Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Subclinical Hypothyroidism is Associated with Cognitive Impairment in Patients with Cerebral Small Vessel Disease
Received 10 December 2022
Accepted for publication 27 January 2023
Published 3 February 2023 Volume 2023:19 Pages 303—310
DOI https://doi.org/10.2147/NDT.S401020
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Zhenjie Teng,1– 3,* Jing Feng,4,* Peiyuan Lv1– 3
1Department of Neurology, Hebei Medical University, Shijiazhuang, People’s Republic of China; 2Department of Neurology, Hebei General Hospital, Shijiazhuang, People’s Republic of China; 3Hebei Provincial Key Laboratory of Cerebral Networks and Cognitive Disorders, Shijiazhuang, People’s Republic of China; 4Department of Endocrinology, Hebei General Hospital, Shijiazhuang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Peiyuan Lv, Department of Neurology, Hebei General Hospital, 348 Heping West Road, Shijiazhuang, Hebei Province, 050051, People’s Republic of China, Tel/Fax +86 31185988906, Email [email protected]
Objective: To investigate the association between subclinical hypothyroidism (SCH) and cognitive function in patients with cerebral small vessel disease (CSVD).
Methods: We evaluated 528 patients with CSVD in this retrospective study. SCH was defined as elevated levels of thyroid stimulating hormone with normal concentrations of free thyroxine. Magnetic resonance imaging was performed to assess the total CSVD burden score and the Montreal Cognitive Assessment was used to measure the cognitive function. Participants were grouped based on cognitive function or total CSVD burden score. Multivariate logistic regression and mediation analysis models were used to estimate the association of SCH with cognitive function and CSVD burden.
Results: SCH was an independent risk factor for cognitive impairment in patients with CSVD after adjustment for potential confounding factors (OR: 1.939; 95% CI: 1.170 to 3.213; P=0.010). Additionally, SCH was independently associated with severe CSVD burden after adjustment for potential confounding factors (OR: 1.668; 95% CI: 1.085 to 2.564; P=0.020). Mediation analysis found a significant moderating effect (P=0.021) of the severe CSVD burden on the relation between SCH and cognitive impairment after adjustment for potential confounding factors. A 30.1% of the total effect between this relation was attributable to the presence of severe CSVD burden.
Conclusion: SCH was associated with an increased risk of cognitive impairment in patients with CSVD. The mediating role of severe CSVD burden suggests that SCH may lead to cognitive impairment through the presence of severe CSVD burden. These findings may suggest strategies for screening for SCH in the context of cognitive impairment in patients with severe CSVD.
Keywords: subclinical hypothyroidism, cognitive function, cerebral small vessel disease
Introduction
Subclinical hypothyroidism (SCH), defined as an elevated thyroid-stimulating hormone (TSH) level with a normal free thyroxine (FT4) concentration, affects 3–15% of the adult population.1,2 Thyroid dysfunction, including SCH, has been considered as a potentially treatable or reversible factor in cognitive impairment, and therefore thyroid function tests have been recommended in clinical guidelines as a basic component in the diagnosis of cognitive impairment.3–6 However, numerous scientific researches on the effect of SCH on cognitive function have yielded inconsistent findings. Several studies have suggested that SCH is associated with a heightened risk of cognitive impairment.7–10 On the other hand, recent studies have suggested no association between SCH and cognitive impairment or dementia.11,12 Differences in the results of these trials may be due to differences in age, sex and clinical setting.
Cerebral small vessel disease (CSVD) is commonly recognized as one of the significant causes of cognitive impairment or dementia.13 CSVD is a whole-brain disorder of cerebral microvessels that causes several common abnormalities seen on brain magnetic resonance imaging (MRI), such as white matter hyperintensity (WMH), cerebral microbleeds (CMBs), lacunes, enlarged perivascular spaces (EPVS) and brain atrophy.13–15 Recent studies have indicated that endothelial dysfunction plays a pivotal role in the pathogenesis of CSVD.16,17 Interestingly, SCH may lead to vascular disturbances and arteriolosclerosis by vascular-mediated mechanisms,2,18,19 which may accelerate the progression of CSVD.16 Therefore, CSVD should be considered when exploring the relationship between SCH and cognitive function, which is rarely done.
In this study, we attempt to investigate the association of SCH with cognitive function in patients with CSVD and further evaluate whether the total CSVD burden has an effect on this association.
Materials and Methods
Participants
Between September 2016 and December 2021, a total of 528 eligible participants who were admitted to Hebei General Hospital were included in this study. Inclusion criteria were as follows: (1) aged 40 years and older; (2) have whole MRI sequences for calculating total CSVD burden scores; (3) own at least one imaging marker of CSVD: severe WMH, one or more lacunes, one or more deep CMBs, or moderate to severe EPVS in basal ganglia; (4) completed thyroid function tests and cognitive function assessment. Exclusion criteria were as follows: (1) hyperthyroidism or overt hypothyroidism; (2) history of thyroid diseases; (3) treated with thyroid hormone-related medication; (4) some specific conditions have an effect on cognition, including acute vascular events, anxiety, depression, schizophrenia, malignancy, epilepsy and severe hepatorenal dysfunction.
Assessment of Clinical Data
The following clinical and laboratory factors were collected: age, sex, education level, body mass index, systolic and diastolic blood pressure, current smoking or drinking, and history of stroke, hypertension, diabetes, coronary heart disease, medication use. Laboratory examination results including thyroid function tests, lipid profile, serum total homocysteine (tHcy) and uric acid were evaluated after 8 hours of overnight fasting. Lipid profile was assayed using an automatic biochemical analyzer and tHcy was evaluated by the enzyme circulation method. Serum TSH and FT4 levels were evaluated using an automated electrochemiluminescence immunoassay. Based on published criteria, the normal reference range is 0.45 to 4.49 mIU/L for serum TSH and 12 to 22 pmol/L for FT4.2,11,12 SCH was defined as a serum TSH concentration of 4.50 to 20 mIU/L and FT4 levels within the reference range.11
Assessment of Total CSVD Burden Scores
Brain MRI (3.0 Tesla, Signa, GE Healthcare, USA) was used to assess imaging markers of CSVD. All patients underwent T1-weighted imaging, T2-weighted imaging, fluid-attenuated inversion recovery and susceptibility weighted imaging. The detailed parameter settings for the four sequences were recorded in our previous studies.20,21 The definition of imaging markers of CSVD was based on the Standards for Reporting Vascular Changes on Neuroimaging (STRIVE).14 The severity of periventricular and deep WMH was evaluated using the Fazekas rating scale.22 CMBs in deep were evaluated using the Microbleed Anatomical Rating Scale.23 The number of EPVS in the basal ganglia or lacunes was recorded. According to the semi-quantitative rating scale, we graded the EPVS into five levels (0 = no EPVS, 1 = 1 to 10 EPVS, 2 = 11 to 20 EPVS, 3 = 21 to 40 EPVS and 4 ≥40 EPVS).24 We used the total CSVD burden scores (range 0 to 4) combining four imaging markers of CSVD to evaluate the severity of overall CSVD. One score was awarded for each of the following: the Fazekas score of periventricular WMH was 3 and/or deepWMH was ≥2, at least one lacunes, one or more CMBs in deep and the grade EPVS in basal ganglia ≥2.25,26 Total CSVD burden scores ≤2 were classified as mild CSVD burden and above 2 categorized as severe CSVD burden.27,28
Assessment of Cognitive Function
In this study, cognitive function was evaluated with standardized translated version of Montreal Cognitive Assessment (MoCA) Beijing version (mocacognition.com). The Hamilton anxiety scale of 14 items and Hamilton depression scale of 24 items were used to assess anxiety or depression. According to previous studies,29 the diagnosis of cognitive impairment was based on the optimal cut-off scores of MoCA: 0–13 for illiterate, 0–19 for 1–6 years of education, 0–24 for 7 or more years of education for Chinese adults.
Statistical Analysis
Statistical analyses were performed using R, version 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria) and SPSS 26.0 (IBM corporation, Armonk, NY). Variables were analyzed by Mann–Whitney U, Student’s t-tests or χ2 tests, as appropriate. Variables with P < 0.1 were forced into the multivariate logistic regression model as covariates to investigate the association of SCH with cognitive impairment or severe CSVD burden. Mediation analysis was performed to evaluate whether severe CSVD burden has an effect on the association between SCH and cognitive impairment by using bruceR and mediation packages in R. All numeric predictors have been mean-centered in the simple mediation model (Model 4). The number of bootstrap samples in mediation analysis was set to 5000 to obtain a more reliable value of the effect size. P < 0.05 was considered statistically significant.
Results
Participants Characteristics
This retrospective study included 528 participants with CSVD. The median (IQR) age was 69 (62–75) and 53.0% (n = 280) were male. Based on the scores of MoCA, participants were divided into no cognitive impairment group (n = 220) and cognitive impairment group (n = 308) and based on the scores of total CSVD burden, were divided into mild CSVD burden group (n = 285) and severe CSVD burden group (n = 243). The characteristics of all participants in different groups are shown in Table 1 and Table 2.
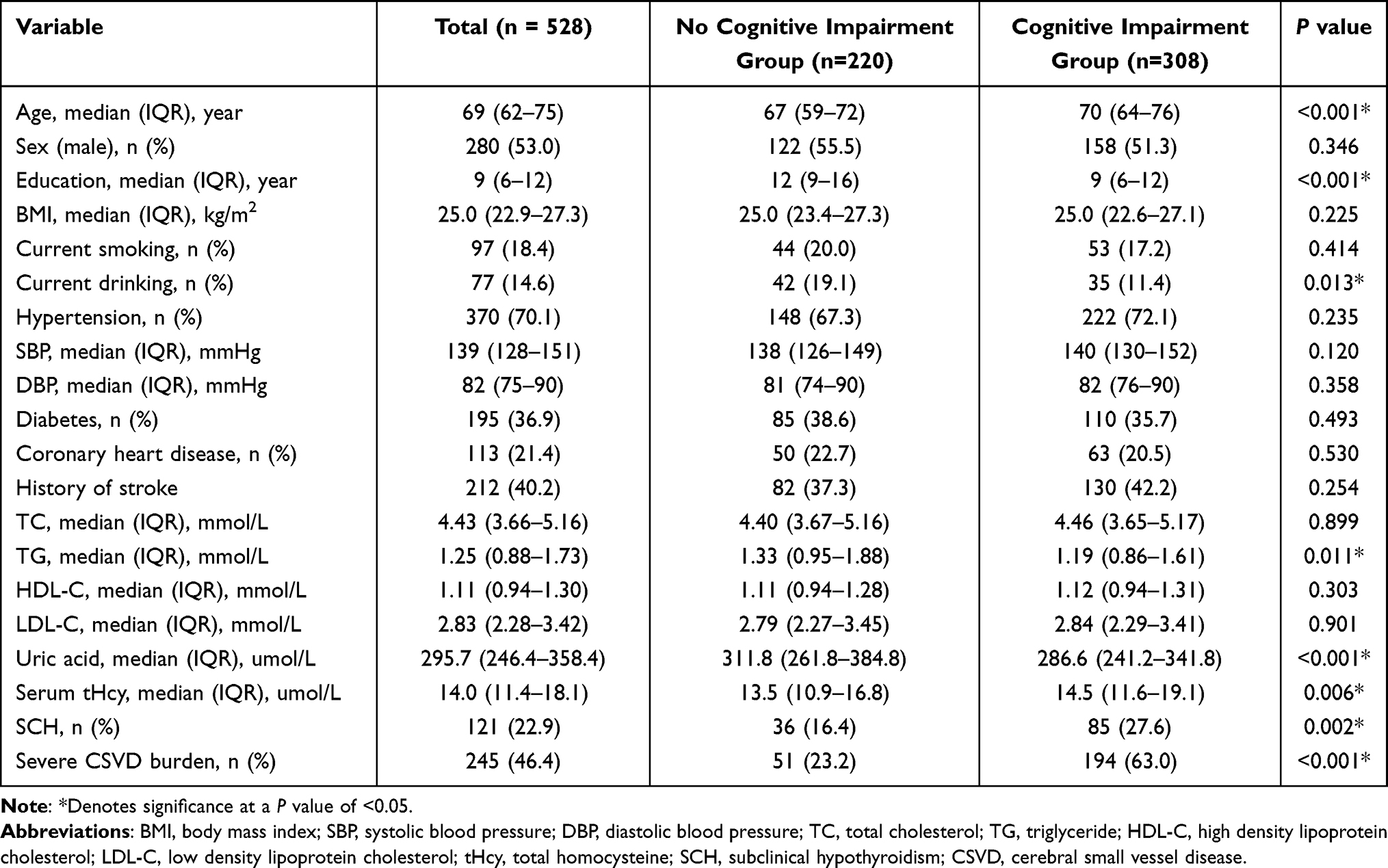 |
Table 1 Characteristics of Participants Between No Cognitive Impairment and Cognitive Impairment Group |
 |
Table 2 Characteristics of Participants Between Mild CSVD Burden and Severe CSVD Burden |
Between no cognitive impairment and cognitive impairment group, statistically significant differences were found in age, education level, current drinking, triglyceride, uric acid, serum tHcy, severe CSVD burden and SCH (P<0.05) (Table 1). Between mild and severe CSVD burden group, statistically significant differences were found in age, education level, history of hypertension or stroke, diastolic blood pressure, serum tHcy and SCH (P<0.05) (Table 2).
Subclinical Hypothyroidism and Cognitive Impairment
The proportion of participants with SCH was significantly higher in the cognitive impairment group than no cognitive impairment group (P=0.002) (Table 1). In unadjusted logistic regression analysis, SCH was associated with cognitive impairment (OR: 1.948; 95% CI: 1.260 to 3.013; P=0.003). This trend remained significant (OR: 1.939; 95% CI: 1.170 to 3.213; P=0.010), after adjusting for age, education level, current drinking, triglyceride, uric acid, serum tHcy, and severe CSVD burden in multivariate logistic regression analysis (Figure 1).
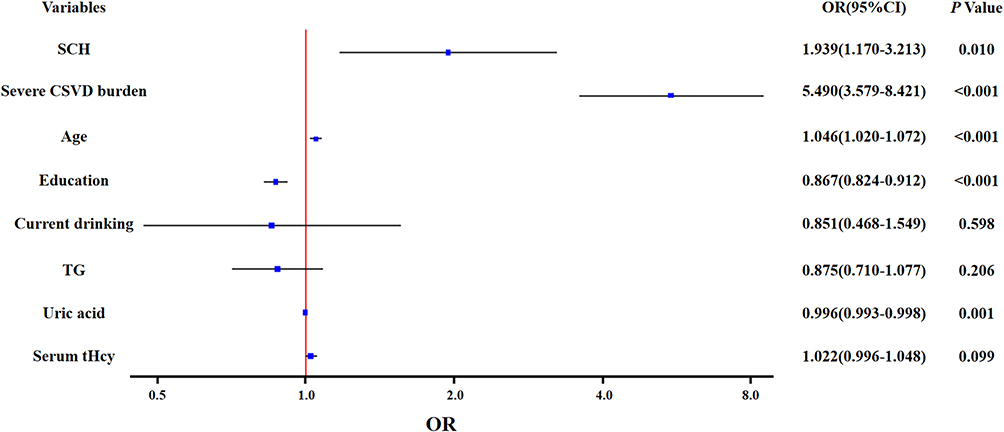 |
Figure 1 The logistic regression analyses between possible predictors and cognitive impairment. Abbreviations: SCH, subclinical hypothyroidism; CSVD, cerebral small vessel disease; TG, triglyceride. |
Subclinical Hypothyroidism and Cerebral Small Vessel Disease Burden
Compared with mild CSVD burden group, the frequencies of SCH were significantly higher in severe CSVD burden group (P=0.014) (Table 2). In unadjusted logistic regression analysis, SCH was associated with severe CSVD burden (OR: 1.667; 95% CI: 1.107 to 2.510; P=0.014). The association remained significant (OR: 1.668; 95% CI: 1.085 to 2.564; P=0.020), after adjustment of potential confounders, such as age, education level, history of hypertension or stroke, diastolic blood pressure, and serum tHcy in multivariate logistic regression analysis (Figure 2).
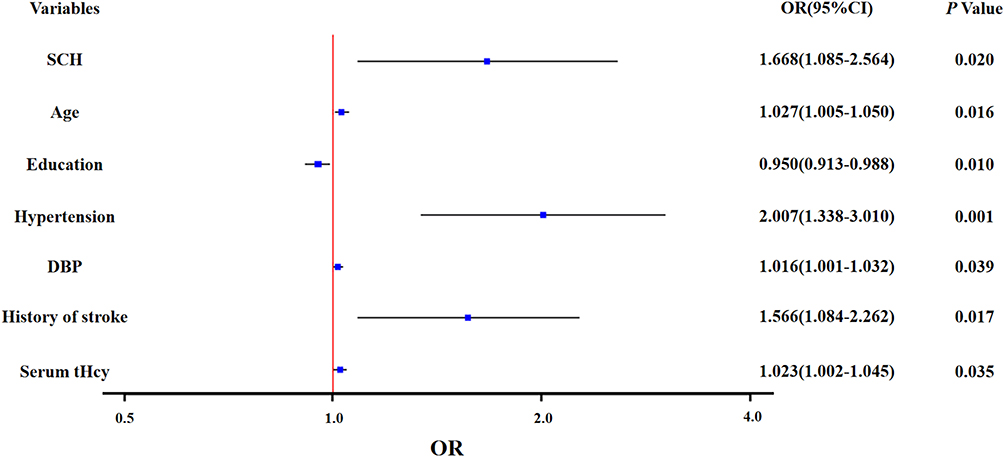 |
Figure 2 The logistic regression analyses between possible predictors and severe CSVD burden. Abbreviations: SCH, subclinical hypothyroidism; DBP, diastolic blood pressure. |
Mediation by Severe CSVD Burden
The result of the mediation analysis model is shown in Figure 3. The direct effect (c’), total effect (c) and mediating (ie, indirect) effect (ab) of severe CSVD burden were statistically significant for SCH in association with cognitive impairment after adjusting for age, education level and serum tHcy (c = 0.153, P=0.001; c’=0.107, P=0.016; ab = 0.046; P=0.021; respectively). 30.1% (ab/c) of the total effect between the association of SCH and cognitive impairment was attributable to the presence of severe CSVD burden.
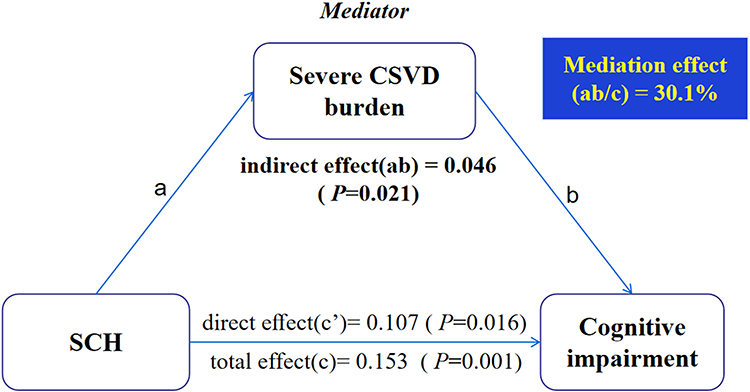 |
Figure 3 Mediation analysis is shown for the presence of severe CSVD burden as a mediator in the relation between SCH and cognitive impairment. Abbreviations: SCH, subclinical hypothyroidism; CSVD, cerebral small vessel disease. |
Discussion
This study demonstrated that SCH is associated with an increased risk of cognitive impairment and severe CSVD burden in patients with CSVD. These associations remained significant after accounting for potential confounders. Furthermore, the association between SCH and cognitive impairment appeared to be mediated by the severe CSVD burden, which partially supported the hypothesis that SCH may lead to severe CSVD burden, which in turn may lead to cognitive impairment.
Thyroid hormones have a wide-ranging effect on the central nervous system. Several previous studies have focused on the association between SCH and cognitive function and reported controversial results. A study involving 337 outpatients aged 64 to 86 suggested that SCH is associated with cognitive impairment.30 In addition, another cross-sectional study of 1750 community-dwelling population indicated that the presence of SCH is an independent risk factor for mild cognitive impairment after adjusting for adjustment for age, sex and education.9 More importantly, existing clinical guidelines recommend screening for subclinical thyroid dysfunction to prevent cognitive impairment or dementia.3,5,11 Consistent with these studies, we found that SCH was associated with an increased risk of cognitive impairment in patients with CSVD. Although the exact mechanism remains elusive, several potential candidate mechanisms for this association have been proposed, including endothelial dysfunction, cerebral hypoperfusion, chronic inflammation and other vascular risk factors.31,32
However, in contrast to our study, two meta-analyses found that SCH was not associated with cognitive impairment in participants older than 60 years33 or 75 years.10 Another subsequent meta-analysis of 11 prospective cohorts showed no association between SCH and cognitive decline or dementia.34 Similarly, no association between SCH and the risk of Alzheimer’s disease was found in recent meta-analyses.35 A further study, combining 74,565 participants from 23 cohorts, confirmed that SCH was not associated with cognitive decline or risk of dementia.11 The underlying cause of this discrepancy may be related to age, gender, vascular risk factors of the enrolled population, outcome measures or even study design. As far as we know, none of the previous studies have taken CSVD into account when evaluated the association of SCH with cognitive function, although CSVD is one of the primary causes of cognitive impairment.13
CSVD is a dynamic, whole-brain disorder that is common observed among elderly individuals.13 Despite being a major cause of stroke and dementia, the underlying pathogenesis is incompletely understood. Substantial literature has indicated that endothelial dysfunction, hypoperfusion, inflammation and oxidative stress contribute to the development of CSVD.13,16,36,37 Interestingly, the factors mentioned above also contribute to potential pathophysiological mechanisms of the effect of SCH on the central nervous system.31,32 Therefore, SCH may accelerate the development of CSVD. SCH has been reported to be associated with EPVS in the stroke-free population38 or WMH and CMBs in subjects with minor ischemic stroke or transient ischemic attack.39 As there are interactions between individual imaging markers of CSVD, total CSVD burden scores may better represent the severity of CSVD.40 Consistent with the results of previous studies,38,39 we found that SCH was associated with an increased risk of severe CSVD burden after accounting for potential confounders, which may support the hypothesis that SCH may accelerate the development of CSVD.
As mentioned above, SCH was closely associated with both CSVD and cognitive impairment. CSVD should be taken into account when exploring the relationship between SCH and cognitive impairment, but to our knowledge very few do. In our study, SCH was associated with an increased risk of cognitive impairment when CSVD was taken into account. Moreover, we observed a significant moderating effect of the severe CSVD burden on the association between SCH and cognitive impairment. This finding may support the hypothesis that SCH may lead to the severe CSVD burden, which in turn may lead to cognitive impairment.
The main strength of the current study is that the CSVD population was enrolled and CSVD was taken into account when exploring the association between SCH and cognitive impairment. However, some limitations exist in our study. First, causality could not be established due to the cross-sectional design. However, the result of the mediation analysis in our study may support a causal pathway in which SCH may accelerate the development of CSVD, which in turn may lead to cognitive impairment. Second, participants in our study were recruited from a single center, which may have generated sampling bias. Third, repeat measurements of serum TSH and FT4 concentrations were not available in this retrospective study, which may lead to misclassification bias. Future prospective or longitudinal studies are warranted to address these issues.
Conclusions
In conclusion, our study found that SCH was associated with an increased risk of cognitive impairment in CSVD patients. More importantly, the association between SCH and cognitive impairment appeared to be mediated by the severe CSVD burden, which partially supported the hypothesis that SCH may lead to severe CSVD burden, which in turn may lead to cognitive impairment. These findings may suggest strategies for screening for SCH in the context of cognitive impairment in patients with severe CSVD.
Ethical Approval
The study followed the principles in the Declaration of Helsinki and was approved by the Ethical Committees of Hebei General Hospital (NO.2022171). We promised that the data of the participants were anonymized or maintained with confidentiality, and the rights or interests of participants were not be invaded. Therefore, the requirement for informed consent in this study was waived in accordance with the national legislation and the institutional requirements.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Peeters RP. Subclinical hypothyroidism. N Engl J Med. 2017;376(26):2556–2565. doi:10.1056/NEJMcp1611144
2. Biondi B, Cappola AR, Cooper DS. Subclinical hypothyroidism: a review. JAMA. 2019;22(2):153–160. doi:10.1001/jama.2019.9052
3. Sorbi S, Hort J, Erkinjuntti T, et al. EFNS-ENS guidelines on the diagnosis and management of disorders associated with dementia. Eur J Neurol. 2012;19(9):1159–1179. doi:10.1111/j.1468-1331.2012.03784.x
4. Muangpaisan W, Petcharat C, Srinonprasert V. Prevalence of potentially reversible conditions in dementia and mild cognitive impairment in a geriatric clinic. Geriatr Gerontol Int. 2012;12(1):59–64. doi:10.1111/j.1447-0594.2011.00728.x
5. Langa KM, Levine DA. The diagnosis and management of mild cognitive impairment: a clinical review. JAMA. 2014;312(23):2551–2561. doi:10.1001/jama.2014.13806
6. Ritchie M, Yeap BB. Thyroid hormone: influences on mood and cognition in adults. Maturitas. 2015;81(2):266–275. doi:10.1016/j.maturitas.2015.03.016
7. Tan ZS, Beiser A, Vasan RS, et al. Thyroid function and the risk of Alzheimer disease: the Framingham study. Arch Intern Med. 2008;168(14):1514–1520. doi:10.1001/archinte.168.14.1514
8. Zhu DF, Wang ZX, Zhang DR, et al. fMRI revealed neural substrate for reversible working memory dysfunction in subclinical hypothyroidism. Brain. 2006;129(Pt 11):2923–2930. doi:10.1093/brain/awl215
9. Juarez-Cedillo T, Basurto-Acevedo L, Vega-Garcia S, et al. Prevalence of thyroid dysfunction and its impact on cognition in older Mexican adults: (SADEM study). J Endocrinol Invest. 2017;40(9):945–952. doi:10.1007/s40618-017-0654-6
10. Pasqualetti G, Pagano G, Rengo G, et al. Subclinical hypothyroidism and cognitive impairment: systematic review and meta-analysis. J Clin Endocrinol Metab. 2015;100(11):4240–4248. doi:10.1210/jc.2015-2046
11. van Vliet NA, van Heemst D, Almeida OP, et al. Association of thyroid dysfunction with cognitive function: an individual participant data analysis. JAMA Intern Med. 2021;181(11):1440–1450. doi:10.1001/jamainternmed.2021.5078
12. Biondi B, Cappola AR. Subclinical hypothyroidism in older individuals. Lancet Diabetes Endocrinol. 2022;10(2):129–141.
13. Wardlaw JM, Smith C, Dichgans M. Small vessel disease: mechanisms and clinical implications. Lancet Neurol. 2019;18(7):684–696.
14. Wardlaw JM, Smith EE, Biessels GJ, et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013;12(8):822–838.
15. Ter Telgte A, van Leijsen E, Wiegertjes K, et al. Cerebral small vessel disease: from a focal to a global perspective. Nat Rev Neurol. 2018;14(7):387–398. doi:10.1038/s41582-018-0014-y
16. Quick S, Moss J, Rajani RM, et al. A vessel for change: endothelial dysfunction in cerebral small vessel disease. Trends Neurosci. 2021;44(4):289–305. doi:10.1016/j.tins.2020.11.003
17. Rajani RM, Quick S, Ruigrok SR, et al. Reversal of endothelial dysfunction reduces white matter vulnerability in cerebral small vessel disease in rats. Sci Transl Med. 2018;10:448. doi:10.1126/scitranslmed.aam9507
18. Dagre AG, Lekakis JP, Papaioannou TG, et al. Arterial stiffness is increased in subjects with hypothyroidism. Int J Cardiol. 2005;103(1):1–6. doi:10.1016/j.ijcard.2004.05.068
19. Owen PJ, Sabit R, Lazarus JH. Thyroid disease and vascular function. Thyroid. 2007;17(6):519–524. doi:10.1089/thy.2007.0051
20. Teng Z, Feng J, Liu R, et al. Cerebral small vessel disease mediates the association between homocysteine and cognitive function. Front Aging Neurosci. 2022;14:868777. doi:10.3389/fnagi.2022.868777
21. Teng Z, Feng J, Qi Q, et al. Long-term use of metformin is associated with reduced risk of cognitive impairment with alleviation of cerebral small vessel disease burden in patients with type 2 diabetes. Front Aging Neurosci. 2021;13:773797. doi:10.3389/fnagi.2021.773797
22. Fazekas F, Kleinert R, Offenbacher H, et al. Pathologic correlates of incidental MRI white matter signal hyperintensities. Neurology. 1993;43(9):1683–1689. doi:10.1212/wnl.43.9.1683
23. Gregoire SM, Chaudhary UJ, Brown MM, et al. The Microbleed Anatomical Rating Scale (Mars): reliability of a tool to map brain microbleeds. Neurology. 2009;73(21):1759–1766. doi:10.1212/WNL.0b013e3181c34a7d
24. Doubal FN, MacLullich AM, Ferguson KJ, et al. Enlarged perivascular spaces on MRI are a feature of cerebral small vessel disease. Stroke. 2010;41(3):450–454. doi:10.1161/STROKEAHA.109.564914
25. Staals J, Booth T, Morris Z, et al. Total MRI load of cerebral small vessel disease and cognitive ability in older people. Neurobiol Aging. 2015;36(10):2806–2811. doi:10.1016/j.neurobiolaging.2015.06.024
26. Huijts M, Duits A, van Oostenbrugge RJ, et al. Accumulation of MRI markers of cerebral small vessel disease is associated with decreased cognitive function. a study in first-ever lacunar stroke and hypertensive patients. Front Aging Neurosci. 2013;5:72. doi:10.3389/fnagi.2013.00072
27. Kim JM, Park KY, Kim HR, et al. Association of bone mineral density to cerebral small vessel disease burden. Neurology. 2021;96(9):e1290–1300. doi:10.1212/WNL.0000000000011526
28. Teng Z, Feng J, Dong Y, et al. Triglyceride glucose index is associated with cerebral small vessel disease burden and cognitive impairment in elderly patients with type 2 diabetes mellitus. Front Endocrinol. 2022;13:970122. doi:10.3389/fendo.2022.970122
29. Lu J, Li D, Li F, et al. Montreal cognitive assessment in detecting cognitive impairment in Chinese elderly individuals: a population-based study. J Geriatr Psychiatry Neurol. 2011;24(4):184–190. doi:10.1177/0891988711422528
30. Resta F, Triggiani V, Barile G, et al. Subclinical hypothyroidism and cognitive dysfunction in the elderly. Endocr Metab Immune Disord Drug Targets. 2012;12(3):260–267. doi:10.2174/187153012802002875
31. Floriani C, Gencer B, Collet TH, et al. Subclinical thyroid dysfunction and cardiovascular diseases: 2016 update. Eur Heart J. 2018;39(7):503–507. doi:10.1093/eurheartj/ehx050
32. Lu M, Yang CB, Gao L, et al. Mechanism of subclinical hypothyroidism accelerating endothelial dysfunction (review). Exp Ther Med. 2015;9(1):3–10. doi:10.3892/etm.2014.2037
33. Akintola AA, Jansen SW, van Bodegom D, et al. Subclinical hypothyroidism and cognitive function in people over 60 years: a systematic review and meta-analysis. Front Aging Neurosci. 2015;7:150. doi:10.3389/fnagi.2015.00150
34. Rieben C, Segna D, Da CB, et al. Subclinical thyroid dysfunction and the risk of cognitive decline: a meta-analysis of prospective cohort studies. J Clin Endocrinol Metab. 2016;101(12):4945–4954. doi:10.1210/jc.2016-2129
35. Tang X, Song ZH, Wang D, et al. Spectrum of thyroid dysfunction and dementia: a dose-response meta-analysis of 344,248 individuals from cohort studies. Endocr Connect. 2021;10(4):410–421. doi:10.1530/EC-21-0047
36. Low A, Mak E, Rowe JB, et al. Inflammation and cerebral small vessel disease: a systematic review. Ageing Res Rev. 2019;53:100916. doi:10.1016/j.arr.2019.100916
37. Grochowski C, Litak J, Kamienia P, et al. Oxidative stress in cerebral small vessel disease. role of reactive species. Free Radic Res. 2018;52(1):1–13. doi:10.1080/10715762.2017.1402304
38. Chu M, Cai Y, Zhong J, et al. Subclinical hypothyroidism is associated with basal ganglia enlarged perivascular spaces and overall cerebral small vessel disease load. Quant Imaging Med Surg. 2022;12(2):1475–1483. doi:10.21037/qims-21-190
39. Zhang X, Xie Y, Ding C, et al. Subclinical hypothyroidism and risk of cerebral small vessel disease: a hospital-based observational study. Clin Endocrinol. 2017;87(5):581–586. doi:10.1111/cen.13383
40. Staals J, Makin SD, Doubal FN, et al. Stroke subtype, vascular risk factors, and total MRI brain small-vessel disease burden. Neurology. 2014;83(14):1228–1234. doi:10.1212/WNL.0000000000000837
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.