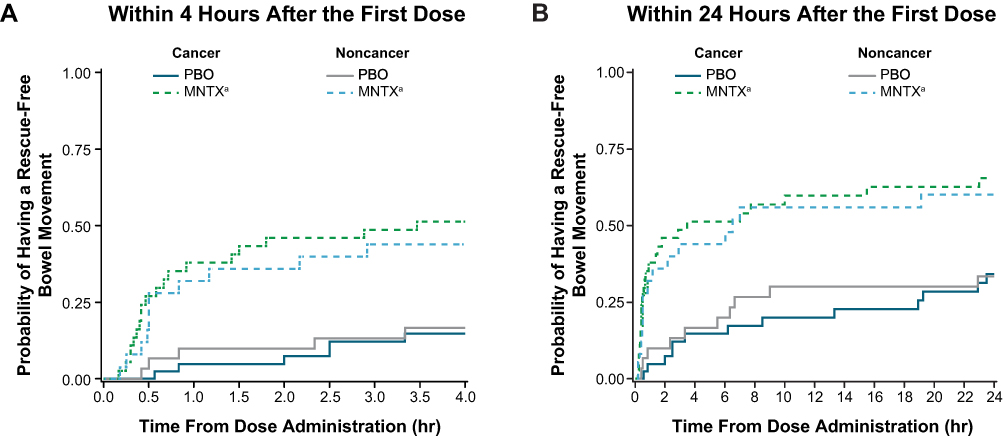 |
Figure 2 Probability of rescue-free laxation (A) within 4 hours after the first dose and (B) within 24 hours after the first dose (pooled ITT population). Abbreviations: hr, hour; ITT, intent to treat; MNTX, methylnaltrexone; PBO, placebo. Notes: Among patients with cancer, n = 114 for PBO; n = 116 for MNTX. Among patients without cancer, n = 71 for PBO; n = 62 for MNTX. aP < 0.001 vs PBO. |
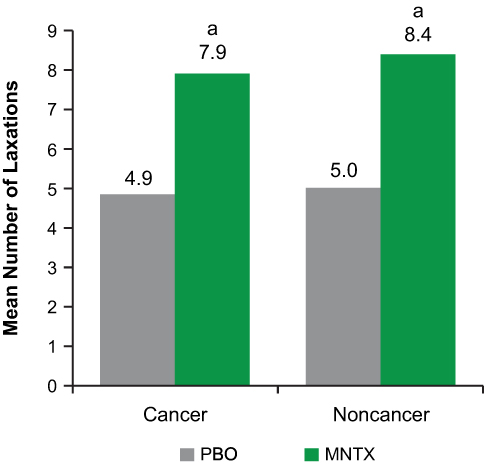 |
Figure 3 Mean weekly number of laxations within 24 hours after dosing by week 2 (pooled ITT population). Abbreviations: ITT, intent to treat; MNTX, methylnaltrexone; PBO, placebo. Notes: Among patients with cancer, n = 99 for PBO; n = 105 for MNTX. Among patients without cancer, n = 68 for PBO; n = 59 for MNTX. aP<0.0001 vs PBO. |
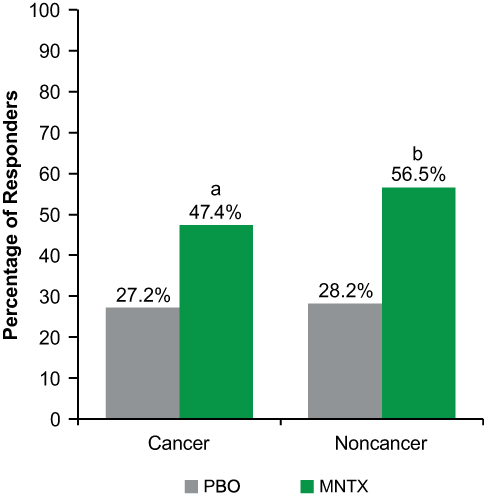 |
Figure 4 Responders with ≥3 rescue-free laxations per week in both weeks 1 and 2 (pooled ITT population). Abbreviations: ITT, intent to treat; MNTX, methylnaltrexone; PBO, placebo. Notes: Among patients with cancer, n = 114 for PBO; n = 116 for MNTX. Among patients without cancer, n = 71 for PBO; n = 62 for MNTX. aP=0.0015 vs PBO; bP = 0.0010 vs PBO. |
Rescue Medication Use and Pain Scores
Smaller proportions of methylnaltrexone-treated patients in both the cancer and noncancer groups required the use of rescue laxatives compared with cancer and noncancer patients receiving placebo. However, these differences did not reach significance (Figure 5). There were no significant changes in current pain scores from baseline to day 7 post-dose among patients treated with methylnaltrexone or placebo in both the cancer (P = 0.7043) and noncancer groups (P = 0.6075). Among patients with cancer, current pain scores were 3.6 at baseline and 2.9 at day 7 post-dose for those receiving methylnaltrexone and 3.5 at baseline and 3.2 at day 7 post-dose for those receiving placebo. Baseline and day 7 post-dose current pain scores for patients without cancer were 4.4 and 3.6, respectively, among those receiving methylnaltrexone and 4.0 and 3.5, respectively, among those receiving placebo. Similarly, worst pain scores were not significantly different from baseline to day 7 post-dose in cancer (P = 0.9200) and noncancer (P = 0.7800) patients treated with methylnaltrexone or placebo. Among patients with cancer, worst pain scores were 5.1 at baseline and 4.0 at day 7 post-dose for those receiving methylnaltrexone and 5.2 at baseline and 4.3 at day 7 post-dose for those receiving placebo. For those without cancer, worst pain scores at baseline and day 7 post-dose were 5.6 and 4.7, respectively, for methylnaltrexone and 5.4 and 4.4, respectively, for placebo.
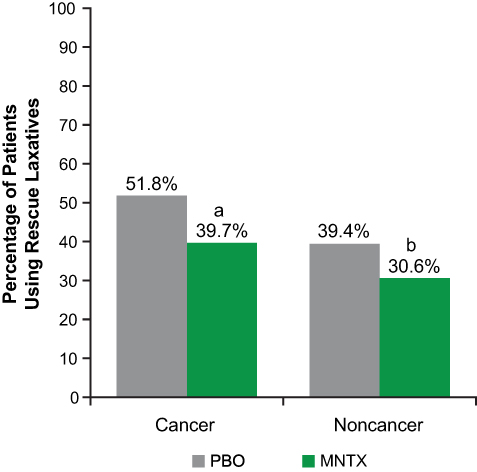 |
Figure 5 Patients using rescue laxatives (pooled ITT population). Abbreviations: ITT, intent to treat; MNTX, methylnaltrexone; PBO, placebo. Notes: Among patients with cancer, n = 114 for PBO; n = 116 for MNTX. Among patients without cancer, n = 71 for PBO; n = 62 for MNTX. aP = 0.0655 vs PBO; bP = 0.2900 vs PBO. |
Adverse Events
Overall, slightly higher proportions of cancer patients (methylnaltrexone group: 87.9% [n = 102]; placebo group: 79.8% [n = 91]) versus noncancer patients (methylnaltrexone group: 69.8% [n = 44]; placebo group: 70.4% [n = 50]) experienced TEAEs. Table 2 shows TEAEs occurring in >5% of patients in any treatment group. The most frequently occurring TEAEs in cancer patients who received methylnaltrexone or placebo included abdominal pain (24.1% [n = 28] and 9.6% [n = 11], respectively), disease progression (8.6% [n = 10] and 14.0% [n = 16], respectively), and nausea (14.7% [n = 17] and 14.0% [n = 16], respectively). Similar TEAEs were reported in the noncancer cohort. The most frequently occurring TEAEs reported in noncancer patients receiving methylnaltrexone or placebo included abdominal pain (17.5% [n = 11] and 11.3% [n = 8], respectively), nausea (4.8% [n = 3] and 9.9% [n=7], respectively), and diarrhea (4.8% [n = 3] and 8.5% [n = 6], respectively). Serious AEs were reported more commonly in methylnaltrexone-treated patients with cancer (17.2% [n = 20]) compared with those without cancer (7.9% [n = 5]). Serious AEs of disease progression (methylnaltrexone, 7.8% [n = 9]; placebo, 11.4% [n = 13]) and malignant neoplasm progression (methylnaltrexone, 5.2% [n = 6]; placebo, 10.5% [n = 12]) were reported in cancer patients. Other serious AEs occurring in ≥2 cancer patients were fall (methylnaltrexone, 0%; placebo, 1.8% [n = 2]), spinal cord compression (methylnaltrexone, 0%; placebo, 1.8% [n = 2]), and dyspnea (methylnaltrexone, 0%; placebo, 1.8% [n = 2]). Serious AEs occurring in ≥2 noncancer patients were aggravated congestive cardiac failure (methylnaltrexone, 1.6% [n = 1]; placebo, 1.4% [n = 1]) and concomitant disease progression (methylnaltrexone, 3.2% [n = 2]; placebo, 1.4% [n = 1]).
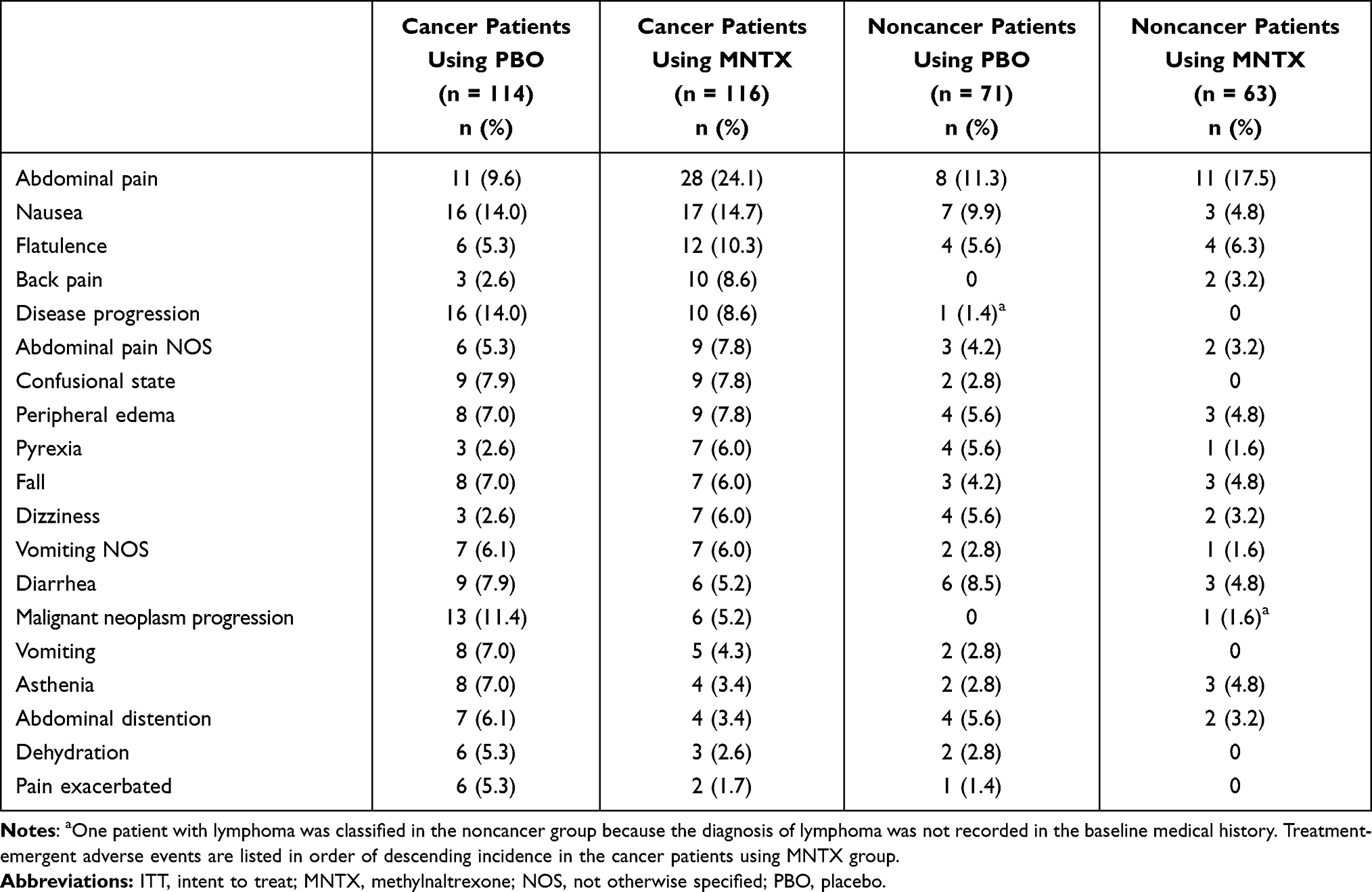 |
Table 2 Treatment-Emergent Adverse Events Occurring in at Least 5% of Patients in Any Treatment Group (Pooled ITT Population) |
Discussion
Nearly two-thirds of patients included in this pooled post hoc analysis had cancer. Baseline characteristics were similar between cancer and noncancer patients, with the exception that cancer patients were receiving a higher dose of opioid morphine equivalents at baseline. Despite this, along with several nonopioid-related factors that could contribute to constipation in cancer patients (eg, cancer-related physiologic dysfunction, concomitant medications, dehydration, immobility, diet, or metabolic causes),11 the percentage of patients achieving a laxation response was similar in cancer and noncancer patients and significantly greater than placebo. Methylnaltrexone induced laxation within 4 hours after administration of the first dose in the majority of patients with and without cancer, versus less than 20% of patients who received placebo. Similar results were obtained within 4 hours after at least 2 of the first 4 doses of methylnaltrexone. The laxation effect of methylnaltrexone was achieved rapidly within 1 hour among the majority of patient responders. Overall, the time to RFL was significantly reduced after treatment with methylnaltrexone compared with placebo. The mean number of weekly laxations within 24 hours of study drug administration by week 2 was significantly higher with methylnaltrexone versus placebo. Among both cancer and noncancer groups, significantly higher proportions of patients receiving methylnaltrexone versus placebo achieved ≥3 RFL per week in both weeks 1 and 2. These results show that methylnaltrexone effectively reduces OIC in cancer patients, despite the likelihood that nonopioid-related factors contributed to constipation in this population and support the use of SC methylnaltrexone in patients with active cancer taking opioids for cancer-related pain.
The laxation response associated with methylnaltrexone decreased the need for rescue laxatives in both patients with and without cancer. Importantly, there were no significant changes from baseline to day 7 post-dose in current or worst pain scores for cancer and noncancer patients receiving methylnaltrexone or placebo. These results demonstrate that methylnaltrexone therapy allowed patients to continue their opioid treatment without experiencing an increase in pain while reducing their constipation.
Consistent with prior studies in patients with advanced illnesses, this study showed that methylnaltrexone was well tolerated in cancer and noncancer patients.13,29–31 Adverse events and serious AEs occurred more frequently in cancer patients, likely as a result of their underlying disease and treatment. Although AEs such as abdominal pain and nausea occurred more frequently with methylnaltrexone, this may have been due to the increased laxation response observed with treatment.33 The AE profile of methylnaltrexone does not suggest symptoms associated with opioid withdrawal, confirming the drug’s selective effect for peripheral μ-opioid receptors.30,31,33
Serious AEs of disease progression and malignant neoplasm progression were reported in cancer patients during these studies. It is important to note that these patients were taking higher doses of opioids at baseline than noncancer patients, and that, in advanced cancer patients, peripheral μ-opioid receptors may play a role in disease progression.24,25,34 Indeed, cellular, animal and human data suggest that targeting these receptors may have potential as anticancer therapy.17,24,25,35 Based on this evidence, Janku et al examined the potential effects of methylnaltrexone on survival.24 Findings revealed significantly longer overall survival times for cancer patients treated with methylnaltrexone versus placebo, and even greater benefits were observed in those patients who had a laxation response to methylnaltrexone. No treatment-related differences in overall survival were observed in noncancer patients. Collectively, these findings may suggest a direct effect of methylnaltrexone on cellular tumor targets related to peripheral μ-opioid receptors24 that could result in the slowing of disease progression. It is unclear if other factors related to OIC relief such as indirect effects on gut function and immunosuppression may be involved in mitigating cancer progression.21,22,24,36,37 Moreover, constipation may be a risk factor for reduced survival as it relates to patients’ global quality of life,21 performance status, including decreased appetite and anorexia-cachexia syndrome,21,22 as well as increased intestinal permeability.38
Data from the current post hoc analysis cannot provide conclusions regarding the effect of opioids on cancer and survival, but they do indicate that methylnaltrexone was safe and effective in an advanced cancer population and that no differences in laxation response to methylnaltrexone were observed between cancer and noncancer patients. These preliminary results provide a basis for a better understanding of the clinical effects of methylnaltrexone in cancer patients who are receiving opioids and help to support future studies of methylnaltrexone as a potential treatment for cancer.
This post hoc analysis has some limitations. The two studies pooled in this analysis were not initially designed to compare outcomes for cancer versus noncancer patients. In addition, the trials were of short duration given the patients’ advanced illnesses. The effect of methylnaltrexone over a 10-week open-label extension was found to be generally consistent with that of a 2-week randomized controlled trial, though again patients were not stratified by cancer/noncancer.29 Given the advanced-illness diagnoses in this population, these patients were inherently very ill; AEs observed during the study could possibly be attributable to underlying disease.
Conclusions
Treatment with methylnaltrexone resulted in significantly higher proportions of both cancer and noncancer patients with OIC achieving laxation responses within 4 hours of administration compared with placebo. Additionally, among those achieving a laxation response, laxation occurred significantly faster with methylnaltrexone than placebo and was associated with a reduced need for rescue laxatives and no significant changes in pain. Methylnaltrexone was also generally well tolerated in all patient groups. These results show that methylnaltrexone effectively reduces OIC in cancer patients as well as noncancer patients, despite the several nonopioid-related factors that may contribute to constipation in the prior population, and support the approval and use of SC methylnaltrexone for OIC in patients with active cancer taking opioids for cancer-related pain.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available at this time due to the proprietary nature of this information. Requests for additional information should be made to the corresponding author.
Acknowledgments
The study was funded by Salix Pharmaceuticals, a division of Bausch Health US, LLC, Bridgewater, NJ, USA, which has licensed the rights to develop and commercialize Relistor® from Progenics Pharmaceuticals, Inc., New York, NY, USA a wholly owned subsidiary of Lantheus Holdings, Inc., North Billerica, MA, USA. Progenics Pharmaceuticals had a role in the study design, implementation of the study, and data collection. Salix had a role in the data collection, data analysis, and the decision to publish. Technical editorial and medical writing assistance was provided under the direction of the authors by Echelon Brand Communications, LLC, an OPEN Health company, Parsippany, NJ, USA. Funding for this support was provided by Salix Pharmaceuticals.
Previous presentations
International Association for the Study of Pain 17th World Congress on Pain; September 12–16, 2018; Boston, MA. American Society of Regional Anesthesia and Pain Medicine, Annual Pain Medicine Meeting; November 15–17, 2018; San Antonio, TX.
Disclosure
Dr. Chamberlain has nothing to disclose. Dr. Israel is an employee of Bausch Health US, LLC, which has a proprietary interest in methylnaltrexone. Dr. Rhiner has received a grant from Wyeth Pharmaceuticals for the 302 study mentioned in this manuscript and was reimbursed by Salix Pharmaceuticals for travel expenses related to poster presentations at the 2018 World Congress on Regional Anesthesia & Pain Medicine and the 2018 Palliative and Supportive Care in Oncology meeting. Dr. Slatkin is an employee of Salix Pharmaceuticals since July 2016, has received personal fees from Salix Pharmaceuticals for consulting/speaking between 2012 and 2016, and has received a grant from Progenics Pharmaceuticals for the 302 study mentioned in this manuscript. Dr. Stambler is an employee of Progenics Pharmaceuticals, Inc., a subsidiary of Lantheus Holdings Inc., New York, NY. The authors report no other conflicts of interest in this work.
References
1. van den Beuken-van Everdingen MH, Hochstenbach LM, Joosten EA, Tjan-Heijnen VC, Janssen DJ. Update on prevalence of pain in patients with cancer: systematic review and meta-analysis. J Pain Symptom Manage. 2016;51(6):1070–1090.e1079.
2. Pappagallo M. Incidence, prevalence, and management of opioid bowel dysfunction. Am J Surg. 2001;182(suppl5A):11S–18S. doi:10.1016/S0002-9610(01)00782-6
3. Glare P, Walsh D, Sheehan D. The adverse effects of morphine: a prospective survey of common symptoms during repeated dosing for chronic cancer pain. Am J Hosp Palliat Care. 2006;23(3):229–235. doi:10.1177/1049909106289068
4. Moore RA, McQuay HJ. Prevalence of opioid adverse events in chronic non-malignant pain: systematic review of randomised trials of oral opioids. Arthritis Res Ther. 2005;7(5):R1046–1051. doi:10.1186/ar1782
5. Muller-Lissner S, Bassotti G, Coffin B, et al. Opioid-induced constipation and bowel dysfunction: a clinical guideline. Pain Med. 2017;18(10):1837–1863.doi: 10.1093/pm/pnw255
6. Weschules DJ, Bain KT, Reifsnyder J, et al. Toward evidence-based prescribing at end of life: a comparative analysis of sustained-release morphine, oxycodone, and transdermal fentanyl, with pain, constipation, and caregiver interaction outcomes in hospice patients. Pain Med. 2006;7(4):320–329. doi:10.1111/j.1526-4637.2006.00184.x
7. Bell TJ, Panchal SJ, Miaskowski C, Bolge SC, Milanova T, Williamson R. The prevalence, severity, and impact of opioid-induced bowel dysfunction: results of a US and European patient survey (PROBE 1). Pain Med. 2009;10(1):35–42. doi:10.1111/j.1526-4637.2008.00495.x
8. Fumita S, Imai H, Harada T, et al. Patients’ self-assessment of the symptoms and impact of opioid-induced constipation: results from a prospective observational cohort study of Japanese patients with cancer. J Pain Symptom Manage. 2020;59(5):1043–1051.e1042. doi:10.1016/j.jpainsymman.2019.11.021
9. Kumar L, Barker C, Emmanuel A. Opioid-induced constipation: pathophysiology, clinical consequences, and management. Gastroenterol Res Pract. 2014;2014:141737. doi:10.1155/2014/141737
10. Nee J, Zakari M, Sugarman MA, et al. Efficacy of treatments for opioid-induced constipation: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2018;16(10):1569–1584. doi:10.1016/j.cgh.2018.01.021
11. Wickham RJ. Managing constipation in adults with cancer. J Adv Pract Oncol. 2017;8(2):149–161.
12. Galligan JJ, Sternini C. Insights into the role of opioid receptors in the GI tract: experimental evidence and therapeutic relevance. Handb Exp Pharmacol. 2017;239:363–378. doi:10.1007/164_2016_116
13. Slatkin N, Thomas J, Lipman AG, et al. Methylnaltrexone for treatment of opioid-induced constipation in advanced illness patients. J Support Oncol. 2009;7(1):39–46.
14. Yuan CS, Foss JF, O’Connor M, Toledano A, Roizen MF, Moss J. Methylnaltrexone prevents morphine-induced delay in oral-cecal transit time without affecting analgesia: a double-blind randomized placebo-controlled trial. Clin Pharmacol Ther. 1996;59(4):469–475. doi:10.1016/S0009-9236(96)90117-4
15. Viscusi ER. Clinical overview and considerations for the management of opioid-induced constipation in patients with chronic noncancer pain. Clin J Pain. 2019;35(2):174–188. doi:10.1097/AJP.0000000000000662
16. Yao YS, Yao RY, Zhuang LK, et al. MOR1 expression in gastric cancer: a biomarker associated with poor outcome. Clin Transl Sci. 2015;8(2):137–142. doi:10.1111/cts.12246
17. Zylla D, Gourley BL, Vang D, et al. Opioid requirement, opioid receptor expression, and clinical outcomes in patients with advanced prostate cancer. Cancer. 2013;119(23):4103–4110. doi:10.1002/cncr.28345
18. Novy DM, Nelson DV, Koyyalagunta D, Cata JP, Gupta P, Gupta K. Pain, opioid therapy, and survival: a needed discussion. Pain. 2020;161(3):496–501. doi:10.1097/j.pain.0000000000001736
19. Zylla D, Kuskowski MA, Gupta K, Gupta P. Association of opioid requirement and cancer pain with survival in advanced non-small cell lung cancer. Br J Anaesth. 2014;113(Suppl 1):i109–i116. doi:10.1093/bja/aeu351
20. Candrilli SD, Davis KL, Iyer S. Impact of constipation on opioid use patterns, health care resource utilization, and costs in cancer patients on opioid therapy. J Pain Palliat Care Pharmacother. 2009;23(3):231–241. doi:10.1080/15360280903098440
21. Brown J, Thorpe H, Napp V, et al. Assessment of quality of life in the supportive care setting of the big lung trial in non-small-cell lung cancer. J Clin Oncol. 2005;23(30):7417–7427. doi:10.1200/JCO.2005.09.158
22. Lee YJ, Suh SY, Choi YS, et al. EORTC QLQ-C15-PAL quality of life score as a prognostic indicator of survival in patients with far advanced cancer. Support Care Cancer. 2014;22(7):1941–1948. doi:10.1007/s00520-014-2173-8
23. Fine PG, Chen YW, Wittbrodt E, Datto C. Impact of opioid-induced constipation on healthcare resource utilization and costs for cancer pain patients receiving continuous opioid therapy. Support Care Cancer. 2019;27(2):687–696. doi:10.1007/s00520-018-4366-z
24. Janku F, Johnson LK, Karp DD, Atkins JT, Singleton PA, Moss J. Treatment with methylnaltrexone is associated with increased survival in patients with advanced cancer. Ann Oncol. 2016;27(11):2032–2038. doi:10.1093/annonc/mdw317
25. Singleton PA, Moss J, Karp DD, Atkins JT, Janku F. The mu opioid receptor: a new target for cancer therapy? Cancer. 2015;121(16):2681–2688. doi:10.1002/cncr.29460
26. Chen DT, Pan JH, Chen YH, et al. The mu-opioid receptor is a molecular marker for poor prognosis in hepatocellular carcinoma and represents a potential therapeutic target. Br J Anaesth. 2019;122(6):e157–e167. doi:10.1016/j.bja.2018.09.030
27. Li Y, Li G, Tao T, et al. The mu-opioid receptor (MOR) promotes tumor initiation in hepatocellular carcinoma. Cancer Lett. 2019;453:1–9. doi:10.1016/j.canlet.2019.03.038
28. Relistor [package insert]. Bridgewater, NJ: Salix Pharmaceuticals; 2018.
29. Bull J, Wellman CV, Israel RJ, Barrett AC, Paterson C, Forbes WP. Fixed-dose subcutaneous methylnaltrexone in patients with advanced illness and opioid-induced constipation: results of a randomized, placebo-controlled study and open-label extension. J Palliat Med. 2015;18(7):593–600. doi:10.1089/jpm.2014.0362
30. Michna E, Blonsky ER, Schulman S, et al. Subcutaneous methylnaltrexone for treatment of opioid-induced constipation in patients with chronic, nonmalignant pain: a randomized controlled study. J Pain. 2011;12(5):554–562. doi:10.1016/j.jpain.2010.11.008
31. Thomas J, Karver S, Cooney GA, et al. Methylnaltrexone for opioid-induced constipation in advanced illness. N Engl J Med. 2008;358(22):2332–2343. doi:10.1056/NEJMoa0707377
32. Murphy DB, Sutton JA, Prescott LF, Murphy MB. Opioid-induced delay in gastric emptying: a peripheral mechanism in humans. Anesthesiology. 1997;87(4):765–770. doi:10.1097/00000542-199710000-00008
33. Slatkin NE, Lynn R, Su C, Wang W, Israel RJ. Characterization of abdominal pain during methylnaltrexone treatment of opioid-induced constipation in advanced illness: a post hoc analysis of two clinical trials. J Pain Symptom Manage. 2011;42(5):754–760. doi:10.1016/j.jpainsymman.2011.02.015
34. Zylla D, Steele G, Shapiro A, Richter S, Gupta P. Impact of opioid use on health care utilization and survival in patients with newly diagnosed stage IV malignancies. Support Care Cancer. 2018;26(7):2259–2266. doi:10.1007/s00520-018-4062-z
35. Singleton PA, Garcia JG, Moss J. Synergistic effects of methylnaltrexone with 5-fluorouracil and bevacizumab on inhibition of vascular endothelial growth factor-induced angiogenesis. Mol Cancer Ther. 2008;7(6):1669–1679. doi:10.1158/1535-7163.MCT-07-2217
36. Cheng WF, Chen LK, Chen CA, et al. Chimeric DNA vaccine reverses morphine-induced immunosuppression and tumorigenesis. Mol Ther. 2006;13(1):203–210. doi:10.1016/j.ymthe.2005.06.479
37. Boehncke S, Hardt K, Schadendorf D, Henschler R, Boehncke WH, Duthey B. Endogenous mu-opioid peptides modulate immune response towards malignant melanoma. Exp Dermatol. 2011;20(1):24–28. doi:10.1111/j.1600-0625.2010.01158.x
38. Annahazi A, Ferrier L, Bezirard V, et al. Luminal cysteine-proteases degrade colonic tight junction structure and are responsible for abdominal pain in constipation-predominant IBS. Am J Gastroenterol. 2013;108(8):1322–1331. doi:10.1038/ajg.2013.152
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.